David P. Tingey,
Bradford J. Shingleton
Long after the immediate problems of ocular trauma have been resolved, glaucoma may persist or reappear even years or decades later. Recent cohort studies have examined the relationship of glaucoma following ocular injury to several baseline structural and functional ocular characteristics. The risk of developing glaucoma in 3627 patients in the United States Eye Injury Registry with penetrating ocular injury was 2.67%. The development of glaucoma in these patients was independently associated with advancing age, lens injury, poor baseline acuity and inflammation.[1] In a similar study, 6021 patients in the registry who experience ocular contusion injury were found to have a risk of developing glaucoma of 3.39% at 6 months after their injury. The development of glaucoma was independently associated with: advancing age, visual acuity worse than 20/200, iris injury, lens injury or angle recession.[2] A smaller prospective review of 100 consecutive patients with traumatic glaucoma in India were found to have a greater risk of postconcussional glaucoma associated with traumatic cataracts, angle recession of more than 180°, significant iris injury and displacement of the lens. Penetrating injuries were more likely to result in glaucoma if there was evidence of an adherent leucoma and/or evidence of lenticular damage or displacement. Awareness of the various forms and pathogenesis of glaucoma in traumatized eyes as well as potential risk factors is important in early detection and treatment as well as in recognizing which eyes might be at future risk for the development of late-onset glaucoma.
After an ocular injury, the intraocular pressure (IOP) may be found to be high or low initially. Several mechanisms exist to explain a low pressure. These mechanisms include aqueous hyposecretion based on ciliary contusion and inflammation, increased egress of aqueous through a cyclodialysis cleft, or loss of integrity of the wall of the globe. Elevated IOP has multiple causes as well, all of which tend to reflect a reduced facility of outflow of aqueous humor.
It is useful to categorize the types of glaucoma in trauma as either immediate onset or delayed onset (Table 206.1). The type of trauma is also important to consider and is conventionally divided into blunt and penetrating trauma. A broader classification would include chemicals, electromagnetic radiation, and surgery as additional causes of trauma that might induce glaucoma.
TABLE 206.1 -- Immediate and Delayed Causes of Traumatic Glaucoma
|
Immediate |
Delayed |
|
Contusion |
Angle recession |
|
Trabecular disruption |
Peripheral anterior synechiae |
|
Hyphema |
Lens-induced |
|
Massive choroidal hemorrhage |
Phacolytic |
|
Chemical (alkali) |
Phacomorphic |
|
Lens particle |
|
|
Lens subluxation |
|
|
Ghost cells |
|
|
Closure of cyclodialysis cleft |
|
|
Fibrous-epithelial downgrowth |
|
|
Retained intraocular foreign body |
|
|
Rhegmatogenous retinal detachment |
IMMEDIATE EARLY-ONSET GLAUCOMA AFTER TRAUMA
CONTUSION
Occasionally, IOP elevation in the setting of blunt trauma is noted in the absence of any obvious intraocular damage. The angle is typically open, and there is no evidence of anglerecession, trabecular disruption, or hyphema. Inflammation in the form of flare and cells in the anterior chamber may be present. The presumed mechanism of this pressure rise is acute inflammation of the trabecular meshwork with a corresponding reduction in the facility of outflow. This pressure rise is typically self-limited, and improvement may be hastened by a short course of topical antiinflammatory agents.
TRABECULAR DISRUPTION
Careful gonioscopy within 48 h of injury in patients with hyphema has documented evidence of trauma-related changes in the trabecular zone.[3] These abnormalities vary from sharply demarcated hemorrhage into Schlemm's canal and possibly the outer trabecular sheets to full-thickness rupture of the trabecular meshwork for part of its circumference. A trabecular flap may be created with a point of rupture at or just below the insertion of the trabecular sheets at Schwalbe's line. Hinging of the flap occurs at the region of the scleral spur. These lesions may or may not be associated with increased IOP at the time of injury. There are often other factors such as inflammation that could also account for the increase in IOP. Trabecular lesions tend to scar with time and become more difficult to recognize. It has been hypothesized by some that angle recession is only a marker for significant injury and that the late development of glaucoma may correlate better with the amount of trabecular disruption observed acutely.[3]
HYPHEMA
|
Key Points |
|||||||||
|
The presence of a hyphema after ocular trauma is an indicator of significant intraocular injury. Cho et al compared the clini-cal characteristics of 18 patients with very poor visual outcome after nonperforating hyphema to 166 patients with better visual outcome after nonperforating hyphema. The presence of posterior segment injuries, anterior segment injuries, poor initial visual acuity, glaucoma, vitreous hemorrhage and eyelid laceration were all associated with long term poor visual outcome.[4] There are several possible mechanisms for the occurrence of glaucoma in the setting of acute hyphema. They include contusion of the outflow apparatus, physical disruption of the meshwork, and plugging of the meshwork with red blood cells.
Acute pressure elevation may pose a threat to vision as a result of optic nerve damage or corneal staining. IOP can be elevated in as many as 27% of patients acutely; however, this pressure elevation is often mild and self-limited.[5]
The level and duration of IOP elevation that is safe for the optic nerve is difficult to quantitate. Susceptibility varies among patients. In a prospective study of 137 patients with traumatic hyphema, Read and Goldberg[5] found that optic atrophy tended to occur with pressures at or greater than 35 mmHg and durations varying from 5 to 14 days. Optic atrophy as a direct result of trauma may be a confounding factor.
The level and duration of IOP elevation required to produce corneal blood staining is also difficult to quantitate. Blood staining occurs more readily in the presence of a total hyphema that is allowed to remain for at least 6 days with IOPs elevated to greater than 25 mmHg.[5] Corneas with endothelial damage secondary to trauma or preexisting disease are more susceptible to blood staining with only marginal pressure elevation.
