Catherine Porter Moore
HIGH-YIELD FACTS
• In all cases of psychiatric emergencies, organic disease etiology must be ruled out!
• The majority of adolescents are relieved to discuss psychiatric issues and actively seek treatment.
• It is essential to introduce community resources such as crisis lines, substance abuse resources, and centers to patients and families.
• Suicide is common in adolescents: 20% to 25% of American adolescents have considered suicide seriously, 9% have attempted, and it is the third leading cause of death in 15- to 24-year olds and fifth in 5- to 14-year olds.
• Suicide National Hotline: 1-800-suicide.
• Schizophrenia tends to run in families.
• Conversion/somatization disorder is characterized by the presence of apparent physical disease that cannot be delineated organically and has pathologic origination in the psyche, which may present as abdominal pain, respiratory difficulty (paradoxical vocal cord dysfunction), pseudoseizures, and other somatoform disorders.
In 1999 the National Institute of Mental Health estimated that 10% of children have mental illness.1 By all estimates the number of children with significant psychiatric emergencies presenting to the emergency department (ED) continues to rise and requires significant resources. The first priority in evaluating and treating psychiatric patients in the ED is to determine the risk the patients pose to themselves and others. This assessment guides how best to care for the patient. Safe rooms that have no equipment and are highly visible to staff are optimal for psychiatric patients. Some patients may need one-on-one supervision by staff, others may need restraint.
Table 145-1 lists the historical information that should be obtained from a patient with psychiatric issues presenting to the ED. Emphasis should be placed on past psychiatric history with current medications taken, and a thorough social history to assess the home living condition, family and school relationship problems, and any history of substance abuse. It is important to ascertain the patient’s use of social networking (Facebook, etc.) as this can comprise a whole layer of social stressors. After collecting the history from the patient and parent in the examining room together, it is also vital to collect history from parents alone as well as from the child in the absence of the parents.
|
TABLE 145-1 |
The Mental Status Examination |
• Chief complaint
• History of present illness
• Past psychiatric history
• Birth and development history
• Past medical and surgical history, current medications, allergies
• Family history of medical and psychiatric issues
• Social history, living situation, use of social media, school, grade, friends, history of abuse
• Substance abuse
• Medical and psychiatric system review
Examination of the psychiatric patient includes a full physical examination as well as complete neuro and mental status examination. The elements of a mental status examination are reviewed in Table 145-2. Attention should be paid to the caretakers as well as the patient. Assessment of the mental status of the caretaker can reveal much about the parent–child relationship and function.
|
TABLE 145-2 |
The Mental Status Examination |
• ORIENTATION: Time, Place, Person, Why they are here?
• APPEARANCE: Neat? Well groomed? Caretaker’s appearance?
• BEHAVIOR: Cooperative? Anxious? Agitated?
• PSYCHOMOTOR: Physical activity? Tics? Movements?
• MOOD: Happy? Angry? Sad? Depressed?
• AFFECT: Flat? Warm?
• THOUGHT PROCESS: Organized? Logical? Stray from topic to topic?
• THOUGHT CONTENT: Delusional? Hallucinating? Paranoid?
• SPEECH: Rambling? Tone? Volume?
• INSIGHT: Understanding of issues that prompted the visit?
