Congenital Vertical Talus
1. Definition—Deformity
a. Congenital dorsolateral dislocation of the navicular on the talus with severe eversion of the subtalar joint and rigid plantar flexion of the talus, creating a rocker-bottom appearance of the foot. The talus is vertically aligned with the tibia (Figure 5-24).
b. Idiopathic etiology or associated with an underlying neuromuscular or chromosomal abnormality
2. Elucidation of the segmental deformities
a. Forefoot—supinated
b. Midfoot
i. Abducted
ii. Medial column—dislocated
• dorsolateral dislocation of the navicular on the talus
iii. Lateral column—subluxated (or mal-oriented)
• dorsolateral subluxation and/or mal-orientation of the calcaneocuboid joint
c. Hindfoot—valgus/everted
d. Ankle—plantar flexed (equinus)

Figure 5-24. A. Medial-side photo of a CVT, the so-called “Persian slipper foot” deformity. B. Lateral radiograph shows the talus to be vertically aligned with the axis of the tibia. The calcaneus is plantar flexed. The axis of the 1st MT aligns with the dome of the talus, rather than the head.
3. Imaging
a. Simulated standing AP of foot (Figure 5-25)
b. Maximum dorsiflexion lateral of foot (Figure 5-26B)
i. The talus does not dorsiflex more than a few degrees from its colinear vertical alignment with the tibia. The calcaneus barely dorsiflexes to a right angle to the tibia. The axis of the 1st MT is dorsally translated onto the body of the talus, indicating dorsal dislocation of the navicular.
c. Maximum plantar flexion lateral of foot (Figure 5-26D)
i. The navicular does not align with the talus with forced plantar flexion. This is manifest by persistence of dorsal translation and angulation of the axis of the 1st MT in relation to the axis of the talus
4. Natural history
a. Persistence of deformity with pain, functional disability, and inability to wear normal shoes
