Melody Smith and Dean Bajorin
Definition
• Often presents as a painless lump or ulcer on the penis
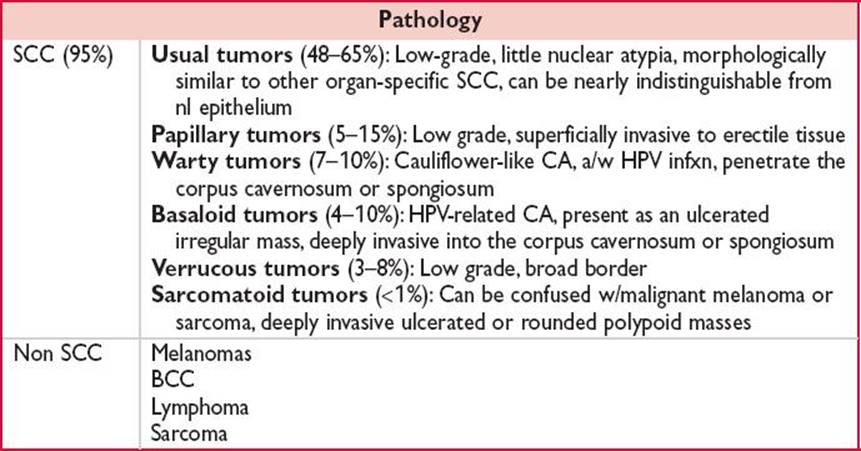
• Majority consist of 1° epithelial SCC
Epidemiology
• Rare in industrialized countries & more common in less developed nations (J Am Acad Dermatol 2006;54:369)
• In US, less than 1% of CA in men
• Disease of older men w/mean dx of 60 y but not uncommon among younger men
Molecular Biology
• Mt in p16 & p53 a/w the development of penile CA
• Increased expression of protein p16NK4A, w/c is encoded by p16 gene, has been seen as a late event of HPV infxn
Risk Factors
• No circumcision or performed at an older age, single, never married, phimosis, HPV or HIV infxn, prior h/o genital warts, h/o penile injury or trauma, known urethral stricture, poor hygiene, tobacco exposure
Diagnosis
• Require careful examination of penis & palpation of inguinal LN
• Need bx of penile CA 1° ± bx of inguinal LN
Prognostic Factors
• Prognosis dictated by grade, stage, lymphovascular invasion, palpable LN (Urology 2010;76:S15)
Workup
• Bx of penile lesion is needed for T stage
• Staging of inguinal nodes is performed by FNA, DSNB (Urologic oncology 2012. pii: S1078–1439 [Epub ahead of print]), or superficial inguinal node dissection
• Staging of regional nodes in men w/a clinically negative inguinal exam is based on risk of occult nodal mets
• Risk of inguinal node positivity is greater w/T2 or greater
• Low-risk disease w/clinically suspicious adenopathy
• Clinically negative nodes does not r/o metastatic disease
• High-risk disease w/clinically suspicious adenopathy
• Nodes can be evaluated by FNA, SNB or superficial inguinal node dissection
• Positive FNA, SNB, or dissection warrants definitive surgical tx
Staging
• Stage I: Involvement of the connective tissue
• Stage II: Involvement of the erectile tissue or to the urethra
• Stage III: Any positive LN
• Stage IV: Spread to tissues near the penis, pelvic area, pelvic LNs, or distant spread
Management
• 1° goal of management is to eliminate malignancy while ensuring a cosmetically acceptable & functional penis
• T stage
• T1: Management of 1° is largely surgical w/a wide local excision but brachytherapy can be considered
• T2 or greater: Partial or total penectomy
• Local disease: Organ preserving strategies can be considered optimally for tumors that are Tis, Ta, or T1 grade 1–2 or for select distal T2–T3 tumors
• Regional disease: Chemotherapy followed by surgery
• Met disease: Chemotherapy ± radiotherapy
• Common chemotherapeutic agents (Urology annals 2012;4:150)
• Cisplatin
• Paclitaxel
• Ifosfamide
• 5-FU
• Combination Rx is frequently used
• Bulky disease (node size ≥4 cm) or unresectable LAN: Proceed w/medical tx
Prognosis in Metastatic Disease
• Median OS 6 mos. Met disease is uncommon until late in the disease course, 1–10% of cases p/w stage IV disease.