TABLE 12 - 1. Normal Respiratory Rates in Children

RESPIRATORY DISTRESS
A common reason to visit emergency department (10% of ED visits).
![]() Intercostal retractions.
Intercostal retractions.
![]() Nasal flaring (indicates
Nasal flaring (indicates ![]() effort is needed to breathe).
effort is needed to breathe).
![]() Use of accessory muscles for breathing (eg, abdominals, sternocleidomastoids).
Use of accessory muscles for breathing (eg, abdominals, sternocleidomastoids).
![]() Restlessness, agitation.
Restlessness, agitation.
![]() Somnolence or lethargy may be due to severe hypoxia or hypercarbia.
Somnolence or lethargy may be due to severe hypoxia or hypercarbia.
![]() Pallor, cyanosis.
Pallor, cyanosis.
![]() Wheezing may or may not be present.
Wheezing may or may not be present.
![]() Stridor is an inspiratory sound that localizes respiratory distress to the upper airway
Stridor is an inspiratory sound that localizes respiratory distress to the upper airway
![]() Grunting:
Grunting:
![]() Due to exhalation against a partially closed glottis.
Due to exhalation against a partially closed glottis.
![]() Occurs during expiration.
Occurs during expiration.
![]() Indicates moderate to severe hypoxia.
Indicates moderate to severe hypoxia.
![]() See Table 12-1 for normal respiratory rates by age.
See Table 12-1 for normal respiratory rates by age.
COMMON COLD (UPPER RESPIRATORY INFECTION, NASOPHARYNGITIS)
![]()
A 7-year-old girl is well when she leaves for school, but arrives home afterwards with a sore throat and runny nose. She is also complaining of cough, sneezing, and facial heaviness. Think: Rhinovirus.Rhinovirus colds frequently start as a sore or “scratchy” throat with runny nose.
![]()
A 17-year-old adolescent has acute onset of fever, cough, conjunctivitis, and pharyngitis. Think: Adenovirus. Characteristic presentation: Pharyngitis, rhinitis, and conjunctivitis. Conjunctivitis is typically follicular.
DEFINITION
Multi-etiology illness with a constellation of symptoms including cough, congestion, and rhinorrhea. Upper respiratory infections (URIs) are the most common pediatric ED presentation.
ETIOLOGY
![]() > 200 viruses—especially rhinoviruses (one-third), parainfluenza, respiratory syncytial virus (RSV), adenovirus.
> 200 viruses—especially rhinoviruses (one-third), parainfluenza, respiratory syncytial virus (RSV), adenovirus.
![]() Risk factors: Child care facilities, smoking, passive exposure to smoke, low income, crowding, and psychological stress.
Risk factors: Child care facilities, smoking, passive exposure to smoke, low income, crowding, and psychological stress.
EPIDEMIOLOGY
![]() Most frequent illness of childhood (three to eight episodes per year).
Most frequent illness of childhood (three to eight episodes per year).
![]() Most common medical reason to miss school.
Most common medical reason to miss school.
![]() Occurs in fall and winter especially.
Occurs in fall and winter especially.

Mucopurulent rhinitis may accompany a common cold and doesn’t necessarily indicate sinusitis; it is not an indication for antibiotics.
SIGNS AND SYMPTOMS
![]() Nasal and throat irritation.
Nasal and throat irritation.
![]() Sneezing, nasal congestion, rhinorrhea.
Sneezing, nasal congestion, rhinorrhea.
![]() Sore throat, postnasal drip.
Sore throat, postnasal drip.
![]() Low-grade fever, headache, malaise, and myalgia.
Low-grade fever, headache, malaise, and myalgia.
![]() Possible complications include otitis media, sinusitis, and trigger asthma.
Possible complications include otitis media, sinusitis, and trigger asthma.
![]() Infants have a variable presentation—feeding and sleeping are difficult due to congestion, vomiting may occur after coughing, may have diarrhea.
Infants have a variable presentation—feeding and sleeping are difficult due to congestion, vomiting may occur after coughing, may have diarrhea.
TREATMENT
![]() Supportive.
Supportive.
![]() Avoid aspirin and over-the-counter cough suppressants or decongestants.
Avoid aspirin and over-the-counter cough suppressants or decongestants.
![]() Direct therapy toward specific symptoms.
Direct therapy toward specific symptoms.
The best treatment for the common cold is to ![]() oral fluids, not pharmacologic treatment.
oral fluids, not pharmacologic treatment.
INFLUENZA
DEFINITION
Viral respiratory illness.
ETIOLOGY
![]() Influenza A and B—epidemic disease: H1N1 (influenza A).
Influenza A and B—epidemic disease: H1N1 (influenza A).
![]() Influenza C—sporadic.
Influenza C—sporadic.
Aspirin is avoided in young children due to theoretical risk of Reye syndrome.
EPIDEMIOLOGY
Common over the winter months.
SIGNS AND SYMPTOMS
![]() Incubation period: 1–3 days.
Incubation period: 1–3 days.
![]() Sudden onset of fever, frequently with chills, headache, malaise, diffuse myalgia, and nonproductive cough.
Sudden onset of fever, frequently with chills, headache, malaise, diffuse myalgia, and nonproductive cough.
![]() Conjunctivitis, pharyngitis.
Conjunctivitis, pharyngitis.
![]() Typical duration of febrile illness is 2–4 days.
Typical duration of febrile illness is 2–4 days.
![]() Complications include otitis media, pneumonia, myositis, and myocarditis.
Complications include otitis media, pneumonia, myositis, and myocarditis.
![]() Diarrhea and vomiting (H1N1).
Diarrhea and vomiting (H1N1).

Influenza is an orthomyxovirus.
DIAGNOSIS
![]() Nasal swab or nasal washing.
Nasal swab or nasal washing.
![]() During epidemic, clinical signs can be used to save on test costs.
During epidemic, clinical signs can be used to save on test costs.
Diagnosis of influenza depends on epidemiologic and clinical consideration.
TREATMENT
![]() Symptomatic treatment is appropriate for healthy children—fluids, rest, acetaminophen.
Symptomatic treatment is appropriate for healthy children—fluids, rest, acetaminophen.
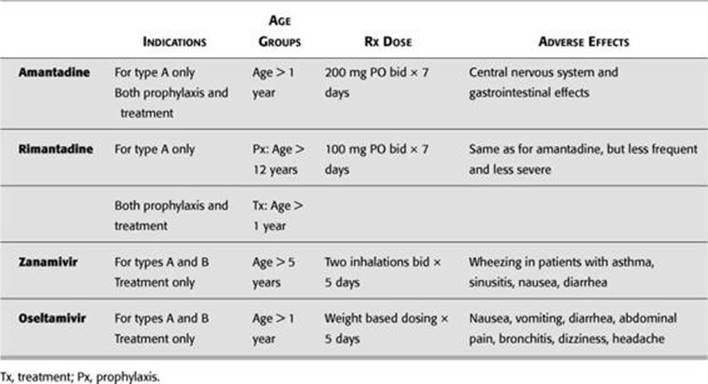
![]() For children at risk, see Table 12-2 for drug options.
For children at risk, see Table 12-2 for drug options.
![]() Pregnant patients with H1N1 should receive a 5-day course of antiviral treatment.
Pregnant patients with H1N1 should receive a 5-day course of antiviral treatment.
![]() Oseltamivir is preferred during pregnancy.
Oseltamivir is preferred during pregnancy.
VACCINE
Influenza can be severe in children with congenital heart disease, bronchopulmonary dysplasia (BPD), asthma, cystic fibrosis, and neuromuscular disease.
Intramuscular
![]() Now recommended for all children over age 6 months, with priority given to high-risk groups.
Now recommended for all children over age 6 months, with priority given to high-risk groups.
![]() High-risk groups include children with chronic diseases such as asthma, renal disease, diabetes, and any other form of immunosuppression.
High-risk groups include children with chronic diseases such as asthma, renal disease, diabetes, and any other form of immunosuppression.
![]() Best administered mid-September to mid-November since the peak of the flu season is late December to early March.
Best administered mid-September to mid-November since the peak of the flu season is late December to early March.
![]() Antibodies take up to 6 weeks to develop in children. Consider prophylaxis in high-risk children during this period.
Antibodies take up to 6 weeks to develop in children. Consider prophylaxis in high-risk children during this period.
![]() Since composition of influenza virus changes, the flu vaccine needs to be administered every year.
Since composition of influenza virus changes, the flu vaccine needs to be administered every year.
![]() Vaccine is a killed virus and therefore cannot cause the flu.
Vaccine is a killed virus and therefore cannot cause the flu.
![]() Not approved for children < 6 months of age.
Not approved for children < 6 months of age.
Intranasal
![]() Live, attenuated vaccine available for children > 5 years old.
Live, attenuated vaccine available for children > 5 years old.
![]() Not licensed for children with reactive airway disease.
Not licensed for children with reactive airway disease.
![]() Contraindicated in immunosuppressed individuals.
Contraindicated in immunosuppressed individuals.
TABLE 12 - 2. Drug Treatments for Influenza (All Pregnancy Category C)
H1N1 VACCINE
![]() Monovalent, inactivated influenza A virus vaccine.
Monovalent, inactivated influenza A virus vaccine.
![]() 6–35 months: 0.25 mL IM. Two doses 4 weeks apart.
6–35 months: 0.25 mL IM. Two doses 4 weeks apart.
![]() 3–9 years: 0.5 mL IM. Two doses 4 weeks apart.
3–9 years: 0.5 mL IM. Two doses 4 weeks apart.
![]() Intranasal:
Intranasal:
![]() Monovalent live virus vaccine.
Monovalent live virus vaccine.
![]() 2–9 years: 0.2 mL/dose (0.1 mL per nostril). Two doses 4 weeks apart.
2–9 years: 0.2 mL/dose (0.1 mL per nostril). Two doses 4 weeks apart.
PARAINFLUENZA
ETIOLOGY
![]() Type 1 and 2—seasonal.
Type 1 and 2—seasonal.
![]() Type 3—endemic.
Type 3—endemic.
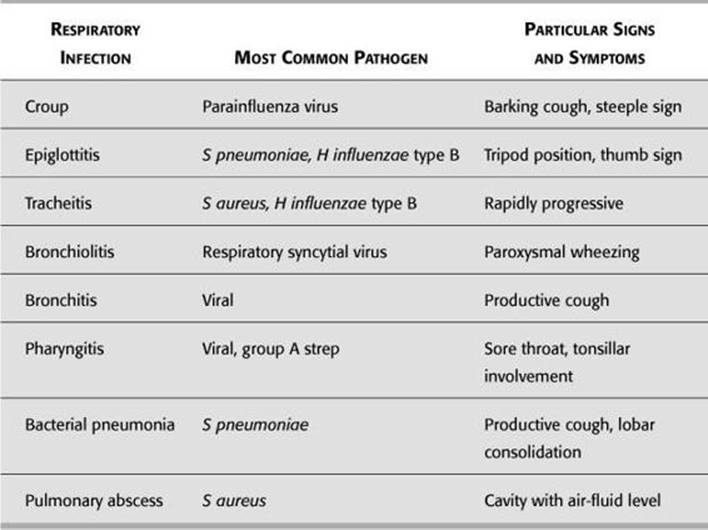
![]() See Table 12-3.
