Neil M. Bressler,
Susan B. Bressler,
Evangelos S. Gragoudas
Although most patients with age-related macular degeneration (AMD) manifest only drusen or abnormalities of the retinal pigment epithelium (RPE), the majority of patients who are at risk for severe loss of vision from AMD can lose vision because of the development of choroidal neovascularization (CNV) and related manifestations such as serous or hemorrhagic detach-ment of the RPE and fibrovascular disciform scarring. The pathogenesis, clinical features, differential diagnosis, impact on quality of life, and mangement of the neovascular form of AMD are reviewed in this chapter. (The nonneovascular form of AMD, including drusen and abnormalities of the RPE such as geographic atrophy, is reviewed in Chapter 144).
PATHOGENESIS
PATHOGENESIS OF DEVELOPMENT OF CNV
The understanding of the pathogenesis of the development of CNV continues to evolve. In part, clinical[1-5] and histologic reports[6-9] suggest that the presence of diffuse thickening of the inner aspect of Bruch's membrane (associated with large, soft drusen clinically) predisposes Bruch's membrane to develop cracks through which ingrowth of new vessels from the choriocapillaris can occur. This hypothesis is supported by the finding of CNV in other pathologic entities in which breaks in Bruch's membrane occur, such as pathologic myopia[10] and angioid streaks.[11] However, it is unlikely that a break in Bruch's membrane alone necessarily predisposes to the development of CNV. Histologic studies have shown that in eyes with AMD, breaks in Bruch's membrane can be identified not only in areas of CNV but also in areas in which no new vessels can be identified.[6]
Experimental studies have also suggested that other cellular processes may have a role in the development of the CNV beyond merely a disturbance in Bruch's membrane. Laboratory studies have shown that endothelial cells can elaborate enzymes necessary for the digestion of a basement membrane such as Bruch's membrane.[12] This finding would support the concept that endothelial cells from the choriocapillaris could produce a break in Bruch's membrane, rather than presuming that CNV grows only through preexisting breaks in Bruch's membrane. Other reports have suggested that a granulomatous inflam-matory response to degenerated Bruch's membrane may be an important factor in the development of CNV. In histologic studies, eyes with AMD had an increased prevalence of lymphocytes, macrophages, and fibroblasts within Bruch's membrane when compared with control eyes without AMD.[13-15] These findings would suggest that a low-grade chronic inflammatory response may be involved in the development of AMD, although inflammation has a role in the involutionary process of CNV (see end of this section on Pathogenesis). Although inflammatory cells have been shown histologically to be associated with the presence of the nonneovascular and neovascular stages of AMD, studies have not shown that inflammatory cells necessarily are directly linked to the devel-opment of CNV. Therefore, these studies cannot determine whether these inflammatory cells represent a response to existing degenerative changes within Bruch's membrane or whether the inflammatory cells act as essential mediators of degeneration, with subsequent development of CNV.
Experimentally produced CNV developing around retinal laser burns in the monkey eye have also shown the presence of macrophages at the site of developing CNV.[16,17] Again, it is not known whether these macrophages represent a response to damaged retina from a laser burn or whether they act as mediators of CNV. Also, this model of CNV differs from CNV in AMD in that experimentally produced CNV proliferates internal to the RPE (between the sensory retina and the RPE),[16] whereas CNV associated with AMD initially proliferates external to the RPE (within the thickened inner aspect of Bruch's membrane).[6-8]
A relationship of scleral rigidity with CNV in AMD has been suggested in a pilot study in which increased scleral rigidity was found to be associated with the presence of AMD.[18] The possibility of compromised blood flow in the vortex veins by progressively increased scleral rigidity was hypothesized to account for these findings, but further investigation is required.
Results from epidemiologic studies[19] also demonstrated that the risk of CNV is associated with low blood levels of micronutrients with antioxidant potential, cigarette smoking, and risk factors for cardiovascular disease. Systemic hypertension also has been reported to be a risk factor for developing CNV in the fellow eye of a patient who presents with CNV in the first eye.[2] Decreased risk was associated with higher levels of carotenoids and use of postmenopausal exogenous estrogens in women. The associations with estrogens, cigarette smoking, and serum cholesterol are intriguing because sphingomyelins and cholesterol esters similar to those found in arteriosclerotic plaques are found in aging sclera.[20] Perhaps these factors in some way account for increased scleral rigidity.
PATHOGENESIS OF PROGRESSION OF CNV
While understanding the development of CNV continues to evolve, researchers have developed a theoretical construct that correlates the growth pattern of CNV with the pathobiologic dynamic stages of CNV progression.[21] Although no two CNV growth patterns are identical, two distinct patterns of CNV have been defined. The first pattern involves growth into the plane between the RPE and Bruch's membrane (sub-RPE, or type 1). The second pattern involves growth between the retina and RPE (subretinal, or type 2). This description of CNV growth patterns represents a spectrum, and it should be noted that both patterns do not necessarily occur in temporal sequence, i.e., subretinal (type 2) may precede sub-RPE (type 1). Also, subretinal and sub-RPE CNV may be present in the same eye, and there may be (and often are), several foci of sub-RPE CNV.[21] Patients with sub-RPE CNV may have few visual symptoms, as is most often seen in some cases imaged on fluorescein angiography with a lesion composition described as occult CNV or with no classic CNV (see section below describing lesion composition on fluorescein angiography of CNV). CNV may be difficult to detect angiographically due to the subtle patterns of fluorescence sometimes associated with occult CNV.[21] This growth pattern is thought to provide nutrients and oxygen to an ischemic RPE/outer retina that is expressing vascular endothelial growth factor (VEGF) and other angiogenic cytokines.[21] The subretinal growth pattern is characterized by CNV occurring between the retina and RPE; tufts of CNV break through Bruch's membrane and extend laterally under the RPE. The subretinal growth pattern of CNV typically has one or a few ingrowth sites.[21] This pattern is characterized by a break in Bruch's membrane, with proliferation of granulation tissue into the subretinal space, and vascular leakage under the RPE/outer retina, leading to relatively acute visual symptoms.[21]
SUMMARY OF VEGF ROLE FROM ANGIOGENESIS/GROWTH TO INHIBITORY (ANTIANGIOGENIC) MODE IN UNTREATED CNV
Over time, different factors have been implicated in the dynamic process of CNV growth. This dynamic nature is characterized by progression from an angiogenesis/growth promotion mode to an inhibitory (or antiangiogenic) mode, and is incompletely understood.[21] However, it is clear that growth factors are associated with progression of CNV.[22] Recent evidence suggests a central role of VEGF (also called VEGF-A), in the development of CNV. VEGF-A is highly regulated by hypoxia, an important benchmark condition necessary for vascularization in general. Experimental findings suggest that hypoxia is involved in a feedback mechanism to accommodate insufficient tissue oxygenation by promoting vessel formation under normal conditions. It is hypothesized that derailment of this feedback mechanism may lead to uncontrolled angiogenesis in neovascular AMD.[22] The vascular endothelial growth factor family includes placenta growth factor (PIGF) VEGF-A, VEGF-B, VEGF-C, VEGF-D, and the viral VEGF homolog VEGF-E).[22] In the human, four isoforms of VEGF-A have been identified: VEGF121, VEGF165, VEGF189, and VEGF206.[22] The role of these growth factors in AMD and tumor progression is an area of active research. However, VEGF has been implicated in the process of pathologic vessel growth in both experimental animal models and in humans.[23] VEGF appears to be causal for the blood-retina barrier breakdown that accompanies neovascular-ization, as well as that which develops independent of it.[23] Other important factors implicated in neovascularization include platelet-derived growth factor (PDGF) and the angiopoietins.[23] Evidence for the roles of these various growth factors in neovascular AMD suggests a therapeutic use for novel drugs aimed at these targets. Pharmaceutical companies have already developed anti-VEGF treatments for the eye. Taken together, research findings suggest an important role for VEGF-A as a suitable candidate for targeted antiangiogenic therapy in AMD patients.[22]
In the early stages of CNV development, VEGF is produced by the RPE and retinal photoreceptors. The RPE also produces monocyte colonization protein (MCP) and interleukin-8 (IL-8). Monocytes (or macrophages) express tumor necrosis factor a, which in turn stimulates IL-8, MCP, and VEGF production by the RPE. VEGF signaling produces other responses, including proliferation and migration of vascular endothelium.[23] Vasculogenesis may also play a role in CNV. Recent evidence supports a role for hematopoietic stem cells (HSC) in the pathobiology of CNV, and these stem cells express the functional VEGF-1 receptor.[21] After this initiation stage, CNV progresses to an inflammatory active stage. At this point, CNV digests through other tissue planes, and macrophages express tissue factor, a protein involved in fibrogenesis, leading to a fibrin scaffold on which CNV grows.[21] Additionally, growth factors are expressed by the RPE and vascular endothelium, including PDGF, angiopoietins,[23] aFGF, bFGF, and transforming growth factor beta.[21] During this stage, CNV stabilizes, and equilibrium appears to be established between the various growth and other factors that are released.[21]
At some point, the balance shifts toward antiangiogenic, antiproteolytic, and antimigratory activity, resulting in the inflammatory inactive or involutional stage of CNV. The CNV may become collagenized and form a disciform scar.[21] The whole process may be orchestrated by the RPE, including the initiation, stabilization, and involution of CNV, much like a 'traffic cop'.[21]
Regardless of the pathogenesis of CNV in AMD, clinico-pathologic correlative studies[6-9,24] and natural history studies[3,25-29] have shown that untreated CNV is often accompanied by the ingrowth of fibrous scar tissue, eventually resulting in a disciform scar. This CNV-scar complex may have a variety of complex clinical and angiographic appearances. An understanding of these clinical features (described in the next section) is critical in the identification, proper management, and treatment of the choroidal neovascular form of AMD.
CLINICAL FEATURES
SYMPTOMS OF CNV
CNV should be suspected in any patient (usually >65 years with large, soft drusen) who complains of metamorphopsia, central or paracentral scotoma, or any sudden, nonspecific change in central vision.[30,31] Any of these symptoms should alert the ophthalmologist to look for signs of CNV, which are outlined further on. However, not all patients with CNV will be symptomatic[32] or will note changes of metamorphopsia on home-testing with an Amsler grid.[33] Therefore, even asymptomatic patients older than 65 years with large, soft drusen on clinical examination should probably be scrutinized for signs of CNV on periodic examination.
SIGNS OF CNV
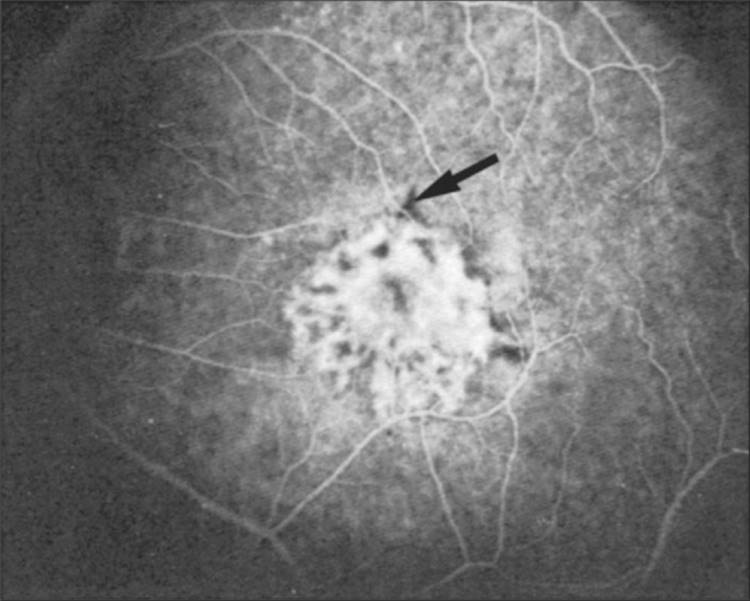
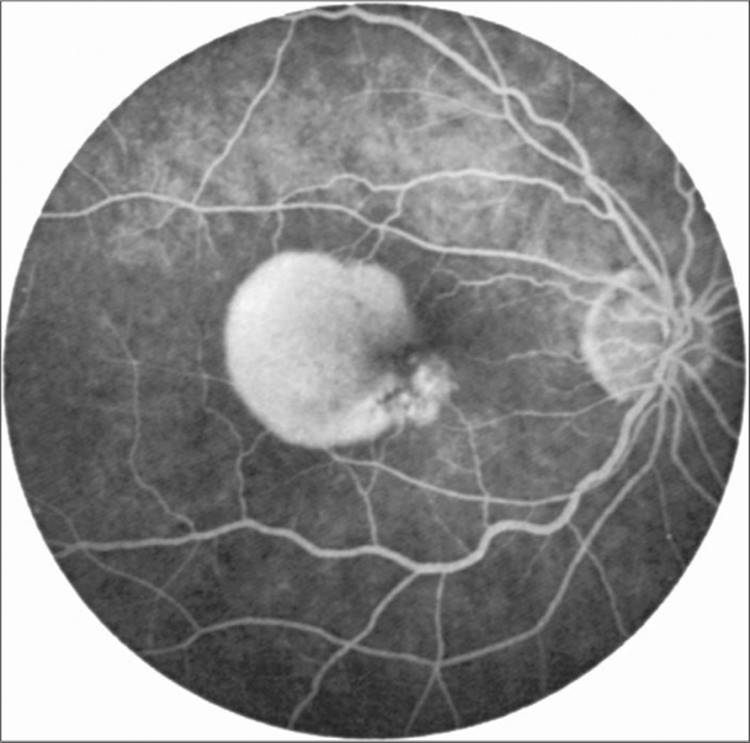
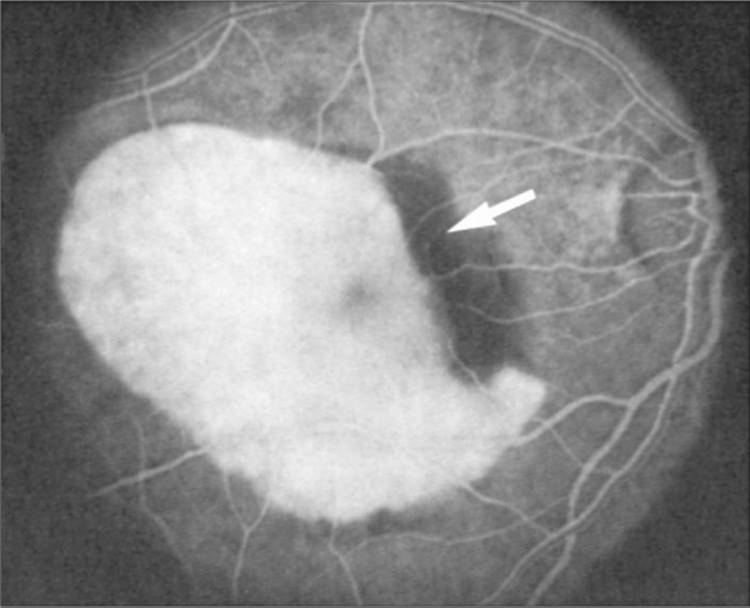
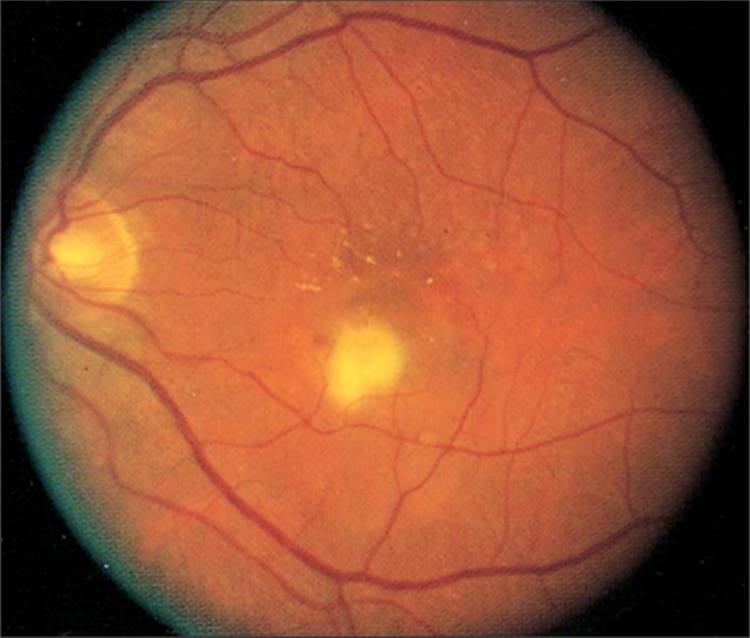
In the early stages of the untreated neovascular form of AMD, before disciform scarring has developed clinically, biomicroscopic clues to the presence of CNV may include any or all of the following: the presence of subretinal or intraretinal lipids, elevation of the RPE, cystic changes in the sensory retina, or visualization of the choroidal neovascular lesion itself. The lesion may be seen as a yellow-green discoloration frequently surrounded by a pigmented ring and is often visualized best with transillumination of the RPE with a thin slit beam on biomicroscopy. The presence of subretinal or sub-RPE blood may be so extensive as to obscure all other signs of CNV; often though, this blood, if present, will be along the periphery of the CNV (Fig. 146.1). Other causes of subretinal or sub-RPE hemorrhage should be ruled out, including macroaneurysms, lacquer cracks in pathologic myopia, traumatic choroidal rupture, choroidal tumors, or subretinal hemorrhage within areas of geographic atrophy when no CNV is seen on angiography. (Presumably, the subretinal hemorrhage within areas of geographic atrophy without CNV on angiography may be due to CNV obscured by the hemorrhage or to disruption of the choriocapillaris in association with the geographic atrophy.[34])
|
|
|
|
FIGURE 146.1 Subfoveal choroidal neovascularization (CNV) with contiguous blood (arrow). The boundaries of the entire lesion (the CNV and blood) are well demarcated; the entire lesion is less than 3.5 disc areas. The lesion would meet the eligibility criteria of the Macular Photocoagulation Study (MPS). |
Although CNV secondary to AMD often has been described in association with subretinal hemorrhage, many cases may present with little or no hemorrhage, the predominant sign being the more subtle finding of subretinal fluid. Often, one needs a contact lens examination with biomicroscopy and a thin slit beam to detect this subretinal fluid or evidence on optical coherence tomography (OCT). On biomicroscopic examination, the anterior portion of the beam will bow forward convexly, and there will be an increased distance between the surface of the slit beam, which is visualized on the surface of the sensory retina, and the posterior portion of the beam, which is visualized on the surface of the RPE. As subretinal fluid is absorbed at the periphery of the CNV, subretinal lipid may precipitate in a circumferential pattern around the CNV and thereby help to alert the ophthalmologist to the presence of CNV. Other biomicroscopic signs of CNV, as already mentioned, include the elevation of the RPE, presumably caused by the presence of CNV and fibrovascular proliferation beneath the RPE,[24,35] pigment proliferation overlying the CNV,[36] or the actual choroidal neovascular vessels themselves (occasionally seen when the overlying RPE pigmentation is markedly attenuated).
