Chiara M. Eandi,
Christina M. Klais,
K. Bailey Freund,
Lawrence A. Yannuzzi
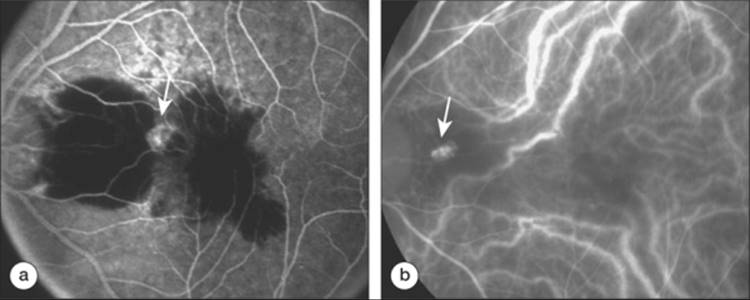
More than two decades ago, a peculiar hemorrhagic disorder of the macula, polypoidal choroidal vasculopathy (PCV) was first described (see Yannuzzi LA: Idiopathic polypoidal choroidal vasculopathy. Presented at the Annual Macular Society Meeting, Miami, FL, 1982) This entity has also been designated by Kleiner and associates as 'posterior uveal bleeding syndrome'[1,2] and by Stern and co-workers as 'multiple recurrent retinal pigment epithelium (RPE) detachments in black women'.[3] In 1990, Yannuzzi and colleagues suggested the term idiopathic polypoidal choroidal vasculopathy (IPCV) because the pathogenesis was unknown, the primary abnormality involved the choroidal circulation, and the characteristic lesion was an inner choroidal vascular network of vessels ending in an aneurismal bulge or outward projection, visible clinically as a reddish-orange, spheroid, polyp-like structure.[4] This entity has characteristic morphological features that distinguish it from other exudative maculopathies. Clinically it was associated with multiple, recurrent, serosanguineous detachments of the RPE and neurosensory retina secondary to leakage and bleeding from the peculiar choroidal vascular lesion (Fig. 151.1).
In recent years, indocyanine green (ICG) angiography has been used to detect and characterize the PCV abnormality with enhanced sensitivity and specificity,[5,6] expanding further the spectrum of PCV. This allows us to describe the pathogenesis, clinical manifestations, demographic profile, fluorescein and ICG angiographic findings, natural course, modalities of treatment, and visual prognosis in patients with PCV with greater detail and precision.[7,8]
|
|
|
|
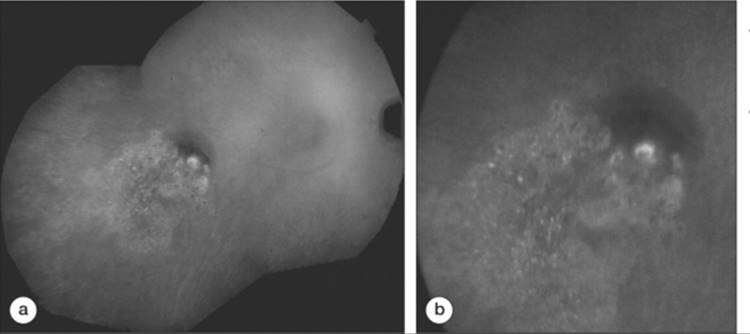
FIGURE 151.1 (a) The fluorescein angiogram shows a large serosanguineous detachment of the pigment epithelium that extends in the inter-papillo-macular region and a subfoveal hemorrhage with an adjacent hyperfluorescent spot (white arrow). (b) The corresponding ICG angiogram reveals the exact location of the vascular choroidal polypoidal abnormality in the peripapillary area (black arrow). |
PATHOGENESIS
Although the pathogenesis of PCV is not completely clear, new information is now available that might help in our understanding of its possible causative factor and clinical nature. PCV has been first described in African-American females.[3,9] However, Asian patients are also at risk for developing PCV, and white patients can definitely develop the disorder as well.[7,9-11] This predisposition for pigmented races contrasts the relative immunity to age-related macular degeneration (AMD) and disciform scarring seen in these individuals.[12-14] Lafaut et al suggested a possible coexistence of AMD and PCV, a finding certainly supported by our own clinical experience.[15] In spite of multiple, recurrent serosanguineous macular detachments, significant fibrous proliferation typical of end-stage neovascularized AMD is unusual in PCV.[16]
Although there is no available clinical pathologic confirmation, in essence the vascular abnormality in PCV appears to be a singular lesion with tubular and polypoidal components that vary in size. The vascular lesion itself appears to be singular and progressive. It does not occur solely in the peripapillary region as originally believed, but it may also present as an isolated island within the central macula. It is generally thought that PCV originates in the inner choroid.
Lafaut et al reported light microscopic findings in submacular tissue removed from an eye with PCV in AMD.[15] They described a sub-RPE, intra-Bruch's fibrovascular membrane containing several dilated thin-walled vessels under diffuse drusen. These abnormal vessels are lined by a thin endothelium with occasional pericytes. Some lesions were associated with islands of lymphocytic infiltration.
In spite of increasing case experience, the pathogenesis of the IPCV is still unknown. Traditionally, IPCV has not been linked to inflammatory processes; however, Ciardella et al reported a link between PCV and chorioretinal inflammation seen in three cases. They identified typical clinical findings of PCV after previous inflammatory disease.[8] Immunohistochemical findings in a case with PCV demonstrated both T and B lymphocytes in the choroid and fibrovascular tissue.[17]
There have been references to the association of PCV with other ocular disorders. Ross et al reported a correlation between retinal macroaneurysms and PCV in two hypertensive black females.[6] They proposed a relation between the retinal vascular changes in retinal macroaneurysms and hypertensive retinopathy such as vascular remodeling, aneurysmal dilation, and focal vascular constriction to the characteristic choroidal lesions in PCV. A recent study confirmed that choroidal blood flow increases significantly with increasing blood pressure.[18] Untreated hypertension was found to be a risk factor in development and progression of choroidal vascular pathologies.