See Table 12-3.
Parainfluenza is a paramyxovirus.
SIGNS AND SYMPTOMS
![]() Incubation period: 2–6 days.
Incubation period: 2–6 days.
![]() Causes:
Causes:
![]() Colds
Colds
![]() Pharyngitis
Pharyngitis
![]() Otitis media
Otitis media
![]() Croup
Croup
![]() Bronchiolitis
Bronchiolitis
![]() Can be severe in immunocompromised patients
Can be severe in immunocompromised patients
TREATMENT
Specific antiviral therapy is not available.
Parainfluenza types 1 and 2 cause croup; type 3 causes bronchiolitis and pneumonia; type 4 is a cause of the common cold.
TABLE 12 - 3. Respiratory Infections and Pathogens
CROUP
Infectious Croup (Acute Laryngotracheobronchitis)
![]()
An 18-month-old boy with inspiratory stridor and a barking cough and agitation when lying down is brought at night to the emergency department (ED) by parents. He has had a sore throat and cough for 2 days. On examination, he has hoarseness, high-pitched barking cough, and stridor. In addition, tachypnea, retractions, and nasal flaring was noted. Steeple sign is seen on x-ray. Think: Croup.
Croup is the most common cause of stridor in a febrile child.
DEFINITION
Viral infection of upper respiratory tract.
Croup is the most common infectious cause of acute upper airway obstruction.
ETIOLOGY
Parainfluenza virus types 1 and 2.
Most common cause of stridor in children is croup.
EPIDEMIOLOGY
Occurs in children 3 months to 3 years of age in fall and winter months.
Stridor and distress at home and calm and free of stridor in ED: Think croup.
SIGNS AND SYMPTOMS
![]() Inspiratory stridor.
Inspiratory stridor.
![]() Seal-like, barking cough with retractions and nasal flaring.
Seal-like, barking cough with retractions and nasal flaring.
![]() May have coryza and fever.
May have coryza and fever.
![]() Can progress to agitation, hypoxemia, hypercapnia, tachypnea, and tachycardia.
Can progress to agitation, hypoxemia, hypercapnia, tachypnea, and tachycardia.
![]() Most cases are mild and last 3–7 days.
Most cases are mild and last 3–7 days.
![]() Symptoms worse at night, and typically worse on second day of illness.
Symptoms worse at night, and typically worse on second day of illness.
Constant stridor and distress both at home and ED despite treatment: Think tracheitis.
DIAGNOSIS
![]() X-ray usually not necessary. Consider only if diagnosis is in doubt.
X-ray usually not necessary. Consider only if diagnosis is in doubt.
![]() Steeple sign—narrowing of tracheal air column just below the vocal cords (see Figure 12-1).
Steeple sign—narrowing of tracheal air column just below the vocal cords (see Figure 12-1).
![]() Ballooning—distention of hypopharynx during inspiration.
Ballooning—distention of hypopharynx during inspiration.
![]() Differentiate croup from epiglottitis.
Differentiate croup from epiglottitis.
Minimum observation of child brought in with croup is 3 hours.
TREATMENT
![]() Position of comfort.
Position of comfort.
![]() Mild—symptomatic care, cool air, nonsteroidal anti-inflammatories (NSAIDs), consider corticosteroids.
Mild—symptomatic care, cool air, nonsteroidal anti-inflammatories (NSAIDs), consider corticosteroids.
![]() Moderate—racemic epinephrine (0.25 mL in 3–5 mL of normal saline [NS]), admit, early corticosteroids.
Moderate—racemic epinephrine (0.25 mL in 3–5 mL of normal saline [NS]), admit, early corticosteroids.
![]() Severe—racemic epinephrine, intensive care unit (ICU), early use of corticosteroids.
Severe—racemic epinephrine, intensive care unit (ICU), early use of corticosteroids.
![]() Dexamethasone 0.6 mg/kg (lower dose [0.15 mg/kg] has also shown be effective).
Dexamethasone 0.6 mg/kg (lower dose [0.15 mg/kg] has also shown be effective).
![]() Maximum: 10 mg/dose.
Maximum: 10 mg/dose.
![]() Admission criteria:
Admission criteria:
![]() Persistent stridor (especially at rest).
Persistent stridor (especially at rest).
![]() Respiratory distress.
Respiratory distress.
Reconsider diagnosis of croup if child is hypoxic.

FIGURE 12-1. Radiograph demonstrating steeple sign of croup.
Note narrowing of airway (arrow). (Courtesy of Dr. Gregory J. Schears.)
Stridor at rest is an indication for hospital admission.
![]() Multiple doses of racemic epinephrine.
Multiple doses of racemic epinephrine.
![]() Possibility of alternate diagnosis.
Possibility of alternate diagnosis.
CORTICOSTEROIDS IN RESPIRATORY PROBLEMS
![]() Dexamethasone (IM or PO 0.6 mg/kg).
Dexamethasone (IM or PO 0.6 mg/kg).
![]() Side effects associated with short-term steroid use are minimal.
Side effects associated with short-term steroid use are minimal.
Give corticosteroids to febrile child with stridor for:
![]() Croup
Croup
![]() Epiglottitis
Epiglottitis
![]() Retropharyngeal abscess
Retropharyngeal abscess
![]() Bacterial tracheitis
Bacterial tracheitis
Spasmodic Croup (Laryngismus Stridulus, Midnight Croup)
DEFINITION
![]() Recurrent, sudden onset of barking cough and inspiratory stridor without preceding respiratory tract infection.
Recurrent, sudden onset of barking cough and inspiratory stridor without preceding respiratory tract infection.
![]() Well known to physicians but still defies definition of pathogenesis.
Well known to physicians but still defies definition of pathogenesis.
![]() Familial predisposition: Family history of allergies.
Familial predisposition: Family history of allergies.
ETIOLOGY
![]() Probable viral etiology.
Probable viral etiology.
![]() Other considerations—allergic, psychological, gastroesophageal (GE) reflux.
Other considerations—allergic, psychological, gastroesophageal (GE) reflux.
Diagnosis of spasmodic croup can be made only on resolution of the symptoms.
EPIDEMIOLOGY
![]() Usually at night.
Usually at night.
![]() Aggravated by excitement.
Aggravated by excitement.
![]() Winter months.
Winter months.
![]() Occurs in children 1–3 years of age.
Occurs in children 1–3 years of age.
SIGNS AND SYMPTOMS
![]() Recurrent episodes of acute-onset barking cough and inspiratory stridor.
Recurrent episodes of acute-onset barking cough and inspiratory stridor.
![]() No symptoms of infection.
No symptoms of infection.
Steroids are not indicated in spasmodic croup.
DIAGNOSIS
Subglottic, noninflammatory edema.
TREATMENT
![]() Reassurance and cool mist.
Reassurance and cool mist.
![]() Spontaneous recovery.
Spontaneous recovery.
EPIGLOTTITIS
![]()
A 4-year-old boy brought to the ED is flushed, making high-pitched noises on forced inspiration, leaning forward in his mother’s lap, and drooling. His illness started with fever and sore throat and rapidly progressed to difficulty swallowing, drooling, restlessness, and stridor or air hunger. He appeared toxic and anxious. Lateral neck x-ray shows thumb sign. Think: Epiglottitis, and get him to an operating room (OR) to intubate and treat!
The classic presentation: “three Ds” (drooling, dysphagia, and distress).
See Figure 12-2.
Minutes count in acute epiglottitis.
DEFINITION
Acute, life-threatening infection of supraglottic tissues.
ETIOLOGY
![]() Haemophilus influenzae type B.
Haemophilus influenzae type B.
![]() Other possible pathogens—Streptococcus pyogenes, Streptococcus pneumoniae, Staphylococcus aureus.
Other possible pathogens—Streptococcus pyogenes, Streptococcus pneumoniae, Staphylococcus aureus.

FIGURE 12-2. Radiograph of lateral soft tissue of neck demonstrating epiglottitis.
Note the thickening of the epiglottic and ariepiglottic folds (arrows). (Reproduced, with permission, from Schwartz DT, Reisdorff BJ. Emergency Radiology. New York: McGraw-Hill, 2000: 608.)
PATHOPHYSIOLOGY
Acute inflammation and edema of epiglottis, aryepiglottic folds, and arytenoids.
EPIDEMIOLOGY
![]()
![]() incidence due to H influenzae type B vaccine (HiB).
incidence due to H influenzae type B vaccine (HiB).
![]() Usually 2–6 years of age, but can occur at any age.
Usually 2–6 years of age, but can occur at any age.
![]() Suspect in unvaccinated children.
Suspect in unvaccinated children.
![]() H influenzae immunization has practically eliminated epiglottitis in young children.
H influenzae immunization has practically eliminated epiglottitis in young children.
In doubtful cases, radiograph alone should not be used to diagnose epiglottitis.
SIGNS AND SYMPTOMS
![]() Sudden onset of inspiratory stridor and respiratory distress.
Sudden onset of inspiratory stridor and respiratory distress.
![]() Muffled voice (“hot potato” voice).
Muffled voice (“hot potato” voice).
![]() High fever (usually the first symptom).
High fever (usually the first symptom).
![]() Toxic appearing.
Toxic appearing.
![]() Tripod position—hyperextended neck, leaning forward, mouth open.
Tripod position—hyperextended neck, leaning forward, mouth open.
![]() Three D’s: Dysphagia, drooling, and distress.
Three D’s: Dysphagia, drooling, and distress.
![]() Cough (less frequent symptom)
Cough (less frequent symptom)
![]() Tachycardia is a constant feature.
Tachycardia is a constant feature.
![]() Severe respiratory distress develops within minutes to hours.
Severe respiratory distress develops within minutes to hours.
![]() May progress to restlessness, pallor/cyanosis, coma, death.
May progress to restlessness, pallor/cyanosis, coma, death.
DIAGNOSIS
![]() Laryngoscopy—swollen, cherry-red epiglottis.
Laryngoscopy—swollen, cherry-red epiglottis.
![]() Lateral neck x-ray to confirm (portable x-ray should be obtained).
Lateral neck x-ray to confirm (portable x-ray should be obtained).
![]() Swollen epiglottis (thumbprint sign).
Swollen epiglottis (thumbprint sign).