Severely elevated IOP may be found in patients with sickle-cell hemoglobinopathy after accumulation of even small amounts of blood in the anterior chamber.[6] The presumed mechanism is obstruction of trabecular outflow by sickled erythrocytes. Optic atrophy at only slightly elevated IOPs has also been reported in these patients.[6,7] Suboptimal blood flow to the optic nerve on the basis of sickling has been proposed as a mechanism for this sensitivity. Patients with either sickle-cell disease or trait are susceptible to these complications. Several of the conventional pharmacologic agents used for lowering IOP may be potentially harmful in the patient with sickle-cell hemoglobinopathy. Carbonic anhydrase inhibitors may increase sickling as a result of systemic acidosis. Since methazolamide theoretically causes less systemic acidosis than does acetazolamide, methazolamide may be a safer choice in this clinical situation. Carbonic anhydrase inhibitors or osmotic agents may increase hemoconcentration and viscosity in an already compromised ocular microvasculature. Acetazolamide can increase ascorbate in the aqueous, and this may worsen the sickling process. Epinephrine agents may further compromise blood flow as a result of vasoconstriction. The successful use of intracameral tissue plasminogen activator in a sickle cell patient with traumatic hyphema and acute glaucoma has been reported.[8] The presence of hyphema in the sickling patient calls for the judicious use of pharmacologic agents to control even mild pressure elevations and a lower threshold on the part of the clinician for performing a washout of sickled erythrocytes from the anterior chamber.
Rebleeding into the anterior chamber after an initial hyphema can be a potentially devastating complication. This typically occurs between days 2 and 6 after the initial injury. The reported incidence of rebleeding varies between 6% and 33%.[5,7,9,10] Rebleeding is of particular concern because it may be accompanied by markedly elevated IOP and its attendant complications. Aminocaproic acid has been shown to decrease the rate of rebleeding in some patients.[7,10] Some authors have advocated the use of systemic steroids for reducing the incidence of secondary hemorrhage[11,12]; however, Spoor and associates[13] showed no benefit from oral corticosteroids in a prospective study. Dieste and associates[14] described an unusual IOP complication with the use of aminocaproic acid. In patients with larger hyphemas (more than one-third of the anterior chamber), exaggerated clot lysis occasionally develops 1-2 days after cessation of aminocaproic acid therapy. The lysed cells and debris obstruct the trabecular outflow of aqueous humor. IOP elevation may be refractory to medical treatment and may require surgery.
The treatment of acute pressure elevation as a result of hyphema entails the use of conventional pharmacologic agents to control pressure elevation, with the exception of miotic agents. Cycloplegic agents and topical steroids are often used as well for the associated traumatic iritis. If topical or systemic steroids are used for the treatment of hyphema, the physician must be aware of the potential effect of IOP elevation with chronic steroid use in some patients.
Surgical intervention is reserved for cases in which the IOP cannot be controlled by conventional medicines and the pressure is potentially threatening to the optic nerve or cornea. Many surgical procedures have been reported, including anterior chamber washout,[15] clot expression,[16] delivery of the clot with a cryoprobe,[17] automated hyphemectomy,[18] and ultrasonic emulsification and aspiration.[19]Adjunctive procedures have included peripheral iridectomy in the setting of pupillary block resulting from the clot.[20] Trabeculectomy for short-term pressure control has been used.[21] Cyclodiathermy to control recurrent bleeding has also been described.[22]
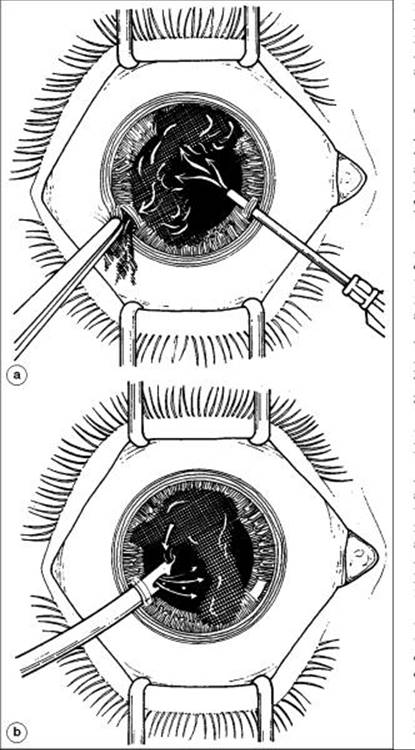
Paracentesis and anterior chamber washout is the simplest and safest procedure. Evacuation of suspended anterior chamber cells and debris is effective in lowering IOP and can be performed by simple irrigation or by manual coaxial irrigation or aspiration. Removal of the entire clot is not required. In addition to being relatively easy to perform, this technique spares the conjunctiva for future filtration surgery if required (Fig. 206.1).
|
|
|
|
FIGURE 206.1 Illustration of the technique of anterior chamber washout for hyphema with the use of direct irrigation (a) and the Simcoe coaxial irrigation-aspiration cannula (b). |
Glaucoma may also occur several years after the initial hyphema. This glaucoma may result from any of several mechanisms that are dealt with later in this chapter.
MASSIVE CHOROIDAL HEMORRHAGE
The occurrence of massive hemorrhage into the choroidal space is a rare cause of acute pressure elevation after ocular trauma. Typically, the anterior chamber is shallow both axially and peripherally. The red reflex is poor, and indirect ophthalmoscopy reveals choroidal elevation. The lens-iris diaphragm is pushed forward, resulting in obstruction of the trabecular meshwork. The IOP may be markedly elevated as a result of this secondary angle closure.
Initial treatment consists of a topical ?-blocker as well as oral carbonic anhydrase inhibitors and a systemic hyperosmotic agent, if needed. Miotics should be avoided because they may cause further shallowing of the anterior chamber. Cycloplegics may be effective in deepening the anterior chamber. High-dose oral steroids are recommended by some individuals who believe that steroids will stabilize the choroidal vessels.
Surgical intervention is required occasionally. Drainage of blood from the suprachoroidal space may be warranted in certain situations. Indications include persistent elevation of IOP that has not responded to medical therapy, lens-cornea apposition, and so-called kissing choroidals with retina-to-retina apposition. Generally, it is advisable to wait for several days if possible before draining the blood because this allows time for the blood to be fully sequestered in the suprachoroidal space.
