George T. Rab, MD
The scope of pediatric orthopedics ranges from congenital anomalies to injuries in the adolescent. The pathophysiologic manifestations of many of these disorders differ from analogous adult problems because of the added dimension of growth. The physician’s relationship with the pediatric patient generally occurs in the context of a protective family environment, in contrast to the more independent relationship the physician may form with an adult. The natural tendency for children to be active and the remarkable regenerative processes of the immature skeleton frequently make formal rehabilitation unnecessary following surgery or serious injury.
![]() Guidelines for Pediatric Orthopedics
Guidelines for Pediatric Orthopedics
The following rules may be helpful when applying general orthopedic principles to the child:
1. A growing bone normally tends to remodel itself toward the adult configuration. This process occurs faster in younger children and in deformities near the ends of bone. Remodeling is faster when deformity is in the plane of motion of the nearest joint.
2. Skeletal deformities worsen as abnormal growth continues (eg, following permanent damage to the growth plate), especially near rapidly growing areas such as the knee. This characteristic is exaggerated in younger children.
3. Children tolerate long-term immobilization better than adults and tend to recover soft-tissue mobility spontaneously following most injuries.
4. Fracture healing is usually more rapid and predictable in the actively growing skeleton than in the adult skeleton.
5. Joint surfaces in children are generally more tolerant of irregularity than those of the adult. Although degenerative arthritic changes may follow childhood injury, there is often an asymptomatic interval of many decades before the process becomes clinically evident.
6. Many so-called deformities, such as metatarsus adductus, internal tibial torsion, genu valgum (knock-knee), and bowed legs, are actually physiologic variations that correct spontaneously with growth. For example, physiologic bowing is common and benign. It is typically symmetric, involves both the femur and tibia, and is most prominent in toddlers. It usually resolves by 2 years of age, but there is great variability. By age 36 months, almost all children will correct spontaneously. The clinician must distinguish between conditions that need no treatment and those requiring early intervention.
GROWTH DISORDERS
General skeletal growth is discussed in detail in Chapter 1.
1. Limb-Length Inequality
![]() Essentials of Diagnosis
Essentials of Diagnosis
• Commonly asymptomatic difference in limb length must be detected to plan for appropriate treatment.
• Congenital anomalies may lead to significant inequality.
• Proper evaluation and planning allow optimal treatment during growth.
![]() General Considerations
General Considerations
Limb-length inequality may reflect either a congenital deficiency or any of a wide variety of acquired conditions (Table 10–1). Posttraumatic physeal arrest occurs most commonly after injury in the distal medial tibia. Injuries of the distal femoral and distal ulnar physis have a high incidence of growth arrest as well. Upper extremities of unequal length are usually only of cosmetic interest and can easily be compensated for by modifying clothing. In the lower extremities, however, length discrepancies may be severe enough—greater than 1 inch (2.5 cm)—to limit function and require treatment. Lesser discrepancies can be managed with a shoe lift.
Table 10–1. Causes of limb-length inequality.

![]() Clinical Findings
Clinical Findings
A. Symptoms and Signs
Most limb inequality in children is asymptomatic, even when severe. Marked deformity may cause a painless limp.
Clinical limb measurement is usually possible by checking for a level pelvis with the child standing on calibrated blocks under the short leg. Severe inequality may require alternate exam techniques.
B. Imaging Studies
All children should have an x-ray of the entire limb at initial visit to screen for anomalies and deformities. Scanograms (special leg-length films) are the standard for accurate measurement of inequality, but they can be inaccurate if the child moves. An option in older children is an anteroposterior (AP) pelvis with the child standing on clinically appropriate blocks under the short leg. Skeletal maturity is measured from wrist bone age films.
C. Calculation of Limb Length at Maturity
Clinical management of limb-length inequality in pediatric patients should include calculation of projected lengths at maturity. Several mathematical methods, based on skeletal age, gender, and normal growth rates, are available. The following general rule can be used to estimate the extent of future growth: The average growth rates of the distal femur and proximal tibia are 10–12 mm/year and 5–6 mm/year, respectively, with growth continuing until bone age 14 in females and 16 in males.
![]() Treatment
Treatment
A. Shoe Lift
A lift is rarely required in children, but adolescents may desire a lift. It generally may be ½ inch (1.27 cm) less than the measured difference in limb length.
B. Epiphysiodesis
The simplest surgical procedure to treat pediatric bone-length discrepancies is epiphysiodesis (surgical closure of the growth plate). In the longer limb, it involves curetting or drilling the physis or inserting small bone grafts across the medial and lateral edges of the plate. Epiphysiodesis is usually performed at the distal femoral physis, proximal tibial physis, or both, because they are rapidly growing and easily accessible surgically. The remaining open physes in the limb allow for continued growth but at a slower rate. The exact timing of epiphysiodesis is crucial to attaining equal limb lengths at skeletal maturity. Timing is calculated by the same method used to predict ultimate adult leg length. The effectiveness of epiphysiodesis requires that bone still be growing and that accurate data be collected on this growth for several years (ie, scanograms for leg-length measurement, skeletal age).
C. Femoral Shortening
If a child reaches the age when bone growth is insufficient to make epiphysiodesis practical, the long leg may be shortened at skeletal maturity by femoral shortening. This may be performed as an open procedure by removing a segment of femur and fixing the bone with a plate and screws. It may also be done as a closed procedure, using an intramedullary femoral rod introduced through a buttock incision for fixation. A cylindrical segment of femur is cut out of the bone using intramedullary saws, and the bone is pushed aside to allow the femur to shorten over the rod. The excised bone segment eventually resorbs.
D. Other Techniques
Leg-length inequalities projected to be 6 cm or more generally do not respond well to the previously described treatments, which in these cases may lead to unacceptably short stature or limb segments. Although some discrepancies are so severe that amputation of the foot and prosthetic fitting are required, techniques of bone lengthening are successful in treating these children (see Chapter 1).
Birch JG, Samchukov ML: Use of the Ilizarov method to correct lower limb deformities in children and adolescents. J Am Acad Orthop Surg 2004;12:144. [PMID: 15161167]
Inan M, Chan G, Littleton AG, Kubiak P, Bowen JR: Efficacy and safety of percutaneous epiphysiodesis. J Pediatr Orthop 2008;28:648. [PMID: 18724201]
Khakharia S, Bigman D, Fragomen AT, Pavlov H, Rozbruch SR: Comparison of PACS and hard-copy 51-inch radiographs for measuring leg length and deformity. Clin Orthop Relat Res 2011;469:244. [PMID: 20625949]
Paley D, Bhave A, Herzenberg JE, Bowen JR: Multiplier method for predicting limb-length discrepancy. J Bone Joint Surg Am 2000;82-A:1432. [PMID: 11057472]
Surdam JW, Morris CD, DeWeese JD, et al: Leg length inequality and epiphysiodesis: review of 96 cases. J Pediatr Orthop 2003; 23:381. [PMID: 12724605]
2. Dwarfism and Other Disorders of Growth
Orthopedic disorders (achondroplasia, multiple epiphyseal dysplasia) or other syndromes (Down syndrome, Marfan syndrome) often accompany dwarfism. The classification of skeletal syndromes and dysplasias is undergoing rapid change as knowledge is gained using molecular, biologic, and genetic techniques. In general, autosomal recessive genes code for enzymatic and biochemical defects and autosomal dominant gene defects cause structural deformities. An example of the latter is achondroplasia that results from mutation of fibroblast growth factor receptor 3 (FGFR3), a structural protein that results in the quantitative decrease in cartilage formation. The gene defects are inherited from one of the parents or are sporadic mutations. A detailed review of skeletal syndromes and dysplasias is outside the scope of this text; Table 10–2 lists some of these conditions and the major orthopedic problems associated with them.
Table 10–2. Orthopedic involvement in selected syndromes and dwarfing conditions.

INFECTIOUS PROCESSES
1. Hematogenous Osteomyelitis
![]() Essentials of Diagnosis
Essentials of Diagnosis
• Limp, bone pain, fever, leukocytosis, and elevation of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) characterize osteomyelitis.
• Methicillin-resistant Staphylococcus aureus (MRSA) osteomyelitis is increasingly common and may include serious life- and limb-threatening complications.
![]() General Considerations
General Considerations
Osteomyelitis, an infection of bone tissue, usually occurs in the marrow cavity but sometimes affects the cortex as well. There is a predilection for metaphyseal involvement of long bones.
![]() Pathogenesis
Pathogenesis
In children, osteomyelitis is most commonly caused by hematogenous bacterial spread, frequently following an upper respiratory infection or partially treated distant infection. Direct inoculation of bacteria into an open fracture or penetrating wound can also lead to infection and may resemble other serious bacterial infections in children (Table 10–3).
Table 10–3. Common pathogens in pediatric bone and joint infections.
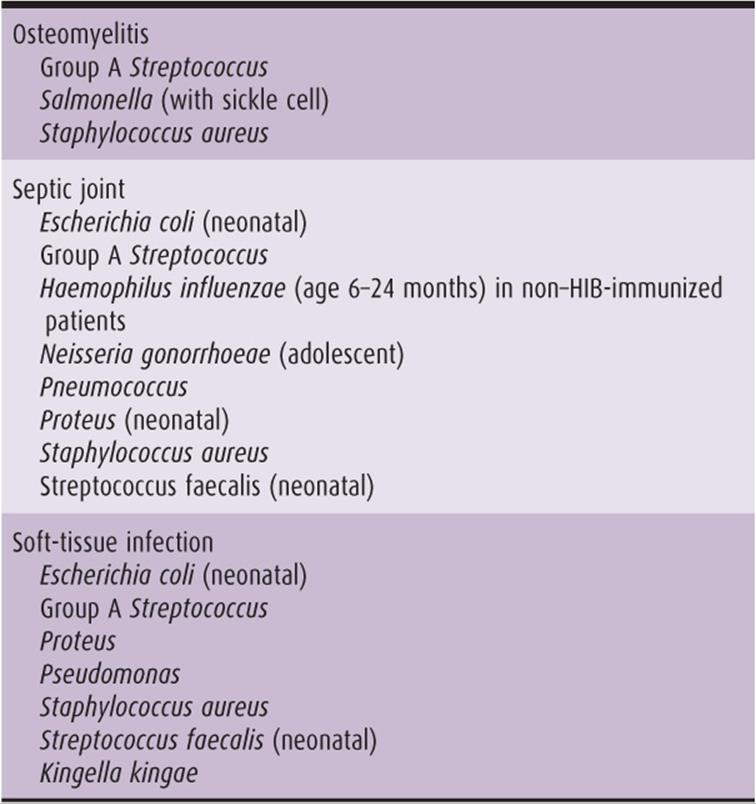
Acute bacterial hematogenous osteomyelitis usually occurs in the metaphysis following sludging of bacteria-laden blood in the venous sinusoids. The majority of cases are caused by Staphylococcus aureus. As the infection progresses, edema fluid and infected purulent tissue invade the porous cortex and elevate the periosteum, which is highly resistant to infection because of its extreme vascularity. The pressure of the pus beneath the richly innervated periosteum causes localized pain. Eventually, if the infection is untreated, the periosteum itself ruptures, and infected tissue spills into the surrounding soft tissue or ruptures the skin (Figure 10–1).

![]() Figure 10–1. Hematogenous osteomyelitis in children. Cellulitic phase (A) can exude through the cortex, raising periosteum (B). Late rupture into soft tissues (C) is rare, unless infection is untreated.
Figure 10–1. Hematogenous osteomyelitis in children. Cellulitic phase (A) can exude through the cortex, raising periosteum (B). Late rupture into soft tissues (C) is rare, unless infection is untreated.
The accumulated purulence in the marrow cavity and under the periosteum creates an efficient avascular culture medium in the cortex between them. This dead cortex is called a sequestrum, and, if it is large, surgical removal may be required to control the infection.
The elevated periosteum responds to infection by producing a shell of periosteal new bone called involucrum, which provides some stability to the infected bone and rarely becomes infected itself.
![]() Clinical Findings
Clinical Findings
Pain and tenderness at the infection site are universal signs, limping is common, and frequently the child is irritable. Fever and leukocytosis are common but not universal, and the ESR is almost always elevated, usually to 50 mm/hour or more. CRP is elevated. Children with MRSA infections may present with severe systemic illness and multisystem involvement. Although the diagnosis is usually clear, osteomyelitis should be suspected if a child has bone pain in the absence of other systemic signs but has recently received antibiotic treatment for other conditions.
![]() Imaging Studies
Imaging Studies
Clinical examination and routine x-rays are usually sufficient to make the diagnosis; occasionally, bone scans or magnetic resonance imaging (MRI) may be required to help localize lesions.
![]() Laboratory Findings
Laboratory Findings
Elevation of ESR (>50 mm/hour) and CRP are typical of osteomyelitis.
![]() Treatment
Treatment
A. Early Treatment
Treatment depends on the duration of symptoms, radiographic findings, and suspected or cultured organism. If the infection is detected early, no visible radiograph changes usually are apparent except for soft-tissue swelling. In that case, intravenous and, later, oral antibiotics may resolve the infection. Aspiration of the metaphysis should be done for culture before beginning antibiotic therapy. Up to 30–40% of cultures may be negative despite other clear evidence of bacterial infection; in that case, empirical treatment (usually with antistaphylococcal antibiotics) is appropriate.
B. Treatment for Advanced Infection or MRSA
In advanced cases, lytic defects or osteoporosis may be present, and periosteal reaction may be visible on radiograph; such cases require open drainage and debridement of the infected metaphysis. Antibiotic treatment must be continued until there is no evidence of residual infection because bacteria can survive in bone tissue that is not well perfused with antibiotic. In such cases, a 3-month prolonged regimen of oral antibiotics minimizes the possibility of chronic osteomyelitis.
MRSA infections are more likely to require surgical drainage for metaphyseal or subperiosteal abscesses, and multiple operative debridements may be necessary.
2. Septic Joint
![]() Essentials of Diagnosis
Essentials of Diagnosis
• Septic joints cause pain, limp, and refusal to move a joint.
• Aspiration of joint for culture, surgical drainage, and antibiotics are generally successful.
• Septic hip is a unique surgical emergency requiring urgent surgery.
![]() General Considerations
General Considerations
Septic arthritis in children, like osteomyelitis, usually is hematogenous in origin. The bacterial complications are similar to those seen in bone infections (see Table 10–3). Septic joints frequently follow upper respiratory infections; they may be delayed in onset by a week or more and may present in an attenuated form when a previous infection was partially treated.
![]() Clinical Findings
Clinical Findings
The classic septic joint in a child presents a dramatic picture: The joint is splinted by muscle spasm, and motion of even a few degrees causes extreme pain. There may be effusion, but findings may be less striking if antibiotics were used in the recent past. During this acute inflammatory phase, children are more comfortable if the involved joint is immobilized.
![]() Laboratory Findings
Laboratory Findings
Although white blood cell counts and the ESR are usually elevated, the definitive diagnosis of septic joint requires aspiration and synovial fluid analysis. Sterile aspiration does not harm the joint and should be done immediately when the diagnosis is suspected. Aspiration of deep joints such as the hip may require radiographic control.
Synovial white blood cell counts range from 50,000/μL (in nonpyogenic infections such as Neisseria gonorrhoeae) to over 250,000/μL (S. aureus). This white cell response, with the concomitant high level of lysosomal enzyme release, is most destructive of articular cartilage in septic joints. Although synovial fluid cultures give definitive guidance for therapy, antibiotic treatment can initially be based on results of Gram staining. In addition, immunochemical tests may offer rapid identification of certain pathogens.
![]() Imaging Studies
Imaging Studies
Most septic joints have normal radiographic findings or nonspecific signs of effusion or local tissue swelling. Late radiographic findings include subluxation, narrowing of joint space, and subchondral bone irregularity. MRI will demonstrate effusion or concurrent osteomyelitis or pyomyositis if present (see below).
![]() Differential Diagnosis
Differential Diagnosis
Like osteomyelitis, septic joint may be mimicked by septic pyomyositis (almost always MRSA), with involvement of periarticular tissues with or without actual joint involvement.
![]() Treatment
Treatment
Treatment always includes drainage of the joint. In easily accessible joints, such as the finger or knee, certain low-grade infections may respond well to repeated aspirations. In most cases, however, surgical drainage by arthrotomy or arthroscopy is preferable.
Antibiotics easily cross the synovial membrane and are continued until the joint inflammation is resolved, usually for at least 3 weeks. Intravenous administration is used initially but may often be followed by oral medication once the temperature, ESR, and leukocyte count return to normal.
Hensinger RN: Impending danger: community-acquired methicillin-resistant Staphylococcus aureus. J Pediatr Orthop 2006;26:703. [PMID: 17065929]
Jagodzinski NA, Kanwar R, Graham K, Bache CE: Prospective evaluation of a shortened regimen of treatment for acute osteomyelitis and septic arthritis in children. J Pediatr Orthop 2009;29:518. [PMID: 19568027]
Kaplan SL: Acute hematogenous osteomyelitis in children: differences in clinical manifestations and management. Pediatr Infect Dis J 2010;29:1128. [PMID: 21099652]
3. Septic Hip
Septic hip is one of the true surgical emergencies in pediatric orthopedics. It must be differentiated from transient synovitis of the hip, which is a benign condition (see the section on transient synovitis of the hip).
![]() Pathogenesis
Pathogenesis
Because of the unique structure and blood supply of proximal femur (Figure 10–2), purulence within the joint capsule can cause thrombosis of epiphyseal vessels and necrosis of the proximal femoral epiphysis. Neglected septic hips may subluxate or dislocate because of effusion and laxity caused by hyperemia. For these reasons, septic hip (or osteomyelitis of the proximal femur) always requires surgical drainage. Delay of even 4–6 hours may compromise the vascularity of the hip. An anterior approach is preferred to reduce the risk of vascular injury and subluxation.

![]() Figure 10–2. The blood supply of the proximal femur is unusual because the capsule interferes with the direct routing of blood vessels. The epiphyseal vessels emerge distal to the capsule and course up the surface of the femoral neck, rendering them susceptible to injury, thrombosis, or blockage by increased intraarticular pressure.
Figure 10–2. The blood supply of the proximal femur is unusual because the capsule interferes with the direct routing of blood vessels. The epiphyseal vessels emerge distal to the capsule and course up the surface of the femoral neck, rendering them susceptible to injury, thrombosis, or blockage by increased intraarticular pressure.
Septic hip in a growing child is also a special orthopedic case because the femoral neck (which is intraarticular) is actually the anatomic metaphysis of the proximal femur. It is thus susceptible to hematogenous osteomyelitis, which may rupture into the hip joint and cause sepsis.
![]() Differential Diagnosis
Differential Diagnosis
A common clinical problem is the differentiation between septic hip and transient synovitis of the hip. Juvenile arthritis may occasionally be included in the differential. Table 10–4 highlights differences in the conditions.
Table 10–4. Clinical differential diagnosis of inflammatory hip conditions.

Sultan J, Hughes PJ: Septic arthritis or transient synovitis of the hip in children: the value of clinical prediction algorithms. J Bone Joint Surg Br 2010;92:1289. [PMID: 20798450]
4. Puncture Wounds of the Foot
Sneakers and tennis shoes offer little protection from nail punctures of the plantar surface of the foot. The penetrating nail may carry Pseudomonas bacteria (which contaminate the soles of tennis shoes) into the plantar fascia, although one series found S. aureus or group A Streptococcus to be most common.
The symptoms of infection include redness, swelling, and pain that persist longer than 1 week. Surgical incision and drainage of the abscess and foreign body excision, when present (approximately one sixth of cases), are usually curative. Interestingly, prophylactic use of antibiotics does not seem to lessen the chance of developing late abscess. Late presentation is a marker for deep infection.
Eidelman M, Bialik V, Miller Y, Kassis I: Plantar puncture wounds in children: analysis of 80 hospitalized patients and late sequelae. Isr Med Assoc J 2003;5:268. [PMID: 14509132]
Schwab RA, Powers RD: Conservative therapy of plantar puncture wounds. J Emerg Med 1995;13:291. [PMID: 7673617]
5. Skeletal Tuberculosis
As in the adult, Mycobacteria organisms may invade the pediatric skeleton by hematogenous spread to bone or synovium while the initial pulmonary infection goes undetected. The most common sites of invasion are the hip and spine. Tuberculosis (TB) should be considered, and skin tests performed, in children suffering from chronic atypical musculoskeletal infections, particularly if the child is immunosuppressed.
![]() Clinical Findings
Clinical Findings
Hip involvement with TB is characterized by a chronic limp associated with a flexion contracture. In addition, muscle atrophy of the thigh may be striking. Radiographic examination discloses osteoporosis, joint narrowing, and irregular erosions. Spine involvement typically has an indolent presentation. Unlike pyogenic infections of the spine, the disk space is usually preserved. Most commonly, the thoracic and lumbar spine are affected. It may include paraspinal abscess (best visualized by computed tomography [CT] scan or MRI), and if untreated, it can lead to vertebral destruction or kyphosis, which may be severe and lead to paralysis.
![]() Laboratory Findings
Laboratory Findings
Laboratory studies may be nonspecific.
![]() Treatment
Treatment
Treatment of skeletal TB consists of combination chemotherapy, with surgical debridement in resistant cases. Occasionally, surgical fusion of a joint may be required. Delayed presentation of spinal TB infection may result in neurologic compromise and a kyphotic deformity. Spinal surgery is occasionally indicated for deformity correction or failure of medical treatment.
Hosalkar HS, Agrawal N, Reddy S, et al: Skeletal tuberculosis in children in the Western world: 18 new cases with a review of the literature. J Child Orthop 2009;3:319. [PMID: 19543761]
6. Diskitis in Children
Diskitis is a low-grade inflammatory process involving the intervertebral disk, usually in the lumbar spine. It affects children at any age, although it is most frequent between 2 and 6 years of age. The disorder is caused by hematogenous bacterial seeding, with the most common cultures growing S. aureus from the disk aspirate. The classic presentation in a toddler is refusal to walk; pain is not a prominent symptom in this age group. Older children (up to early teen years) may have either back or abdominal pain.
![]() Clinical Findings
Clinical Findings
Small children may have limitation of passive hyperextension of the spine (in the prone position) with no other findings. Older children have splinting of the paraspinous muscles and pain with percussion.
![]() Laboratory Findings
Laboratory Findings
The ESR may be normal or elevated; patients with an elevated ESR are more likely to have bacterial growth if cultures are done. Aspirate cultures may be negative in up to 40% of patients.
![]() Imaging Studies
Imaging Studies
Radiographs at first are normal but eventually demonstrate disk space narrowing with sclerosis of adjoining endplates, best visualized on spot lateral views. Bone scan is positive in children with negative radiographs.
![]() Treatment
Treatment
Management depends on the severity of clinical findings because a large number of diskitis patients have self-limited disease and improve spontaneously. Children with sepsis or elevated ESR may benefit from disk aspiration and culture. Less ill children are usually treated with empirical anti-staphylococcal oral antibiotics for 6 weeks. Pantaloon spica cast may occasionally be required for symptom relief. Long-term outcome is universally favorable, although occasional spontaneous fusion of the disk space occurs.
Early SD, Kay RM, Tolo VT: Childhood diskitis. J Am Acad Orthop Surg 2003;11:413. [PMID: 14686826]
Hamdy RC, Lawton L, Carey T, et al: Subacute hematogenous osteomyelitis: are biopsy and surgery always necessary? J Pediatr Orthop 1996;16:220. [PMID: 8742289]
Scott RJ, Christofersen MR, Robertson WW Jr, et al: Acute osteomyelitis in children: a review of 116 cases. J Pediatr Orthop 1990; 5:649. [PMID: 2203820]
METABOLIC DISORDERS
![]() Essentials of Diagnosis
Essentials of Diagnosis
• There is growth abnormality and weakening or bowing of long bones in children.
• There is widening, bowing, and cupping of the physes.
• Serum calcium, phosphorus, alkaline phosphate, blood urea nitrogen, and endocrine studies usually confirm the diagnosis.
1. Rickets and Rickets-Like Conditions
Nutritional rickets is a dietary deficiency of vitamin D that interferes with skeletal ossification. Although vitamin supplementation of food and milk has virtually eliminated the dietary form of rickets, there is still an increased frequency of nutritional rickets in the United States in children with dark skin pigmentation who are breast fed past 6 months of age without vitamin D supplementation. Nutritional rickets is rare in light-skinned children or those who are formula fed. Numerous rickets-like metabolic conditions persist with orthopedic consequences, however.
![]() Renal Osteodystrophy
Renal Osteodystrophy
Renal osteodystrophy, a disorder of calcium, phosphorus, vitamin D, and parathyroid function in children with chronic renal disease, has potentially serious skeletal manifestations. In transplantation patients, the condition can be aggravated by chronic illness and antimetabolite or steroid usage.
Osteoporosis, leading to compression fractures of the spine, is a common complication. Delayed healing of fractures is also common. Inadequate metaphyseal ossification during skeletal growth results in wide, irregular cartilaginous growth plates, which tend to slip slowly, sometimes producing grotesque hip, knee, and ankle deformities. Such deformities are usually best treated only after transplantation or other improvement in renal status. Occasionally, severe functional disabilities may require osteotomy to correct deformity before renal transplantation. Healing may be delayed, however, and the condition may recur.
![]() Hypophosphatemic Rickets
Hypophosphatemic Rickets
Hypophosphatemic rickets (vitamin D–resistant rickets) is a dominant X-linked condition in which vitamin D production and metabolism are normal but renal tubular loss of phosphate interferes with skeletal ossification. The major manifestations are a mild-to-moderate decrease in stature and bowing of the lower extremities. The medical history usually discloses a parent or sibling with short stature and bowlegs.
A. Laboratory Findings
Serum phosphorus is reduced, and serum calcium is normal. This is because the disorder is caused by phosphorus excretion in the urine (detectible in 24-hour urine sample). Vitamin D levels are normal.
B. Imaging Studies
Characteristic widening of growth plates, funnel-like beaking of the metaphyses, and curvature of the femoral and tibial shafts, which are normally straight (Figure 10–3), are typical.