![]() Thickened aryepiglottic fold.
Thickened aryepiglottic fold.
![]() Obliteration of vallecula.
Obliteration of vallecula.
TREATMENT
![]() True medical emergency—potentially lethal airway obstruction.
True medical emergency—potentially lethal airway obstruction.
![]() Comfort.
Comfort.
![]() Anticipate.
Anticipate.
![]() Secure airway (endotracheal intubation in OR).
Secure airway (endotracheal intubation in OR).
![]() Ceftriaxone (100 mg/kg/day) 7–10 days.
Ceftriaxone (100 mg/kg/day) 7–10 days.
![]() Rifampin prophylaxis for close contacts.
Rifampin prophylaxis for close contacts.
Epiglottitis is a true medical emergency. If suspected, do not:
![]() Examine the throat
Examine the throat
![]() Use narcotics or sedatives, including antihistamines
Use narcotics or sedatives, including antihistamines
![]() Attempt venipuncture or other tests
Attempt venipuncture or other tests
![]() Place patient supine
Place patient supine
TRACHEITIS/LARYNGITIS
DEFINITION
Rapidly progressive upper airway obstruction due to infection of the trachea and/or larynx.
ETIOLOGY
![]() S aureus and H influenzae type b.
S aureus and H influenzae type b.
![]() Also Moraxella catarrhalis.
Also Moraxella catarrhalis.
![]() High association with preceding influenza A infection.
High association with preceding influenza A infection.
SIGNS AND SYMPTOMS
![]() Often present with croup symptoms. Differentiation can be made by the presence of:
Often present with croup symptoms. Differentiation can be made by the presence of:
![]() High fever
High fever
![]() Toxicity
Toxicity
![]() Inspiratory stridor (constant)
Inspiratory stridor (constant)
![]() Purulent sputum
Purulent sputum
![]() A toxic-appearing child with croupy symptoms who responds poorly to croup management should be evaluated for tracheitis.
A toxic-appearing child with croupy symptoms who responds poorly to croup management should be evaluated for tracheitis.
![]() Tracheitis has features of both croup (stridor and croupy cough) and epiglottitis (high fever and toxic appearance).
Tracheitis has features of both croup (stridor and croupy cough) and epiglottitis (high fever and toxic appearance).
Bacterial tracheitis has a slower onset than epiglottitis.
DIAGNOSIS
![]() X-ray—may be normal or identical to croup. Look for pseudomembrane on lateral view.
X-ray—may be normal or identical to croup. Look for pseudomembrane on lateral view.
![]() Epiglottis size normal
Epiglottis size normal
![]() Tracheal narrowing
Tracheal narrowing
![]() Pseudomembrane
Pseudomembrane
![]() Endoscopy.
Endoscopy.
![]() Copious purulent secretion distal to glottis.
Copious purulent secretion distal to glottis.
![]() Secretions should be obtained for Gram stain and culture.
Secretions should be obtained for Gram stain and culture.
TREATMENT
![]() Secure an adequate airway (endotracheal intubation):
Secure an adequate airway (endotracheal intubation):
![]() Should be performed in an operating room under anesthesia.
Should be performed in an operating room under anesthesia.
![]() Suction endotracheal tube of purulent material.
Suction endotracheal tube of purulent material.
![]() Specialty consultation: Ear, nose, and throat (ENT), and anesthesia.
Specialty consultation: Ear, nose, and throat (ENT), and anesthesia.
![]() Ceftriaxone 100 mg/kg/day.
Ceftriaxone 100 mg/kg/day.
![]() Ampicillin-sulbactam 200 mg/kg/day.
Ampicillin-sulbactam 200 mg/kg/day.
![]() ICU admission.
ICU admission.
BRONCHIOLITIS
![]()
A previously healthy 4-month-old who had rhinorrhea, cough, and a low-grade fever develops tachypnea, mild hypoxemia, and hyperinflation of lungs. Think: RSV bronchiolitis.
Classic presentation: Acute onset of cough, wheezing, and ![]() respiratory effort after an upper respiratory tract prodrome (fever and runny nose), during the winter season.
respiratory effort after an upper respiratory tract prodrome (fever and runny nose), during the winter season.
DEFINITION
Viral infection of upper and lower respiratory tract (medium and small airways).
ETIOLOGY
![]() RSV—most common cause.
RSV—most common cause.
![]() Adenovirus.
Adenovirus.
![]() Parainfluenza 3.
Parainfluenza 3.
![]() Influenza.
Influenza.
Bronchiolitis is the most common serious respiratory infection in children < 2 years.
![]() Human metapneumovirus (hMPV): First recognized in 2001 and now increasingly implicated.
Human metapneumovirus (hMPV): First recognized in 2001 and now increasingly implicated.
![]() Mycoplasma pneumoniae (rare).
Mycoplasma pneumoniae (rare).
PATHOPHYSIOLOGY
![]() Inflammatory obstruction (edema and mucus) of the bronchioles secondary to viral infection.
Inflammatory obstruction (edema and mucus) of the bronchioles secondary to viral infection.
![]() Alterations in gas exchange are most frequently the result of mismatching of pulmonary ventilation and perfusion.
Alterations in gas exchange are most frequently the result of mismatching of pulmonary ventilation and perfusion.
RSV causes more than 50% of cases of bronchiolitis.
EPIDEMIOLOGY
![]() Occurs in first 2 years of life.
Occurs in first 2 years of life.
![]() Reinfection is common.
Reinfection is common.
![]() Ninety percent are aged 1–9 months.
Ninety percent are aged 1–9 months.
![]() Occurs in winter and early spring.
Occurs in winter and early spring.
![]() Risks: Crowded conditions, not breast-fed, mothers who smoke, male gender.
Risks: Crowded conditions, not breast-fed, mothers who smoke, male gender.
![]() High-risk infants:
High-risk infants:
![]() Cardiac disease
Cardiac disease
![]() Pulmonary disease
Pulmonary disease
![]() Neuromuscular disease
Neuromuscular disease
![]() Premature infants
Premature infants
![]() Immunocompromised
Immunocompromised
Humans are the only source of RSV infection.
SIGNS AND SYMPTOMS
![]() Starts with mild respiratory illness.
Starts with mild respiratory illness.
![]() Respiratory distress gradually develops.
Respiratory distress gradually develops.
![]() Paroxysmal wheezing—common but may be absent, cough, dyspnea.
Paroxysmal wheezing—common but may be absent, cough, dyspnea.
![]() Apneic spells—young infants should be monitored.
Apneic spells—young infants should be monitored.
![]() Frequent complications include bacteremia, pericarditis, cellulitis, empyema, meningitis, and suppurative arthritis.
Frequent complications include bacteremia, pericarditis, cellulitis, empyema, meningitis, and suppurative arthritis.
![]() Most common complication is hypoxia.
Most common complication is hypoxia.
![]() Dehydration is the most common secondary complication.
Dehydration is the most common secondary complication.
Symptoms of asthma can be identical to bronchiolitis. Suspect asthma if:
![]() Family history
Family history
![]() Prior episodes
Prior episodes
![]() Response to bronchodilator
Response to bronchodilator
DIAGNOSIS
![]() Viral detection in nasopharyngeal secretions via culture, polymerase chain reaction (PCR), or antigen detection.
Viral detection in nasopharyngeal secretions via culture, polymerase chain reaction (PCR), or antigen detection.
![]() Chest x-ray (rule out pneumonia or foreign body)—hyperinflation of lungs,
Chest x-ray (rule out pneumonia or foreign body)—hyperinflation of lungs, ![]() anteroposterior (AP) diameter of rib cage.
anteroposterior (AP) diameter of rib cage.
![]() Oxygen saturation is the single best objective predictor.
Oxygen saturation is the single best objective predictor.
TREATMENT
![]() Low threshold for hospitalization for high-risk infants.
Low threshold for hospitalization for high-risk infants.
![]() Humidified oxygen.
Humidified oxygen.
![]() Trial of nebulized albuterol (only 20–50% are responders, discontinue if no objective benefit).
Trial of nebulized albuterol (only 20–50% are responders, discontinue if no objective benefit).
![]() Hypertonic saline—potential to reduce airway edema and mucous plugging.
Hypertonic saline—potential to reduce airway edema and mucous plugging.
![]() Steroids not indicated.
Steroids not indicated.
![]() Respiratory isolation.
Respiratory isolation.
![]() Ribavirin (aerosol form) if high-risk patients such as immunocompromised, need for mechanical ventilation, or < 6 weeks old.
Ribavirin (aerosol form) if high-risk patients such as immunocompromised, need for mechanical ventilation, or < 6 weeks old.
![]() RSV intravenous immune globulin (RSV-IVIG) or palivizumab given prior to and during RSV season in high-risk infants < 2 years old.
RSV intravenous immune globulin (RSV-IVIG) or palivizumab given prior to and during RSV season in high-risk infants < 2 years old.
Indications for rapid antigen detection in suspected RSV bronchiolitis: cohorting RSV-positive patient or to confirm RSV in high-risk patient.
BRONCHIECTASIS
![]()
A 7-year-old boy presents with an upper respiratory infection (URI) with productive cough (with purulent sputum). On examination, localized rales on the right side of his chest were noted. X-ray shows two discrete densities located in the right upper lobe of the lungs. Think: Bronchiectasis. Predisposition: Cystic fibrosis and ciliary dyskinesia.
DEFINITION
Abnormal and permanent dilatation of bronchi.
ETIOLOGY
![]() Viruses: Adenovirus, influenza virus.
Viruses: Adenovirus, influenza virus.
![]() Bacteria: S aureus, Klebsiella, anaerobes.
Bacteria: S aureus, Klebsiella, anaerobes.
![]() Primary ciliary dyskinesia.
Primary ciliary dyskinesia.
![]() Kartagener syndrome.
Kartagener syndrome.
![]() Cystic fibrosis: Pseudomonas aeruginosa.
Cystic fibrosis: Pseudomonas aeruginosa.
![]() α1-antitrypsin deficiency.
α1-antitrypsin deficiency.
PATHOPHYSIOLOGY
Consequence of inflammation and destruction of structural components of bronchial wall.
SIGNS AND SYMPTOMS
![]() Physical exam quite variable.
Physical exam quite variable.
![]() Persistent or recurrent cough.
Persistent or recurrent cough.
![]() Purulent sputum.
Purulent sputum.
![]() Hemoptysis.
Hemoptysis.
![]() Dyspnea.
Dyspnea.
![]() Wheezing.
Wheezing.
![]() Clubbing.
Clubbing.
DIAGNOSIS
![]() Chest x-ray.
Chest x-ray.
![]() Bronchography.
Bronchography.
![]() Computed tomographic (CT) scan.
Computed tomographic (CT) scan.