Other potential pathogenic factors include the possibility of a peculiar choroidal tumor, vascular malformation, or systemic hypertension. In spite of these observations, the association of PCV, inflammation or other ocular disorders is still inconclusive and must be investigated further.
DEMOGRAPHIC FEATURES
AGE
PCV is usually diagnosed in patients between the age of 50 and 65 years, but the age of diagnosis can range from 20 to 80 years. The average age of onset for all affected patients from the literature is 60.1 years. Caucasian subjects usually present the disease at an older age.[19]
SEX
Previously, it was thought that PCV exclusively affects women. In recent studies it has been demonstrated that females are involved predominantly over males by a ratio of approximately 4.7:1. Among Asians, men seem to be more frequently affected.[16]
RACE
Individuals of African-American and Asian descent are at higher risk of developing PCV.[3,16] as this distinct disorder seems to preferentially affect pigmented individuals by a ratio of 4.2:1. However, more recent reports have shown that PCV occurs broadly in patients of other racial descents than it has been demonstrated in the past.[16,20-23]
Lafaut et al studied the prevalence of PCV in Caucasians with occult choroidal neovascularization (CNV). In a consecutive series of 374 eyes with occult CNV, 4% were diagnosed with PCV by ICG angiographic findings.[10] Pauleikhoff et al diagnosed PCV in 13.9% of 101 consecutive German patients with pigment epithelium detachment (PED).[24] Other investigators diagnosed PCV in 85% among a consecutive series of Caucasians presenting with large exudative or hemorrhagic PEDs in the absence of drusen.[25] Yannuzzi et al diagnosed PCV in 13 (7.8%) of 167 consecutive Caucasian patients with presumed neovascular AMD.[19] Scassellati-Sforzolini et al found a prevalence of 9.8% in Italian patients with newly diagnosed neovascular AMD.[11] PCV has also been reported in Irish,[26] French,[27] and German[28] subjects.
The prevalence of PCV among Chinese patients with AMD was found to be 9.3%.[29] In this patient series, the most common clinical finding at presentation was subretinal hemorrhage (63.6%) followed by exudative neurosensory detachment (59.1%), and hemorrhagic PED (59.1%). There was a predominance for males (68.4%). Most of the polypoidal lesions were at the macula (63.6%) and unilateral (84%). In contrast, a Japanese study reported a much higher prevalence of PCV among patients with newly diagnosed neovascular AMD.[30] They studied 164 eyes with PEDs and CNV and detected PCV in 59% of the eyes. In 70% of the patients, the PED had a hemorrhagic component. Other investigators confirmed the predilection for male gender in the Japanese population, as well as unilateral involvement.[16]
Recently, we found PCV in 14 (14%) of 100 consecutive newly diagnosed cases with neovascular AMD. They all presented occult or minimally classic lesion on fluorescein angiography, but the polyp-like CNV was visible when studied with ICG angiography (see Eandi CM, Iranmanesh R, Garuti S, et al: The nature and frequency of neovascular age related macular degeneration. ARVO 2005; Abstract 3311).
CLINICAL FINDINGS
PCV is a bilateral disease.[4] Most patients with the evidence of PCV in one eye eventually develop similar lesions in the fellow eye; however, several patients with PCV have been followed up for more than 10 years and so far demonstrate no evidence of the condition in the other eye. The lesion is characterized by the presence of dilated, choroidal vascular channels ending in orange, bulging, polyp-like dilations in the peripapillary and macular area. Vitreous hemorrhage, relatively minimal fibrous scarring, absence of drusen, retinal vascular disease, pathologic myopia, and signs of intraocular inflammation are accepted clinical features. Iida et al demonstrated that retinal microangiopathy may occur in a chronic macular detachment secondary to polypoidal CNV.[31]
THE VASCULAR LESION
In order to define the vascular lesion it is essential to use ICG angiography because it images the active neovascularization, whereas it does not show leakage at the site of serous pigment epithelial elevations (Fig. 151.1). Although the lesion of PCV is invariably localized to the choroidal vascular network, other characteristics of the lesion often differ. Significant variance is observed in size and location to the optic disk, fovea, and cross section of the retina.
SIZE
PCV usually categorized into small, medium or large lesions. The width of the lesions varies depending on the affected vascular channels. With involvement of outer choroidal vessels, the polypoidal lesions appear larger in size. Such lesions are easily diagnosed on biomicroscopy, especially when atrophic RPE is overlying; whereas angiography is needed to detect vascular lesions of small dimension. Teitawa et al reported large vascular networks expanding across the vascular arcade in 12 of 60 consecutive eyes diagnosed with PCV.[32]
When the middle choroidal vasculature is affected, polypoidal lesions appear smaller. In this case it is more challenging to diagnose on clinical examination, and the preferential method for diagnosis is ICG angiography.[4,5,33]
LOCATION
Choroidal vascular lesions of PCV are usually located in the peripapillary area (Figs 151.2 and 151.3), although recent evidence suggests that lesions could also be found in the central macula (Figs 151.4 and 151.5) and in the midperiphery (Fig. 151.6).[34,35] Lesions can be localized to a single location in the fundus or can be widespread involving more than one site.
