Although not exclusive to obstetric anaesthesia, a sound knowledge of the anatomy pertinent to epidural and spinal anaesthesia is fundamental to obstetric anaesthetists. In addition, knowledge of the relevant peripheral nerves is important in order to differentiate central from peripheral causes of neurological impairment.
The structures involved in obstetric neuraxial anaesthesia comprise the vertebrae and sacral canal, vertebral ligaments, epidural space, meninges and spinal cord. The important peripheral aspects are the lumbar and sacral plexuses and the muscular and cutaneous supply of the lower part of the body.
Vertebrae (Figure 10.1)
The vertebral column has two curves, with the cervical and lumbar regions convex anteriorly and the thoracic and sacral regions concave. Traditionally, T4 is described as the most posterior part (most dependent in the supine position), although T8 has been suggested by recent imaging studies. L3-4 is the most anterior part (uppermost in the supine position), although this curve may be flattened by flexing the hips. In the lateral position, the greater width of women’s hips compared with their shoulders imparts a downward slope from the caudal end of the vertebral column to the cranial end.
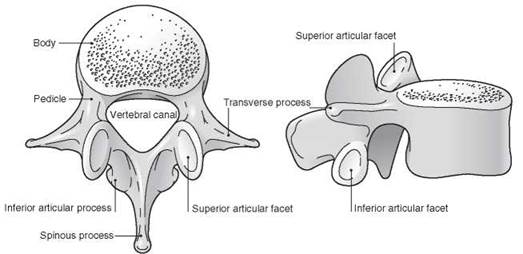
Figure 10.1 A lumbar vertebra, seen from superior and lateral aspects. Reproduced with permission from Yentis SM, Hirsch NP, Smith GB. Anaesthesia and Intensive Care A-Z, 4th edn. Churchill Livingstone. © Elsevier 2009.
There are seven cervical vertebrae, twelve thoracic, five lumbar, five fused sacral and three to five fused coccygeal. A number of ligaments connect them (see below). Vertebrae have the following components:
• Body. This lies anteriorly, with the vertebral arch behind. It is kidney-shaped in the lumbar region. Fibrocartilaginous vertebral discs, accounting for about 25% of the spine’s total length, separate the bodies of C2 to L5. Each disc has an outer fibrous annulus fibrosus and a more fluid inner nucleus pulposus (the latter may prolapse through the former: a ‘slipped disc’). The bodies of the thoracic vertebrae are heart-shaped and articulate with the ribs via superior and inferior costal facets at their rear. The bodies of the sacral vertebrae are fused to form the sacrum, which encloses the sacral canal; the coccygeal vertebral bodies are fused to form the triangular coccyx, the base of which articulates with the sacrum.
• Pedicles. These are round in cross-section. They project posteriorly from the body and join the laminae. Each intervertebral foramen is formed by the pedicles of the vertebra above and below.
• Laminae. These are flattened in cross-section. They complete the vertebral arch by meeting in the midline at the spinous process. The superior and inferior articular processes bear facets for articulation with adjacent vertebrae; those of the thoracic vertebrae are flatter and aligned in the coronal plane, whereas those of the lumbar vertebrae are nearer the sagittal plane.
• Transverse processes. In the lumbar region these are thick and pass laterally.
The transverse processes of L5 are particularly massive but short. The transverse processes of thoracic vertebrae are large and pass backwards and laterally; they bear facets that articulate with the tubercles of the ribs (except T11 and T12).
• Spinous process. These project horizontally backwards in the lumbar region; in the thoracic region they are longer and inclined at about 60 degrees to the horizontal. The spinous process of T12 has a notched lower edge.
The cervical vertebrae have a number of features that distinguish them from the others, including the foramen transverarium in the transverse processes, bifid spinous processes and the particular characteristics of C1 and C2.
A line drawn between the iliac crests (Tuffier’s line) usually crosses the L3-4 interspace (slightly higher than in the non-pregnant state because of rotation of the pelvis), although this is unreliable, and it has been shown that even experienced anaesthetists can be one or more interspaces lower (or more commonly, higher) than that intended.