• JUDGMENT: Test of rational, clear thinking
• MEMORY: Short-term and delayed recall
• COGNITION: Reasoning, interpretation of complex ideas (calculations)
THE SUICIDAL PATIENT
![]() ETIOLOGY/PATHOGENESIS
ETIOLOGY/PATHOGENESIS
Biological correlations have been made with suicidal ideation. Low CSF levels of 5-hydroxy-indolacetic acid, low platelet imipramine binding, anomalies in the hypothalamic–pituitary–adrenal axis, sleep EEG abnormalities, and decreased REM sleep have been noted in patients with suicidal tendencies.2 Most suicidal patients have psychiatric pathology with the most common being major depressive disorder (MDD)/dysthymia followed by disruptive behavior disorder, drug/alcohol abuse, and dependence and anxiety disorder.2
![]() RECOGNITION
RECOGNITION
Many tools and psychiatric assessment modules have been designed to assess the suicidal patient. Usually patients present with a chief complaint of a suicide attempt that they confessed to or were confronted about. It is important to assess whether a patient with mental illness is at risk of suicide while in the ED. This can be ascertained in the interview. Horowitz and colleagues suggested a four-question (yes/no/don’t know) screening tool that yields the highest sensitivity and negative predictive value to rapidly detect suicide risk.3: (1) Are you here because you tried to hurt yourself? (2) In the past week, have you been having thoughts about killing yourself? (3) Have you ever tried to hurt yourself in the past other than this time? (4) Has something very stressful happened to you in the past few weeks? The more “yes” answers, the greater the risk of the patient posing a threat to themselves.
MANAGEMENT
In the initial management of patients with suicidal tendency, it is vital that the interviewer be compassionate. The interviewer should ascertain: (1) the reason the patients desire to hurt themselves, (2) the plan to do so, (3) whether the patients have the means necessary to carry out the plan, and (4) the timing of the plan’s execution. Recent data suggest increased urgency when suicidal patients have psychotic symptoms as they are 20 times more likely to execute a plan of suicide as compared with their nonpsychotic counterparts.4 Hospitalization is warranted if there are any medical issues, or the patient is not deemed safe for discharge. Concerns for patient safety include the following:
• Inability to maintain a safety (no-suicide) contract
• Active suicidal ideation (plan and intent)
• High intent or lethality of attempt
• Psychosis
• Volatile/unsafe family and home environment
Treatment of the patient with suicidal tendency may include both medical therapy and counseling. Multiple studies suggest that combining medical therapy (antidepressants such as a selective serotonin reuptake inhibitor [SSRI]) and cognitive behavioral therapy has the highest success rate. Treatment of depression with SSRI drugs has come under fire in recent years. In 2004, the FDA issued a black box warning for all SSRIs, warning that “antidepressants increased the risk compared to placebo of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults in short-term studies of MDD and other psychiatric disorders.”5 Bridge et al. published a meta-analysis that showed antidepressant use in children, adolescents, and young adults causes greater benefit than harm.6 This study suggested close follow-up and evaluation of the patient and that patients on SSRIs are not at a greater risk in the ED than those who are not on SSRIs.
![]() ANCILLARY STUDIES
ANCILLARY STUDIES
If the patient’s mental status is altered, a toxicology screen and ethanol level are warranted. Many intoxicated suicidal patients are no longer suicidal once the intoxicant wears off. Organic disease must be ruled out. Thyroid disease, autoimmune disease, and other organic disease states can cause or augment a patient’s depression and tendency to commit suicide.
THE PSYCHOTIC PATIENT
![]() ETIOLOGY/PATHOGENESIS
ETIOLOGY/PATHOGENESIS
Pediatric schizophrenia presents with psychosis at or before 12 years of age. DSM-IV-TR criteria include hallucinations (79%–82%), delusions (54%–63%), and thought disorder (40%–100%). Disorganized behavior, negative symptoms and impaired functioning, and symptoms of later onset disease are not particularly diagnostic in children.7 Psychosis can be a feature of many other psychiatric diagnoses including MDD, bipolar disorder, and schizoform disorder.
Most pediatric patients present with a chief complaint of auditory and/or visual hallucinations. The etiology can be basic psychiatric illness, but again it is essential that organic disease be ruled out. There are many medical conditions that produce psychosis including infection, rheumatic disease, especially lupus,8 cerebral blood flow changes/hypoxia, temporal lobe epilepsy,9 toxicological, vitamin deficiencies, metabolic and endocrine disorders, Reye syndrome, Wilson disease, and encephalopathy with varied etiologies from infectious to Hashimoto encephalopathy.10
![]() MANAGEMENT
MANAGEMENT
Treatment of psychosis in the acute care setting is mostly pharmacological. Antipsychotics such as olanzapine, risperidone, and haloperidol have been used in pediatric ED settings. Acute psychosis always warrants hospitalization until the etiology is elucidated. Chronic psychosis merits hospitalization when it is impairing the patient’s normal function, or the patient has any suicidal or homicidal ideation.
