I will use treatment to help the sick according to my ability and judgment, but never with a view to injury and wrongdoing. And whatsoever I shall see or hear in the course of my profession in my discourse with others, ... I will never divulge, holding such things to be holy secrets.
From The Physician's Oath, Hippocrates (460-377) bce
Ethical Challenges
Since the mid-1960s, there has been an increased awareness of and interest in medical ethics. With the first human heart transplant operation by Dr. Christiaan Barnard in 1967, the U.S. Supreme Court's declaration in 1973 that state laws prohibiting abortion were unconstitutional, and the controversy in 1975 over removing the respirator from a patient with irreversible brain damage in the case of Karen Ann Quinlan, modern medical ethics was born. Touching on three key issues—organ transplantation, abortion, and the standards of death—these landmarks set the stage for current thoughts about the ethical dimensions of health care.
Since then, there have been many other ethical challenges to the health-care system. In 1978, the first baby to be conceived in a test tube, Louise Brown, was born. In 1982, Dr. Barney Clark was the first person to receive a mechanical artificial heart, the Jarvik-7. In 1984, the infant Baby Fae received a heart transplanted from a baboon. In 1988, the Baby M case involved the ethical issues of Mary Beth Whitehead's ''surrogate motherhood'' for William Stern. From 2003 to 2005, legal and political conflict raged around the maintenance of life support (tube feedings) for Terri Schiavo, a severely brain-damaged woman who had been kept alive for 15 years.
As clinicians in the 21st century, you will be faced with many ethical issues: standards of brain death, physician-assisted suicide, in vitro fertilization, autonomy, informed consent, ''do-not-resuscitate'' orders, surrogate motherhood, euthanasia versus letting-die issues, rights of disabled persons, confidentiality, coerced surgery, abortion, ''Baby Doe'' regulations, interracial transplantation, surrogacy arrangements, allocation of scarce medical resources, whistle-blowing on unethical colleagues, use of patients as research subjects, mandatory* testing for acquired immunodeficiency syndrome (AIDS), and genetic manipulation. One of the first ethical issues you may face is the use of patients as ''teaching tools.''
*This Epilogue was written in collaboration with Talia H. Swartz, MD, PhD, Department of Internal Medicine, Mount Sinai Medical Center, New York, New York.
A current ethical issue is the mandatory testing for human immunodeficiency virus (HIV). Should an HIV test be required as part of premarital testing, preadmission to hospitals, preinsurance examinations, or preemployment testing? Several arguments have been made in its favor, including a person's right to donate blood, the tracing of potential infected contacts, determination of the incidence and rate of spread of HIV, quarantine of infected persons, and tattooing of infected persons. Some of the arguments against mandatory testing concern discrimination, ''social purification,'' violation of a person's privacy, false-positive test results, and health insurance difficulties.
An ethical problem is one in which two or more norms or principles create a challenge about what to do. There are many types of ethical problems. These problems can be divided into four main groups:
1. Ethical distress: An individual knows the course of action, but a barrier prevents its accomplishment.
2. Ethical dilemma: There exist two or more courses of action, each of which is right or wrong, and selecting one will compromise the end result.
3. Distributive justice: Benefits are given to several individuals, but not to everyone. On what basis should the distribution be made?
4. Locus of authority: There are two or more authorities, all believing that they know which outcome will best benefit the patient, but only one will prevail.
Consider the following examples of contemporary issues in medical ethics:
• Avia and Hal are newlyweds. They want to have children, but each is from a family with a known inherited illness. Any or all of their children may be affected. Genetic alteration may be an option. Is it right for such couples to endeavor to change their future children's genetic makeup? Is modification of natural biology a human right?
• Florence is 31 years of age. When Florence became pregnant, she was overjoyed. She is now in her second month of pregnancy. Recently she developed fever, tender lym- phadenopathy, rash, and sore throat. Rubella was diagnosed. Although Florence dreads the thought of giving birth to a retarded, blind, or congenitally malformed child, her religion does not allow abortion. Nonetheless, she questions whether it is right to bear a child that she knows will live a life of suffering.