|
|
|
|
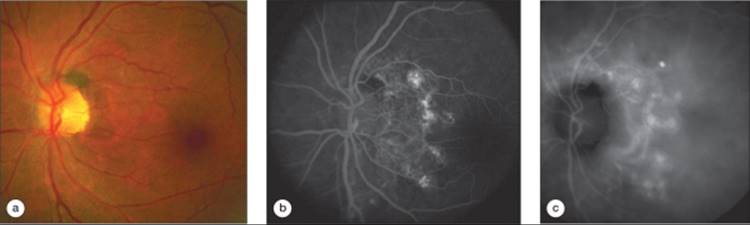
FIGURE 151.2 (a) Color photograph of a patient with IPCV. A choroidal abnormality in the peripapillary area shows a barely evident vascular pattern and polypoidal changes. (b) The fluorescein angiogram reveals the vascular abnormality because of the large size of the vascular element's abnormality and the overlying pallor or atrophy of the pigment epithelium. (c) The corresponding ICG angiogram more clearly delineates the vascular abnormality with branching inner choroidal vessels ending in polypoidal choroidal lesions. |
|
|
|
|
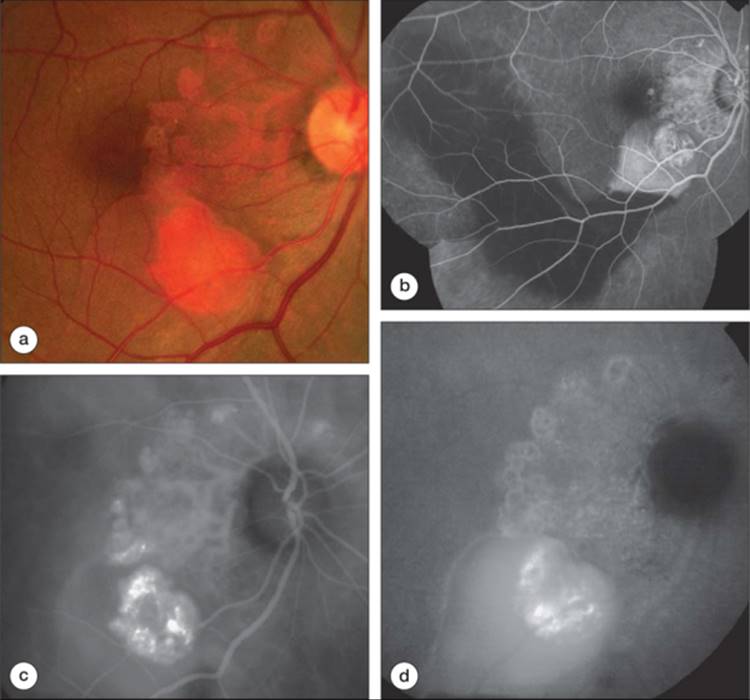
FIGURE 151.3 (a) Patient with IPCV shows the vascular abnormality, along with the reddish-orange elevation, beneath a PED. (b) The corresponding fluorescein angiogram highlights the vascular lesion in the peripapillary area and the serosanguineous detachment of the pigment epithelium that extends to the inferior and temporal macular area. (c) The early ICG study accentuates the polypoidal choroidal vascular changes. The reddish-orange lesion is shown to represent a ring of polypoidal lesions that project anteriorly into the subpigment epithelial space. (d) The late-stage ICG study shows staining of the margins of the polypoidal lesions with relative fading of the branching vessels (washout). |
|
|
|
|
FIGURE 151.4 (a) Color photograph of a patient with IPCV who presented with chronic serous lipid exudation in the macula, simulating central serous chorioretinopathy. (b) The ICG angiogram reveals the vascular abnormality and leaking polypoidal lesion. (c) The same patient after photocoagulation of leaking polypoidal lesions shows resolution of the exudative changes. |
|
|
|
|
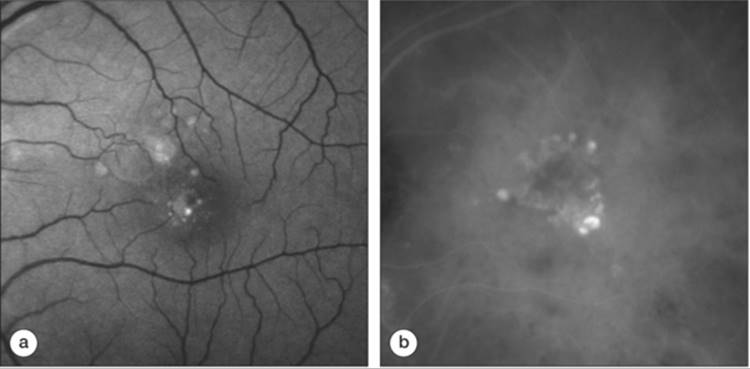
FIGURE 151.5 (a) The red-free photograph shows a small serosanguineous RPE detachment in the center of the fovea with pigmentary defects surrounding. (b) The ICG angiogram reveals a cluster of actively leaking polypoidal vessels in the corresponding area. |
|
|
|
|
FIGURE 151.6 (a) ICG composite late angiogram of a patient with a midequatorial PCV lesion presenting as a subretinal hemorrhage. (b) A magnified image of the lesion reveals the polypoidal vascular abnormality beneath the blood. |
Lafaut et al detected polypoidal lesion in the macula in 22 of 45 eyes, in the peripapillary area in 16 of 45, under the temporal vascular arcade in six of 45, and in the midperiphery in six of 45 eyes.[10]Yannuzzi and associates described a case of PCV isolated in the midperiphery of the temporal fundus associated with recurrent vitreous hemorrhage.[35]
Due to limited reports on clinocopathologic relationship between PCV lesions and retinal layers the precise location of the polypoidal vascular lesion in the cross-sectional structure remains unknown. Optical coherence tomography (OCT) studies were able to localize the polypoidal lesions under Bruch's membrane[36] but further studies are required to correlate the histologic finding and the results of OCT imaging.
