11.1 Epilepsy and Seizures
The term epilepsy is a collective designation for a group of chronic central nervous system (CNS) disorders characterized by recurrent abnormal discharges of CNS neurons. The abnormal discharge may be limited to a focal area or encompass diffuse areas of the brain. Although the abnormal discharge itself may have no clinical manifestations, such a discharge often leads to a seizure. The epileptic seizure takes many forms, ranging from brief cessations of responsiveness without loss of consciousness to convulsions with accompanying loss of consciousness. Table 11.1 describes the different seizure types.
|
Table 11.1 |
||
|
Seizure Type |
Features |
|
|
Partial seizures (focal, local) |
Simple |
Motor, somatosensory, autonomic, or psychic symptoms, with loss of consciousness |
|
Complex |
Impaired consciousness at the outset Simple partial seizure followed by impaired consciousness |
|
|
Generalized seizures (convulsive or nonconvulsive) |
Absence Typical Atypical |
Sudden brief lapses of consciousness with loss of posture Typical form + brief motor activity or loss of muscle tone |
|
Myoclonic |
Isolated jerking movements |
|
|
Clonic |
Repetitive jerking movements without muscle rigidity |
|
|
Tonic |
Muscle rigidity without jerking movements |
|
|
Tonic-clonic |
Muscle rigidity followed by rhythmic jerking movements |
|
|
Atonic |
Loss of muscle tone |
|
|
* Partial seizures can evolve to generalized tonic-clonic. |
||
Misdiagnosis or improper drug selection generally makes epilepsy worse, so it is critical that the correct seizure disorder is identified and that it is treated with the most efficacious drug. If the drug of choice fails to control the seizures, then a follow-up agent is used.
Status epilepticus
Status epilepticus is the term used to describe prolonged seizures (usually lasting 30 minutes or more) or multiple seizures that occur without recovery of consciousness. Status epilepticus constitutes a medical emergency, as the risk of death or brain damage increases the longer the seizures continue. Treatment involves maintaining the patient's airway and giving oxygen, a bolus of glucose (as the brain is a huge consumer of glucose), and intravenous (IV) or rectal diazepam to terminate the seizure. IV diazepam is given in the form of an emulsion to prevent thrombophlebitis (inflammation of a vein due to a blood clot).
11.2 Antiepileptic Agents
Phenytoin
Mechanism of action. Phenytoin limits the repetitive firing of action potentials in brain neurons by slowing the rate of recovery of voltage-activated Na+ channels from inactivation (Fig. 11.1).
Pharmacokinetics
– Slow, unpredictable absorption
– Ninety percent bound to plasma proteins
– Metabolized in liver to inactive metabolites
Uses
– Effective in all types of epilepsy except absence and atonic seizures
– Trigeminal neuralgia
Side effects. Phenytoin is relatively safe, but the following may occur:
– Gingival hyperplasia is the most common side effect in children (20% of patients). Infections are minimized by good oral hygiene.
– CNS: nystagmus, ataxia, vertigo, and diplopia
– Hyperglycemia, osteomalacia, lymphadenopathy, rashes (Stevens-Johnson syndrome [erythema multiforme bullosum]), and hematological reactions (leukopenia, megaloblastic anemia, thrombocytopenia, agranulocytosis, and aplastic anemia). These are allergic reactions that require cessation of therapy.
– Hirsutism
– Fetal abnormalities
– Cardiovascular collapse can occur after IV phenytoin.
Drug interactions
– Metabolism of phenytoin can be increased or decreased by agents that can induce or inhibit cytochrome P-450 enzymes.
– Phenytoin induces hepatic microsomal enzymes; it thus reduces the plasma concentration of drugs that are metabolized by these enzymes, including warfarin, oral contraceptives, carbamazepine, and some antibiotics.
– Drugs that bind to plasma proteins will displace phenytoin, which could result in toxicity.
Carbamazepine
Mechanism of action. Carbamazepine limits the repetitive firing of action potentials by slowing the rate of recovery of voltage-activated Na+ channels from inactivation (Fig. 11.1).
