Larry W. Lynn
The incidence of attention deficit hyperactivity disorder (ADHD) has increased dramatically in the past two decades. Current studies estimate up to 8.7% of individuals under 18 years of age are affected by ADHD (Froelich, Lamphear, & Epstein, 2007). Parents of children with ADHD and other individuals are concerned these children are unable to function well at home and in the community, unable to maximize their own potential, and certainly strain their parents’ satisfaction and joy in parenting. Practitioners must be vigilant to thoroughly evaluate and appropriately treat patients presenting with possible ADHD. This includes performing a detailed history and physical examination, utilizing behavioral screening tools, ordering appropriate laboratory tests, closely working with psychologists, and titrating medications to an optimal dose.
Educational Objectives
1. Use DSM-IV-TR criteria to develop conversational questions with parents and child as part of the assessment process when screening patients for possible ADHD.
2. Develop differential diagnoses to rule out other behavioral problems.
3. Identify strategies to collaborate with parents, teachers, and psychologists as a treatment team to assist in patient management.
4. Identify strategies to best utilize follow-up appointments in person or by telephone to assist in treatment decisions.
5. Understand the appropriate use of various psychoactive medications for the treatment of ADHD.
6. Know the warnings about treating children and adolescents with stimulant and nonstimulant medications to control ADHD symptoms.
7. Consider the implications of ADHD as a lifelong condition that can possibly lead to problems throughout the lifetime for affected individuals.
Case Presentation and Discussion
Jason Black is an 8-year-old male child who presents to your office accompanied by his mother for a behavioral consultation. He began third grade 3 months ago and is having academic and behavioral problems at school. Despite the efforts of his parents and teachers to help him organize, Jason remains unorganized with his work and belongings. He often fails to bring homework home and frequently forgets to turn in completed assignments at school. He is restless and impulsive. He often blurts out answers in class, interrupting the teacher or his classmates. He tends to violate the personal space of his peers and interferes with their play and interaction during recess and physical education. As a result, he is being socially isolated by peers.
At home, he fails to follow through with parental instructions. He often loses important items such as homework and even his favorite toys. His room is described by his mother as “looking like a tornado came through.” The parents have tried time out, restricting activities, and spankings but have seen no improvement in his behavior. He is beginning to see himself as different and describes himself as “dumb” and states, “I have no friends.” His teacher suggested the parents seek medical advice and “get some medicine to calm him down.” The mother knows there is a problem with Jason’s behavior, but is concerned for him to be labeled with ADHD. She is also concerned with the negative comments she reads on various Web sites about treating children with medications to control the symptoms of ADHD. She describes feeling lost because she doesn’t know how to help her child.
What questions would you ask Jason and his mother to expand on the information above? ![]()
It is important to base your questions on the diagnostic criteria for ADHD listed in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision (DSM-IV-TR; APA, 2000). Refer to Table 12-1 and become familiar with these criteria. The child must exhibit six of nine symptoms associated with inattention or six of nine symptoms associated with hyperactivity-impulsivity to consider the diagnosis of ADHD and avoid overidentification and underidentification of the disease. The DSM-IV-TR criteria define three different subtypes of ADHD: 1) ADHD that is predominately inattentive (meets six of nine inattentive behaviors); 2) ADHD that is predominately hyperactive-impulsive (meets six of nine hyperactive-impulsive behaviors); 3) combined type ADHD (has six of nine behaviors in both the inattention and hyperactive-impulsivity behavioral realms).
Are there guidelines to help clinicians deal with ADHD problems?![]()
A combination of open- and closed-ended questions based on DSM-IV-TR criteria (APA, 2000) will provide insight into the patient’s behavioral history and current problems. The clinician needs to develop questions that are a part of a conversation with parents and children to uncover these issues. The American Academy of Pediatrics (AAP) developed clinical practice guidelines for ADHD in 2000 that highlight the importance of obtaining input from parents, teachers, other caregivers, and professional consultants when evaluating a child for possible ADHD (American Academy of Pediatrics, 2000). Working with these individuals as members of a team will provide information to assist in making the diagnosis of ADHD to help guide you in effective patient management.
Table 12–1 DSM-IV Criteria for ADHD
I. Either A or B:
A. Six or more of the following symptoms of inattention have been present for at least 6 months to a point that is disruptive and inappropriate for developmental level:
Inattention
1. Often does not give close attention to details or makes careless mistakes in schoolwork, work, or other activities.
2. Often has trouble keeping attention on tasks or play activities.
3. Often does not seem to listen when spoken to directly.
4. Often does not follow instructions and fails to finish schoolwork, chores, or duties in the workplace (not due to oppositional behavior or failure to understand instructions).