NATURAL COURSE
The natural course of PCV is becoming better understood as the knowledge of PCV expands. This disease often follows a remitting-relapsing course, and clinically, it is associated with chronic, multiple, recurrent serosanguineous detachments of the neurosensory retina and the RPE with long-term preservation of good vision. Despite multiple recurrent serosanguineous macular detachments, fibrous proliferation resulting in typical plaque characteristics of end-stage neovascular AMD is not seen in eyes with PCV. On the other hand, this may present difficulties with the diagnosis of PCV when the lesion is inactive. In some cases, polypoidal lesions have evolved with resolution of the serosanguineous changes, and ICG angiography reveals a nonspecific plaque which can be interpreted as CNV of the usual type. Still, some patients may develop chronic atrophy and cystic degeneration of the fovea associated with severe vision loss. Others may experience vitreous hemorrhage or secondary CNV with disciform scarring and central vision loss (see Yannuzzi LA: Idiopathic polypoidal choroidal vasculopathy. Presented at the Annual Macular Society Meeting, Miami, FL, 1982).[2,13,17,37] Massive spontaneous choroidal hemorrhage is a rare but severe complication. Despite immediate drainage procedure the visual outcome is poor.[38]
Uyama et al followed 14 eyes of 12 consecutive patients with PCV for at least 2 years without any treatment.[16] They demonstrated that 50% of the eyes had a favorable course. In the remaining half, the disorder persisted for a long time with occasional recurrent hemorrhages and leakage, resulting in macular degeneration and vision loss. Eyes with cluster of grape-like polypoidal dilations of the vessels had a high risk for severe visual loss.
No underlying systemic factor has ever been associated with this disorder, except for recent evidence suggesting a possible association of PCV to hypertension and acquired macroaneurysms.[6] Smith et al reported a patient with PCV and concurrent sickle cell disease.[39] Other cases of PCV have been described in eyes with melanocytoma of the optic nerve, and central retina vein occlusion.[40,41] Neither of these case reports nor our own clinical experience demonstrates sufficient evidence finding an association between PCV and retinal vascular ischemic diseases, chorioretinal inflammation, or sickle cell disease.
When the lesion increases in size, it usually does so by three proposed mechanisms. The lesion may enlarge by simple vessel hypertrophy, by conversion of the lesion into the advancing edge of a vascular channel, and by unfolding of a cluster of aneurysmal elements and subsequent transformation into enlarging, vascular, tubular components. The latter mechanism is usually apparent on clinical examination as a large, reddish-orange subretinal mass corresponding to a cluster of aneurysmal elements that, on ICG angiography, project anteriorly from the inner choroid toward the outer retina. With time, these mass-like lesions flatten out and expand tangentially in their plane. The overlying RPE may show signs of variable atrophy.
DIAGNOSIS
The appearance of the vessels in PCV often depends on their location in the posterior pole. In patients with juxtapapillary lesions, the vascular channels may follow a radial, arching pattern and may be interconnected with smaller spanning branches which are more evident and numerous at the edges of the lesion. In patients with PCV limited to the macula, a vascular network often arises in the macula and follows an oval distribution pattern.
ICG angiography is useful to image the PCV choroidal abnormality.[5] In the initial phases of ICG videoangiograms, when the larger choroidal vessels fill with dye, a distinct network of vessels within the choroid becomes visible. Early in the course of the ICG study, the larger vessels of the PCV network start to fill before the retinal vessels, but the area within and immediately surrounding the network is relatively hypofluorescent compared with the uninvolved choroid. The vessels of the network appear to fill more slowly than the retina vessels. The network of vessels with ICG angiography generally appear to be more numerous than one would expect from clinical examination. Shortly after the network can be identified on the ICG angiogram, small hyperfluorescent 'polyps' become visible within the choroid.
During the mid-phase of the angiogram, however, the size of the lesions approximates the choroidal excrescences observed clinically. They appear to leak slowly and the surrounding hypofluorescent area becomes increasingly hyperfluorescent.
The late phase of angiogram is associated with a reversal of the pattern of fluorescence observed previously. The area surrounding the lesion becomes hyperfluorescent and the center of the lesion demonstrates hypofluorescence. The size of the lesion seems to influence the reversal pattern. The lesions that are less than 0.5-disk diameter in size appear to have intense uniform fluorescence, whereas internal details seem to be visible in larger polypoidal structures.[5] These findings, in turn, suggest presence of an internal architecture.[5]
The very late stages of ICG angiography demonstrate disappearance of the fluorescence from the lesions thus defining the term 'washout' (Fig. 151.3d). The 'washout' is only seen in nonleaking lesions, whereas the leaking lesions remain hyperfluorescent. Varying degrees of hypopigmentation of the RPE overlying an involved area may enhance visualization of the abnormal vessels, yet the late ICG staining results from the intrinsic characteristics of the lesion rather than from RPE alterations.[5]
OCT has also proved to be useful in the diagnosis of PCV. Iijima and co-workers were able to demonstrate the presence of the polypoidal lesions with OCT.[36,42] They also proposed that OCT may be able to differentiate the orange-red lesions in PCV from serous PEDs. Otsuji et al were able to demonstrate with OCT the presence of dome-like elevation of the RPE, and nodular appearance beneath the RPE in 14 patients with PCV[23]. Giovannini et al studied with OCT four eyes with PCV and found in all cases a characteristic hyper-reflectivity in the choroidal layers.[43] The use of OCT is of importance in these patients, as we recently reported. Although the polypoidal CNV eyes seldom had associated CME (7%), a dome-like pigment epithelium detachment was detected in 13 of 14 (93%) patients with PCV (see Eandi CM, Iranmanesh R, Garuti S, et al: The nature and frequency of neovascular age related macular degeneration. ARVO 2005; Abstract 3311).