5. Nonoperative treatment
a. Reverse Ponseti (Dobbs) casting
6. Operative indications
a. Failure to achieve full deformity correction with nonoperative treatment
7. Operative treatment with reference to the surgical techniques section of the book for each individual procedure
a. Tendo-Achilles tenotomy (see Chapter 7) and limited open talonavicular joint capsulotomy with retrograde pinning (Dobbs method)—perform this if the talonavicular joint has become aligned with reverse Ponseti (Dobbs) casting, but there is persistent equinus. This is not a plication of the medial soft tissues, but merely a capsulotomy for visualization while pinning thetalonavicular (TN) joint.
b. Dorsal approach release for CVT and COT (see Chapter 7)—perform this for failure of the reverse Ponseti (Dobbs) nonoperative method to align the talonavicular joint
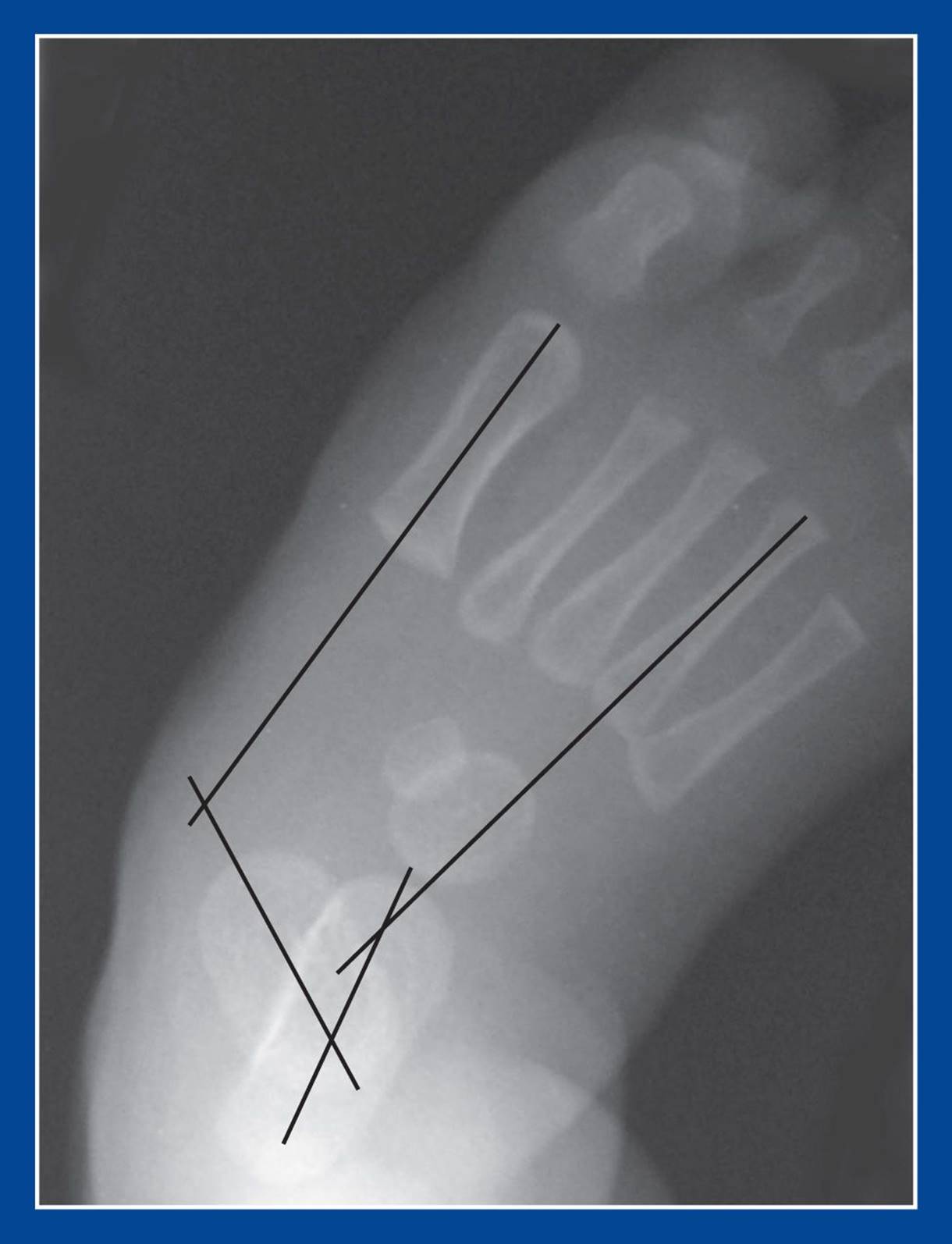
Figure 5-25. AP radiograph of a CVT. The midfoot is abducted, as indicated by the calcaneus–4th MT angle, which is straight in a normal foot and also in most flexible flatfoot deformities. The subtalar joint is severely everted, as indicated by the talus–1st MT angle. The foot-CORA (see Assessment Principle #18, Chapter 3) in CVT is often not in the talar head, whereas it is always in the talar head in a flexible flatfoot. The two possible reasons for that observation are (1) a projectional artifact created by the dorsal dislocation at the talonavicular joint and (2) a long medial column of the foot.
Congenital Oblique Talus
1. Definition—Deformity
a. There is no consensus definition
b. Congenital dorsolateral subluxation of the navicular on the talus with moderately severe eversion of the subtalar joint and moderately rigid plantar flexion of the talus, creating a mild rocker-bottom appearance of the foot. Complete inversion of the subtalar joint is not possible (Figure 5-27).