If CNV secondary to AMD is suspected from symptoms or signs, fluorescein angiography is indicated for the following reasons: (1) to confirm the diagnosis of CNV, (2) to determine whether treatment is indicated (as discussed further on), (3) if treatment is indicated, to serve as a guide to treatment response, and (4) rarely, if laser photocoagulation is indicated for well-demarcated symptomatic extrafoveal lesions (see more description below), to guide the placement of photocoagulation.
FLUORESCEIN ANGIOGRAPHIC FEATURES OF CNV
A set of photographs to facilitate the identification of the variety of appearances of CNV secondary to AMD includes (1) a black-and-white stereo pair of the macula obtained with green (monochromatic) filter; (2) rapid-sequence photographs of the macula taken during the dye transit, including at least one stereo pair; (3) stereo pairs of the macula taken at approximately 30, 40, 60, 90, 120, and 180s after dye injection; (4) late stereo pairs of the macula taken at 5 and 10 min after dye injection; and (5) stereoscopic color fundus photographs of the macula.[37] Since CNV growth can be a continuous process,[38,39]the size of the CNV and the lesion composition can change within a short time. Therefore, a fluorescein angiogram should ideally be obtained within 2 weeks of initiation of treatment, unless laser photocoagulation is considered, in which case angiography should be performed ideally on the same day as any contemplated laser treatment and probably no more than 96h before treatment.
Two basic angiographic patterns of CNV, recognized in the macular photocoagulation studies[37,40,41] as well as photo-dynamic therapy trials,[42] the submacular surgery trials, 43 trials evaluating anti-VEGF treatments[44-46] and described by independent investigators,[24,27,30,31,47-49] include classic and occult CNV.
Classic CNV
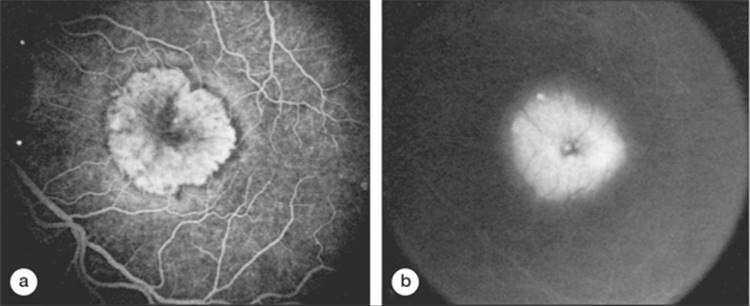
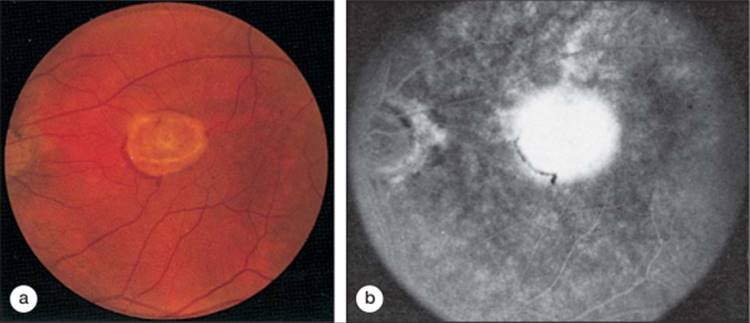
This condition is characterized by an area of well-demarcated hyperfluorescence that can be discerned in the early phase of the angiogram (Fig. 146.2a) with progressive dye leakage pooling in the overlying subsensory retinal space (Fig. 146.2b). The dye leakage identified by the late phase of the angiogram will obscure the borders of the classic CNV detected in the early phase of the angiogram. Only occasionally will fluorescein angiography identify the actual capillary network of the CNV secondary to AMD. This latter observation is contrary to the widely held view that CNV presents angiographically as a lacy network of vessels. This lacy pattern may be seen commonly in CNV secondary to other pathologic entities, such as the ocular histoplasmosis syndrome, but is unusual in AMD.
|
|
|
|
FIGURE 146.2 Classic CNV. (a) Early phase of a fluorescein angiogram of classic CNV in which the boundaries of the neovascular lesion are well demarcated. (b) Late phase of the angiogram shows pooling of dye in the subsensory retinal space, obscuring the boundaries of CNV demarcated in the earlier phase of the angiogram. |
OCCULT CNV
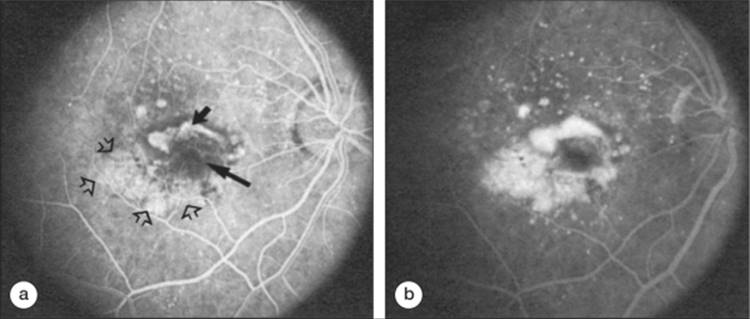
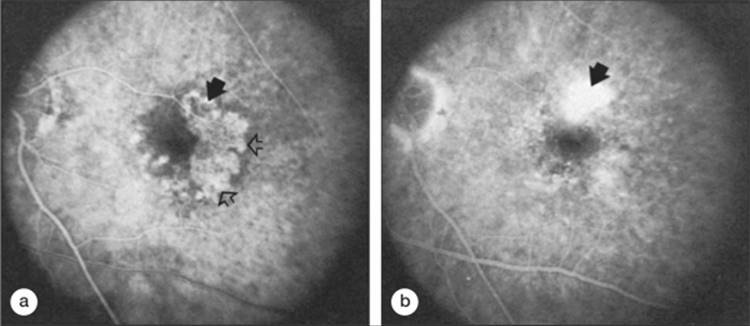
This condition encompasses a variety of fluorescein angiographic appearances that do not conform to the classic description of CNV. The occult forms may be categorized into fibrovascular pigment epithelial detachments (PEDs) and late leakage of undetermined source. In fibrovascular PEDs (Fig. 146.3), areas of irregular elevation of the RPE are often most easily detectable on stereoscopic fluorescein angiography. These areas usually are not as discrete or bright as areas of classic CNV in pictures taken during the transit; by 1-2 min after fluorescein injection, an area of stippled hyperfluorescence becomes apparent (Fig. 146.3b). By 10 min, there is persistence of fluorescein staining or leakage within a sensory retinal detachment overlying this area. These fibrovascular PEDs should not be confused with serous PEDs (discussed further on).
|
|
|
|
FIGURE 146.3 Recurrent classic and occult CNV (with fibrovascular pigment epithelial detachment (PED)). (a) Early phase of fluorescein angiogram shows areas of classic CNV (small solid arrow), scar from prior laser treatment (large solid arrow), and irregular elevation of the retinal pigment epithelium (RPE) with stippled hyperfluorescence (open arrows) representing fibrovascular PED inferotemporal to the scar. (b) One minute after fluorescein injection, fluorescein leakage is apparent from the classic CNV, and increased intensity of stippled hyperfluorescence corresponding to fibrovascular PED is noted. The boundaries of the fibrovascular PED remain well demarcated. At each clock hour, the boundary of the lesion is clearly demarcated and would meet eligibility criteria in the MPS trials. |
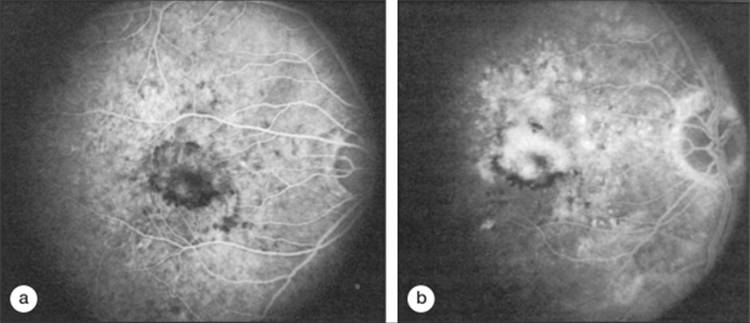
Late leakage of undetermined source consists of areas of late choroidal fluorescein leakage, often appearing as speckled hyperfluorescence, with pooling of dye in the overlying subsensory retinal space, in which there is no discernible, discrete, well-demarcated area of hyperfluorescence that might be considered the source of leakage from earlier photography (Fig. 146.4).
|
|
|
|
FIGURE 146.4 Occult CNV with late leakage of undetermined source. (a) Early phase of the angiogram. (b) Middle phase of the angiogram shows pinpoints of speckled hyperfluorescence and larger areas of hyperfluorescence with accumulation of fluorescein leakage in the overlying subsensory retinal space. The source of the leakage cannot be discerned from earlier phases of the angiogram. The lesion does not meet the MPS eligibility criteria that the boundaries of neovascularization be well demarcated. Therefore, treatment is not considered for this lesion. |
Numerous clinicopathologic correlations on postmortem examination[8,9] or after submacular surgical removal of CNV[50,51] have confirmed that all of these angiographic patterns (classic CNV, fibrovascular PED, and late leakage of an undetermined source) correlate with fibrovascular tissue. These studies have not identified pathologic features to differentiate classic from occult CNV. When adequate stereoscopic photographs are obtained, recognizing a pattern of fibrovascular PED rather than late leakage of an undetermined source might depend on the thickness[9] of the fibrovascular tissue, with thicker tissue corresponding to a pattern of fibrovascular PED on fluorescein angiography.
ANGIOGRAPHIC FEATURES THAT OBSCURE THE BOUNDARIES OF CNV
Three features can obscure the boundaries of CNV and are important to recognize when attempting to delineate the boundaries of the choroidal neovascular lesion. They include (1) blood contiguous with the CNV that is thick enough to obscure the normal choroidal fluorescence, (2) elevated areas of blocked fluorescence due to hyperplastic pigment or fibrous tissue, and (3) a serous detachment of the RPE (Fig. 146.5). The first two of these features block the angiographic view of choroidal fluorescence. Lesions which are predominantly hemorrhage, or predominantly serous PED (serous PED is an area of uniform bright fluorescence in the early phase, with staining of this area in later phase frames) have not been subject to trials evaluating treatments. However, often areas of occult CNV that are irregular elevations of the RPE may be confused with a serous PED if one does not realize that a fibrovascular PED (a form of occult CNV) has a stippled, nonuniform fluorescence, often not visible, and certainly not uniformly bright, in the early phase frames. Such areas of fibrovascular PED were considered occult CNV, not an area of serous PED, and were subjected to trials evaluating treatments. The bright, reasonably uniform early hyperfluorescence associated with a serous detachment of the RPE (described further on) may obscure hyperfluorescence from classic or occult CNV and interfere with the ability to judge whether CNV extends under the area of the serous detachment.
|
|
|
|
FIGURE 146.5 Early-phase fluorescein angiogram of a serous detachment of the RPE. A uniform elevation of the RPE, with uniform pooling of fluorescein dye, and a smooth contour to the surface of the elevated RPE, with well-demarcated borders in the early phase of the angiogram, are noted. The nasal aspect of the lesion shows irregular elevation of the RPE with mottled and speckled fluorescence indicative of occult CNV. |
Thus, lesions which were predominantly serous PED, predominantly hemorrhage, or predominantly scar were excluded from trials evaluating treatments for CNV and it may not be appropriate to extrapolate results of trials that excluded these lesions in the management of them. On the other hand, one should include fibrovascular PEDs as occult CNV and make treatment decisions as described for occult CNV below based on trials evaluating treatments that included occult CNV defined in this way.
OTHER CLINICAL AND ANGIOGRAPHIC FEATURES OF CNV SECONDARY TO AMD
STAINING SCAR
Given variable amounts of time, as the lesion develops obvious scarring on examination or fundus photographs, the composition of the lesion may include staining of this scar rather than having the scar block fluorescence when a lot of pigment or pigment epithelium is within the scar. When a majority of the lesion is composed of scar that stains on fluorescein angiography, such lesion is described as being predominantly scar and has not been subjected to trials evaluating treatments.
FADING CNV
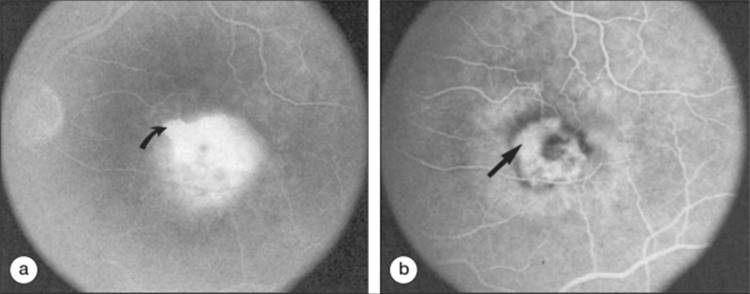
CNV occasionally may be recognized in the early- or middle-transit phase of the angiogram with fading in the late phase, so that no leakage can be discerned in the area that was presumed to harbor CNV[37](Fig. 146.6). These areas most likely represent CNV histologically, but without evidence of subretinal fluid or late leakage, one cannot be sure that this pattern definitively represents CNV.
|
|
|
|
FIGURE 146.6 Fading fluorescence of CNV. (a) Early phase of the angiogram shows classic CNV (solid arrow) with contiguous areas of slightly elevated hyperfluorescent RPE (open arrows), presumably representing a fibrovascular PED, and other less well demarcated areas of hyperfluorescence nasal to fovea. (b) Later phase of the angiogram shows fluorescein leakage from classic CNV (arrow). However, areas of elevated hyperfluorescent RPE noted on the early phase of the angiogram begin to fade in the later phase. Faded areas are not considered a lesion component to be treated in 1991 by MPS treatment protocol because hyperfluorescence does not have enough leakage or staining in the late phase of the angiogram to be considered occult CNV. Before 1988, most ophthalmologists would have considered treatment of the classic CNV with late leakage (arrow). By current interpretations, treatment of the area of classic CNV still might be contemplated, but ophthalmologists would be concerned about the untreated areas of presumed occult CNV that fade in the late phase of the angiogram. |
FEEDER VESSELS
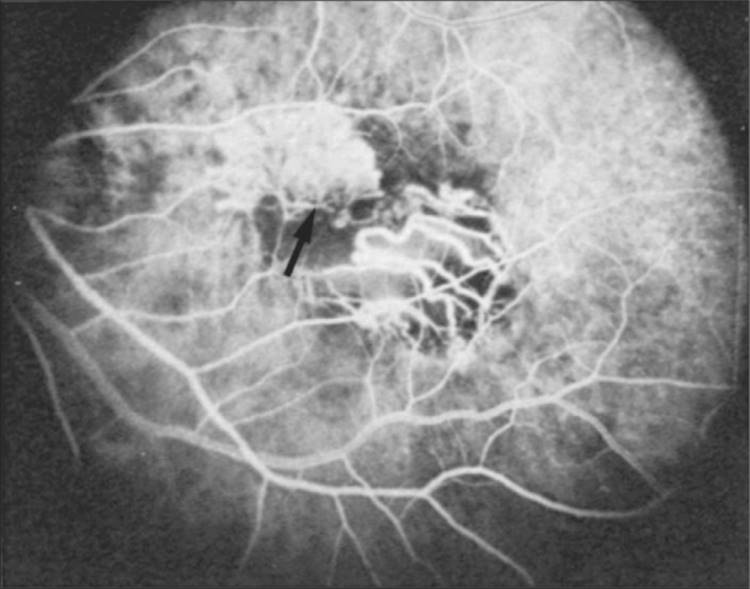
These vessels may be identified as choroidal vessels apparent during the transit phase of the angiogram connected unequivocally to leaking choroidal capillaries (Fig. 146.7). Although feeder vessels have been described as extending from a laser-treated area to recurrent CNV across the perimeter of the laser-treated area,[30,37,52] feeder vessels may also be seen in untreated eyes. In the latter situation, peripheral untreated areas of CNV may be connected by feeder vessels to more central areas of CNV that are evolving toward natural scar formation.37
|
|
|
|
FIGURE 146.7 Recurrent CNV with feeder vessel (arrow) as well as larger choroidal vessels seen within the central portion of the scar from previous laser treatment. |
LOCULATED FLUID
This fluid consists of a well-demarcated area of hyper-fluorescence that appears to represent pooling of fluorescein in a compartmentalized space anterior to the choroidal neovascular leakage.[53] Although the loculated fluid may conform to a pattern of typical cystoid macular edema, it can also pool within an area deep to the sensory retina in a shape that does not bear any resemblance to cystoid macular edema[53] (Fig. 146.8).
|
|
|
|
FIGURE 146.8 Example of an eye in which the borders of loculated fluid extend beyond the borders of CNV. In late-transit frames (a), the area of loculated fluid (arrow) extends beyond the area of the borders of the CNV (arrow in (b) as defined in the early-transit phase of the angiogram. |
TEARS OR RIPS OF THE RPE
An acute tear or rip of the RPE may occur spontaneously (Fig. 146.9) or during laser photocoagulation of a choroidal neovascular lesion.[54-59] Visual acuity may fall precipitously, especially when associated CNV has an opportunity to destroy foveal photoreceptors. When there is no CNV, RPE tears through the fovea may be associated with preservation of good central visual acuity provided that the torn area, and not the scrolled-up RPE, underlies the foveal center.[60] Angiography demonstrates early, bright, sharply demarcated hyperfluorescence within the torn region. Blocked fluorescence corresponding to heaped-up RPE will be noted at one side of the lesion. The bright hyperfluorescence presumably corresponds to fluorescein dye within the choriocapillaris that quickly leaks into the choroidal and scleral tissues and is not blocked by pigment that is normally otherwise present within the overlying RPE. No leakage of dye is seen if no overlying sensory retinal detachment is present. The lack of a sensory retinal detachment over a tear of the RPE may be due to the higher osmotic pressure of the choroid compared with that of the subretinal space, which allows fluid to be removed from the subretinal space at a rapid rate when the tight junctions of the RPE are lacking and unable to prevent free movement of fluid.61
|
|
|
|
FIGURE 146.9 RPE tear seen on the early-transit phase of the fluorescein angiogram demonstrates extremely sharp, well-demarcated hyperfluorescence. Continued intense staining was seen in the late phase of the angiogram with no leakage. An early blocked fluorescence (arrow) presumably corresponds to the redundant, folded, torn RPE. |
DISCIFORM SCAR
The term disciform scar is used to describe the yellow-white fibrous tissue that often accompanies CNV and is an extension of the description of 'scar' above. The lesion may also contain brown or black pigment, depending on the degree of pigment proliferation from the RPE within the scar. The disciform scarring may have a variety of appearances depending on its location within the retina (sub-RPE or subretinal), the degree of associated CNV with the scarring, the presence of chorioretinal anastomosis within the scar, or the amount of RPE atrophy accompanying the scar (Fig. 146.10). The natural course of most choroidal neovascular lesions secondary to AMD consists of scarring within the central portion of the lesion with continued signs of active CNV at the periphery of the lesion (including subretinal fluid, hemorrhage, or lipid). Therefore, most disciform scars secondary to AMD could be termed CNV-scar when they include both a fibrous component noted on biomicroscopy and a neovascular component represented by subretinal fluid-hemorrhage-lipid on biomicroscopy and accompanied by leakage from CNV on angiography (Fig. 146.10b). Occasionally, these disciform scars may develop anterior to the posterior pole. These peripheral disciform scars may become quite large with irregular shapes or they may be accompanied by hemorrhage, leading to the suspicion of a tumor such as a melanoma, until they are evaluated with ultrasound (see further on).
|
|
|
|
FIGURE 146.10 CNV-disciform scarring. (a) Subretinal and sub-RPE fibrosis, as well as subretinal fluid and hemorrhage, is seen on the color photograph. The latter presumably are indicative of persistent vascular tissue within the fibrosis. (b) Fluorescein angiography of CNV scarring demonstrates leakage toward the periphery of the lesion, presumably from CNV associated with the scarring. |
VITREOUS HEMORRHAGE
Occasionally, hemorrhage from CNV or CNV scarring extends into the vitreous space.[62,63] Any patient with a massive vitreous hemorrhage in one eye and features of AMD in the fellow eye should be suspected of harboring CNV in the eye with vitreous hemorrhage. Ultrasonography should be performed to rule out a rhegmatogenous retinal tear or detachment, choroidal melanoma, and other less common causes of vitreous hemorrhage. Sonographically, the posterior pole or peripheral lesion is relatively flat and broad-based, with a fairly homogeneous pattern and without signs of choroidal excavation. The vitreous hemorrhage clears in approximately 75% of patients. If the hemorrhage does not clear, a vitrectomy to restore peripheral vision should be considered, taking into account how restoration of that peripheral vision will improve the patient's quality of life, given the unlikelihood of restoration of central vision. Whether or not submacular surgery should be considered to remove any subretinal hemorrhage or fibrovascular tissue identified at the time of vitrectomy probably should await results of clinical trials evaluating the benefits and risks of this intervention.