Chronic synechial closure of the angle may be a long-term sequela of massive suprachoroidal hemorrhage. This may require later intervention in the form of medical therapy, laser iridoplasty (gonioplasty), surgical goniosynechialysis, conventional filtration surgery, or a cycloablative procedure, depending on the individual circumstances.
In the setting of age-related macular degeneration, trauma may rarely lead to massive choroidal detachment with intraretinal dissection. This results in a 'Y-suture' apposition of posterior segment tissues pushing the lens-iris diaphragm forward and leading to angle closure.[23] IOP rises dramatically, and vision is often reduced to no light perception. Medical or surgical therapy rarely restores vision.
CHEMICAL TRAUMA
Alkali burns are well known for their ability to cause severe damage to the ocular structures as a result of tissue saponification. This is in contrast to acids, which more often produce an injury that is self-limited as a result of tissue coagulation. Glaucoma is more often associated with alkali burns, and thus this section is restricted to alkali burns.
Glaucoma may be an immediate or late complication of an alkali burn. Hughes[24] in 1946 documented several cases of elevated IOP that occurred late after an alkali burn. It was not until the 1960s that pressure elevation was documented acutely following an alkali burn.[25,26] This pressure rise occurred in the setting of a gonioscopically open angle.
The nature of the acute pressure rise was studied in rabbits by Chiang and associates,[27] who demonstrated a dicrotic pressure rise after the application of sodium hydroxide. There was an immediate pressure rise of 40 mmHg, followed by a gradual decline in pressure to 20 mmHg above normal in 10 min. A second, gradual pressure rise then occurred, reaching 40 mmHg above normal at 1 h. At 3 h after application, the pressure was 20 mmHg above normal.
Paterson and Pfister[28] set out to determine the exact mechanisms of these pressure rises in rabbits. They believed that shrinkage of the outer coats of the eye was the major cause of the initial pressure spike. Lid contraction and extraocular muscle spasm were not significant factors in raising the pressure. Prostaglandin release with inflammation was implicated as the major factor in the second hypertensive phase. They also postulated that blockage of the trabecular meshwork with inflammatory debris might play a later role in the rise in IOP.
IOP may be overlooked in the initial evaluation and treatment of the patient with a severe alkali burn. In addition to the conventional therapies directed at the anterior segment consequences of an alkali burn, treatment of any pressure elevation is important. This includes topical ?-blocker therapy, oral carbonic anhydrase inhibitors, and systemic hyperosmotic agents as needed. Miotics should be avoided in the setting of intense inflammation. Topical epinephrine has been effective in blunting the second hypertensive phase in experimental animal models. Antiinflammatory medications and adequate cycloplegia are also important. Anterior chamber paracentesis and aspiration of aqueous fluid may be required if the IOP is extremely high during the initial hypertensive phase. This reduces the IOP and removes debris and alkali directly from the anterior chamber.
Glaucoma may appear or reappear years after the initial alkali burn. This is generally considered to be a result of ongoing inflammation with secondary peripheral anterior synechiae. The treatment of this late-onset glaucoma would include conventional medical and surgical therapies addressed at this underlying mechanism of chronic angle closure.
LATE-ONSET GLAUCOMA AFTER OCULAR TRAUMA
ANGLE RECESSION
Collins[29] gave the first pathologic description of angle recession resulting from blunt trauma to the eye in 1892. In 1949, D'Ombrain[30] commented on his observations of a chronic traumatic glaucoma that he believed was the result of a proliferative lesion scarring the trabecular meshwork. He made no observation of pathologic deepening of the anterior chamber angle. In 1962, Wolff and Zimmerman[31] tied together the pathologic entity of angle recession and the clinical phenomenon of unilateral chronic glaucoma following trauma.
Angle recession is common after blunt ocular trauma. In patients with traumatic hyphema, angle recession occurs in 71-100% of eyes.[32-35] Despite this high incidence of angle recession, glaucoma is uncommon, occurring in ?7-9% of eyes.[32,34,36] Some authors have attempted to correlate the degree of angle recession with the development of glaucoma. Alper[37] believed that the risk of glaucoma developing was highest if more than 240° of angle appeared recessed. One large population-based glaucoma survey found glaucoma in 8% (7/87) of eyes with 360° of angle recession.[38]
Elevated IOP may occur months or decades after the initial injury. Blanton[32] observed a bimodal pattern, with glaucoma occurring either within the first year or after 10 years. The earlier-onset group often had less angle recession, and the IOP rise was transient in some patients. Other authors have found that extensive angle recession equal to or more than 270° was usually present in the early-onset group.[1]
Pathologically, recession of the anterior chamber angle appears as a separation between the longitudinal and circular fibers of the ciliary body muscle.[31] The longitudinal muscles characteristically remain attached to the scleral spur. There is retrodisplacement of the iris root. Iridodialysis or cyclodialysis may also be observed. The lens may display changes such as cataract, subluxation, or dislocation. In the acute setting, frank hyphema may also be observed. Late evaluation shows the effects of healing. The inner circular muscle of the ciliary muscle may be atrophied, giving the ciliary body band a broad and more fusiform appearance. The trabecular meshwork displays variable degrees of fibrosis and hyalinization.
A newly formed hyaline membrane may be observed. This hyaline change is continuous with Descemet's membrane and extends over the trabecular meshwork for variable distances. Peripheral anterior synechiae may also be present.