5. Often has trouble organizing activities.
6. Often avoids, dislikes, or doesn’t want to do things that take a lot of mental effort for a long period of time (such as schoolwork or homework).
7. Often loses things needed for tasks and activities (e.g., toys, school assignments, pencils, books, or tools).
8. Is often easily distracted.
9. Is often forgetful in daily activities.
B. Six or more of the following symptoms of hyperactivity-impulsivity have been present for at least 6 months to an extent that is disruptive and inappropriate for developmental level:
Hyperactivity
1. Often fidgets with hands or feet or squirms in seat.
2. Often gets up from seat when remaining in seat is expected.
3. Often runs about or climbs when and where it is not appropriate (adolescents or adults may feel very restless).
4. Often has trouble playing or enjoying leisure activities quietly.
5. Is often “on the go” or often acts as if “driven by a motor.”
6. Often talks excessively.
Impulsivity
1. Often blurts out answers before questions have been finished.
2. Often has trouble waiting one’s turn.
3. Often interrupts or intrudes on others (e.g., butts into conversations or games).
II. Some symptoms that cause impairment were present before age 7 years.
III. Some impairment from the symptoms is present in two or more settings (e.g., at school/work and at home).
IV. There must be clear evidence of significant impairment in social, school, or work functioning.
V. The symptoms do not happen only during the course of a pervasive developmental disorder, schizophrenia, or other psychotic disorder. The symptoms are not better accounted for by another mental disorder (e.g., mood disorder, anxiety disorder, dissociative disorder, or a personality disorder).
Based on these criteria, three types of ADHD are identified:
1. ADHD, Combined Type: if both criteria 1A and 1B are met for the past 6 months
2. ADHD, Predominantly Inattentive Type: if criterion 1A is met but criterion 1B is not met for the past 6 months
3. ADHD, Predominantly Hyperactive-Impulsive Type: if criterion 1B is met but criterion 1A is not met for the past 6 months.
Source: American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.). Washington, DC: American Psychiatric Association.
Further questioning provides the following information about the history of these behaviors. Jason has always been a very active boy. The mother describes him as “on the go and all boy since he could walk.” He attended a preschool class 2 days each week for 3 hours per day at age 4 years and got along well except for trouble sharing and an occasional disagreement with peers. At that time he was described as “energetic” and “loud” on caregiver reports. There has been some concern about behavior since he began kindergarten. He has always been more loud and restless than his peers. Teachers have complained that Jason requires frequent redirection in the classroom. He has performed well academically until this year. Though he was always disorganized and messy, he made A’s and B’s on most papers in first and second grade. He had no problem learning to read, but does not enjoy sitting and reading because he would rather do something active. This has become a problem area because more reading has been required at school this year. Currently, there is less directed study and more independent study expected within the classroom. Jason cannot keep on task and often interrupts other students while they are working. When asked to complete assignments, he often gets up from his seat. He runs in the hall when the class moves between classrooms. He rarely completes an assignment unless there is one-on-one encouragement from the teacher. His work contains many careless mistakes despite his ability. He has academic potential, as suggested by his scoring above the 90th percentile on the state standards test last spring; however, he has fallen behind this school year in reading and mathematics. He is currently making all D’s on his report card. He usually makes B’s on tests, but only turns in half his homework assignments, which has a negative impact on his overall grades.
What additional information might be helpful in evaluating this patient? ![]()
It is important to rule out other medical and psychological causes of inattention and poor behavior when evaluating a child for ADHD. A thorough medical history and review of systems should be performed to exclude other conditions in the differential diagnosis. Table 12-2 provides a differential diagnosis list to consider when evaluating a child for possible ADHD. The history should include questions about:
• Pregnancy, delivery, and developmental milestones
• Sleep and dietary habits
• Family dynamics to rule out family stress or dysfunction as the cause of behavioral problems.
• Possible environmental relationships such as lead poisoning or Lyme disease, if the history warrants consideration.