c. Idiopathic etiology or associated with an underlying neuromuscular or chromosomal abnormality
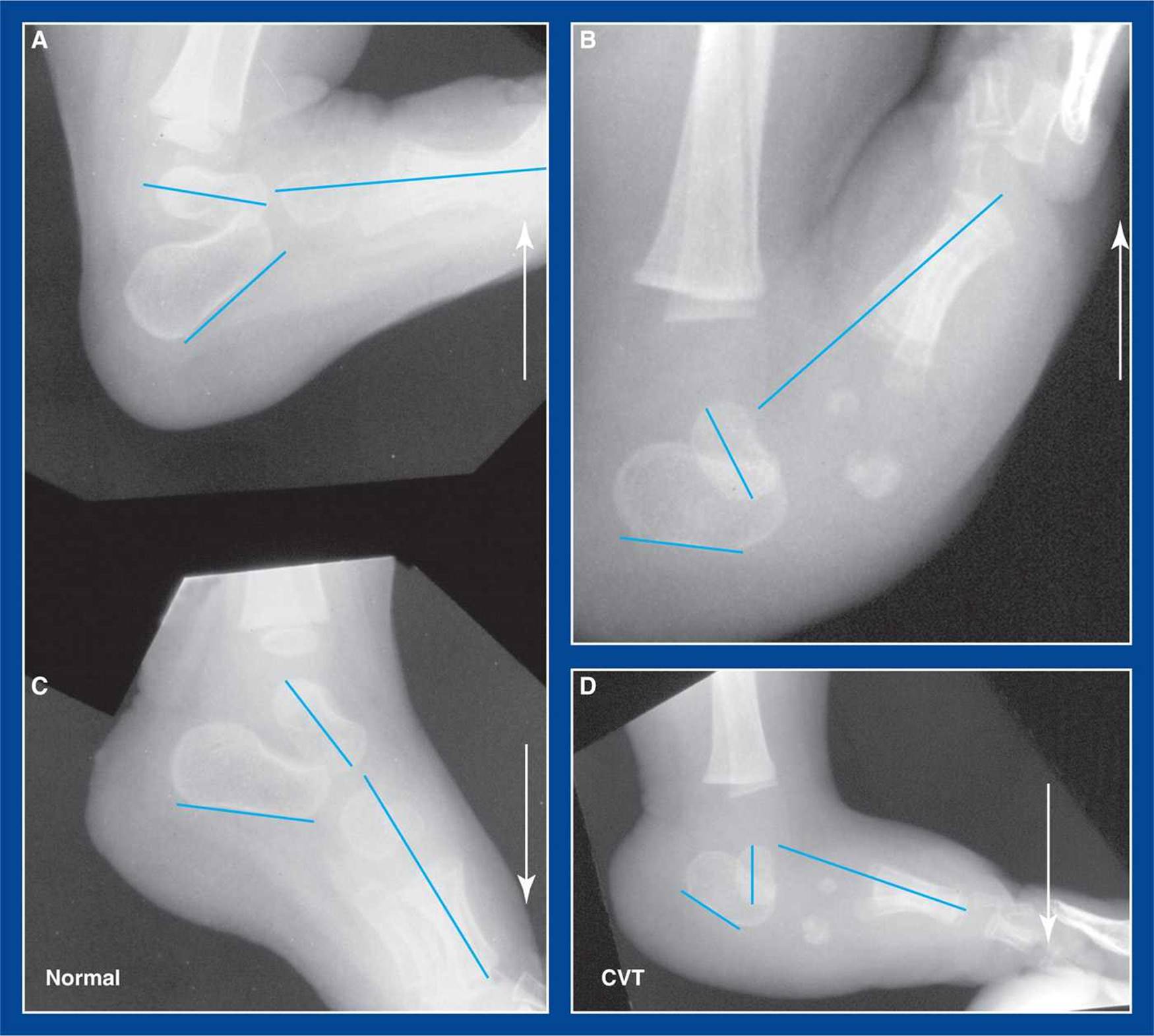
Figure 5-26. Maximum dorsiflexion and plantar flexion lateral radiographs of a normal foot and a foot with CVT. A. Maximum dorsiflexion lateral of a normal foot. The talus is perpendicular to the tibia. The talus–1st MT angle is 0°, though several degrees of dorsiflexion of the forefoot on the hindfoot are normal. The calcaneus is dorsiflexed well above perpendicular to the tibia. B. Maximum dorsiflexion lateral of a CVT. The talus rotates very slightly from its full plantar flexed position. The calcaneus is merely perpendicular to the tibia. The axis of the first MT is translated dorsally with the foot-CORA (see Assessment Principle #18,Chapter 3) in the body of the talus, indicating dorsal dislocation of the navicular at the talonavicular joint. C. Maximum plantar flexion lateral of a normal foot. The talus plantar flexes to no more than about 45°. The calcaneus plantar flexes slightly beyond perpendicular to the tibia. The axis of the 1st MT is slightly plantar flexed in relation to the axis of the talus with the foot-CORA in the talonavicular joint. D. Maximum plantar flexion lateral of a CVT. The talus is vertically in line with the axis of the tibia. The calcaneus is plantar flexed well beyond perpendicular to the tibia. The axis of the 1st MT remains dorsally translated with the foot-CORA in the body of the talus, confirming fixed dorsal dislocation of the navicular at the talonavicular joint.