The clinical presentation of glaucoma secondary to angle recession is variable and depends somewhat on the time of presentation relative to the initial injury. Elevated IOP immediately after injury may be due to extensive angle recession, although it may also be due to other causes, as cited earlier in this chapter. More often, angle-recession glaucoma presents years after the initial event as a chronic unilateral glaucoma. In a pathologic review of 100 eyes enucleated for unilateral glaucoma, Miles and Boniuk[39] found 11 eyes with angle deformity as the principal cause for the glaucoma. None of these deformities had been recognized clinically. Eight of these 11 patients gave a history of previous trauma to the eye ranging from 6 months to 24 years before the onset of glaucoma. In a population-based survey Salmon et al performed gonioscopy on 987 inhabitants of a small South African village. They found a cumulative lifetime prevalence of angle recession in the community of 14.6%. The prevalence of glaucoma in people with angle recession was 5.5% (8/146). Of 87 eyes with 360° of angle recession, only seven (8.0%) had glaucoma.[40]
It is important to attempt to elicit a history of previous ocular trauma when confronted with a case of unilateral glaucoma. Examination can often reveal asymmetry of anterior chamber depth between the two eyes, with the involved eye having a greater chamber depth. There are often associated findings of ocular trauma, such as tears in the iris sphincter or root. The iris stroma may be thinned, with pigmentation occurring in clumps. There may be a difference in pigmentation between thetwo irises as a result of blood or pigment having been dispersed into the chamber at the time of injury. Tonjum[41] evaluated injured eyes acutely and found that the pupillary sphincter was often paretic or paralyzed in the same sector as the chamber angle deformity. This pupillary change often, but not always, recovered with time. The lens may demonstrate subluxation with iridodonesis or phacodonesis, or it may be frankly dislocated. Cataractous changes may also be present. The posterior segment can also display signs of previous trauma such as pigment in the vitreous, macular edema, retinal pigment epithelial hyperplasia, choroidal or retinal scars, retinal tearing, or frank retinal detachment.
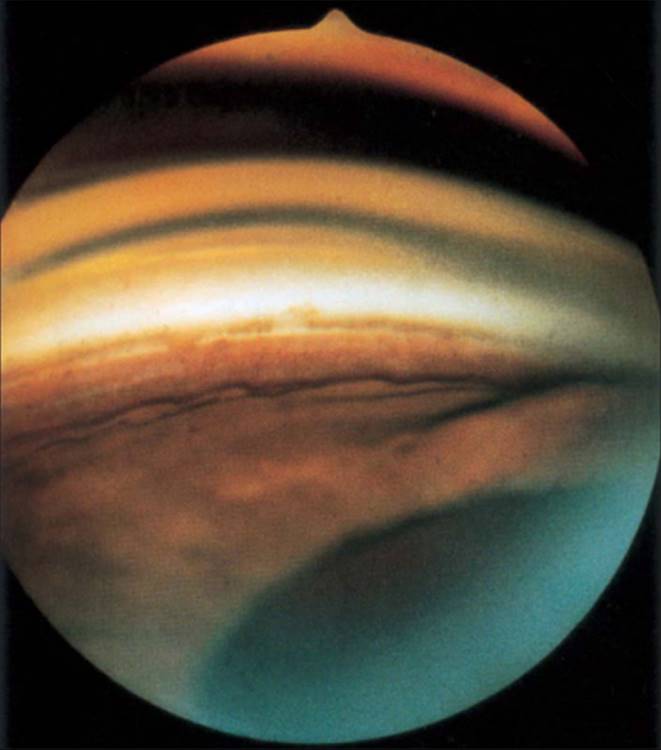
Gonioscopy reveals a deepening of the angle in which the exposed face of the ciliary body appears wider than is usual and the iris root appears posteriorly displaced (Fig. 206.2). Uveal processes are disrupted, and the scleral spur may appear abnormally white. Bilateral, simultaneous Koeppe gonioscopy is an effective technique for detecting subtle recession. A gray-white membrane is often observed covering the angle recess many years after the initial injury.[37] The optic nerve may display typical glaucomatous cupping that may be far advanced because the late and insidious onset of this glaucoma occasionally avoids early detection.
|
|
|
|
FIGURE 206.2 Gonioscopic view of traumatic angle recession. |
The mechanism of IOP elevation in this secondary open-angle glaucoma appears to be a decrease in aqueous filtration. Herschler[3] emphasized that the tear into the ciliary body is more of a marker for significant injury and that the glaucoma itself is related to accompanying scarring of the trabecular meshwork. He was able to document a high incidence of visible damage to the trabecular meshwork and Schlemm's canal in eyes undergoing gonioscopy within 48 h of injury. These trabecular lesions became less apparent over time as opposed to the ciliary body tears. The facility of outflow, as measured by tonography, is reduced and correlates with the degree of angle recession and glaucoma.[33] Tesluk and Spaeth[42] studied 13 patients in whom unilateral angle recession glaucoma had developed and found that ?50% of these patients had evidence of frank or probable glaucoma in their fellow eye on the basis of IOP, disk appearance, or visual field changes. This has raised the question of a possible underlying predisposition to the development of glaucoma in some injured patients.