As you listen to parents and children discuss pertinent information about behavior, consider comorbid disorders being present that may obscure or make the diagnosis less clear. They include conduct disorder, oppositional defiant disorder, and bipolar disorder, which are more common in children with ADHD (Biederman, 2004). These comorbidities can result in incorrect diagnoses and/or inappropriate treatment. For example, treating a bipolar child with a stimulant medication can cause behavior to deteriorate. Comorbid conditions must be considered alone and as potentially existing in conjunction with ADHD for the child to receive appropriate treatment.
|
Table 12–2 Differential Diagnosis of ADHD |
|
|
Sleep disorder |
|
|
Thyroid disease |
|
|
Autistic spectrum disorder |
|
|
Psychiatric disorder |
|
|
• Anxiety disorder |
|
|
• Oppositional defiant disorder |
|
|
• Mood disorder |
|
|
• Adjustment disorder |
|
|
Family dysfunction |
|
|
Physical or emotional abuse |
|
|
Developmental disorder/learning disability |
|
|
Seizure disorder |
|
|
Substance abuse |
|
|
Central auditory processing disorder |
|
|
Visual or hearing impairment |
|
Jason perceives himself in a negative way, as his earlier comments suggest. Some children with ADHD become depressed to some degree because of the recurring negative interactions or consequences brought about by their behavior. This depression and low self-esteem often improve when the symptoms of ADHD are treated. Persistent depression warrants referral to a psychologist.
What findings are important on the physical examination? ![]()
The first part of any thorough physical examination is to simply observe the patient. Get a feeling for the gestalt of this patient. Appreciate any abnormal physical, movement, or behavioral findings as you enter the room and begin to speak with the patient and parents. Is there any syndromic appearance to the patient? Is there evidence of an organic disease such as thyroid disease? Evaluate the pattern of speech and word selection for age appropriateness. Direct questions to the patient and observe the content of responses. Observe how the patient interacts during the interview and examination. Is restlessness, hyperkinetic behavior, or excessive talking present during the interview?
The clinician should perform a thorough physical examination for two reasons. First, one wants to exclude medical conditions from the differential diagnosis. Second, if treatment is necessary, one must be sure there is no underlying medical condition, such as a congenital heart defect or arrhythmia, that might preclude or alter pharmacologic intervention.
Hearing screening should be an initial part of the assessment process.
Jason’s physical examination and hearing screening are both normal in all aspects. No neurological, cardiac, sensory, or thyroid abnormalities are identified.
What testing should be done? ![]()
Testing falls into two broad and general categories during an ADHD workup: medical and psychological testing. Evaluations should be thorough, but judicious use of potentially expensive tests should be practiced. Order tests based on an adequate index of suspicion.
First, findings during the interview or physical examination might indicate laboratory tests or imaging studies are necessary. For example, if thyroid disease is suspected, then order thyroid function studies. Expensive imaging studies such as MRI or CT scans of the brain should be ordered only if there is a high index of suspicion for neuropathology because these studies do not diagnose or rule out ADHD.
Second, the clinician should administer a DSM-IV-TR–based ADHD screening tool such as the revised Conners’ Scales or the Vanderbilt assessment, each of which has teacher and parent versions. Scoring and interpretation of these screening tests is very simple and thoroughly explained in the assessment manual for each tool. Such ADHD rating scales for parents and teachers have been shown to have an odds ratio of 3.0 (equivalent to a sensitivity and specificity greater than 94%) in studies differentiating children with ADHD from normal, age-matched community controls (Green, Wong, & Atkins, 1999).
Additionally, the clinician may want to refer the patient to a psychologist for an extensive evaluation and psychometric testing to rule out low IQ, psychiatric diagnoses, learning difficulties, or developmental problems as contributing factors or as the actual diagnosis. Ideally, when behavioral consultation appointments are scheduled, Conners’ Scales or Vanderbilt assessments should be sent to the parents and teachers for completion prior to the appointment. Include a preprinted instruction letter for teachers that requests additional written information she or he believes is important in the evaluation of the child. This allows more information to be discussed at the appointment and also, if indicated, pharmacologic treatment to immediately begin.
In this case, Conners’ Scales were completed by Jason’s parents and two teachers prior to the appointment. The results are significant for elevation in measures of hyperactivity-impulsivity and inattention by all four evaluators. The teachers scored Jason significantly higher on the hyperactivity-impulsivity scale than the parents did.
