Most testicular tumors originate in gonadal cells. About 40% are seminomas—uniform, undifferentiated cells resembling primitive gonadal cells. The remainder are nonseminomas—tumor cells showing various degrees of differentiation. The prognosis varies with the cell type and disease stage. When treated with surgery and radiation, almost all patients with localized disease survive beyond 5 years.
![]() Age Alert
Age Alert
Malignant testicular tumors primarily affect young to middle-aged men and are the most common solid tumor in these age-groups. Incidence peaks between ages 20 and 40. Testicular tumors seldom occur in children.
Testicular cancer is rare in nonwhite males and accounts for fewer than 1% of male cancer deaths.
Causes
Primary cause unknown
Associated conditions
· Cryptorchidism (even if surgically corrected)
· Maternal use of diethylstilbestrol during pregnancy
Pathophysiology
Testicular cancer may metastasize to the lungs, liver, viscera, or bone. It spreads through the lymphatic system to the iliac, para-aortic, and mediastinal lymph nodes.
Signs and symptoms
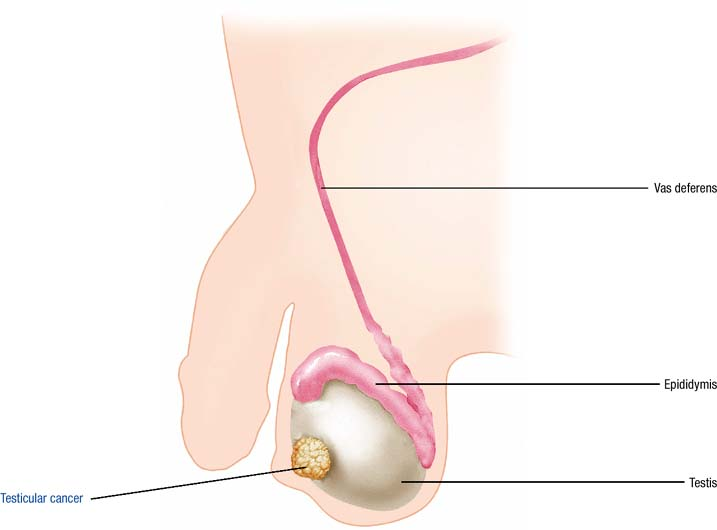
· Firm, painless, smooth testicular mass, varying in size and sometimes producing a sense of testicular heaviness
· Gynecomastia and nipple tenderness may result if tumor produces chorionic gonadotropin or estrogen may result
· Dull ache in the lower abdomen or back
· Lump or swelling in either testicle
In advanced stages
· Ureteral obstruction
· Abdominal mass
· Cough, hemoptysis, shortness of breath
· Weight loss
· Fatigue, pallor, lethargy
Diagnostic test results
· Scrotal ultrasound confirms the presence of a solid mass.
· Laboratory studies show elevated human corticotropin, human chorionic gonadotropin (HCG), and alfa fetoprotein (AFP) (nonseminoma) or elevated HCG and normal AFP (seminoma).
· Tissue biopsy confirms the diagnosis and stages the disease.
Treatment
Surgery
· Orchiectomy and retroperitoneal node dissection
· Hormone replacement therapy after bilateral orchiectomy
Postoperative radiation
· Seminoma—retroperitoneal and homolateral iliac nodes
· Nonseminoma—all positive nodes
· Retroperitoneal extension—mediastinal and supraclavicular nodes prophylactically
Combination chemotherapy
· Essential for tumors beyond stage 0
· Agents include bleomycin, etoposide, and cisplatin; cisplatin, vindesine, and bleomycin; cisplatin, vinblastine, and bleomycin; cisplatin, vincristine, methotrexate, bleomycin, and leucovorin
Unresponsive malignancy
· Chemotherapy and radiation
· Autologous bone marrow transplantation
P.341
TESTICULAR CANCER
|
|
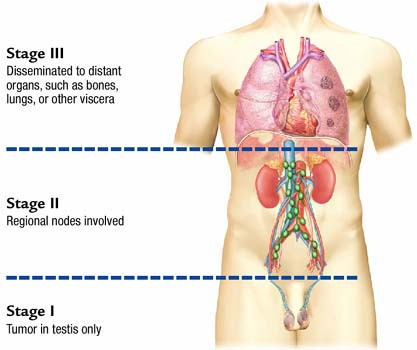
![]() Clinical Tip: Staging Testicular Cancer
Clinical Tip: Staging Testicular Cancer
|
The extent of metastasis determines the stage of testicular cancer. |
|