![]() Sputum culture.
Sputum culture.
TREATMENT
![]() Elimination of underlying cause.
Elimination of underlying cause.
![]() Clearance of secretion.
Clearance of secretion.
![]() Chest physiotherapy.
Chest physiotherapy.
![]() Mucolytic agents.
Mucolytic agents.
![]() Control of infection—antibiotics.
Control of infection—antibiotics.
![]() Reversal of airflow obstruction—bronchodilators.
Reversal of airflow obstruction—bronchodilators.
BRONCHITIS
DEFINITION
Infection of conductive airways of lung.
Cough is the most common symptom of chronic bronchitis.
ETIOLOGY
![]() Viruses: Influenza A and B, adenovirus, parainfluenza, rhinovirus, RSV, coxsackievirus.
Viruses: Influenza A and B, adenovirus, parainfluenza, rhinovirus, RSV, coxsackievirus.
![]() Bacteria: Bordetella pertussis, M pneumoniae, Chlamydia pneumoniae, S pneumoniae.
Bacteria: Bordetella pertussis, M pneumoniae, Chlamydia pneumoniae, S pneumoniae.
SIGNS AND SYMPTOMS
![]() Acute productive cough (< 1 week).
Acute productive cough (< 1 week).
![]() Rhinitis.
Rhinitis.
![]() Myalgia.
Myalgia.
![]() Fever.
Fever.
![]() No evidence of sinusitis, pneumonia, or chronic pulmonary disease.
No evidence of sinusitis, pneumonia, or chronic pulmonary disease.
![]() Normal arterial oxygenation.
Normal arterial oxygenation.
TREATMENT
![]() Mostly self-limited.
Mostly self-limited.
![]() Bronchodilators may help.
Bronchodilators may help.
![]() Antibiotics for high-risk patients.
Antibiotics for high-risk patients.
Pharyngitis is the second most common diagnosis in children aged 1–15 years in the pediatric clinic.
PHARYNGITIS
DEFINITION
Infection of the tonsils and/or the pharynx.
Viruses (most common cause of pharyngitis): Rhinovirus, adenovirus, coxsackievirus.
ETIOLOGY
SIGNS AND SYMPTOMS
![]() Viral pharyngitis:
Viral pharyngitis:
![]() Gradual onset.
Gradual onset.
![]() Fever, malaise, throat pain.
Fever, malaise, throat pain.
![]() Conjunctivitis, rhinitis, coryza, viral exanthem, diarrhea.
Conjunctivitis, rhinitis, coryza, viral exanthem, diarrhea.
![]() Streptococcal pharyngitis (> 2 years) (see Figure 12-3):
Streptococcal pharyngitis (> 2 years) (see Figure 12-3):
![]() Headache, abdominal pain, and vomiting.
Headache, abdominal pain, and vomiting.
![]() Fever (> 104°F [40°C]).
Fever (> 104°F [40°C]).
![]() Tonsillar enlargement with exudates.
Tonsillar enlargement with exudates.
![]() Fetid odor.
Fetid odor.
![]() Cervical adenopathy.
Cervical adenopathy.
![]() Palatal petechiae and uvular edema.
Palatal petechiae and uvular edema.
![]() It is not possible to distinguish clinically viral from bacterial pharyngitis, though high fever, cervical adenopathy, and absence of URI symptoms suggest bacterial etiology.
It is not possible to distinguish clinically viral from bacterial pharyngitis, though high fever, cervical adenopathy, and absence of URI symptoms suggest bacterial etiology.
Acute rheumatic fever occurs more after throat than skin infections and in children who have had acute rheumatic fever before.

FIGURE 12-3. Streptococcal pharyngitis.
Note white exudates on top of erythematous swollen tonsils.
DIAGNOSIS
Rapid (DNase) antigen detection test (sensitivity 95–98%):
![]() Culture if negative.
Culture if negative.
![]() Treat if positive.
Treat if positive.
TREATMENT
![]() Oral penicillin (25–50 mg/kg/day) for 10 days.
Oral penicillin (25–50 mg/kg/day) for 10 days.
![]() Alternatively, intramuscular (IM) benzathine and procaine penicillin can be used (single dose, weight based).
Alternatively, intramuscular (IM) benzathine and procaine penicillin can be used (single dose, weight based).
![]() Macrolides or clindamycin for penicillin-allergic patients for 10 days.
Macrolides or clindamycin for penicillin-allergic patients for 10 days.
![]() Tetracycline and sulfonamides should not be used to treat group A beta-hemolytic streptococci (GABHS).
Tetracycline and sulfonamides should not be used to treat group A beta-hemolytic streptococci (GABHS).
![]() Antibiotics are not indicated for pharyngitis negative for GABHS.
Antibiotics are not indicated for pharyngitis negative for GABHS.
Penicillin remains the drug of choice for GABHS.
COMPLICATIONS
![]() Suppurative:
Suppurative:
![]() Peritonsillar abscess
Peritonsillar abscess
![]() Retropharyngeal abscess
Retropharyngeal abscess
![]() Cervical adenitis
Cervical adenitis
![]() Otitis media
Otitis media
![]() Sinusitis
Sinusitis
![]() Nonsuppurative:
Nonsuppurative:
![]() Acute glomerulonephritis
Acute glomerulonephritis
![]() Acute rheumatic fever
Acute rheumatic fever
The more mucous membranes involved, the more likely an infection is viral.
PNEUMONIA
![]()
A 2-month-old with fever, tachypnea, and mottled skin has a chest x-ray showing infiltrate of the right upper lung lobe, a pneumatocele, and a pleural effusion. Think: S aureus pneumonia.
![]()
A previously healthy 9-year-old boy has a 7-day history of increasing cough, low-grade fever, and fatigue on exertion. Chest x-ray shows widespread diffuse perihilar infiltrates. Think: Mycoplasma pneumonia. Initially, nonproductive cough and no fever. Later, productive cough with fever, headache, coryza, otitis media, and malaise.
DEFINITION
Inflammation of lung parenchyma.
Round pulmonary infiltrate on chest x-ray. Think: S pneumoniae pneumonia.
ETIOLOGY
![]() Viruses: RSV, influenza, parainfluenza, adenovirus.
Viruses: RSV, influenza, parainfluenza, adenovirus.
![]() Bacteria: Less common, but more severe—S pneumoniae, S pyogenes, S aureus, H influenzae type B, M pneumoniae.
Bacteria: Less common, but more severe—S pneumoniae, S pyogenes, S aureus, H influenzae type B, M pneumoniae.
Pneumonia with hilar adenopathy on chest x-ray. Think: Adenovirus. However, it is difficult to make an accurate etiologic diagnosis only on the basis of clinical presentation.
SIGNS AND SYMPTOMS
![]() Tachypnea, dyspnea.
Tachypnea, dyspnea.
![]() Fever and feeding difficulty (infant).
Fever and feeding difficulty (infant).
![]() Productive cough, chest pain (children).
Productive cough, chest pain (children).
![]() Chlamydia trachomatis (pneumonitis syndrome).
Chlamydia trachomatis (pneumonitis syndrome).
![]() Occurs in children 1–3 months of age.
Occurs in children 1–3 months of age.
![]() Staccato cough, tachypnea, progressive respiratory distress.
Staccato cough, tachypnea, progressive respiratory distress.
![]() Lack of fever and other systemic signs.
Lack of fever and other systemic signs.
![]() Conjunctivitis.
Conjunctivitis.
The most reliable sign of pneumonia is tachypnea.
DIAGNOSIS
![]() Chest x-ray (Figure 12-4):
Chest x-ray (Figure 12-4):
![]() Viral (hyperinflation, perihilar infiltrate, hilar adenopathy, and atelectasis).
Viral (hyperinflation, perihilar infiltrate, hilar adenopathy, and atelectasis).
![]() Bacterial (alveolar consolidation).
Bacterial (alveolar consolidation).
![]() Mycoplasma (interstitial infiltrates).
Mycoplasma (interstitial infiltrates).
![]() Tuberculosis (hilar adenopathy).
Tuberculosis (hilar adenopathy).
![]() Pneumocystis (reticulonodular infiltrates).
Pneumocystis (reticulonodular infiltrates).
![]() Blood culture (positive in 10–30% of bacterial cases).
Blood culture (positive in 10–30% of bacterial cases).
Consider pneumonia in children with neck stiffness or acute abdominal pain.

FIGURE 12-4. Chest x-ray demonstrating diffuse bilateral pulmonary infiltrates.
Note tip of endotracheal tube (arrow) is in good position.
In young children, auscultation may be normal with impressive x-ray findings.
TREATMENT
![]() Inpatient:
Inpatient:
![]() 1–3 months old: Macrolide (pneumonitis syndrome) or third-generation cephalosporin.
1–3 months old: Macrolide (pneumonitis syndrome) or third-generation cephalosporin.
![]() ≥ 3 months and older: Third-generation cephalosporin.
≥ 3 months and older: Third-generation cephalosporin.
![]() Outpatient:
Outpatient:
![]() Patients should have normal O2 saturation and be able to take oral fluids in order to be outpatients.
Patients should have normal O2 saturation and be able to take oral fluids in order to be outpatients.
![]() Amoxicillin or erythromycin.
Amoxicillin or erythromycin.
PERTUSSIS
DEFINITION
![]() “Whooping cough.”
“Whooping cough.”
![]() Highly infectious form of bronchitis.
Highly infectious form of bronchitis.
ETIOLOGY
![]() Bordetella pertussis gram-negative coccobacilli.
Bordetella pertussis gram-negative coccobacilli.
![]() Humans are the only known host.
Humans are the only known host.
![]() Whooping cough syndrome also may be caused by:
Whooping cough syndrome also may be caused by:
![]() Bordetella parapertussis
Bordetella parapertussis
![]() M pneumoniae
M pneumoniae
![]() C trachomatis
C trachomatis
![]() C pneumoniae
C pneumoniae
![]() Adenoviruses
Adenoviruses
Pertussis means “intense cough.”
PATHOPHYSIOLOGY
![]() Pertussis toxin is a virulence protein that causes lymphocytosis and systemic manifestations.
Pertussis toxin is a virulence protein that causes lymphocytosis and systemic manifestations.
![]() Aerosol droplet transmission.
Aerosol droplet transmission.
Despite having “whooping cough,” most patients with pertussis do not whoop.
EPIDEMIOLOGY
![]() Endemic, but epidemic every 3–4 years.
Endemic, but epidemic every 3–4 years.
![]() 60 million cases/year worldwide.
60 million cases/year worldwide.
![]() 500,000 deaths/year worldwide.
500,000 deaths/year worldwide.
![]() July to October.
July to October.
![]() Occurs in 1- to 5-year-olds worldwide, 50% < 1-year-olds in United States.