Figure 5-27. Right COT. As with CVT, there is often a single posterior heel crease. There is only one deep posterior crease on the right ankle, but a deep and multiple shallow creases on the left ankle. The right foot longitudinal arch is slightly convex plantar, i.e., rocker-bottom.
2. Elucidation of the segmental deformities
a. Forefoot—supinated
b. Midfoot
i. Abducted
ii. Medial column—subluxated
• dorsolateral subluxation of the navicular on the talus
iii. Lateral column—subluxated (or mal-oriented)
• dorsolateral subluxation and/or mal-orientation of the calcaneocuboid joint
c. Hindfoot—valgus/everted
d. Ankle—plantar flexed (equinus)

Figure 5-28. COT radiographs. A. AP radiograph of an apparent flatfoot, but with the foot-CORA (see Assessment Principle #18, Chapter 3) distal to the head of the talus. B. Weight-bearing lateral radiograph shows dorsal translation of the axis of the 1st MT intersecting the neck/body of the talus. This indicates dorsal subluxation at the talonavicular joint. C. With maximum dorsiflexion of the foot, the talus does not fully dorsiflex, while the calcaneus dorsiflexes around the talus through exaggerated eversion. The axis of the 1st MT appears to be even further dorsally translated than in the weight-bearing view. D. With maximum plantar flexion of the foot, the talus assumes a nearly vertical alignment with the tibia and the calcaneus plantar flexes well. However, the axis of the 1st MT remains slightly dorsally translated in relation to the talus, confirming incomplete reduction of the navicular on the head of the talus. The lateral foot-CORA should be in the head of the talus with a convex dorsal angle between the lines (see Figure 5-26A, C).
3. Imaging (Figure 5-28)
a. Simulated standing AP of foot
b. Maximum dorsiflexion lateral of foot (Figure 5-28C)
i. The talus dorsiflexes partially, though never completely, while the calcaneus hyper-dorsiflexes past the talus through eversion. These are also features of a flexible flatfoot with a short tendo-Achilles, but in COT, the axis of the 1st MT is dorsally translated, creating a foot-CORA (center of rotation of angulation) (see Assessment Principle #18, Chapter 3) in the neck/body of the talus rather than in the head.
c. Maximum plantar flexion lateral of foot (Figure 5-28D)
i. The navicular does not completely align with the talus. The axis of the 1st MT remains dorsally translated in relation to the axis of the talus
4. Natural history
a. Persistence of deformity with pain and, possibly, functional disability (see Basic Principle #10, Chapter 2)
5. Nonoperative treatment
a. Reverse Ponseti (Dobbs) casting
6. Operative indications
a. Failure to achieve full deformity correction with nonoperative treatment
7. Operative treatment with reference to the surgical techniques section of the book for each individual procedure
a. Tendo-Achilles tenotomy (see Chapter 7) and limited open talonavicular joint capsulotomy with retrograde pinning (Dobbs method)—perform this if the talonavicular joint has become aligned with reverse Ponseti (Dobbs) casting, but there is persistent equinus. This is not a plication of the medial soft tissues, but merely a capsulotomy for visualization while pinning the TN joint.
