Bengt Källén1
(1)
Tornblad Institute, Lund University, Lund, Sweden
Most interest has been paid to the risk of congenital malformations (see Chap. 6). Maternal use of drugs during pregnancy may, however, affect pregnancy outcome in many ways. We will discuss the most important such outcomes and methods to identify them in epidemiological studies.
5.1 Maternal Pregnancy Complications
Such complications are usually identified from medical records or – if available – from medical birth registers and are usually defined by International Classification of Diseases (ICD) codes. Interview or questionnaire data are less reliable and may be biased.
5.1.1 Preeclampsia
Mild to severe preeclampsia is registered in about 4 % of all pregnancies in the Swedish Medical Birth Register. Among women who had used antidepressants in early pregnancy, 5.4 % had preeclampsia and among women who did not use antidepressants, 3.9 % did – a crude odds ratio is 1.40 (95 % CI 1.32–1.50). There are many factors which can influence both the use of antidepressants in early pregnancy and preeclampsia later in pregnancy. With increasing maternal age, antidepressant use increases and so does the risk for preeclampsia. The use of antidepressants and also the preeclampsia risk decreases with parity. The same trend of an increase with maternal prepregnancy BMI is seen for both phenomena. Maternal smoking is associated with the use of antidepressants but has a protective effect on the development of preeclampsia. After adjustment for these factors and year of delivery, the odds ratio for preeclampsia in women who had used antidepressants in early pregnancy was 1.26 (95 % CI 1.12–1.34), and these factors thus only explained one-third of the crude risk. A strong risk factor for preeclampsia is chronic hypertension which is evident from the odds ratio for preeclampsia when the woman used antihypertensives in early pregnancy (4.22, 95 % CI 3.86–4.21). An existing association between chronic hypertension and use of antidepressants could explain the effect of the latter, but exclusion of women who had used antihypertensives changed the odds ratio only little (1.24, 95 % CI 1.18–1.33). The link between the use of antidepressants and preeclampsia seems not to be due to chronic hypertension. If the effect is caused by the drugs, the underlying disease or some common factor is not clear. Palmsten et al. (2013) claimed that untreated depression during pregnancy was associated with an increased risk for preeclampsia which was further increased if antidepressant drugs (notably TCA or SNRI) had been used.
Preeclampsia is a serious pregnancy complication which often results in preterm birth and increases the risk for post-pregnancy hypertension, cardiovascular disease, and chronic kidney disease (Vest and Cho 2014). It can also develop into eclampsia even if this is relatively rare in developed countries or into the life-threatening HELLP syndrome.
5.1.2 Placenta Previa
Placenta previa is a less common complication than preeclampsia and is due to an abnormally low implantation of the embryo so the placenta will lie below the fetus in the uterus. In the Swedish Medical Birth Register, this diagnosis was given to 0.3 % of all women who did not use antidepressants and 0.5 % of all women who used antidepressants. The crude odds ratio for placenta previa after maternal use of antidepressants is 1.42 (95 % CI 1.15–1.76). The risk of placenta previa increases with maternal age or maternal smoking but is not much influenced by parity or BMI. Adjustment for year of delivery, maternal age, parity, smoking, and BMI changes the odds ratio only little: 1.46 (95 % CI 1.17–1.81). The condition usually results in a cesarean section (96 % of the diagnosed cases in the Swedish Medical Birth Register).
5.1.3 Placenta Abruption
This condition means that the placenta is detached, partially or completely, before the baby has been born. It results in major bleeding and threatens the life of the baby. In the Swedish Medical Birth Register, this complication was registered in 0.3 % among women who did not use antidepressants and 0.4 % in women who used such drugs. The crude odds ratio was 1.22 (95 % CI 0.97–1.54), thus not statistically significant. Also the risk of this complication increases with maternal age, is higher at first parity than at second to third parity, increases with smoking, and is increased at low BMI. After adjustment for these factors, the odds ratio decreased to 1.04 (95 % CI 0.80–1.35), so the suggested effect seemed mainly to be due to maternal characteristics (Reis and Källén 2010).
5.1.4 Other Pregnancy Complications
Among other pregnancy complications which may be related to drug use during pregnancy (or underlying disease) can be mentioned hyperemesis gravidarum, gestational diabetes, premature rupture of the membranes, and bleeding around delivery. The possibly two-way association between maternal complication and drug use can be exemplified with hyperemesis. This condition is treated with various drugs, including antihistamines, but there are data published which suggests that the use of antihistamines could increase the risk for the adverse effects of hyperemesis (Fejzo et al. 2013).