RPE DETACHMENTS IN AMD
Various changes in AMD may result in elevation or detachment of the RPE as seen on stereoscopic biomicroscopic or angiographic evaluation. The term RPE detachment secondary to AMD in the ophthalmic literature remains confusing because various RPE detachments may have quite different prognoses and managements, and yet several series may have included some or all of these RPE detachments in their reports. RPE detachments secondary to AMD that may be readily recognized and probably should be differentiated include (1) fibrovascular PEDs, which are a subset of occult CNV (Fig. 146.3); (2) elevated areas of RPE that block fluorescence because of hyperplastic pigment or fibrous tissue (Fig. 146.3); (3) serous detachments of the RPE (Fig. 146.5); (4) hemorrhagic detachments of the RPE, in which blood from a choroidal neovascular lesion is noted beneath or exterior to the RPE; and (5) drusenoid RPE detachments, in which large areas of confluent, soft drusen are noted.[64]
Elevated blocked fluorescence may be differentiated from fibrovascular PEDs and serous detachments of the RPE in that blocked fluorescence is noted within the area of elevated RPE throughout the angiogram. One of the more difficult differentiations is between fibrovascular PEDs and serous detachment of the RPE. Although, they probably have been lumped together in several series that have examined RPE detachments,[65-70] some of these clinical reports have attempted to identify certain features that might distinguish between serous detachments of the RPE and areas of elevation of the RPE that may harbor occult CNV.[67] Using descriptions from the Macular Photocoagulation Study (MPS), fibrovascular PEDs (as a subset of occult CNV) have been distinguished from classic serous detachments of the RPE in that the former have slow filling with a stippled appearance to the surface of the RPE by the middle phase of the angiogram and may show pooling of dye in the overlying subsensory retinal space in the late phase, whereas the latter show uniform, bright hyperfluorescence in the early phase with a smooth contour to the RPE by the middle phase and little, if any, leakage at the borders of the PED by the late phase. As mentioned earlier, the fluorescent pattern of a serous PED obscures the ability to determine whether classic or occult CNV exists within the area of the serous PED.
A hemorrhagic detachment of the RPE will block choroidal fluorescence just as blocked fluorescence from hyperplastic pigment or fibrous tissue does. However, in hemorrhagic detachments of the RPE, the dark appearance on biomicroscopy caused by the mound-like collection of blood beneath the RPE will help to differentiate it from areas of elevated blocked fluorescence caused by hyperplastic pigment or fibrous tissue as discussed previously. Occasionally, a hemorrhagic detachment of the RPE may be mistaken for a choroidal melanoma, but usually hemorrhagic detachments of the RPE will not demonstrate low internal reflectivity, as is seen characteristically in choroidal melanomas.
The final feature of AMD that will appear as an elevated or detached RPE is a drusenoid RPE detachment or extensive areas of large confluent drusen.[64] Drusenoid RPE detachments can be distinguished from serous detachments of the RPE in that drusenoid RPE detachments will fluoresce faintly during the transit and do not progress to bright hyperfluorescence in the late phase of the angiogram. In contrast, serous detachments of the RPE will fluoresce brightly in the early-transit phase and remain brightly hyperfluorescent in the late phase. In addition, serous detachments usually will have a smoother, sharper boundary compared with drusenoid RPE detachments. Drusenoid RPE detachments can be distinguished from fibrovascular PEDs in occult CNV by noting that fibrovascular PEDs will show areas of stippled hyperfluorescence with persistence of staining or leakage within a sensory retinal detachment overlying the area in the late phase of the angiogram. RPE detachments associated with large, soft, confluent drusen are usually smaller, more shallow, and more irregular in outline than are fibrovascular PEDs. In addition, the drusenoid RPE detachments will often have reticulated pigment clumping overlying the large, soft, confluent drusen, and a scalloped border.
IMPACT OF NEOVASCULAR AMD ON QUALITY OF LIFE
Health-related quality of life (QOL), also known as patient-centered QOL, refers to those aspects of life that either foster or compromise the ability to participate fully in daily life, such as driving, recognizing faces, reading small print, judging the depth of stairs or curbs, or watching TV. Because patient-centered QOL is subjective,[71] AMD patients with similar visual acuity (VA) may rate their QOL quite differently, depending on which activities and skills are valued most.[72] To systematically measure health-related QOL, researchers have developed standardized questionnaires that can be self-administered or conducted as an interview.
WHY IS IT IMPORTANT TO EVALUATE QOL IN AMD PATIENTS?
QOL instruments are widely used to assess patients with other chronic diseases that are common in the population at risk for AMD, such as arthritis, depression, cancer, hypertension, and stroke. QOL measures are often added to clinical trials to evaluate the cost-effectiveness and therapeutic value of new treatments.[71] Researchers and clinicians recognize the psychosocial determinants of health, such as the skyrocketing cost of healthcare, and patients' desire to participate more actively in treatment decisions.[73] This has led to active soliciting of patient input about QOL. Patient-reported visual function can reinforce treatment decisions for practitioners, providing evidence of treatment benefits.
Ophthalmologists may underestimate the impact that AMD can have on patients' health-related QOL. In one study,[54] ophthalmologists were asked to imagine that they had AMD in both eyes and were given the hypothetical scenario: regain perfect vision by giving up some remaining lifespan.[74] The same hypothetical scenario was offered to 72 AMD patients. For every 10 years of life remaining, AMD patients with VA of 20/30 to counting fingers would give up more years than would ophthalmologists with the same hypothetical VA (Table 146.1).
TABLE 146.1 -- Time Trade-off Values.[4] Values Represent the Number of Years (of Every 10 Years of Remaining Life Expectancy) That Participants Would Trade for Perfect Vision.
|
Best Corrected VA |
Ophthalmologists (n = 46) |
AMD Patients (n = 72) |
|
20/30 to 20/50 |
0.3 |
1.9 |
|
20/60 to 20/100 |
1.1 |
4.3 |
|
20/200 to 20/400 |
2.3 |
4.9 |
|
Counting fingers to hand motions |
3.3 |
6.0 |
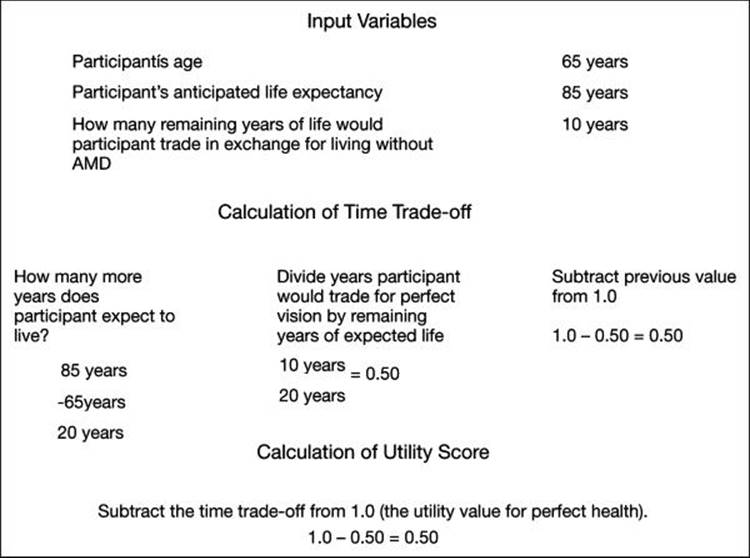
Another way to measure patient-centered QOL is with preference values. In the submacular surgery trials, 996 participants with subfoveal CNV were asked to pretend that they were completely blind at their current level of general health. Participants were also asked to pretend that they had perfect vision and their current level of general health.[75] They rated these hypothetical situations on a scale of 0 (death) to 100 (perfect health with perfect vision). Among the 792 evaluable participants, the mean preference value assigned to current vision with CNV was 0.64.[75] Preference values were higher in younger patients and those with better VA, and lower in patients with anxiety or depression.[75] These mid-range values imply that some CNV patients may consider an expensive or potentially risky treatment to improve their QOL.[75] In a utility study, Brown and colleagues used a time trade-off method, dividing 65 consecutive ambulatory patients into three groups.[76] In the time trade-off technique, the investigator calculates each participant's life expectancy and then asks how many years of remaining life expectancy an individual would be willing to trade in return for perfect vision[77] (Fig. 146.11).
|
|
|
|
FIGURE 146.11 Time trade-off calculation. |
One group, with no light perception (NLP) in at least one eye, was asked to imagine that they had NLP in both eyes. One group had bilateral vision with light perception to counting fingers, and another group had 20/200 to 20/400 vision. Mean utility values were lowest in the group with the worst vision. (Table 146.2) 6 Patients in the NLP group were willing to trade almost three out of every 4 years of remaining life expectancy in return for perfect vision in each eye.[76] Even patients in the 20/200 to 20/400 group would trade one-third of their remaining life expectancy for perfect vision.[76]
TABLE 146.2 -- Time Trade-off Utility Values Stratified by Level of Vision.[6]
|
VA (n) |
Utility Value |
P value[?] |
P value[§] |
|
20/200 to 20/400[*] (33) |
0.65 |
0.6 × 10?12 |
0.03 |
|
LP to counting fingers[*] (17) |
0.47 |
0.007 |
NA |
|
NLP[?] (15) |
0.26 |
NA |
0.007 |
|
LP = light perception; NLP = no light perception. |
|
* |
In the better eye. |
|
? |
NLP in one eye; postulated NLP in other eye. |
|
? |
P value from Student's t test when compared with NLP group. |
|
§ |
P value from Student's t test when compared with LP to counting fingers group. |
THE IMPACT OF AMD ON ACTIVITIES OF DAILY LIVING (ADLS)
Visual changes affect physical function, even in patients with unilateral advanced AMD. The submacular surgery trials interviewed 789 patients with subfoveal CNV to evaluate QOL. Investigators used the National Eye Institute Visual Function Questionnaire (NEI-VFQ). As noted earlier, the NEI-VFQ is a validated questionnaire that assesses physical aspects of health (general health, visual health, pain, and near and distance vision activities), and how visual disability affects mental health, role difficulties, social functioning and dependency, driving, and color and peripheral vision. Scores range from 0 (worst functioning) to 100 (best functioning).[78] Patients with bilateral AMD scored 6-10 points lower on the NEI-VFQ than patients with unilateral AMD even after adjusting for VA.[79] Preventing and or delaying the progression of AMD is crucial to reducing the risk of rapidly declining QOL for patients with vision loss.[79] Cahill and colleagues evaluated patient-centered QOL among 70 patients with bilateral severe AMD using the NEI-VFQ. The mean QOL scores for these important quality of vision (general vision, difficulty with distance and near tasks), and vision-specific subscales (dependency, role difficulties, mental health, social function limitations) were significantly worse for patients with bilateral severe AMD than for patients with AMD of varying severity, and persons without eye disease.[80] These data further support the assertion that visual changes affect physical function even in patients with relatively mild AMD.
THE SOCIAL AND PSYCHOLOGICAL IMPACT OF NEOVASCULAR AMD ON QOL
Not surprisingly, many patients with bilateral advanced AMD, usually neovascular, are hesitant and sometimes unable to drive.[80] Among a group of patients with AMD of mixed severity, there was a direct correlation between higher severity of AMD and poorer scores on the driving activities subscale of the Activities of Daily Vision Scale (ADVS), a 21-item questionnaire about vision-specific activities, including driving in darknessor daylight, and nondriving activities involving distance or near vision, or glare.[81] The loss of driving ability has widespread implications: 1) a decreased ability to care for oneself (eg., earning a living, grocery shopping, getting to doctor appointments) and 2) a decreased ability to care for others, such as a chronically ill, elderly spouse.[82] Data on contrast sensitivity loss for patients with macular disease suggest that patients with moderate visual loss (20/70 to 20/200) may have difficulty recognizing faces.[83] Patients with visual disabilities in general are at risk of becoming socially isolated, due to difficulties with moving around and performing ADLs. The inability to recognize a friend or loved one would also increase feelings of social isolation and impact functioning.[84]
DEPRESSION AND ANXIETY
The fear of progression and potential blindness among AMD patients remains an important factor in patient-centered QOL.[77,85] A subgroup of patients with newly diagnosed subfoveal CNV who participated in the Submacular Surgery Trials had measurable anxiety and depression at baseline. In particular, among the participants who had no prior laser treatment in the affected eye, 60/447 (13%) were classified as having either doubtful or definite anxiety, and 57/447 (12%) as having doubtful or definite depression, using the Hospital Anxiety and Depression Scale.[79] In one study, patients with severe bilateral AMD scored significantly lower in the social and mental health domains of the NEI VFQ-25 than patients with AMD of varying severity and persons without ocular disease.[80]
MANAGEMENT OF CHOROIDAL NEOVASCULARIZATION IN AMD
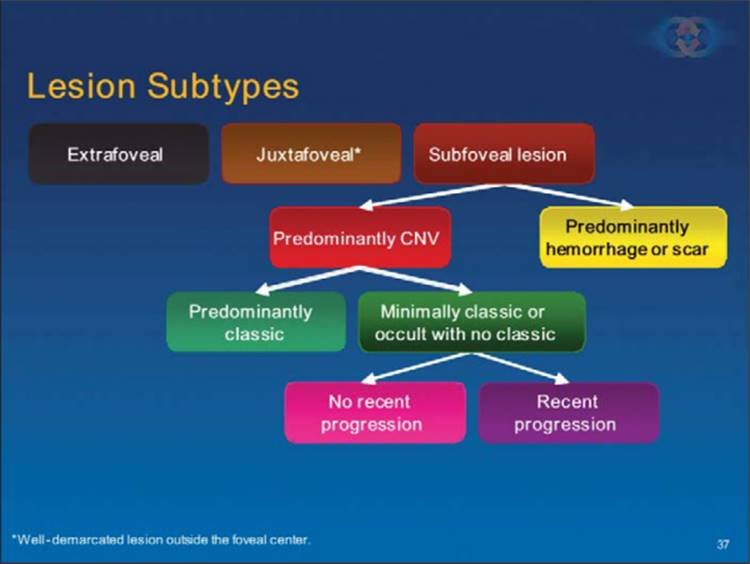
When neovascular AMD is suspected, a fluorescein angiogram is obtained to determine the location of the lesion, and its composition. Following the algorithm outlined in Fig. 146.12 after one determines the entire extent of the lesion, one can determine if the most posterior extent of the lesion is extrafoveal (at least 200 ?m from the geometric center of the foveal avascular zone). While not very common in AMD, in such cases, if the lesion has well-demarcated boundaries, and the patient is symptomatic, then laser photocoagulation is indicated. The immediate goal of laser treatment in all clinical trials evaluating laser use for CNV[38,39,86-91] was to photocoagulate the entire area of CNV. In order to treat the entire area of CNV, the ophthalmologist has to be able to identify the boundaries of the choroidal neovascular lesion. Therefore, at the present time, treatment is indicated only when the boundaries of the CNV are well demarcated. If the boundaries are not well-demarcated, or if one is not certain if the lesion extends under the foveal center, or if the lesion is so close to the foveal center that the treating ophthalmologist believes the scotoma from treatment will outweigh any benefits of treatment, then one could manage the lesion as if its location were subfoveal as described below.