DIFFERENTIAL DIAGNOSIS
The reddish-orange, subretinal masslike lesion seen in PCV is composed of multiple, polypoidal elements that extend from the PCV vascular lesion in the plane of the inner choroid, beneath the detached pigment epithelium toward the outer retina. The differential diagnosis of such a reddish-orange lesion under the retina includes choroidal hemangioma, metastasis from carcinoid syndrome, or more rarely, renal cell carcinoma, posterior scleritis, choroidal osteoma, and even CNV. ICG angiography is useful in differentiating the reddish-orange mass as it demonstrates an incomplete ring of polypoidal lesions emanating from the PCV vascular lesion. The cluster of polypoidal elements may be seen stereoscopically to extend toward the overlying retina. The other mimicking orange mass-like entities are not associated with these dilated inner choroidal vessels and polypoidal vascular elements beneath a pigment epithelial detachment.
Two decades ago, PCV was considered an entity with a distinct set of demographic characteristics, risk factors, natural course, clinical interpretation, and outcome from AMD. Features like Caucasian origin, macular location, presence of drusen, frequent recurrences, rapid rate of progression, disciform scarring, and poor visual prognosis were considered typical of AMD and used to differentiate the two entities.[13] Since the definition of PCV has expanded over the past two decades, the diagnosis is no longer restricted to those specific demographic attributes or to a specific retinal location.[10,35] In addition, it becomes more evident from the increasing volume of reports about PCV and our own clinical experience that the patients may have manifestations attributable to PCV and AMD. For example, some of our patients diagnosed with AMD undergoing ICG guided-laser treatment in the past had an exceptional and unexpected good outcome. Later, on reviewing their records, we determined that the patients with better results were actually patients with PCV-type CNV rather than a typical form of AMD.
Presently, we believe that PCV represents a subtype of CNV in AMD. PCV has also been reported in association with dry AMD.[44] However, some characteristics distinguish PCV from other types of CNV observed in AMD. Vascular proliferative changes associated with nonpolypoidal CNV tend to produce small caliber vessels that are associated with grayish colored membrane and grayish discoloration of the overlying retina. These vessels are not easily detected clinically.[21,45] In contrast, eyes with vascular changes typical for PCV form a network of vessels ending with saccular polypoidal lesions which have a redish-orange color and evident with slit lamp biomicroscopy unless they are covered by overlying blood or exudates.[4,9] Other angiographic and histopathologic characteristics tends to distinguish other types of CNV from PCV. AMD is associated with diminishing choroidal thickness and with signs of stromal fibrosis without any changes in the choriocapillaris size or evidence of inflammatory changes.[46]These findings were not observed clinocopathological reports on PCV.[15,17] Moreover, poorly defined CNV secondary to AMD is clinically associated with indistinct subretinal thickening and is not manifested by the detectable choroidal vascular channels terminating in polyp-like structures.
Fluorescein and ICG angiography can be used to distinguish the two types of vascular abnormalities. In both, CNV is characterized by diffuse late staining plaque.[12] In contrast, early-phase ICG angiography reveals PCV as a prominent vascular network which becomes 'washed out' during the late phase. The late phase is also distinguished by a typical outline of the nonleaking large choroidal vessels. If the vessels leak, staining in the walls of aneurysmal lesions and exudation into the surrounding choroid and subretinal space is observed.[5]
The natural course and clinical location of PCV are different from those of CNV. Subfoveal CNV tends to organize into a fibrotic or disciform scar leading to severe macular damage and vision loss.[21] PED seen in eyes with PCV virtually never forms a fibrotic scar,[4] whereas PED associated with occult CNV in AMD usually has a poor prognosis.[47] However, the spontaneously involuted or regressed lesion looks like a well-delineated plaque of occult CNV, even with ICG angiography.
Some eyes with PCV may present purely exudative changes masquerading chronic decompensation of the RPE, a variant of central serous chorioretinopathy (Fig. 151.4).[33] PCV lesions presenting with symptoms of central serous chorioretinopathy are usually small in size. Polypoidal lesions may resemble small PEDs clinically and on fluorescein angiography. The diagnosis becomes especially challenging in a patient with chronic central serous chorioretinopathy presenting lipid deposits in the central macula due to subfoveal polypoidal lesion. The principle of differentiating a small serous PED from a polypoidal lesion is with ICG angiography. Late staining of the PED is seen with fluorescein angiography and hypofluorescence with ICG imaging. In contrast, the polypoidal lesion is usually hyperfluorescent with ICG angiography because of its vascular nature. It is important to consider that the PCV lesion may exist under a PED. The portion of the PED overlying the polypoidal lesion will be hypofluorescent, and, if there is leakage, ICG dye may pool into the subpigment epithelial space. However, the majority of patients with PCV present with serosanguineous detachment of the RPE and neurosensory retina. These findings imply the presence of new blood vessel formation or CNV as causative factor.[21]
TREATMENT
Treatment for PCV is not yet well established. If the characteristic vascular lesion of PCV is observed, a conservative approach to management is recommended unless the lesion is associated with persistent or progressive exudative change threatening central vision. In this case conventional thermal laser treatment of the leaking polypoidal choroidal abnormality may be successful in causing resolution of the serosanguineous manifestation.[20,25,48] Yuzawa et al reported on visual improvement after conventional laser treatment of the entire PCV complex in nine of 10 eyes.[49] However, no randomized, controlled studies have been performed to prove the efficacy or safety of laser treatment. Moreover, when the CNV extends beneath the center of the fovea thermal laser treatment is not indicated due to damage of the overlying neurosensory retina and subsequent lead to reduced central vision.[50] It is possible that the loss of central vision due to the subfoveal treatment may exceed the damage produced by the natural course of PCV, although this is not known with any certainty. Conversely, it is not uncommon for patients with untreated subfoveal involvement with PCV to experience severe visual loss.