![]() Figure 10–3. Hypophosphatemic rickets. Radiographs demonstrate bowing of long bones and flared, irregular physes (see text).
Figure 10–3. Hypophosphatemic rickets. Radiographs demonstrate bowing of long bones and flared, irregular physes (see text).
C. Treatment
Medical treatment with megadoses of vitamin D and phosphorus supplementation may not be curative. Functionally disabling deformities can be corrected by growth plate manipulation using hemiepiphyseodesis in younger children, or by multiple-level osteotomies, which usually require bilateral surgery. Because postosteotomy healing is delayed and recurrence of deformity is common during growth, such surgery should be postponed until adolescence, if possible.
Kocaoglu M, Bilen FE, Sen C, Eralp L, Balci HI: Combined technique for the correction of lower-limb deformities resulting from metabolic bone disease. J Bone Joint Surg Br 2011;93:52. [PMID: 21196543]
Novais E, Stevens PM: Hypophosphatemic rickets: the role of hemiepiphysiodesis. J Pediatr Orthop 2006;26:238. [PMID: 16557142]
Saland JM: Osseous complications of pediatric transplantation. Pediatr Transplant 2004;8:400. [PMID: 15265169]
Santos F, Carbajo-Pérez E, Rodríguez J, et al: Alterations of the growth plate in chronic renal failure. Pediatr Nephrol 2004; 20:330. [PMID: 15549411]
HIP DISORDERS
1. Transient Synovitis of the Hip
Transient synovitis of the hip is a benign, nontraumatic, self-limited disorder that mimics septic hip in clinical presentation. The physician confronting this condition must exclude septic hip, which is a surgical emergency.
Although the cause of transient synovitis is unclear, evidence suggests it is associated with immune responses to viral or bacterial antigens, mediated through the synovial membrane. Aseptic synovial fluid rapidly accumulates under pressure in the hip joint, and there may be severe pain from capsular distension. The fluid is resorbed within 3–7 days, with no long-term sequelae.
![]() Clinical Findings
Clinical Findings
As with septic hip, upper respiratory tract infections often precede transient synovitis by a few days to 2 weeks. The hip contains excess synovial fluid and is held in flexion, abduction, and external rotation because this is the joint’s position of maximum capacity. The joint may be sore and resistant to movement, but subluxation does not occur. Usually, the patient allows careful passive movement.
![]() Laboratory Findings
Laboratory Findings
Leukocytosis is absent, and ESR and CRP are not elevated. Synovial fluid does not show elevation of the white blood cell count, and bacterial cultures are negative.
![]() Imaging Studies
Imaging Studies
Radiographs reveal only capsular swelling, and effusion may be detected on ultrasound. Although experienced physicians frequently suspect transient synovitis based only on clinical examination, aspiration of the hip following confirmation of needle position by radiograph or ultrasound is the safest approach.
![]() Differential Diagnosis
Differential Diagnosis
The most important differential diagnosis is septic hip, which must be excluded. Also, early stages of Legg-CalvéPerthes disease (see section on Legg-Calvé-Perthes disease) may include a synovitic stage that, until the development of characteristic radiograph findings, is indistinguishable from transient synovitis. No evidence indicates that transient synovitis leads to Legg-Calvé-Perthes disease itself. Typically, the pain is less severe than in transient synovitis, the children are a bit older (older than 4–5 years), and there is no history of recent illness.
![]() Treatment
Treatment
Treatment of transient synovitis includes simple analgesics and splintage, usually by bed rest, until symptoms resolve.
Sultan J, Hughes PJ: Septic arthritis or transient synovitis of the hip in children: the value of clinical prediction algorithms. J Bone Joint Surg Br 2010;92:1289. [PMID: 20798450]
2. Developmental Dysplasia of the Hip
![]() Essentials of Diagnosis
Essentials of Diagnosis
• Certain infants (breech babies, babies with a family history, and females) are at higher risk for developmental dysplasia of the hip.
• Diagnosis is made clinically or by ultrasound.
• Early treatment gives the best results.
Developmental dysplasia of the hip is one of the most serious problems in pediatric orthopedics. The neonatal hip is a relatively unstable joint because the muscle is undeveloped, the soft cartilaginous surfaces are easily deformed, and the ligaments are lax. Exaggerated positioning in acute flexion and adduction in utero may occur, especially in breech presentation. This situation may cause excess stretching of the posterior hip capsule, which renders the joint unstable after delivery. Laxity may reflect family history or the presence of maternal relaxin hormone in the fetal circulatory system.
This relative instability may lead to asymptomatic subluxation (partial displacement) or dislocation (complete displacement) of the hip joint. Displacement of the femoral head in the infant is proximal (posterior and superior) because of the pull of the gluteal and hip flexor muscles. In the subluxated hip, asymmetric pressure causes progressive flattening of the posterior and superior acetabular rim and medial femoral head (dysplasia is the term to describe these structural deviations from normal).
In the completely dislocated hip, dysplasia also occurs because normal joint development requires concentric motion with normally mated joint surfaces. The shallow, deformed dysplastic joint surfaces predispose to further mechanical instability and the inexorable progression of the disorder.
Developmental dysplasia of the hip (DDH) occurs in approximately 1 in 1000 live births in whites, is less common in blacks, and may be more common in certain ethnic groups such as North American Indians. In all groups, this disorder is more likely if certain risk factors are present, such as positive family history, ligamentous laxity, breech presentation (and, by association, cesarean delivery), female gender, large fetal size, and first-born status. Dislocations may be bilateral but are more often unilateral and on the left side.
![]() Clinical Findings
Clinical Findings
Reversal of dysplasia and subsequent normal hip development depend on early detection of DDH. Early detection is made more challenging by lack of a definitive test or finding on examination. Moreover, because this disorder is painless, there are no symptoms in the infant. Detection of bilateral dislocations may be particularly difficult.
Radiographs are usually not useful in newborn infants because the femoral head is composed of radiolucent cartilage. Ultrasound examination is helpful, but false-positive results are common before 8–10 weeks of age. The test is expensive, and interpretation requires comprehensive training. Thus, the best test for this disorder is careful physical examination at birth, repeated at each well-infant check until the child is walking normally. A high index of suspicion is mandatory, especially if risk factors are present.
A. Tests for Dysplasia
Several examination maneuvers require a quiet, relaxed infant and commonly produce false-negative findings. Although it is imperative to detect subluxated or dislocated hips, it is also helpful to identify the very lax (unstable) but still located hip. This type of joint may either dislocate later or exhibit subtle dysplasia during growth that can cause premature osteoarthritis.
1. Asymmetric skin folds—A dislocated hip displaces proximally, causing the leg to be marginally shorter. This occasionally leads to the accordion phenomenon, with wrinkling of thigh skin folds. The most significant fold is between the genitals and gluteus maximus region. This test is not very reliable, frequently producing false-positive and false-negative results (Figure 10–4A).

![]() Figure 10–4. Clinical examination of developmental dislocation of the hip. In all pictures, the child’s left hip is the abnormal side. A: Asymmetric skin folds. B: Galeazzi test. C: Limitation of abduction. D, E, F: Ortolani and Barlow tests (see text).
Figure 10–4. Clinical examination of developmental dislocation of the hip. In all pictures, the child’s left hip is the abnormal side. A: Asymmetric skin folds. B: Galeazzi test. C: Limitation of abduction. D, E, F: Ortolani and Barlow tests (see text).
2. Galeazzi test—With the child lying on a flat surface, flex the hips and knees so the heels rest flat on the table, just distal to the buttock (Figure 10–4B). A dislocated hip is signaled by relative shortening of the thigh compared with the normal leg, as shown by the difference in knee height level. This test is almost always useless in children younger than 1 year and is negative if dislocation is bilateral.
3. Passive hip abduction—The flexed hips are gently abducted as far as possible (Figure 10–4C). If one or both hips are dislocated, the femoral head (the pivot point during abduction) is posterior, causing relative tightness of the adductor muscles. Asymmetric abduction or limited abduction (usually < 70 degrees from the midline) is a positive finding. When the hip is lax (dislocatable but not dislocated), the abduction test is normal despite the presence of subluxation or dislocation.
4. Barlow test—A provocative test that picks up an unstable but located hip, the Barlow test is unsuitable for a dislocated hip. The flexed calf and knee are gently grasped in the hand, with the thumb at the lesser trochanter and fingers at the greater trochanter (knee flexion relaxes the hamstrings). The hip is adducted slightly and gently pushed posteriorly and laterally with the palm (Figure 10–4D, F). Detection of so-called pistoning, or the sensation of the femoral head subluxating over the posterior rim of the acetabulum, is a positive finding.
5. Ortolani test—This test detects hips that are already dislocated. The flexed limb is grasped as in the Barlow test. The hip is abducted while the femur is gently lifted with the fingers at the greater trochanter (Figure 10–4D, E). In a positive test, there is a sensation of the hip reducing back into the acetabulum. Reduction is felt but not heard: The old concept of a so-called hip click is incorrect. The Ortolani test may be negative at 2–3 months of age, even when the hip is dislocated, because of the development of soft-tissue contracture.
B. Imaging Studies
In the infant, diagnosis is made by physical examination alone, and radiographs are generally unnecessary. Dysplasia, instability, and dislocation may appear on ultrasound studies, which can allow visualization of hip contour and stability before ossification is present. Sonography is a dynamic examination that requires an experienced interpreter, and there can be false positives prior to 6–10 weeks of age. Radiographs may be used at any age, but the absence of ossified structures renders them inaccurate in the newborn. After 4–6 months, when the ossific nucleus appears in the femoral head, radiographs are more helpful. Because much of the skeleton is cartilaginous at this age, certain lines and angles may be drawn on radiographs to allow estimates of geometric parameters (Figure 10–5). These may suggest evidence of acetabular dysplasia (a more vertical slope of the acetabular roof, measured as the acetabular index), femoral dysplasia (small or absent ossification center in the femoral head), or lateral superior displacement of the femoral head.

![]() Figure 10–5. Lines drawn for measurement in developmental dysplasia of the hip. In the figure, the patient’s left hip (on the right of the figure) is the subluxated one. A: Hilgenreiner line is a horizontal line of the pelvis, drawn between the triradiate cartilages. The proximal femoral ossification center should be below this line. B: Perkins line is a vertical line (perpendicular to Hilgenreiner line) drawn down from the lateral edge of the acetabulum. The femoral head ossification center, as well as the medial beak of the proximal metaphysis, should fall medial to this line. C: The acetabular index is the angle between Hilgenreiner line and a line joining the acetabular center (triradiate) with the acetabular edge as it intersects Perkins line. It measures acetabular depth and should be below 30 degrees by 1 year of age and below 25 degrees by 2 years of age. D: The center-edge angle is the angle between Perkins line and a line joining the lateral edge of the acetabulum with the center of the femoral head. It is a measure of lateral subluxation that becomes smaller as the hip subluxates laterally. Normal is 20 degrees or greater.
Figure 10–5. Lines drawn for measurement in developmental dysplasia of the hip. In the figure, the patient’s left hip (on the right of the figure) is the subluxated one. A: Hilgenreiner line is a horizontal line of the pelvis, drawn between the triradiate cartilages. The proximal femoral ossification center should be below this line. B: Perkins line is a vertical line (perpendicular to Hilgenreiner line) drawn down from the lateral edge of the acetabulum. The femoral head ossification center, as well as the medial beak of the proximal metaphysis, should fall medial to this line. C: The acetabular index is the angle between Hilgenreiner line and a line joining the acetabular center (triradiate) with the acetabular edge as it intersects Perkins line. It measures acetabular depth and should be below 30 degrees by 1 year of age and below 25 degrees by 2 years of age. D: The center-edge angle is the angle between Perkins line and a line joining the lateral edge of the acetabulum with the center of the femoral head. It is a measure of lateral subluxation that becomes smaller as the hip subluxates laterally. Normal is 20 degrees or greater.
Increased femoral anteversion (external rotation of the femoral head and neck) is often present in DDH but not visible. Increased anteversion may be seen as an increase in relative femoral neck valgus in the older child.
C. Detection of Dysplasia in the Older Child
As the infant grows older, many diagnostic maneuvers that are positive in a young infant become negative because soft-tissue changes accommodate the displaced structures. Thus, the Ortolani and Barlow signs can be negative, even in the face of grossly abnormal hip development, making detection particularly difficult (especially between 4 and 15 months of age). The first signs of developmental dysplasia may then not be recognized until the child begins to walk and demonstrates a waddling gait with excessive lumbar lordosis. Radiographs at this age are diagnostic.
![]() Treatment
Treatment
Treatment of DDH should be initiated as soon as the diagnosis is suspected. Early treatment is generally successful, whereas a delay in treatment may result in permanent dys-plastic changes. Exact treatment depends on patient age at presentation and degree of involvement. Regardless of age, treatment may fail, and the physician may need to institute a more complex treatment plan. The current recommendations described next.
A. Age 0–6 Months
A dislocated hip at this age may spontaneously reduce over 2–3 weeks if the hip is held in a position of flexion. This is best accomplished with the Pavlik harness (Figure 10–6), a canvas device that holds the hips flexed at 100 degrees and prevents adduction but does not limit further flexion. Movement in the harness is beneficial for the joint and helps achieve gradual spontaneous reduction and stabilization of the hip. Treatment with a Pavlik harness has a low risk of avascular necrosis (see section on avascular necrosis of the hip). This treatment should not be continued beyond 3–4 weeks if there is no improvement. The failure rate of the Pavlik harness is approximately 10%, necessitating more invasive treatment, such as closed or open reduction.

![]() Figure 10–6. The Pavlik harness, a device used for treatment of hip dislocation, subluxation, and dysplasia.
Figure 10–6. The Pavlik harness, a device used for treatment of hip dislocation, subluxation, and dysplasia.
B. Age 6–12 Months (Before Walking)
Gentle manipulative reduction of the dislocation under a general anesthetic and maintenance of a located position for 2–3 months in a spica cast usually stabilizes the joint. Even after the hip is stable, any residual dysplasia must be treated by bracing or surgery. In the past, prereduction skin traction was thought to reduce the risk of avascular necrosis. It is now believed that adequate hip flexion and limited abduction in the spica cast are the most important safety factors, and most surgeons no longer use traction.
C. Age 12 Months to 2 Years
In toddlers or young children in whom closed reduction failed, open reduction of the hip is required. Severe flattening of the acetabulum with distortion of the normal spherical femoral head shape is found on opening the hip. The limbus (acetabular rim) may be flattened and inverted, and the ligamentum teres is always hypertrophic. Fibrofatty tissue occupying the center of the acetabulum must be removed. Femoral shortening osteotomy may be required at the time of open reduction to reduce soft-tissue tension and minimize the risk of avascular necrosis. After reduction, the position is maintained by capsular repair (capsulorrhaphy) and a cast, until stability is achieved. Prolonged bracing or surgery is often required to resolve the residual dysplasia that accompanies untreated dysplasia in this group of children.
D. Age Older Than 2 Years
Significant residual dysplasia is present in children with DDH who are untreated at this age. Dysplasia may also persist despite successful reduction performed by any method at an earlier age. The dysplasia may be accompanied by a limp, and radiographs show a high acetabular index (more vertical acetabular roof), increased valgus of the femoral neck, and subluxation of the femoral head.
Surgical correction of dysplasia creates a stable mechanical environment that permits remodeling to a more normal joint during growth. Treatment requires bony procedures, either on the acetabular or femoral sides of the joint, or on both sides. Acetabular procedures, such as the Salter or Pemberton osteotomies, improve the acetabular index and increase the mechanical stability of the joint.
Femoral osteotomy corrects the anteversion and femoral neck valgus that characterize femoral dysplasia. The exact selection of osteotomy site may be based on maximum radiographic dysplasia or on the individual surgeon’s preference. All of the osteotomies require that the femoral head be spherical and the hip joint concentrically reduced before an attempt can be made to correct the dysplasia. In general, the osteotomy should address the site of dysplasia, that is, ace-tabular dysplasia is not ideally treated with femoral osteotomy. Nevertheless, femoral osteotomy, if performed before 4 years of age, stimulates a dysplastic shallow acetabulum to remodel into a more normal shape. This occurs because the femoral osteotomy renders the hip joint more stable, thus allowing the normal mechanisms of growth to take over. Similarly, patients exhibit a progressive decrease in femoral dysplasia following successful acetabular osteotomy.
1. Salter osteotomy—Salter osteotomy is a surgical procedure to redirect the acetabulum in DDH (Figure 10–7). Animal models demonstrate that residual hip dysplasia is accompanied by acetabular malrotation and deficiency in the anterolateral acetabular rim. Salter osteotomy corrects this deficiency by rotating the acetabular region anteriorly and laterally.

![]() Figure 10–7. Salter innominate osteotomy, used for managing acetabular dysplasia. After a transverse cut is made above the acetabulum (A), the acetabular fragment is rotated forward and outward (B) to improve acetabular coverage.
Figure 10–7. Salter innominate osteotomy, used for managing acetabular dysplasia. After a transverse cut is made above the acetabulum (A), the acetabular fragment is rotated forward and outward (B) to improve acetabular coverage.
The procedure is indicated in children 18 months to 10 years of age in whom concentric reduction of the hip was achieved. It is used to correct moderate acetabular dysplasia and can improve the acetabular index by 15 degrees. It may also be used to stabilize the hip at the time of open reduction. The pelvis above the hip joint is exposed subperiosteally. A transverse cut is made, using a wire saw, from the sciatic notch to the anteroinferior iliac spine, and the entire distal fragment (including the acetabulum) is spun on the pivot points of the notch and the pubic symphysis. This redirects the entire dysplastic acetabulum to a more horizontal stable position. A bone graft and pins hold the osteotomy open until it heals. A spica cast is used for 6 weeks to protect the graft during healing.
Salter osteotomy requires a second operation to remove the fixation pins. Because the geometric reorientation afforded is limited, there may be residual dysplasia. In addition, failure to achieve a concentric reduction before pelvic osteotomy usually renders the procedure ineffective.
2. Pemberton osteotomy—Indications for the Pemberton osteotomy (Figure 10–8) are similar to those of the Salter osteotomy, and frequently one or the other is selected according to the surgeon’s experience or preference. The Pemberton procedure is particularly suited for correction of the long stretched-out dysplastic acetabulum because it reduces the capacity of an overly spacious acetabulum. This is done by cutting above the acetabular roof, down to the flexible triradiate cartilage (the growth plate of the center of the acetabulum). The roof fragment is then pried down to a more horizontal position and held in place by wedging a bone graft into the resulting defect. The fold thus produced in the center of the acetabulum may cause temporary stiffness. In younger children, this quickly remodels, but it is the major reason many surgeons do not perform this procedure on children older than 7–8 years.

![]() Figure 10–8. Pemberton pericapsular iliac osteotomy. An osteotomy cut is made above the acetabulum down to the flexible triradiate cartilage (A). The fragment is pried down to improve acetabular coverage and held with a bone graft (B).
Figure 10–8. Pemberton pericapsular iliac osteotomy. An osteotomy cut is made above the acetabulum down to the flexible triradiate cartilage (A). The fragment is pried down to improve acetabular coverage and held with a bone graft (B).
Like the Salter procedure, Pemberton osteotomy requires concentric reduction before it is performed. For the Pemberton osteotomy, the pelvis is exposed above the joint. Under radiographic guidance, a curved osteotome is used to cut the pelvic bone from the acetabular roof down to the tri-radiate cartilage (the central growth plate of the acetabulum). The flexible cartilage allows the fragment to be hinged down over the femoral head, producing a more horizontal acetabular roof. A bone graft from the upper ilium wedges into the osteotomy site to maintain correction, and a spica cast is used until healing, which takes approximately 6 weeks.
Rarely, early extrusion or graft collapse occurs, and transient stiffness may be seen in older children. Because there is no internal fixation, a second procedure is unnecessary.
3. Femoral osteotomy—Femoral osteotomy (Figure 10–9) may be used to correct severe increased femoral anteversion or coxa valga (a high neck-shaft angle), conditions that are sometimes seen in residual DDH.