Occurs in 1- to 5-year-olds worldwide, 50% < 1-year-olds in United States.
With pertussis, fever may be absent or minimal; cough may be only complaint.
SIGNS AND SYMPTOMS
![]() Incubation period 1–2 weeks.
Incubation period 1–2 weeks.
![]() Three stages: Catarrhal, paroxysmal, and convalescent.
Three stages: Catarrhal, paroxysmal, and convalescent.
![]() Duration: 6 weeks.
Duration: 6 weeks.
![]() Catarrhal stage: Congestion and rhinorrhea.
Catarrhal stage: Congestion and rhinorrhea.
![]() Paroxysmal stage (2–4 weeks):
Paroxysmal stage (2–4 weeks):
![]() Paroxysmal cough, with characteristic whoop following (chin forward, tongue out, watery, bulging eyes, purple face).
Paroxysmal cough, with characteristic whoop following (chin forward, tongue out, watery, bulging eyes, purple face).
![]() Fever is typically absent.
Fever is typically absent.
![]() Post-tussive emesis and exhaustion.
Post-tussive emesis and exhaustion.
Apnea is common in infants with pertussis.
![]() Convalescent stage: Number and severity of paroxysms plateaus.
Convalescent stage: Number and severity of paroxysms plateaus.
![]() Each stage lasts ∼ 2 weeks; shorter if immunized.
Each stage lasts ∼ 2 weeks; shorter if immunized.
![]() Complications include apnea, physical sequelae of forceful coughing, brain hypoxia/hemorrhage, secondary infections (bacterial pneumonia is the cause of death).
Complications include apnea, physical sequelae of forceful coughing, brain hypoxia/hemorrhage, secondary infections (bacterial pneumonia is the cause of death).
Suspect pertussis if paroxysmal cough with color change.
DIAGNOSIS
![]() Diagnosis is primarily clinical:
Diagnosis is primarily clinical:
![]() Inspiratory whoop
Inspiratory whoop
![]() Post-tussive emesis
Post-tussive emesis
![]() Lymphocytosis
Lymphocytosis
![]() Chest x-ray—perihilar infiltrate or edema (butterfly pattern).
Chest x-ray—perihilar infiltrate or edema (butterfly pattern).
![]() Positive immunofluorescence test or PCR on nasopharyngeal secretions.
Positive immunofluorescence test or PCR on nasopharyngeal secretions.
No single serologic test is diagnostic for pertussis.
TREATMENT
![]() Goal—to
Goal—to ![]() spread of organism. Antibiotics do not affect illness in paroxysmal stage, which is toxin mediated.
spread of organism. Antibiotics do not affect illness in paroxysmal stage, which is toxin mediated.
![]() Macrolide antibiotic for patient and household contacts.
Macrolide antibiotic for patient and household contacts.
![]() Isolation until 5 days of therapy.
Isolation until 5 days of therapy.
![]() Admit if:
Admit if:
![]() Infant < 3 months.
Infant < 3 months.
![]() Apnea.
Apnea.
![]() Cyanosis.
Cyanosis.
![]() Respiratory distress.
Respiratory distress.
![]() DTP (diphtheria, tetanus, pertussis)/DTaP (diphtheria, tetanus, acellular pertussis) vaccine.
DTP (diphtheria, tetanus, pertussis)/DTaP (diphtheria, tetanus, acellular pertussis) vaccine.
There is a risk of hypertrophic pyloric stenosis in infants younger than 6 weeks treated with oral erythromycin.
DIPHTHERIA
DEFINITION
Membranous nasopharyngitis or obstructive laryngotracheitis.
ETIOLOGY
![]() Corynebacterium diphtheriae.
Corynebacterium diphtheriae.
![]() Humans are the only reservoir.
Humans are the only reservoir.
SIGNS AND SYMPTOMS
![]() Incubation period: 2–7 days.
Incubation period: 2–7 days.
![]() Erosive rhinitis with membrane formation.
Erosive rhinitis with membrane formation.
![]() Tonsillopharyngeal—sore throat, membranous exudate.
Tonsillopharyngeal—sore throat, membranous exudate.
![]() Cardiac symptoms.
Cardiac symptoms.
![]() Tachycardia out of proportion to fever.
Tachycardia out of proportion to fever.
DIAGNOSIS
![]() Culture (nose, throat, mucosal, or cutaneous lesion).
Culture (nose, throat, mucosal, or cutaneous lesion).
![]() Material should be obtained from beneath the membrane or a portion of membrane.
Material should be obtained from beneath the membrane or a portion of membrane.
![]() All C diphtheriae isolates should be sent to diphtheria laboratory.
All C diphtheriae isolates should be sent to diphtheria laboratory.
For treatment of diphtheria, antibiotics are not a substitute for antitoxin.
TREATMENT
Most tuberculosis infections in children are asymptomatic with positive PPD.
![]() Antitoxin—dose depends on:
Antitoxin—dose depends on:
![]() Site of membrane
Site of membrane
![]() Degree of toxic effects
Degree of toxic effects
![]() Duration of illness
Duration of illness
![]() Antibiotics:
Antibiotics:
![]() Erythromycin or penicillin G for 14 days.
Erythromycin or penicillin G for 14 days.
![]() Elimination of organism should be documented by two consecutive cultures.
Elimination of organism should be documented by two consecutive cultures.
A patient may develop TB despite prior bacillus Calmette-Guérin (BCG) vaccination.
TUBERCULOSIS (TB)
DEFINITION
![]() Signs and symptoms and/or radiographic manifestations caused by M tuberculosis are apparent.
Signs and symptoms and/or radiographic manifestations caused by M tuberculosis are apparent.
![]() May be pulmonary, extrapulmonary, or both.
May be pulmonary, extrapulmonary, or both.
ETIOLOGY
Mycobacterium tuberculosis.
A positive PPD skin test results from infection, not from exposure.
PATHOPHYSIOLOGY
Primary portal of entry into children is lung.
Asymptomatic children with a positive PPD should be considered infected and get treatment.
EPIDEMIOLOGY
![]() Children are never the primary source (look for adult contacts).
Children are never the primary source (look for adult contacts).
![]() Risk factors:
Risk factors:
![]() Urban living
Urban living
![]() Low income
Low income
![]() Recent immigrants
Recent immigrants
![]() HIV
HIV
All cases of active TB should be referred to public health department.
SIGNS AND SYMPTOMS
![]() Chronic cough (nonproductive)
Chronic cough (nonproductive)
![]() Hemoptysis
Hemoptysis
![]() Fever
Fever
![]() Night sweats
Night sweats
![]() Weight loss
Weight loss
![]() Anorexia
Anorexia
![]() Lymphadenopathy
Lymphadenopathy
![]() Present to ED with:
Present to ED with:
![]() Primary pneumonia
Primary pneumonia
![]() Miliary TB (may mimic sepsis)
Miliary TB (may mimic sepsis)
DIAGNOSIS
![]() When to suspect TB:
When to suspect TB:
![]() Hilar adenopathy.
Hilar adenopathy.
![]() Pulmonary calcification.
Pulmonary calcification.
![]() Pneumonia with infiltrate and adenopathy.
Pneumonia with infiltrate and adenopathy.
![]() Pneumonia with pleural effusion.
Pneumonia with pleural effusion.
![]() Painless unilateral cervical adenopathy (scrofula).
Painless unilateral cervical adenopathy (scrofula).
![]() Meningitis of insidious onset.
Meningitis of insidious onset.
Persons with TB should be tested for HIV.
![]() Bone or joint disease.
Bone or joint disease.
![]() When any of the above are unresponsive to antibiotics.
When any of the above are unresponsive to antibiotics.
![]() PPD test (Mantoux test).
PPD test (Mantoux test).
![]() QuantiFERON®-TB Gold test.
QuantiFERON®-TB Gold test.
![]() Culture (gastric aspirates, sputum, pleural fluid, cerebrospinal fluid, urine, or other body fluids).
Culture (gastric aspirates, sputum, pleural fluid, cerebrospinal fluid, urine, or other body fluids).
![]() Look for the adult source.
Look for the adult source.
![]() Acid-fast stain or PCR.
Acid-fast stain or PCR.
TREATMENT
![]() Two to four or more drugs (isoniazid, rifampin, pyrazinamide, ethambutol, streptomycin) for a minimum of 6 months for active disease.
Two to four or more drugs (isoniazid, rifampin, pyrazinamide, ethambutol, streptomycin) for a minimum of 6 months for active disease.
![]() Isoniazid for 9 months for latent disease.
Isoniazid for 9 months for latent disease.
TB in children < 4 years of age is much more likely to disseminate; prompt and vigorous treatment should be started when the diagnosis is suspected.
CYSTIC FIBROSIS (CF)
![]()
A 3-year-old child presents with constant cough with sputum. He has had six episodes of pneumonia, with Pseudomonas being isolated from sputum; loose stools; and is at the 20th percentile for growth. Think: CF.
CF is an inherited multisystem disorder resulting in chronic lung disease, exocrine pancreatic insufficiency, and failure to thrive.
Cystic fibrosis is the most common lethal inherited disease of Caucasians.
DEFINITION
Disease of exocrine glands that causes viscous secretions:
![]() Chronic respiratory infection
Chronic respiratory infection
![]() Pancreatic insufficiency
Pancreatic insufficiency
![]()
![]() electrolytes in sweat
electrolytes in sweat
ETIOLOGY
![]() Defect of cyclic adenosine monophosphate (cAMP)-activated chloride channel of epithelial cells in pancreas, sweat glands, salivary glands, intestines, respiratory tract, and reproductive system.
Defect of cyclic adenosine monophosphate (cAMP)-activated chloride channel of epithelial cells in pancreas, sweat glands, salivary glands, intestines, respiratory tract, and reproductive system.
![]() Autosomal recessive.
Autosomal recessive.
The gene for cystic fibrosis is CFTR; the mutation is delta F508.
PATHOPHYSIOLOGY
![]() Chloride does not exit from cells.
Chloride does not exit from cells.
![]()
![]() osmotic pressure inside cells attracts water and
osmotic pressure inside cells attracts water and ![]() thick secretions.
thick secretions.
EPIDEMIOLOGY
![]() Most common cause of severe, chronic lung disease in children.
Most common cause of severe, chronic lung disease in children.
![]() One in 2000–3000 live births (Caucasians).
One in 2000–3000 live births (Caucasians).
SIGNS AND SYMPTOMS
![]() Respiratory:
Respiratory:
![]() Cough—most common pulmonary symptom.
Cough—most common pulmonary symptom.
![]() Wheezing, dyspnea, exercise intolerance.
Wheezing, dyspnea, exercise intolerance.
![]() Bronchiectasis, recurrent pneumonia.
Bronchiectasis, recurrent pneumonia.