• Baby John is born with significant birth defects. As his condition continues to deteriorate, is there a point when aggressive therapy should be discontinued?
• Natalie and Marshall have been unsuccessful in conceiving a child, and evaluation indicates that Natalie is unable to bear a child. The couple decides on a surrogate pregnancy with Marshall's sperm. They meet the surrogate mother, whom they like, and she conceives their child. During a conversation in her second trimester, the surrogate mother-to-be indicates that she would be unwilling to undergo a cesarean section if the child's life were in jeopardy. Who has the right to make that decision?
• Sam, a major benefactor to the hospital, is 76 years of age. He has Parkinson's disease and diabetes mellitus. Sam is in the emergency department complaining of severe chest pain. Brittany is a 41-year-old nurse with a history of angina who is also in the emergency department complaining of severe chest pain. There is only one bed left in the coronary intensive care unit. Who should get the bed?
• Jack is a 42-year-old man who has sex with only men and is HIV-positive. Although counseled about his promiscuous sexual behavior, he is unwilling to curb his unprotected sexual encounters, posing a threat to his partners and to the community at large. What is your role as his physician as it relates to confidentiality and the ''politics'' of disease?
• Maria is 20 years of age and is the single mother of two children. She is in the first trimester of her third pregnancy. Recent symptoms of severe weakness and gingival bleeding brought her to medical attention. A work-up revealed acute monomyelocytic leukemia and anemia with a hemoglobin measurement of 7.8 g/dL. Therapy for the leukemia would be a great risk to the life of the fetus, but the patient refuses to terminate her pregnancy. To complicate the issue, her fiance, a Jehovah's Witness, has persuaded the patient to refuse any transfusion of blood or blood products. How do you, as her physician, handle this situation?
• Lynn is a 62-year-old woman with a 2-year history of lung cancer. Because of severe back pain for the past 3 months, she is evaluated, and it is determined that she has
multiple metastases to her spine impinging on nerve roots. Despite analgesic therapy, she continues to have debilitating, unrelenting pain. She now consults you, requesting physician-assisted suicide.
Unethical Labeling of Patients
One of the significant problems currently seen in health care is the unethical labeling of patients. Terms such as ''gomer'' (''get out of my emergency room''), ''albatross, turkey,'' and ''slug'' are examples of disrespect. Health-care providers who use such terms are often reacting negatively to certain social and personal traits of their patients, as well as to certain medical conditions. This is particularly evident with illnesses that are usually incurable, are self-inflicted, or that challenge the health-care provider's faith in the ''science'' of medicine. Often, these patients have illnesses that defy medical intervention, thus frustrating the healthcare provider. A patient who is of low socioeconomic class, has an illness engendering fear or disgust, is uncooperative, or is psychologically dysfunctional is at the greatest risk of being labeled in this derogatory manner.
Health-care providers may use these negative terms as ''safety valves'' for the emotionally charged environment in which they work, but this only further distances them from their patients. Each provider must recognize and come to grips with his or her anxieties about dealing with illness and treating patients and must not allow these destructive attitudes to interfere with the care of the sick. Remember the quotation from Francis Weld Peabody that introduces this book: ''the secret in the care of the patient is in caring for the patient.''
Health-Care Proxy
A health-care proxy form is an extremely important document that every patient should have in order to serve as protection of his or her wishes at a time when he or she might be incapacitated. A health-care proxy is a person who is appointed to make decisions on behalf of the patient if the patient is unable to do so. This health-care proxy is anyone whom the patient designates as someone he or she trusts: for example, a family member or close friend. Once this health-care proxy is designated, that person is authorized to make health-care decisions for the patient should the patient lose the ability to make decisions for himself or herself. It is not necessary to have a lawyer fill out this health-care proxy form; it is a form that can be completed by the patient with understanding on the part of the health-care proxy of this designation and the signatures of two witnesses. This becomes hospital record and can be used in the future as necessary. Any adult, 18 years of age or older, may be the health-care proxy. It is important that once the proxy is designated, the patient discuss wishes about advanced directives if such a situation should arise: the desire to be maintained on artificial nutrition, mechanical ventilation, renal replacement, or organ/tissue donation. Knowledge of the patient's viewpoints of these measures will help improve the ability of the health-care proxy to make decisions that best reflect the patient's wishes. The patient may even give the healthcare proxy specific instructions to follow, and this may be documented in the health-care proxy form, but this is not required.