![]() ANCILLARY STUDIES
ANCILLARY STUDIES
Ancillary studies are aimed at ruling out organic disease. These patients should be assessed for altered mental status. This workup should include toxicology, electrolytes, kidney and liver functions, and ammonia level. Imaging including CT scan, MRI, and EEG may be necessary in selected cases. A lumbar puncture may be warranted to evaluate for meningitis and encephalitis.
POSTTRAUMATIC STRESS DISORDER
![]() ETIOLOGY/PATHOGENESIS
ETIOLOGY/PATHOGENESIS
Posttraumatic stress disorder (PTSD) emerges after traumatic events that evoke intense fear, helplessness, or horror. The patient may have been involved in or been a witness to the trauma.
Children with burn injuries have over a 50% chance of having symptoms of PTSD.11 The hypothalamic–pituitary–adrenal axis has been noted to be hyperactive in children and adolescents diagnosed with PTSD. Overall, these patients have elevated cortisol levels in urine and saliva.12 Elevations in sympathetic nervous activity are consistently demonstrated in PTSD.13 In the acute setting of trauma, pain and anxiety control are paramount in preventing PTSD. Studies examining medical treatments (propranolol, hydrocortisone, SSRIs) following acute trauma to prevent PTSD are few and small. More needs to be done to better delineate appropriate prevention of PTSD in regard to age and sex in the pediatric population.14
![]() RECOGNITION
RECOGNITION
In the acute care setting, PTSD is something that should be recognized by its symptoms of intrusive memories and/or dreams of the traumatizing event, avoidance of stimuli connected to the traumatic event, symptoms of excessive arousal/anxiety including inability to concentrate on tasks, exaggerated startle response, hypervigilance, insomnia, and inappropriate outbursts. These symptoms will manifest differently in different developmental stages. PTSD is distinguished from acute stress disorder with 4 or more weeks of symptoms.
![]() MANAGEMENT
MANAGEMENT
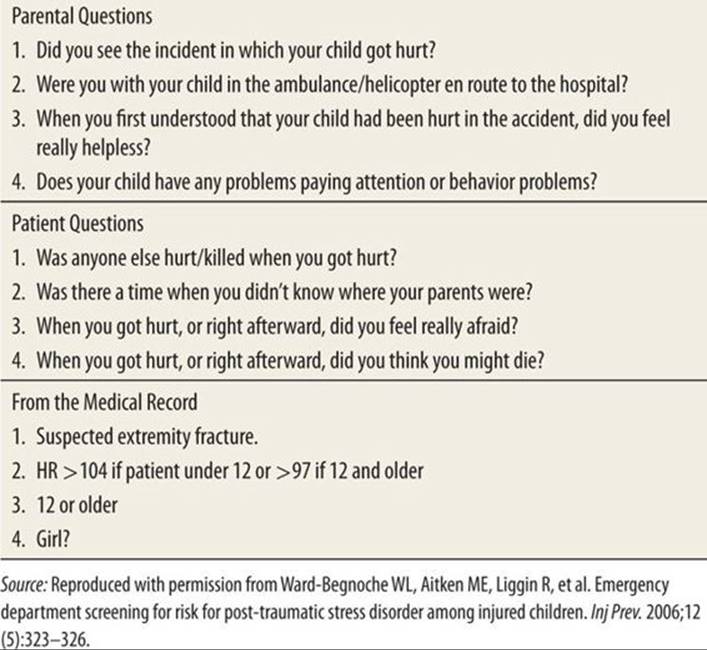
The Screening Tool for Early Predictors of PTSD (STEPP) at the initial trauma presentation is composed of four questions for the patient, four questions for the parents, and four items from the medical record, which, based on previous studies, have shown to correlate with a greater likelihood of developing PTSD.15 Table 145-3 lists the items shown to increase the risk of developing PTSD. More questions answered with a “yes” indicate a higher probability to develop PTSD. Patients at greater risk of PTSD need ongoing follow-up to ensure that their pathology does not become more severe. There is no laboratory or radiographic test to confirm or deny the existence of PTSD.