Sacral canal (Figure 10.2)
The sacral canal is 10-15 cm long, triangular in cross-section, runs the length of the sacrum and is continuous cranially with the lumbar vertebral canal. The fused bodies of the sacral vertebrae form the anterior wall, and the fused sacral laminae form the posterior wall. The sacral hiatus is a deficiency in the fifth laminar arch, has the cornua laterally and is covered by the sacrococcygeal membrane. Congenital variants are common, possibly contributing to unreliable caudal analgesia.
Vertebral ligaments (Figure 10.3)
• Anterior longitudinal ligament. This is attached to the anterior aspects of the vertebral bodies, and runs from C2 to the sacrum.

Figure 10.2 Sacrum, posterior aspect. Reproduced with permission from Yentis SM, Hirsch NP, Smith GB. Anaesthesia and Intensive Care A-Z, 4th edn. ChurchillLivingstone. © Elsevier 2009.
• Posterior longitudinal ligament. This is attached to the posterior aspects of the vertebral bodies, and runs from C2 to the sacrum.
• Ligamentum flavum (yellow ligament). This is attached to the laminae of adjacent vertebrae, forming a V-shaped structure with the point posteriorly. It is more developed in the lumbar than in the thoracic region.
• Interspinous ligament. This passes between the spinous processes of adjacent vertebrae.
• Supraspinous ligament. This is attached to the tips of the spinous processes from C7 to the sacrum.
In addition, there are posterior, anterior and lateral sacrococcygeal ligaments. Other ligaments are involved in the attachments of C1 and C2 to the skull. The ligaments may become softer during pregnancy because of the hormonal changes that occur.
Epidural space
• Boundaries. The space extends from the foramen magnum to the sacrococcygeal membrane. It is triangular in cross-section in the lumbar region, its base anterior; it is very thin anteriorly and up to 5 mm wide posteriorly. It lies external to the dura mater of the spinal cord and internal to the ligamenta flava and vertebral laminae posteriorly, the posterior longitudinal ligament anteriorly and the intervertebral foramina and vertebral pedicles laterally. Magnetic resonance imaging suggests the space is divided into segments by the laminae. The space may extend through the intervertebral foramina into the paravertebral spaces.
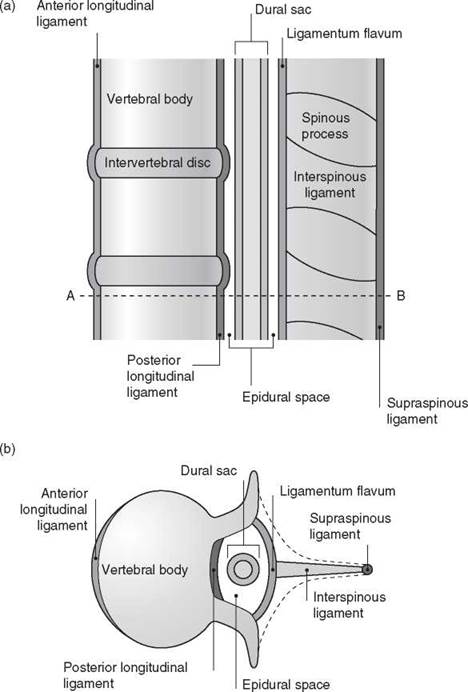
Figure 10.3 Vertebralligaments: (a) longitudinal section and (b) transverse section through A-B. Reproduced with permission from Yentis SM, Hirsch NP, Smith GB. Anaesthesia and Intensive Care A-Z, 4th edn. ChurchillLivingstone. © Elsevier 2009.
• Contents. These include epidural fat, epidural veins (Batson’s plexus), lymphatics and spinal nerve roots. The veins become engorged in pregnancy as a result of the hormonal changes and any aortocaval compression. Connective tissue layers have been demonstrated by radiology and endoscopy within the epidural space, in some cases dividing it into right and left portions.
