(Pediatric Lymphomas. Berlin, Heidelberg: Springer-Verlag; 2007; Ped Rev 2003;24:380)
Definition
• Includes both B- and T-cell neoplasms with Reed–Sternberg cells absent
• Non-Hodgkin lymphomas comprise 10% of all childhood cancers
• In general, vs. Hodgkin lymphoma, sx of NHL more rapid onset and short duration and ⅔ of pts have widespread dz at time of dx
• 4 primary histologic subtypes of pediatric NHL, detailed below
• Presenting signs/sx similar to those for Hodgkin lymphoma above; except as below
Burkitt Lymphoma
• A B-cell lymphoma, most common pedi NHL: ∼40–50% of cases
• Clinical presentation: Rapidly proliferating tumor often p/w extranodal dz. Intra-abd dz common and may p/w intussusception (acts as lead point in up to 50% of kids >6 yo)
• 95% pts w/ translocation of c-myc oncogene (chromo 8) w/ Ig heavy- or light-chain gene; 80% of time, translocation is t(8:14)
• Treatment: No benefit of XRT added to chemo demonstrated
• Generally 2–6 mo chemo w/ many agents, e.g., cyclophosphamide, doxorubicin, vincristine, HD-MTX w/ AraC, ifosfamide, etoposide, and intense IT chemo for advanced stage dz
• Overall survival: 85–95% depending on stage
Diffuse Large B-cell Lymphoma
• A B-cell lymphoma; represents 20% of pediatric NHLs
• Clinical presentation: May occur at single site in nodes or bone. 1° mediastinal presentations in adolescent females and is the type of NHL associated w/ immunodeficiency and post solid organ transplant (PTLD)
• Treatment: Same as that for Burkitt lymphoma
Anaplastic Large Cell Lymphoma
• A T-cell lymphoma;10–15% of pediatric NHLs
• Clinically: B sx (∼50%) more common than other NHLs. LAD (usually periph) & usually p/w skin or soft tissue sites (skin lesions may wax/wane) 60% pts w/ extranodal involve
• Cells express CD30 and usually have a T-cell phenotype
• Treatment: Minimal risk for CNS relapse (minimal intrathecal therapy)
• Regimens vary; most w/ steroids, vincristine, doxorubicin MTX, +/− alkylating agents
Precursor B- and Precursor T-cell Lymphoblastic Lymphoma
• ∼30% of pediatric NHL
• Histologically identical to pre-B/pre-T acute lymphoblastic leukemia, but by definition has <25% involvement of bone marrow
• Clinically: Periph nodal or Waldeyer ring, T-cell lymphoma, may p/w anter mediastin mass
• Treatment: Based on high-risk ALL Rx regimens and includes intrathecal chemo
Diagnostic Evaluation of Non-Hodgkin Lymphoma (Pediatr Rev 2003;24:380)
• Same as for Hodgkin lymphoma as previous, plus CSF examination and uric acid level
Staging and Prognosis (Pediatr Rev 2003;24:380)
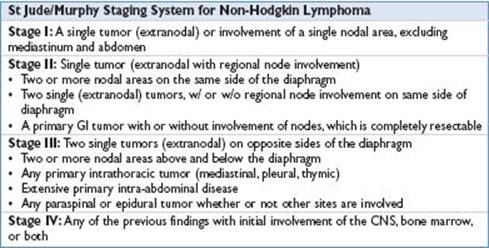
Overall Survival for Non-Hodgkin Lymphoma
• Stage I/II: ∼90–98%; stage III/IV: 70–90%