|
TABLE 144-3 |
Screening for Posttraumatic Stress Disorder |
THE PSYCHOPATHIC PATIENT: WHEN JUNIOR KILLS FIDO
American Heritage Dictionary defines psychopath as “a person with an antisocial personality disorder, manifested in aggressive, perverted, criminal, or amoral behavior without empathy or remorse.”16Antisocial personality disorder (APD) can only be diagnosed at 18 years of age or older. Children and adolescents often are diagnosed with oppositional defiant disorder (ODD) and conduct disorder (CD) prior to their diagnosis of APD. ODD is characterized by a pattern of negativity, hostility, and defiance lasting for at least 6 months during which four DSM-IV criteria are met. Diagnosis of CD is based on persistent history of “when a child seriously misbehaves with aggressive or nonaggressive behaviors against people, animals or property that may be characterized as belligerent, destructive, threatening, physically cruel, deceitful, disobedient, or dishonest. This may include stealing, intentional injury, and forced sexual activity.”16
ETIOLOGY/PATHOGENESIS
It has been suggested that APD, CD, and ODD originate in poor bonding with the mother in the first 5 years of life. It is noted that these patients have deficits in fear recognition similar to patients with amygdala damage.17 Rarely does a case of ODD present in the ED. Certain behaviors of great concern to parents may present in the ED and can be characteristic of serious pathology. Fire starting and animal torture/killing are two such behaviors that deserve psychiatric evaluation. These patients may require intensive and long-term therapy, which should commence at the time of presentation to prevent worsening and progression to APD.
CONVERSION/SOMATIZATION DISORDER
![]() ETIOLOGY/PATHOGENESIS
ETIOLOGY/PATHOGENESIS
Conversion/somatization disorder is thought to be triggered by psychosocial stressors. It has been postulated that emotional pain turns to physical pain in patients whose families address physical pain preferentially.18 These complaints are not intentional, unlike factitious disorder and malingering. In one study, it was noted that boys with somatoform disorders had significantly poorer interpersonal relations and communications, whereas girls had higher rates of conflicts with family members.19
![]() RECOGNITION
RECOGNITION
Once the possibility of organic disease has been excluded, psychiatric evaluation can make the diagnosis. In the case of paradoxical vocal cord dysfunction, the patient presents in refractory respiratory distress. Direct visualization of abnormal vocal cord movement (closing of the cords on inhalation) is the definite means of establishing the diagnosis.20 Nonepileptic seizures (NESs) are associated with the DSM-IV diagnosis of conversion disorder and often take years to differentiate from epileptic seizures. Historically, NESs occur more in stressful situations and not during sleep. They also register negative on the EEG.21
![]() TREATMENT/MANAGEMENT
TREATMENT/MANAGEMENT
Often hospitalized for the somatic complaint, once diagnosed with conversion/somatizaion, these patients are treated with psychotherapy and medical management (often SSRIs) to help the patients cope with the underlying stressor(s). These can be very serious in the case of abuse (physical or sexual) or bullying (personal or cyber), and may require acute interventions by family services as well as psychiatric teams and counselors.