It is common to see children suspected of having ADHD score higher on the scales of hyperactivity-impulsivity and inattention in a structured setting. Often, the behaviors are less noticed or less problematic at home where activities are not as structured and the child is not required to follow group rules. There can be great variation between parental observations as well. Depending on how much time and under what circumstances a parent interacts with a child, this parent may not be exposed to the problem behaviors voiced by teachers and the other parent. It is not uncommon for divorced parents to claim completely different behaviors are observed when the child is in each household. Reviewing the results of these screening tests allows parents to see how their child compares to similar aged peers in the areas of attention and impulsivity from the viewpoint of several adults while the child is in different settings.
Making the Diagnosis
Based on the interview and information obtained from the Conners’ Scales, it appears that Jason meets the criteria for ADHD. His mother has indicated that she has reservations about her son being labeled with a psychiatric diagnosis and is concerned about medical management. Additionally, she explains that his father believes these behaviors are just a part of being a boy, although the father has agreed to a short trial of the medication because Jason is having academic difficulties. However, he remains skeptical about treating for a prolonged period of time. The mother asks how long Jason will be treated and what side effects they should expect to see with medication.
Management
What type of education should you provide to a family when treating a child diagnosed with ADHD? ![]()
It is extremely important to educate the parents and child about why ADHD is treated, what medications are used, and what follow-up care will be needed in the short term and long term. There is much confusion in the general population about the medications used to treat ADHD. This confusion often results from misinformation obtained through the news media, the Internet, or friends and family members. Clinicians must educate parents and patients about the expected results and potential side effects when treating ADHD with a prescription medication. Free information is available online for parents and clinicians from the American Academy of Pediatrics (http://www.aap.org), the American Academy of Child and Adolescent Psychiatry (http://www.aacap.org), and the organization Children and Adults with Attention Deficit/Hyperactivity Disorder (http://www.chadd.org). During the visit provide an overview of medications used to treat ADHD. Outline the categories of medications, how they work, and what side effects to expect.
The patient will need to be followed up by telephone and in person as the medication is titrated to an effective dose. Inform the parents about titrating the dose based upon the response in their child as an individual. Then, follow-up at various intervals to assess the efficacy of the medication over time. Follow-up visits provide an opportunity for the healthcare provider to assess the patient while giving parents and patients a voice in how the medication is titrated. This type of communication also lessens the likelihood of confusion leading to a medication being unnecessarily discontinued.
A caveat to remember is that if there is no observable change or minimal improvement seen when treating ADHD with medication at a therapeutic dose, then another medication should be considered. If two or more medications have been tried without success, then additional workup and consideration of other diagnoses is indicated. It is important to utilize evidence-based medicine practices when treating ADHD to assure the correct diagnosis is made and an effective treatment strategy is providing desired results (Epstein, Rabinar, & Johnson, 2007; Leslie, Weekerly, Plemmons, Landsvere, & Eastman, 2004).
What medication should be used in the first line of treatment of ADHD? ![]()
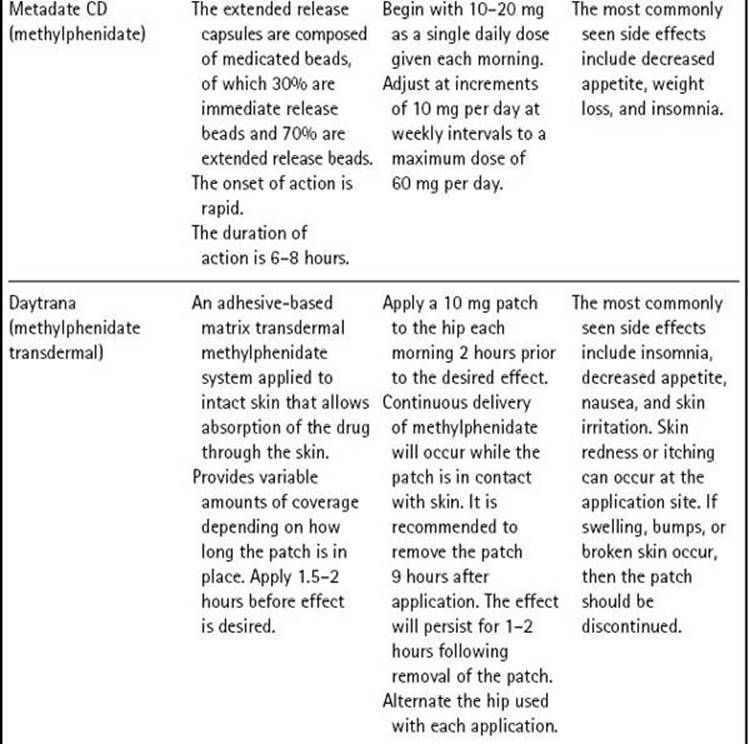
Two classes of FDA-approved medications are used as first-line treatment of ADHD in children and adolescents—stimulants and nonstimulants. The stimulants include the various methylphenidate and amphetamine products; the only approved nonstimulant is atomoxetine. Table 12-3 lists these medications. Note that several medications are used off label for the treatment of ADHD. It is recommended that these medications be prescribed and monitored by a clinician who specializes in treating this disease. Therefore, these medications will not be discussed in this case study.