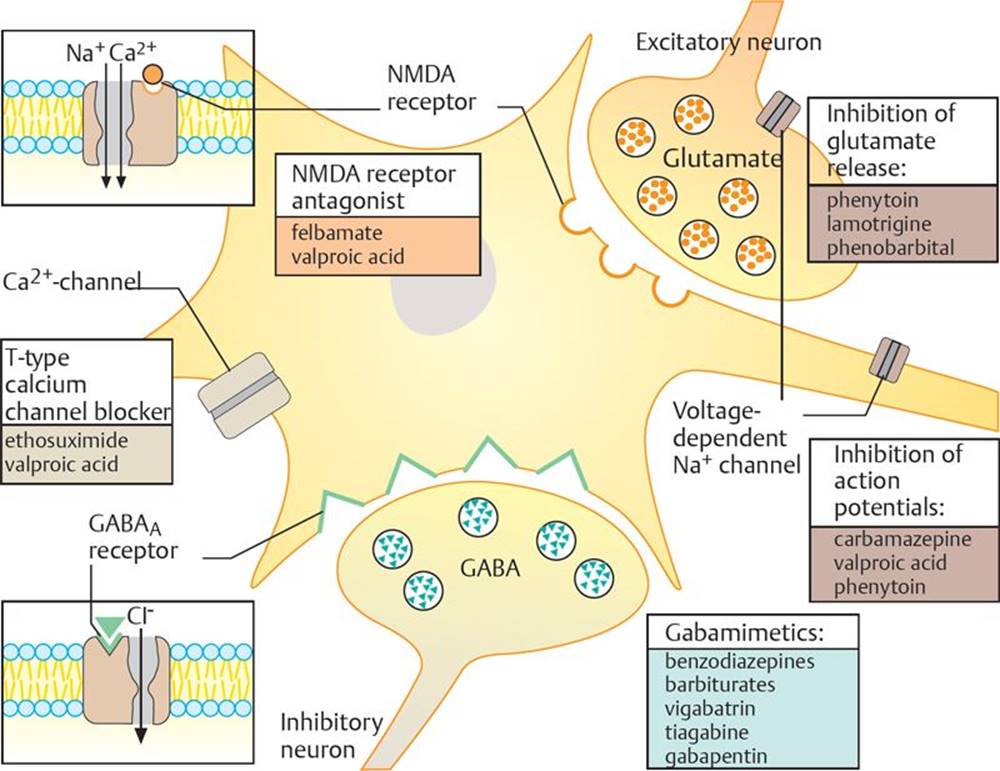
Fig. 11.1 ![]() Neuronal sites of action of antiepileptics.
Neuronal sites of action of antiepileptics.
Antiepileptic drugs act at many neuronal sites to inhibit excitation of the neuron. Gamma-aminobutyric acid (GABA) mimetics enhance the inhibitory effects of GABA at the GABAA receptor/Cl– channel. Other antiepileptics block voltage-dependent Na+ channels, which can inhibit the release of the excitatory neurotransmitter glutamate, or they can act on the neurons themselves to inhibit action potentials. Other drugs block the N-methyl-d-aspartate (NMDA) glutamate receptor or T-type Ca2+ channels.
Pharmacokinetics
– Absorption slow and erratic
– Metabolized in liver; may induce hepatic enzymes
Uses
– Generalized tonic-clonic seizures
– Complex partial seizures
– Trigeminal neuralgia
Note: Carbamazepine is ineffective for absence seizures.
Side effects
– Gastrointestinal (GI) upset
– Vertigo, diplopia, and blurred vision
– Hematological disorders: aplastic anemia, thrombocytopenia (low platelet count), agranulocytosis (failure of bone marrow to produce white blood cells), and leucopenia (low white blood cell count)
– Hypersensitivity
Drug interactions
– Metabolism of carbamazepine can be increased or decreased by agents that can induce or inhibit cytochrome P-450 enzymes.
– Carbamazepine induces hepatic microsomal enzymes; it thus reduces the plasma concentration of drugs that are metabolized by these enzymes, including warfarin, oral contraceptives, and some antibiotics.
Phenobarbital
Mechanism of action. Phenobarbital is a long-acting barbiturate that potentiates and mimics gamma-aminobutyric acid (GABA; see Chapter 9). It increases the threshold for action potential firing and inhibits the spread of activity from focus (Fig. 11.1).
Pharmacokinetics
– Effective orally
– Induces hepatic enzymes
Uses
– Generalized tonic-clonic epilepsy
– Partial seizures
– Prophylaxis or treatment of febrile convulsions
Side effects
– Sedation (tolerance develops)
– Rashes are seen in 1 to 2% of patients. These may be scarlatiniform or morbilliform and are symptomatic of allergic reaction.