Even though the patient has signed this health-care proxy form, he or she still has the right to make health-care decisions for himself or herself as long as he or she is able to do so. Treatment cannot be given to the patient or stopped if the patient objects, and the proxy has no power to object. The patient may also cancel the authority given to the health-care proxy by telling him or her orally or in writing.
Appointing a health-care proxy is voluntary. No one can require a patient to appoint one. Copies of the health-care proxy form should be given to the proxy, the physician, family members, an attorney, and close friends. A copy should also be kept in the patient's wallet. If the patient is hospitalized, the form should be brought in and included in the medical record.
It is important to understand the difference between a living will and a health-care proxy form. A living will is a document that provides specific instructions about health-care decisions. A patient may put such instructions on his or her health-care proxy form. Unlike a living will, a health-care proxy form does not require that a patient knows in advance all the decisions that may arise. Instead, the health-care proxy can interpret a patient's wishes as medical circumstances change and can make decisions that a patient could not have known would have to be made.
Adapted from the New York State Health Proxy Form.
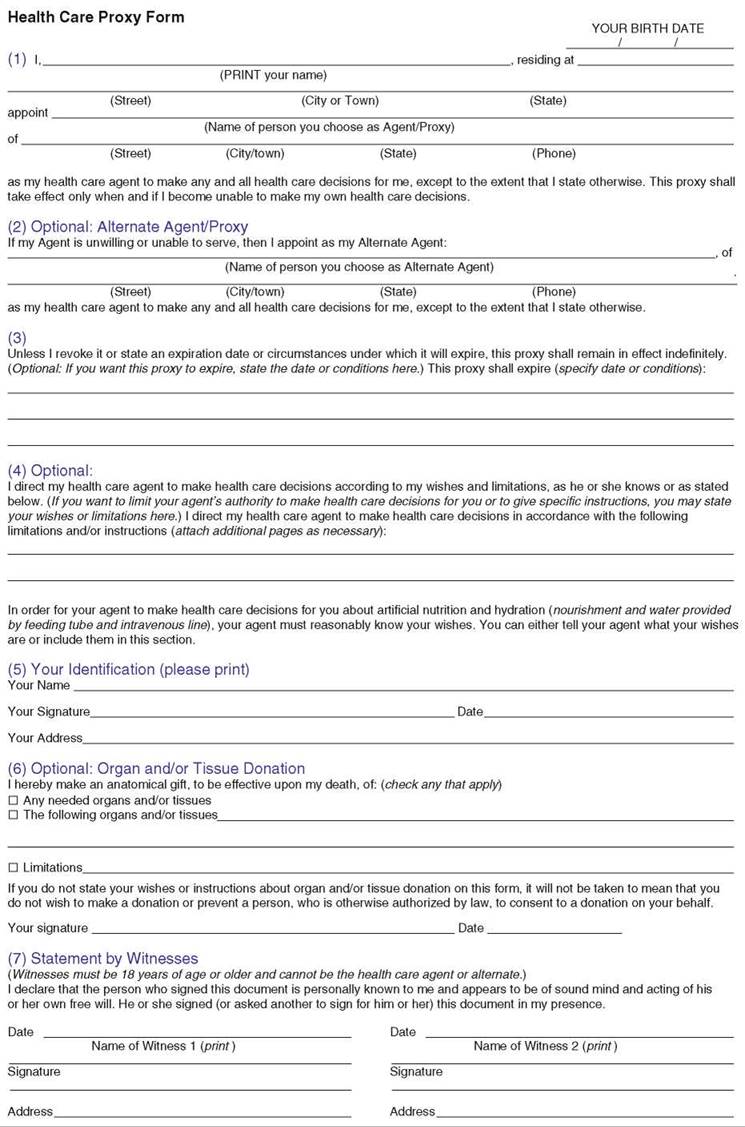
The structure of the health-care proxy form may differ from state to state, but the common elements all include the following:
• Name and address of the agent/proxy
• Name and address of an alternative agent
• Duration of the proxy (not indicating a duration means it is valid unless stated otherwise)
• Special instructions: these can broaden or limit the powers of the agent. If the patient does not want to be sustained by feeding tubes no matter what, this can be stated here. If there are certain treatments that the patient does not want to receive, such as blood transfusion, then they must be indicated. However, if the patient wants to give the agent more flexibility with some or no restriction, this too must be written.