• Pressure. A negative pressure is usually found in the epidural space upon entering it; the reason is unclear but may involve anterior dimpling of the dura by the epidural needle, sudden posterior recoil of the ligamentum flavum when it is punctured, stretching of the dural sac during extreme flexion of the back, transmitted negative intrapleural pressure via thoracic paravertebral spaces and/or relative overgrowth of the vertebral canal compared with the dural sac. Occasionally a positive pressure is found.
Meninges
• Pia mater. This delicate and vascular layer adheres closely to the brain and spinal cord. Between it and the arachnoid mater is the cerebrospinal fluid (CSF) within the subarachnoid space containing blood vessels, the denticulate ligament laterally along its length and the subarachnoid septum posteriorly. The pia terminates as the filum terminale, which passes through the caudal end of the dural sac and attaches to the coccyx.
• Arachnoid mater. This membrane is also delicate and lies between the dura externally and the CSF internally. The potential subdural space lies between the dura and arachnoid mater, which fuses with the dura at S2.
• Dura mater. This fibrous layer has an outer component that is adherent to the inner periosteum of the vertebrae, and an inner one that lies against the outer surface of the arachnoid. The dura projects into the epidural space, especially in the midline. It ends at about S2.
Spinal cord
The spinal cord ends inferiorly level with L3 at birth, rising to the adult level of L1-2 (sometimes T12 or L3) by 20 years. Below this level (the conus medullaris), the lumbar and sacral nerve roots (comprising the cauda equina) and filum terminale occupy the vertebral canal. The main ascending and descending tracts are shown in Figure 10.4.
The blood supply of the spinal cord is of relevance to obstetric anaesthetists, since cord ischaemia may result in neurological damage:
• Anterior spinal artery. This descends in the anterior median fissure and supplies the anterior two-thirds of the cord. The anterior spinal artery syndrome (e.g. arising from profound hypotension) thus results in lower motor neurone paralysis at the level of the lesion, and spastic paraplegia, reduced pain and temperature sensation below the level, with normal joint position sense and vibration sensation.
• Posterior spinal arteries. These descend along each side of the cord, one anterior and one posterior to the dorsal nerve roots.
• Radicular branches. These arise from local arteries (from the aorta) and feed the spinal arteries. Those at T1 and the lower thoracic/upper lumbar level (artery of Adamkiewicz - usually unilateral) are the most important. The cord at T3-5 and T12-L1 is thought to be most at risk from ischaemia. The conus medularis and cauda equina are supplied by a vascular plexus arising from the artery of Adamkiewicz above and pelvic vessels below. In 15% of the population, the artery of Adamkiewicz is the main source of arterial blood to the conus medullaris and cauda equina; compression during delivery may result in permanent paraplegia.
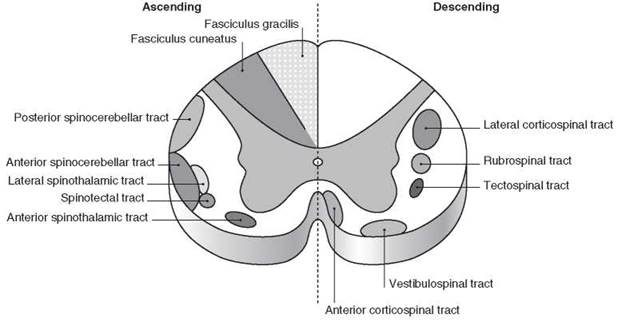
Figure 10.4 Ascending and descending tracts of the spinalcord. Reproduced with permission from Yentis SM, Hirsch NP, Smith GB. Anaesthesia and Intensive Care A-Z, 4th edn. ChurchillLivingstone. © Elsevier 2009.
Venous drainage is via the internal iliac, intercostal, azygos and vertebral veins.
Peripheral nerves of the lower body
The lumbar and sacral plexuses are shown schematically in Figure 10.5. They form at the posterior of the pelvis, and their branches pass round the interior of the pelvis, where they may be exposed to pressure during labour and delivery (Figure 10.6; see also Chapter 53, Peripheral nerve lesions following regional anaesthesia).