|
|
|
|
FIGURE 146.12 Algorithm for management of CNV in AMD. |
RISKS AND BENEFITS OF TREATMENT OF EXTRAFOVEAL CNV (POSTERIOR BOUNDARY OF CNV BETWEEN 200 AND 2500 ?m FROM GEOMETRIC CENTER OF THE FAZ)
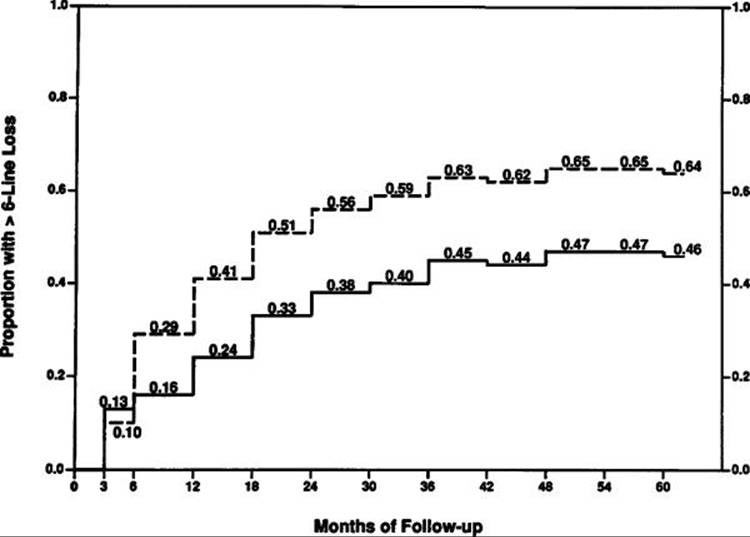
In the MPS, laser treatment was beneficial at decreasing the risk of severe visual loss in eyes with extrafoveal CNV secondary to AMD when compared with no treatment.[88] The proportion of eyes with severe visual loss (6 lines or more of vision loss) 1 year after presenting with extrafoveal CNV was 41% in the eyes assigned to no treatment and 24% in the eyes assigned to laser treatment. By 3 years, 63% of the eyes assigned to no treatment and 45% of the eyes assigned to treatment had severe visual loss. This treatment benefit was maintained by 5 years after treatment, at which time 64% of the eyes assigned to no treatment and 46% of the eyes assigned to treatment had severe visual loss[92] (Fig. 146.13). The relative risk of losing 6 lines or more of visual acuity from baseline among untreated eyes (n = 117) compared with laser-treated eyes (n = 119) was 1.5 from 6 months through 5 years after entry into the study (P =0.001). Furthermore, after 5 years, untreated eyes had lost a mean of 7.1 lines of visual acuity, whereas laser-treated eyes had lost 5.2 lines.
|
|
|
|
FIGURE 146.13 Proportion of eyes at each follow-up examination with a decrease in visual acuity of 6 or more lines from baseline in the Senile Macular Degeneration Study of the MPS. Dashed line indicates eyes assigned randomly at entry to no treatment; solid line, eyes assigned at entry to laser treatment. All eyes at baseline (time zero) had well-demarcated extrafoveal CNV. |
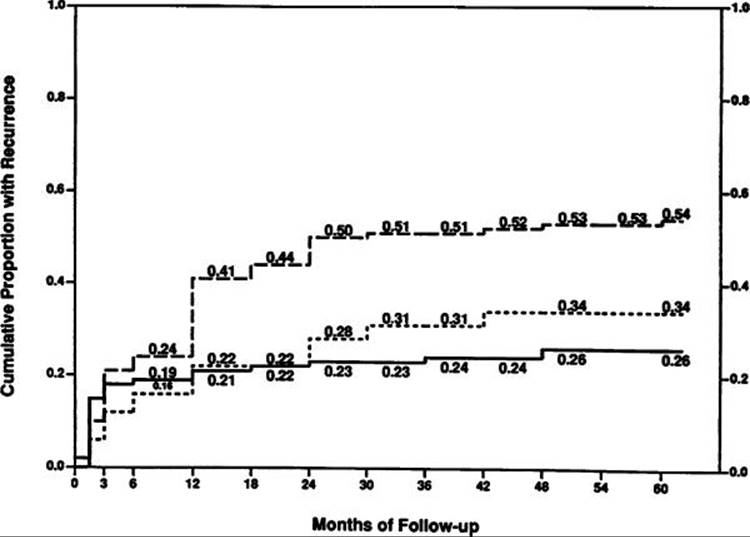
Recurrent CNV was observed in 54% of laser-treated eyes by the end of the 5 year follow-up period[92] (Fig. 146.14). About 75% of all these recurrences occurred by the end of the first year after treatment. An additional 17% of all the recurrences occurred between 1 and 2 years of follow-up. The remaining 7% of all recurrences occurred between the end of the second year and the fifth year of follow-up (Fig. 146.14). The effect of recurrence on visual acuity can be seen in Table 146.3; by 3 years, only 10% of the treated eyes with no recurrence had severe visual loss compared with 80% of the treated eyes with recurrence. At the end of the third year of follow-up, the average visual acuity of the treated eyes with no recurrence was 20/50 and that of the treated eyes with recurrence was 20/250.[92] This treatment benefit has been confirmed by two independent trials comparing treatment and the natural course.[86,87] Although, the treatment protocol did not permit treatment of recurrences through the foveal center in this trial, the treatment benefit for these lesions might have been even greater if anti-VEGF therapies now in use (see below) for subfoveal lesions had been applied to the subfoveal recurrences that would have met current criteria for consideration of treatment of subfoveal lesions.
|
|
|
|
FIGURE 146.14 Cumulative proportion of laser-treated eyes ever having recurrent CNV documented after initial laser treatment. Dashed line indicates eyes assigned to laser treatment in the Senile Macular Degeneration Study in which patients had extrafoveal CNV secondary to AMD. For comparison to a cumulative proportion of recurrences after treatment of CNV secondary to other causes, solid line indicates eyes assigned to laser treatment in the Ocular Histoplasmosis Study, and dotted line, eyes in the Idiopathic Neovascularization Study. |
TABLE 146.3 -- Visual Acuity by History of Recurrence after Laser Treatment of Extrafoveal Choroidal Neovascularization Secondary to AMD
|
Years since Treatment |
Recurrence |
Number of Eyes |
Average Visual Acuity |
Eyes With 6-Line Loss n (%) |
|
1 |
Yes |
62 |
20/40 |
4 (6) |
|
No |
49 |
20/125 |
20 (41) |
|
|
2 |
Yes |
49 |
20/40 |
4 (8) |
|
No |
54 |
20/160 |
31 (57) |
|
|
3 |
Yes |
48 |
20/50 |
5 (10) |
|
No |
46 |
20/250 |
37 (80) |
|
|
4 |
Yes |
43 |
20/50 |
5 (12) |
|
No |
47 |
20/250 |
37 (79) |
|
|
5 |
Yes |
42 |
20/50 |
7 (17) |
|
No |
50 |
20/250 |
39 (78) |
The term persistence was used by the MPS group to indicate the presence of fluorescein leakage on the periphery of the foveal side of the laser-treated area within 6 weeks after treatment. The investigators believed that fluorescein leakage within this time might represent persistence of neovascularization. The MPS investigators chose to use the term recurrence when angiography confirmed no leakage for at least 6 weeks after treatment, with leakage subsequently noted sometime later than 6 weeks after treatment.[93] These terms were strictly defined for analysis of the data from these trials. However, one could consider using the term recurrence whenever the following conditions apply: (1) leakage is seen at the periphery of a laser-treated area and (2) one has previously documented unequivocal lack of peripheral leakage after treatment. A persistence could be defined as leakage at the periphery of the laser-treated area without any prior unequivocal documentation of lack of peripheral leakage on prior fluorescein angiograms.
When treatments with photodynamic therapy or anti-VEGF drugs are applied, then other terms may be used to describe angiographic appearances after treatment[43] Specifically, progression used for leakage from CNV beyond the boundaries of the lesion identified prior to treatment. Absence of leakage implies that there is no progression and no leakage within the area of CNV identified prior to treatment. Minimal leakage means that there is no progression and that less than 50% of the area of leakage from CNV identified prior to treatment still shows fluorescein leakage from CNV. Finally, moderate leakage means that there is no progression and that 51-to 99% of the area of leakage from CNV identified prior to treatment still shows fluorescein leakage from CNV.
MANAGEMENT OF CHOROIDAL NEOVASCULARIZATION IN AMD
When neovascular AMD is suspected, a fluorescein angiogram is obtained to determine the location of the lesion, and its composition. Following the algorithm outlined in Fig. 146.12 after one determines the entire extent of the lesion, one can determine if the most posterior extent of the lesion is extrafoveal (at least 200 ?m from the geometric center of the foveal avascular zone). While not very common in AMD, in such cases, if the lesion has well-demarcated boundaries, and the patient is symptomatic, then laser photocoagulation is indicated. The immediate goal of laser treatment in all clinical trials evaluating laser use for CNV[38,39,86-91] was to photocoagulate the entire area of CNV. In order to treat the entire area of CNV, the ophthalmologist has to be able to identify the boundaries of the choroidal neovascular lesion. Therefore, at the present time, treatment is indicated only when the boundaries of the CNV are well demarcated. If the boundaries are not well-demarcated, or if one is not certain if the lesion extends under the foveal center, or if the lesion is so close to the foveal center that the treating ophthalmologist believes the scotoma from treatment will outweigh any benefits of treatment, then one could manage the lesion as if its location were subfoveal as described below.
|
|
|
|
FIGURE 146.12 Algorithm for management of CNV in AMD. |
RISKS AND BENEFITS OF TREATMENT OF EXTRAFOVEAL CNV (POSTERIOR BOUNDARY OF CNV BETWEEN 200 AND 2500 ?m FROM GEOMETRIC CENTER OF THE FAZ)
In the MPS, laser treatment was beneficial at decreasing the risk of severe visual loss in eyes with extrafoveal CNV secondary to AMD when compared with no treatment.[88] The proportion of eyes with severe visual loss (6 lines or more of vision loss) 1 year after presenting with extrafoveal CNV was 41% in the eyes assigned to no treatment and 24% in the eyes assigned to laser treatment. By 3 years, 63% of the eyes assigned to no treatment and 45% of the eyes assigned to treatment had severe visual loss. This treatment benefit was maintained by 5 years after treatment, at which time 64% of the eyes assigned to no treatment and 46% of the eyes assigned to treatment had severe visual loss[92] (Fig. 146.13). The relative risk of losing 6 lines or more of visual acuity from baseline among untreated eyes (n = 117) compared with laser-treated eyes (n = 119) was 1.5 from 6 months through 5 years after entry into the study (P =0.001). Furthermore, after 5 years, untreated eyes had lost a mean of 7.1 lines of visual acuity, whereas laser-treated eyes had lost 5.2 lines.
|
|
|
|
FIGURE 146.13 Proportion of eyes at each follow-up examination with a decrease in visual acuity of 6 or more lines from baseline in the Senile Macular Degeneration Study of the MPS. Dashed line indicates eyes assigned randomly at entry to no treatment; solid line, eyes assigned at entry to laser treatment. All eyes at baseline (time zero) had well-demarcated extrafoveal CNV. |
Recurrent CNV was observed in 54% of laser-treated eyes by the end of the 5 year follow-up period[92] (Fig. 146.14). About 75% of all these recurrences occurred by the end of the first year after treatment. An additional 17% of all the recurrences occurred between 1 and 2 years of follow-up. The remaining 7% of all recurrences occurred between the end of the second year and the fifth year of follow-up (Fig. 146.14). The effect of recurrence on visual acuity can be seen in Table 146.3; by 3 years, only 10% of the treated eyes with no recurrence had severe visual loss compared with 80% of the treated eyes with recurrence. At the end of the third year of follow-up, the average visual acuity of the treated eyes with no recurrence was 20/50 and that of the treated eyes with recurrence was 20/250.[92] This treatment benefit has been confirmed by two independent trials comparing treatment and the natural course.[86,87] Although, the treatment protocol did not permit treatment of recurrences through the foveal center in this trial, the treatment benefit for these lesions might have been even greater if anti-VEGF therapies now in use (see below) for subfoveal lesions had been applied to the subfoveal recurrences that would have met current criteria for consideration of treatment of subfoveal lesions.
|
|
|
|
FIGURE 146.14 Cumulative proportion of laser-treated eyes ever having recurrent CNV documented after initial laser treatment. Dashed line indicates eyes assigned to laser treatment in the Senile Macular Degeneration Study in which patients had extrafoveal CNV secondary to AMD. For comparison to a cumulative proportion of recurrences after treatment of CNV secondary to other causes, solid line indicates eyes assigned to laser treatment in the Ocular Histoplasmosis Study, and dotted line, eyes in the Idiopathic Neovascularization Study. |
TABLE 146.3 -- Visual Acuity by History of Recurrence after Laser Treatment of Extrafoveal Choroidal Neovascularization Secondary to AMD
|
Years since Treatment |
Recurrence |
Number of Eyes |
Average Visual Acuity |
Eyes With 6-Line Loss n (%) |
|
1 |
Yes |
62 |
20/40 |
4 (6) |
|
No |
49 |
20/125 |
20 (41) |
|
|
2 |
Yes |
49 |
20/40 |
4 (8) |
|
No |
54 |
20/160 |
31 (57) |
|
|
3 |
Yes |
48 |
20/50 |
5 (10) |
|
No |
46 |
20/250 |
37 (80) |
|
|
4 |
Yes |
43 |
20/50 |
5 (12) |
|
No |
47 |
20/250 |
37 (79) |
|
|
5 |
Yes |
42 |
20/50 |
7 (17) |
|
No |
50 |
20/250 |
39 (78) |
The term persistence was used by the MPS group to indicate the presence of fluorescein leakage on the periphery of the foveal side of the laser-treated area within 6 weeks after treatment. The investigators believed that fluorescein leakage within this time might represent persistence of neovascularization. The MPS investigators chose to use the term recurrence when angiography confirmed no leakage for at least 6 weeks after treatment, with leakage subsequently noted sometime later than 6 weeks after treatment.[93] These terms were strictly defined for analysis of the data from these trials. However, one could consider using the term recurrence whenever the following conditions apply: (1) leakage is seen at the periphery of a laser-treated area and (2) one has previously documented unequivocal lack of peripheral leakage after treatment. A persistence could be defined as leakage at the periphery of the laser-treated area without any prior unequivocal documentation of lack of peripheral leakage on prior fluorescein angiograms.
When treatments with photodynamic therapy or anti-VEGF drugs are applied, then other terms may be used to describe angiographic appearances after treatment[43] Specifically, progression used for leakage from CNV beyond the boundaries of the lesion identified prior to treatment. Absence of leakage implies that there is no progression and no leakage within the area of CNV identified prior to treatment. Minimal leakage means that there is no progression and that less than 50% of the area of leakage from CNV identified prior to treatment still shows fluorescein leakage from CNV. Finally, moderate leakage means that there is no progression and that 51-to 99% of the area of leakage from CNV identified prior to treatment still shows fluorescein leakage from CNV.
APPLICATION OF LASER PHOTOCOAGULATION
Preparation
An angiogram is projected onto a screen or monitor near the laser, so that the ophthalmologist can make rapid and repeated extrapolations from the fluorescein's retinal vascular landmarks to the patient's fundus when identifying the location of the CNV with respect to these landmarks. Careful evaluation of vascular landmarks in the patient's fundus in comparison with landmarks concurrently viewed on a projection of a fluorescein angiogram during treatment should enable the ophthalmologist to identify the boundaries of the lesion with confidence and accuracy and avoid inadvertent treatment of retina that is not involved with the lesion.
Topical anesthesia usually is sufficient if one is careful to ensure that neither ocular motility nor patient discomfort will compromise the success of treatment by preventing the ophthalmologist from delivering laser of sufficient intensity and duration of exposure to produce a uniform white treatment burn. This is especially true when small amounts of undertreatment may allow persistence of neovascularization[93,94]or small amounts of overtreatment might obliterate foveal structures unnecessarily.95
Treatment Parameters
Initial laser burns are placed along the boundary of the CNV using a 200 ?m spot size and 0.2-0.5s duration. These parameters allow the ophthalmologist to get sufficient heat to the retina (with the long duration) without risking a sudden break in Bruch's membrane and to minimize the frequency of bleeding (by spreading the intensity of the burn over a 200-?m spot rather than a 50 or 100 ?m spot). The area to be covered, if one is following the protocol used in the MPS, differs depending on the location of the lesion and is outlined in Table 146.4. After the boundaries of the lesion have been treated, the area within the boundaries is treated subsequently with burns of the same spot size or larger, using a duration of 0.5-1s. The desired endpoint for the intensity of the laser lesion is to create a uniformly relatively white lesion. The ophthalmologist can achieve this end-point in either of the following ways: (1) by initially applying relatively white laser burns that meet or exceed the intensity illustrated by a standard photograph from the MPS[89] or (2) by applying lighter gray-white laser spots that overlap again and again until the entire laser lesion is a uniform white treatment burn at least as white as the treatment intensity standard[37] (Fig. 146.15).
TABLE 146.4 -- Treatment Protocol for Choroidal Neovascularization from the Macular Photocoagulation Study
|
All Lesions |
|
Angiogram <96 hr old |
|
Extrafoveal Lesions (>199 ?m from Foveal Center) |
|
Extend treatment additional 100 mm beyond any adjacent blood, pigment ring circumferentially surrounding the lesion, or other blocked fluorescence surrounding the lesion |
|
Juxtafoveal Lesions (1-199 ?m from Foveal Center) |
|
Extend treatment additional 100 ?m beyond the neovascular lesion on border away from fovea |
|
Extend treatment additional 100 ?m into any blood present on the foveal side if the hyperfluorescence from the neovascular lesion itself is 100 ?m or farther from foveal center |
|
Subfoveal Lesions (CNV Underlies Foveal Center) |
|
Extend treatment additional 100 ?m beyond peripheral boundaries of all lesion components except blood |
|
Cover, but not necessarily extend 100 ?m beyond areas of blocked fluorescence into thick blood |
|
Subfoveal Recurrent Lesions (Prior Laser Treatment with Recurrent Lesion Underlying Foveal Center) |
|
Extend treatment 300 ?m into previous treatment scar-recurrent neovascular lesion interface |
|
If feeder vessels present, extend treatment 100 ?m beyond lateral borders of recurrent vessels and 300 ?m radially beyond base (origin) of feeder vessel |
|
|
|
|
FIGURE 146.15 Treatment intensity standard. The treatment protocol of the MPS specified a uniform, white burn at least as intense as the treatment standard. |
Wavelength Selection
When the MPS was begun in 1978, the argon blue-green laser was the one most commercially available to investigators. This laser is no longer recommended for treatment within the macular region because macular xanthophyll pigment directly absorbs the blue light of the argon blue-green laser, thereby inducing thermal damage to the inner retina.[96] In addition, the risk of inducing internal limiting membrane wrinkling, although rarely of clinical significance, is probably greatest with the argon blue-green laser.[97] Subsequent trials in the MPS for juxtafoveal lesions employed the krypton red laser because of its theoretical advantage of penetrating through xanthophyll and passing through thin layers of red hemorrhage, allowing the uptake of the laser to be concentrated within the RPE and melanocytes of the inner choroid. When the MPS trials for subfoveal lesions were designed, eyes randomized to the treatment group were further randomized to either the argon green or the krypton red wavelength for treatment. None of the findings from the subfoveal trials suggests a reason to favor either the argon green or the krypton red wavelength.[40,41] If there were any theoretical advantage to using one wavelength over another for treatment of CNV, one might have expected to have detected a difference within the MPS subfoveal trials. Although these trials did not have sufficient power to demonstrate a small or moderate difference between the two wavelengths, a large difference has been ruled out by these studies.[40,41] Recurrence and persistence rates also were similar between the two laser wavelengths. The recurrence and persistence rates were similar to those observed when the krypton red laser alone was used to treat neovascular lesions in the MPS trial of juxtafoveal neovascularization. Thus, no visible wavelength appears to have a significant advantage over other wavelengths. Small differences in convenience of achieving the endpoint of a uniform white burn might be seen with red or yellow wavelengths when penetrating through the increased nuclear yellow in the older age group afflicted with CNV secondary to AMD, but any significant differences of clinical importance have not been shown.