• Name, date, and signature of the primary individual
• Instructions about tissue or organ donation
• Signatures of two adult witnesses, stating that they have witnessed this agreement and that both parties appear to be competent. The witnesses must be 18 years of age or older. The agent and primary individual do not qualify as witnesses.
A copy of a sample proxy form is shown on the previous page. You should copy this form and give it to all your patients if they have not already designated a health-care proxy.
Health-care proxy forms have become increasingly important today as a result of conflicts among relatives of the primary individual. The Terri Schiavo case is a famous modern-day example that lasted for 15 years of court battles (1990-2005). The patient was an American woman who suffered brain damage and became dependent for survival on a feeding tube. Her husband wanted to remove her feeding tube, but her parents opposed this action. This resulted in lengthy court battles that raised many moral, political, and medical issues. The whole controversy may have been avoided had the patient designated either her parents or her husband as her health-care proxy. Without a health-care proxy, a surrogate that follows next of kin becomes designated; however, the decision-making capacity of a surrogate is much more limited and varies by state. Therefore, if any individual can designate a health-care proxy while he or she is in good health, much agonizing and conflict can be avoided if a situation warrants this need in the future.
The reader should review the DVD-ROM included with this book for an example of discussing a health-care proxy with a patient.
Concluding Thoughts
As a health-care professional, you will be faced with many types of problems that involve complex decision-making. Always treat your patients and colleagues with fairness, respect, and dignity. Your medical training may be harsh at times; however it is important to maintain the enthusiasm that sparked your desire to join this profession. I wish you the best of luck in dedicating your career to caring for your patients.
Bibliography
Freeman JM, McDonnell K: Tough Decisions: Cases in Medical Ethics, 2nd ed. New York, Oxford University Press, 2001.
Glannon W: Biomedical Ethics. New York, Oxford University Press, 2004.
Jonsen AR, Siegler M, Winslade WJ: Clinical Ethics: A Practical Approach to Ethical Decisions in Clinical Medicine. New York, McGraw-Hill Medical, 2002.
Kurland G: My Own Medicine: A Doctor's Life as a Patient, New York, Henry Holt & Company, 2002. Lynne D: Terri's Story: The Court-Ordered Death of an American Woman. Nashville, Tenn, Cumberland House, 2005.
Pellegrino ED, Thomasma DC: The Virtues in Medical Practice. New York, Oxford University Press, 1993. Pence GE: Classic Cases in Medical Ethics: Accounts of the Cases That Have Shaped Medical Ethics, with Philosophical, Legal, and Historical Backgrounds, 4th ed. New York, McGraw-Hill, 2003.
Petrinovich L: Living and Dying Well. New York, Plenum Press, 1996.
Rosner F: Modern Medicine and Jewish Ethics, 2nd ed. New York, Yeshiva University Press, 1991. Weisman J: As I Live and Breathe: Notes of a Patient-Doctor. New York, Farrar, Straus and Giroux, 2003.