Table 12–3 Medications Approved to Treat ADHD in Children




Psychostimulants are the most frequently used medications for treating ADHD. Stimulants provide an effect in treating ADHD by blocking presynaptic reuptake of the neurotransmitters dopamine and norepinephrine and increasing the release of these monoamines into the synaptic cleft. With more neurotransmitter available at the synapse, signals are transmitted more efficiently. Atomoxetine blocks reuptake of norepinephrine, but does not significantly influence dopamine reuptake. Norepinephrine enhances relevant signals while dopamine suppresses irrelevant signals in the attentional areas of the brain.
Studies have shown that 80% of children treated with a stimulant medication have a good clinical response, with approximately 50% of those responders showing equivalent efficacy with methylphenidate or amphetamine, both of which have been used to treat attention problems for decades (Elia, Borcherding, Rappoport, & Keysor, 1991; MTA Cooperative Group, 1999). It is important to realize that methylphenidate and amphetamine have different potencies. The typical conversion is 5 mg of amphetamine has potency equivalent to 10 mg of methylphenidate (Elia et al., 1991). Keep this in mind when changing from one of these products to the other.
Timing of Doses
The immediate release forms of these drugs require multiple daily doses. Usually medication is given between 7:00 and 8:00 a.m. and again between 11:00 a.m. and 12:00 noon. Ideally, each dose results in 3–4 hours of positive clinical effect. The problem with immediate release formulations is that patients often have a window of subtherapeutic time prior to the next dose, during which symptoms return. This often occurs during the late morning at school or after school when homework needs to be completed. A third dose is sometimes given after school to allow patients to concentrate on homework. Multiple daily dosing becomes cumbersome for parents and teachers.
In the last decade, extended release formulations of methylphenidate and mixed amphetamine salts providing 8–12 hours of clinical effect following a single dose were introduced to the market. These medications revolutionized the treatment of ADHD with one dose per day providing extended control of symptoms. Studies show 8–12 hours of efficacy with a single morning dose. In 2006, a transdermal patch that delivers methylphenidate in an extended fashion was introduced to the market. Delivery through transdermal methylphenidate patches has allowed flexibility in treating ADHD over the waking day.
Atomoxetine is not a scheduled drug and has shown efficacy in reducing the symptoms of ADHD; it has safety and tolerability similar to that of methylphenidate (Michelson et al., 2002). It also may be given as a single daily dose. Decreased appetite and insomnia are side effects commonly seen in patients treated with atomoxetine (Wernicke & Kratochvil, 2002). Children and adolescents treated with atomoxetine were noted to have minor increases in diastolic blood pressure and heart rate, although there were no differences found on ECG tracings of patients treated with atomoxetine compared to those given placebo (Wernicke & Kratochvil). However, monitoring blood pressure and auscultating the heart should be a part of the routine examination.
A sample treatment plan is outlined in Table 12-4. Remember that feedback from the before-mentioned team is necessary before titrating these medications to their optimum dose. Poor communication between the clinician and parents should not be the reason a child receives less than optimal care for ADHD.
You suggest starting a long-acting medication each morning (5 mg of Focalin XR) and outline follow-up visits or interviews as listed in Table 12-4. The mother reiterates her concern about the safety of stimulant medications. In particular, she has read this class of medication can cause heart attacks and be fatal.