![]() Sinusitis, nasal polyps.
Sinusitis, nasal polyps.
![]() Reactive airway disease, hemoptysis.
Reactive airway disease, hemoptysis.
A patient with severe CF breathing room air can have an arterial blood gas (ABG) showing ![]() chloride and
chloride and ![]() bicarbonate.
bicarbonate.
![]()
![]() AP chest diameter.
AP chest diameter.
![]() Hyperresonant lungs.
Hyperresonant lungs.
![]() Clubbing of nails.
Clubbing of nails.
![]() Gastrointestinal (GI):
Gastrointestinal (GI):
![]() Failure to thrive.
Failure to thrive.
![]() Meconium ileus (10%).
Meconium ileus (10%).
![]() Constipation, rectal prolapse.
Constipation, rectal prolapse.
![]() Intestinal obstruction.
Intestinal obstruction.
![]() Pancreatic insufficiency:
Pancreatic insufficiency:
![]() Malabsorption.
Malabsorption.
![]() Fat-soluble vitamin deficiencies.
Fat-soluble vitamin deficiencies.
![]() Glucose intolerance.
Glucose intolerance.
![]() Biliary cirrhosis (uncommon): Jaundice, ascites, hematemesis from esophageal varices
Biliary cirrhosis (uncommon): Jaundice, ascites, hematemesis from esophageal varices
![]() Reproductive tract:
Reproductive tract: ![]() /absent fertility—female, thick cervical secretions; male, azoospermic.
/absent fertility—female, thick cervical secretions; male, azoospermic.
![]() Sweat glands:
Sweat glands:
![]() Salty skin.
Salty skin.
![]() Hypochloremic alkalosis in severe cases.
Hypochloremic alkalosis in severe cases.
![]() Complications may include pneumothorax, chronic pulmonary hypertension, cor pulmonale, atelectasis, allergic bronchopulmonary aspergillosis, respiratory failure, gastroesophageal reflux.
Complications may include pneumothorax, chronic pulmonary hypertension, cor pulmonale, atelectasis, allergic bronchopulmonary aspergillosis, respiratory failure, gastroesophageal reflux.
False-positive sweat test (not CF):
![]() Nephrogenic diabetes insipidus
Nephrogenic diabetes insipidus
![]() Myxedema
Myxedema
![]() Mucopolysaccharidosis
Mucopolysaccharidosis
![]() Adrenal insufficiency
Adrenal insufficiency
![]() Ectodermal dysplasia
Ectodermal dysplasia
DIAGNOSIS
![]() Sweat test—chloride concentration > 60 mEq/L (gold standard).
Sweat test—chloride concentration > 60 mEq/L (gold standard).
![]() Genetic studies.
Genetic studies.
![]() In utero screen available.
In utero screen available.
![]() Pulmonary function tests (PFTs): Obstructive and restrictive abnormalities.
Pulmonary function tests (PFTs): Obstructive and restrictive abnormalities.
![]() Prenatal diagnosis via gene proves CF mutations or linkage analysis.
Prenatal diagnosis via gene proves CF mutations or linkage analysis.
TREATMENT
![]() Multidisciplinary team approach—pediatrician, physiotherapist, dietitian, nursing staff, teacher, child, and parents.
Multidisciplinary team approach—pediatrician, physiotherapist, dietitian, nursing staff, teacher, child, and parents.
![]() Respiratory:
Respiratory:
![]() Chest physical therapy.
Chest physical therapy.
![]() Exercise.
Exercise.
![]() Coughing to move secretions and mucous plugs.
Coughing to move secretions and mucous plugs.
![]() Bronchodilators.
Bronchodilators.
![]() Normal saline aerosol.
Normal saline aerosol.
![]() Anti-inflammatory medications.
Anti-inflammatory medications.
![]() Dornase-alpha nebulizer (breaks down DNA in mucus).
Dornase-alpha nebulizer (breaks down DNA in mucus).
![]() Pancreatic/digestive:
Pancreatic/digestive:
![]() Enteric coated pancreatic enzyme supplements (add to all meals).
Enteric coated pancreatic enzyme supplements (add to all meals).
![]() Fat-soluble vitamin supplements.
Fat-soluble vitamin supplements.
![]() High-calorie, high-protein diet.
High-calorie, high-protein diet.
![]() Antibiotics—sputum cultures used to guide antibiotic choice. Pseudomonal infections are especially common.
Antibiotics—sputum cultures used to guide antibiotic choice. Pseudomonal infections are especially common.
![]() Lung transplant.
Lung transplant.
![]() Gene therapy is being aggressively studied.
Gene therapy is being aggressively studied.
Features of CF: CF PANCREAS
Chronic cough
Failure to thrive
Pancreatic insufficiency
Alkalosis
Nasal polyps
Clubbing
Rectal prolapse
Electrolytes ![]() in sweat
in sweat
Absence of vas
Sputum mucoid
PROGNOSIS
Advances in therapy have ![]() life expectancy into adulthood.
life expectancy into adulthood.
Ninety-nine percent of cases of meconium ileus are due to CF.
TONSILS/ADENOIDS
Tonsillitis/Adenoiditis
DEFINITION
Inflammation of:
![]() Tonsils—two faucial tonsils.
Tonsils—two faucial tonsils.
![]() Adenoids—nasopharyngeal tonsils.
Adenoids—nasopharyngeal tonsils.
SIGNS AND SYMPTOMS
![]() Sore throat.
Sore throat.
![]() Pain with swallowing.
Pain with swallowing.
![]() May have whitish exudate on tonsils.
May have whitish exudate on tonsils.
![]() Chronic tonsillitis:
Chronic tonsillitis:
![]() Seven in past year.
Seven in past year.
![]() Five in each of the past 2 years.
Five in each of the past 2 years.
![]() Three in each of the past 3 years.
Three in each of the past 3 years.
Fat-soluble vitamin deficiencies:
A—night blindness
D—![]() bone density
bone density
E—neurologic dysfunction
K—bleeding
TREATMENT
![]() < 2–3 years old: Tonsillectomy is performed for obstructive sleep symptoms.
< 2–3 years old: Tonsillectomy is performed for obstructive sleep symptoms.
![]() Large size alone is not an indication to remove tonsils.
Large size alone is not an indication to remove tonsils.
Enlarged Adenoids
DEFINITION
Nasopharyngeal lymphoid tissue.
Tonsils and adenoids are part of Waldeyer’s ring that circles the pharynx.
SIGNS AND SYMPTOMS
![]() Mouth breathing
Mouth breathing
![]() Persistent rhinitis
Persistent rhinitis
![]() Snoring
Snoring
It can be normal for tonsils to be relatively large during childhood.
DIAGNOSIS
![]() Digital palpation
Digital palpation
![]() Indirect laryngoscopy
Indirect laryngoscopy
TREATMENT
![]() Adenoidectomy:
Adenoidectomy:
![]() Persistent mouth breathing.
Persistent mouth breathing.
![]() Hyponasal speech.
Hyponasal speech.
![]() Adenoid facies.
Adenoid facies.
![]() Recurrent otitis media or nasopharyngitis.
Recurrent otitis media or nasopharyngitis.
![]() Tonsillectomy should not be performed routinely unless separate indication exists.
Tonsillectomy should not be performed routinely unless separate indication exists.
Peritonsillar Abscess
DEFINITION
Walled-off infection occurring in the space between the superior pharyngeal constrictor muscle and tonsils.
ETIOLOGY
![]() GABHS
GABHS
![]() Anaerobes
Anaerobes
EPIDEMIOLOGY
Usually preadolescent.
Trismus is limited opening of the mouth.
SIGNS AND SYMPTOMS
![]() Preceded by acute tonsillopharyngitis.
Preceded by acute tonsillopharyngitis.
![]() Severe throat pain.
Severe throat pain.
![]() Trismus.
Trismus.
![]() Refusal to swallow or speak.
Refusal to swallow or speak.
![]() “Hot potato voice.”
“Hot potato voice.”
![]() Markedly swollen and inflamed tonsils.
Markedly swollen and inflamed tonsils.
![]() Uvula displaced to opposite side.
Uvula displaced to opposite side.
TREATMENT
![]() Antibiotics covering staph and strep. Typically, ampicillin—sulbactam.
Antibiotics covering staph and strep. Typically, ampicillin—sulbactam.
![]() Incision and drainage.
Incision and drainage.
RETROPHARYNGEAL ABSCESS
DEFINITION
Potential space between the posterior pharyngeal wall and the prevertebral fascia. Commonly occurs in children < 5 years old.
ETIOLOGY
Usually a complication of pharyngitis:
![]() GABHS
GABHS
![]() Oral anaerobes
Oral anaerobes
![]() S aureus
S aureus
SIGNS AND SYMPTOMS
![]() Sudden onset of high fever with difficulty in swallowing.
Sudden onset of high fever with difficulty in swallowing.
![]() Refusal of feeding.
Refusal of feeding.
![]() Throat pain.
Throat pain.
![]() Hyperextension of the head.
Hyperextension of the head.
![]() Toxicity is common.
Toxicity is common.
![]() May cause meningismus—extension of the neck causes pain.
May cause meningismus—extension of the neck causes pain.
DIAGNOSIS
Lateral neck x-ray: Normal retropharyngeal space should be less than one-half of width of adjacent vertebra (see Figure 12–5).
TREATMENT
Clindamycin or ampicillin-sulbactam.
Lymph nodes in the retropharyngeal space usually disappear by the third to fourth year of life.

FIGURE 12-5. Lateral radiograph of the soft tissue of the neck.
Note the large amount of prevertebral edema (solid arrow) and the collection of air (dashed arrow). Findings are consistent with retropharyngeal abscess. (Courtesy of Dr. Gregory J. Sc-hears.)
ASTHMA
![]()
A 5-year-old boy with a history of sleeping problems presents with a non-productive nocturnal cough and shortness of breath and cough during exercise. Think: Asthma.
Start on a trial of a bronchodilator, which is helpful in confirming the diagnosis by the demonstration of reversible airways obstruction (![]() in forced expiratory volume in 1 second [FEV1]). Asthma is an inflammatory disease. Diagnosis of asthma should be considered in the presence of recurrent wheezing in a child with a family history of asthma.
in forced expiratory volume in 1 second [FEV1]). Asthma is an inflammatory disease. Diagnosis of asthma should be considered in the presence of recurrent wheezing in a child with a family history of asthma.
DEFINITION
Respiratory hypersensitivity, inflammation, and reversible airway obstruction.
ETIOLOGY
Hyperresponsiveness to a variety of stimuli:
![]() Respiratory infection
Respiratory infection
![]() Air pollutants
Air pollutants
![]() Allergens
Allergens
![]() Foods
Foods
![]() Exercise
Exercise
![]() Emotions
Emotions
Asthma is the most common chronic lung disease in children.