Special Circumstances
When treating CNV that lies under a major retinal vessel, the laser burns should straddle the retinal vessel to reduce the possibility of causing hemorrhage or damaging the vessel by thermal vasculitis. There is no evidence to suggest that this technique compromises the effectiveness of treatment.
When treating CNV that is contiguous with the optic nerve, one must consider that laser treatment directly over the optic nerve can cause thermal necrosis of disc tissue and nerve fiber bundle defects.[98]Therefore, one should consider refraining from treatment within 100-200 ?m of the optic nerve. Similarly, when treating a parapapillary area of CNV, one may want to consider treatment only when at least 1 1/2 clock hours of papillomacular bundle on the temporal side of the disc is uninvolved with CNV, so that at least 1 1/2 clock hours of papillomacular bundle can be spared treatment, as was done in several of the MPS trials.[88,99] Treatment to nasal or parapapillary lesions likely will not lead to severe visual loss from damage to the nerve fiber layer that serves the central macula if the treatment guidelines outlined previously are employed.[100] In these situations, the MPS group reported that severe visual acuity loss was noted after treatment only when recurrent CNV extended through the center of the fovea.[100] This finding suggests that severe visual loss only from nerve fiber layer damage after this treatment approach, in the absence of subfoveal recurrence, must be a rare complication.
Certain subgroups in the various trials had different treatment benefits, which should be considered when determining whether treatment would be beneficial for a particular patient.[89,101] This subgroup analysis should probably not completely sway someone in recommending or denying treatment. Rather, the subgroup analysis data should serve as a guideline when trying to decide whether treatment should be recommended to a particular individual. For instance, in the krypton trial of juxtafoveal lesions,[89] patients who were normotensive had a marked treatment benefit. Patients who had evidence of hypertension, either by elevated systolic or diastolic blood pressures or by the use of antihypertensive medications, had no treatment benefit. Although similar trends were noted in the argon trial for patients with CNV secondary to the ocular histoplasmosis syndrome,[99] similar trends were not noted in the argon trial of CNV secondary to AMD[102] nor in the subfoveal trials in AMD.[40,41] Therefore, although the data in the juxtafoveal trial failed to detect a treatment benefit for hypertensive patients, lack of corroboration of this finding in two other prospective trials on CNV secondary to AMD cautions one from withholding treatment from patients who are hypertensive.
There is only weak evidence that laser photocoagulation of extrafoveal fluorescent spots ('hot spots') on ICG angiography or feeder vessels on high speed video ICG angiography within a neovascular lesion leads to a better outcome than no treatment. The lack of controls in these trials, or comparisons to anti-VEGF treatments now used for subfoveal lesions, precludes one from concluding with much confidence that such treatments should be considered. This conclusion also applies to such fluorescent spots seen within serous RPE detachments.[103]
On rare occasions, a patient will present with extrafoveal CNV contiguous to a serous detachment of the RPE in which the serous detachment extends through the foveal center. There have been case reports in which only the extrafoveal CNV in these lesions is treated, resulting in prompt flattening of the RPE detachment with improvement of vision in selected cases.[104] Nevertheless, with follow-up, many of these eyes have acquired recurrent CNV with extensive scarring and visual loss. The more likely situation is that the extrafoveal CNV actually is associated with fibrovascular PED that extends through the foveal center in which treatment of the extrafoveal CNV alone has not been shown to be of any benefit,[91] and anti-VEGF treatment, when indicated as described below, should be considered.
Postoperative management of laser photocoagulation
Data from the MPS group have shown that eyes in which laser treatment did not cover the CNV completely on the foveal side or did not meet the required level of intensity (a uniform relatively white burn, as shown in Fig. 146.15) had ?3 times the risk of having persistent CNV within 6 weeks after treatment compared with eyes in which the CNV was covered completely by intense, confluent burns.94 Because of this information, it is essential not only to obtain a uniform relatively white laser burn during treatment but also to ensure that the extent of the intense confluent burns completely covers the extent of the CNV.
When a CNV lesion is extrafoveal, it usually is not difficult for an ophthalmologist who is experienced in treating CNV to extend laser treatment over the entire extent of the CNV.[88,99] There is probably little hesitancy in extending treatment slightly beyond the borders of the CNV in an effort to ensure adequate coverage when the CNV is far away from the foveal center. Slight extension of treatment should have little effect on the visual acuity, since the treatment in these situations will not affect central foveal photoreceptors.
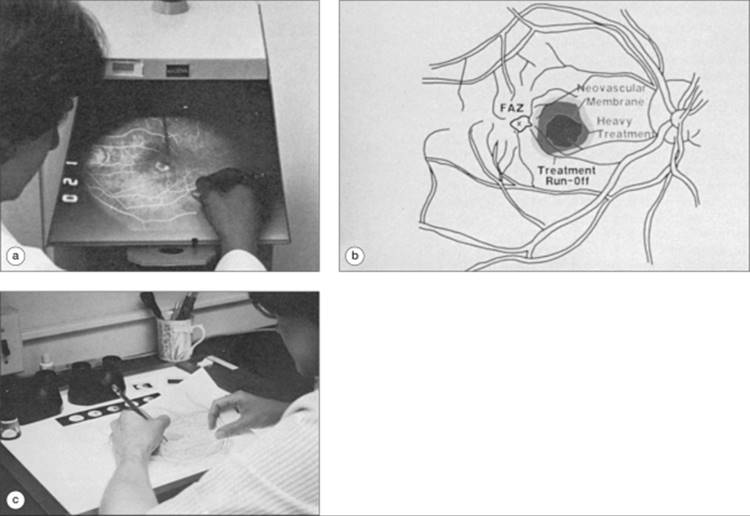
In an attempt to minimize persistent CNV caused by inadequate coverage, one may evaluate the laser treatment by comparing the area of laser treatment from a posttreatment photograph to the area of the lesion to be covered from the pretreatment angiogram.[30,105,106] The MPS group has described their methods for this evaluation.[106] In step 1, the extent and location of the CNV with respect to the vascular landmarks (Fig. 146.16a) is traced, either on paper of a projected slide or on available imaging software with digital imaging systems. In step 2, immediately after treatment, a posttreatment photograph (digitally) or Polaroid (film) is taken. The area of heavy treatment and the same landmark vessels are outlined on a separate piece of plain white paper (Fig. 146.16b) or with the image software. In step 3, the treatment drawing from step 2 is placed on a light box, and the pretreatment drawing from step 1 is placed over this, superimposing the landmark vessels, or superimposed by digital image software. The area of heavy treatment can then be traced onto the pretreatment drawing to determine whether the treatment has covered the CNV in its entirety (Fig. 146.16c). Any areas not adequately treated can be 'touched up' while the patient is still in the office. The MPS group proved the usefulness of this method using 1-day posttreatment stereoscopic color photographs; areas of inadequate treatment were identified, and these eyes did indeed have a higher rate of persistent CNV in the juxtafoveal trials,[93,94] it is likely that inadequate treatment to extrafoveal lesions would result in the same problem.
|
|
|
|
FIGURE 146.16 Evaluation of CNV treatment. (a) Angiogram is projected onto an apparatus (such as a microfilm reader or slide viewer) such that the CNV and key landmarks around the CNV such as subretinal blood, retinal vessels, and foveal center can be drawn. (b) The foveal avascular zone (FAZ) and the foveal center (x) are indicated. (c) A posttreatment photograph is then projected, and the area of heavy treatment and the same landmark vessels can be outlined on a separate piece of paper. Evaluation of photocoagulation treatment can be determined by placing the treatment drawing (c) under the pretreatment drawing (a) on a lightbox. The area of heavy treatment can then be traced onto the pretreatment drawing to determine whether the treatment has entirely covered the CNV. Alternatively, digital imaging software can be used to overlay the boundaries of treatment from a post-treatment photograph onto the boundaries of a lesion from a pre-treatment frame from the fluorescein angiogram. |
Subfoveal Lesions
For treatment of subfoveal lesions (Fig. 146.12), one first determines if the lesion is predominantly CNV (at least 50% of the lesion is CNV, totaling areas of any classic CNV and any occult CNV). If the lesion is predominantly CNV, one then determines (Fig. 146.12) if the lesion is minimally classic or occult with no classic. If so, then one determines if the patient has had presumed recent disease progression in this eye. Presumed recent disease progression includes any of the following: blood associated with the lesion, visual acuity loss within the past 3 months, or growth of the lesion on fluorescein angiography within the last 3 months. In the absence of presumed recent disease progression for a subfoveal lesion with a minimally classic or occult with no classic lesion composition, careful follow-up, perhaps at 3 week, and then 6 week, and 3 month, intervals is indicated to watch for progression to a predominantly classic lesion (see below) or development of presumed recent disease progression. Lesions with these compositions were excluded from the anti-VEGF trials described below, and may have a different natural course from the lesions in these trials, suggesting that it would be inappropriate to extrapolate the results of these anti-VEGF trials to minimally classic or occult with no classic lesions in the absence of presumed recent disease progression.
If presumed recent disease progression is noted, then treatment with ranibizumab is considered based on the MARINA (Minimally Classic/Occult Trial of the Anti-VEGF Antibody Ranibizumab in the Treatment of Neovascular AMD) trial. The MARINA trial was a Phase III study of 716 patients with presumed recent disease progression (blood associated with CNV, recent visual acuity loss, or recent growth of CNV on fluorescein angiography) associated with minimally classic or occult with no classic CNV in AMD. Participants were randomized 2:1 to receive either ITV ranibizumab, or sham injections. The active treatment group was further randomized to either a 0.3-mg or 0.5 mg-dose of ranibizumab every 4 weeks for 2 years. One-year data showed that compared with baseline, 95% (452/478) of ranibizumab-treated patients lost fewer than 15 letters of visual acuity (VA), compared with 62% (148/238) of patients in the control group.[107] Twenty-five percent (59/238) of patients treated with 0.3 mg of ranibizumab and 34% (81/240) treated with 0.5 mg of ranibizumab improved vision by 15 letters or more compared with approximately 5% (11/238) of patients in the control group. Nearly 40% (188/478) of ranibizumab-treated patients achieved a VA score of 20/40 or better compared with 11% (26/238) in the control group. Side effects that occurred more frequently in the ranibizumab arms than in the control group at 1 year included mild to moderate conjunctival hemorrhage, eye pain, and vitreous floaters. Uveitis and endophthalmitis occurred in fewer than 1% of patients in the ranibizumab and control groups. Serious nonocular adverse events occurred essentially as frequently among ranibizumab-treated patients as among controls.[108] These data indicate that ranibizumab not only reduces the risk of moderate or severe visual acuity loss, but also increases the chance of moderate visual acuity gain. While a majority of treated patients did not improve by 15 or more letters, patients who do have this level of improvement following ranibizumab treatment may regain abilities dependent on vision they had previously lost, and may be able to participate in productive and enjoyable activities such as reading a newspaper or recognizing faces in social situations.
If the lesion is predominantly classic (Fig. 146.12), one need not have presumed recent disease progression since trials evaluating treatments for these lesions did not include a requirement for presumed recent disease progression. The ANCHOR (Anti-VEGF Antibody for the Treatment of Predominantly Classic Choroidal Neovascularization in AMD) trial involved 423 patients with predominantly classic neovascular AMD. This randomized, double-masked, active treatment-controlled study compared safety and efficacy of 0.3-mg and 0.5-mg doses of ranibizumab over the course of 2 years. Results from this study showed that 94% (132/140) of ranibizumab-treated patients assigned to 0.3 mg and 96% (134/139) of ranibizumab-treated patients assigned to 0.5 mg avoided 15 or more letter loss compared with 64% (92/143) of patients assigned to verteporfin PDT (P.0001). No additional ocular or systemic safety problems were identified beyond the information summarized above from the MARINA trial.[109,110]Since the ranibizumab-treated subjects without PDT in ANCHOR had similar outcomes to the predominantly classic cases enrolled by investigators in the FOCUS trial (where subjected were assigned randomly to verteporfin PDT with sham injection or verteporfin PDT plus ranibizumab), it seems unlikely that adding PDT to ranibizumab will result in better vision outcomes for these lesions. It remains unknown at this time if this combination therapy will lead to the need for fewer injections, and no trial has compared PDT plus ranibizumab to ranibizumab alone.
To examine effects of ranibizumab on patient-reported vision-specific QOL, investigators administered the NEI VFQ-25 to participants in both the MARINA and ANCHOR trials. The MARINA trial demonstrated a marked increase in the proportion of patients with clinically relevant improvement in vision-specific QOL following pharmacologic intervention in AMD (Fig. 146.17) (Chang TS, Fine JT, Bressler N. Self-reported vision-specific quality of life at 1 year in patients with neovascular age-related macular degeneration in 2 Phase III randomized clinical trials of ranibizumab (Lucentis). Poster presented at: Annual Meeting of the Association for Research in Vision and Ophthalmology, Fort Lauderdale, Fl, May 1-52006: Poster B667) In the MARINA trial, investigators administered the NEI-VFQ 25-716 subjects with subfoveal CNV due to AMD with minimally classic or occult with no classic types at baseline and at months 1, 2, 3, 6, 9, and 12. MARINA patients treated with ranibizumab 0.5 mg were more likely to improve 10 or more points on the NEI-VFQ in activities related to near and distance vision than were patients who received sham injections (P < 0.001), who experienced overall decreases in their ability to perform these activities (Fig. 146.17) (Chang TS, Fine JT, Bressler N. Self-reported vision-specific quality of life at 1 year in patients with neovascular age-related macular degeneration in 2 Phase III randomized clinical trials of ranibizumab (Lucentis). Poster presented at: Annual Meeting of the Association for Research in Vision and Ophthalmology, Fort Lauderdale, Fl, May 1-5, 2006: Poster B667). In addition, ranibizumab-treated patients were more likely to improve 10 or more points in ratings of dependency on others because of vision than were sham injection patients.
|
|
|
|
FIGURE 146.17 MARINA trial. Improvement in vision-specific QOL following pharmacologic intervention in AMD. |
Similar benefits of ranibizumab for patients with predomi-nantly classic lesions were confirmed in the ANCHOR trial. Investigators administered the NEI-VFQ 25 to 418 AMD patients with predominantly classic type at baseline and at months 1, 2, 3, 6, 9, and 12 as reported at the 2006 Annual Meeting of the American Society of Retina Specialists, although QOL data have not yet been published in a peer-reviewed journal.
Other treatments for subfoveal neovascular AMD
Bevacizumab was approved by the FDA for intravenous administration to patients with metastatic colorectal cancer in February 2004. Bevacizumab has a similar molecular structure to ranibizumab. Initially, a report about a series of AMD patients who were treated with systemic bevacizumab, and one case report of bevacizumab ITV administration, showed short-term vision and anatomic outcomes that appeared similar to those seen with ranibizumab and unlike the natural history of this disease. Based on these reports, some ophthalmologists began to administer bevacizumab off-label to treat AMD.
Specifically, an open-label, uncontrolled, clinical study evaluated the short-term safety of systemic bevacizumab in nine AMD patients with subfoveal CNV, with best-corrected VA of 20/40 to 20/400. Patients received an infusion of bevacizumab (5 mg/kg) at baseline, followed by one or two additional doses at 2 week intervals. By 12 weeks, the median VA scores in the study eyes increased by 8 letters (P = 0.011). The median central retinal thickness decreased by 157 ?m (P = 0.008). No serious ocular or systemic adverse events were identified during safety assessments, which were performed at all visits. The only treatment-related adverse event was a treatable, reversible, mild elevation of systolic blood pressure (+12 mm Hg; P=.035). Although, the improvements in VA, OCT measurements, and angiography (marked improvement in vessel leakage in all eyes) in this small sample suggest that systemic bevacizumab may be efficacious in neovascular AMD, a case series of nine patients does not constitute an adequate evidence base to conclude that systemic bevacizumab©therapy is safe and effective for neovascular AMD patients.[107]
The single case report of ITV bevacizumab involved a 63-year-old woman with neovascular AMD, whose vision had deteriorated despite treatment with PDT/triamcinolone acetate and pegaptanib was a sentinel event leading to ophthalmologists' use of intravitreal bevacizumab while FDA approval for ranibizumab was pending.[108] The patient received a single 1.0 mg ITV dose of bevacizumab. Within 1 week, the subretinal fluid resolved such that the macular contour appeared normal on OCT, and remained so for at least 4 weeks. VA remained stable, and neither ocular inflammation nor angiographic leakage was observed. This case report represents proof of concept that a drug which is usually administered intravenously to prevent neovascularization in cancer patients could be effective and safe over the short term, administered ITV in an AMD patient who had responded poorly to previous treatments. The report also indicates that, although it is a larger molecule than ranibizumab, bevacizumab apparently penetrated the retina well enough to inhibit VEGF in the vitreous cavity. Since then, additional reports have appeared in the literature presenting safety evaluations of the drug when injected into the vitreous of rabbits,[109] immunofluorescent studies suggesting the ability of bevacizumab to penetrate the retina,[109] and evidence of potential clinical efficacy.[110] A large, well-designed, clinical trial would be needed to establish more definitively the strength of applying these results to patients with neovascular AMD.
In summary, the strength of the evidence to warrant the tse of ranibizumab for specific lesions described above is based on multiple randomized clinical trials with relevant endpoints with respect to visual acuity and a patient's perception of vision-related quality of life. The strength of evidence to support use of bevacizumab is weaker, based on case series and anecdotal reports. It is unknown at this time if intravitreal bevacizumab is almost as good, better, or worse than ranibizumab for reducing the risk of visual acuity loss and increasing the chance of visual acuity gain. However, the evidence may be strong enough to warrant consideration of bevacizumab when ranibizumab is not available to a patients because of regulatory limitations (e.g., not yet approved for use in a country) or financial limitations (since a single-use vial of ranibizumab costs a physician approximately $2000 in 2007 compared with approximately $50 when 1.25 mg of bevacizumab in 0.05 ml is obtained from a compounding pharmacy making multiple doses from a single-use vial of bevacizumab that was packaged for intravenous use in the treatment of certain cancers).