Peripheral cutaneous innervation may be characterised according to the dermatomal distribution or peripheral nerves (Figures 10.5 and 10.7, Table 53.1). Both representations may vary considerably between individuals. Peripheral motor innervation may also be considered according to myotomal innervation or peripheral nerves (Table 10.1).
Dermatomal innervation of the upper body is also important when determining the upper extent of regional blockade.
Key points
• A clear understanding of the anatomy of the spine and peripheral nerves is essential when delivering neuraxial anaesthesia and analgesia, and when assessing neurological complications related to delivery.
Further reading
Richardson J, Groen G. Applied epidural anatomy. Contin Educ Anaesth Crit Care Pain 2005; 5: 98-100.
Westbrook JL. Anatomy of the epidural space. Anaesth Intensive Care Med 2012; 13: 551-4.
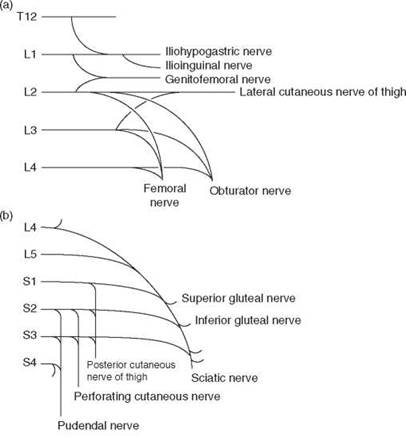
Figure 10.5 Plan of (a) lumbar plexus and (b) sacralplexus.
Reproduced with permission from Yentis SM, Hirsch NP, Smith GB. Anaesthesia and Intensive Care A-Z,4th edn. Churchill
Livingstone. © Elsevier 2009.
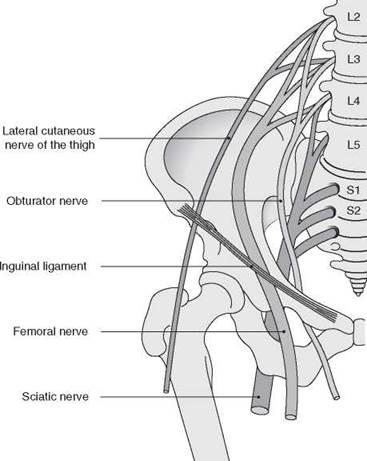
Figure 10.6 Relationship of peripheral nerves with the pelvis. Adapted with permission from Holdcroft A, Thomas TA. Principles and Practice of Obstetric Anaesthesia.
BlackwellScience Ltd. © John Wiley & Sons Ltd 1999.
Table 10.1 Motor innervation of lower limbs by myotomes and peripheral nerves
|
Joint |
Movement |
Myotomes |
Nerve supply |
|
Hip |
Flexion |
L1-3 |
Lumbar plexus |
|
L2-4 |
Femoral nerve |
||
|
Extension |
L5-S2 |
Sacral plexus |
|
|
L5-S2 |
Sciatic nerve |
||
|
Abduction |
L5-S2 |
Sacral plexus |
|
|
Adduction |
L2-4 |
Obturator nerve |
|
|
Knee |
Extension |
L2-4 |
Femoral nerve |
|
Flexion |
L5-S2 |
Sciatic nerve |
|
|
S1-2 |
Tibial nervea |
||
|
Ankle/foot |
Dorsiflexion |
L4-5 |
Deep peroneal nerveb |
|
Eversion |
L5-S1 |
Superficial peroneal nerveb |
|
|
Plantar flexion |
S1-2 |
Tibial nervea |
|
|
Inversion |
L4-5 |
Tibial nervea |
a Branch of sciatic nerve.
b Branch of common peronealnerve, itself a branch of the sciatic nerve.

Figure 10.7 Dermatomes of upper and lower body. Reproduced with permission from Yentis SM, Hirsch NP, Smith GB. Anaesthesia and Intensive Care A-Z, 4th edn. ChurchillLivingstone. © Elsevier 2009.