![]() Figure 10–9. Femoral osteotomy is performed at the intertrochanteric level and fixed with a plate and screws.
Figure 10–9. Femoral osteotomy is performed at the intertrochanteric level and fixed with a plate and screws.
The procedure is particularly indicated when radiographs taken with the hip in abduction and internal rotation show improvement in the overall congruency of the hip. Redirection of an anteverted, valgus hip stimulates spontaneous improvement in dysplastic acetabula in children younger than 4 years.
Femoral osteotomy is performed using a lateral approach, with the cut made across the intertrochanteric region of the femur. This site is chosen both because it is distal to the blood supply of the femoral head and because the cancellous bone heals easily. A metal blade-plate is placed in the proximal (femoral neck) fragment, usually after positioning with a provisional guidewire. The femoral neck fragment is rotated into a more horizontal position (varus) and is then internally rotated to correct excessive anteversion. The exact degree of correction is determined by preoperative radiograph positioning to achieve maximum congruence and correction of radiographic dysplasia. The plate portion is then clamped to the shaft of the bone and fixed with screws. A spica cast is usually used to supplement fixation.
After healing (6 weeks), the patient may resume walking. A Trendelenburg limp is common for 1–2 years after femoral osteotomy because of the geometric distortion of the relationship between the joint and insertion of the abductor muscles. This resolves as the femur remodels with growth and does not present a long-term problem.
4. Late salvage operations—After age 6–10 years, reduction and reconstruction of severely dysplastic or dislocated hips may be impossible. If acetabular coverage is poor but the joint is concentric, major reorientation of the acetabulum may be indicated. Salter osteotomy (see above) may be inadequate for this degree of reorientation, necessitating the addition of osteotomy cuts in the pubis and ischium to allow more aggressive repositioning of the joint surface (triple innominate osteotomy).
For children older than 10 years with hip pain and nonreconstructable joints, Chiari osteotomy reliably improves pain. After a slightly upwardly angled cut is made through the ilium just at the proximal edge of the hip capsule, the hip joint is medially displaced half the width of the iliac cut. After healing, the lateral protruding shelf of the ilium blends with the hip capsule to create a functional equivalent of an augmented hip socket, lined with the smooth capsule, which serves as part of the joint surface.
E. Complications of Surgery for DDH
1. Avascular necrosis of the hip—If a reduction maneuver for DDH was forceful or if there is tension in the soft tissues around the hip, the resulting compression of the joint may cause transient blockage of the blood supply to the femoral head. The subsequent death of the ossific nucleus and proximal growth plate of the femur (avascular necrosis) is a complication of treatment rather than of the disorder itself. A well-recognized cause of avascular necrosis is exaggerated forced abduction in the spica cast used after closed or open reduction. Avascular necrosis may be mild (involving a small fraction of the ossific nucleus), in which case it may go undetected and be of little significance. At the other extreme, avascular necrosis may lead to complete femoral head death and loss of future growth at the proximal physis. As it revascularizes, a dead femoral head may deform significantly, subluxate further, and require abduction bracing or osteotomy. Thus, it can cause leg-length inequality or early osteoarthritis of the hip. The best treatment for avascular necrosis is prevention.
2. Residual dysplasia and degenerative arthritis—No form of treatment uniformly resolves hip dysplasia, and residual dysplasia is common. It may lead to resubluxation or cause failure of remodeling. Older children are more prone to residual problems and may require repeat surgery to help resolve them. Dysplasia is a major cause of premature osteoarthritis of the hip.
Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics2000;105:E57. [PMID: 10742378]
Rejholec M: Combined pelvic osteotomy for the bipartite acetabulum in late developmental dysplasia of the hip: a ten-year prospective study. J Bone Joint Surg Br 2011;93:257. [PMID: 21282768]
Walton MJ, Isaacson Z, McMillan D, Hawkes R, Atherton WG: The success of management with the Pavlik harness for developmental dysplasia of the hip using a United Kingdom screening programme and ultrasound-guided supervision. J Bone Joint Surg Br 2010;92:1013. [PMID: 20595124]
Weinstein SL, Mubarak SJ, Wenger DR: Developmental hip dysplasia and dislocation: part II. Instr Course Lect 2004;53:531. [PMID: 15116642]
3. Legg-Calvé-Perthes Disease
![]() Essentials of Diagnosis
Essentials of Diagnosis
• Legg-Calvé-Perthes disease is most common in children age 4–8 years and is largely self-healing.
• Flexion contracture and loss of abduction are uniform and characteristic.
• There may be a small subgroup of patients with Legg-Calvé-Perthes disease who benefit from surgical treatment.
Legg-Calvé-Perthes disease (LCP, Perthes disease) is a serious but mostly self-limited pediatric hip disorder. Although its cause is unknown, the disease is thought to be related to avascular necrosis of the hip. It affects children between 4 and 10 years of age and is somewhat more common in boys. Children with the disease are often small for their age and have retarded bone age. The disease is generally unilateral. Although bilateral LCP of the hips occurs in about 10% of cases, in patients with symmetric changes/stages, other conditions such as Gaucher disease or multiple epiphyseal dysplasia must be considered. Multiple epiphyseal dysplasia is most readily diagnosed by evaluation of other radiographs, in particular of the knee and, if confirmatory, of the spine to assess for spondyloepiphyseal dysplasia. Patients with multiple epiphyseal dysplasia generally have heights in the fifth percentile or below. Newer investigations suggesting that some cases of LCP might be related to a variety of transient or permanent hypercoagulation states are intriguing but not confirmed in multiple centers. Surprisingly, trauma is not considered a causative factor in LCP.
Although early radiographs may be negative, they eventually show fragmentation, irregularity, and collapse of part or the entire femoral head ossification center (Figure 10–10). The few pathologic specimens that were examined suggest that multiple rather than single episodes of avascular necrosis occur over a period of months. Early bone scans may show a filling defect corresponding to areas of necrosis, and MRI is typical of avascular necrosis. The disease has a characteristic course (see Figure 10–10). Initially, the avascular episodes are silent and the child is asymptomatic. As the disease progresses, the necrotic femoral epiphysis is revascularized. Osteoclasts remove dead bone while osteoblasts simultaneously lay down new bone on the dead trabeculae (a process known as creeping substitution). During this phase, the femoral head is mechanically weak. Fragmentation and collapse of the bony structure may then occur, causing geometric flattening and deformity of the ossific nucleus and femoral head. The newly replaced bone takes the shape of the collapsed head. At this point, continued growth may allow gradual remodeling and improvement of the femoral head shape until maturity. The symptomatic collapse phase rarely exceeds 1–1.5 years, but full revascularization and remodeling may continue silently for several years thereafter. Although cartilage is not specifically injured by the avascular events, hyperemia can cause articular cartilage thickening, ectopic ossification, and physeal damage that affects femoral neck growth.

![]() Figure 10–10. Legg-Calvé-Perthes disease. A: Central necrotic fragment with collapse. B: Same patient after healing and partial remodeling.
Figure 10–10. Legg-Calvé-Perthes disease. A: Central necrotic fragment with collapse. B: Same patient after healing and partial remodeling.
![]() Clinical Findings and Classification
Clinical Findings and Classification
A. Symptoms and Signs
The initial presentation of LCP is usually a painless limp, with aching pain in older children. If pain is present, it may be mild and referred to the thigh or knee. Physical examination discloses atrophy of the thigh on the affected side and, usually, limited hip motion. The typical patient has a flexion contracture of 0–30 degrees, loss of abduction compared with the opposite side (in severe cases, no abduction beyond 0 degrees), and loss of internal rotation of the hip.
B. Imaging Studies
Radiographs may be negative at first, probably because the initial softening of the femoral head is sufficient to cause symptoms but insufficient to change the radiographic appearance of the femoral head. The eventual characteristic collapse of portions of the femoral head is diagnostic of the disease, however.
The exact extent of necrosis, which is estimated in fourths of the head using the Catterall classification (Figure 10–11), is helpful in determining whom to treat. This may require additional radiographs.

![]() Figure 10–11. The Catterall classification is used to determine probable course and prognosis of Legg-CalvéPerthes disease. It is based on progressive involvement of approximate fourths of the femoral head. AP, anteroposterior.
Figure 10–11. The Catterall classification is used to determine probable course and prognosis of Legg-CalvéPerthes disease. It is based on progressive involvement of approximate fourths of the femoral head. AP, anteroposterior.
An alternative radiograph classification uses the lateral third of the femoral epiphysis (the so-called lateral pillar). Collapse of this structure suggests a poor prognosis for late deformity (class C), whereas maintenance of pillar height correlates with good long-term results (class A). Partial collapse suggests an intermediate prognosis (class B). The difficulty with all classification systems is their reproducibility and the need to delay until the collapse phase before the exact extent of involvement is clear.
There is little value in bone scans or MRI in the clinical management of LCP.
![]() Treatment Options
Treatment Options
A. No Treatment
Age at presentation and range of motion (ROM) of the hip are the two most significant predictors of long-term outcome. Children with bone age less than 5 years and children who exhibit relatively minor involvement (less than half of the femoral head) rarely need treatment. In these children, so much of the femoral head is cartilage, and therefore unaffected by necrosis, that mechanical collapse does not markedly decrease sphericity. Also, younger children have tremendous remodeling potential, and minor collapse can be outgrown before maturity. Limited hip ROM may be due to muscle spasm early on, or synovitis; but in late disease, it may reflect incongruity of the joint. Older children who exhibit some radiographic changes but have excellent ROM may require only observation and serial reexamination.
B. Nonoperative and Operative Treatment
The issues surrounding selection of patients with LCP who need treatment are as highly controversial as the treatment itself. Most experts agree that children who maintain excellent motion (particularly abduction greater than 30 degrees in the absence of flexion contracture) may not require intervention. In children older than 4–5 years with significant collapse or progressive loss of abduction, treatment is frequently recommended.
No evidence indicates that use of crutches or relief of weight bearing has any effect on femoral head collapse in this disease. For those children requiring it, however, treatment should minimize the effects of collapse and subluxation that often occur when the femoral head deforms. This is best achieved by abduction of the hip until subluxation resolves. The molding action of the acetabular shape is thought to help improve the contour of the collapsing femoral head. Abduction can be accomplished nonoperatively by holding the legs in abduction (Petrie) casts or using an ambulatory brace (Figure 10–12).

![]() Figure 10–12. Abduction bracing is one method used for ambulatory treatment of Legg-Calvé-Perthes disease.
Figure 10–12. Abduction bracing is one method used for ambulatory treatment of Legg-Calvé-Perthes disease.
Operative procedures are advocated by some and include varus femoral osteotomy and Salter osteotomy, which were adapted from hip dysplasia treatment to control the subluxation seen in some cases of LCP. Healing usually occurs within 18 months. The best current investigations suggest that children over 8 years who have partial head collapse (lateral pillar B-C or Catterall III) may ultimately have better radiographic outcome if treated by surgery.
Despite many studies, there is still no consensus for the best method of treatment; some patients do well without treatment, whereas others have a poor result after aggressive treatment. Prognosis can often be predicted from the knowledge of certain factors (Table 10–5), with age being the most important.
Table 10–5. Factors in long-term prognosis for patients with Legg-Calvé-Perthes disease.

Herring JA, Kim HT, Browne R: Legg-Calvé-Perthes disease. Part II: prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86-A:2121. [PMID: 15466720]
Karol LA: Legg-Calvé-Perthes disease 100 years on: what have we learned? J Am Acad Orthop Surg 2010;18:643. [PMID: 21041798]
Kim HK: Legg-Calvé-Perthes disease. J Am Acad Orthop Surg 2010; 18:676. [PMID: 21041802]
Terjesen T, Wiig O, Svenningsen S: The natural history of Perthes’ disease. Acta Orthop 2010;81:708. [PMID: 21067434]
4. Slipped Capital Femoral Epiphysis
![]() Essentials of Diagnosis
Essentials of Diagnosis
• Slipped capital femoral epiphysis is most common in overweight children entering puberty.
• Early diagnosis and surgical management give the best results.
Slipped capital femoral epiphysis is an adolescent hip disorder characterized by displacement of the femoral head on the femoral neck through failure of the proximal femoral physis (growth plate). Displacement changes the geometry of the upper end of the femur and hinders hip function (Figure 10–13). This disorder is one of the main causes of premature osteoarthritis in young adults.

![]() Figure 10–13. Anteroposterior (AP) and frog-leg views of a slipped epiphysis. The dotted lines show the normal position of the femoral head.
Figure 10–13. Anteroposterior (AP) and frog-leg views of a slipped epiphysis. The dotted lines show the normal position of the femoral head.
Slipped capital femoral epiphysis affects both male and female adolescents 11–13 years of age. In 30–40% of patients, the condition is bilateral, although both legs are not always affected simultaneously. The typical patient is overweight—often markedly so—and is in either late prepuberty or early puberty. Rarely, the patient is tall, asthenic, and rapidly growing.
This disorder occurs at a time when the cartilage physis of the proximal femur is thickening rapidly under the influence of growth hormone. The vigorous secretion of sex hormone has not yet begun, however, so the biological effect of sex hormones on closure and stabilization of the growth plate is absent. This combination of thick growth plate cartilage (weaker than bone and subject to shear), lack of sexual maturity (which would stabilize the physis), mechanical stress (caused by obesity), and the peculiar anatomic mechanics of the hip joint renders the growth plate susceptible to slippage.
The direction of the slip is always posterior and often medial, and the mechanical bases of chronic and acute disorders are the same. In chronic slipped capital femoral epiphysis, the most common form (90% of patients), the femoral head slips insidiously at the growth plate over the course of several months. In the acute form, the femoral head is suddenly displaced, a condition that can be superimposed on chronic changes. Displacement may occur during normal activity or following minor trauma.
Because slipped capital femoral epiphysis is a progressive disorder and the prognosis depends on the severity of the slippage, early detection and prompt treatment are imperative.
![]() Clinical Findings
Clinical Findings
A. Symptoms and Signs
There are two forms of the disorder: chronic and acute. The onset of chronic slipped capital femoral epiphysis is usually insidious, with a history of a painful limp for 1 to several months prior. The pain is characteristically aching and located in the thigh or knee rather than the hip. This referred pain to the knee is responsible for many misdiag-noses. Patients may be seen for knee pain and dismissed as normal after a negative knee examination and radiographs. A high index of suspicion is required to detect slipped capital femoral epiphysis in the obese limping adolescent complaining of knee pain. The change in hip ROM is usually diagnostic: loss of abduction and internal rotation of the hip are evident, although these may be difficult to identify in the grossly overweight child. There is almost always a characteristic obligatory external rotation of the hip when it is flexed because of the distorted hip anatomy caused by the disorder. The femoral head is posterior to its normal position, so the flexed hip must externally rotate to keep the head within the acetabulum.
Acute slipped capital femoral epiphysis is accompanied by severe pain and limping, which may render the patient immobile. The onset is sudden, following little or no trauma, and examination discloses a painful, guarded, restricted range of hip motion. An acute slip is analogous to an epiphy-seal fracture. In its unstable form, the patient is unable to bear weight, and there is a high rate of avascular necrosis. In its stable form, the sudden increase in displacement is painful, but limited weight bearing is possible and the risk of avascular necrosis appears to be lower.
B. Imaging Studies
Slipped capital femoral epiphysis can be difficult to detect on standard AP radiographs (Figure 10–14). A frog-leg lateral view is the best for detecting mild forms because slippage is always posterior. A radiograph also shows changes suggesting acute or chronic forms, information that may be critical to management of the disorder.

![]() Figure 10–14. Radiograph diagnosis of left slipped capital femoral epiphysis. A: Anteroposterior film shows subtle medial displacement of left epiphysis, best appreciated by drawing a line (Klein line) along the lateral side of the normal and abnormal femoral neck. The slipped epiphysis does not protrude lateral to this line. B: Frog-leg lateral radiograph clearly demonstrates posterior displacement.
Figure 10–14. Radiograph diagnosis of left slipped capital femoral epiphysis. A: Anteroposterior film shows subtle medial displacement of left epiphysis, best appreciated by drawing a line (Klein line) along the lateral side of the normal and abnormal femoral neck. The slipped epiphysis does not protrude lateral to this line. B: Frog-leg lateral radiograph clearly demonstrates posterior displacement.
Establishing the severity of slippage is important in determining treatment and prognosis. Severity is estimated by the percentage of femoral neck left exposed. Slippage of less than 25% of neck width is mild; 25–50% is moderate; and more than 50% is severe.
![]() Treatment
Treatment
Slipped capital femoral epiphysis is usually a progressive disease that requires prompt surgical treatment. Because the changes in the chronic form occur so slowly, it is impossible to manipulate the femoral head into a better position. Treatment consists of fixing the slip in its current position and preventing progression. This is done by inserting one or more screws or pins across the growth plate, regardless of the severity of the slip (pinning in situ).
Following surgery, aching rapidly resolves, and during the remaining 2–3 years of skeletal growth, the extent of remodeling of the distorted proximal femur may be considerable, leading to an improved ROM.
Because of bilateral involvement, some surgeons recommend prophylactic screw fixation of the normal side at the time of initial treatment. This is particularly indicated in children ages 10 years and under.
Acute slips, if unstable, may be gently reduced before fixation, but the risk of further damage to the tenuous blood supply of the proximal femur and subsequent avascular necrosis is always significant. For this reason, many surgeons accept the position of an acute slip and pin it in situ.
In some cases, high-grade slipped capital femoral epiphysis does not remodel sufficiently with growth, despite treatment. In these cases, a residual, chronically painful limp is present, requiring correction by proximal femoral osteotomy. The osteotomy site may be at the level of the slip, which is mechanically effective but relatively risky for the blood supply. Alternatively, osteotomy can be performed at the trochanteric level; this is a safer procedure for correction of the functional deformity but does not resolve the exact anatomic deformity.
![]() Complications
Complications
A. Chondrolysis
In addition to the problems of impingement of the anterior metaphyseal prominence, which can impede motion, patients with slipped capital femoral epiphysis may rarely develop chondrolysis, a poorly understood degeneration of the hip articular cartilage. It may be painful and may progress to severe joint narrowing and degenerative changes within 6 months.
During chondrolysis, cartilage is replaced by fibrous tissue, the joint capsule thickens and contracts, and joint motion is lost. Typically, the joint stiffens in flexion, abduction, and external rotation. Radiographs reveal joint narrowing, irregularity, and subchondral sclerosis, as well as regional osteoporosis from disuse.
Chondrolysis can result from iatrogenic malposition (permanent penetration) of pins or screws used for fixation of slipped capital femoral epiphysis. Although brief penetrations during surgery are probably common and cause no complications, unrecognized permanent pin penetration is disastrous. Chondrolysis also appears without obvious penetration and occasionally is detected in patients before treatment begins.
Chondrolysis is treated by nonsteroidal anti-inflammatory drugs (NSAIDs), aggressive physical therapy and ROM exercises, and observation. Capsular release is sometimes useful in resistant cases. Approximately half of patients eventually recover satisfactory painless motion. The other half may require hip fusion for symptomatic relief.
B. Avascular Necrosis
Patients with an acutely slipped capital femoral epiphysis can develop avascular necrosis of the femoral head (see section on developmental dysplasia of the hip). These patients are usually teenagers so their hips lack potential for remodeling, and the prognosis is therefore poor. Yet, some patients with partial head involvement regain a painless hip after 1–2 years of symptoms. Some patients with painless but abnormal ROM may be treatable by intertrochanteric osteotomy to reorient the arc of motion. Long-term pain following avascular necrosis is treated by hip fusion.
![]() Prognosis
Prognosis
Slipped epiphysis is a major cause of early osteoarthritis. In general, the higher the degree of slip, the earlier the degenerative changes begin. In fact, a statistical increase in degenerative arthritis is evident even in the radiographically normal hip of patients with a contralateral slipped epiphysis. This suggests that subclinical bilateral involvement is more common than recognized.
Loder RT, Greenfield ML: Clinical characteristics of children with atypical and idiopathic slipped capital femoral epiphysis: description of the age-weight test and implications for further diagnostic investigation. J Pediatr Orthop2001;21:481. [PMID: 11433161]
Peck D: Slipped capital femoral epiphysis: diagnosis and management. Am Fam Physician 2010;82:258. [PMID: 20672790]
Sankar WN, McPartland TG, Millis MB, Kim YJ: The unstable slipped capital femoral epiphysis: risk factors for osteonecrosis. J Pediatr Orthop 2010;30:544. [PMID: 20733417]
FOOT DISORDERS
1. Metatarsus Adductus
Metatarsus adductus (metatarsus varus) is the most common foot deformity in the newborn infant, occurring in 5 in 1000 live births, frequently bilaterally. Although it is usually isolated, several apparently unrelated deformities (such as DDH) are statistically more likely to occur in the presence of this disorder. The cause is unknown but might be related to so-called uterine packing.
![]() Clinical Findings
Clinical Findings
The hallmark of metatarsus adductus is medial deviation of the forefoot, with the apex of the deformity at the midtarsal region. The hindfoot is normal. A deep skin crease frequently is evident at the medial border of the foot, suggesting the deformity has been present for some time. The adducted forefoot usually can be passively corrected to a neutral position but occasionally is fairly rigid. Ankle motion is normal, without contracture of the gastrocnemius-soleus muscles.
![]() Treatment
Treatment
Metatarsus adductus tends to be self-correcting. Even severe cases generally resolve by 12–18 months of age without treatment. Nevertheless, many orthopedists use passive stretching to reassure parents the child is being treated. There is no scientific evidence that passive correction and serial plaster casting will speed resolution of the disorder.
2. Congenital Clubfoot
![]() Essentials of Diagnosis
Essentials of Diagnosis
• Clubfoot is characterized by equinus, smaller foot size, smaller calf muscles, and stiffness of tarsal joints.
• Treatment with casting and minor surgical tenotomy is usually successful but technique dependent.
• Bracing for 1–4 years after cast correction improves the ultimate outcome.
Congenital clubfoot (equinovarus foot; talipes equinovarus) is a severe fixed deformity of the foot (Figure 10–15). It is characterized by fixed ankle plantar flexion (equinus), inversion and axial internal rotation of the subtalar (talocalcaneal) joint (varus), and medial subluxation of the talonavicular and calcaneocuboid joints (adductus). Severe cavus may be present, with a medial and plantar midfoot crease. Calf atrophy, while variable, is always present. Whether unilateral or bilateral, the deformity is more common in males, although when it occurs in females, it tends to be more severe.