Pegaptanib sodium
During two concurrent, 48 week, randomized, double-blind, controlled clinical trials, patients received ITV pegaptanib in one eye at a dosage of 0.3 mg, 1.0 mg, or 3.0 mg. The control group was given sham injections every 6 weeks.[44] The primary outcome variable was the proportion of patients who lost fewer than 15 letters of VA at week 54. As compared to 164 (55%) of 296 patients in the control group, 206 (70%) of 294 patients treated with 0.3 mg pegaptanib responded (P < 0.001), as did 213 (71%) of 300 those treated with 1.0 mg pegaptanib (P < 0.001), and 193 (65%) of 296 those treated with 3.0 mg pegaptanib (P = 0.03). The majority of patients in all three pegaptanib groups (95-97%) and in the sham group (95% experienced at least one adverse event.[111]
Vitreous hemorrhage occurred in 2% of pegaptanib-treated eyes, endophthalmitis in 1.3%, traumatic cataract in 0.6%, and retinal tear or detachment in 0.7%.[44,111] Based on this study, pegaptanib was approved for the treatment of neovascular AMD and could be considered for patients with lesions similar to those of patients enrolled in these trials. However, because the results were far different from that obtained with ranibizumab, most ophthalmologists would not consider the use of pegaptanib over ranibizumab at this time.
A retrospective post hoc analysis was performed in AMD patients with 'early' disease defined retrospectively in two ways: Group 1 (n=34) characteristics include lesion size <2 disc areas, baseline VA letter score ?54, and no prior PDT or laser photocoagulation; Group 2 (n = 30) characteristics included occult with no classic CNV, no lipid, and VA in study eye worse than that in fellow eye.[112] It is unknown how many combinations of characteristics were examined to form with these groups. In pegaptanib-treated Groups 1 and 2, 26 (76%) and 24 (80%) of 34 and 30 subjects, respectively, lost <15 letters of VA (the primary efficacy measure), compared with 14 (50%) and 20 (57%) of 28 and 35 subjects assigned to sham injections. In the pegaptanib Groups 1 and 2, 4 (12%; Group 1) to 6 (20%; Group 2) of 34 and 30 subjects, respectively, gained at least 15 letters of VA compared with 1 (4%) and none of 28 and 35 subjects, respectively, receiving sham injections. These data suggest that pegaptanib may be more effective if treatment is started early in the natural history of a patient's disease. This conclusion should be evaluated with caution, however, as based on these small numbers, the confidence intervals surrounding the estimated percentage values are likely to be rather wide.
While PDT with verteporfin was shown to be superior to no treatment for predominantly classic subfoveal lesions (TAP REPORT NO. 1 1999), its inferiority to ranibizumab in the ANCHOR trial for these lesions suggests that few ophthal-mologists would consider verteporfin PDT over ranibizumab in most circumstances if both drugs are available. Similarly, although no head-to-head trial of ranibizumab to verteporfin PDT has been done for minimally classic or occult with no classic lesions with presumed recent disease progression, the outcomes reported in the MARINA trial for such lesions with ranibizumab seem far superior to those reported to verteporfin PDT (VIP REPORT NO. 2).
With respect to safety, the risk of endophthalmitis in any invasive ocular procedure may be minimized with proper aseptic technique, the use of a lid speculum, careful postinjection monitoring, and educating patients about which postinjection symptoms to report to the physician. Bevacizumab is not manufactured with the strict particulate matter limits that are required for ocular drugs, such as ranibizumab, nor does it contain preservatives. Theoretically, when dividing bevacizumab into smaller doses required for ITV administration, contamination could be introduced if not done under aseptic technique, and the label currently indicates the need to use the drug within 6 h of opening a vial.
Although it is possible that the body could develop antibodies against VEGF inhibitors, no serum antibodies to ranibizumab were detected in the dose-ranging trial.[113] One published trial of pegaptanib did not report evaluations of serum antibodies,[114] and another reported that there were no serum antibodies or hypersensitivity reactions to pegaptanib.[44]
Another potential concern is the possibility that VEGF inhibitors may potentiate myocardial infarction and stroke, which has occurred at higher rates in treatment than control groups in trials of intravenous bevacizumab among cancer patients.[115] Thromboembolic events have occurred among intraocular ranibizumab and pegaptanib trial participants, but the frequency was not statistically different between treatment and control groups.[44] No data has been published regarding the risk of such events following intraocular injection of bevacizumab.
In summary, based on clinical trials, ranibizumab appears to offer the best outcome at this time in the treatment of selected cases of neovascular AMD similar to those enrolled in MARINA, ANCHOR, VISION, the TAP Investigation, or the VIP Trial compared with pegaptanib or PDT with verteporfin. Additional data are needed to determine if bevacizumab results in similar efficacy and safety to warrant its use when ranibizumab is available. When ranibizumab is not available because of regulatory limitations or cost, bevacizumab might be considered. However, the patient must be informed of the risks and benefits of extrapolating the ranibizumab trial results to bevacizumab based on the limited evidence published to date regarding potential benefits of bevacizumab and the limited safety data available compared with the more extensive safety data available on pegaptanib or verteporfin PDT (assuming the short-term efficacy noted with bevacizumab translates to the longer-term efficacy seen with ranibizumab, but not shown for pegaptanib or verteporfin PDT).
The necessity for ITV administration of ranibizumab as often as every month and pegaptanib as often as every 6 weeks is a distinct disadvantage compared to topical applications used to treat other eye diseases and different from the potential disadvantages of the intravenous administration of verteporfin PDT, with sunlight restrictions for several days and follow-up as often as every 3 months. However, clinical trials with ranibizumab and pegaptanib were able to successfully recruit participants who continued treatment throughout the 2 years of the trials, despite the administration of ITV, so it appears to be acceptable despite the invasiveness of the procedure.
MANAGING PATIENTS AND PHYSICIANS' EXPECTATIONS IN THE TREATMENT OF NEOVASCULAR AMD
Ophthalmology patients' satisfaction in care hinges on an adequate explanation of diagnosis, treatment, and prognosis. Based on interviews of 163 ophthalmology patients interviewed at either a Veteran's Administration hospital or private practice, more than 90% of patients rate these explanations as the most important determinant of their satisfaction with the medical visit.[116] Although all 19 ophthalmologists interviewed as part of this study rated explanations of diagnosis and treatment as very important to patient satisfaction, only 40% of them also rated a discussion of prognosis as highly. Trobe Ophthalmology 1983, P53A, T2, items 1-3 This dichotomy in expectations about revealing prognosis indicates that patients' expectations may be at odds with those of their physicians on this issue.
Patients expect that their ophthalmologists will explain AMD treatment options in ways they can understand, yet a sizable group of patients may have problems with health literacy. In one study of Medicare enrollees in a nationwide managed-care system, one third of English-speaking patients, and more than one half of Spanish-speaking patients, exhibited either marginal or inadequate health literacy, and thus were unable to understand consent forms or medicine labels. In addition, health literacy tended to decline with age, with inadequate health literacy exhibited in only 15.6% of participants 65-69 years old and increasing to 58.0% of those older than 85. If an ophthalmologist uses the same level of language with all patients, there is a risk, therefore, that a substantial minority of patients will be unable to comply with treatment plans. This, in turn, can lead to patient disappointment and ophthalmologist frustration, since a treatment would likely be more effective if the patient were compliant with instructions.
Those patients with AMD who are literate enough to understand the implications of the disease process expect that their preferences and concerns with regard to treatment options will be considered by their ophthalmologists. They may arrive at the ophthalmologist's office clutching reams of printouts from the Internet, expecting that their physician will embrace what they have found from web sites that may or may not be reliable.[117] As a result, patients with AMD may develop unrealistic expectations of treatment effectiveness and safety, based on selective attention to potential positive outcomes that are widely publicized on the Internet or in popular publications. Patients may misunderstand and assume that positive outcomes in a proportion of participants treated during a clinical trial will occur to them as individuals. A patient who has read about ranibizumab, for example, may assume that if treated with that drug, he or she will regain vision and be able to drive, read, and recognize faces again because ?40% of ranibizumab-treated patients did so.[118]
PATIENT EXPECTATIONS
In the face of AMD, a disease with uncertain outcomes, several strategies may be useful to manage patient expectations. These strategies, first identified among general medical practitioners, include an honest discussion of the natural history of the disease without treatment, the potential outcomes with treatment, and the prognosis with or without treatment (watchful waiting).[119]
The ophthalmologist should first explain that some patients with treatment will lose vision. For example, when discussing ranibizumab as a possible treatment with patients, it should be explained that 5% of treated patients lost a moderate amount of vision (15 or more letters, ?3 or more lines on the eye chart). However, without treatment, patients should understand that 35-40% will lose at least a moderate amount of vision. Likewise, patients should understand that treatment does not take away one's chance of improving, but that not all treated patients will improve. Clinical trials suggest that few untreated patients will improve a moderate amount (three or more lines on an eye chart), and that with verteporfin PDT or pegaptanib injections only ?5-10% will gain this amount of vision. With ranibizumab, 25-40% (depending on drug dose and lesion composition) gained three or more lines of vision by 1 year, with the proportion of study subjects having this improvement remaining fairly stable through 2 years. This means that a majority of patients will not have noticeable improvement, but it is far more likely that one will experience improvement with ranibizumab treatment than without treatment or with other treatments currently available.
Another strategy that is essential to managing patients' expectations is to be sure the patient understands, and is willing and able to comply with, the treatment plan. Hewson J Gen Int Med 1996; P483, T1, item 5 If pegaptanib or ranibizumab is being considered as a treatment option, for example, one should describe the need for multiple visits, multiple imaging procedures, and multiple injections. While it is unclear at this time whether monthly injections (MARINA, ANCHOR) are superior to less frequent injections (PIER), patients receiving ranibizumab need to know that injections could be as often as monthly for at least 2 years, and possibly for a longer time. As more knowledge is gained regarding longer term outcomes, this information should be shared with patients. The ophthalmologist also must make the patient aware that there are potential risks of treatment due to either the drug itself (none known definitively at this time with ranibizumab) or to the administration of the drug by injection (e.g., such as endophthalmitis or retinal tears.[120]
Given the expenses of some drugs in the management of neovascular AMD, the treating ophthalmologist should be sure the patient understands the total expected cost of treatment over time, and what proportions will be paid by the patient's third-party payer, if any, compared with those that the patient must pay out-of-pocket. A 2 year course of pegaptanib injections every 6 weeks, for example, may cost more than $19000.[121] The price of ranibizumab, which was administered once a month in the pivotal trials, will be $1950 per injection to the ophthalmologist, with an additional mark-up to the patient, for a total of $23000 per year to the heath care provider just for the drug. Additional costs for visits, imaging, and mark-up on the drug need to be explained as well.
OPHTHALMOLOGISTS' EXPECTATIONS
The factors mentioned above that govern patient expectations for treatment also influence their physicians. Ophthalmologists want their patients to be satisfied with their care, and share with them the desire for explanations of diagnosis, treatment, prognosis that the patients can understand and apply. Most patients will accept treatment that the physicians suggest (e.g., watchful waiting, surgery, photodynamic treatment, intravitreal injection). Clinicians cannot predict which patients will benefit from a given therapeutic intervention and which will not. Thus, treatment decisions for AMD patients should be weighed carefully to maximize the chances for vision retention or improvement. One way to maximize rational treatment choice involves the concept of the number needed to treat (NNT). NNT is an estimate of the number of patients who need to be treated with a given regimen (instead of the standard treatment) for one additional patient to benefit from a specific outcome. This benefit is often expressed as an outcome to avoid, e.g., three or more lines of vision loss, or a desirable outcome, e.g., 3 or more line gain. The ideal NNT would be one, meaning that every patient treated with a given regimen would benefit.
The NNT is the reciprocal of the absolute risk reduction. Assuming the standard treatment is verteporfin PDT, the NNT for ranibizumab to avoid three or more line loss is calculated as shown in Figure 146.18, based on efficacy data from the ANCHOR (Anti-VEGF Antibody for the Treatment of Predominantly Classic CHORoidal Neovascularization in AMD) Trial. If the clinician is considering ranibizumab or pegaptanib for an AMD patient, for example, the treatment with the lower NNT with avoidance of vision loss as the specified outcome would be the optimal choice for the patient.[122]
|
|
|
|
FIGURE 146.18 Calculation of NNT based on data from the ANCHOR clinical trial. |
Ophthalmologists want to prescribe treatments that are cost-effective for their patients. A costly intervention for AMD may be worth the financial outlay if it truly benefits patients, as the gift of sight may be considered priceless. The next newsletter in this series will discuss cost-effectiveness of AMD treatments in detail.
MANAGEMENT CONSIDERATIONS FOR PHYSICIANS
Between one-quarter and one-half of Americans read at the 8th grade level or below, despite having graduated from high school.[123] Ideally, therefore, the ophthalmologist should determine the patient's health literacy level. In a research setting, clinicians might determine the patient's health literacy level using the Short Test of Functional Literacy in Adults, which is available in both English and Spanish, and takes only 12 min to administer. If that is not possible in the private setting due to time and staffing constraints, simply asking the patient, "How often do you need to have someone help you to read instructions, pamphlets, or other written material from your doctor or pharmacy?" can be used as a proxy.[124]
The ophthalmologist should consider providing AMD patients with recommendations for easy-to-understand educational materials, such as those available from the American Academy of Ophthalmology. The Medline Plus Macular Degeneration Patient Education Page (http://www.nlm.nih.gov/medlineplus/maculardegeneration.html![]() ) also provides reliable material targeted to the lay public. Frequent updates may be needed as new data are presented or published.
) also provides reliable material targeted to the lay public. Frequent updates may be needed as new data are presented or published.
MONITORING PATIENTS FOLLOWING INITIATION OF RANIBIZUMAB THERAPY FOR NEOVASCULAR AMD
Several investigators have published case series about monitoring retinal structure with OCT following intravitreal bevacizumab when used to treat CNV. Avery and colleagues treated 79 patients with intravitreal bevacizumab monthly. While they did not specify whether fluorescein angiography was performed at each visit, patients followed for 4-15 weeks showed a decline in central retinal thickness as measured by OCT of at least 10% in 41 (55%) of 75 patients seen 1 week postinjection.[116] Spaide and colleagues used changes in retinal thickness (as measured in the central subfileld on OCT) as a primary outcome measure in a retrospective study of 266 patients who had been treated with intravitreal bevacizumab.[125] Ophthalmologists for patients in this series justified performing FA as needed, rather than at every follow-up visit, because they deemed slit-lamp biomicroscopy and OCT adequate to measure initial response to VEGF-inhibitor therapy.[125] However, measuring a response to therapy does not determine if retreatment decisions based on OCT, or fluorescein angiography, or both, lead to better outcomes than if none of these evaluations are performed after initiating anti-VEGF therapy.
The pivotal trials leading to the FDA approval of ranibizumab, ANCHOR (Anti-VEGF Antibody for the Treatment of Predominantly Classic CHORoidal Neovascularization in AMD) and MARINA (Minimally Classic/Occult Trial of the Anti-VEGF Antibody Ranibizumab in the Treatment of Neovascular AMD) gave monthly injections of ranibizumab through 2 years, without considering withholding retreatment based on OCT or fluorescein angiographic findings. Thus, these trials do not permit one to determine if almost as good, worse, or better outcomes would be obtained if treatment were withheld when it was judged that there was no room for continued improvement or when it was judged that the condition appeared 'stabilized'.
Although the protocols for these pivotal trials specified follow-up visits and retreatment with ranibizumab once per month, the possibility that the interval between ranibizumab treatments could be extended to balance efficacy with comfort and safety has not been determined definitively. The PIER trial (Phase 3b, Randomized, Double-Masked, Sham Injection-Controlled Study of the Efficacy and Safety of Ranibizumab in Subjects With Subfoveal Choroidal Neovascularization With or Without Classic CNV Secondary to AMD) showed that at month 12, patients treated with ranibizumab lost 1.6 letters and 0.2 letters (0.3 mg and 0.5 mg) compared to a loss of 16.3 letters in the sham group, on average (P < 0.0001)[126] The 1 year results of PIER suggest that an initial induction with 3 monthly ranibizumab treatments followed by quarterly injections may confer visual acuity, FA, and OCT benefits compared with sham. While such a regimen decreases the inconvenience and risk of more frequent injections, it is unknown how this regimen compares with respect to visual acuity outcomes to the monthly treatments used in the MARINA and ANCHOR trials.
While waiting for data to determine if withholding treatment based on parameters that indicate no room for further improvement or a stable lesion leads to outcomes that are almost as good, better, or worse than monthly injections of ranibizumab or bevacizumab, and while waiting for evidence if either retreatment approach with bevacizumab is almost as good, better, or worse than either retreatment approach with ranibizumab, ophthalmologists are approaching follow-up in one of two ways.
One, they may be applying ranibizumab treatments as it was done in the trials proving its benefits, i.e., monthly injections for up to 2 years. Two, knowing from the PIER study that less frequent treatments also are beneficial compared with no treatment (although not knowing if this is almost as good, better, or worse than monthly injections), some ophthalmologists are withholding additional treatments when there no longer is room for improvement or the lesion is stabilized. One might consider that there is no longer room for improvement when the visual acuity is as good as it could possibly be, for example, is 20/25, taking into consideration the patient's media opacities, refraction, and structural damage to the macula from atrophy or scarring or other degeneration. One might consider a lesion stabilized when certain parameters appear absolutely the same as the previous one or two months with respect to symptoms, visual acuity, biomicroscopic appearance (aided by documentation with fundus photographs), OCT, and fluorescein angiography.
Clearly, this latter approach is more time intensive for the patient and physician, with no strong evidence that outcomes based on this approach are almost the same or better than those obtained by monthly injections regardless of these parameters. Also, while symptoms, visual acuity, and biomicroscopic appearance add little cost to a visit, it is unknown if more costly fundus photographs aid in determining if a lesion is stable (as has been demonstrated with follow-up of diabetic retinopathy.[127] It is also unknown if making treatment decisions based on the increased cost of periodic OCTs are beneficial or preclude the need for the increased cost of fluorescein angiography (with its occasional difficulties with interpretation and its attendant side effects of nausea, vomiting, itching, or rash),[128] or making treatment decisions based on fluorescein angiography are beneficial or preclude the need for OCT. Since ranibizumab is expensive to the patient and third party payers, if periodic fundus photographs, OCT, or fluorescein angiograms were shown to identify situations when retreatment could be withheld with outcomes that were almost as good as monthly injections, the cost savings on the drug could outweigh the additional monitoring costs of fundus photographs, or OCT, or fluorescein angiography or a combination of these. If bevacizumab, which costs far less than ranibizumab for intraocular injection, were shown to provide outcomes that were almost as good or better than ranibizumab outcomes, then avoiding the cost of a few injections might not balance the costs of the photographs, or OCT, or angiograms.