|
Table 12–4 Sample Treatment Approach for ADHD |
|
|
Type of Patient Interaction |
Treatment Decisions to Consider |
|
The diagnosis is established and treatment initiated at the first visit. |
Education including proper dosing, onset of action, and potential side effects should be discussed prior to the first prescription being written. |
|
A follow-up call from the parents following 1 week of treatment to check for efficacy, tolerability, and potential side effects. |
Titrate to a higher dose if indicated. Reassure if typical side effects such as appetite decrease and trouble falling asleep are present. |
|
A follow-up call from the parents following 1–2 additional weeks of treatment. |
There should be some noticeable effect obvious to parents and/or teachers at this point. You must decide if an additional dosage increase is warranted now or wait until the next appointment. |
|
1 month in office follow-up visit. Weight and blood pressure should be recorded. |
Inquire about efficacy at home, in school, and in social situations. Discuss appetite and sleep. Titrate to a higher dose if indicated. |
|
Routine medication checks or maintenance visits every 3–4 months. |
It is important to monitor continued efficacy and adverse effects. In particular, appetite and weight gain must be followed over time. Medication should be discontinued if the patient loses ≥ 10% of his or her body weight. |
What specific information about potential adverse effects in this class of medication should be given to the mother? ![]()
Cardiac Problems
There has been concern of an association between sudden death and using stimulant medications (Gutgesell et al., 1999). The American Heart Association (AHA, 2008) released a statement recommending a screening ECG in all children prior to beginning treatment with a stimulant medication (Vetter, Elia, & Erickson, 2008) to rule out any conduction disturbance that could be exacerbated by taking a stimulant medication. The AHA statement has been met with skepticism in the medical community because it contradicts the evidence-based medicine recommendations of the American Academy of Child and Adolescent Psychiatry and the American Academy of Pediatrics (American Academy of Pediatrics, 2000; Pliszka & American Academy of Child and Adolescent Psychiatry, 2007). A policy statement from the AAP published in August 2008 states there is no evidence to demonstrate the likelihood of sudden death is higher in children receiving medications for ADHD than in the general population. Also, the text of this policy statement notes it has not been shown that screening ECGs before starting stimulants have an appropriate balance of benefit, risk, and cost effectiveness for general use in identifying risk factors for sudden death (Perrin, Friedman, & Knilans, 2008).
Despite these warnings, stimulant medications are widely used and historically have a safe profile with regard to adverse events. Many studies have shown participants have no significant cardiac events when treated with a stimulant medication. An important point for parents and patients to understand is that some of the concern is over effects with no clinical significance. For example, a study of one extended release methylphenidate product showed a statistically significant increase in heart rate, systolic blood pressure, and diastolic blood pressure (Quinn, 2005). However, these values were not clinically significant, meaning the changes are not detrimental to otherwise healthy patients using such medications.
It is the obligation of practitioners to ensure that patients are at minimal or no risk when taking medications to treat the symptoms of ADHD. Therefore, prior to prescribing such medications, a thorough physical examination should be performed with emphasis on the cardiac portion of the examination including measuring the blood pressure. Additionally, blood pressure should be measured and the heart should be auscultated at each medication follow-up visit. Caution should be exercised when using stimulant medications in patients with any cardiac abnormality, whether the etiology is structural or is a problem with electrical conduction. In such patients, a cardiology consultation is recommended before initiating therapy.
An important part of treating patients with ADHD is spending time educating parents and patients about the much more likely side effects seen with stimulant medications. The most common side effects seen secondary to using stimulant medications are appetite suppression and insomnia (Efron, Friedrich, & Barker, 1997).
Appetite
Some authors suggest the appetite suppression subsides after 1–3 months of treatment; however, some children will have appetite suppression for the duration of treatment with a stimulant.
Sleep Disturbances
Insomnia is often present in children with ADHD. It can be a basic part of the disease or can be secondary to medications prescribed to control the symptoms of ADHD. A small number of children sleep better after medication is started. Other children will require a medication to help with sleep. The medical literature has scant information about using medications to enhance sleep in children with ADHD. Most clinicians do not want to treat children with sedative hypnotics. Clinicians have a few options when the treatment of insomnia is necessary. Melatonin is used to treat circadian rhythm disturbances and will induce sleep in children with ADHD. It can be purchased over the counter without a prescription. Also, the central alpha agonist clonidine helps induce sleep and has a rapid onset of action; however, clonidine has a variable half-life and should be carefully titrated to avoid “morning hangover” or hypotension in children. Additionally, the antidepressant trazodone effectively induces sleep and is used in patients with ADHD who have insomnia. Consulting with a pediatrician or child psychiatrist experienced in managing insomnia may be the safest and most effective means of achieving good sleep hygiene in patients with ADHD.
Jason’s mother agrees that a medication trial is indicated for Jason at this point. Focalin XR (methylphenidate) is started at 5 mg 7:45 a.m. each morning.
First Management Evaluation Visit
The mother phones in 8 days later with a report that Jason seems to be less hyperkinetic at school and pays more attention in the early part of the morning. By 10:00 a.m., however, he is behaving in the typical restless manner.