The treatment of angle-recession glaucoma falls along conventional medical therapeutic routes. Failure of medicines to control the pressure requires further intervention. Argon laser trabeculoplasty may be helpful in some patients provided that the initial IOP is not too high.[43,44] Neodymium:yttrium-aluminum garnet laser trabeculopuncture was much more effective than argon laser trabeculoplasty in a small series of 11 Japanese patients with angle-recession glaucoma.[45] Filtration surgery is often effective in controlling the pressure if the conjunctiva has not been previously scarred by the injury itself or from previous surgical interventions resulting from related ocular injuries such as cataract or retinal detachment. Trabeculectomy may be less successful in posttraumatic angle-recession glaucoma. Mermoud et al found the success rate of trabeculectomy for angle-recession glaucoma to be 43% in 35 consecutive patients compared to a success rate of 74% in 35 consecutive matched primary open glaucoma patients. These authors advocated the routine use of antimetabolites in such cases.[46] These results were also supported by a retrospective analysis of 87 drainage procedures performed over an 8-year period in which trabeculectomy with antimetabolite outperformed trabeculectomy without antimetabolite and molteno implantation.[47] The effectiveness of using mitomycin C in filtering surgery for angle-recession glaucoma was demonstrated in a retrospective review of 43 consecutive procedures. Cumulative probability of success was 85% at 1 year and 81% at 2 years.[48] Failure of conventional filtration techniques may lead to the subsequent placement of a seton or to a cyclodestructive procedure, depending on the individual circumstances. A prospective case series examined 38 patients who received a molteno implant with a mean follow-up of 10.9 years. IOP of 21 mmHg or less (with or without hypotensive medication) occurred with a probability of 0.80 at 5 years and 0.72 at 10 years.[49]
PERIPHERAL ANTERIOR SYNECHIAE
Attachment of peripheral iris to the cornea or chamber angle has many causes. The essential elements required for peripheral anterior synechia formation are apposition and inflammation. Both of these may occur in the setting of ocular trauma. Organization of blood and inflammatory debris in the angle can occur following hyphema. Penetrating trauma may shallow the chamber for extended periods, resulting in extensive synechial closure of the angle. Endothelialization of the angle has been observed after blunt trauma with resultant angle closure. Penetrating trauma may result in epithelial or fibrous downgrowth into the anterior chamber, causing synechial closure. Massive choroidal hemorrhage leads to apposition, which may remain after the hemorrhage has resolved. The occurrence of synechial closure after trauma necessitates careful and repeated gonioscopy after a traumatic event.
Treatment of synechial closure can often be directed at attempting to reopen the angle, particularly if the intervention occurs early rather than late. Iridogonioplasty with the argon laser may be sufficient to pull the iris away from the angle. Failing this, surgical goniosynechialysis may be effective in reopening the angle for filtration. If the angle is permanently closed, with ensuing high IOP, therapy is directed at lowering the pressure with more conventional medical and surgical methods.
GHOST-CELL GLAUCOMA
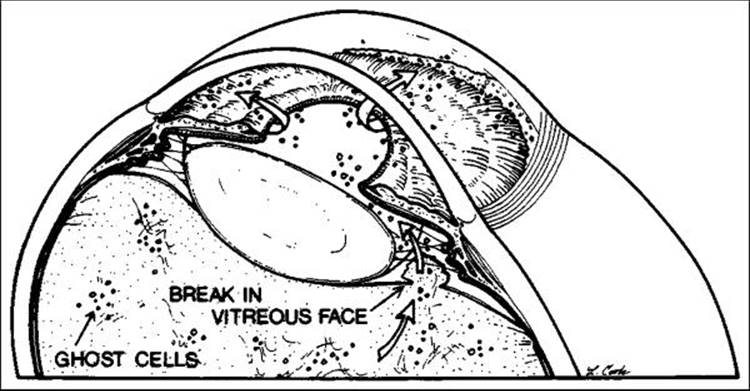
Ghost-cell glaucoma was initially described by Campbell and colleagues.[50] They showed that after vitreous hemorrhage, fresh red blood cells degenerated into ghost cells in the vitreous usually within 1 or 2 weeks (Fig. 206.3). In the event of anterior hyaloid face disruption, these cells gain access to the anterior chamber. The normal red blood cell is pliable and passes through the trabecular meshwork, whereas the ghost cells are rigid and do not pass through the meshwork easily. These cells produce an obstruction to aqueous outflow with a resultant rise in IOP. Ghost-cell glaucoma has been reported to occur after cataract extraction, vitrectomy, or trauma.
|
|
|
|
FIGURE 206.3 Ghost-cell glaucoma, demonstrating hemorrhage within the vitreous cavity and escape of ghost cells through a break in the anterior hyaloid face into the anterior chamber. Open arrows indicate route of egress of ghost cells from the posterior chamber into the anterior chamber. |
Campbell reviewed the clinical characteristics of 14 patients with traumatic ghost-cell glaucoma.[51] He found that all patients shared a common clinical course: severe trauma to the eye causing anterior chamber and vitreous hemorrhages. The anterior chamber hemorrhages gradually cleared. In the vitreous, the fresh red blood cells slowly converted to ghost cells that were then able to pass forward through a disrupted hyaloid face. The ghost cells had a characteristic ochre color that distinguished them from fresh red blood cells. Occasionally, they would layer out in the anterior chamber and create a 'pseudohypopyon'. The glaucoma occurred anywhere from 2 weeks to 3 months after the trauma but was most common 1 month after the injury. The IOP was usually in the range of 30-50 mmHg.
Histopathologic examination of one eye revealed a relatively normal-looking angle with ghost cells in the anterior chamber. The vitreous cavity demonstrated degenerated macrophages laden with red blood cell debris along the hyaloid face. Ghost cells were present in the vitreous cavity. The anterior hyaloid face appeared disrupted. Ghost cells had a characteristic crenated shrunken appearance by phase contrast microscopy. Heinz bodies representing denatured hemoglobin were appreciated in the cytoplasm of some ghost cells.[51]
The treatment of ghost-cell glaucoma includes conventional medical therapy followed by surgery in patients who do not respond. Campbell[51] found that less than half of his patients responded to medical therapy alone. The surgery of choice is anterior chamber irrigation, which is often effective. If this should fail, a pars plana vitrectomy may be necessary to ensure complete removal of all blood components trapped in the vitreous body.