Clearly more data is needed to make the ophthalmologist confident that use of monitoring with one or more procedures, including fundus photographs, OCT, and fluorescein angiograms, to determine retreatment leads to almost as good, or better outcomes than seen with monthly ranibizumab treatments. Until strong evidence is available, some ophthalmologists appropriately will apply retreatment each month for up to 2 years, while others will use weaker evidence (inference from case series, biologic rationale, and experience) to consider withholding treatment when there is no room for further improvement or when the situation appears stabilized. A trial announced by the National Eye Institute[129] will address some of these issues both with ranibizumab and bevacizumab.
NATURAL COURSE OF SUBFOVEAL SUBRETINAL HEMORRHAGE IN AMD
Several reports have noted that whereas some eyes with subfoveal subretinal hemorrhage associated with AMD have poor outcomes, the visual acuity of other eyes do not deteriorate or may improve spontaneously.[8,130,131] Such findings underscore the importance of evaluating the role of therapeutic interventions for these cases, such as surgery to remove subretinal hemorrhage,[132,133] in randomized clinical trials. In one such trial from the Submacular Surgery Trials, surgical removal of blood and any associate neovascular lesion was not shown to reduce the risk of vision loss in most cases and was associated with a high risk of rhegmatogenous retinal detachments. (ref sst report no. 13) The control group (no treatment) did note that ?20% of predominantly hemorrhagic lesions will have a breakthough vitreous hemorrhage. Other treatments under investigation include the use of intravitreal ranibizumab (although these lesions were excluded from the MARINA and ANCHOR trials), as well as using intravitreal gas to displace the hemorrhage.
RISK OF FELLOW EYE INVOLVEMENT WITH SUBSEQUENT CNV SCARRING
It is important to have the patient monitor the vision in the fellow eye if its macula does not already have CNV scarring. The MPS group has shown that if a patient presents with CNV in one eye and no evidence of CNV or scarring in the fellow eye, about 40% of these eyes will have CNV in the fellow eye within 5 years.1,2 The risk of CNV developing in these eyes may be further specified depending on the drusen and RPE abnormalities within 1500 ?m of the foveal center present in the fellow eye and certain patient characteristics at baseline.2 Specific risk factors include: (1) definite hypertension (systolic pressure ?140 mm Hg, diastolic pressure ?90 mm Hg, or use of antihypertensive medications), (2) five or more drusen, (3) greatest linear dimension of largest druse greater than 63 ?m, or (4) focal hyperpigmentation. The risk of CNV developing within 5 years after presenting with CNV in the first eye ranged from 7% if none of these risk factors was present to 87% if all four risk factors were present (Fig. 146.19).[2] As one might have suspected, for the fellow eyes that had no evidence of CNV or scarring at baseline and subsequently developed CNV within 5 years, the average visual acuity loss was eight lines of vision.141 In contrast, for the two-thirds of fellow eyes that had no evidence of CNV or scarring at baseline and did not have CNV within 5 years, the average visual acuity loss was less than half a line of vision (specifically, 0.4 line).[141] Therefore, the risk of moderate or severe loss of visual acuity is highly correlated with the development of CNV during follow-up. Eyes that do not acquire CNV during follow-up have little or no visual acuity loss. This finding should be considered when evaluating the role of vitamins, minerals, or other treatment modalities in preventing visual acuity loss for eyes with drusen or RPE abnormalities without the presence of CNV or scarring.
|
|
|
|
FIGURE 146.19 Incidence of CNV by number of risk factors present including definite hypertension, 5 or more drusen, greatest linear dimension of largest druse ?63 ?m, and focal hyperpigmentation. |
If one couples this information of fellow eye involvement with success of treatment in the first eye from the extrafoveal argon MPS trial, one can determine the risk of legal blindness (visual acuity of 20/200 or worse in both eyes) when treating the first eye. The risk of legal blindness, again, is highly correlated with whether or not the fellow eye had CNV or scarring at baseline. If CNV or scarring was present in the fellow eye at baseline, it was likely that the fellow eye already had significant loss of visual acuity and that there was a high risk of recurrence developing in the treated eye. Forty-nine percent of patients in the argon AMD MPS trial were legally blind within 5 years of follow-up when the fellow eye initially had CNV or scarring, whereas only 12% of patients were legally blind within 5 years of follow-up when the fellow eye had no evidence of CNV or scarring initially.[134] Similar analyses currently are under way for patients who participated in the MPS trials of juxtafoveal or subfoveal lesions from AMD. Of course, if the visual acuity of the fellow eye is compromised at all, and the first eye has CNV, low-vision aids are probably indicated to assist with magnification for near visual tasks, as are telescopic aids for spotting at distance.
LOW-VISION AIDS
Patients who have central visual impairment in both eyes should be advised about the availability of a variety of low-vision aids. A low-vision evaluation includes not only prescribing appropriate lenses, magnifying aids (optical or electronic), and other items of assistance but also properly training and encouraging the patient to use them. Patients should also be told of community resources available to assist them with visual impairment such as might be obtained from the directory of agencies serving the visually handicapped in the United States provided by the American Foundation for the Blind. A realistic appraisal of the prognosis coupled with appropriate counseling and support is necessary to enable the visually impaired patient to continue functioning as normally as possible despite the central visual impairment. The American Foundation for the Blind can also inform patients as to which aids, such as talking books, large-print books, watches that 'tell' time, closed-circuit television readers, and other devices, are available through the directory of products for people with vision problems.
Visual aids for detailed near and distance tasks, such as reading, writing, typing, sedentary distance viewing, and distance spotting for street signs, can be prescribed with a thorough low-vision examination conducted in a room with glare-free high-intensity lighting and large trial lenses to allow for eccentric fixation. There is a wide range of magnification levels available in the present armamentarium of low-vision aids. Some incorporate their own illumination source. Each aid has certain advantages and limitations, so a patient must decide with a low-vision aid specialist what combination of aids is best for her or his visual objectives and visual needs.
Four types of reading aids are available: reading glasses, hand-held lenses, stand magnifiers, and electronic devices. Reading glasses (convex lenses) provide relatively large fields of vision, but the strongest lenses require short working distances. Telescopic reading glasses increase the working distance; however, they allow a relatively smaller field of view and shorter depth of focus than a simple high plus reader of comparable magnification. Hand-held magnifiers may suffice for quick, simple tasks that are conducted at arm's length, such as adjusting a stove dial. A stand magnifier consists of a mounted lens that will remain in focus if placed on the reading material and held so that its focal point corresponds to the focal point of the patient's near correction. This device offers an alternative to the high plus lens for the weak or tremulous patient; it is also useful when the patient wishes an increase in working distance or wants to have an illumination source incorporated into the magnifying system. Closed-circuit television and hand-held electronic devices provide electronic magnification at greater levels than is possible with optical systems. These also provide binocular viewing and can be used at a comfortable reading distance. Unfortunately, not all systems are readily portable and all are quite costly. Writing assistance may be provided with a weak hand lens or a +5.00 add-in spectacle. Additional invaluable and simple tools to aid in writing include signature guides, black felt-tip pens, and bold wide-ruled paper.
Distance vision may be enhanced with binocular field glasses and opera glasses. Lightweight telescopes can be hand-held or mounted onto spectacles. Unfortunately, these instruments distort distances and limit peripheral vision; therefore, their applicability is limited to tasks of sedentary distance viewing and distance spotting.
Finally, the success of each of these aids is highly variable, depending on the visual deficit and the motivation of the patient. They can attempt to enhance only lighting or magnification for the remaining vision. The patient should not look on them as a treatment for macular degeneration nor expect to regain central vision. Nevertheless, it is important to give these patients every opportunity to be evaluated for and trained in the use of optical and nonoptical systems that may serve to improve the quality of life.
CONCLUSIONS AND FUTURE RESEARCH
The 1980s and 1990s provided enormous progress in the management of AMD. Specifically, laser treatment has been shown to be beneficial when compared with no treatment. However, the fact that laser treatment is more beneficial for preserving vision when compared with observation alone is only a start. Successful cases of laser treatment still result in central visual acuity loss for the patient, especially when treatment involves the foveal center as it so often does in AMD. Furthermore, treatment is applicable in only a minority of cases.
Therefore, future research in the management of CNV in AMD will have to evaluate other modalities of treatment that do not cause destruction of the foveal center or therapies that prevent the development of CNV in the first place.[135] Such investigations will require interdisciplinary approaches to this problem that will probably include epidemiologists, clinicians, psychophysicists, vitreoretinal surgeons, geneticists, and cellular biologists. These investigations may include therapies to prevent the development of CNV or to minimize the damage it causes. Medical interventions that affect angiogenesis may hold some promise. Unfortunately, one randomized clinical trial evaluating interferon-? showed no benefit and possible harm in the treatment of CNV from AMD.[136] Surgical interventions that could remove the neovascular process before it destroys a large area of the central retina also may hold some promise, especially because these interventions, as with medical interventions, may be considered for lesions obscured by blood or that have poorly demarcated boundaries.[137] Other currently unproven investigational therapies in the 1990s include consideration of indocyanine green-guided laser photocoagulation,[103,138,139] radiation,[140] and photodynamic therapy.[141,142] Given the variable natural history of CNV in AMD, acceptance of any of these new therapies likely will require therapeutic benefits proved through carefully designed randomized clinical trials. As the number of people over the age of 65 years in the United States and elsewhere doubles by about 2030, the importance of finding treatments for CNV in AMD will grow tremendously.
REFERENCES
1. Bressler SB, Maguire MG, Bressler NM, Fine SL: Macular Photocoagulation Study Group: Relationship of drusen and abnormalities of the retinal pigment epithelium to the prognosis of neovascular macular degeneration. Arch Ophthalmol 1990; 108:1442-1447.
2. Macular Photocoagulation Study Group : Risk factors for choroidal neovascularization in the second eye of patients with juxtafoveal or subfoveal choroidal neovascularization secondary to age-related macular degeneration. Arch Ophthalmol 1997; 115:741-747.
3. Gass JDM: Drusen and disciform macular detachment and degeneration. Arch Ophthalmol 1973; 90:206-217.
4. Smiddy WE, Fine SL: Prognosis of patients with bilateral macular drusen. Ophthalmology 1984; 91:271-277.
5. Strahlman E, Fine SL, Hillis A: The second eye of patients with senile macular degeneration. Arch Ophthalmol 1983; 101:1191-1193.
6. Green WR, McDonnell PH, Yeo JH: Pathologic features of senile macular degeneration. Ophthalmology 1985; 92:615-627.
7. Sarks SH: Ageing and degeneration in the macular region: A clinicopathologic study. Br J Ophthalmol 1976; 60:324-341.
8. Avery RL, Fekrat S, Hawkins BS, Bressler NM: Natural history of subfoveal subretinal hemorrhage in age-related macular degeneration. Retina 1996; 16:183-189.
9. Green RW, Enger C: Age-related macular degeneration histopathologic studies. The 1992 Lorenz E. Zimmerman Lecture. Ophthalmology 1993; 100:1519-1535.
10. Gass JDM: Pathogenesis of disciform detachment of the neuroepithelium. VI: Disciform detachment secondary to heredodegenerative, neoplastic and traumatic lesions of the choroid. Am J Ophthalmol 1967; 63:689.
11. Lim JI, Bressler NM, Marsh MJ, Bressler SB: Laser treatment of choroidal neovascularization in patients with angioid streaks. Am J Ophthalmol 1993; 116:414-423.
12. Heriot WJ, Henkind P, Bellhorn RW, Burns MS: Choroidal neovascularization can digest Bruch's membrane: A prior break is not essential. Ophthalmology 1984; 91:1603-1608.
13. Öffler KU, Lee WR: Basal linear deposit in the human macula. Graefes Arch Clin Exp Ophthalmol 1986; 224:493-501.
14. Penfold PL, Killingsworth MC, Sarks SH: Senile macular degeneration: The involvement of immunocompetent cells. Graefes Arch Clin Exp Ophthalmol 1985; 223:69-76.
15. Penfold PL, Provis JM, Billson FA: Age-related macular degeneration: ultrastructural studies of the relationship of leucocytes to angiogenesis. Graefes Arch Clin Exp Ophthalmol 1987; 225:70-76.
16. Ryan SJ: Development of an experimental model of subretinal neovascularization in disciform macular degeneration. Trans Am Ophthalmol Soc 1979; 77:707-745.
17. Ryan SJ: Subretinal neovascularization: natural history of an experimental model. Arch Ophthalmol 1982; 100:1804-1809.
18. Friedman E, Ivry M, Ebert E, et al: Increased scleral rigidity and age-related macular degeneration. Ophthalmology 1989; 96:104-108.
19. Eye Disease Case-Control Study (EDCCS) Group : Risk factors for neovascular age-related macular degeneration. Arch Ophthalmol 1992; 111:1701-1708.
20. Broekhuyse RM: The lipid composition of the aging sclera and cornea. Ophthalmologica 1975; 171:82.
21. Grossniklaus HE and Green WR: Choroidal neovascularization. Am J Ophthalmol 2004; 137:496-503.
22. Witmer AN, et al: Vascular endothelial growth factors and angiogenesis in eye disease. Prog Retin Eye Res 2003; 22:1-29.
23. Adamis AP, Shima DT: The role of vascular endothelial growth factor in ocular health and disease. Retina 2005; 25:111-118.
24. Bressler SB, Bressler NM, Alexander J, Green WR: Clinicopathologic correlation of occult choroidal neovascularization in age-related macular degeneration. Invest Ophthalmol Vis Sci 1991; 32:689.
25. Bressler SB, Bressler NM, Fine SL, et al: Natural course of choroidal neovascular membranes within the foveal avascular zone in senile macular degeneration. Am J Ophthalmol 1982; 93:157-163.
26. Bird AC: Macular disciform response and laser treatment. Trans Ophthalmol Soc UK 1977; 97:490-493.
27. Bressler NM, Frost LA, Bressler SB, et al: Natural course of poorly de-ned choroidal neovascularization associated with macular degeneration. Arch Ophthalmol 1988; 106:1537-1542.
28. Chandra SR, Gragoudas ES, Friedman E, et al: Natural history of disciform degeneration of the macula. Am J Ophthalmol 1974; 78:579-582.
29. Gragoudas ES, Chandra SR, Friedman E, et al: Disciform degeneration of the macula. II: Pathogenesis. Arch Ophthalmol 1976; 94:755-757.
30. Bressler NM, Bressler SB, Fine SL: Age-related macular degeneration. Surv Ophthalmol 1988; 32:375-413.
31. Boldt C, Bressler NM, Fine SL, Bressler SB: Age-related macular degeneration. Curr Opin Ophthalmol 1990; 1:247-257.
32. Moisseiev J, Bressler NM: Asymptomatic neovascular membranes in the second eye of patients with visual loss from age-related macular degeneration (AMD). Invest Ophthalmol Vis Sci 1990; 31:462.
33. Fine AM, Elman MJ, Ebert JE, et al: Earliest symptoms caused by neovascular membranes in the macula. Arch Ophthalmol 1986; 104:513-514.
34. Nasrallah F, Jalkh AE, Trempe CL, et al: Subretinal hemorrhage in atrophic age-related macular degeneration. Am J Ophthalmol 1989; 107:38-41.
35. Small ML, Green WR, Alpar JJ, et al: Senile macular degeneration: Clinicopathologic correlation of two cases with neovascularization beneath the retinal pigment epithelium. Arch Ophthalmol 1976; 94:601-607.
36. Doyle WJ, Davidorf FH, Makley TA, Dieruf WJ: Histopathology of an active lesion of ocular histoplasmosis. Ophthalmic Forum 1984; 2:106-111.
37. Macular Photocoagulation Study Group : Subfoveal neovascular lesions in age-related macular degeneration: Guidelines for evaluation and treatment in the Macular Photocoagulation Study. Arch Ophthalmol 1991; 109:1242-1257.
38. Klein ML, Zorizzo PA, Watzke RC: Growth features of choroidal neovascular membranes in age-related macular degeneration. Ophthalmology 1989; 96:1416-1421.
39. Vander JF, Morgan CM, Schatz H: Growth rate of subretinal neovascularization in age-related macular degeneration. Ophthalmology 1989; 96:1422-1429.
40. Macular Photocoagulation Study Group : Laser photocoagulation of subfoveal neovascular lesions in age-related macular degeneration. Results of a randomized clinical trial. Arch Ophthalmol 1991; 109:1219-1231.
41. Macular Photocoagulation Study Group : Laser photocoagulation of subfoveal recurrent neovascular lesions in age-related macular degeneration. Results of a randomized clinical trial. Arch Ophthalmol 1991; 109:1232-1241.
42. Submacular Surgery Trials Research Group : Guidelines for interpreting retinal photographs and coding -ndings in the submacular surgery trials (SST). SST report no. 8. Retina 2005; 25:253-268.
43. Barbazetto I, Burdan A, Bressler NM, et al: Treatment of Age-Related Macular Degeneration with Photodynamic Therapy Study Group; Vertepor-n in Photodynamic Therapy Study Group. Photodynamic therapy of subfoveal choroidal neovascularization with vertepor-n: fluorescein angiographic guidelines for evaluation and treatment - TAP and VIP report no. 2. Arch Ophthalmol 2003; 121:1253-1268.
44. Gragoudas ES, Adamis AP, Cunningham Jr ET, et al: VEGF Inhibition Study in Ocular Neovascularization Clinical Trial Group. Pegaptanib for neovascular age-related macular degeneration. N Engl J Med 2004; 351:2805-2816.
45. Rosenfeld PJ, Brown DM, Heier JS, MARINA Study Group , et al: Ranibizumab for neovascular age-related macular degeneration. N Engl J Med 2006; 355:1419-1431.
46. Brown DM, Kaiser PK, Michels M, ANCHOR Study Group , et al: Ranibizumab versus vertepor-n for neovascular age-related macular degeneration. N Engl J Med 2006; 355:1432-1444.
47. Soubrane G, Coscas G, Francais C, Koenig F: Occult subretinal new vessels in age-related macular degeneration. Ophthalmology 1990; 97:649-657.
48. Jalkh AE, Nasrallah FP, Marinelli I, Van de Velde F: Inactive subretinal neovascularization in age-related macular degeneration. Ophthalmology 1990; 97:1614-1619.
49. Schatz H, McDonald HR, Johnson RN: Retinal pigment epithelial folds associated with retinal pigment epithelial detachments in macular degeneration. Ophthalmology 1990; 97:658-665.