Many of these complications are more likely to be affected by maternal drug use in middle and late pregnancy than in early pregnancy, but some early effects are possible, for instance, by affecting placenta development. Many pregnancy complications result in an increased use of instrumental deliveries, notably cesarean sections.
5.2 Spontaneous Abortion
Spontaneous abortion or miscarriage is the death of an embryo or fetus before it has reached the age of becoming an infant. This age varies somewhat between populations. The classical limit is drawn when an infant born has a chance to survive after birth. Today the limit is around 22 weeks and this limit is therefore used for instance in Sweden as the lower gestational age limit to define an infant which was born dead. Historically, the limit was higher. Up to 2002 an age limit of 28 weeks was used in Sweden to define a dead fetus as an infant – if it was alive at birth it was defined as an infant, also if born before the 28th week. The variability in definition will not much affect rate estimates as most stillbirths occur late in pregnancy and most spontaneous abortions occur early.
One can also discuss if there should be a lower age limit in analyses of miscarriages. Most likely, a high percentage of fertilized eggs and early embryos – which thus have the potential to develop into an infant – stop developing and the pregnancy may never be realized by the woman. It is possible to identify very early pregnancies with biochemical methods, and some studies have indicated that nearly half of them will never reach the age limit for an infant; most will succumb very early before the woman knows she is pregnant.
In most circumstances studies are made only on miscarriages after the time point when the woman knows about her pregnancy. This will in itself introduce a degree of uncertainty because of the variation in that time point between women. Information on miscarriages is usually obtained from interviews or questionnaires; in some countries it is possible to use medical diagnosis registers which will only identify those women with miscarriage who have searched medical advice or have been hospitalized. When different groups of women are compared (for instance, with reference to drug use), differences in these features may exist which make comparisons uncertain.
From an epidemiological point of view the relatively high number of miscarriages is an advantage. At least 10–15 % of all known pregnancies ends with a miscarriage. This relatively high rate is balanced by the difficulty to identify miscarriages without bias and, as we will see, there is a problem in the analyses of the data.
Most miscarriages occur early in pregnancy and the majority of these represent abnormal embryos, often with gross chromosome anomalies. Later occurring miscarriages (after week 12–14) are usually normal fetuses that miscarry because of some maternal condition. They are actually biologically more closely related to stillbirths than to early miscarriages.
If we suppose that we have succeeded to adequately identify all miscarriages in two groups of women and want to compare the miscarriage rates in the groups, we have to consider what type of denominator should be used. Strictly speaking, the risk for a woman to miscarry is the number of miscarriages occurring among the number of pregnancies at risk at that time of the pregnancy. Pregnancies at risk include pregnancies which will go to delivery but also pregnancies which will, at a later stage of pregnancy, be interrupted by an induced abortion (legal or in some populations illegal). Therefore, exposure rates among pregnancies that miscarry should be compared with the exposure rate among all intrauterine pregnancies which were alive at the time of the miscarriage. This will result in the need for a type of life-table analysis. If the exposure rate among miscarriages is only compared with the exposure rate in pregnancies which continue to delivery, the result will be biased if induced abortion is associated with the exposure under study (as may notably be the case with many psychoactive drugs or drugs with a suspected teratogenic activity). A further discussion of this problem can be found in Källén (2012).
It is often difficult to perform a life-table analysis of miscarriage rate due to lack of adequate data. Various shortcuts have been suggested, e.g., to use as denominator the sum of spontaneous and half of the induced abortions plus births – this means that one supposes that as an average half of induced abortions occur after the gestational age of the studied spontaneous abortions (Susser 1983).
This problem can be illustrated with data from an old study, based on prospectively collected information on drug use during pregnancy (Kullander and Källén 1976). The use of psychoactive drugs was studied. The use of such drugs was nearly twice as common among women with an unwanted pregnancy as among women with a wanted pregnancy. The drug use rate among women who miscarried was 10 %, among women who gave birth only 6 %, but among women who later had an induced abortion it was about 30 %. Estimates indicated that the nearly doubling of the exposure rate in women who will miscarry was due to the effect of the association between drug use and induced abortions. Similar results were reached for maternal smoking and early – but not late – miscarriages.
The literature on maternal drug use and miscarriage risk has usually not taken these complications into consideration. It is typical that in a review and meta-analysis of the problem of antidepressant use during pregnancy and miscarriages, no discussion was made of this basic problem (Hemels et al. 2005). Other studies excluded women with an induced abortion (e.g., Nakhai-Pour et al. 2010) which of course does not solve the problem.
A moderate increase of the miscarriage risk is difficult to demonstrate with certainty because of these complications.