![]() Figure 10–15. Clinical appearance of congenital right clubfoot.
Figure 10–15. Clinical appearance of congenital right clubfoot.
The incidence in the newborn population is 1 in 1000, with increased risk for families in which even distant members have the deformity. There is considerable evidence that clubfoot is an inherited trait, but the disorder appears to reflect polygenetic expression, and exact inheritance patterns are unclear. Although most are isolated deformities and considered idiopathic, clubfoot may be present in association with a wide variety of syndromes that affect the musculoskeletal system.
![]() Clinical Findings
Clinical Findings
A. Symptoms and Signs
Clinical diagnosis of clubfoot is uncomplicated. Because it is a rigid deformity, clubfoot cannot be passively corrected the way metatarsus adductus can. Frequently, the foot is so severely internally rotated and inverted that the sole faces superiorly. Occasionally, the plantar flexion of the ankle is not obvious because the posterior tip of the calcaneus is small, high, and difficult to palpate. Clubfoot is always associated with a permanent decrease in calf circumference related to fibrosis of the calf musculature. This may not be obvious at birth but becomes more apparent after the child begins to walk.
Special attention should be paid to the presence of spine deformity, caudal dimpling, or midline spinal hairy patches, all of which may imply a neurogenic component. Thus, the examining physician should carefully search for features of other deformities or syndromes.
B. Imaging Studies
Increasingly, clubfoot is suspected from prenatal ultrasound examination. Radiographs are rarely of value in the initial clubfoot evaluation because the bones of the foot are minimally ossified at birth. Radiographs become more important if the physician is considering surgical intervention or if the child has reached walking age, and radiographs can quantify the completeness of correction achieved by casting or surgery.
The typical radiographic findings of incompletely treated clubfoot include the following features:
1. Presence of hindfoot plantar flexion
2. Lack of the normal angular relationship between the talus and calcaneus (so-called parallelism of talus and calcaneus)
3. Residual medial subluxation or displacement of the navicular on the talus and the cuboid on the calcaneus (Figure 10–16)
![]() Figure 10–16. Diagrammatic appearance of radiograph in clubfoot. A: Normal foot. B: Clubfoot.
Figure 10–16. Diagrammatic appearance of radiograph in clubfoot. A: Normal foot. B: Clubfoot.
![]() Treatment
Treatment
A. Manipulative Treatment
Clubfoot always requires treatment, which should begin at birth. The initial approach is passive manipulation and positioning to the corrected position. In the United States, the majority of orthopedists use serial manipulation and casting, usually at 1-week intervals in the first month of life, and at 1- to 2-week intervals thereafter if required. In other parts of the world, strapping (with adhesive tape) and splinting with a variety of braces are popular methods (in addition to serial casting) for maintaining the manipulated correction. When casting is performed, there is agreement that specific techniques are more likely to be successful. Even when the deformity responds to casting, there is usually sufficient Achilles tightness that a heel cord lengthening needs to be done at 4 weeks or later to facilitate cast correction.
The Ponseti method of casting has been widely adopted in many parts of the world as an effective cast protocol. In this method, a specific sequence of casts is applied weekly for 3–4 weeks, followed by early percutaneous Achilles tenotomy. After a brief additional period of casting, the foot position is maintained by use of a brace for up to 3 years, worn at nights and during naps.
B. Surgical Treatment
Most clubfeet are successfully treated with casting and limited release, but severe clubfeet (often associated with syndromes) may require more extensive surgery. Surgical correction of all clubfoot deformities is generally performed in one stage. At times, the casting corrects most of the midfoot deformity, and simple posterior release (ankle capsulotomy and Achilles tendon lengthening) are all that is required. Frequently, the surgeon must consider correction of the entire group of deformities through a comprehensive, extensive surgical approach.
One common approach uses the so-called Cincinnati incision, which extends from the navicular bone medially, around the superior portion of the heel, to the cuboid bone laterally (Figure 10–17). During surgery, the medial posterior tibial neurovascular bundle must be identified and protected. The tendons of the posterior tibialis, flexor digitorum longus, flexor hallucis longus, and Achilles tendon are Z-lengthened. The capsules of the talonavicular joint, subtalar (talocalcaneal) joint, and posterior ankle joint are released to allow repositioning of the bones of the hindfoot and midfoot.

![]() Figure 10–17. Cincinnati incision used for surgical correction of clubfoot.
Figure 10–17. Cincinnati incision used for surgical correction of clubfoot.
The navicular is usually subluxated medially on the head of the talus and must be repositioned onto its normal location. The calcaneus is both inverted and internally rotated on the talus. This is corrected by manually derotating the subtalar joint and tilting the calcaneus back into a neutral position. These corrections are usually held in place after reduction by inserting small K-wires, which are removed after 4–6 weeks.
The ankle is repositioned by dorsiflexion to neutral prior to repair of the lengthened Achilles tendon. Postoperative casting allows the gaping capsule to reform with the bones of the clubfoot in their appropriate, corrected position.
C. Complications
Early complications of clubfoot surgery are rare, but the rate of recurrence within 3 years is 5–10%. Mild recurrence of deformity is fairly common, and even when deformity is permanently corrected, the foot always remains smaller and stiffer than normal and calf circumference is reduced. Families must be informed of this possibility early in treatment so they have realistic expectations about the outcome.
If surgical release is too aggressive, overcorrection with late heel valgus and an overlengthened heel cord can occur. There is broad agreement that a slightly underreleased clubfoot is much more functional than an overreleased one, and the trend to less surgery and more conservative treatment is currently strong.
Dobbs MB, Morcuende JA, Gurnett CA, et al: Treatment of idiopathic clubfoot: an historical review. Iowa Orthop J 2000;20:59. [PMID: 10934626]
Herzenberg JE, Radler C, Bor N: Ponseti versus traditional methods of casting for idiopathic clubfoot. J Pediatr Orthop 2002; 22:517. [PMID: 12131451]
Matos MA, de Oliveira LA: Comparison between Ponseti’s and Kite’s clubfoot treatment methods: a meta-analysis. J Foot Ankle Surg 2010;49:395. [PMID: 20610205]
Richards BS, Faulks S, Rathjen KE, Karol LA, Johnston CE, Jones SA: A comparison of two nonoperative methods of idiopathic clubfoot correction: the Ponseti method and the French functional (physiotherapy) method. J Bone Joint Surg Am 2008; 90:2313. [PMID: 18978399]
Zionts LE, Dietz FR: Bracing following correction of idiopathic clubfoot using the Ponseti method. J Am Acad Orthop Surg 2010;18:486. [PMID: 20675641]
Zionts LE, Zhao G, Hitchcock K, Maewal J, Ebramzadeh E: Has the rate of extensive surgery to treat idiopathic clubfoot declined in the United States? J Bone Joint Surg Am 2010;92:882. [PMID: 20360511]
3. Calcaneovalgus Foot
Calcaneovalgus foot is generally considered a uterine-packing problem in which the foot is markedly dorsiflexed at birth so the dorsum of the foot sits against the anterior surface of the tibia (Figure 10–18). The hindfoot is usually in moderate eversion (valgus) as well. Although some flexibility is present with the deformity, there is resistance to full motion, and most cases do not allow ankle plantar flexion beyond a right angle.

![]() Figure 10–18. Calcaneovalgus foot as it appears in relaxed position (A) and maximally plantar flexed (B).
Figure 10–18. Calcaneovalgus foot as it appears in relaxed position (A) and maximally plantar flexed (B).
Despite its dramatic appearance, calcaneovalgus foot corrects spontaneously within 2–3 months. Although some orthopedists brace or apply serial casts and many recommend stretching exercises, all true calcaneovalgus feet resolve without treatment.
![]() Congenital Vertical Talus
Congenital Vertical Talus
Calcaneovalgus foot must be differentiated from a much rarer condition known as congenital vertical talus (congenital rocker-bottom foot, congenital complex pes valgus). In this deformity, although the foot appears to lie against the anterior tibia, the hindfoot is actually plantar flexed (positioned in equinus) because of contracture of the posterior calf muscles. To accommodate plantarflexion of the hindfoot and dorsiflexion of the forefoot, the midfoot joints (talonavicular and calcaneocuboid joints) must subluxate or dislocate dorsally.
Congenital vertical talus often accompanies genetic disorders, syndromes such as arthrogryposis, or neuromuscular disorders such as spina bifida. It is occasionally found in otherwise normal infants, however. Treatment is usually surgical, and casting frequently does not resolve the disorder.
4. Cavus Foot
Cavus foot is a foot with an abnormally high arch. Although it is difficult to ascribe a particular threshold of arching beyond which treatment is necessary, most deformities are dramatic enough to make diagnosis straightforward (Figure 10–19).

![]() Figure 10–19. Cavus foot: clinical appearance and radiographic appearance.
Figure 10–19. Cavus foot: clinical appearance and radiographic appearance.
Cavus foot frequently accompanies hindfoot varus deformity (cavovarus foot), and there may be clawing of the toes and demonstrable weakness of ankle or foot muscles. In addition, calluses beneath the metatarsal heads and heel skin are common. Hindfoot varus in individuals with a cavovarus deformity is nonstructural if it can be corrected with the “block test,” and surgical procedures directed at correcting the hindfoot deformity are not necessary. If the patient is symptomatic, the treatment of choice is plantar release with first metatarsal osteotomy and possible tendon transfers.
![]() Clinical Findings
Clinical Findings
One of the most common symptoms of cavus foot is anterior ankle pain, sometimes associated with toe walking. This paradoxical situation occurs because of the pathologic anatomy of the cavus foot. The forefoot is severely plantar flexed on the hindfoot, requiring marked ankle dorsiflexion to compensate. When the cavus becomes too severe, ankle dorsiflexion is blocked, leading to anterior ankle impingement and pain. The inability to dorsiflex further compromises forefoot clearance, and eventually, only the metatarsals can contact the floor. This can be misinterpreted as ankle plan-tarflexion contracture, leading to unnecessary (and possibly harmful) heel cord release.
![]() Pathogenesis
Pathogenesis
The cause of cavus foot is usually muscle imbalance in a growing foot. Thus, cavus is rarely found in early childhood but is fairly frequent after 8–10 years of age. Although intrinsic muscle weakness is a major cause of cavus foot, weakness of the peroneal or anterior tibialis muscles is also implicated. Cavus foot is rarely found in the absence of an underlying neuromuscular condition.
Cavus foot is a marker for neuromuscular disease. Diagnosis requires a thorough search for the underlying cause and may require neurologic consultation, spinal MRI, and electromyographic (EMG) studies. Table 10–6 lists common neuromuscular causes of cavus foot.
Table 10–6. Common neuromuscular causes of cavus foot.

![]() Treatment
Treatment
Conservative treatment of cavus foot includes accommodation by shoe modifications or inserts. These modalities do not actually correct the condition; severe deformity requires surgical correction by tendon transfers to restore muscle balance, by midfoot wedge osteotomy to correct bony deformity, or by triple arthrodesis (hindfoot fusion in a corrected position).
Schwend RM, Drennan JC: Cavus foot deformity in children. J Am Acad Orthop Surg 2003;11:201. [PMID: 12828450]
5. Pes Planus (Flatfoot)
Flatfoot refers to loss of the normal longitudinal arch of the medial foot. Many cases of flatfoot are inherited, and a careful family history may uncover other persons with the condition. The foot is usually flexible, so the arch appears when the foot is not bearing weight. Hindfoot valgus (heel eversion) is often present. In severe cases, flatfoot may be painful, but this aspect of the deformity is often overemphasized.
![]() Clinical Findings
Clinical Findings
Physical determination of the flexibility of the flatfoot requires careful examination. Subtalar motion is usually normal. In feet that exhibit a flat arch and valgus heel while standing, examination from the posterior aspect frequently discloses a normal arch and varus heel by muscle action when the patient stands on tiptoe. If these signs of a flexible flatfoot are not present, alternative diagnoses such as tarsal coalition (see section on tarsal coalition) should be considered. The physician should also look for painful plantar calluses.
![]() Imaging Studies
Imaging Studies
Standing radiographs disclose loss of the normal medial longitudinal arch and may show mild lateral subluxation of the talonavicular joint as well. In severe chronic cases, degenerative talonavicular spurring may be present.
![]() Treatment
Treatment
Symptomatic treatment (shoe modifications, arch supports, and plantar inserts) is appropriate because no long-term treatment can alter the anatomic features of the disorder. Posterior tibial advancement, subtalar joint elevation or fusion, and elongation osteotomy of the lateral calcaneal neck are surgical options, but they may not provide reproducible, predictable resolution of the problem.
6. Tarsal Coalition
Tarsal coalition is a congenital connection between two or more tarsal bones. Coalitions may be fibrous, cartilaginous, or bony. Coalitions usually occur between two bones and are cartilaginous in early life but eventually ossify (or nearly ossify) as the foot matures. Frequently bilateral, coalitions often follow an autosomal dominant inheritance pattern.
The most common sites for tarsal coalition are between the calcaneus and the navicular laterally (Figure 10–20) and between the talus and the calcaneus medially.

![]() Figure 10–20. Calcaneonavicular tarsal coalition is best seen on oblique radiograph projection.
Figure 10–20. Calcaneonavicular tarsal coalition is best seen on oblique radiograph projection.
![]() Clinical Findings
Clinical Findings
Symptoms of tarsal coalition may include foot pain and stiffness as the lesion begins to ossify during early adolescence. The resulting stiffness and abnormal intertarsal movement patterns in the hindfoot lead to progressive loss of subtalar motion and fixed valgus (eversion) of the heel. Tarsal coalition is often called peroneal spastic flatfoot because the peroneals appear to be protectively overactive. As the lesion matures, pain may diminish but stiffness increases, and the abnormal valgus posture persists.
This diagnosis should be suspected in adolescents with foot pain, valgus heel, and decreased subtalar motion.
![]() Imaging Studies
Imaging Studies
Lateral, anteroposterior, and oblique radiographs of the foot confirm the diagnosis of calcaneonavicular coalition, but special subtalar radiographs (Harris views), CT scan, or MRI may be necessary to delineate medial talocalcaneal lesions.
![]() Treatment
Treatment
Not all coalitions require treatment. The decision to initiate treatment depends on the severity of pain, stiffness, and fixed valgus deformity. Conservative treatment consists of casting to reduce pain and peroneal spasm. If this fails, the coalition can be surgically resected and the resultant space filled with autologous fat or muscle to prevent recurrence. In late or neglected cases with pain or deformity, hindfoot fusion by triple arthrodesis is effective treatment for both symptoms.
Sankar WN, Weiss J, Skaggs DL: Orthopaedic conditions in the newborn. J Am Acad Orthop Surg 2009;17:112. [PMID: 19202124]
Yeagerman SE, Cross MB, Positano R, Doyle SM: Evaluation and treatment of symptomatic pes planus. Curr Opin Pediatr 2011;23:60. [PMID: 21169838]
7. Toe Deformities
Toe deformities occur as isolated conditions, in association with similar hand deformities, and as part of other syndromes. The more commonly found deformities are presented here, with mention of associated hand problems.
![]() Simple Syndactyly
Simple Syndactyly
Simple syndactyly, a connection of two or more toes, is the most common toe deformity. It is most common between the second and third toes. The webbing is usually complete. This disorder demonstrates a strongly familial inheritance pattern and causes no symptoms. It is rarely treated in the foot. In the hand, however, surgical separation is required to restore normal finger function.
![]() Polydactyly
Polydactyly
Polydactyly is the presence of more than five digits on either the hands or the feet. It is frequently hereditary and often bilateral. Duplication of the thumbs may mirror duplication of the great toes, and both generally require surgical treatment. Both preaxial (duplication of medial toes and radial digits) and postaxial polydactyly (duplication of the lateral toes or ulnar digits) often accompany genetic syndromes and should prompt the physician to look for other symptoms. Treatment is by surgical excision at about 1 year of age; the actual surgery, particularly for medial duplications, may be complex.
8. Constriction Bands (Amniotic Bands) and Acrosyndactyly
During gestation, protein-laden amniotic material can condense around limb segments. These amniotic bands may indent delicate embryonic tissues, causing constriction rings or even necrosis and resorption of the distal segment (congenital amputation). Constriction bands may be isolated or associated with Streeter dysplasia. The syndactyly of Streeter dysplasia differs from simple syndactyly in that the distal, rather than proximal, web is obliterated (acrosyndactyly). It is thought to be an acquired, rather than hereditary, condition, caused by shearing of the delicate tips of the embryonic digits, followed by conjoined healing of distal digits. Although acrosyndactyly of the fingers must be released to allow independent function, acrosyndactyly of the toes is rarely symptomatic, and does not need treatment.
Constriction bands may be very deep and circumferential and occasionally must be released surgically by Z-plasty immediately after birth to avoid postnatal necrosis. Usually, only half of the circumference of a band is released at one time, to protect any remaining blood supply in the other half. Reports of successful one-stage resection and Z-plasty of constriction bands suggest that the remaining blood supply is probably subfascial and interosseous.
9. Adolescent Bunions (Hallux Valgus)
Although bunion (prominence of the medial metatarsophalangeal joint of the great toe) is rare in children, this troublesome deformity often requires treatment. It is frequently hereditary, usually seen in early adolescence, and almost always found in conjunction with a wide forefoot caused by varus (medial deviation) of the first metatarsal shaft (metatarsus primus varus). The wide forefoot allows severe lateral deviation of the great toe (hallux valgus), causing the prominent base of the great toe to rub against the inside of the shoe and create a painful bunion (Figure 10–21).

![]() Figure 10–21. Adolescent bunion (hallux valgus) is generally accompanied by a wide forefoot with splaying of the first metatarsal (metatarsus primus varus).
Figure 10–21. Adolescent bunion (hallux valgus) is generally accompanied by a wide forefoot with splaying of the first metatarsal (metatarsus primus varus).
Although conservative measures may relieve discomfort, many adolescent bunions are progressive and require surgical management. Surgery must address each aspect of the deformity. The surgeon must trim the bunion, correct the varus angulation of the first metatarsal by osteotomy, and centralize and balance the hallux valgus by lengthening the adductor hallucis muscle. There is a fairly high incidence of recurrence of the deformity following surgery.
Johnson AE, Georgopoulos G, Erickson MA, et al: Treatment of adolescent hallux valgus with the first metatarsal double osteotomy: the Denver experience. J Pediatr Orthop 2004;24:358. [PMID: 15205615]
TORSIONAL AND ANGULAR DEFORMITIES OF THE KNEE AND LEG
![]() Essentials of Diagnosis
Essentials of Diagnosis
• Most torsional deformities are benign and self-correcting with growth.
• Angular deformities at the knee, particularly genu varum, must be distinguished from more common physiologic variants, since they often need early treatment.
Torsional (rotational) and angular deformities are a major source of referrals to pediatric orthopedic surgeons (Figure 10–22). Most of these patients are young (< 5 years) and have internal rotational deformities resulting in a so-called pigeon-toed gait.

![]() Figure 10–22. The major causes of clinical in-toeing include increased femoral anteversion (A), internal tibial torsion (B), and metatarsus adductus (C).
Figure 10–22. The major causes of clinical in-toeing include increased femoral anteversion (A), internal tibial torsion (B), and metatarsus adductus (C).
The internal rotation, which can occur at the level of the thigh, leg (shin), or foot, is a cosmetic problem. Little evidence indicates that any of the so-called torsional deformities are harmful to the child or cause significant disability in the adult. Angular deformities (usually varus or valgus at the knee) are also usually benign, although careful evaluation and workup, including radiographic or other imaging modalities, occasionally disclose conditions requiring treatment. Nevertheless, most torsional and angular deformities are physiologic variations of normal anatomy, and they correct spontaneously over time.
![]() Increased Femoral Anteversion
Increased Femoral Anteversion
The normal femoral neck does not lie exactly in the frontal (coronal) plane but rather projects anteriorly from the plane at an angle called the angle of anteversion (Figure 10–23). Infants have anteversion of as much as 40 degrees, but this angle gradually reduces with growth, so normal adult femurs exhibit anteversion of 15 degrees. In some children, this gradual regression is slow or incomplete, causing the child to have excessive anteversion compared with an average child of the same age. This excessive anteversion produces a relative increase in internal femoral rotation, since the hip joint seeks to center itself regardless of the rotational profile of the femur. The clinical manifestation of this increased internal rotation and decreased external rotation of the hip is in-toeing during walking.

![]() Figure 10–23. The angle of anteversion describes the inclination of the femoral neck forward of (anterior to) the frontal plane.
Figure 10–23. The angle of anteversion describes the inclination of the femoral neck forward of (anterior to) the frontal plane.
Observation of the walking child discloses internal rotation of the entire femur by the medial position of the patella. Although parents may consider this pigeon-toed gait unsightly, increased femoral anteversion is a normal variant that has no effect on function.
Increased femoral anteversion gradually decreases, with improvement in in-toeing, until 9–11 years of age. Subsequently, persistent in-toeing in the adult becomes more likely. Increased femoral anteversion requires no treatment.
![]() Internal Tibial Torsion
Internal Tibial Torsion
Some infants are born with a relatively dramatic internal twisting (torsion) of the tibia that makes the foot and ankle appear markedly rotated inward, relative to the axis of the knee. This internal tibial torsion is usually bilateral, frequently familial, and inevitably a normal variant in the wide torsional range seen in infants.
Internal tibial torsion can be clinically measured by comparing the bimalleolar axis (imaginary line connecting the medial and lateral malleoli of the ankle) with the frontal plane of the knee as determined by the position of the patella.
Torsion of 30–40 degrees is not uncommon in the newborn. When the child starts to walk, torsion can cause significant in-toeing, which, in turn, causes excessive tripping.
With growth, internal tibial torsion spontaneously resolves, and normal foot position and walking eventually occur. Some children improve by 24 months of age but may require up to 4 years for full resolution of the torsion. Internal tibial torsion requires no treatment. There is no scientific evidence that braces or shoe modifications alter the natural correction of the deformity.
![]() Metatarsus Adductus
Metatarsus Adductus
Metatarsus adductus may cause apparent in-toeing in the young child, leading to its inclusion as a torsional deformity. It is described in the previous section on the foot (Table 10–7).
Table 10–7. In-toeing summary.

Staheli LT, Corbett M, Wyss C, King H: Lower-extremity rotational problems in children. Normal values to guide management. J Bone Joint Surg Am 1985;67:39. [PMID: 3968103]
![]() Bowlegs, Knock-Knee, and Genu Varum
Bowlegs, Knock-Knee, and Genu Varum
Many infants have bilateral symmetric bowing of the legs, which may persist in the first 1–2 years of walking before developing into an exaggerated knock-kneed condition. The knock-knee is most dramatic at 3–6 years of age when it is known as physiologic genu valgum. At this time, the anatomic angle may be as high as 15–20 degrees of valgus. The genu valgum then gradually remodels spontaneously to the adult average value of 5–7 degrees of valgus.
Bowing of the legs in infants and excessive valgus of the knees in children 6 years of age are normal phenomena that require no treatment, although parents may have to be reassured that the condition is benign. The rare case of bowing that persists beyond 3 years of age may require further evaluation or treatment. Following are disorders that cause bowing.
A. Internal Tibial Torsion
Internal tibial torsion may masquerade as bowing when the child walks with the feet forward and the knees rotated externally rather than internally. As the laterally facing knees flex, they give the appearance of bowlegs. Careful physical examination discloses internal tibial torsion, which spontaneously resolves by 4 years of age. As the torsion corrects, the apparent bowlegs disappear.
B. Blount Disease
Also known as tibia vara, Blount disease is a poorly understood loss of medial tibial physeal growth that causes progressive bowing of the leg (Figure 10–24). It may occur as early as 3 years of age and can be bilateral or unilateral. If unilateral, the condition may be suspected earlier because it is obvious by comparison with the other leg. Excessive loading of the knee by early walking in heavy children with physiologic bowing of the legs may contribute to the development of Blount disease, but this is not proven. It occurs in all racial groups but is particularly common in blacks and Hispanic children.