b. Deep plantar–medial plication (see Chapter 7), tendo-Achilles tenotomy (see Chapter 7), ± peroneus brevis tendon lengthening—perform this in an infant or young child for failure of the reverse Ponseti (Dobbs) nonoperative method to align the talonavicular joint
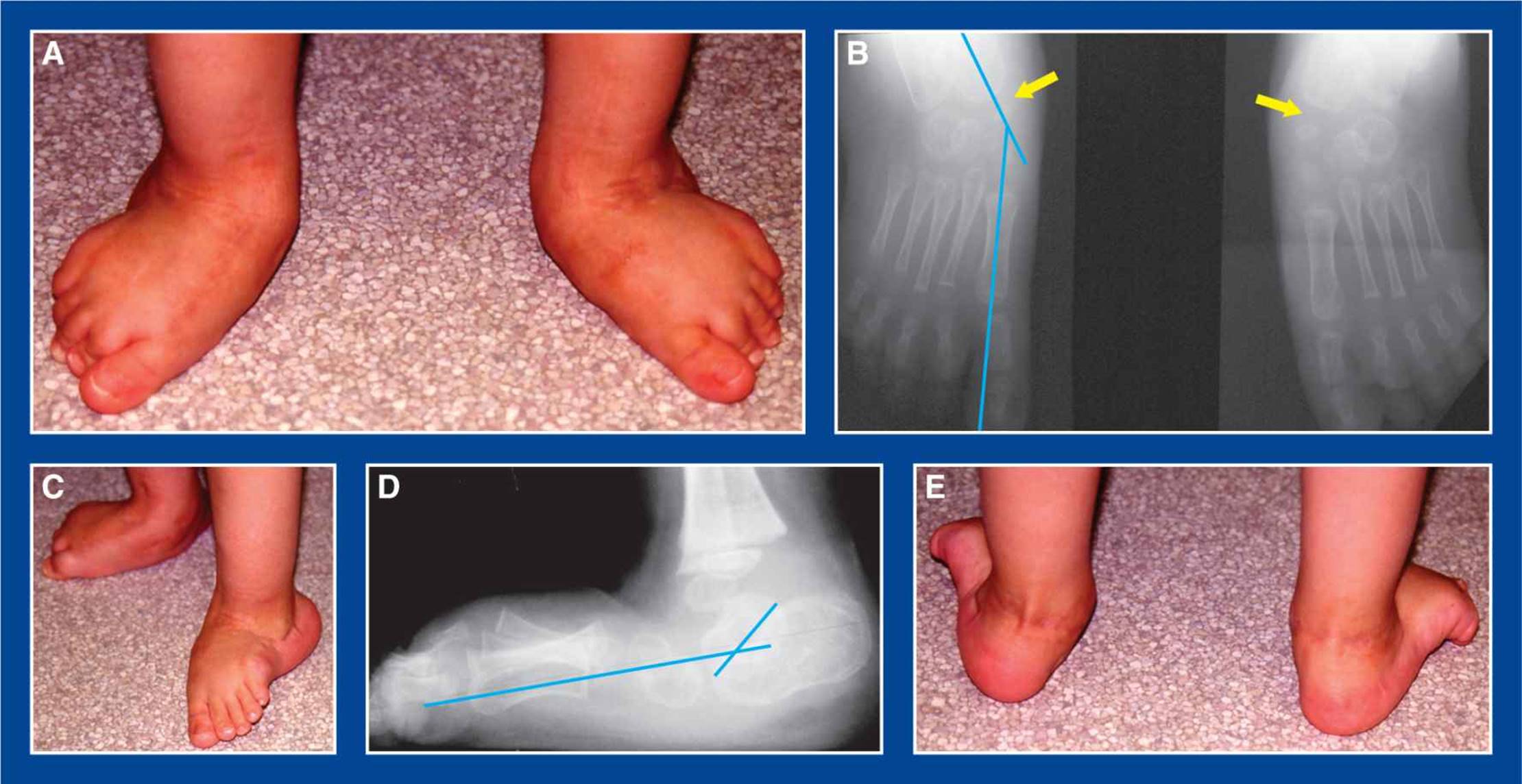
Figure 5-29. Example of a residual CVT in a recently operated 3-year-old child. A. Following circumferential release and realignment surgery in this older child, there is severe residual abduction/valgus deformity in both feet. B. Though not always the case, the talonavicular joints are well-aligned (yellow arrows) despite severe residual deformities. The foot-CORA is in the navicular bone (crossing of the blue axis lines of the 1st MT and talus), indicating that the deformity is not primary eversion of the subtalar joint (in which case the foot-CORA would be in the head of the talus). Instead, the foot-CORA indicates that the residual deformity is, at least in part, related to a longer medial than lateral column in each foot. This has implications for treatment, such as the possible/probable need to shorten the medial column by naviculectomy. C. Lateral photos show a concave, short lateral column of the left foot, and a convex, long medial column of the right foot. D. Standing lateral radiograph shows moderate residual hindfoot equinus with sag at the talonavicular joint. The foot-CORA is in the head of the talus, indicating no residual dorsal subluxation or dislocation at the talonavicular joint. E. Posterior views of the feet show severe hindfoot valgus and midfoot abduction.