Due to limitations and uncertainty of the value of thermal laser coagulation and the potential devastating outcome of untreated subfoveal lesions, alternative modalities of treatment are currently being evaluated. These include vitrectomy and submacular removal of polypoidal vessels and subretinal blood. In some cases, vitrectomy is required to clear the media and recover the vision. Shiraga et al reported anatomic success in the surgical treatment of submacular hemorrhage associated with PCV.[51] However, the value of submacular surgery has been questioned in AMD because of the recurrences and poor vision outcomes.[52-54] Macular translocation is another surgical approach, but most patients diagnosed with PCV have relatively large vascular lesions and the surgical procedure has a number of serious complications.[55] Low-dose external beam irradiation does not appear to offer dramatic results, neither beneficial nor harmful[37,56]; on the other hand, it has been demonstrated that radiation therapy for AMD is a possible triggering factor for the development of PCV.[57]
Transpupillary thermotherapy may show promise in treating occult CNV,[58] but the value in PCV is not known. Diode laser photocoagulation has also been successfully used for the treatment of PCV.[20]
Recent studies reported encouraging results without complications after photodynamic therapy with verteporfin in subfoveal PCV lesions.[59-65] Spaide et al reported on improvement in visual acuity in 56% of patients undergoing photodynamic therapy, while in 31% of the patients the vision was stable, and in 12% a decrease in visual acuity was noted.[59] Quaranta et al found beneficial functional results in two cases of PCV treated with PDT with verteporfin.[63]
We recently reported stabilization or improvement on visual acuity in 80% of eyes with PCV treated with ICG guided PDT treatment. In our series of 30 eyes with PCV, the PDT treatment was applied only on the active lesion visible with ICG angiography, possibly reducing the collateral damage to the choriocapillaries. Angiographic and tomographic findings confirmed the resolution of the neovascular process in all cases (see Eandi CM, Freund KB, Ober MD, et al: Minimally selective treatment for neovascular age related macular degeneration. Annual Meeting of the Retina Society, Coronado, CA; 2005). Further trials of photodynamic therapy with verteporfin for PCV are required to address long-term efficacy and safety issues.
CONCLUSION
PCV appears to be a distinct clinical entity involving the choroidal circulation. The vascular abnormality is in the inner choroid, composed of two fundamental elements, a dilated network of vessels terminating in multiple areas of aneurysmal swelling in a polypoidal configuration. The polypoidal lesion itself accounts for the episodic leakage and bleeding seen in these patients. In patients with serosanguineous detachment of the pigment epithelium, particularly those with increased risk factors like African-American or Asian race, ICG angiography should be performed to evaluate the choroidal vascular abnormality in an attempt to establish a more definitive diagnosis. If the characteristic vascular lesion of PCV is seen, a conservative approach to management should be entertained unless there is a persistent or progressive exudative change that is threatening central macula. In that event, there may be a rationale for photocoagulation treatment of leaking aneurysmal or polypoidal components within the vascular lesion, but not the entire vascular complex. Photodynamic therapy seems to be a promising therapeutic modality; however, randomized clinical trials are needed to establish the efficacy and safety of the PDT treatment in the management of these patients.
SUMMARY
PCV seems to be a distinct clinical entity that should be differentiated from other forms of CNV associated with AMD and other known choroidal degenerative, inflammatory, and ischemic disorders. The principal abnormalities in PCV, notably the branching vascular network and polypoidal structures at the borders of the lesion, seem to be unique to this entity. In patients with serosanguineous detachment of the RPE, especially in those with increased risk factors, such as pigmented race, ICG angiography should be performed to evaluate the choroidal vascular abnormality in an attempt to establish a more definitive diagnosis. When ICG angiography confirms the characteristic vascular polyp-like lesion, a conservative management approach should be considered, unless there is a persistent or progressive exudative change threatening the fovea and the central vision. In that event, thermal lasercoagulation of leaking aneurysmal or polypoidal components within the vascular lesion may be a rationale. Reports on photodynamic therapy for PCV demonstrating encouraging results, but randomized clinical trials are required to establish this therapeutic modality in the management of patients with PCV.
REFERENCES
1. Kleiner RC, Brucker AJ, Johnson RL: Posterior uveal bleeding syndrome. Ophthalmology 1984; 91(Suppl 9):110.
2. Kleiner RC, Brucker AJ, Johnson RL: Posterior uveal bleeding syndrome. Retina 1990; 10:9-17.
3. Stern RM, Zakov N, Zegarra H, et al: Multiple recurrent serous sanguineous retinal pigment epithelial detachments in black women. Am J Ophthalmol 1985; 100:560-569.
4. Yannuzzi LA, Sorenson J, Spaide RF, Lipson B: Idiopathic polypoidal choroidal vasculopathy. Retina 1990; 10:1-8.
5. Spaide RF, Yannuzzi LA, Slakter JS, et al: Indocyanine green videoangiography of idiopathic polypoidal choroidal vasculopathy. Retina 1995; 15:100-110.
6. Ross RD, Gitter GA, Cohen C, Shoemaker KS: Idiopathic polypoidal choroidal vasculopathy associated with retinal arterial macroaneurysm and hypertensive retinopathy. Retina 1996; 16:105-111.
7. Yannuzzi LA, Ciardella AP, Spaide RF, et al: The expanding clinical spectrum of idiopathic polypoidal vasculopathy. Arch Ophthalmol 1997; 115:478-485.