What is the best treatment intervention at this time? ![]()
There appears to be some effect early in the morning, which fades away in a few hours. This is typical of a subtherapeutic medication dose. At this point increase the dose of Focalin XR to 10 mg given in the morning. Additionally, have the parents begin behavior modification by slowly integrating various chores and tasks into Jason’s daily routine. Keeping his school supplies neat and ready for school the next day is a good starting point. Encourage the parents to visit the Web sites previously mentioned to further their understanding of ADHD.
Second Management Evaluation Visit
Jason presents for the 1-month follow-up appointment with both parents. The father is concerned because Jason has lost 4 pounds of body weight and does not have much appetite. Also, he expresses concern that Jason will “become a zombie because this medicine sedates him so much.” Despite these concerns, both parents agree that Jason is behaving better at home and school. The teacher reported that Jason turned in all his homework last week and correctly spelled 19 of 20 words on his spelling test. However, by 2:00 p.m. he becomes restless and continues to be unable to concentrate on homework.
What is the appropriate next step in treating Jason? ![]()
The following should now be done to treat Jason:
![]() Increase the dose to 15 mg given as a single morning dose. Tell the parents 15–20 mg appears to be the necessary dose to provide efficacy over time. Observe him on the 15 mg dose for approximately 1–2 weeks, then decide if additional medication is necessary.
Increase the dose to 15 mg given as a single morning dose. Tell the parents 15–20 mg appears to be the necessary dose to provide efficacy over time. Observe him on the 15 mg dose for approximately 1–2 weeks, then decide if additional medication is necessary.
![]() Discuss a strategy for encouraging him to eat more. Some children will eat well at breakfast before taking medication, but then have no appetite the remainder of the day. Drinking or eating a small amount of food with complex carbohydrates and protein is sometimes the best plan at lunchtime. Often it is helpful to have the evening meal as late as possible.
Discuss a strategy for encouraging him to eat more. Some children will eat well at breakfast before taking medication, but then have no appetite the remainder of the day. Drinking or eating a small amount of food with complex carbohydrates and protein is sometimes the best plan at lunchtime. Often it is helpful to have the evening meal as late as possible.
![]() If he has difficulty following through with tasks at home or he remains oppositional, then referral to a psychologist is necessary.
If he has difficulty following through with tasks at home or he remains oppositional, then referral to a psychologist is necessary.
![]() Plan to see him for follow-up in 1 month. At that point, if he is stable on medication, visits may be every 3 months.
Plan to see him for follow-up in 1 month. At that point, if he is stable on medication, visits may be every 3 months.
It is important to provide education at each visit. Behavioral modification through instructions from the clinician prescribing medication or, in more difficult cases, from a psychologist, is necessary for the best clinical results according to the major MTA study (MTA Cooperative Group, 1999). However, stimulant or nonstimulant medications alone are far superior to behavioral modification alone.
What is the long-term prognosis for ADHD? ![]()
Parents must understand that ADHD is often a lifelong condition. Parents are often concerned about medicating a child for a prolonged or indefinite period of time. At some point, a controlled wean of the medication can be attempted. This is often requested by middle school–and high school–age patients. However, parents and providers must understand that the symptoms or expression of ADHD change with age. The typical adolescent is not as hyperkinetic as an 8-year-old child. The symptoms may be more subtle in appearance to those involved with these patients, but they nonetheless interfere with life. A prospective study in Wisconsin followed cohorts of teenagers with ADHD who were either treated or not treated with medication to control symptoms of ADHD for more than 13 years as they became young adults. The study found that those with untreated ADHD were more likely to not graduate from high school, be fired from a job, have an STD, have an unwanted pregnancy, be divorced, and be a substance abuser (Barkley, Fische, Smallish, & Fletcher, 2006). This is compelling evidence that ADHD should never be considered cured. Symptoms that have been controlled without medication can return throughout the affected individual’s lifetime, especially during times of stress. Keep these points in mind and make patients and parents aware of the potential lifelong nature of this disease.
Key Points from the Case
1. It may take time before the symptoms of ADHD interfere with the child’s functioning in a manner that warrants intervention.
2. Symptoms are often more obvious in structured environments.
3. Impairment can be different in different settings, such as home, school, and social situations.
4. Diagnosing ADHD is based on criteria outlined in the DSM-IV-TR.
5. Patient and parent education is mandatory for optimal outcomes. Education should begin with the first visit and be continued at subsequent follow-up visits.