Neglected/Recurrent/Residual CVT
1. Definition—Deformity
a. Untreated, recurrent, or residual congenital dorsolateral dislocation of the navicular on the talus with severe eversion of the subtalar joint and rigid plantar flexion of the talus, creating a rocker-bottom appearance of the foot in an older child. There is suggestive evidence that the medial column of the foot grows faster and is longer than the lateral column in neglected (untreated), recurrent, and residual CVT deformities (Figure 5-29)
b. Idiopathic etiology or associated with an underlying neuromuscular or chromosomal abnormality
2. Elucidation of the segmental deformities
a. Forefoot—supinated
b. Midfoot
i. Abducted
ii. Medial column—dislocated
• dorsolateral dislocation of the navicular on the talus
iii. Lateral column—subluxated (or mal-oriented)
• dorsolateral subluxation and/or mal-orientation of the calcaneocuboid joint
c. Hindfoot—valgus/everted
d. Ankle—plantar flexed (equinus)
3. Imaging
a. Simulated standing or standing AP of foot
b. Maximum dorsiflexion lateral of foot
i. The talus is vertically and rigidly aligned with the tibia in untreated cases, and dorsiflexes incompletely in recurrent and residual cases
c. Maximum plantar flexion lateral of foot
i. The navicular does not align with the talus
4. Natural history
a. Persistence of deformity with pain, functional disability, and inability to wear normal shoes
5. Nonoperative treatment
a. Reverse Ponseti (Dobbs) casting
6. Operative indications
a. Failure to achieve full deformity correction with nonoperative treatment