THE AGGRESSIVE PATIENT
Aggressive patients are rare in the pediatric ED compared to the adult world, but they present a unique set of challenges. It is important to look for the etiology of the patient’s aggression/discontent. If it can be easily removed from the patient’s environment, it should be. Aggressive patients need to be well supervised where they do not have the means to harm themselves or others. If verbal reassurance is ineffective in diffusing the aggression, positioning law enforcement within view of the patient can add gravity to verbal direction given by medical personnel. Escalation in care proceeds to seclusion and therapeutic holding with at least two people physically restraining the patient.22 In brief, the recommendations of the American Academy of Pediatrics are to: (1) explain the necessity of restraint to the patient, (2) have specific physician orders including indication for and duration of restraint, (3) explain everything to the family, and (4) perform and document ongoing assessment of correct application of restraints, skin and neurovascular integrity, as well as efficacy of the restraints in meeting the indication for application.22 Documentation for all restraints (physical/chemical) should mention what was done to protect the patient’s well-being, best interest, rights, privacy, and self-respect.
Physical restraint is a good initial step in stabilization. If care requires escalation, chemical restraint may be warranted. The goals of chemical restraint are to: (1) decrease the patient’s anxiety and discomfort, (2) minimize disruptive behavior, (3) prevent escalation of behavior, and (4) reverse the underlying cause.23 Many agents have been employed, about half of which have FDA approval for indications in children. All chemical restraint use requires careful monitoring of the patient on cardiac, apnea, and pulse oximetry monitoring. Benzodiazepines work to sedate patients by activating GABA receptors and can, therefore, be helpful in aggressive behavior modification. Midazolam has the shortest duration of action of the benzodiazepines. Diazepam is available in a per rectum (PR) formulation as well. The major side effect is respiratory depression. Neuroleptic drugs, such as haloperidol, have been utilized extensively in treating the aggressive patient in the acute care setting, owing to their sedating effects rather than their antipsychotic effect, which usually takes 7 to 10 days to take effect. The rare incidence (1%) of extrapyramidal symptoms (EPSs) can occur after one dose of neuroleptic drugs. Most commonly seen is dystonic reaction involving eyes, neck, and/or back. Rarely does EPS affect the airway. The treatment for EPS is diphenhydramine (IV or IM) and/or benztropine (IV or IM).23 Neuroleptic malignant syndrome is a potentially fatal reaction characterized by fever, sweating, hypertension, severe muscle rigidity, and delirium sometimes progressing to coma. Patients should be treated with dantrolene and supportive care. Droperidol is another neuroleptic drug used in the treatment of the aggressive patient. It alters the action of dopamine at subcortical levels to produce sedation and a dissociative state with a faster onset of action than haloperidol. In 2001, the FDA issued a black box warning of fatal arrthymias associated with droperidol use; however, subsequent studies have not corroborated this particular risk, but have confirmed the most common side effect of dystonia.23 Atypical antipsychotics, such as ziprasidone and olanzapine, are gaining favor in the acute management of aggressive patients. With a lower incidence of EPS, multiple routes of administration, and better tolerance, they are commonly used in the pediatric ED. Ziprasidone and olanzapine are recommended for the agitated schizophrenic patients. Olanzapine is also indicated for aggression/agitation associated with bipolar disorder. Hydroxyzine is an antihistamine that has been used as an anxiolytic, can be administered IM, and has an onset of action comparable to that of lorazapam.
PSYCHOTROPIC MEDICATIONS
Many medications are utilized in the management of psychiatric conditions in childhood and adolescence. It is important to understand the pharmacology of these medications in the context of the ED. Table 145-4 reviews agents used in the outpatient/long-term setting with potential side effects that could bring patients to the ED.
|
TABLE 144-4 |
Psychiatric Medications with Side Effects often Requiring ED Visits |

REFERENCES
1. US Department of Health and Human Services; US Department of Education; US Department of Justice. Report of the Surgeon General’s Conference on Children’s Mental Health: A National Action Agenda. Washington DC: US Department of Health and Human Services; 2000
2. Greydanus DE, Calles J Jr. Suicide in children and adolescents. Prim Care Office Pract. 2007;34:259–273.
3. Horowitz LM, Wang PS, Koocher GP, et al. Detecting suicide risk in a pediatric emergency department: development of a brief screening tool. Pediatrics. 2001;107:1133–1137.