![]() Figure 10–24. The Langenskiöld diagrammatic classification of radiographic changes in Blount disease (infantile tibia vara). The higher grades are associated with permanent closure of the medial tibial physis, which leads to progressive varus and internal rotation deformity with growth.
Figure 10–24. The Langenskiöld diagrammatic classification of radiographic changes in Blount disease (infantile tibia vara). The higher grades are associated with permanent closure of the medial tibial physis, which leads to progressive varus and internal rotation deformity with growth.
Diagnosis of Blount disease is based on radiographic evidence of decreased medial tibial physeal growth. Later, the medial articular surface is distorted and the medial physis fuses. This causes progressive angular deformity to develop as the lateral growth plate continues elongating while the medial side is tethered.
Spontaneous resolution of adolescent tibia vara is uncommon but can occur in mild cases. Although some orthopedists recommend bracing to assist the process, there is no consensus that this is necessary or effective.
Severe or progressive cases of Blount disease require surgical correction by tibial osteotomy to regain the normal physiologic valgus angle of the knee. Surgery reduces the physiologic load on the medial tibial plateau and may allow normal growth. Slight overcorrection of the bowing often ensures load reduction, and the resulting valgus slowly resolves as the child grows.
Surgical treatment early in life is now popular, and many orthopedists recommend osteotomy after 3–4 years of age if radiographic changes are present. In early cases, surgical correction may cause reversal before there is permanent growth arrest that would require physeal bridge resection and/or repeated osteotomies. Once physeal bridging occurs, however, there is no alternative to repeated surgical correction of angular deformity and leg-length inequality until growth ceases at maturity. Surgical elevation of the medial tibial plateau is a procedure that is occasionally necessary in individuals with early-onset Blount disease but is not indicated for individuals with late-onset Blount disease. Distal femoral varus deformity is commonly present and must be addressed as well. Controlled studies of the issues involved in treatment of Blount disease by bracing and surgery are not available.
C. Rickets
Metabolic disorders of calcium intake (nutritional rickets) can decrease the rate of calcification and ossification of physeal cartilage, causing the development of softer bones that are prone to bowing. Vitamin and calcium dietary supplements have virtually eliminated nutritional rickets in the United States. Hypophosphatemic rickets was discussed earlier in the section on metabolic bone disease.
Jones JK, Gill L, John M, Goddard M, Hambleton IR: Outcome analysis of surgery for Blount disease. J Pediatr Orthop 2009; 29:730. [PMID: 20104154]
Rab GT: Oblique tibial osteotomy revisited. J Child Orthop 2010; 4:169. [PMID: 20234769]
![]() Tibial Bowing and Pseudarthrosis
Tibial Bowing and Pseudarthrosis
The tibia has a propensity to exhibit congenital angular deformities (bowing of the tibial shaft), which, although rare, are significant. The direction of the bowing is important in both diagnosis and prognosis and usually detectable at birth. Bowing direction is described by the apex of the bow, not the direction of displacement of the distal part (Figure 10–25).

![]() Figure 10–25. The major types of tibial bowing. A: Posteromedial bowing. The angulation spontaneously corrects, but with limb-length inequality. B: Anterolateral bowing. This disorder eventually progresses to spontaneous tibial fracture with resistant pseudarthrosis (see text).
Figure 10–25. The major types of tibial bowing. A: Posteromedial bowing. The angulation spontaneously corrects, but with limb-length inequality. B: Anterolateral bowing. This disorder eventually progresses to spontaneous tibial fracture with resistant pseudarthrosis (see text).
A. Congenital Posteromedial Bowing of Tibia
Congenital posteromedial bowing of the tibia is a unilateral birth deformity of the distal fourth of the tibia. The apex of the bow is posteromedial, and often a skin dimple is present over the area. Because of the angle of bowing (often approximately 50 degrees) and the proximity to the ankle joint, the clinical appearance often mimics calcaneovalgus foot. The spatial position of the ankle joint, however, not the foot itself, is responsible for the deformity. Radiographs of posteromedial bowing disclose the curvature of the distal tibia, often with sclerosis in the underlying section of bone.
Despite its dramatic appearance, posteromedial tibial bowing corrects spontaneously in all cases. Some recommend casting to bring the dorsiflexed foot down to plantigrade position, but because the actual deformity is not related to the foot, this advice is not logical: Patients who are never casted resolve as quickly as those who are.
The tibial curvature remodels enough by 3 years of age that the limb appears cosmetically straight, although some bowing may be evident on radiograph for 5–8 years. All patients with posteromedial bowing are left with a leg-length discrepancy. At maturity, the involved limb is relatively as much shorter than the longer limb as it was at birth, usually in the range of 4 cm. The residual limb-length discrepancy presents the greatest challenge but can usually be handled with limb-lengthening techniques. Therefore, although the angular deformity needs no treatment, long-term follow-up and treatment of limb inequality are necessary.
B. Congenital Anterolateral Bowing of Tibia and Congenital Pseudarthrosis of the Tibia
Congenital anterolateral bowing of the tibia and congenital pseudarthrosis of the tibia represent the other extreme of tibial bowing. For reasons not understood, anterolateral bowing in the tibia and fibula is associated with inevitable progressive sclerosis and atrophy of the tibial shaft underlying the deformity. The ultimate fate of this atrophic abnormal bone is spontaneous fracture, which does not heal readily as most fractures in children do (ie, pseudarthrosis). Some children with this condition are born with a tibial fracture, whereas others simply have anterolateral bowing and sclerosis at birth, with fractures occurring up to 8–10 years of age. In approximately 50% of cases, confirmed neurofibromatosis is present.
All children with variations of this disorder require treatment. Because the prognosis is worse for those whose fracture occurs at a younger age, treatment methods vary. If anterolateral bowing is present but fracture has not occurred, protective bracing may be helpful. The fracture may heal in children whose first fracture occurs at 8 years or older, using prolonged casting or surgical bone grafting (with or without internal fixation).
Bone grafting in children whose fracture occurs before 3 years of age almost always fails, although repeated attempts to graft show some success.
The dismal results with conventional treatment of congenital pseudarthrosis of the tibia in younger patients prompted some surgeons to try innovative treatments. Electrical stimulation, free microvascular transfer of the fibula, and Ilizarov transport of normal bone to the defect are all reported to improve the success of treatment. So much surgery may be required to achieve a functional result, however, that many patients eventually undergo amputation to achieve rapid return to the normal functional activities of childhood.
Feldman DS, Jordan C, Fonseca L: Orthopaedic manifestations of neurofibromatosis type 1. J Am Acad Orthop Surg 2010;18:346. [PMID: 20511440]
Tudisco C, Bollini G, Dungl P, et al: Functional results at the end of skeletal growth in 30 patients affected by congenital pseudarthrosis of the tibia. J Pediatr Orthop B 2000;9:94. [PMID: 10868385]
Vander Have KL, Hensinger RN, Caird M, Johnston C, Farley FA: Congenital pseudarthrosis of the tibia. J Am Acad Orthop Surg 2008;16:228. [PMID: 18390485]
KNEE DISORDERS
1. Discoid Meniscus
The normal menisci of the knee are semilunar in shape and wedge shaped in cross section. They deepen the flat tibial articular surface to allow cupping of the rounded femoral condyles. The medial meniscus is longer and narrower than the lateral meniscus.
Rarely, the lateral meniscus remains congenitally round (or discoid) instead of acquiring its normal semilunar shape (Figure 10–26). This reduces its cupping function and may cause some instability of either the lateral compartment of the knee or of the lateral meniscus itself.

![]() Figure 10–26. A: Normal lateral meniscus. B: Discoid lateral meniscus, which may cause clicking, effusion, or pain.
Figure 10–26. A: Normal lateral meniscus. B: Discoid lateral meniscus, which may cause clicking, effusion, or pain.
![]() Clinical Findings
Clinical Findings
The classic physical finding of discoid meniscus is loud clicking over the lateral meniscus during flexion and extension of the knee. This clicking is usually painless but may be accompanied by aching or effusion. Physical exam may demonstrate an extension block. Discoid meniscus may be suspected on radiograph by widening of the lateral knee compartment, a subtle increase in subchondral sclerosis laterally, and convexity of the lateral tibial articular surface. Confirmation is attained on arthrography or MRI. The abnormal mechanical function of discoid lateral meniscus makes it susceptible to tears, particularly in children older than 10 years.
![]() Treatment
Treatment
In the past, symptomatic discoid menisci were treated by total lateral meniscectomy, but the resultant late degenerative knee changes dictate a far more conservative course. Current practice is to avoid treatment unless symptoms are significant and disabling. If treatment is required, the safest approach appears to be arthroscopic removal of the central portion of the discoid shape, thus sculpting the lateral meniscus into a roughly semilunar form.
Good CR, Green DW, Griffith MH, Valen AW, Widmann RF, Rodeo SA: Arthroscopic treatment of symptomatic discoid meniscus in children: classification, technique, and results. Arthroscopy 2007;23:157. [PMID: 17276223]
Kramer DE, Micheli LJ: Meniscal tears and discoid meniscus in children: diagnosis and treatment. J Am Acad Orthop Surg 2009;17:698. [PMID: 19880680]
2. Chondromalacia and Internal Derangements of the Knee
Patellar chondromalacia and patellar subluxation are common in active adolescents, particularly in females who have small patellas and a slight exaggeration of knee valgus and quadriceps (Q) angle. Meniscal and ligament injuries are managed as in the adult, although these injuries are not as common in children.
A somewhat more conservative approach to suspect internal knee derangements is warranted in most children. The diagnostic accuracy of both physical exam and complex imaging studies (such as MRI) is surprisingly low in children. False-positive MRIs are particularly typical in children.
These disorders are described in Chapter 2, “Musculoskeletal Trauma Surgery,” and Chapter 3, “Sports Medicine.”
3. Osteochondritis Dissecans
Osteochondritis dissecans is a poorly understood disorder most commonly of the distal femoral condyle ossification center, although other joints (talus, elbow) can be affected. A portion of the joint surface softens, shears, or separates through the articular cartilage and underlying bone (Figure 10–27). This disorder is common, but not exclusive, in children 8–14 years of age; however, it is an infrequent problem in the adult.

![]() Figure 10–27. Various forms of the osteochondritis dissecans lesion found in children. A: Defect in ossification center without cartilage defect. B: Lesion with a hinged flap. C: Complete separation of bone and cartilage, which can lead to loose body in the knee joint.
Figure 10–27. Various forms of the osteochondritis dissecans lesion found in children. A: Defect in ossification center without cartilage defect. B: Lesion with a hinged flap. C: Complete separation of bone and cartilage, which can lead to loose body in the knee joint.
The disease appears to be caused by a combination of two factors: (1) mechanical shearing or injury from activity and (2) femoral condyle susceptibility (fragility) resulting from immature ossification of the femoral condyle (which can be quite irregular in children). The importance of each factor depends on age. Athletic trauma seems more important in older children and adults, whereas in younger children, ossification defects render the femoral condyle more susceptible to minor repetitive injury.
![]() Clinical Findings
Clinical Findings
A. Symptoms and Signs
Symptoms and physical findings can be highly variable. Younger children may have an asymptomatic radiographic abnormality of condylar fragmentation or may simply have a vague aching after strenuous activity. Older children and adults may have pain, effusion, and locking or catching if the affected fragment actually separates and becomes a loose body in the knee joint.
B. Imaging Studies
Plain radiographs show an irregular fragment of the surface that is usually sclerotic but may be osteopenic and is usually on the lateral side of the medial condyle. It is often necessary to obtain tangential views of the condyle such as notch views. Occasionally, the defect is visible only on lateral projection. Contralateral comparison views should always be obtained. So-called ossification defects that mimic osteochondritis dissecans may be normal ossification fronts, seen to be bilateral and symmetric.
In children older than 11–12 years, MRI or arthrography is used to determine whether the underlying bone alone is involved or whether there is an actual separation of overlying cartilage. Although these studies are helpful in refining treatment strategy in this age group, they are seldom useful in younger children.
![]() Treatment
Treatment
Young children with asymptomatic osteochondritis disse-cans need not be treated because most of these lesions heal spontaneously. In preadolescents with symptoms or with large lesions seen on radiographs, simple immobilization with either a knee immobilizer or cylinder cast for 6 weeks frequently heals the defect and eliminates symptoms.
Sometimes immobilization is not effective, though. If the lesion is large and accompanied by cartilage separation or displacement, or if the skeleton has reached maturity, treatment may be the same as in the adult. This includes arthroscopic debridement and stabilization of the loose fragment using pins for internal fixation. Excision is less likely to result in a good result. The presence of open physes may necessitate modifications of standard adult techniques.
Gudas R, Simonaityte R, Cekanauskas E, Tamosi![]() nas R: A prospective, randomized clinical study of osteochondral autologous transplantation versus microfracture for the treatment of osteochondritis dissecans in the knee joint in children. J Pediatr Orthop 2009;29:741. [PMID: 20104156]
nas R: A prospective, randomized clinical study of osteochondral autologous transplantation versus microfracture for the treatment of osteochondritis dissecans in the knee joint in children. J Pediatr Orthop 2009;29:741. [PMID: 20104156]
Kocher MS, DiCanzio J, Zurakowski D, Micheli LJ: Diagnostic performance of clinical examination and selective magnetic resonance imaging in the evaluation of intraarticular knee disorders in children and adolescents. Am J Sports Med 2001;29:292. [PMID: 11394597]
4. Ligament and Epiphyseal Injury
Children who have not reached skeletal maturity have far fewer major ligament injuries of the knee than do older children and adults. Smaller children tend to participate in lower impact activities and sports, and their lack of muscle bulk (which increases during adolescence) limits body acceleration and the force of collision. In addition, ligaments are relatively strong in the immature skeleton compared with bone or cartilaginous physes. Therefore, physeal fractures and bony avulsions of ligament attachments are more likely than traumatic ruptures of the ligaments themselves.
Residual instability may occur in the child’s knee after varus or valgus injury. In the adult, such instability is considered clinical evidence of ligament injury. In children, however, the physis rather than the ligament may be the site of failure. Instability can be caused by a physeal fracture that hinges open rather than the joint opening (Figure 10–28). It is usually clinically obvious that fracture is present, although stress radiographs may help in questionable cases.

![]() Figure 10–28. Stress radiograph of the unstable knee in an immature patient may reveal ligament rupture (A) or separation of the femoral physis (B).
Figure 10–28. Stress radiograph of the unstable knee in an immature patient may reveal ligament rupture (A) or separation of the femoral physis (B).
Major intraarticular disruptions of the knee joint (meniscal tear or cruciate ligament injury) are rare in children. Detection may be delayed because symptoms may be less severe than in the adult and their presence not given as much weight in the differential diagnosis. Meniscus injury, particularly when peripheral, may lend itself to arthroscopic repair because of the excellent blood supply in children. Anterior cruciate rupture can be difficult to manage surgically in children because the anatomic sites of the tibial or femoral physes limit the options for reattachment. With the exception of cruciate injuries, most childhood knee ligament injuries are treatable by 2–4 weeks of splinting and return to function, as tolerated by pain. Physical therapy is rarely necessary in children younger than 15 years. A review of the major signs, symptoms, diagnostic procedures, and treatment options can be found in Chapter 3, “Sports Medicine.”
![]() Differential Diagnosis
Differential Diagnosis
Not all effusions in the knee are traumatic, particularly in younger children. Because children at play are always suffering minor injuries, a history of injury may be inaccurate. The physician must remember to consider septic arthritis and pauciarticular juvenile rheumatoid arthritis in the differential diagnosis of effusion.
Beasley LS, Chudik SC: Anterior cruciate ligament injury in children: update of current treatment options. Curr Opin Pediatr 2003;15:45. [PMID: 12544271]
Luhmann SJ: Acute traumatic knee effusions in children and adolescents. J Pediatr Orthop 2003;23:199. [PMID: 12649021]
OSGOOD-SCHLATTER DISEASE
The proximal tibial physis contains a transverse component that contributes to longitudinal growth and an anterior tongue that contains the attachment of the patellar tendon. In preadolescent and adolescent children (usually boys), the distal tip of this tongue may undergo fragmentation from chronic tensile stress and enlargement from the resultant hyperemic response, which is known as Osgood-Schlatter disease. As the tibial tubercle becomes increasingly prominent, a painful bursa can form over it.
![]() Clinical Findings
Clinical Findings
Symptoms vary from mild aching at the tubercle to severe pain with patellar function and exaggerated bursal tenderness. Radiographs of the lateral proximal tibia show the characteristic fragmentation (Figure 10–29).

![]() Figure 10–29. Osgood-Schlatter disease. The radiographs would show characteristic fragmentation of the tibial tubercle apophysis, similar to diagram.
Figure 10–29. Osgood-Schlatter disease. The radiographs would show characteristic fragmentation of the tibial tubercle apophysis, similar to diagram.
![]() Treatment
Treatment
Treatment is symptomatic, including analgesics, knee pads to avert direct pressure, quadriceps stretching, avoidance of sports activities, and brief casting or splinting for painful cases. The disorder resolves spontaneously when the physis closes at skeletal maturity. No evidence indicates that physical activity within the limits of pain is harmful to the child with Osgood-Schlatter disease.
Adirim TA, Cheng TL: Overview of injuries in the young athlete. Sports Med 2003;33:75. [PMID: 12477379]
Krause BL, Williams JP, Catterall A: Natural history of OsgoodSchlatter disease. J Pediatr Orthop 1990;10:65. [PMID: 2298897]
SPINAL CURVATURE
Spinal curvature may occur in any age group and present with variable findings. Curvatures may be idiopathic, congenital, or accompany a wide variety of neuromuscular disorders, tumors, and infections. Curvatures may be small and nonprogressive or may worsen and require aggressive treatment. Sometimes, spinal curvature is the first clue to important underlying disease. Figure 10–30 shows the different types of spinal deformities.

![]() Figure 10–30. Definitions of spinal deformities. A: Scoliosis. B: Kyphosis. C: Lordosis. Frequently, a combination of deformities occurs in individual patients (ie, kyphoscoliosis).
Figure 10–30. Definitions of spinal deformities. A: Scoliosis. B: Kyphosis. C: Lordosis. Frequently, a combination of deformities occurs in individual patients (ie, kyphoscoliosis).
![]() Types of Curvatures
Types of Curvatures
A. Scoliosis
Scoliosis is a lateral spinal curvature in the frontal plane, best appreciated by physical examination from the patient’s back and by anteroposterior radiographs. Curvatures, which may be single or multiple, are described by the direction of their convexity. In a flexible spine, the presence of a single (more rigid) curvature can lead to physiologic compensatory curvatures in the opposite direction, above and below the primary curvature. True scoliosis always includes a rotational component that may not be fully appreciated on radiograph and generally includes a lordotic component as well (see section on lordosis). Surprisingly, lateral curvature is often undetected externally. The rotation of vertebrae that accompanies scoliosis is the physical feature that allows clinical detection.
B. Kyphosis
Kyphosis is a forward (flexed) curvature of the spine in the sagittal plane, best appreciated from the side and by lateral radiographs. If kyphosis is acutely angular, a posterior prominence called a gibbus may be evident in the sagittal plane.
C. Lordosis
Lordosis is a hyperextension deformity of the spine, most common in the lumbar spine but also often accompanying scoliosis. Lumbar lordosis may be secondary to flexion contracture of the hip.
![]() Detection of Curvature
Detection of Curvature
Although spinal curvatures may be detected first during routine radiograph, most lesions are best diagnosed by physical examination. Spinal examination should proceed according to the following specific protocol:
1. Place the patient in the standing position (Figure 10–31).

![]() Figure 10–31. Examination of the spine for deformity is best carried out by observing for asymmetry and deformity as the patient bends forward (see text).
Figure 10–31. Examination of the spine for deformity is best carried out by observing for asymmetry and deformity as the patient bends forward (see text).
2. Check the level of the pelvis and look for obvious asymmetry of the rib, scapula, neck, and shoulder height (leg-length inequality can cause apparent scoliosis, which disappears when the short leg is elevated on blocks).
3. Level the pelvis by seating the child on a firm surface if the pelvis cannot be leveled while standing. This is the case in children with hip contracture from neuromuscular disease.
4. Have the child bend forward, carefully noting any asymmetric prominence of the lumbar paraspinous muscle, rib cage, or scapula, which suggests the rotational portion of scoliosis. The magnitude of asymmetry corresponds to the severity of the curvature, with convexity of the curvature directed toward the most prominent side.
5. From the side, check for prominence of the spine that might indicate kyphosis, both in the upright and forward-bending position.
6. Perform a careful neurologic exam, including upper extremity reflexes and abdominal reflexes in addition to thorough lower extremity neurologic examination.
7. Use radiographs to assess type, severity, and location of the curvature and to look for underlying lesions. Because primary scoliosis and kyphosis curvatures are always stiffer than uninvolved spine segments, bending radiographs may reveal which curvatures are “structural” and which are more flexible compensations (secondary curvature). The Cobb method is usually used to measure curvatures (Figure 10–32). The degree of tilt between the most affected vertebral endplates describes curvature magnitude.
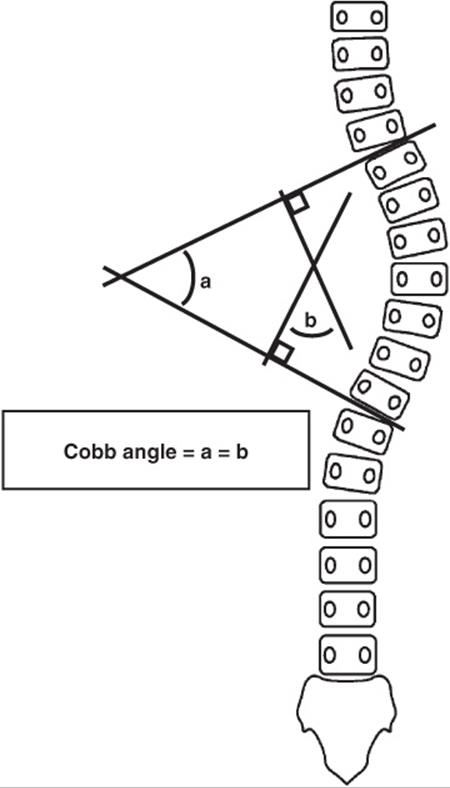
![]() Figure 10–32. The Cobb method of measurement is commonly used to assess spinal curvature. It measures the angle between the far (top and bottom) endplates of the most inclined vertebrae. To allow the measurement lines to fit on the radiograph, lines at 90-degree angles to the endplates are often drawn, and their relative angles measured. Geometrically, these angles are the same.
Figure 10–32. The Cobb method of measurement is commonly used to assess spinal curvature. It measures the angle between the far (top and bottom) endplates of the most inclined vertebrae. To allow the measurement lines to fit on the radiograph, lines at 90-degree angles to the endplates are often drawn, and their relative angles measured. Geometrically, these angles are the same.
![]() Scoliosis
Scoliosis
A. Idiopathic Scoliosis
Idiopathic scoliosis has no apparent underlying cause and can be separated into adolescent (>10 years), juvenile (3–10 years), and infantile (<3 years). Adolescent idiopathic scoliosis accounts for 80% of all idiopathic scoliosis and is found most commonly in early adolescent girls, although it can be found in either gender at any age. There is typically a convex curvature to the right in the thoracic portion of the spine (right thoracic curve pattern). Patients with atypical curvature patterns, such as left thoracic curves and idiopathic curvature in younger children may require more extensive testing (eg, EMG, MRI) before the cause can be definitively designated idiopathic.
Many idiopathic curvatures progress in magnitude with growth and continue to do so until skeletal maturity. Therefore, the clinician must determine if the curvature is progressing and if the spine is still growing. Radiographs document progression, and observations of the ossification pattern of the iliac crest apophysis (Risser sign) are used to estimate skeletal maturity. This ossification pattern begins laterally at puberty and spreads medially across the ilium, capping and fusing with the bone at maturity. A variety of spinal braces are available to treat progression of idiopathic scoliosis, although there is debate about their actual effectiveness. Progressive curves in children with substantial growth potential (Risser 2), any curve of greater than 30 degrees, or patients with a curve of greater than 20–25 degrees with more than 5 degrees of documented progression should be treated. Children who mature with small curves have no symptoms and no progression in adulthood. Specifically, curves smaller than 35–40 degrees in adults generally do not progress. If a curvature progresses despite adequate bracing, surgery is the treatment of choice. Some curves are too rigid to brace effectively and can only be observed if they are relatively small. Bracing may help with curves up to 40 or 45 degrees, but for curves that exceed this magnitude, bracing is generally ineffective.
Surgery for scoliosis corrects the deformity using metal rods that can be configured to push, pull, distract, or compress portions of the spine with curvature. The involved spinal segments are then fused together using iliac or allograft bone. Typically, a posterior fusion of the laminas and facets is sufficient for many cases of idiopathic scoliosis. Severe cases may also require anterior fusion through the thorax or retroperitoneal space.
In those with juvenile scoliosis with more than a 20-degree Cobb angle, there is about a 20% prevalence of a neurologic abnormality. Therefore, workup in these children should include an MRI of the entire spine.
Lastly, infantile idiopathic scoliosis occurs more commonly in boys, with a 3 to 1 male-to-female ratio. Spinal cord abnormalities have about 20% prevalence, similar to juvenile idiopathic scoliosis. Hip dysplasia and congenital heart disease are also associated with the condition. Spontaneous correction occurs in some individuals. In others, the curves progress, and this can be predicted by the rib vertebral angle difference or the phase of the rib head. Rib overlap of the apical vertebral body or a rib vertebral angle difference of greater than 20 degrees indicates that the curve is likely to progress. Gender, family history, and age at presentation have not been found to be risk factors for progression.
B. Congenital Scoliosis
Congenital scoliosis is caused by malformations of vertebral shape. It does not refer to the age of the patient: Newborns can have idiopathic scoliosis, despite being born with spinal curvatures. Congenital vertebral malformations generally occur in early embryonic life (before 7 weeks) and are thought to represent errors in formation or segmentation of the spinal segments that originate from primitive mesenchymal condensations of embryonic cells (Figure 10–33).