50. Grossniklaus HE, Green RW: Histopathologic and ultrastructural -ndings of surgically excised choroidal neovascular membranes in the submacular surgery trials. Arch Ophthalmol 1998; 116:745-749.
51. Lopez PF, Lambert HM, Grossniklaus HE, Sternberg Jr P: Well-de-ned subfoveal choroidal neovascular membranes in age-related macular degeneration. Ophthalmology 1993; 100:415-422.
52. Sorenson JA, Yannuzzi LA, Shakin JL: Recurrent subretinal neovascularization. Ophthalmology 1985; 92:1059-1075.
53. Bressler NM, Bressler SB, Alexander J, et al: Macular Photocoagulation Study Reading Center: loculated fluid: A previously undescribed fluorescein angiographic -nding in choroidal neovascularization associated with macular degeneration. Arch Ophthalmol 1991; 109:211-215.
54. Cantrill HL, Ramsay RC, Knobloch WH: Rips in the pigment epithelium. Arch Ophthalmol 1983; 101:1074-1079.
55. Decker WL, Sanborn GE, Ridley M, et al: Retinal pigment epithelial tears. Ophthalmology 1983; 90:507-512.
56. Gass JDM: Pathogenesis of tears of the retinal pigment epithelium. Br J Ophthalmol 1984; 68:514-519.
57. Green SN, Yarian D: Acute tear of the retinal pigment epithelium. Retina 1983; 3:16-20.
58. Hoskin A, Bird AC, Sehow K: Tears of detached retinal pigment epithelium. Br J Ophthalmol 1981; 65:417-422.
59. Yeo JH, Marcus S, Murphy RP: Retinal pigment epithelial tears: patterns and prognosis. Ophthalmology 1988; 95:8-13.
60. Bressler NM, Finkelstein D, Sunness JS, et al: Retinal pigment epithelial tears through the fovea with preservation of good visual acuity. Arch Ophthalmol 1990; 108:1694-1697.
61. Marmor MF: Mechanisms of normal retinal adhesion. In: Ryan SJ, ed. Retina, St. Louis: CV Mosby; 1989:76.
62. Tani PM, Buettner H, Robertson DM: Massive vitreous hemorrhage and senile macular choroidal degeneration. Am J Ophthalmol 1980; 90:525-533.
63. Kreiger AE, Sterling JH: Vitreous hemorrhage in senile macular degeneration. Retina 1983; 3:318-321.
64. Caswell AG, Kohen D, Bird AC: Retinal pigment epithelial detachments in the elderly: Classi-cation and outcome. Br J Ophthalmol 1985; 69:397-403.
65. Bird AC, Marshall J: Retinal pigment epithelial detachments in the elderly. Trans Ophthalmol Soc UK 1986; 105:674-682.
66. Elman MJ, Fine SL, Murphy RP, et al: The natural history of serous retinal pigment epithelium detachments in patients with age-related macular degeneration. Ophthalmology 1986; 93:224-230.
67. Gass JDM: Serous retinal pigment epithelial detachment with a notch. A sign of occult choroidal neovascularization. Retina 1984; 4:205-220.
68. Poliner LS, Olk RJ, Burgess D, Gordon ME: Natural history of retinal pigment epithelial detachments in age-related macular degeneration. Ophthalmology 1986; 93:543-550.
69. Teeters VW, Bird AC: The development of neovascularization in senile disciform macular degeneration. Am J Ophthalmol 1973; 76:1-18.
70. Singerman L: Laser photocoagulation for choroidal new vessel membrane complicating age-related macular degeneration associated with pigment epithelial detachments. Retina 1988; 8:115-121.
71. Melsop KA, Boothroyd DB, Hlatky MA: Quality of life and time trade-off utility measures in patients with coronary artery disease. Am Heart J 2003; 145:36-41.
72. Slakter JS, Stur M: Quality of life in patients with age-related macular degeneration: impact of the condition and bene-ts of treatment. Surv Ophthalmol 2005; 50:263-273.
73. Sharma S, Oliver-Fernandez A: Age-related macular degeneration and quality of life: how to interpret a research paper in health-related quality of life. Curr Opin Ophthalmol 2004; 15:227-231.
74. Brown GC, Brown MM, Sharma S: Difference between ophthalmologists' and patients' perceptions of quality of life associated with age-related macular degeneration. Can J Ophthalmol 2000; 35:127-133.
75. Bass EB, Marsh MJ, Mangione CM, et al: Submacular Surgery Trials Research Group. Patients' perceptions of the value of current vision: assessment of preference values among patients with subfoveal choroidal neovascularization - The submacular surgery trials vision preference value scale: SST report no. 6. Arch Ophthalmol 2004; 122:1856-1867.
76. Brown MM, Brown GC, Sharma S, et al: Utility values associated with blindness in an adult population. Br J Ophthalmol 2001; 85:327-331.
77. Stein JD, Brown GC, Brown MM, et al: The quality of life of patients with hypertension. J Clin Hypertens 2002; 4:181-188.
78. Mangione CM, Lee PP, Pitts J, et al: Psychometric properties of the National Eye Institute Visual Function Questionnaire (NEI-VFQ). NEI-VFQ Field Test Investigators. Arch Ophthalmol 1998; 116:1496-1504.
79. Dong LM, Childs AL, Mangione CM, et al: Submacular Surgery Trials Research Group. Health- and vision-related quality of life among patients with choroidal neovascularization secondary to age-related macular degeneration at enrollment in randomized trials of submacular surgery: SST report no. 4. Am J Ophthalmol 2004; 138:91-108.
80. Cahill MT, Banks AD, Stinnett SS, Toth CA: Vision-related quality of life in patients with bilateral severe age-related macular degeneration. Ophthalmology 2005; 112:152-158.
81. Mangione CM, Gutierrez PR, Lowe G, et al: Influence of age-related maculopathy on visual functioning and health-related quality of life. Am J Ophthalmol 1999; 128:45-53.
82. Stevenson MR, Hart PM, Montgomery AM, et al: Reduced vision in older adults with age related macular degeneration interferes with ability to care for self and impairs role as carer. Br J Ophthalmol 2004; 88:1125-1130.
83. Peli E, Goldstein RB, Young GM, et al: Image enhancement for the visually impaired. Simulations and experimental results. Invest Ophthalmol Vis Sci 1991; 32:2337-2350.
84. Rovner BW, Ganguli M: Depression and disability associated with impaired vision: the MoVies Project. J Am Geriatr Soc 1998; 46:617-619.
85. Krummenauer F, Braun M, Dick HB: Clinical outcome and subjective quality of life after photodynamic therapy in patients with age-related macular degeneration. Eur J Ophthalmol 2005; 15:74-80.
86. Coscas G, Soubrane G: Photocoagulation des neovaisseaux sous-retiniens dans la degenerescence maculaire senile par laser a argon. Resultats de l'etude randomisee de 60 cas. Bull Mem Soc Fr Ophthalmol 1982; 94:149-154.
87. Moor-elds Macular Study Group : Treatment of senile disciform macular degeneration: A single-blind randomized trial by argon laser photocoagulation. Br J Ophthalmol 1982; 66:745-753.
88. Macular Photocoagulation Study Group : Argon laser photocoagulation for senile macular degeneration: results of a randomized clinical trial. Arch Ophthalmol 1982; 100:912-918.
89. Macular Photocoagulation Study Group : Krypton laser photocoagulation for neovascular lesions of age-related macular degeneration. Results of a randomized clinical trial. Arch Ophthalmol 1990; 108:816-824.
90. Macular Photocoagulation Study Group : Laser photocoagulation for juxtafoveal choroidal neovascularization. Five-year results from randomized clinical trials. Arch Ophthalmol 1994; 112:500-509.
91. Macular Photocoagulation Study Group : Occult choroidal neovascularization: Influence on visual outcome in patients with age-related macular degeneration. Arch Ophthalmol 1996; 114:400-412.
92. Macular Photocoagulation Study Group : Argon laser photocoagulation for neovascular maculopathy after -ve years. Results from randomized clinical trials. Arch Ophthalmol 1991; 109:1109-1114.
93. Macular Photocoagulation Study Group : Persistent and recurrent neovascularization after krypton laser photocoagulation for neovascular lesions of age-related macular degeneration. Arch Ophthalmol 1990; 108:825-831.
94. Macular Photocoagulation Study Group : Persistent and recurrent neovascularization after krypton laser photocoagulation for neovascular lesions of ocular histoplasmosis. Arch Ophthalmol 1989; 107:344-352.
95. Macular Photocoagulation Study Group : The influence of treatment coverage on the visual acuity of eyes treated with krypton laser for juxtafoveal choroidal neovascularization. Arch Ophthalmol 1995; 113:190-194.
96. Smiddy WE, Fine SL, Quigley HA, et al: Comparison of krypton and argon laser photocoagulation in simulated clinical treatment of primate retina. Arch Ophthalmol 1984; 102:1086-1092.
97. Han DP, Folk JC: Internal limiting membrane wrinkling after argon and krypton laser photocoagulation of choroidal neovascularization. Retina 1986; 6:215-219.
98. Goldberg MF, Herbst RW: Acute complications of argon laser photocoagulation. Arch Ophthalmol 1973; 89:311-318.
99. Macular Photocoagulation Study Group : Argon laser photocoagulation for ocular histoplasmosis. Results of a randomized clinical trial. Arch Ophthalmol 1983; 101:1347-1357.
100. Macular Photocoagulation Study Group : Laser photocoagulation for neovascular lesions nasal to the fovea associated with ocular histoplasmosis or idiopathic causes. Arch Ophthalmol 1995; 113:56-61.
101. Macular Photocoagulation Study Group : Visual outcome after laser photocoagulation for subfoveal choroidal neovascularization secondary to age-related macular degeneration: The influence of initial lesion size and initial visual acuity. Arch Ophthalmol 1994; 112:480-488.
102. Jampol LM: Hypertension and visual outcome in the Macular Photocoagulation Study. Arch Ophthalmol 1991; 109:789-790.
103. Bressler NM, Bressler SB: Indocyanine green angiography: can it help preserve the vision of our patients. Arch Ophthalmol 1996; 114:747-749.
104. Maguire JI, Benson WE, Brown GC: Treatment of foveal pigment epithelial detachments with contiguous extrafoveal choroidal neovascular membranes. Am J Ophthalmol 1990; 109:523-529.
105. Bressler NM, Bressler SB: Laser treatment in macular degeneration and histoplasmosis. Ophthalmol Clin North Am 1989; 4:565-581.
106. Chamberlin JA, Bressler NM, Bressler SB, et al: The use of fundus photographs and fluorescein angiograms in the identi-cation and treatment of choroidal neovascularization in the Macular Photocoagulation Study. Ophthalmology 1989; 96:1526-1534.
107. Schachat AP, Chambers WA, Liesegang TJ, Albert DA: Safe and effective. Ophthalmology 2003; 110:2073-2074.
108. Rosenfeld PJ, Moshfeghi AA, Pulia-to CA: Optical coherence tomography -ndings after an intravitreal injection of bevacizumab (Avastin) for neovascular age-related macular degeneration. Ophthalmic Surg Lasers Imaging 2005; 36:331-335.
109. Shahar J, Avery RL, Heilweil G, et al: Electrophysiologic and retinal penetration studies following intravitreal injection of bevacizumab (Avastin). Retina 2006; 26:262-269.
110. Avery RL, Pieramici DJ, Rabena MD, et al: Intravitreal bevacizumab (Avastin) for neovascular age-related macular degeneration. Ophthalmology 2006; 113:363-372.
111. Eyetech Pharmaceuticals Inc : Brie-ng Document for the Dermatologic and Ophthalmic Drugs Advisory Committee. Pegaptanib sodium injetion in the treatment of neovascular age-related macular degeneration. NDA 21.756, Aug 27, 2004. Available: http://www.fda.gov/ohrms/dockets/ac/04/brie-ng/2004-4053B1_01_Eyetech-Brie-ng-Doc.pdf![]() May 9, 2006
May 9, 2006
112. Gonzales CR: VEGF Inhibition Study in Ocular Neovascularization (VISION) Clinical Trial Group. Enhanced ef-cacy associated with early treatment of neovascular age-related macular degeneration with pegaptanib sodium: an exploratory analysis. Retina 2005; 25:815-827.
113. Rosenfeld PJ, Schwartz SD, Blumenkranz MS, et al: Maximum tolerated dose of a humanized anti-vascular endothelial growth factor antibody fragment for treating neovascular age-related macular degeneration. Ophthalmology 2005; 112:1048-1053.
114. Eyetech Study Group : Anti-vascular endothelial growth factor therapy for subfoveal choroidal neovascularization secondary to age-related macular degeneration: phase II study results. Ophthalmology 2003; 110:979-986.
115. Kabbinavar F, Hurwitz H, Fehrenbacher L, et al: Phase II, randomized trial comparing bevacizumab plus fluorouracil (FU)/leucovorin (LV) with FU/LV alone in patients with metastatic colorectal cancer. J Clin Oncol 2003; 21:60-65.
116. Trobe JD, Kraft R, Krischer JP: Doctor: patient communication in ophthalmic outpatient visits. Ophthalmology 1983; 90:51a-55a.
117. Taub SJ: The Internet's role in patient/physician interaction: bringing our understanding in line with online reality. Compr Ophthalmol Update 2006; 7:25-30.
118. Genentech, Press release. Preliminary phase III data from head-to-head study of lucentis shows lucentis improved vision compared to visudyne in patients with wet age-related macular degeneration. Jan 14, 2006. Available: http://www.gene.com/gene/news/press-releases/display.do?method=detail&id=9307![]() Jul 25, 2006
Jul 25, 2006
119. Hewson MG, Kindy PJ, Van Kirk J, et al: Strategies for managing uncertainty and complexity. J Gen Intern Med 1996; 11:481-485.
120. Rosenfeld PJ, Heier JS, Hantsbarger G, Shams N: Tolerability and ef-cacy of multiple escalating doses of ranibizumab (Lucentis) for neovascular age-related macular degeneration. Ophthalmology 2006; 113:632.e1.
121. Charters L: Intravitreal anti-VEGF drugs are step forward in AMD management. Ophthalmology Times. Dec 15, 2005. Available: http://www.agingeye.net/mainnews/lucentis.php![]() Jul 21, 2006
Jul 21, 2006
122. American College of Physicians : Primer on 95% CIs for the number needed to treat. Eff Clin Pract 1999. Available: www.acponline.org/journals/ecp/mayjun99/primer.pdf![]() Jul 21, 2006
Jul 21, 2006
123. Ebrahimzadeh H, Davalos R, Lee PP: Literacy levels of ophthalmic patient education materials. Surv Ophthalmol 1997; 42:152-156.
124. Morris NS, MacLean CD, Chew LD, Littenberg B: The Single Item Literacy Screener: evaluation of a brief instrument to identify limited reading ability. BMC Fam Pract 2006; 24(7):21.
125. Spaide RF, Laud K, Fine HF, et al: Intravitreal bevacizumab treatment of choroidal neovascularization secondary to age-related macular degeneration. Retina 2006; 26:383-390.
126. Press release: PIER year 1 clinical trial results. Available: http://www.medicalnewstoday.com/medicalnews.php?newsid=44460![]() Nov 7, 2006
Nov 7, 2006
127. Edwards MG, Schachat AP, Bressler SB, Bressler NM: Outcome of cataract operations performed to permit diagnosis, to determine eligibility for laser therapy, or toperform laser therapy of retinal disorders. Am J Ophthalmol 1994; 118:440-444.
128. Kwiterovich KA, Maguire MG, Murphy RP, et al: Frequency of adverse systemic reactions after fluorescein angiography. Results of a prospective study. Ophthalmology 1991; 98:1139-1142.
129. Press release: NEI Statement: NIH Stimulates the development and testing of new therapies for advanced AMD. Available: www.nei.nih.gov/news/statements/amd_therapy.asp![]() Nov 7, 2006
Nov 7, 2006
130. Bennett SR, Folk JC, Blodi CF, Klugman M: Factors prognostic of visual outcome in patients with subretinal hemorrhage. Am J Ophthalmol 1990; 109:33-37.
131. Berrocal MH, Lewis ML, Flynn Jr HW: Variations in the clinical course of submacular hemorrhage. Am J Ophthalmol 1996; 122:486-493.
132. Vander JF, Federman JL, Greven C, et al: Surgical removal of massive subretinal hemorrhage associated with age-related macular degeneration. Ophthalmology 1991; 98:23-27.
133. Lewis H: Intraoperative -brinolysis of submacular hemorrhage with tissue plasminogen activator and surgical drainage. Am J Ophthalmol 1994; 118:559-568.
134. Macular Photocoagulation Study Group : Five-year follow-up of fellow eyes of individuals with ocular histoplasmosis and unilateral extrafoveal or juxtafoveal choroidal neovascularization. Arch Ophthalmol 1996; 114:677-688.
135. Bressler NM, Bressler SB: Preventative ophthalmology: Age-related macular degeneration. Ophthalmology 1995; 102:1206-1211.
136. Bressler NM, Maguire MG, Murphy PL, et al: Macular scatter ('grid') laser treatment of poorly demarcated subfoveal choroidal neovascularization in age-related macular degeneration: results of a randomized pilot trial. Arch Ophthalmol 1996; 114:1456-1464.
137. Bressler NM: Submacular surgery: Are randomized trials necessary. Arch Ophthalmol 1995; 113:1557-1560.
138. Slakter JS, Yannuzzi LA, Sorenson JA, et al: A pilot study of indocyanine green videoangiography-guided laser photocoagulation of occult choroidal neovascularization in age-related macular degeneration. Arch Ophthalmol 1994; 112:465-472.
139. Guyer DR, Yannuzzi LA, Ladas I, et al: Indocyanine green-guided laser photocoagulation of focal spots at the edge of plaques of choroidal neovascularization. Arch Ophthalmol 1996; 114:693-697.
140. Hart PM, Chakravarthy U, Mackenzie G, Archer DB: Telepathy for subfoveal choroidal neovascularization of age-related macular degeneration: Results of follow up in a non-randomised study. Br J Ophthalmol 1996; 80:1046-1050.
141. Gragoudas ES, Schmidt-Erfurth U, Sickenberg M, et al: Results and preliminary dosimetry of photodynamic therapy for choroidal neovascularization in age-related macular degeneration in a phase I/II study. Invest Ophthalmol Vis Sci 1997; 38-4:S17.
142. Schmidt-Erfurth U, Miller JW, Sickenberg M, et al: Photodynamic therapy for choroidal neovascularization in a phase I/II study. Preliminary results of multiple treatments. Invest Ophthalmol Vis Sci 1997; 38-4:S17.