4. Kelleher I, Lynch F, Harley M, et al. Psychotic Symptoms in Adolescence Index Risk for Suicidal Behavior: Findings From 2 Population-Based Case-Control Clinical Interview Studies. Arch Gen Psychiatry. 2012;1–7. doi:10.1001/archgenpsychiatry.2012.164.
5. Food and Drug Administration. Anti Depressant Box Warning. Beltsville, MD: 2007. http://www.fda.gov/cder/drug/antidepressants/antidepressants_label_change_2007.pdf.
6. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. J Am Med Assoc. 2007;297:1684–1696.
7. Pavuluri MN, Janicak PG, Naylor MW, et al. Early recognition and differentiation of pediatric schizophrenia and bipolar disorder. Adolesc Psychiatry. 2003;27:117–134.
8. Benseler SM, Silverman ED. Neuropsychiatric involvement in pediatric systemic lupus erythematosus. Lupus. 2007;16:564–571.
9. Oner O, Unal O, Deda G. A case of psychosis with temporal lobe epilepsy: SPECT changes with treatment. Pediatr Neurol. 2005;32:197–200.
10. Bismilla Z, Sell E, Donner E. Hashimoto encephalopathy responding to risperidone. J Child Neurol. 2007;22:855–857.
11. Pervanidou P, Chrousos GP. Post-traumatic stress disorder in children and adolescents: from Sigmund Freud’s “trauma” to psychopathology and the (Dys)metabolic syndrome. Horm Metab Res. 2007;39:413–419.
12. Langeland W, Olff M. Psychobiology of posttraumatic stress disorder in pediatric injury patients: a review of the literature. Neurosc Beh Rev. 2008;32:161–174.
13. Maccani MA, Delahanty DL, Nugent NR, Berkowitz SJ. Pharmacological secondary prevention of PTSD in youth: Challenges and opportunities for advancement. J Trauma Stress. 2012;25:543–550.
14. Ward-Begnoche WL, Aitken ME, Liggin R, et al. Emergency department screening for risk for post-traumatic stress disorder among injured children. Inj Prev. 2006;12:323–326.
15. The American Heritage Dictionary of the English Language. 4th ed. Boston, MA: Houghton Mifflin Company. http://www.bartleby.com/61/61/P0636100.html. Accessed December 4, 2006.
16. American Psychiatry Association. BehaveNet® Clinical Capsule. APA Diagnostic Classification DSM-IV-TR. Bellevue, WA: 2000. http://www.behavenet.com/capsules/disorders/dsm4TRclassification.htm. Accessed January 10, 2005.
17. Dadds MR, Perry Y, Hawes DJ, et al. Attention to the eyes and fear-recognition deficits in child psychopathy. Br J Psychiatry. 2006;189:280–281.
18. Silber TJ. Somatization disorders: diagnosis, treatment, and prognosis. Pediatr Rev. 2011;32:56–63.
19. Bisht J, Sankhyan N, Kaushal R, Sharma RC, Grover N. Clinical profile of pediatric somatoform disorders. Indian Pediatr. 2008;45:111–115.
20. Loe RJ, Konakanchi R. Psychogenic respiratory distress: a case of paradoxical vocal cord dysfunction and literature review. J Clin Psychiatry. 1999;1:39–46.
21. Plioplys S, Asato MR, Bursch B, Salpekar JA, Shaw R, Caplan R. Multidisciplinary management of pediatric nonepileptic seizures. J Am Acad Child Adolesc Psychiatry. 2007;46:1491–1495.
22. American Academy of Pediatrics, Committee on Pediatric Emergency Medicine. The use of physical restraint interventions for children and adolescents in the acute care setting. Pediatrics. 1997;99:497.
23. Sorrentino A. Chemical restraints for the agitated, violent, or psychotic pediatric patient in the emergency department: controversies and recommendations. Curr Opin Pediatr. 2004;16:201–205.