Acute infections of the nervous system may occur at any time during pregnancy or the peripartum period. The most important infection for the anaesthetist to consider is meningitis, as this can (rarely) occur as a sequel to spinal anaesthesia and confuse the differential diagnosis of a postdural puncture headache.
Women may also present having previously had meningitis.
Problems and special considerations
Meningitis may be:
• Infective, caused by bacteria, viruses and, rarely, as a complication of other diseases such as tuberculosis or fungal infections
• Aseptic, caused by topical chemical agents (e.g. disinfectants) and, rarely, systemic drugs, e.g. H2-blockers, non-steroidal anti-inflammatory drugs and antibiotics
Meningitis that occurs as a complication of regional anaesthesia may be either of the above, and in each case prevention is better than cure. Meticulous attention to aseptic technique is an essential part of minimising the risk of infection or chemical contamination at the time of performing the regional block.
The classic signs of meningitis are headache, neck stiffness, photophobia, vomiting, fever and raised white cell count. Many of these symptoms are also produced by an accidental dural puncture, and so the exclusion of meningitis is essential in the differential diagnosis of any headache that develops after a regional anaesthetic.
Almost all women with a history of previous meningitis have had a diagnostic lumbar puncture, which may have been a frightening experience, leading to apprehension of any further similar procedures. Some may have residual neurological impairment, although this is uncommon with modern management.
Management options
Preventive measures include full aseptic precautions (including the use of a facemask to prevent droplet spread) during the performance of neuraxial techniques, and bacterial filters must be used with epidural catheters. Disconnected epidural systems may carry an increased risk of contamination, and obstetric units should have local guidance on their management. If within 15-30 minutes of witnessed disconnection, this may include wiping the epidural catheter with alcohol, letting it dry and cutting the catheter with a sterile blade, 5-10 cm proximal to the fluid meniscus, before reconnecting. Some may advocate re-siting of the catheter; however, the risk of repeated instrumentation of the epidural space, particularly in obese women or those in whom the initial placement was technically difficult, must be weighed against that of introducing infection into the neuraxis.
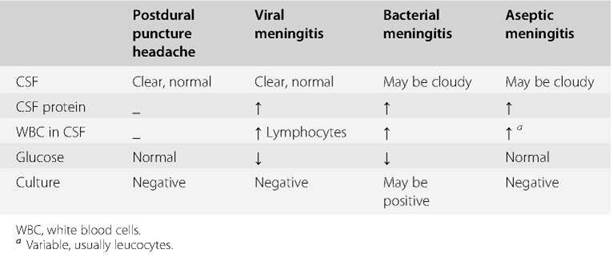
Table 119.1 Typicalcerebrospinalfluid (CSF) findings in postdural puncture headache and meningitis
The performance of regional anaesthesia in women in labour with features of bacter- aemia is controversial, and the decision should be based on an individual risk-benefit assessment (see Chapter 144, Pyrexia during labour).
Meningitis should be considered as a possible diagnosis in any patient who has a raised temperature or white cell count associated with a headache. Differentiation between meningitis and accidental dural puncture as the cause of the headache may be difficult. When there is any doubt, a neurological consultation is essential, and where appropriate a diagnostic lumbar puncture should be performed (Table 119.1). Antibiotics are usually prescribed empirically while awaiting the results of microbiological investigation.
Ideally, women with a previous history of meningitis should be seen antenatally by the obstetric anaesthetist for assessment and reassurance. In general, most women can be reassured that they are not at extra risk from regional analgesia and anaesthesia.
Key points
• Meningitis is the most important acute neurological infection in obstetrics.
• Meningitis should always be considered in a woman with severe postpartum headache.
• Adherence to aseptic technique during the performance of regional anaesthesia is essential, to minimise the risk of introducing contaminants into the neuraxial space.
Further reading
American Society of Anesthesiologists, American Society of Regional Anaesthesia and Pain Medicine. Practice advisory for the prevention, diagnosis, and management of infection complications associated with neuraxial techniques: an updated report by the American Society of Anesthesiologists Task Force on infectious complications associated with neuraxial techniques and the American Society of Regional Anaesthesia and Pain Medicine.
Anesthesiology 2017; 126: 585-601.
Association of Anaesthetists of Great Britain and Ireland, Obstetric Anaesthetists’ Association, Regional Anaesthesia UK, Association of Paediatric Anaesthetists of Great Britain and Ireland. Safety guideline: skin antisepsis for central neuraxial blockade. Anaesthesia 2014; 69: 1279-86.
Horlocker TT, Wedel DJ. Infectious complications of regional anesthesia. Best Pract Res Clin Anaesthesiol 2008; 22: 451-75.
McGill F, Heyderman RS, Michael BD, et al. The UK joint specialist societies guideline on the diagnosis and management of acute meningitis and meningococcal sepsis in immunocompetent adults. J Infect 2016; 72: 405-38.