– Nystagmus (a rapid, involuntary, oscillatory motion of the eyeball) and ataxia (the inability to coordinate voluntary muscular movement) at excessive doses
Note: Respiratory depression is not seen with this long-acting barbiturate given orally, but it may be observed after IV injection.
Drug interactions
– Phenobarbital induces hepatic microsomal enzymes; it thus reduces the plasma concentration of drugs that are metabolized by these enzymes including warfarin, oral contraceptives, carbamazepine, and some antibiotics
– Additive effects are seen when phenobarbital is taken with other CNS depressants.
– Valproic acid increases phenobarbital blood levels by inhibiting cytochrome P-450 enzymes.
Febrile convulsions
Febrile seizures (seizures associated with elevated body temperature) are the most common type in children, affecting 2 to 5% between the ages of 6 months and 5 years, with the peak incidence at 18 months. These seizures are not associated with trauma, infection, metabolic disturbances, or a history of seizures, and most last less than 10 minutes. More serious i llnesses must be ruled out, but treatment of simple febrile seizures with anticonvulsants is generally not recommended, as the potential drug toxicities associated with these medications outweigh the relatively minor risks associated with the convulsion. There is also no need to specifically cool the child in a cooling bath or to administer an antipyretic drug, e.g., acetaminophen, to reduce the fever. Most febrile convulsions will stop on their own after a few minutes.
Primidone
Mechanism of action. Mechanism is similar to that of phenobarbital.
Pharmacokinetics. Primidone is metabolized in the liver to phenobarbital and phenylethylmalonamide (PEMA).
Uses
– Complex partial seizures (primidone is more effective than phenobarbital)
– Generalized tonic-clonic seizures and simple partial seizures
– Frequently combined with phenytoin in refractory cases
Side effects
– Rashes, leukopenia, thrombocytopenia, and systemic lupus erythematosus
– CNS depression
Drug interactions. Drug interactions are the same as for phenobarbital.
Valproic Acid
Mechanism of action. Valproic acid increases Na+ channel inactivation, increases GABA-mediated synaptic inhibition, and inhibits T-type Ca2+ channel activation (Fig. 11.1). Its anti-convulsant action continues after the drug has been withdrawn.
Pharmacokinetics
– Ninety percent bound to plasma proteins
– Metabolized by the cytochrome P-450 enzymes, but it does not induce these enzymes.
Uses
– Absence seizures, especially of the myoclonic types that are difficult to treat with other drugs. It appears to have an equivalent effect as ethosuximide for absence seizures.
– Combination therapy in the treatment of generalized tonic-clonic seizures and for complex partial seizures
Side effects
– Alopecia (reversible) in 5% of patients
– Transient GI effects in 16% of patients
– CNS: mild behavioral effects, ataxia, and tremor; not a CNS depressant
– Hepatic failure has been reported but is rare.
Note: Valproic acid should not be used in pregnancy, as it has been shown to be teratogenic in animals.
Drug interactions
– Valproic acid increases blood levels of phenobarbital and primidone by inhibiting their metabolism
– Valproic acid lowers phenytoin levels
Benzodiazepines
Mechanism of action. Benzodiazepines augment the action of GABA at GABAA receptors, which are ligand-gated chloride ion channels (Figs. 9.1 and 11.2).
Fig. 11.2 ![]() Sites of action of antiepileptics in GABAergic synapse.
Sites of action of antiepileptics in GABAergic synapse.
Many antiepileptic drugs act on GABA in a number of ways. Some drugs act presynaptically to increase the production of GABA or to reduce its degradation. Others act to inhibit the reuptake of GABA from the synaptic cleft. Progabide mimics the inhibitory effects of GABA at the GABAAreceptor, whereas benzodiazepines act on the GABAA receptor to enhance the effects of GABA.

Uses
– Chronic treatment of epilepsy (clonazepam and clorazepate)
– Status epilepticus (lorazepam or diazepam IV)
– Atonic and akinetic seizures, especially as adjuncts
– Absence seizures, but not preferred because of CNS depression
Note: Benzodiazepines do not prevent generalized tonic-clonic seizures
Side effects
– Sedation is the most common side effect.
– Ataxia
– Behavioral problems, such as aggression, anxiety, and restlessness
– Amnesia
Ethosuximide
Mechanism of action. The mechanism of action for ethosuximide is unknown, but it does enhance CNS inhibition.
Uses. Ethosuximide is effective only in absence seizures. It is the drug of choice for this condition.