![]() Figure 10–33. Vertebral anomalies of congenital scoliosis. A: Hemivertebra. B: Butterfly vertebra. C: Block vertebra. D: Unilateral unsegmented bar.
Figure 10–33. Vertebral anomalies of congenital scoliosis. A: Hemivertebra. B: Butterfly vertebra. C: Block vertebra. D: Unilateral unsegmented bar.
Curvatures can originate when vertebral parts fail to form (eg, hemivertebrae, wedge vertebrae, butterfly vertebrae) or when embryonic somites fail to segment properly into individual vertebrae (eg, block vertebrae, unilateral unsegmented bar). Because of the embryonic timing of this process, children with congenital scoliosis frequently have abnormalities of other organ systems that form during the same embryonic period. About 60% of patients with congenital anomalies of the spine have other associated findings. The spine develops around the same time as the cardiovascular system, the genitourinary system, and the musculoskeletal system. Around 20% of patients with congenital scoliosis have an associated urologic abnormality. Approximately 25% of patients with congenital scoliosis have an associated cardiac defect. Diagnosis of congenital scoliosis must be followed by a careful cardiac examination and by ultrasound or intravenous pyelography evaluation of the kidneys. Spinal cord abnormalities may be present in as many as 30%, so evaluation of the spinal canal (MRI, EMG) may be required, especially if surgery is contemplated.
Congenital scoliosis may encompass one or many deformed vertebrae, and different types of vertebral abnormalities are often seen in the same patient. Sometimes, two deforming vertebrae “cancel each other out” and no curvature is visible. For this reason, prediction of progression of the scoliosis depends on serial radiographs. If progression occurs, bracing is usually the first treatment, although surgery is indicated if progression is not halted by external means. Curvatures caused by unilateral unsegmented bars have such a strong tendency to progress that they should be treated by surgery as soon as they are detected.
C. Neuromuscular Scoliosis
Neuromuscular scoliosis includes a diverse group of curvature patterns that occur in association with various neuromuscular diseases. The cause varies with the disease. For example, scoliosis in children with cerebral palsy is usually caused by a combination of spasticity (overactivity of muscle) and weakness. Scoliosis in children with muscular dystrophy is the result of severe progressive muscle weakness that eliminates the paraspinous stability of the spinal column. Scoliosis in infants with spina bifida (myelomeningocele) is frequently congenital (see previous discussion), related to loss of posterior elements, or associated with the development of a syrinx (central cystic fluid collection) in the spinal cord, a process similar to hydrocephalus.
Patients with neuromuscular scoliosis often develop curvatures at an early age, when surgical treatment is either impossible or would result in severe stunting of spinal growth. It is common to treat such children by daytime bracing, despite the fact that bracing alone is rarely sufficient to eliminate progression or the need for later surgery. In such cases, some surgeons feel that bracing may slow progression enough to allow additional skeletal growth, and spinal correction and fusion are postponed until puberty.
D. Other Scolioses
Childhood scoliosis can be associated with benign tumors of the spine, usually osteoid osteoma and osteoblastoma. Treatment of the tumor is usually curative, although longstanding lesions may require fusion as well.
Neurofibromatosis is associated with both scoliosis and kyphosis and characteristically leads to short high-grade curvatures requiring surgical treatment. Anterior and posterior spinal fusion is required to achieve correction and fusion in neurofibromatosis.
More than 90% of preadolescent children who sustain a significant spinal cord injury subsequently develop scoliosis. Bracing has not been shown to be effective in the prevention of scoliosis in the preadolescent patient with spinal cord injury.
![]() Kyphosis
Kyphosis
Kyphosis may be congenital, traumatic, or acquired. Some patients with kyphosis need no treatment, whereas others require immediate surgical attention.
A. Postural Kyphosis (Postural Roundback)
Postural kyphosis, a variation of normal posture, is a cosmetic problem. There is no associated underlying disease, and the spine is flexible and capable of hyperextension. Although it may be worrisome to parents, little scientific evidence indicates that it requires, or responds to, treatment.
B. Scheuermann Kyphosis
Scheuermann kyphosis is a disorder of growth of the vertebral endplates that affects adolescents, particularly boys, and produces a progressive rigid forward curvature of the thoracic spine. Less commonly, it involves the lumbar spine, causing decreased lumbar lordosis (relative kyphosis). It is often moderately painful. Radiographs show wedging of vertebral bodies, irregularity of the endplates with radiographic lucent pits known as Schmörl’s nodes, and kyphosis (Figure 10–34).

![]() Figure 10–34. Scheuermann kyphosis is characterized by vertebral wedging, endplate changes, and kyphosis.
Figure 10–34. Scheuermann kyphosis is characterized by vertebral wedging, endplate changes, and kyphosis.
Lumbar Scheuermann kyphosis responds to symptomatic treatment with nonnarcotic pain medications or a supportive lumbar corset. Thoracic involvement with pain or kyphosis of 15–20 degrees greater than normal can be managed with a Milwaukee brace. Brace treatment is usually effective in controlling pain and producing structural correction of the kyphosis, but it is very unpopular with adolescents. Braces may sometimes be used at night only so it will not have to be worn during school hours.
Scheuermann disease is the exception to the general rule that spinal bracing must be done during the active growth phase to improve deformity. Patients as old as 18 years of age show improvement with the Milwaukee brace. Severe cases (40 degrees excessive kyphosis) may require surgical correction by spinal instrumentation and fusion.
C. Congenital Kyphosis
Congenital kyphosis is a rare but important group of diseases, which, like congenital scoliosis, may be caused by failure of formation of vertebrae (hemivertebrae) or failure of embryonic segmentation (anterior unsegmented bar). In most cases, the lesion tends to cause uneven growth, so kyphosis gradually increases as the spine elongates. The risk of neurologic compromise associated with congenital kyphosis is normally secondary to risk of progression. The combination of an anterolateral bar with contralateral quadrant vertebrae has the greatest risk. Bowstringing of the spinal cord over the kyphotic prominence can occur and eventually cause paraplegia. Any progressive congenital kyphosis must be fused to prevent neurologic complications, regardless of the child’s age.
D. Traumatic Kyphosis
Traumatic kyphosis is a traumatic compression of vertebrae that may lead to either cosmetic or symptomatic kyphosis. This may be prevented by early surgical stabilization of high-grade unstable traumatic spinal injuries.
E. Infectious Kyphosis
Infectious kyphosis refers to septic destruction of vertebral bodies, which can lead to severe kyphosis. In particular, tuberculous vertebral osteomyelitis can produce soft-tissue abscess, high-grade kyphosis, a sharp gibbus, and paraplegia. Bacterial infection can mimic this, although dramatic deformities are far more unusual.
Treatment includes antibiotics, surgical debridement and drainage, decompression of the spinal cord, and spinal fusion to prevent further deformity.
![]() Treatment
Treatment
A. Bracing
Bracing can be used to slow progression of spinal curvatures, prevent progression, or improve underlying structural deformities. Many different types of braces are available, each with its own advocates and specific applications (Figure 10–35). When the goal is to provide postural support, slow progression, or postpone (but not prevent) surgery, a polypropylene body jacket, or so-called clamshell brace, may suffice for waking or sitting hours.
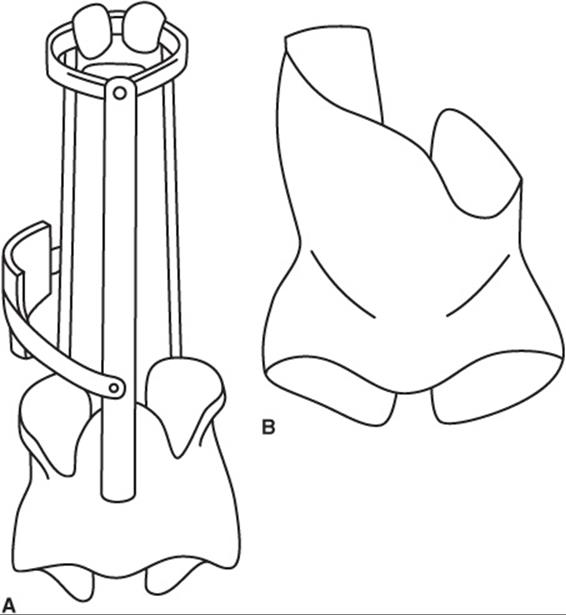
![]() Figure 10–35. Two popular brace styles used for the treatment of spinal deformity are the Milwaukee brace (A) and the low-profile (Boston-type) brace (B).
Figure 10–35. Two popular brace styles used for the treatment of spinal deformity are the Milwaukee brace (A) and the low-profile (Boston-type) brace (B).
Long-term braces designed to arrest progression must be custom molded for the patient, with pads placed to exert appropriate pressure to reduce deformity. Depending on the anatomic level of the curvature, they may be positioned under the arm or may extend to the neck (Milwaukee brace). This type of brace is usually worn 24 hours a day.
All braces must be modified or replaced to accommodate growth. In general, bracing is only effective with flexible curvatures in growing children.
B. Surgical Treatment
Surgical intervention is indicated for curvatures that progress despite adequate conservative treatment (usually bracing). It is also required when spinal compression is imminent (tuberculous kyphosis, congenital kyphosis) or when a curvature is so severe that bracing is impossible and future progression likely.
1. Surgical stages—Surgery involves two separate stages: correction and stabilization. After posterior exposure of the spine, correction is achieved with a variety of mechanical internal fixation devices. These are usually rods with hooks, screws, wires, or other mechanisms to distract, compress, or bend spinal segments. Correction is rarely complete because mechanical and safety considerations limit the force that can be applied. Once correction is obtained, the cortex of spine is removed and bone graft (autograft or allograft) is placed over the raw bone. Subsequently, solid fusion occurs within 6 months, permanently stabilizing the spine (Figure 10–36).

![]() Figure 10–36. Treatment of a scoliotic curve by instrumentation and fusion. Preoperative view (A) and postoperative view (B).
Figure 10–36. Treatment of a scoliotic curve by instrumentation and fusion. Preoperative view (A) and postoperative view (B).
2. Treatment of severe curvatures—For small curvatures, posterior instrumentation and fusion are sufficient. Some large idiopathic curves and neuromuscular curves require anterior release and bone grafting to render enough acute flexibility for curvature correction and enough late stability for dependable fusion. Occasionally, fusion may fail, causing a pseudarthrosis that may be painful or may allow progression of a previously corrected curvature. In this case, fusion must be repeated.
Belmont PJ Jr, Kuklo TR, Taylor KF, et al: Intraspinal anomalies associated with isolated congenital hemivertebrae: the role of routine magnetic resonance imaging. J Bone Joint Surg 2004: 86-A:1704. [PMID: 15292418]
Danielsson AJ, Nachemson AL: Radiologic findings and curve progression 22 years after treatment for adolescent idiopathic scoliosis: comparison of brace and surgical treatment with matching control group of straight individuals. Spine 2001; 26:516. [PMID: 11242379]
Dobbs MB, Lenke LG, Szymanski DA, et al: Prevalence of neural axis abnormalities in patients with infantile idiopathic scoliosis. J Bone Joint Surg Am 2002;84:2230. [PMID: 12473713]
Dobbs MB, Weinstein SL: Infantile and juvenile scoliosis. Orthop Clin North Am 1999;30:331. [PMID: 10393759]
Feldman DS, Jordan C, Fonseca L: Orthopaedic manifestations of neurofibromatosis type 1. J Am Acad Orthop Surg 2010;18:346. [PMID: 20511440]
Nakahara D, Yonezawa I, Kobanawa K, et al: Magnetic resonance imaging evaluation of patient with idiopathic scoliosis: a prospective study of four hundred seventy-two outpatients. Spine 2011;36:E482. [PMID: 20479697]
Negrini S, Negrini F, Fusco C, Zaina F: Idiopathic scoliosis patients with curves more than 45 Cobb degrees refusing surgery can be effectively treated through bracing with curve improvements. Spine J2011;11:369. [PMID: 21292562]
Richards BS, Vitale MG: Screening for idiopathic scoliosis in adolescents. An information statement. J Bone Joint Surg Am 2008;90:195. [PMID: 18171974]
Suh SW, Modi HN, Yang JH, Hong JY: Idiopathic scoliosis in Korean schoolchildren: a prospective screening study of over 1 million children. Eur Spine J 2011;20:1087. [PMID: 21274729]
Ueno M, Takaso M, Nakazawa T, et al: A 5-year epidemiological study on the prevalence rate of idiopathic scoliosis in Tokyo: school screening of more than 250,000 children. J Orthop Sci 2011;16:1. [PMID: 21293892]
NEUROMUSCULAR DISORDERS
![]() Essentials of Diagnosis
Essentials of Diagnosis
• Neuromuscular diseases may cause significant deformities (especially of feet, hips, and spine) due to muscle imbalance during growth.
• There is considerable overlap in clinical appearance associated with different diagnoses, so accurate assessment is essential.
• Treatment should be influenced by function as well as deformity.
Because muscle weakness or imbalance changes the underlying structure of a growing skeleton, neuromuscular diseases of children often require orthopedic evaluation. Treatment may be required to reverse skeletal deformity and contracture or to effect functional improvement.
Many childhood neuromuscular diseases require coordinating the services of the pediatrician, neurologist, radiologist, physiatrist, therapist, educator, social worker, nurse, and parent.
1. Cerebral Palsy
Cerebral palsy is a static encephalopathy in a growing child. Although it is often birth related, the term also includes childhood head injury, stroke, metabolic brain conditions, and degenerative neurologic conditions.
The challenges to physicians evaluating cerebral palsy are making an accurate diagnosis and detecting correctable conditions. It is essential that functional evaluation of the child’s condition take into account the need for education, communication, socialization, and mobility.
![]() Types of Cerebral Palsy
Types of Cerebral Palsy
The hallmark of most cases of cerebral palsy is alteration in motor tone (spasticity or dystonia). Spasticity is increased tone associated with stretching of muscle; dystonia is present without changing muscle length. Diagnosis of spasticity can be direct (increased tone, increased deep tendon reflexes, clasp-knife rigidity, and clonus) or inferred (shortening of muscles, contractures of joints, joint dislocations, and scoliosis). Dystonia can be confused with spasticity, but it does not generally lead to contractures.
A. Hemiplegia
Hemiplegia is spasticity involving only one side of the body. Most hemiplegia involves the pyramidal tract, especially at the cerebral cortex. It may be mild or severe and typically is more pronounced in the distal skeleton (hand and foot-ankle). Hemiplegia is usually caused by congenital loss of portions of the parietal, contralateral cerebral cortex. This loss may reflect vascular insufficiency, trauma, or porencephalic cysts.
Many patients with hemiplegia have normal development and intelligence. Children with hemiplegia frequently walk at a normal age, although sometimes with marked posturing of the involved side. Right hemiplegia (left cerebral cortex) may involve the Broca area and thus cause speech deficits. Because sensory and motor cortex areas are contiguous, hemiplegia is strongly associated with abnormalities of sensation and proprioception in the affected limbs, and particularly in the hand. This may prove more disabling than the spasticity because a child may not appreciate an insensate limb as part of overall body image.
B. Diplegia
Diplegia, or diplegic cerebral palsy, is an encephalopathy usually associated with prematurity. It is characterized by relatively symmetric involvement of the lower extremities and lesser involvement of the upper extremities. Prematurity is often accompanied by intracerebral hemorrhage and periventricular leukomalacia, which lead to edema and necrosis in the region of the trigone. This involvement of the pyramidal tract and associated basal ganglia is the main cause of diplegia.
Most diplegic children exhibit mixed patterns of spasticity with a variety of less obvious neurologic symptoms, including ataxia, rigidity, and athetosis (dystonia). Many have normal intelligence (if the cortex is spared) but may suffer developmental delays caused by damage to associative fibers in the brain. Although they may initially be hypotonic (“floppy”), most diplegic patients develop high tone (spasticity and/or dystonic rigidity) by 12–18 months of age.
Diplegia is relatively symmetric and usually more severe in the lower extremities. Many children with diplegia eventually walk, exhibiting a crouching gait characterized by flexed, internally rotated hips, flexed knees, and plantarflexed ankles.
C. Quadriplegia
Quadriplegia (total body involvement) often occurs in children who suffer birth asphyxia, metabolic encephalopathy, or encephalitis. Severe spasticity, seizures, mental retardation, joint contractures, and scoliosis are typical but not always individually present in this type of cerebral palsy. Children with quadriplegia are particularly susceptible to spontaneous hip dislocations (because of hip muscle imbalance) and high-grade scoliosis. Both of these conditions interfere with sitting and may require surgery. Most quadriplegic patients require wheelchair assistance and do not walk.
D. Mixed Neurologic Involvement
Mixed neurologic involvement of extrapyramidal portions of the brain can cause athetosis, dystonia, ballismus, and ataxia. Many children with cerebral palsy exhibit subtle signs of some of these disorders, in addition to spasticity. In some children, one of these signs may predominate, but spasticity is absent. In general, prognosis varies with the anatomy of involvement.
![]() Treatment
Treatment
Before treating cerebral palsy, specific goals should be set for the patient. Although many important goals are not orthopedic, the surgeon may help the patient achieve them. Increased mobility, for instance, may facilitate achieving a variety of nonorthopedic goals. Especially urgent are the patient’s ability to communicate, move independently, and socialize. Orthopedic treatment may improve sitting position in the wheelchair or improve walking by releasing muscles or joints.
Many children benefit from physical or occupational therapy during the first few years of life. Although the exact role of such therapy in cerebral palsy remains undefined, therapists often help parents and children deal more effectively with the complex problems presented by the disease. Therapists also help parents and children set optimistic and realistic goals for the future.
Bracing or surgery may be required to control effects of spasticity on individual joints and to decrease spasticity, correct dislocation or contracture, or control scoliosis. Surgery is ineffective in the case of extrapyramidal neurologic symptoms. A variety of nonorthopedic treatments are also used for cerebral palsy. Selective dorsal rhizotomy, a neurosurgical procedure to cut a portion of the posterior roots of the lumbar spinal cord, may reduce spasticity in selected patients by interrupting the reflex arc. Botulinum toxin injection (or phenol injection) into the motor endplate region of a muscle temporarily interrupts the myoneural junction, relaxing a spastic muscle for several months and allowing therapy or other evaluation. Oral baclofen can reduce overall spasticity. Intrathecal baclofen, delivered by a subcutaneous pump, may offer relaxation of troublesome lower extremity muscle tension in both dystonic and spastic patients.
Hip subluxation is common in quadriplegia, and pelvic radiographs in young quadriplegic patients are needed to detect early, reversible involvement. Subluxation may be treated in children younger than 3 years by adductor muscle release, which improves abduction. Rarely, the anterior obturator nerve (which innervates the adductor longus muscle) is resected to weaken the adductors. In older children, bony reconstruction by varus-derotation osteotomy and acetabular reorientation or supplementation may be necessary to correct the bone malformation that results from the force of spastic muscles on the growing skeleton. Children who develop hip subluxation often develop scoliosis as well (see section on scoliosis).
A. Adductor Release
Adductor release may be done as an open procedure (usually by myotomy or transverse sectioning of the adductor longus and a portion of the adductor brevis) or by percutaneous adductor tenotomy (section of the tendon origin of the adductor longus at the pelvis). The exact technique and amount of release is dictated by the severity of contracture and other factors. When done for hip subluxation, adductor release is most effective before 3 years of age. Release should be sufficient to allow hip abduction of 70–80 degrees on the operating table. When frank subluxation is present, some surgeons perform an anterior obturator neurectomy in addition to the adductor myotomy. This open procedure removes a segment of the obturator nerve that supplies the released adductor longus muscle, so the muscle remains loose after spontaneously reattaching after surgery.
Obturator neurectomy must be used carefully because it can cause excessive weakening of the adductors and, subsequently, late hip abduction contracture. After each of these procedures, the patient is casted in abduction for 3–4 weeks to allow muscle healing in the new elongated position.
Dynamic spasticity or joint contracture (the result of chronic spasticity) can interfere with walking in children with hemiplegia or diplegia. This may be treated by bracing involved joints in a functional position or by surgical lengthening of the muscle–tendon unit. Such muscle releases can be done by complete tenotomy, tendon Z-lengthening (common at the Achilles tendon), or lengthening of the aponeurosis of a muscle, which is often done for the iliopsoas or hamstrings (Figure 10–37).