5.3 Stillbirth and Infant Death
Biologically, stillbirths and late spontaneous abortions represent a continuum and the borderline is mainly of administrative nature. Intrauterine death may be the result of some of the pregnancy complications mentioned above, e.g., placenta abruption, but often the mechanism is not known and a specification of the cause of death is often not made. The rate of stillbirths depends somewhat on the definition of the lower age limit, but most stillbirths occur much later. In developed countries with a well-functioning prenatal care, the stillbirth rate is 0.3–0.4 %. The risk for intrauterine death increases with maternal age, is higher at first parity compared with higher parities, and increases with smoking and also with maternal overweight or obesity. Relatively few drugs have been linked to intrauterine deaths, for example, ACE inhibitors and angiotensin II antagonists used as antihypertensives (Pucci et al. 2015).
Among infants born of women using antidepressants, 0.40 % was stillborn and among women not using such drugs, 0.35 %. The crude odds ratio was 1.12 (95 % CI 0.90–1.42) and after adjustment for year of delivery, maternal age, parity, smoking, and BMI, it decreased to 1.04 (95 % CI 0.81–1.33). In spite of the rather large size of the study (3420 stillbirths among which 78 were born of women using antidepressants), the upper confidence limit permits a 33 % excess risk even though the risk estimate is rather close to 1.0.
The distinction between stillbirths and death immediately after birth is not always clear. Sometimes, one uses the concept of perinatal death, including both stillbirths and early neonatal deaths (<7 days after birth). Such deaths are usually identifiable from obstetric records, but if survival should be followed for a longer time, linkage with registers of death gives more complete results. Neonatal death risk is strongly associated with very short gestational duration and gross congenital malformations.
5.4 Gestational Duration and Birth Weight
Gestational duration and birth weight are standard information on all infants born in most data sources and invite analyses.
Classically, gestational duration is calculated from the last menstrual period (LMP) as stated by the woman. Nowadays, gestational duration is often estimated by fetal size determined with sonography. This gives a better estimate even though some minor uncertainties may exist. After in vitro fertilization, exact gestational age is known from the date of embryo transfer and length of embryo incubation, and this could be compared with the age estimated from sonography (Källén et al. 2013a). Even though in general the estimates agreed well, it could be shown that overweight or obesity could influence the exactness of the estimate. Infants born growth retarded may also have been sensitive for estimate errors.
Gestational duration is shorter in twins or higher-order births than in singleton births. For this reason analyses of effects on gestational duration are usually restricted to singleton births.
A common measure consists of preterm birth, that is, births less than 37 weeks. A clinically more important distinction is very preterm birth, shorter than 32 weeks, which of course is a more rare (less than 1 %) but for the neonate a more critical condition. The rate of preterm births varies markedly between different populations, partly because of socioeconomic conditions, partly because of the quality of prenatal and delivery care. In the Swedish Medical Birth Register, 5.2 % of male infants and 4.7 % of the female infants were preterm, and the total preterm rate was 4.9 %. Some extremely preterm infants are, however, missing from the register.
Another method is to determine the mean gestational duration. We can illustrate this with a comparison of the two measurements in singleton infants born by women who had or had not used antidepressants during pregnancy. After antidepressants use, the rate of preterm births increased from 4.9 to 7.8 %, and at the same time the mean gestational duration decreased from 39.4 to 39.0 weeks, a difference of about 3 days. The difference in the rates of preterm birth is clinically important; the difference in mean gestational duration is hardly that.
Numerous factors affect gestational duration and rate of preterm births. In Fig. 5.1 it can be seen that the relationship between maternal age and preterm birth varies with parity and is nonlinear and of different shape at different parities.
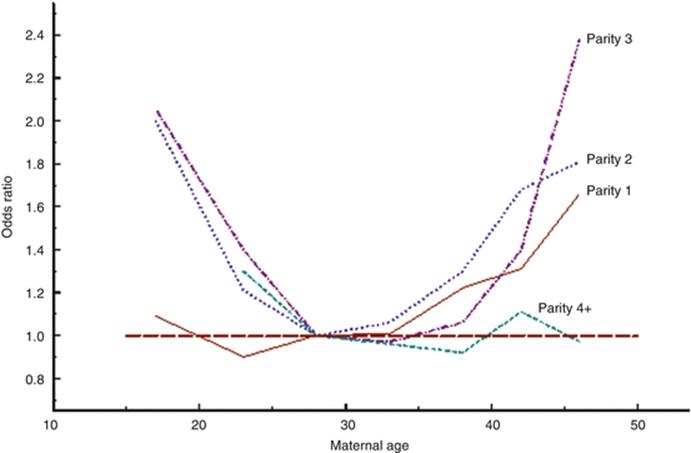
Fig. 5.1
Diagram showing the relationship between maternal age and parity and the risk for preterm birth, adjusted for year of birth, smoking, and body mass index
The effect of maternal smoking (in early pregnancy) on preterm birth is dose dependent and stronger for <32 weeks than for <37 weeks as is seen in Table 5.1.