8. Ciardella AP, Donsoff IM, Huang SJ, et al: Polypoidal choroidal vasculopathy. Surv Ophthalmol 2004; 49:25-37.
9. Perkovich BT, Zakov ZN, Berlin LA, et al: An update on multiple recurrent serosanguineous retinal pigment epithelial detachments in black women. Retina 1990; 10:18-26.
10. Lafaut BA, Leyes AM, Snyders B, et al: Polypoidal choroidal vasculopathy in Caucasians. Graefe's Arcg Clin Exp Ophthalmol 2000; 238:752-759.
11. Scassellati-Sforzolini B, Mariotti C, Bryan R, et al: Polypoidal vasculopathy in Italy. Retina 2001; 21:121-125.
12. Yannuzzi LA, Slakter JS, Sorenson JA, et al: Digital indocyanine videoangiography and choroidal neovascularization. Retina 1992; 12:191-223.
13. Ferris III FL: Senile macular degeneration: a review of epidemiological features. Am J Epidemiol 1983; 118:213-221.
14. Capone Jr A, Wallace RT, Meredith TA: Symptomatic choroidal neovascularization in blacks. Arch Ophthalmol 1994; 112:1091-1097.
15. Lafaut BA, Aisenbrey S, van den Broecke C, et al: Polypoidal choroidal vasculopathy pattern in age-related macular degeneration. A clinicopathologic correlation. Retina 2000; 20:650-654.
16. Uyama M, Wada M, Nagai Y, et al: Polypoidal choroidal vasculopathy: natural history. Am J Ophthalmol 2002; 133:639-648.
17. MacCumber MW, Dastgheib K, Bressler NM, et al: Clinicopathological correlation of the multiple recurrent serosanguineous retinal pigment epithelium detachments syndrome. Retina 1994; 14:143-152.
18. Polak K, Polska E, Luksch A, et al: Choroidal blood flow and arterial blood pressure. Eye 2003; 17:84-88.
19. Yannuzzi LA, Wong DW, Sforzolino MS, et al: Polypoidal choroidal vasculopathy and neovascularized age-related macular degeneration. Arch Ophthalmol 1999; 117:1503-1510.
20. Gomez-Ulla F, Gonzalez F, Torreiro MG: Diode laser photocoagulation in idiopathic polypoidal choroidal vasculopathy. Retina 1998; 18:481-483.
21. Green WR, McDonnel PJ, Yeo JH: Pathological features of senile macular degeneration. Ophthalmology 1985; 92:615-627.
22. Okubo A, Sameshima M, Uemara A: Clinicopathological correlation of polypoidal choroidal vasculopathy revealed by ultrastructural study. Br J Ophthalmol 2002; 86:1093-1098.
23. Otsuji T, Takahasi K, Fukushima I, Uyama M: Optical coherence tomographic findings of idiopathic polypoidal choroidal vasculopathy. Ophthalmic Surg Lasers 2000; 31:210-214.
24. Pauleikhoff D, Löffert D, Spital G, et al: Pigment epithelial detachment in the elderly. Clinical differentiation, natural course and pathogenic implications. Graefe's Arch Clin Exp Ophthalmol 2002; 240:533-538.
25. Ahuja RM, Stanga PE, Vingerling JR, et al: Polypoidal choroidal vasculopathy in exudative and hemorrhagic pigment epithelium detachments. Br J Ophthalmol 2000; 84:479-484.
26. Lip PL, Hope-Ross MW, Gibson JM: Idiopathic polypoidal choroidal vasculopathy: a disease with diverse clinical spectrum and systemic associations. Eye 2000; 5:695-700.
27. Mohand-Said M, Nodarian M, Salvanet-Bouccara A: Idiopathic polypoidal choroidal vasculopathy: 2 case report. J Fr Ophthalmol 2002; 25:517-521.
28. Schneider U, Gelisken F, Inhoffen W: Clinical characteristics of idiopathic polypoidal choroidal vasculopathy. Ophthalmologe 2001; 98:1186-1191.
29. Kwok AKH, Lai TYY, Chan CWN, et al: Polypoidal choroidal vasculopathy in Chinese patients. Br J Ophthalmol 2002; 86:892-897.
30. Imaizumi H, Takeda M: Knobby-like choroidal neovascularization accompanied with retinal pigment epithelial detachment. Nippon Ganka Gakkai Zasshi 1999; 103:527-537.
31. Iida T, Yannuzzi LA, Freund KB, et al: Retinal angiopathy and polypoidal choroidal vasculopathy. Retina 2002; 22:455-463.
32. Tateiwa H, Kuroiwa S, Gaun S, et al: Polypoidal choroidal vasculopathy with large vascular network. Graefe's Arch Clin Exp Ophthalmol 2002; 240:354-361.
33. Yannuzzi LA, Freund KB, Goldbaum M, et al: Polypoidal choroidal vasculopathy masquerading as central serous chorioretinopathy. Ophthalmology 2000; 107:767-777.
34. Moorthy RS, Lyon AT, Rabb MF, et al: Idiopathic polypoidal choroidal vasculopathy of the macula. Ophthalmology 1998; 105:1380-1385.
35. Yannuzzi LA, Nogueira FB, Spaide RF, et al: Idiopathic polypoidal choroidal vasculopathy: a peripheral lesion. Arch Ophthalmol 1998; 116:382-383.
36. Iijima H, Iida T, Imai M, et al: Optical coherence tomography of orange-red subretinal lesions in eyes with idiopathic polypoidal vasculopathy. Am J Ophthalmol 2000; 129:21-26.