LENS-INDUCED GLAUCOMA
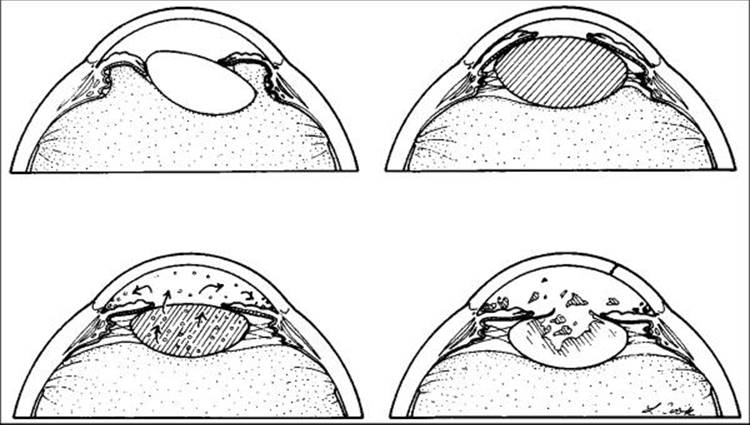
The lens-induced glaucomas are a group of secondary glaucomas that share the lens as a common pathogenic cause (Fig. 206.4). The angle in this category of glaucomas may be open or closed. The major categories of lens-induced glaucoma are lens dislocation, lens swelling, phacolytic glaucoma, and lens particle glaucoma.[52] All these glaucomas may be associated with previous trauma to the eye
|
|
|
|
FIGURE 206.4 The four types of lens-induced glaucoma. Clockwise from upper left: lens subluxation, phacomorphic, lens particle, and phacolytic. |
Lens Dislocation
The lens may be dislocated or subluxed as a direct result of trauma that disrupts the zonules. Once mobilized, the lens may advance forward, producing pupillary block with angle closure. With a complete dislocation of the lens posteriorly, the pupil may become blocked with vitreous, which can also produce a pupillary block angle-closure glaucoma. Secondary glaucoma as a result of traumatic lens dislocation was found to occur in 88% of 106 patients in a review from China.[53]
Clinically, such patients may present with an acutely painful red eye and decreased vision. A previous history of trauma is helpful in making a diagnosis because the presentation may mimic primary acute angle-closure glaucoma. The cornea is edematous. The chamber is shallowed both axially and peripherally with iris convexity. The angle appears closed gonioscopically. Comparison of refractive error, chamber depth, and angle depth of both eyes may help to rule out primary angle-closure glaucoma if the unaffected eye does not have a shallow configuration. If vitreous is blocking the pupil, this may be appreciated at slit-lamp examination. The posteriorly dislocated lens may also be seen by ophthalmoscopy in these cases.
Treatment of this form of glaucoma is directed at relieving the pupillary block. Generally, this is achieved with laser iridotomy or surgical iridectomy. Lensectomy may be undertaken only when other methods of visual rehabilitation prove unsuccessful or if pupillary block recurs. Lensectomy may be performed by using an intracapsular technique with anterior vitrectomy as needed, or the lens may be removed via a pars plana lensectomy-vitrectomy approach.
Lens Swelling
A cataract may develop as a result of trauma. Occasionally a cataractous lens becomes intumescent. Such swollen lenses can subsequently cause angle-closure glaucoma as a result of pupillary block or direct angle compromise by mass effect.
A previous history of trauma and asymmetry of anterior chamber depth on clinical examination are vital in establishing a reason for this type of glaucoma.
Cataract surgery relieves the pupillary block and angle compromise and restores vision. Peripheral anterior synechiae may contribute to an elevated IOP as a result of chronic pupillary block, and each patient should be evaluated carefully for this. Iridogonioplasty or goniosynechialysis may be required. When any potential for vision is negligible, iridotomy or iridectomy may be performed without cataract extraction, although cataract removal is still the treatment of choice.
Phacolytic Glaucoma
Phacolytic glaucoma is seen in the setting of a hypermature cataract. An open-angle glaucoma occurs as a result of leakage of high molecular weight proteins through an intact lens capsule. For diagnosis and management, see Chapter 207
Lens Particle Glaucoma
Lens particle glaucoma is characterized by the presence of a frankly disrupted lens capsule with obvious fragments of lens material in the anterior chamber. For the clinical presentation, diagnosis, and management of this condition, see Chapter 207.
DELAYED CLOSURE OF A CYCLODIALYSIS CLEFT
The occurrence of a cyclodialysis cleft after trauma is associated with hypotony as a result of suppression of aqueous production and increased aqueous outflow via the uveoscleral pathway. Goldmann[54]postulated that a reduction in the normal flow of aqueous across the trabecular meshwork resulted in a reduced permeability of the meshwork to aqueous outflow. This is believed to account for the marked acute pressure elevation that can be seen to occur after closure of an existing cyclodialysis cleft.
Delayed closure of a cyclodialysis cleft can be a difficult diagnosis to make. The patient presents with an acutely elevated pressure, corneal edema, a formed anterior chamber, and a gonioscopically open angle. A previous history of trauma should raise the examiner's suspicion. When closure of a cleft is suspected, treatment with miotics and phenylephrine may be effective in reopening the cleft and in lowering the pressure. A repeat gonioscopy then often provides the diagnosis.
EPITHELIAL DOWNGROWTH
The downgrowth of epithelium into the eye may occur in the presence of a patent fistula from the external surface of the eye to its internal surface or after the implantation of epithelial cells within the eye. This is a rare occurrence that has a poor prognosis when it occurs. The common clinical settings include previous cataract surgery, filtration surgery, and penetrating trauma.
RETAINED INTRAOCULAR FOREIGN BODY
As a form of trauma and penetrating injury, a retained foreign body may be associated with several types of glaucoma. A flat anterior chamber combined with inflammation can result in secondary angle-closure glaucoma after the formation of extensive peripheral anterior synechiae. Prolonged leakage and fistulization at the site of penetration can produce an epithelial downgrowth situation, as discussed previously. Frank disruption of the lens capsule may result in lens particle glaucoma, phacomorphic glaucoma, or phacolytic glaucoma. A late manifestation of iron-containing foreign bodies is siderotic glaucoma with its associated heterochromia, mydriasis, and rustlike discoloration of the anterior subcapsular surface of the lens and the posterior corneal surface.
Patients may present immediately with a clear history and evidence of an intraocular foreign body, or they may appear months or years after the initial event in a more subtle fashion with unilateral cataract, chronic inflammation, glaucoma, or reduced retinal function. Ocular examination is directed at looking for evidence of penetration such as a discrete area of iris transillumination, a small lenticular capsular rupture, or a corneal or scleral wound.