PATHOPHYSIOLOGY
![]() Bronchospasm (acute).
Bronchospasm (acute).
![]() Mucus production (acute).
Mucus production (acute).
Lack of wheezing does not exclude asthma.
![]() Inflammation and edema of the airway mucosa (chronic).
Inflammation and edema of the airway mucosa (chronic).
![]() Two types:
Two types:
![]() Extrinsic:
Extrinsic:
![]() Immunologically mediated
Immunologically mediated
![]() Develop in childhood
Develop in childhood
![]() Intrinsic:
Intrinsic:
![]() No identifiable cause
No identifiable cause
![]() Late onset
Late onset
![]() Worsen with age
Worsen with age
![]() Underlying abnormalities in asthma include
Underlying abnormalities in asthma include ![]() pulmonary vascular pressure, diffuse narrowing of airways,
pulmonary vascular pressure, diffuse narrowing of airways, ![]() residual volume and functional residual capacity, and
residual volume and functional residual capacity, and ![]() total ventilation maintaining normal or reduced PCO2 despite
total ventilation maintaining normal or reduced PCO2 despite ![]() dead space.
dead space.
Asthma is the most common cause of cough in school-age children.
SIGNS AND SYMPTOMS
![]() Cough, wheezing, dyspnea.
Cough, wheezing, dyspnea.
![]()
![]() work of breathing (retractions, use of accessory muscles, nasal flaring, abdominal breathing).
work of breathing (retractions, use of accessory muscles, nasal flaring, abdominal breathing).
![]()
![]() breath sounds.
breath sounds.
![]() Prolongation of expiratory phase.
Prolongation of expiratory phase.
![]() Acidosis and hypoxia may result from airway obstruction.
Acidosis and hypoxia may result from airway obstruction.
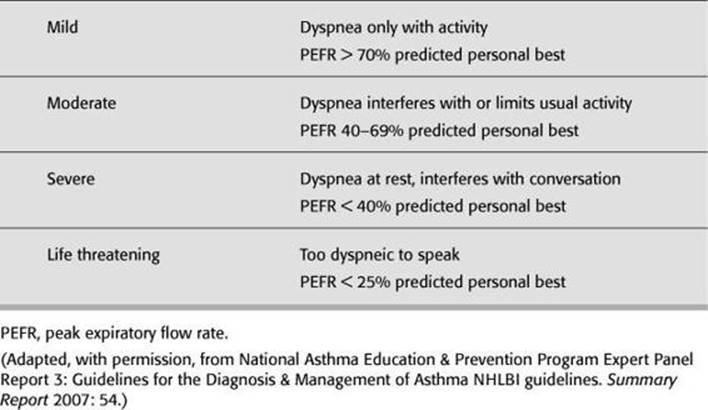
![]() See Table 12-4 for classification of severity.
See Table 12-4 for classification of severity.
Classic trilogy of asthma:
![]() Bronchospasm
Bronchospasm
![]() Mucus production
Mucus production
![]() Inflammation and edema of the airway mucosa
Inflammation and edema of the airway mucosa
DIAGNOSIS
![]() Clinical diagnosis, usually.
Clinical diagnosis, usually.
![]() Peak expiratory flow rate (PEFR):
Peak expiratory flow rate (PEFR):
![]() Maximal rate of airflow during forced exhalation after a maximal inhalation.
Maximal rate of airflow during forced exhalation after a maximal inhalation.
![]() Normal values depend on age and height:
Normal values depend on age and height:
![]() Mild (80% of predicted).
Mild (80% of predicted).
![]() Moderate (50–80% of predicted).
Moderate (50–80% of predicted).
![]() Severe (< 50% of predicted).
Severe (< 50% of predicted).
Respiratory drive is not inhibited in asthma.
TABLE 12 - 4. Asthma Severity Classification
CLASSIFYING SEVERITY OF ASTHMA EXACERBATIONS IN THE URGENT OR EMERGENCY CARE SETTING
![]() Chest x-ray will demonstrate hyperinflation and can be useful to look for pneumonia.
Chest x-ray will demonstrate hyperinflation and can be useful to look for pneumonia.
![]() Pulse oximetry may demonstrate hypoxia.
Pulse oximetry may demonstrate hypoxia.
![]() Fever and focal lung exam—think pneumonia.
Fever and focal lung exam—think pneumonia.
![]() Unresponsive to usual URI therapy.
Unresponsive to usual URI therapy.
![]() ABG—hypoxia in severe exacerbations; hypercapnia suggestive of impending respiratory failure.
ABG—hypoxia in severe exacerbations; hypercapnia suggestive of impending respiratory failure.
![]() Bloodwork should not be routinely ordered in the evaluation of asthma.
Bloodwork should not be routinely ordered in the evaluation of asthma.
All wheezing is not caused by asthma; all asthmatics do not wheeze.
TREATMENT
Goals: Improve bronchodilation, avoid allergens, ![]() inflammation, educate patient.
inflammation, educate patient.
Asthmatic patient in severe respiratory distress may not wheeze.
First-Line Agents
1. Oxygen.
2. Inhaled β2 agonist:
![]() Albuterol (2.5 mg) (nebulized).
Albuterol (2.5 mg) (nebulized).
![]() Short-acting/rescue medication—treats only symptoms, not underlying process.
Short-acting/rescue medication—treats only symptoms, not underlying process.
![]() Bronchial smooth-muscle relaxant.
Bronchial smooth-muscle relaxant.
![]() Side effects: Tachycardia, tremors, hypokalemia.
Side effects: Tachycardia, tremors, hypokalemia.
3. Corticosteroids (sooner is better):
![]() For treatment of chronic inflammation.
For treatment of chronic inflammation.
![]() Oral prednisone (2 mg/kg, max 60 mg) or IV methylprednisolone 2 mg/kg max 125 mg).
Oral prednisone (2 mg/kg, max 60 mg) or IV methylprednisolone 2 mg/kg max 125 mg).
![]() Contraindication: Active varicella or herpes infection.
Contraindication: Active varicella or herpes infection.
4. Anticholinergic agents:
![]() Ipratropium bromide (nebulized).
Ipratropium bromide (nebulized).
![]() Act synergistically with albuterol.
Act synergistically with albuterol.
![]() Bind to cholinergic receptors in the medium and large airways.
Bind to cholinergic receptors in the medium and large airways.
Second-Line Agents
1. Magnesium sulfate—bronchodilation via direct effect on smooth muscle.
2. Epinephrine or terbutaline.
3. No role in acute asthma for theophylline; not recommended.
Others
1. Heliox—mixture of 60–70% helium and 30–40% oxygen:
![]()
![]() work of breathing by improving laminar gas flow (nonintubated patient).
work of breathing by improving laminar gas flow (nonintubated patient).
![]() Improves oxygenation and
Improves oxygenation and ![]() peak airway pressure (intubated patients).
peak airway pressure (intubated patients).
2. Mechanical ventilation indications:
![]() Failure of maximal pharmacologic therapy.
Failure of maximal pharmacologic therapy.
![]() Hypoxemia.
Hypoxemia.
![]() Hypercarbia.
Hypercarbia.
![]() Change in mental status.
Change in mental status.
![]() Respiratory fatigue.
Respiratory fatigue.
![]() Respiratory failure.
Respiratory failure.
3. Leukotriene modifiers:
![]() Inflammatory mediators.
Inflammatory mediators.
![]() Improve lung function.
Improve lung function.
![]() No role in acute asthma.
No role in acute asthma.
4. Cromolyn and nedocromil:
![]() Effective in maintenance therapy.
Effective in maintenance therapy.
![]() Exercise-induced asthma.
Exercise-induced asthma.
![]() May reduce dosage requirements of inhaled steroid.
May reduce dosage requirements of inhaled steroid.
Spirometry is the most important study in asthma.
O2 is indicated for all asthmatics to keep O2 saturation > 95%.
Long-acting β2 agonist (salmeterol) should not be used for acute asthma exacerbation.
Admit if:
![]() Respiratory failure requiring intubation.
Respiratory failure requiring intubation.
![]() Status asthmaticus.
Status asthmaticus.
![]() Return ED visit in 24 hours.
Return ED visit in 24 hours.
![]() Complete lobar atelectasis.
Complete lobar atelectasis.
![]() Pneumothorax/pneumomediastinum.
Pneumothorax/pneumomediastinum.
![]() Underlying cardiopulmonary disease.
Underlying cardiopulmonary disease.
Asthmatic child’s ability to use inhaler correctly should be regularly assessed.
Inhaled corticosteroids are recommended as the first-line prophylactic therapy.
Status Asthmaticus
DEFINITION
![]() Life-threatening form of asthma.
Life-threatening form of asthma.
![]() Condition in which a progressively worsening attack is unresponsive to usual therapy.
Condition in which a progressively worsening attack is unresponsive to usual therapy.
SIGNS AND SYMPTOMS
Most important risk factor for morbidity is failure to diagnose asthma from recurrent wheezing.
Look for:
![]() Pulsus paradoxus > 20 mm Hg.
Pulsus paradoxus > 20 mm Hg.
![]() Hypotension, tachycardia.
Hypotension, tachycardia.
![]() Cyanosis.
Cyanosis.
![]() One- to two-word dyspnea.
One- to two-word dyspnea.
![]() Lethargy.
Lethargy.
![]() Agitation.
Agitation.
![]() Retractions.
Retractions.
![]() Silent chest (no wheezes—poor air exchange).
Silent chest (no wheezes—poor air exchange).
![]() white blood cell (WBC) count does not always signify infection in status asthmaticus.
white blood cell (WBC) count does not always signify infection in status asthmaticus.
Dehydration may be present in status asthmaticus, but overhydration should be avoided (risk for syndrome of inappropriate antidiuretic hormone secretion [SIADH]).
FOREIGN BODY ASPIRATION
![]()
A 2-year-old boy is brought to the ED with a history of a choking or gagging episode, followed by a coughing spell. In the ED, he was noted to have wheezing. His respiratory rate is 24, and he has mild intercostal retractions. His babysitter found him playing in his room. Think: Foreign body aspiration.
![]()
A previously healthy 12-year-old boy presented with cough for almost a year. He had a persistent dry cough during the day and night that was occasionally productive. His parents reported a history of pneumonia with consolidation of the right lower lobe on three different occasions in 6 months. On physical examination, no nasal congestion is noted. ![]() air entry and wheezing is noted on the right side of his chest. Think: Foreign body aspiration.
air entry and wheezing is noted on the right side of his chest. Think: Foreign body aspiration.
However, this classic triad (sudden onset of paroxysmal coughing, wheezing, and diminished breath sounds on the ipsilateral side) may not be present in all children with foreign body aspiration.