![]() Figure 10–37. Schematic representation of surgical options for muscle release or lengthening in cerebral palsy. A: Myotomy; B: tenotomy; C: aponeurotomy.
Figure 10–37. Schematic representation of surgical options for muscle release or lengthening in cerebral palsy. A: Myotomy; B: tenotomy; C: aponeurotomy.
It is convenient to combine multiple procedures for children with cerebral palsy. For example, a typical hemiplegic with a tiptoe (equinus) gait may benefit from lengthening the Achilles tendon to make the foot plantargrade. A typical diplegic patient with a crouching gait may benefit from hip flexor, hamstring, and Achilles tendon lengthenings performed bilaterally during a single operation. The exact timing and extent of surgery are controversial among experts in cerebral palsy. Three-dimensional computerized gait analysis, performed in motion laboratories, can guide the surgeon.
B. Muscle Release for Dynamic Deformity
Muscle releases for dynamic deformity may be done in several ways, depending on the specific muscle, the presence of contracture, and the surgeon’s preference. The goal is to weaken spastic muscles to reduce their abnormal influence while not lengthening them so much that the opposite deformity occurs. The more common procedures are described here.
1. Achilles tendon lengthening—Achilles tendon lengthening is usually done by Z-lengthening of the distal tendon. Cuts for Z-lengthening can be either open or percutaneous. The ankle is carefully dorsiflexed just beyond neutral to allow the tendon fibers to slide into an elongated position. The surgeon must avoid overlengthening (a matter of judgment) because an excessively weakened gastrocnemiussoleus group hinders walking and can actually encourage a deeper crouching gait.
2. Gastrocnemius lengthening—Gastrocnemius lengthening is required in patients whose gastrocnemius is considerably more spastic than the soleus. In such cases, ankle dorsiflexion is limited and ankle clonus occurs when the knee is extended, but free dorsiflexion occurs when the knee is flexed. In such patients, the gastrocnemius alone may be released by approaching the musculotendinous junction in the calf and sectioning the aponeurosis or by release of the insertion of the gastrocnemius where it attaches to the soleus and Achilles tendon. This effectively recesses the muscle, selectively weakening it while retaining soleus strength for pushoff during walking.
3. Hamstring lengthening—Hamstring lengthening is indicated when the hamstrings are tight (limited straight-leg raising) and knee flexion is persistent during the stance phase of gait (crouching gait). Usually, the distal medial and lateral hamstrings are released, but procedures vary widely among surgeons. On the medial side, the gracilis and semitendinosus tendons are usually Z-lengthened or tenotomized (transversely released). The semimembranosus is lengthened by transverse incision of its aponeurosis, which allows the interior muscle fibers to stretch and lengthen. Laterally, both heads of the biceps femoris can be managed by aponeurotic lengthening as well. The procedure must be done carefully to avoid cutting or stretching the sciatic or peroneal nerves. The leg is splinted or casted in extension for 3–4 weeks to allow soft-tissue healing.
4. Iliopsoas lengthening—The hip flexors (psoas and iliacus) may be released at the insertion of the conjoined tendon into the lesser trochanter, usually done in sitters also undergoing adductor release for spastic hip subluxation. If the child is walking and less weakening of hip flexion is desired, the psoas tendon alone can be sectioned at the level of the pelvic brim, retaining the iliacus portion of the muscle for strength.
Gordon GS, Simkiss DE: A systematic review of the evidence for hip surveillance in children with cerebral palsy. J Bone Joint Surg Br 2006;88:1492. [PMID: 17075096]
Muthusamy K, Chu HY, Friesen RM, Chou PC, Eilert RE, Chang FM: Femoral head resection as a salvage procedure for the severely dysplastic hip in nonambulatory children with cerebral palsy. J Pediatr Orthop 2008;28:884. [PMID: 19034183]
Schwartz MH, Viehweger E, Stout J, Novacheck TF, Gage JR: Comprehensive treatment of ambulatory children with cerebral palsy: an outcome assessment. J Pediatr Orthop 2004;24:45. [PMID: 14676533]
2. Myelomeningocele (Spina Bifida)
Myelomeningocele (or meningomyelocele) is a complex birth defect affecting the spinal cord and central nervous system. Although the cause is not fully understood, there is a hereditary component. Lack of maternal folic acid is identified as a causative factor in an estimated 50–70% of cases.
![]() Embryologic Defect
Embryologic Defect
The basic embryologic defect is a failure of complete tubulation and dorsal closure of the embryonic neural tube and placode, including incomplete closure of the skin over the spinal cord, resulting from lack of induction. In its mildest form, this spinal dysraphism consists of a simple spina bifida occulta or isolated meningocele (protrusion of spinal membranes, but not nerve, outside of the spinal canal, without neurologic deficit). The more severe varieties include herniation of membranes and nervous tissue through large dorsal bony and skin defects at birth and hydrocephalus with cerebral malformations (Figure 10–38).

![]() Figure 10–38. Spina bifida (myelomeningocele). The sac includes dysplastic spinal cord and membrane elements, and it must be surgically closed in the first days of life. Hydrocephalus and congenital scoliosis are commonly associated.
Figure 10–38. Spina bifida (myelomeningocele). The sac includes dysplastic spinal cord and membrane elements, and it must be surgically closed in the first days of life. Hydrocephalus and congenital scoliosis are commonly associated.
Myelomeningocele can occur at any spinal level but usually is seen between levels T12 and S2. Because neural tissue fails to form properly, the child is paraplegic and insensate below the level of the dysraphism. The clinical determination of neurologic level is most easily accomplished by describing the last muscles contracting under active voluntary motor control (Table 10–8). This may be difficult because of anatomic variability, the age of the child, and other central nervous system involvement.
Table 10–8. Muscle function at neurologic levels in myelomeningocele (spina bifida).

![]() Treatment of Orthopedic Problems
Treatment of Orthopedic Problems
Orthopedic problems associated with myelomeningocele include clubfoot or congenital vertical talus, torsional deformities of the legs, contractures, hip dislocations, and scoliosis. The lack of sensation may allow extensive pressure sores to develop, or painless fractures may go undetected by patients. The health defects of children with spina bifida, in addition to their paralysis, usually include nonmusculo-skeletal organ system problems such as hydrocephalus or Arnold-Chiari malformation (brain), syrinx formation or tethering (spinal cord), and neurogenic bladder or hydronephrosis (renal system). Early in life, most of these are more important than the orthopedic manifestations, and a team approach is needed to decide when and how best to coordinate management. The most pressing needs of the infant born with spina bifida are usually neural defect closure and ventricular shunting.
Orthopedic management depends on the deformities and the long-term mobility goals for the child. The level of paralysis often is helpful in determining whether the child will ultimately be able to walk (L5 or S1 function usually required) or will require a wheelchair (because of function only proximal to L4 or L5). Foot deformities such as clubfoot or congenital vertical talus usually require surgery. If foot deformities recur or progress, tethered cord should be suspected.
Spina bifida is theoretically a static neurologic disease, but many children exhibit a drifting deterioration of neurologic function as they grow; progression of foot deformities, especially during growth spurts, suggests tethering (and therefore stretching) of the cord. Hip dislocations, although dramatic on radiograph, frequently require no treatment; they are painless and tend to occur in children with neurologic involvement at L2 to L4, which precludes long-term walking.
A young child with scoliosis may require bracing until the thorax is long enough for spinal fusion. Scoliosis surgery is complicated by absent posterior neural arches. Some scoliosis seen with spina bifida is congenital (see section on scoliosis). If rapidly progressive scoliosis occurs, the physician should suspect a neurologic cause such as syrinx. Because of chronic exposure to latex materials in contact with mucous membranes and internal tissues (shunts, catheters), children with spina bifida are exceedingly susceptible to latex allergy, which can be fatal. Steps to limit latex exposure are essential in this population and must be observed by medical personnel working with them.
Bartonek A, Saraste H: Factors influencing ambulation in myelomeningocele: a cross-sectional study. Dev Med Child Neurol 2001;43:253. [PMID: 11305403]
Centers for Disease Control and Prevention: Spina bifida and anencephaly before and after folic acid mandate—United States, 1995–1996 and 1999–2000. MMWR Morb Mortal Wkly Rep 2004;53:362. [PMID: 15129193]
3. Muscular Dystrophy
Duchenne muscular dystrophy is an X-linked disorder that presents in boys 6–9 years of age. The disorder is one of progressive muscle weakness, usually first involving more proximal muscles of the limb girdles. Pseudohypertrophy caused by replacement of gastrocnemius muscles (or other muscles) with fat is a classic finding, as is Gower sign (an inability to rise from the floor without using the hands to “walk up” the body and legs). As the muscles weaken, imbalance can cause fixed flexion contractures of the hip, knee, and ankle plantar flexors, which limits walking ability. Because weakness eventually forces patients into a wheelchair, a decision to brace or correct these contractures surgically depends on estimates of remaining strength and likely duration of ambulation after treatment. Most often, progressive foot deformities (usually equinovarus) require muscle release and correction (including bracing) because use of the wheelchair also requires relatively well-positioned feet.
As weakness progresses, the child requires an electric wheelchair for mobility. At this point, scoliosis begins to appear and is usually relentlessly progressive. Attempts to control the scoliosis of muscular dystrophy by wheelchair inserts and braces are ineffective. Early surgery (before cardiorespiratory status deteriorates) is often the best answer. Chapter 12, “Rehabilitation,” provides more information.
4. Myotonic Dystrophy
Myotonic dystrophy is a genetic muscle disease whose name reflects the hallmark of the disease: myotonic EMG potentials. The disease is often associated with mild-to-moderate retardation, obesity, and foot deformities. Initial diagnosis is made by identifying the characteristic myotonic face (weak perioral muscles with a distinctive pyramidal mouth), confirmed by EMG. Myotonic dystrophy worsens with each succeeding generation; genetic markers are available for diagnosis.
The most frequent foot deformity is equinovarus, often with weakness of the anterior tibialis and overactivity of the posterior tibialis. Surgery is often required, and recurrence requiring additional surgery is common. Surgical treatment of myotonic dystrophy foot deformities includes joint release (for passive correction of the deformity) and muscle transfers (for rebalancing muscle forces).
5. Spinal Muscular Atrophy
This heterogeneous group of disorders includes static and degenerative lesions of the anterior horn cell population in the spinal cord. These disorders all involve muscle weakness caused by a lower motor neuron lesion, that is, flaccid paralysis. Sensation is intact, and the major goals are mobility (with electric wheelchair), adaptive devices to aid in daily living (eg, feeding devices), and control of scoliosis, which is similar to management of scoliosis in advanced muscular dystrophy (see section on muscular dystrophy).
King WM, Ruttencutter R, Nagaraja HN, et al: Orthopedic outcomes of long-term daily corticosteroid treatment in Duchenne muscular dystrophy. Neurology 2007;68:1607. [PMID: 17485648]
Mercado E, Alman B, Wright JG: Does spinal fusion influence quality of life in neuromuscular scoliosis? Spine (Phila Pa 1976) 2007;32 (19 Suppl):S120. [PMID: 17728678]
Voisin V, de la Porte S: Therapeutic strategies for Duchenne and Becker dystrophies. Int Rev Cytol 2004;240:1. [PMID: 15548414]
6. Arthrogryposis (Arthrogryposis Multiplex Congenita)
Arthrogryposis is not a disease per se but rather a symptom complex that includes joint contractures or dislocations, rigid skeletal deformities (especially clubfoot), shiny skin with decreased wrinkling and subcutaneous tissue, weakness, and muscle wasting. Although many factors contribute to arthrogryposis, the common link among the symptoms appears to be decreased fetal movement during a critical period in limb development. This can be caused by neurologic lesions (congenital absence of anterior horn cells, Werdnig-Hoffman spinal muscular atrophy, myelomeningocele), myopathic lesions (myotonic dystrophy, congenital myopathies), various syndromes (Moebius syndrome), or physical restriction associated with oligohydramnios.
Arthrogrypotic infants frequently have extension or flexion contractures of knees and elbows, dislocated hips, and severe clubfeet. The contractures may partially resolve with passive ROM therapy in the first 6–12 months of life; however, they must be released surgically after that if they interfere with walking or arm use. Hip dislocations may not limit function and often are not treated. Clubfeet require surgery, which is often of limited success; multiple operations are frequently necessary. Arthrogrypotic children are generally highly resourceful in achieving mobility, and they care for themselves completely independently, despite seemingly overwhelming skeletal problems.
Bernstein RM: Arthrogryposis and amyoplasia. J Am Acad Orthop Surg 2002;10:417. [PMID: 12470044]
Fassier A, Wicart P, Dubousset J, Seringe R: Arthrogryposis multiplex congenita. Long-term follow-up from birth until skeletal maturity. J Child Orthop 2009;3:383. [PMID: 19669823]
TUMORS
Skeletal neoplasms, particularly benign ones, are fairly common in children. Common benign bone lesions of childhood include osteochondroma, osteoid osteoma, unicameral (simple) bone cysts, chondroblastoma, hemangioma, histiocytosis X (eosinophilic granuloma), and fibrous dysplasia. Malignant tumors, which are usually seen after 10 years of age, include Ewing sarcoma and osteosarcoma. Certain systemic diseases can be manifested in childhood as apparent bone tumors (hyperparathyroidism, renal disease, leukemia). Chapter 5 offers a detailed discussion of bone tumors.
AMPUTATIONS
![]() Congenital Amputations and Absence of Segments
Congenital Amputations and Absence of Segments
Congenital absence of limb segments at birth can occur sporadically, as part of a syndrome (Streeter dysplasia) or as a result of mutagens (eg, thalidomide). Absence may be terminal (eg, congenital below-knee amputation) or intercalary (eg, congenital shortening or absence of the humerus).
Although congenital amputations can be dramatic in appearance, the missing limb is not part of the child’s body image. Thus, the child has a natural instinct to be mobile. Children with severe limb deficiencies at birth are almost always able to be completely independent and functional. They accept prostheses quite readily but only if the device truly improves their efficiency. For example, nearly all congenital above-elbow amputees reject artificial limbs, opting for function over appearance. Parents may harbor strong feelings of guilt over the child’s condition, so the psychological issues associated with the condition are more those of the adults than the child.
It is not unusual for congenital amputations to require conversion to a level more easily fitted with a prosthesis. For example, fibular hemimelia (severe shortening of the tibia with absent fibula and foot deformity) sometimes can be most effectively treated by removing the foot and converting the limb to an ankle disarticulation level. This facilitates prosthetic fitting and simplifies management of the leg-length discrepancy, thus permitting normal function.
Boostra AM, Rijnders LJ, Groothoff JW, et al: Children with congenital deficiencies or acquired amputations of the lower limbs: functional aspects. Prosthet Orthot Int 2000;24:19. [PMID: 10855435]
Ephraim PL, Dillingham TR, Sector M, et al: Epidemiology of limb loss and congenital limb deficiency: a review of the literature. Arch Phys Med Rehabil 2003;84:747. [PMID: 12736892]
Fixsen JA: Major lower limb congenital shortening: a mini review. J Pediatr Orthop B 2003;12:1. [PMID: 12488764]
Klaassen Z, Shoja MM, Tubbs RS, Loukas M: Supernumerary and absent limbs and digits of the lower limb: a review of the literature. Clin Anat 2011;24:570. [PMID: 21204092]
![]() Traumatic Amputation
Traumatic Amputation
In contrast to the congenital amputee, the child with a traumatic amputation is particularly likely to be male, adolescent, rebellious, and troubled. Although pediatric traumatic amputations are often caused by inadvertent incidents, many result from high-risk behavior. These factors must be taken into account when dealing with the psychological issues of the patient and family; social, as well as medical, intervention is often appropriate.
The orthopedic management of traumatic amputees is modified in children by the presence of growth plates and the remarkable healing and rehabilitation powers of children. This must be considered during surgical completion of amputations because injury to the physis may cause severe shortening or angulation of a stump, rendering the amputation far less satisfactory than a similar amputation in the adult. The child amputee rarely has vascular problems, however, and the use of split-thickness skin grafting may allow preservation of length that would be impossible in most adults.
![]() Overgrowth of Amputation Stump
Overgrowth of Amputation Stump
Amputations through the long bones of children exhibit the unique phenomenon of terminal overgrowth. Eventually, the distal end of the stump may develop a long, thin, sometimes painful bony prominence. Overgrowth is not physeal in origin (ie, closure of the physis by epiphysiodesis does not eliminate its formation), and it appears to be related to aggressive bone formation associated with the periosteal membrane.
Although overgrowth can occur in any bone, it is most troublesome in the tibia, fibula, and humerus. When symptomatic, overgrowth is treated by resecting the spike of bone (revision of the amputation), but the process does continue, and recurrence is common. Some pediatric amputees require two or more surgical revisions during growth. Overgrowth ceases at skeletal maturity. Various attempts at capping the overgrowing bone end (using foreign materials or free epiphyseal grafts) have met with inconsistent success.
Jeans KA, Browne RH, Karol LA: Effect of amputation level on energy expenditure during overground walking by children with an amputation. J Bone Joint Surg Am 2011;93:49. [PMID: 21209268]
Tenholder M, Davids JR, Gruber HE, et al: Surgical management of juvenile amputation overgrowth with a synthetic cap. J Pediatr Orthop 2004;24:218. [PMID: 15076611]
FRACTURES
![]() Common Pediatric Fracture Patterns
Common Pediatric Fracture Patterns
Many fractures in children are similar to their counterparts in adults. However, the added factor of growth contributes to the unique issues of fracture care in children. Pediatric bone is softer and more easily broken than adult cortical bone. Thus, the amount of energy required to produce a fracture is less in the child, even as soft-tissue injury is frequently less severe in the child than in the adult. In addition, the periosteal membrane in children is far thicker and more osteogenic than in adults. The periosteum is so leathery in immature humans that it frequently holds bone ends together, contributing greatly to stability and ease of manipulative reduction. The excellent osteogenic potential of pediatric periosteum permits rapid, aggressive fracture healing, so nonunions are extremely rare in children.
Less brittle pediatric bone is subject to fracture patterns unique to children (Figure 10–39). A greenstick fracture is a transverse crack that retains its continuity, just as a small moist twig breaks without actually snapping apart.

![]() Figure 10–39. Softer bone in children can lead to unique fracture behavior (in addition to the fracture patterns seen in adults). A: Greenstick fracture; B: torus fracture; C: plastic deformation.
Figure 10–39. Softer bone in children can lead to unique fracture behavior (in addition to the fracture patterns seen in adults). A: Greenstick fracture; B: torus fracture; C: plastic deformation.
A torus fracture is a small buckle or impaction of one cortex with a slight bend on the opposite cortex. Plastic deformation is a change in the natural shape of a bone without a detectable fracture line.
Remodeling (gradual correction in alignment or size of a fractured bone back to normal) is generally far more rapid in children than in adults. Remodeling of angular deformities is particularly rapid when the deformity is in the same plane of motion as the nearest joint (Figure 10–40) or when the deformity is near a rapidly growing physis. Remodeling of rotational deformities is less reliable. Overgrowth is a singular feature of remodeling that occurs in certain fractures of the long bones, particularly the femur. It is a product of physeal stimulation by the hyperemic response to fracture and healing and may increase the length of a bone by 2 cm or more over the course of a year.

![]() Figure 10–40. Remodeling of bone after fracture is most rapid when it is in the plane of a nearby joint. Schematically, if the joint is thought of as a hinge, the fracture above (in the plane of the hinge) is likely to remodel faster than the fracture below the hinge (out of plane).
Figure 10–40. Remodeling of bone after fracture is most rapid when it is in the plane of a nearby joint. Schematically, if the joint is thought of as a hinge, the fracture above (in the plane of the hinge) is likely to remodel faster than the fracture below the hinge (out of plane).
The combination of low-energy injury, rapid bone healing, and dependable remodeling of angular deformity makes it possible to treat many pediatric fractures by simple closed reduction (often incomplete) and casting. Surgical management of children’s fractures is rarely required. The surgeon may accept a less-than-perfect reduction if the fracture is known to remodel into satisfactory alignment.
1. Epiphyseal Fracture
The cartilage physeal plates are a region of low strength relative to the surrounding bone and are susceptible to fracture in the child. They are analogous to a scratch on a pane of glass, in which concentrated force facilitates damage. Once injury occurs, the physis usually is able to recover and resume growth. But if an offset occurs in the physeal substance, bone may grow across it (from epiphyseal bone to metaphyseal bone), forming a bridge that anchors further growth and leads to either progressive shortening or a worsening angulation (Figure 10–41).
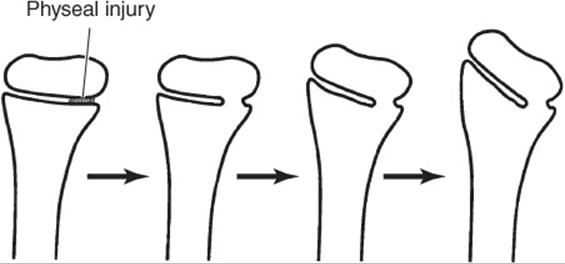
![]() Figure 10–41. Progressive angular deformity can occur if there is asymmetric closure of the physis after fracture.
Figure 10–41. Progressive angular deformity can occur if there is asymmetric closure of the physis after fracture.
Because physes are near joints and physeal fractures are common, children may suffer injuries to joint surfaces that require careful surgical repair and realignment. Thus, open reduction is more likely in fractures involving physes and joints than in other pediatric fractures.
Most physeal fractures propagate through the weakest region of the cartilage. Physeal cartilage begins in a dense resting zone on the epiphyseal side, and chondrocytes gradually multiply, elongate, and arrange into longitudinal columns that produce longitudinal growth. Hypertrophic, balloon-like chondrocyte columns then undergo cell death, and the remaining cell walls are calcified and eventually ossify to form metaphyseal bone.
The weakest spot is usually the interface between hyper-trophic dying columns of cells and the stiff calcified cell walls beneath them; this area is highly susceptible to shearing forces. So, physeal fractures (eg, Salter-Harris fractures) typically occur through the zone of hypertrophy. Fortunately, the region also represents the boundary between the process of epiphyseal elongation (supported by the epiphyseal blood supply) and metaphyseal ossification (supported by the metaphyseal blood supply). Thus, physeal fractures do not often damage the growth potential of the physis because they do not interrupt its critical blood supply. An exception to the usual location of these fractures is the growth plate in the distal femur. It has an undulating topography, with prominences called mammillary bodies that interdigitate with other portions of the physis to provide stability at the distal femur. A typical distal femoral physeal fracture propagates through multiple layers of the growth plate. This results in displaced physeal fractures of the distal femur being at high risk for causing premature growth arrest of the involved physis and subsequent deformity.
Although physeal fractures can occur in a wide variety of configurations, certain patterns are seen frequently enough that a descriptive classification aids in understanding phy-seal injury (Figure 10–42). Fractures that either cross the joint or result in spatial malalignment of portions of the physis have the worst prognosis.