Table 5.1
Relation between preterm birth and maternal smoking status
|
<32 weeks |
<37 weeks |
|||
|
OR |
95 % CI |
OR |
95 % CI |
|
|
No smoking |
1.00 |
Reference |
1.00 |
Reference |
|
Smoking <10 cigarettes/day |
1.62 |
1.48–1.78 |
1.11 |
1.07–1.48 |
|
Smoking ≥10 cigarettes/day |
2.00 |
1.80–2.42 |
1.79 |
1.68–1.41 |
Also maternal BMI has an effect on the preterm risk as seen in Fig. 5.2. There is a moderate excess of preterm births when the mother has a low BMI, and with a higher than normal BMI (18.5–24.9) the risk increases and is higher for preterm births <32 weeks than for <37 weeks.
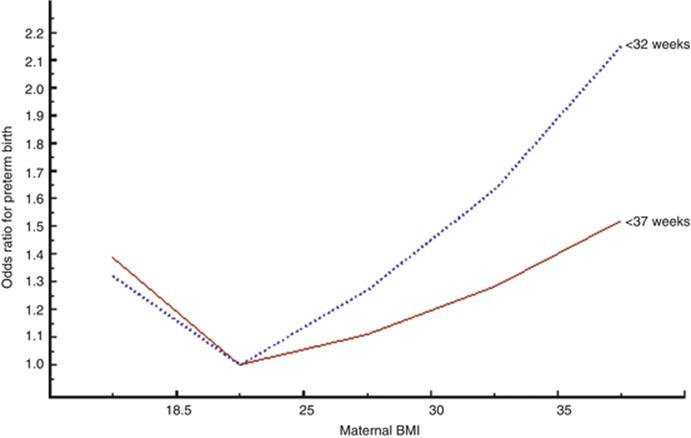
Fig. 5.2
Risk of preterm birth (<32 weeks and <37 weeks) according to maternal BMI, adjusted for year of delivery, maternal age, parity, and smoking
Smoking and overweight or obesity are related to the socioeconomic situation. In Sweden the socioeconomic differences are moderate, and pregnancy care is the same for everyone and is free of charge. There are other factors associated with socioeconomic level which may play a role, e.g., nutrition. In a recent study (Smith et al. 2015), it was shown that a diet rich in fruit and vegetables or with Mediterranean characteristics reduced the preterm rate (32–36 weeks). In countries with large social differences, socioeconomy probably plays a larger role than in Sweden. In the paper by Smith et al., no effect of alcohol or recreational drugs was seen. In abuse situations, such effects are seen, however. Thus preterm birth is a feature of the fetal alcohol syndrome, and abuse of opioids also increases the risk for preterm birth together with a number of other ill effects on the neonate.
Birth weight is a consequence of two factors: gestational age at birth and intrauterine growth. An advantage in using birth weight as an outcome in an epidemiological study is the relative certainty of the information. The usual definition of very low birth weight is <1500 g and of low birth weight, <2500 g. This variable is usually studied in singleton births because twins or higher-order births have lower birth weight in each gestational week than singleton infants have.
5.5 Intrauterine Growth
Intrauterine growth can be followed with sonography, but the end result of a disturbance of intrauterine growth is shown by the infant weight given the week in which it was born. In order to evaluate this, normal growth diagrams are used. These are specific for the studied populations. The definition of intrauterine growth retardation also varies between studies. Often the tenth percentile is used to define growth retardation, sometimes two standard deviations from the mean weight. Usually such growth diagrams are based on the mean and distribution of the birth weights for each gestational week. This means that pathological conditions are included in what is supposed to be a normal population. Other methods have instead used weight modes for each week and estimated the standard deviation as 12 % of that weight – the 12 % come from 40-week pregnancies where the vast majority is normal (Källén 1995). One method was based on intrauterine sonographic weight estimates of infants which were later born at term and were normal (Marsál et al. 1996).
As long as the same growth curves are used for all studied groups, their exact appearance is of less importance. There is, however, a principal difference between the different manners to construct the curves. In most curves based on data in the newborns including the Källén curve (which can be standardized for infant sex and maternal parity), one compares the birth weight of a certain infant with the most common birth weight or the mean weight at that gestational age. As infants born preterm are often growth retarded, this factor is eliminated and the estimate tells if an infant is more growth retarded than the majority of infants born that week. The two growth curves of the Källén and the Marsál diagrams will be identical in term infants, but the latter will lie above the former for preterm births as a result of the fact that infants born preterm are often growth retarded.