PATHOPHYSIOLOGY
Cough reflex usually protects against aspiration.
EPIDEMIOLOGY
![]() Twice as likely to occur in males, particularly 6-month-olds to 3-year-olds.
Twice as likely to occur in males, particularly 6-month-olds to 3-year-olds.
![]() Most common age: 1–2 years.
Most common age: 1–2 years.
Prevention is key! Keep small food and objects away from young children.
SIGNS AND SYMPTOMS
![]() Determined by nature of object, location, and degree of obstruction.
Determined by nature of object, location, and degree of obstruction.
![]() Narrowest portion of the pediatric airway is at the cricoid ring.
Narrowest portion of the pediatric airway is at the cricoid ring.
![]() Foreign body in the upper airway: Respiratory distress with severe retractions and stridor.
Foreign body in the upper airway: Respiratory distress with severe retractions and stridor.
![]() Foreign body in the lower airway (most foreign bodies lodge in the lower airways [80%]). Symptoms may be subtle.
Foreign body in the lower airway (most foreign bodies lodge in the lower airways [80%]). Symptoms may be subtle.
![]() Initial respiratory symptoms may disappear for hours to weeks after incident.
Initial respiratory symptoms may disappear for hours to weeks after incident.
![]() Vegetal/arachidic bronchitis due to vegetable (usually peanut) aspiration causes cough, high fever, and dyspnea.
Vegetal/arachidic bronchitis due to vegetable (usually peanut) aspiration causes cough, high fever, and dyspnea.
![]() Most common aspirated foreign body: Peanut.
Most common aspirated foreign body: Peanut.
![]() Most common foreign body aspirations resulting in death: Balloons.
Most common foreign body aspirations resulting in death: Balloons.
![]() Complications if object is not removed include pneumonitis/pneumonia, abscess, bronchiectasis, pulmonary hemorrhage, erosion, and perforation.
Complications if object is not removed include pneumonitis/pneumonia, abscess, bronchiectasis, pulmonary hemorrhage, erosion, and perforation.
Caution! Do not try to remove foreign bodies causing partial upper airway obstruction because these attempts may result in complete glottic obstruction.
DIAGNOSIS/TREATMENT
Foreign Body Aspiration
![]() Toddlers: R = L mainstem
Toddlers: R = L mainstem
![]() Adults: R mainstem predominates
Adults: R mainstem predominates
Larynx
![]() Croupy cough; may have stridor, aphonia, hemoptysis, cyanosis.
Croupy cough; may have stridor, aphonia, hemoptysis, cyanosis.
![]() Lateral x-ray.
Lateral x-ray.
![]() Direct laryngoscopy—confirm diagnosis and remove object.
Direct laryngoscopy—confirm diagnosis and remove object.
Trachea
![]() Stridor, audible slap, and palpable thud due to expiratory impaction.
Stridor, audible slap, and palpable thud due to expiratory impaction.
![]() Chest x-ray (see Figure 12-6), bronchoscopy.
Chest x-ray (see Figure 12-6), bronchoscopy.
Bronchi
![]() Initial choking, gagging, wheezing, coughing.
Initial choking, gagging, wheezing, coughing.
![]() Latent period with some coughing, wheezing, possible hemoptysis, recurrent lobar pneumonia, or intractable asthma.
Latent period with some coughing, wheezing, possible hemoptysis, recurrent lobar pneumonia, or intractable asthma.
Percussion of Lung Fields
![]() Hyperresonant = overinflation
Hyperresonant = overinflation
![]() Dull = atelectasis
Dull = atelectasis
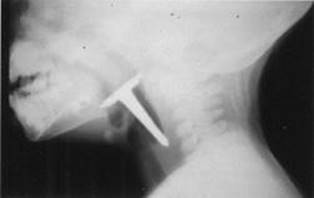
FIGURE 12-6. Radiograph of lateral soft tissue of the neck demonstrates a foreign body (nail) in the pharynx.
(Courtesy of Dr. Gregory J. Schears.)
FIGURE 12-7. Foreign body (peanut) in the right mainstem bronchus visualized by bronchoscopy.
Foreign bodies tend to lodge most commonly in the right mainstem bronchus due to the larger anatomic angle that makes traveling down right mainstem easier. (Courtesy of Dr. Gregory J. Schears.)
![]() Tracheal shift,
Tracheal shift, ![]() breath sounds.
breath sounds.
![]() Midline obstruction can cause severe dyspnea or asphyxia.
Midline obstruction can cause severe dyspnea or asphyxia.
![]()
![]() chronic bronchopulmonary disease if not treated.
chronic bronchopulmonary disease if not treated.
![]() Direct bronchoscopic visualization (Figure 12-7).
Direct bronchoscopic visualization (Figure 12-7).
![]() Antibiotics for secondary infection if prolonged exposure.
Antibiotics for secondary infection if prolonged exposure.
![]() Emergency treatment of local upper airway obstruction if necessary.
Emergency treatment of local upper airway obstruction if necessary.
![]() If the child can cough and verbalize:
If the child can cough and verbalize:
![]() Provide supplemental oxygen.
Provide supplemental oxygen.
![]() Maintain position of comfort.
Maintain position of comfort.
![]() Immediate consultation with ENT and anesthesia.
Immediate consultation with ENT and anesthesia.
![]() If the child cannot cough or verbalize, initiate basic life support.
If the child cannot cough or verbalize, initiate basic life support.
TRACHEOESOPHAGEAL FISTULA (TEF)
DEFINITION
Connection between the trachea and esophagus (see Figure 12-8).
FIGURE 12-8. Types of tracheoesophageal fistulas (TEFs).
Type A, esophageal atresia (EA) with distal TEF (87%). Type B, isolated EA. Type C, isolated TEF. Type D, EA with proximal TEF. Type E, EA with double TEF.
ETIOLOGY
![]() Congenital
Congenital
![]() Acquired
Acquired
SIGNS AND SYMPTOMS
![]() Suspect esophageal atresia.
Suspect esophageal atresia.
![]() Maternal polyhydramnios.
Maternal polyhydramnios.
![]() Inability to pass catheter into stomach.
Inability to pass catheter into stomach.
![]()
![]() oral secretions—drooling.
oral secretions—drooling.
![]() Choking, cyanosis, or coughing with an attempt to feed.
Choking, cyanosis, or coughing with an attempt to feed.
![]() Tachypnea.
Tachypnea.
DIAGNOSIS
![]() X-ray: Radiopaque feeding tube passes no further than proximal esophagus.
X-ray: Radiopaque feeding tube passes no further than proximal esophagus.
![]() Barium swallow: Aspiration of barium into the tracheobronchial tree.
Barium swallow: Aspiration of barium into the tracheobronchial tree.
TREATMENT
Esophageal atresia is a surgical emergency.
TRACHEOMALACIA/LARYNGOMALACIA
DEFINITION
![]() Floppy epiglottis and supraglottic aperture.
Floppy epiglottis and supraglottic aperture.
![]() Disproportionately small and soft larynx.
Disproportionately small and soft larynx.
SIGNS AND SYMPTOMS
![]() Usually begins within first month.
Usually begins within first month.
![]() Noisy breathing.
Noisy breathing.
![]() Stridor—laryngomalacia is the most frequent cause of stridor in children.
Stridor—laryngomalacia is the most frequent cause of stridor in children.
![]() Symptoms can be intermittent.
Symptoms can be intermittent.
![]() Hoarseness or aphonia (laryngeal crow).
Hoarseness or aphonia (laryngeal crow).
![]() Feeding difficulty.
Feeding difficulty.
![]() Symptoms worse when crying or lying on back.
Symptoms worse when crying or lying on back.
DIAGNOSIS
![]() Direct laryngoscopy.
Direct laryngoscopy.
![]() Collapse of laryngeal structures during inspiration especially arytenoid cartilages.
Collapse of laryngeal structures during inspiration especially arytenoid cartilages.
TREATMENT
![]() Reassurance.
Reassurance.
![]() No specific therapy required.
No specific therapy required.
![]() Usually resolves spontaneously by 18 months.
Usually resolves spontaneously by 18 months.
There is an association of tracheoesophageal fistulae with esophageal atresia.
H-type tracheoesophageal fistula is the least common but the most likely to be seen in ED.
CONGENITAL LOBAR EMPHYSEMA (INFANTILE LOBAR EMPHYSEMA)
DEFINITION
Overexpansion of the airspaces of a segment or lobe of the lung.
EPIDEMIOLOGY
Most common congenital lung lesion.
PATHOPHYSIOLOGY
No significant parenchymal destruction.
SIGNS AND SYMPTOMS
![]() Normal at birth.
Normal at birth.
![]() Cough, wheezing, dyspnea, and cyanosis within a few days.
Cough, wheezing, dyspnea, and cyanosis within a few days.
DIAGNOSIS
![]() Chest x-ray.
Chest x-ray.
![]() Radiolucency.
Radiolucency.
![]() Mediastinal shift to opposite side.
Mediastinal shift to opposite side.
![]() Flattened diaphragm.
Flattened diaphragm.
TREATMENT
![]() Remove bronchial obstruction (foreign bodies, mucous plug).
Remove bronchial obstruction (foreign bodies, mucous plug).
![]() Lobectomy.
Lobectomy.
CYSTIC ADENOMATOID MALFORMATION
DEFINITION
![]() Developmental anomaly of the lower respiratory tract.
Developmental anomaly of the lower respiratory tract.
![]() Excessive overgrowth of bronchioles.
Excessive overgrowth of bronchioles.
![]()
![]() in terminal respiratory structure.
in terminal respiratory structure.
![]() Hamartomatous lesions.
Hamartomatous lesions.
EPIDEMIOLOGY
Second most common congenital lung lesion.
In patients with cystic adenomatoid malformation, avoid attempted aspiration or chest tube placement, as there is the risk of spreading infection.
SIGNS AND SYMPTOMS
![]() Neonatal respiratory distress.
Neonatal respiratory distress.
![]() Recurrent pneumonia in same location.
Recurrent pneumonia in same location.
![]() Pneumothorax.
Pneumothorax.
![]() May be confused with diaphragmatic hernia in neonatal period.
May be confused with diaphragmatic hernia in neonatal period.
DIAGNOSIS
![]() Chest x-ray (posteroanterior [PA], lateral, and decubitus).
Chest x-ray (posteroanterior [PA], lateral, and decubitus).
![]() Cystic mass (multiple grapelike sacs) and mediastinal shift.
Cystic mass (multiple grapelike sacs) and mediastinal shift.
![]() Air-fluid level.
Air-fluid level.
![]() CT scan.
CT scan.
Cystic adenomatoid malformation ![]() the risk for pulmonary neoplasia.
the risk for pulmonary neoplasia.
TREATMENT
Surgical excision of affected lobe.