6. ADHD is a lifelong condition and should be considered as influencing any behaviors that interfere with life functioning from the time of diagnosis as a child and continuing throughout adulthood.
7. Refer children with an underlying cardiac problem to a cardiologist prior to treatment with stimulant medications.
8. Use a psychologist to assess for comorbidities and to help with behavior management.
REFERENCES
American Academy of Pediatrics, Subcommittee on Attention Deficit/Hyperactivity Disorder. (2000). Clinical practice guideline: Diagnosis and evaluation of the child with attention-deficit/hyperactivity disorder. Pediatrics, 105, 1158–1170.
American Heart Association. (2008). Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/ hyperactivity disorder. Retrieved April 15, 2009, from http://circ.ahajournals.org/cgi/content/full/117/18/2407
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: APA.
Barkley, R. A., Fische, R. M., Smallish, L., & Fletcher, K. (2006). Young adult outcome of hyperactivity in children: Adaptive functioning in major life activities. Journal of the American Academy of Child and Adolescent Psychiatry, 45, 192–202.
Biederman, J. (2004). Impact of comorbidity in adults with attention-deficit/ hyperactivity disorder. Journal of Clinical Psychiatry, 65(suppl 3), 3–7.
Efron, D., Friedrich, J., & Barker, M. (1997). Side effects of methylphenidate and dexamphetamine in children with attention deficit hyperactivity disorder: A double-blind, crossover trial. Pediatrics, 100(4), 662–666.
Elia, J., Borcherding, B., Rappoport, J., & Keysor, C. (1991). Methylphenidate and dextroamphetamine treatment of hyperactivity: Are there true nonresponders? Psychiatric Research, 36, 141–155.
Epstein, J. N., Rabinar, D., & Johnson, D. E. (2007). Presenting implication of evidence based practices for ADHD children among primary care pediatricians. Archives of Pediatric and Adolescent Medicine, 161(9), 835–840.
Froelich, T. E., Lamphear, B. P., & Epstein, J. N. (2007). Prevalence, recognition and treatment of attention-deficit/hyperactivity disorder in a national sample of U.S. children. Archives of Pediatric and Adolescent Medicine, 161, 857–864.
Green, M., Wong, M., & Atkins, D. (1999). Diagnosis of attention deficit/hyperactivity disorder: Technical review. Rockville, MD: U.S. Department of Health and Human Services, Agency for Health Care Policy and Research.
Gutgesell, H., Atkins, D., Barst, R., Buck, M., Franklin, W., Hanes, R., Ringel, R., et al. (1999). Cardiovascular monitoring of children and adolescents receiving psychotropic drugs. Circulation, 99, 979–982.
Leslie, L., Weckerly, J., Plemmons, D., Landsvere, J., & Eastman, S. (2004). Implementing the American Academy of Pediatrics attention deficit/hyperactivity disorder guidelines in primary care settings. Pediatrics, 114, 129–140.
Michelson, D., Allen, J., Busner, J., Casat, C., Dunn, D., Kratochvil, C., et al. (2002). Once-daily atomoxetine treatment for children and adolescents with attention-deficit/hyperactivity disorder: A randomized, placebo-controlled study. American Journal of Psychiatry, 159, 1896–1901.
MTA Cooperative Group. (1999). A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Archives of General Psychiatry, 56, 1073–1086.
Perrin, J., Friedman, R., & Knilans, T. (2008). The Black Box Working Group and the Section on Cardiology and Cardiac Surgery. Cardiovascular monitoring and stimulant drugs for attention-deficit/hyperactivity disorder. Pediatrics, 122, 451–453.
Pliszka, S., & American Academy of Child and Adolescent Psychiatry, Work Group on Quality Issues. (2007). Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 46(7), 894–921.
Quinn, D. (2005). Poster presented at the 45th annual meeting of New Clinical Drug Evaluation Unit. Boca Raton, FL.
Vetter, V. L., Elia, J., & Erickson, C. (2008). Cardiovascular monitoring of children and adolescents with heart disease receiving stimulant drugs: A scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Heart Defects Committee and the Council on Cardiovascular Nursing. Circulation, 117(18), 2407–2423.
Wernicke, J. F., & Kratochvil, C. J. (2002). Safety profile of atomoxetine in the treatment of children and adolescents with ADHD. Journal of Clinical Psychiatry, 63(Suppl 12), 50–55.