An ocular examination with eyes dilated may allow direct visualization of a foreign body. Occasionally, a foreign body is located in the anterior chamber angle and is evident only on gonioscopy. Some patients may have signs of chalcosis or siderosis, as outlined previously.
Appropriate studies, including plain films, computed tomography scans, and ultrasonography are helpful in confirming the diagnosis.
RHEGMATOGENOUS RETINAL DETACHMENT
Rhegmatogenous retinal detachment is most commonly associated with ocular hypotension due to a decrease in aqueous production.[55] As many as 5-10% of patients with rhegmatogenous retinal detachment demonstrate ocular hypertension.[56] This may be the result of preexisting open-angle glaucoma or inflammation secondary to a long-standing detachment. However, there exists a small group of patients with no preexisting glaucoma who acquire secondary open-angle glaucoma that resolves when the retinal detachment is repaired. This was well described by Schwartz,[57] who collected 11 such cases. Interestingly, five of the 11 cases were associated with previous ocular trauma.
The original proposed mechanism was inflammation of the trabecular meshwork with a resultant decrease in outflow facility. Others[58] hypothesized that pigment was being released and obstructed the trabecular meshwork. Matsuo and associates[59] demonstrated photoreceptors in the aqueous humor by transmission electron microscopy in seven patients with this syndrome. They first proposed that the photoreceptors could be obstructing aqueous outflow.
Unilateral glaucoma in the presence of a rhegmatogenous retinal detachment is an unusual presentation and emphasizes the importance of careful funduscopic examination in all cases of unilateral glaucoma.
Treatment consists of repairing the retinal detachment. This promptly and permanently returns the IOP to normal provided that there are no associated ocular abnormalities, such as angle recession, that could contribute to chronic elevation of IOP.
REFERENCES
1. Girkin CA, McGwin Jr G, Morris R, Kuhn F: Glaucoma following penetrating ocular trauma: a cohort study of the United States Eye Injury Registry. Am J Ophthalmol 2005; 139(1):100-105.
2. Girkin CA, McGwin G Jr, Long C, et al: Glaucoma after ocular contusion: a cohort study of the United States Eye Injury Registry. J Glaucoma 2005; 14:470-473.
3. Herschler J: Trabecular damage due to blunt anterior segment injury and its relationship to traumatic glaucoma. Trans Am Acad Ophthalmol Otolaryngol 1977; 83:239-248.
4. Cho J, Jun BK, Lee YJ, Uhm KB: Factors associated with the poor final visual outcome after traumatic hyphema. Korean J Ophthalmol 1998; 12:122-129.
5. Read J, Goldberg MF: Comparison of medical treatment for traumatic hyphema. Trans Am Acad Ophthalmol Otolaryngol 1974; 14(4):57-97.
6. Goldberg MF: Sickled erythrocytes, hyphema, and secondary glaucoma: I. The diagnosis and treatment of sickled erythrocytes in human hyphemas. Trans Am Ophthalmol Soc 1979; 10:17-31.
7. Crouch ER, Frenkel M: Aminocaproic acid in the treatment of traumatic hyphema. Am J Ophthalmol 1976; 81(3):355-360.
8. Karaman K, Culic S, Erceg I, et al: Treatment of post-traumatic trabecular mashwork thrombosis and secondary glaucoma with intracameral tissue plasminogen activator in previously unrecognized sickle cell anemia. Coll Antropol 2005; 29(Suppl 1):123-126.
9. Edwards WC, Layden WE: Traumatic hyphema: A report of 184 consecutive cases. Am J Ophthalmol 1973; 75(1):110-116.
10. McGetrick JJ, Jampol LM, Goldberg MF, et al: Aminocaproic acid decreases secondary hemorrhage after traumatic hyphema. Arch Ophthalmol 1983; 101(7):1031-1033.
11. Yasuna E: Management of traumatic hyphema. Arch Ophthalmol 1974; 91(3):190-191.
12. Rynne MV, Romano PE: Systemic corticosteroids in the treatment of traumatic hyphema. J Pediatr Ophthalmol Strabismus 1980; 17(3):141-143.
13. Spoor TC, Hammer M, Belloso H: Traumatic hyphema: Failure of steroids to alter its course: A double-blind prospective study. Arch Ophthalmol 1980; 98(1):116-119.
14. Dieste MC, Hersh PS, Kylstra JA, et al: Intraocular pressure increase associated with epsilon-aminocaproic acid therapy for traumatic hyphema. Am J Ophthalmol 1988; 106(4):383-390.
15. Belcher CD, Brown SVL, Simmons RJ: Anterior chamber washout for traumatic hyphema. Ophthalmic Surg 1985; 16(3):475-479.
16. Sears ML: Surgical management of black ball hyphema. Trans Acad Ophthalmol Otolaryngol 1970; 74(4):820-825.
17. Hill K: Cryoextraction of total hyphema. Arch Ophthalmol 1968; 80(3):368-370.
18. McCuen BW, Fung WE: The role of vitrectomy instrumentation in the treatment of severe traumatic hyphema. Am J Ophthalmol 1979; 88(5):930-934.
19. Kelman CD, Brooks DL: Ultrasonic emulsification and aspiration of traumatic hyphema: A preliminary report. Am J Ophthalmol 1971; 71(6):1289-1291.
20. Parrish RK, Bernardino V: Iridectomy in the surgical management of eight ball hyphema. Arch Ophthalmol 1982; 100:435.
21. Weiss JS, Parrish RK, Anderson DR: Surgical therapy of traumatic hyphema. Ophthalmic Surg 1983; 14(4):343-345.
22. Gilbert HD, Smith RE: Traumatic hyphema: Treatment of secondary hemorrhage with cyclodiathermy. Ophthalmic Surg 1975; 7(3):31-35.
23. Pesin SR, Katz LJ, Augsburger JJ, et al: Acute angle closure glaucoma from spontaneous massive hemorrhagic retinal or choroidal detachment. Ophthalmology 1990; 97(1):76-84.