Side effects
– GI irritation: nausea, vomiting, and anorexia (a lack or loss of appetite for food)
– CNS depression: drowsiness, lethargy, euphoria, dizziness, headache, and hiccups
– Rashes: urticaria (hives) and Stevens-Johnson syndrome (rare)
– Blood dyscrasias (an abnormal condition of the blood) (rare)
Gabapentin
Mechanism of action. The mechanism of action for gabapentin is unknown. Gabapentin is chemically related to GABA but is not an agonist at GABA receptors. It may enhance GABA release (Fig. 11.2).
Uses
– Treatment of partial seizures as an adjunctive to other drugs
Side effects
– Sedation, dizziness, ataxia, nystagmus, and tremor
Note: Gabapentin should be used with caution in children because it may produce adverse psychiatric symptoms, including thought disorders and hostility.
Drug interactions. This agent does not alter serum concentration of other a nticonvulsants.
Felbamate
Uses
– Partial seizures
– Lennox-Gastaut syndrome in children
Side effects
– CNS: insomnia and headache
– GI: anorexia, vomiting, and nausea
– Allergic reactions: hematological and dermatological reactions
– Acute liver failure
Drug interactions. Felbamate may alter concentrations of other anticonvulsants.
Lennox-Gastaut syndrome
Lennox-Gastaut syndrome is a disorder of childhood characterized by multiple difficult-to-treat seizure types. It is usually accompanied by some form of cognitive impairment. Antiepileptic drugs may control seizures for a time, but tolerance frequently develops.
Lamotrigine
Mechanism of action. Lamotrigine inhibits voltage-dependent Na+ channels of presynaptic membrane, which decreases the release of excitatory amino acid neurotransmitters.
Uses
– Monotherapy and adjunctive therapy for partial and secondarily generalized tonic-clonic seizures in adults
– Lennox-Gastaut syndrome in both children and adults
Side effects. Approximately 1 in 1000 people experience severe and potentially life-threatening skin rashes. These are rarely fatal, but children are at higher risk. This can be reduced by slowly increasing the dose.
Topiramate
Mechanisms of action
– Inhibits voltage-dependent Na+ channels of presynaptic membrane
– Potentiates the action of GABA by a unique mechanism, different from that of the benzodiazepines or barbiturates
– Blocks excitatory amino acid receptors
Uses
– Monotherapy in patients 10 years of age and older with partial onset or primary generalized tonic-clonic seizures
– Adjunctive therapy in partial seizures
Side effects
– Mainly involve CNS depression: fatigue, dizziness, ataxia, and decreased cognition
– Hypersensitivity
Tiagabine
Mechanism of action. Tiagabine is a GABA reuptake inhibitor (Fig. 11.2).
Uses
– Adjunctive therapy in partial seizures
Side effects
– Mainly involve CNS depression: fatigue, dizziness, ataxia, and decreased cognition
Levetiracetam
Mechanism of action. The mechanism of action for levetiracetam is unknown.
Uses
– Adjunctive therapy in partial seizures
Side effects
– Mainly involve CNS depression: fatigue, dizziness, ataxia, and decreased cognition
Zonisamide
Mechanism of action. Zonisamide prolongs Na+ channel inactivation and inhibits T-type Ca2+ current.
Uses
– Adjunctive therapy in partial seizures
Side effects
– Mainly involve CNS depression: fatigue, dizziness, ataxia, and decreased cognition
Table 11.2 summarizes the drug(s) of choice for each seizure disorder, as well as alternative drugs.
|
Table 11.2 |
||
|
Seizure Disorder |
Drug(s) of Choice |
Alternative Drugs |
|
Partial, including secondarily generalized |
Carbamazepine or phenytoin |
Lamotrigine or levetiracetam or topiramate or valproic acid |
|
Typical absence |
Ethosuximide |
Valproic Acid |
|
Atypical absence |
Valproic Acid |
Combination of valproic acid and ethosuximide or lamotrigine |
|
Myoclonic |
Valproic Acid |
Lamotrigine or topiramate |
|
Clonic or tonic |
Valproic Acid |
Phenytoin |
|
Tonic-clonic |
Carbamazepine or phenytoin or valproic acid |
Lamotrigine or topiramate |
|
Atonic/akinetic |
Valproic Acid |
Clonazepam or phenytoin |
|
Recurrent febrile |
Diazepam |
Phenobarbital |
|
Status epilepticus |
Lorazepam or diazepam, followed by phenytoin |
Phenytoin or phenobarbital |