![]() Figure 10–42. The Salter-Harris classification of physeal fractures is widely used to describe such injuries. With some exceptions, the potential for problems with growth arrest is greater in the higher numbered patterns.
Figure 10–42. The Salter-Harris classification of physeal fractures is widely used to describe such injuries. With some exceptions, the potential for problems with growth arrest is greater in the higher numbered patterns.
Physeal fractures heal rapidly, usually within 4 weeks. Careful monitoring is required to detect early posttraumatic closure of the growth plate. Occasionally, an epiphyseal–metaphyseal bony bridge forms and tethers growth. If this growth is minor, surgical removal of the bridge (epiphyseal bar resection) may successfully restore physeal growth. Otherwise, the procedures for evaluation and treatment of limb-length inequality should be followed (see previous section on limb-length inequality).
Salter RB, Harris WR: Injuries involving the growth plate. J Bone Joint Surg Am 1963;45:587. [No PMID]
2. Upper Extremity Fractures
![]() Clavicle Fracture
Clavicle Fracture
Clavicle fractures are among the most common injuries in children. They are usually closed and may be treated with a simple sling. Healing occurs rapidly with abundant callus, which leaves a lump that may concern parents. This enlargement remodels over several years of growth.
Clavicle fractures can occur at birth and heal rapidly but are sometimes accompanied by neurologic injury. Then, return of active biceps before 3 months and preservation of full passive shoulder ROM are predictors of a good outcome. Breech delivery is usually associated with preganglionic injury. Preganglionic injury can result in a Horner sign, which includes ptosis, miosis, and anhydrosis. Preganglionic injuries are unlikely to recover. The Moro reflex is elicited by dropping a baby’s head a short distance and observing active elbow extension and fanning of the fingers, followed by elbow flexion and crying. Absence of the Moro reflex suggests a poor prognosis.
An extremely rare condition, atraumatic congenital pseudarthrosis of the clavicle can mimic the radiographic appearance of fracture. It may be right sided or bilateral, with little or no pain and no history of trauma. Treatment is generally unnecessary.
![]() Proximal Humerus Fracture
Proximal Humerus Fracture
Proximal humerus fractures are usually epiphyseal injuries (usually Salter-Harris type II injuries) that may progress into significant varus angulation (medial deviation). Fortunately, the proximal humerus is a rapidly growing physis and shoulder motion is full in all planes, so remodeling is rapid. These fractures generally require only a sling or shoulder immobilization for 3–4 weeks, without reduction. Rarely, fractures with extreme angulation (>90 degrees) may require surgical reduction and fixation.
![]() Elbow Region Fracture
Elbow Region Fracture
Most elbow region fractures are indirect injuries caused by a fall on the outstretched hand. Both diagnosis and treatment can be difficult in this serious group of injuries. Epiphyseal ossification is incomplete in the group that is susceptible to falls (2–10 years of age), making radiographs difficult to interpret (Figure 10–43). Swelling, if severe, can block venous or arterial structures and lead to forearm compartment syndromes. Reductions are often unstable, and operative intervention may be required. Most surgeons immobilize pediatric elbow fractures for 4 weeks after treatment. The most important fractures are listed next.

![]() Figure 10–43. Ages of appearance of ossification centers. The ossification centers of the elbow region emerge at different ages as indicated and can complicate the interpretation of radiographs. It is often advisable to obtain comparison radiographs of the opposite elbow if injury is suspected.
Figure 10–43. Ages of appearance of ossification centers. The ossification centers of the elbow region emerge at different ages as indicated and can complicate the interpretation of radiographs. It is often advisable to obtain comparison radiographs of the opposite elbow if injury is suspected.
A. Supracondylar Fracture of Humerus
Supracondylar fracture of the humerus occurs at the metaphyseal bone, proximal to the elbow joint, and does not involve the growth plate (Figure 10–44). Displacement may be severe, and nerve injury, usually caused by stretching, is common. If swelling is marked, there may be interruption of the blood supply; it is not uncommon for such a distal extremity to lack a pulse.

![]() Figure 10–44. Displaced supracondylar fracture of the humerus. Injury film (A); after closed reduction and internal fixation using percutaneous pins (B).
Figure 10–44. Displaced supracondylar fracture of the humerus. Injury film (A); after closed reduction and internal fixation using percutaneous pins (B).
The most appropriate treatment is rapid anatomic reduction under general anesthesia. Because the reduction is highly unstable, many surgeons prefer to fix the fracture after reduction with percutaneous wires. Once the fracture is reduced, the swelling recedes rapidly and the pulse returns. On rare occasions, the surgeon must perform vascular or nerve exploration or repair.
Some displaced supracondylar humerus fractures are incompletely reduced or lose position because of fracture instability after apparently adequate initial reduction. This progresses to a characteristic malunion with an apex-lateral angular deformity of the elbow (known as cubitus varus or so-called gunstock deformity). Although cosmetically unsightly, cubitus varus rarely has any significant functional consequences. If desired, it may be corrected by valgus osteotomy at the old fracture site.
B. Lateral Condyle Fracture
The lateral condyle fracture is an oblique shearing fracture of the lateral portion of the joint surface that occurs when the radial head drives into the capitulum of the humerus during a fall. The lack of significant ossification may obscure the fracture or give the false appearance of a benign Salter-Harris II fracture pattern, but most lateral condyle fractures are highly unstable Salter-Harris IV fractures (Figure 10–45). Because both the joint surface and the physis are displaced, they usually require open reduction and fixation using pins.

![]() Figure 10–45. Lateral condyle fracture of the humerus (A) can easily be mistaken for a relatively simple Salter-Harris type II injury, which carries a good prognosis (B). In reality, however, it is almost always a Salter-Harris type IV injury, with a fracture pattern crossing both the joint surface and the physis (C); unless it is not displaced, it requires open reduction.
Figure 10–45. Lateral condyle fracture of the humerus (A) can easily be mistaken for a relatively simple Salter-Harris type II injury, which carries a good prognosis (B). In reality, however, it is almost always a Salter-Harris type IV injury, with a fracture pattern crossing both the joint surface and the physis (C); unless it is not displaced, it requires open reduction.
C. Radial Neck Fracture
Fracture of the radial neck is similar to a lateral condyle fracture. The radial neck just distal to the joint may angulate up to 70–80 degrees, although lesser angulation is more common (Figure 10–46). It is important to determine the location of the radial head despite traumatic angulation of the radial neck. Surprisingly, angulation of 45 degrees or less usually remodels spontaneously and requires only symptomatic treatment that permits early return to activity. Larger degrees of angulation can often respond to closed manipulation.

![]() Figure 10–46. Fracture of the radial neck may angulate greatly yet still remodel spontaneously in the younger child.
Figure 10–46. Fracture of the radial neck may angulate greatly yet still remodel spontaneously in the younger child.
D. Forearm Fracture
Forearm fractures are a common result of falls. If they involve both bones, one bone may be completely displaced while the other only bends or suffers a greenstick fracture. In children, most forearm fractures that involve both bones can be treated successfully by closed reduction and casting; minor angular malalignment can easily be tolerated if rotational alignment of the bone ends is accurate. In addition, the ends of fractured bones often overlap. This is not necessarily of concern if alignment is satisfactory because side-to-side bone healing and remodeling are rapid in children.
E. Monteggia Fracture
Monteggia fracture is fracture of the ulna only, with the radius remaining intact. Because two-bone systems generally must fail in two spots if they break at all, the radial head dislocates from the capitulum. In such cases, reduction must include the elbow component. As with other pediatric forearm fractures, closed reduction is usually successful, although some Monteggia fractures require open reduction. The physician should be alert to the possibility of Monteggia fracture because the fracture can lead to chronic loss of elbow motion if it is not properly reduced.
In children, Galeazzi fracture of the radius, in which the distal radioulnar joint is dislocated, is far less common than the analogous Monteggia fracture.
F. Torus Fracture of Radius
Torus fracture of the radius is a minor buckle of the dorsal cortex of the distal radius, usually 1–2 cm proximal to the distal radial physis. It occurs after a minor fall on the hand. Many torus fractures are mistaken for wrist sprains because they are stable and not as painful as unstable fractures. They heal uneventfully in 3–4 weeks, with excellent long-term results.
Mirsky EC, Karas EH, Weiner LS: Lateral condyle fractures in children: evaluation of classification and treatment. J Orthop Trauma 1997;11:117. [PMID: 9057147]
Price CT: The treatment of displaced fractures of the lateral humeral condyle in children. J Orthop Trauma 2010;24:439. [PMID: 20577076]
Wattenbarger JM, Gerardi J, Johnston CE: Late open reduction internal fixation of lateral condyle fractures. J Pediatr Orthop 2002;22:394. [PMID: 11961463]
Weiss JM, Graves S, Yang S, Mendelsohn E, Kay RM, Skaggs DL: A new classification system predictive of complications in surgically treated pediatric humeral lateral condyle fractures. J Pediatr Orthop2009;29:602. [PMID: 19700990]
![]() Metacarpal and Phalangeal Fractures
Metacarpal and Phalangeal Fractures
Fractures of the metacarpals and phalanges commonly occur from crush injuries in children (eg, catching a hand or finger in a door) and are generally quite stable because the periosteum remains intact. Rarely severely angulated or rotationally malaligned, they can usually be managed by immobilization for 2–3 weeks.
3. Lower Extremity Fractures
![]() Pelvic Fracture
Pelvic Fracture
Pelvic fractures in children are usually seen in conjunction with major blunt trauma. Gross displacement is fairly uncommon and usually can be treated symptomatically because the intact periosteum stabilizes the large flat bones. The patient should be carefully evaluated for intraabdominal and other injuries. Properly treated pelvic fractures in an immature skeleton resolve satisfactorily.
Adolescents exhibit a special type of avulsion fracture of apophyses because aggressive pulling of muscles during sports can detach an apophysis from its parent bone. These avulsion fractures are sometimes called transitional fractures because the physes are in transition within 2 years of skeletal maturity. During this time, relatively weak cartilage physes may not be strong enough to withstand the pull of growing muscles suddenly grown powerful under the influence of hormones. Transitional avulsion fractures may occur at the iliac crest (abdominal muscles), lesser trochanter of the femur (iliopsoas muscle), or ischial tuberosity (hamstring muscle). Transitional fractures of the pelvis and femur are treated symptomatically. Although these fractures do not require reduction, they may heal with a significant bump that requires excision later.
Tsirikos AI, Spiegel PG, Laros GS: Transepiphyseal fracture-dislocation of the femoral neck: A case report and review of the literature. J Orthop Trauma 2003;17:648. [PMID: 14574194]
![]() Hip Fracture
Hip Fracture
Pediatric hip fractures are rare but may be serious because trauma to this area may produce significant injury. As in the adult, the fracture pattern may disrupt the blood supply of the proximal femoral head and lead to avascular necrosis of the proximal femoral epiphysis, femoral neck, or both. In older children, this can be a devastating complication; it is treated like LCP but may result in such severe collapse that hip fusion is required.
Femoral neck fractures in children are highly unstable and treated by reduction and internal fixation. The mechanical fixation may be imperfect because the surgeon must avoid injury to the proximal femoral physis. For this reason, a spica cast (body and legs) is generally used as well.
Odent T, Glorion C, Pannier S, et al: Traumatic dislocation of the hip with separation of the capital epiphysis: 5 adolescent patients with 3–9 years of follow-up. Acta Orthop Scand 2003; 74:49. [PMID: 12635793]
![]() Femoral Shaft Fracture
Femoral Shaft Fracture
Fractures of the femoral shaft are common injuries caused by falls as well as bicycle and motor vehicle accidents. In young children, they may be the result of child abuse. Although most are closed injuries, blood loss can be significant because of bleeding into the soft tissues of the thigh. Nerve injury is rare, and the fact that the fracture is surrounded by richly nourished muscle ensures rapid solid union (usually within 6 weeks).
Longitudinal muscle pull and spasm cause femoral shaft fractures to shorten and angulate. Initial treatment requires longitudinal traction (skin traction in younger children, skeletal traction in older children) to restore length and alignment. At this point, treatment largely depends on the patient’s age.
Femur fractures in children 2–10 years of age have a strong tendency to exhibit overgrowth of 1–2.5 cm because of fracture hyperemia. In this age group, therefore, it may be desirable to use a cast and allow some shortening to occur. Rapid remodeling of the bone makes perfect reduction unnecessary. Most surgeons apply a spica cast immediately or within the first week.
Femoral overgrowth following fracture becomes unlikely in children older than 10 years. In these older children, the bone either must be kept to anatomic length by traction for 3–4 weeks (until sufficient callus has formed to stabilize length) or treated by intramedullary nails or other operative measures, as in the adult. The medial femoral circumflex artery supplies blood to the femoral head. Its position along the posterior-superior femoral neck places this structure at risk with intramedullary nailing of the femur. Therefore, lateral entry through the greater trochanter is preferred when intramedullary fixation is performed. Currently, flexible intramedullary nails are popular because they do not require reaming prior to insertion, and they are less likely to disrupt the precarious blood supply of the proximal femur. There is now a tendency at many centers to fix femur fractures using flexible nails in children 6 years and older.
After healing or cast removal, the child may begin walking. Limping is common in the first month after fracture because the hip girdle musculature regains its strength only slowly. No physical therapy is required, however, because normal walking permits spontaneous recovery, and long-term results of pediatric femur fractures are excellent.
![]() Epiphyseal Separation
Epiphyseal Separation
Epiphyseal separations (fracture) of the distal femoral physis are usually Salter-Harris type I or II injuries. All are caused by significant trauma, and injury to the growth mechanism of the plate is common. As many as 50% of cases exhibit subsequent growth arrest. Major neurovascular injury can occur, as with knee dislocations. Displaced epiphyseal separations require gentle reduction under general anesthesia. Some are so unstable, however, that they require percutaneous pin fixation for several weeks until the fracture is sticky, as it were, or healed enough so displacement does not occur. If physeal closure occurs, the treatment depends on age and remaining growth potential. (See earlier discussion of limb-length inequality.)
![]() Tibial Eminence Injury
Tibial Eminence Injury
The tibial eminence (spine), located entirely on the proximal tibial epiphysis, is the site of attachment of the anterior cruciate ligament. Twisting injuries of the knee can shear off the eminence and may displace it within the joint. Most fractures occur in children ages 8 to 14 years, and they typically present with a painful hemarthrosis and refusal to bear weight. A type I fracture is minimally displaced, type II is anteriorly displaced with an intact posterior hinge, and type III is completely displaced. Long leg casting for 6 weeks, until the bone heals (Figure 10–47), is advocated for type I fractures, although there is debate about whether the knee should be maintained in full extension or in 10–20 degrees of flexion. Management of type II and III fractures is much more controversial. Type II fractures can be treated closed if adequate reduction can be achieved, but if not, surgical management is indicated. Surgery is also indicated for type III fractures. In these displaced injuries, the medial meniscus can be trapped under the fragment and/or the lateral meniscus; if the anterior cruciate ligament is still attached to the avulsed fracture fragment, this may cause pulling on the fragment and therefore block reduction. Unlike many other pediatric fractures, tibial eminence injuries often lead to mild long-term knee symptoms, especially during athletic activities

![]() Figure 10–47. Tibial eminence fracture usually includes an anterior cruciate avulsion component. It can be treated nonoperatively if the fragment reduces with extension of the knee.
Figure 10–47. Tibial eminence fracture usually includes an anterior cruciate avulsion component. It can be treated nonoperatively if the fragment reduces with extension of the knee.
![]() Tibial Tubercle Avulsion Fracture
Tibial Tubercle Avulsion Fracture
Tibial tubercle avulsion fractures are most often seen in adolescent males (13–14 years of age) who suffer sports-related injuries. The anterior tongue of the proximal tibial epiphysis is the site of attachment of the patellar tendon. During strenuous jumping, as in basketball, the tongue may avulse and displace. Tibial tubercle avulsions are transitional fractures in that they occur immediately before physeal closure and are not seen in younger children. They are classified as follows: type I, a small fragment of the tuberosity is avulsed and is displaced upward; type II, the whole tongue formed by the anterior aspect of the tibial epiphysis is hinged upward without being completely fractured at its base; and type III, the entire tibial tuberosity is fractured at its base, with the line of fracture directed proximally and posteriorly into the articular surface. Nearly all these fractures require open reduction and internal fixation, although the surgeon need not take the usual precautions when operating near the physis because maturity follows too rapidly to permit deformity. There is a high incidence of compartment syndrome seen in type III tibial tubercle fractures. Fasciotomy should be considered at the time of initial repair. Type III tibial tubercle fractures extending through the joint are often associated with meniscal injuries, which must be repaired. Delayed complications included recurvatum and refracture.
![]() Proximal Tibial Metaphyseal Fracture
Proximal Tibial Metaphyseal Fracture
Proximal tibial metaphyseal fractures are usually undis-placed or minimally displaced. In the absence of fibular overgrowth (Figure 10–48), they can exhibit troublesome late angular deformity (valgus) caused by tibial overgrowth after fracture. The phenomenon is most pronounced at the age of maximum physiologic valgus (3–6 years). Over a number of years, the valgus has a tendency to remodel, so the best approach is observation.

![]() Figure 10–48. Even when not displaced, fracture of the proximal tibial metaphysis can stimulate the tibial physis and cause progressive valgus deformity, especially in patients younger than 6 years. Long-term observation indicates that slow remodeling eventually occurs.
Figure 10–48. Even when not displaced, fracture of the proximal tibial metaphysis can stimulate the tibial physis and cause progressive valgus deformity, especially in patients younger than 6 years. Long-term observation indicates that slow remodeling eventually occurs.
![]() Tibial Shaft Fracture
Tibial Shaft Fracture
Tibial shaft fractures, which are usually accompanied by fibula fractures, generally result from major trauma. An exception is the nondisplaced, isolated spiral tibial fracture often seen after minor trauma in children just learning to walk (toddler’s fracture). In the pediatric population, open tibia fractures are fairly common. As in the adult, injury to neurovascular structures and compartment syndromes are major risks (see Chapter 2, “Musculoskeletal Trauma Surgery”). Open fractures of the tibia and fibula require surgical debridement, but because skin loss is less likely than in the adult, they can often be managed the same way as closed fractures, following lavage.
Most tibial fractures in children can be adequately aligned and immobilized in above-knee casts. Rare, unstable cases, some open fractures, or fractures in older children also may require external fixation or other devices to maintain reduction and alignment. As in the adult, pediatric tibia fractures are relatively slow to heal, frequently requiring 10–12 weeks; nonunion is rare, however.
![]() Ankle Fracture and Distal Tibial Fracture
Ankle Fracture and Distal Tibial Fracture
Ankle fractures and distal tibial fractures in younger children are often either metaphyseal or Salter-Harris type II distal tibial physeal injuries that heal rapidly. These fractures have very little tendency to suffer growth arrest or other serious consequences (Figure 10–49). Posttraumatic physeal arrest occurs most commonly after injury in the distal medial tibia. In children 8–11 years of age, inversion injuries can push off the medial malleolus, causing an oblique Salter-Harris type IV fracture that disrupts both the joint and the growth plate. These fractures generally require open reduction for accurate realignment of the physis and articular surface. Subsequent growth arrest can cause a medial physeal bridge and produce a progressive varus deformity of the distal tibial articular surface as the lateral physis continues untethered elongation. If this occurs, either epiphyseal bar resection or corrective tibial osteotomy should be considered.

![]() Figure 10–49. Simple fracture of the distal tibia (and fibula) at the ankle is usually a Salter-Harris type II pattern in patients younger than 10 years.
Figure 10–49. Simple fracture of the distal tibia (and fibula) at the ankle is usually a Salter-Harris type II pattern in patients younger than 10 years.
The distal tibia is the site of several distinct transitional fracture patterns. These physeal injuries occur only at the end of growth, shortly before complete distal tibial physeal closure at maturity. The distal physis begins early closure medially, with gradual lateral closure over the next year. The exact fracture pattern depends on how much of the plate is still open and on the force applied (ie, mechanism of injury). When just the medial physis is closed, a triplane fracture (ie, sagittal, transverse, and frontal) of the distal tibia occurs (Figure 10–50). This fracture contains a complex of fracture lines and crosses the growth plate. Triplane fractures usually require open reduction, although minimally displaced injuries can be managed nonoperatively. CT scans may be necessary to define the exact fracture configuration for accurate treatment.

![]() Figure 10–50. The triplane (A) and juvenile Tillaux (B) fractures are variations of ankle fracture that occur in the adolescent shortly before physeal closure. Because they involve the joint surface, such fractures may require open reduction.
Figure 10–50. The triplane (A) and juvenile Tillaux (B) fractures are variations of ankle fracture that occur in the adolescent shortly before physeal closure. Because they involve the joint surface, such fractures may require open reduction.
In slightly older patients, when only a small anterolateral segment of the physis remains open, this anterolateral fragment can be avulsed by fibers of the distal tibiofibular syndesmosis (juvenile Tillaux fracture). This is a Salter-Harris type III fracture involving the articular surface and frequently requires open reduction to restore perfect joint anatomy.
Leary JT, Handling M, Talerico M, Yong L, Bowe JA: Physeal fractures of the distal tibia: predictive factors of premature physeal closure and growth arrest. J Pediatr Orthop 2009;29:356. [PMID: 19461377]
Spiegel PG, Cooperman DR, Laros GS: Epiphyseal fractures of the distal ends of the tibia and fibula: a retrospective study of two hundred and thirty-seven cases in children. J Bone Joint Surg Am1978;60:1046. [PMID: 721852]
INJURIES RELATED TO CHILD ABUSE
Child abuse crosses all socioeconomic boundaries and takes many forms. The musculoskeletal system is frequently the site of abuse-related injuries, but findings may be subtle or misleading. The most critical issue to consider in suspected abuse is whether the history can explain the injury adequately and believably.
The classic radiographic picture of abuse is the presence of multiple healing fractures of various ages; in the absence of a bone fragility syndrome, the diagnosis may thus be obvious (Figure 10–51). Soft-tissue injuries were found in 92% of children suspected of having been physically abused, with ecchymosis as the most common finding, increasing in incidence with age. Long bones (femur or humerus) are the bones most commonly fractured during child abuse. These fractures are transverse or oblique shaft injuries, a common pattern that is not by itself diagnostic. The history is often one of a minor fall or a limb “catching” in the side of the crib. But studies of fractures in young children disclosed that injury mechanisms of this type are almost never the cause of serious skeletal injury, and the dichotomy between story and findings is highly suggestive of abuse. A good rule of thumb is to consider any long bone fracture in a child younger than 3 years as abuse until proved otherwise.

![]() Figure 10–51. The presence of multiple fractures of various ages as well as unexplained long-bone fracture in a young child should suggest the diagnosis of child abuse.
Figure 10–51. The presence of multiple fractures of various ages as well as unexplained long-bone fracture in a young child should suggest the diagnosis of child abuse.
The orthopedic management of abuse fractures is rarely complex, and simple closed methods usually suffice. Nearly all such fractures carry an excellent prognosis and heal or remodel rapidly. It is the detection of the abuse, and its subsequent social management, that are the main determinant of outcome.
McMahon P, Grossman W, Gaffney M, et al: Soft-tissue injury as an indication of child abuse. J Bone Joint Surg Am 1995;77:1179. [PMID: 7642662]
Oral R, Blum KL, Johnson C: Fractures in young children: are physicians in the emergency department and orthopedic clinics adequately screening for possible abuse? Pediatr Emerg Care 2003;19:148. [PMID: 12813297]