24. Hughes WF: Alkali burns of the eye. 1: Review of the literature and summary of present knowledge. Arch Ophthalmol 1946; 35:423.
25. Grant WM: Ophthalmic pharmacology and toxicology, Springfield, IL: Charles C Thomas; 1965:299-316.(2)
26. Highman VN: Early rise in intraocular pressure after ammonia burns. BMJ 1969; 1(5640):359-360.
27. Chiang TS, Moorman LR, Thomas RP: Ocular hypertensive response following acid and alkali burns in rabbits. Invest Ophthalmol Vis Sci 1971; 10(4):270-273.
28. Paterson CA, Pfister RR: Intraocular pressure changes after alkali burns. Arch Ophthalmol 1974; 91(3):211-218.
29. Collins ET: On the pathological examination of three eyes lost from concussion. Trans Ophthalmol Soc UK 1892; 12:180.
30. D'Ombrain A: Traumatic monocular chronic glaucoma. Trans Ophthalmol Soc Aust 1986; 5:116.
31. Wolff SM, Zimmerman LE: Chronic secondary glaucoma: Associated with retrodisplacement of iris root and deepening of the anterior chamber angle secondary to contusion. Am J Ophthalmol 1962; 54:547-563.
32. Blanton FM: Anterior chamber angle recession and secondary glaucoma: A study of the aftereffects of traumatic hyphemas. Arch Ophthalmol 1964; 72:39-43.
33. Tonjum AM: Intraocular pressure and facility of outflow late after ocular contusion. Acta Ophthalmol 1968; 46(5):886-908.
34. Monney D: Angle recession and secondary glaucoma. Br J Ophthalmol 1973; 57(8):608-612.
35. Canavan YM, Archer DB: Anterior segment consequences of blunt ocular injury. Br J Ophthalmol 1982; 66(9):549-565.
36. Kaufman JH, Tolpin DW: Glaucoma after traumatic angle recession: A ten year prospective study. Am J Ophthalmol 1974; 78(4):648-654.
37. Alper MG: Contusion angle deformity and glaucoma: gonioscopic observations and clinical course. Arch Ophthalmol 1963; 69:455-467.
38. Salmon JF, Mermoud A, Ivey A, et al: The detection of post-traumatic angle recession by gonioscopy in a population-based glaucoma survey. Ophthalmology 1994; 101(11):1844-1850.
39. Miles DR, Boniuk M: Pathogenesis of unilateral glaucoma: A review of 100 cases. Am J Ophthalmol 1962; 62(3):493-499.
40. Salmon JF, Mermoud A, Ivey A, et al: The detection of post-traumatic angle recession by gonioscopy in a population-based glaucoma survey. Ophthalmology 1994; 101:1844-1850.
41. Tonjum AM: Gonioscopy in traumatic hyphema. Acta Ophthalmol 1968; 44(4):650-664.
42. Tesluk GC, Spaeth GL: The occurrence of primary open angle glaucoma in the fellow eye of patients with unilateral angle cleavage glaucoma. Ophthalmology 1958; 92(7):904-911.
43. Robin AL, Pollack IP: Argon laser trabeculoplasty in secondary forms of open angle glaucoma. Arch Ophthalmol 1983; 97(3):292-295.
44. Thomas JV, Simmons RJ, Belcher CD: Argon laser trabeculoplasty in the pre-surgical glaucoma patient. Ophthalmology 1982; 89(3):187-197.
45. Fukuchi T, Iwata K, Schoichi S, et al: Nd:YAG laser trabeculopuncture (YLT) for glaucoma with traumatic angle recession. Graefes Arch Clin Exp Ophthalmol 1993; 231(10):571-576.
46. Mermoud A, Salmon JF, Straker C, Murray AD: Post-traumatic angle recession glaucoma: a risk factor for bleb failure after trabeculectomy. Br J Ophthalmol 1993; 77(10):631-634.
47. Mermoud A, Salmon JF, Barron A, et al: Surgical management of post-traumatic angle recession glaucoma. Ophthalmology 1993; 100(5):634-642.
48. Manners T, Salmon JF, Barron A, et al: Trabeculectomy with mitomycin C in the treatment of post-traumatic angle recession glaucoma. Br J Ophthalmol 2001; 85(2):159-163.
49. Fuller JR, Bevin TH, Molteno AC: Long-term follow-up of traumatic glaucoma treated with Molteno implants. Ophthalmology 2001; 108(10):1796-1800.
50. Campbell DG, Simmons RJ, Grant WM: Ghost cells as a cause of glaucoma. Am J Ophthalmol 1976; 81(4):441-450.
51. Campbell DG: Ghost cell glaucoma following trauma. Ophthalmology 1981; 88(11):1151-1158.
52. Epstein DL: Diagnosis and management of lens-induced glaucoma. Ophthalmology 1982; 89(3):227-230.
53. Peng SX, Zhou WB: Traumatic lens dislocation-related glaucoma. Zhonghua Yan Ke Za Zhi 1993; 29(6):332-335.
54. Goldmann H: Klinische Studien zum Glaucomproblem. Clinical studies on the glaucoma problem. I. The role of Schlemm's canal after arrangement of new outflow channels. Ophthalmologica 1953; 125(1):16-21.
55. Dobbie JG: A study of the intraocular fluid dynamics in retinal detachment. Arch Ophthalmol 1963; 69:159-164.
56. Linner E: Intraocular pressure in retinal detachment. Acta Ophthalmol 1966; 84:101.
57. Schwartz A: Chronic open angle glaucoma secondary to rhegmatogenous retinal detachment. Am J Ophthalmol 1973; 75(2):205-211.
58. Baruch E, Bracha R, Godel V, et al: Glaucoma due to rhegmatogenous retinal detachment; Schwartz's syndrome. Glaucoma 1981; 3:229.
59. Matsuo N, Takabatake M, Ueno H, et al: Photoreceptor outer segments in the aqueous humor in rhegmatogenous retinal detachment. Am J Ophthalmol 1986; 101(6):673-679.