7. Operative treatment with reference to the surgical techniques section of the book for each individual procedure
a. Posterolateral soft tissue release and plantar–medial plication (see Chapter 7) and tendo-Achilles lengthening (see Chapter 7) ± peroneus brevis tendon lengthening—perform this in an infant or young child for failure of the reverse Ponseti (Dobbs) nonoperative method to align the talonavicular joint
b. Naviculectomy (see Chapter 8)—perform this:
i. if the talonavicular joint is well-aligned (Figure 5-29) or becomes well-aligned with serial casting or posterolateral release, yet the deformity persists
ii. or, if the talonavicular joint cannot be aligned with a posterolateral soft tissue release because of resistance of the lateral soft tissues or too short a lateral column of the foot (too long a medial column)
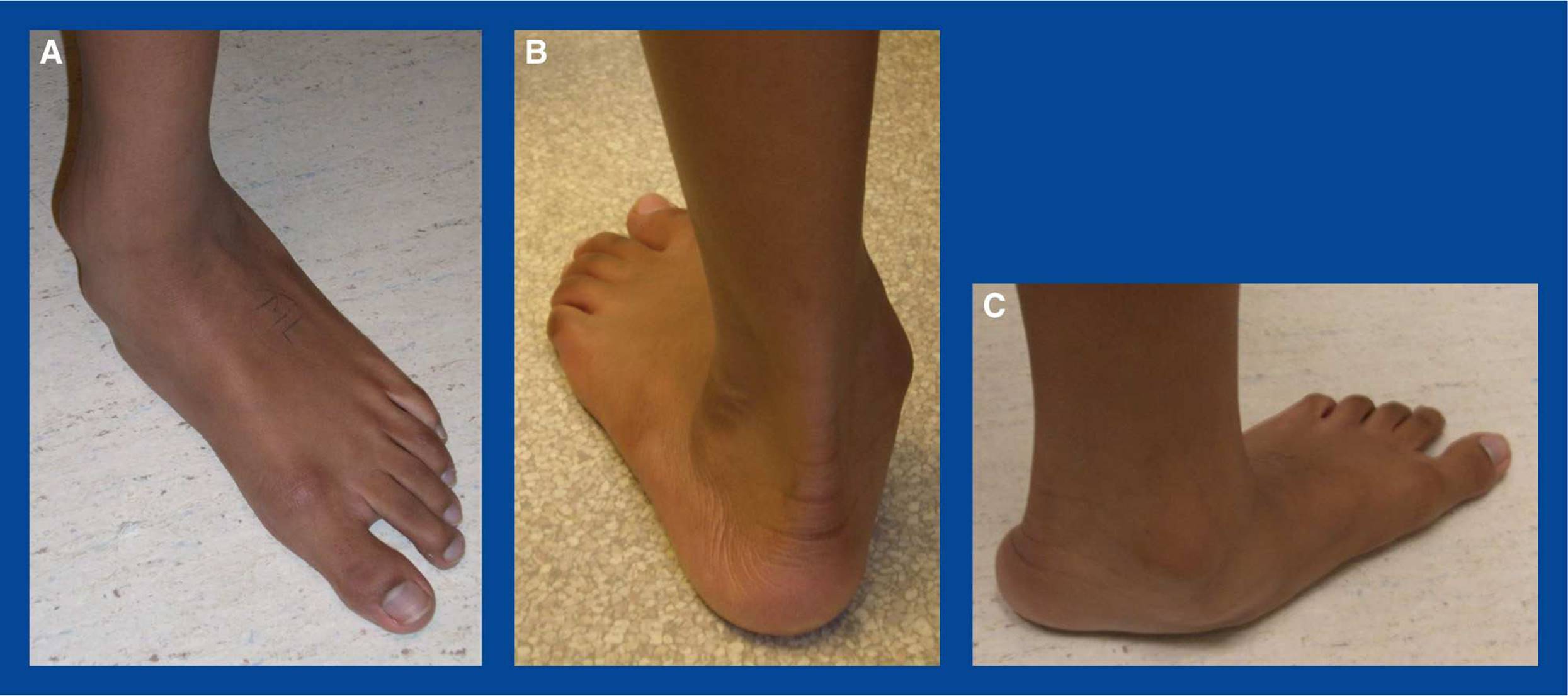
Figure 5-30. Flatfoot. A. Top view shows the outward (external) rotation of the foot in relation to the lower extremity that takes place in the subtalar joint (see Basic Principle #6, Figure 2-7, Chapter 2). The patella is facing directly forward (toward the bottom of the picture) in this image. B. Back view shows valgus alignment of the hindfoot and “too many toes” seen laterally. C. Medial view shows depression of the longitudinal arch and a convex medial border of the foot. Supination of the forefoot in relation to the hindfoot is apparent because all MT heads are on the ground despite valgus alignment of the hindfoot (see Assessment Principle #8, Figure 3-2, Chapter 3).