37. Spaide RF, Guyer DR, McCormick B, et al: External beam radiation therapy for choroidal neovascularization. Ophthalmology 1998; 105:24-30.
38. Yang SS, Fu AD, McDonald HR, et al: Massive spontaneous choroidal hemorrhage. Retina 2003; 23:139-144.
39. Smith RE, Wise K, Kingsley RM: Idiopathic polypoidal choroidal vasculopathy and sickle cell retinopathy. Am J Ophthalmol 2000; 129:105-111.
40. Bartlett HM, Willoughby B, Mandava N: Polypoidal choroidal vasculopathy in a patients with melanocytoma of the optic nerve. Retina 2001; 21:396-399.
41. Katsimpris JM, Petropoulas IK, Pharmakakis NM, Pournaras CJ: Idiopathic polypoidal choroidal vasculopathy associated with central retinal vein occlusion. J Fr Ophtalmol 2003; 26:489-492.
42. Iijima H, Imai M, Gohodo T, et al: Optical coherence tomography of idiopathic polypoidal choroidal vasculopathy. Am J Ophthalmol 1999; 127:301-305.
43. Giovannini A, Amato GP, D'Altobrando E, Giuliani M: Optical coherence tomography (OCT) in idiopathic polypoidal choroidal vasculopathy. Doc Ophthalmol 1999; 97:367-371.
44. Lois N: Idiopathic polypoidal choroidal vasculopathy in a patient with atrophic age-related macular degeneration. Br J Ophthalmol 2001; 85:1011-1012.
45. Gass JDM: Stereoscopic atlas of macular diseases, St Louis, CV Mosby, 1997.
46. Arnold JJ, Sarks SH, Killingworth MC, Sarks JP: Reticular pseudodrusen. Retina 1995; 15:183-191.
47. Pauleikhoff D, Radermacher M, Spital , et al: Visual prognosis of second eyes in patients with unilateral late exudative age-related macular degeneration. Graefe's Arch Clin Exp Ophthalmol 2002; 240:539-542.
48. Guyer DR, Yannuzzi LA, Ladas I, et al: Indocyanine green guided laser photocoagulation of focal spots at the edge of plaque of choroidal vascularization. Arch Ophthalmol 1996; 114:693-697.
49. Yuzawa M, Mori R, Haruyama M: A study of laser photocoagulation for polypoidal choroidal vasculopathy. Jpn J Ophthalmol 2003; 47:379-384.
50. Gass JDM: Biomicroscopical and histopathologic considerations regarding the feasibility of surgical excision of subfoveal neovascular membranes. Am J Ophthalmol 1994; 118:285-298.
51. Shiraga F, Matsuo T, Yokoe S, et al: Surgical treatment of submacular hemorrhage associated with idiopathic polypoidal choroidal vasculopathy. Am J Ophthalmol 1999; 128:147-152.
52. Merill PT, LoRusso FJ, Lomeo MD, et al: Surgical removal of subfoveal choroidal neovascularization in age-related macular degeneration. Ophthalmology 1999; 106:782-789.
53. Thomas MA, Grand MG, Williams DF, et al: Surgical management of subfoveal choroidal neovascularization. Ophthalmology 1992; 99:952-968.
54. Yazawa M, Isomae T, Mori R, Shimade H, Utsunomiya : I. Surgical excision versus laser photocoagulation for subfoveal choroidal neovascularization membranes with age-related macular degeneration: comparison of visual outcomes. Jpn J Ophthalmol 2001; 45:192-198.
55. Fujii GY, Pieramici DJ, Humayun MS, et al: Complications associated with limited macular translocation. Am J Ophthalmol 2000; 130:751-762.
56. Marcus D, Sheils W, Johnson M, et al: External beam irradiation of subfoveal choroidal neovascularization complicating age-related macular degeneration: one-year results of a prospective, double-masked, randomized clinical trial. Arch Ophthalmol 2001; 119:171-180.
57. Spaide RF, Leys A, Herrman-Delemazure B, et al: Radiation associated choroidal neovasculopathy. Ophthalmology 1999; 106:2254-2260.
58. Reichel E, Berrocal AM, Ip M, et al: Transpupillary thermotherapy of occult subfoveal choroidal neovascularization in patients with age-related macular degeneration. Ophthalmology 1999; 106:1908-1914.
59. Spaide RF, Donsoff I, Lam DL, et al: Treatment of polypoidal choroidal vasculopathy with photodynamic therapy. Retina 2002; 22:529-535.
60. Silva RM, Figueira J, Cachulo ML, et al: Polypoidal choroidal vasculopathy and photodynamic therapy with vertepor-n. Graefes Arch Clin Exp Ophthalmol 2005; 243:973-979.
61. Chan WM, Lam DS, Lai TY, et al: Photodynamic therapy with vertepor-n for symptomatic polypoidal choroidal vasculopathy: one-year results of a prospective case series. Ophthalmology 2004; 111:1576-1584.
62. Quaranta M, Mauget-Faysse M, Coscas G: Exudative idiopathic polypoidal vasculopathy and photodynamic therapy with vertepor-n. Am J Ophthalmol 2002; 134:277-280.
63. Hussain N, Hussan A, Natarajan S: Role of photodynamic therapy in polypoidal choroidal vasculopathy. Indian J Ophthalmol 2005; 53:101-104.
64. Lee SC, Seong YS, Kim SS, et al: Photodynamic therapy with vertepor-n for polypoidal choroidal vasculopathy of the macula. Ophthalmologica 2004; 21:193-201.
65. Rogers AH, Greenberg PB, Martidis A, Pulia-to CA: Photodynamic therapy of polypoidal choroidal vasculopathy. Ophthalmic Surg Lasers Imaging 2003; 34:60-63.