Whichever growth curve is used, one can identify three groups of infants: small for gestational (SGA), appropriate for gestational age (AGA), and large for gestational age (LGA) infants. Even though there is an association between SGA and preterm births and LGA and post-term births, it is useful to be able to study the two phenomena independently: does a drug affect the gestational age at which the infant is born or does it affect intrauterine growth without necessarily affecting gestational duration?
Disturbed intrauterine growth resulting in small-for-date babies has important implications for the later development of the child.
5.6 Other Body Dimensions
Like body weight, infant length and head circumference depend on gestational duration. These variables are seldom used in epidemiological studies of the effect of maternal drug use. The effect of maternal anticonvulsant use on infant head circumference was studied by Almgren et al. (2009). They adjusted head circumference for 500 g birth weight classes and calculated the deviation for each exposed infant expressed as standard deviations from the mean head circumference in the birth weight class to which the infant belonged. In this way it was possible to compare infants exposed for anticonvulsants with unexposed infants and also to compare the effect of different anticonvulsants. The clinical significance of a moderately reduced head circumference is uncertain.
5.7 Perinatal Morbidity
Maternal drug use may be associated with perinatal morbidity. Such effects are known for some drugs of abuse, e.g., heroin, but have also been described for instance after maternal use of antidepressants. They may appear as intrauterine asphyxia, respiratory problems in the neonate, hypoglycemia, jaundice, symptoms of central nervous system disturbances, etc. and are identified from diagnoses in medical records or from medical birth registers. Interview or questionnaire data are less reliable and may be biased. A summary evaluation of the status of the infant the first few minutes after birth is given by the Apgar score (0–10), which is usually given after at least 1 and 5 min after birth. Often <7 at the 5-min test is used as a sign of low Apgar score, but in some studies the 1-min score were used. The predictive capacity of the Apgar score has been debated but is usually regarded as of value (Casey et al. 2001; Stuart et al. 2011; Tweed et al. 2015).
An increased risk for perinatal morbidity may be a consequence of an increase in preterm births or a direct effect on the fetus. Among all infants 2.9 % had one or more such diagnoses, 4.6 % among post-term infants, 2.6 % among term infants, 26.5 % among infants born <37 weeks, and 67.1 % among infants born <32 weeks. Table 5.2 shows the effect of maternal use of antidepressants on respiratory diagnoses in singleton newborns. It can be seen that the strongest effect is seen on term infants while no certain effect is seen on post-term or preterm infants. This speaks for a direct effect of the drug which is partly hidden by the increased risks associated with post-term or preterm births.
Table 5.2
Effect of maternal antidepressant use on respiratory diagnoses in the infant according to pregnancy duration
|
Group of infants |
OR |
95 % CI |
|
All |
1.71 |
1.62–1.81 |
|
Post-term infants (≥42 weeks) |
1.20 |
0.89–2.62 |
|
Term infants (37–41 weeks) |
1.89 |
1.77–2.03 |
|
Preterm infants (<37 weeks) |
1.07 |
0.95–1.22 |
|
Very preterm infants (<32 weeks) |
1.28 |
0.82–2.02 |
Some neonatal diagnoses are uncommon and large materials are needed to study them. An example is PPHN which in pregnancies with more than 34 weeks duration occurs in only some three per 1000 births. Another example is necrotizing enterocolitis which is also a rare complication, typically a consequence of very preterm birth.
5.8 Long-Term Effects
It has long been known that abuse of alcohol or recreational drugs may cause long-term effects on the cognitive development of the exposed child and also other developmental disturbances. Less is known about such effects of medically used drugs but has been described for anticonvulsants (notably valproic acid) and also for some other psychoactive drugs. During the last decade or so, other long-term effects of maternal drug use have been discussed, e.g., effects on the risk of childhood asthma, ADHD, and autism.
Different approaches can be used in order to identify long-term outcomes. In small studies, various psychological tests can be applied in order to identify effects of maternal drug use. Usually mean values are compared between exposed and unexposed groups, a method which is un-sensitive if the exposure has caused an increased risk of an uncommon outcome. The mean intelligent quotient may be nearly the same in the two study groups, but the exposure may have increased the risk for mental retardation. This is a situation similar to that when mean gestational duration is compared with the rate of preterm birth (see above).
With modern health and other registers, it is sometimes possible to follow a large number of children which have been exposed in utero for specific drugs. This makes it possible to identify also risk increases for less common outcomes. For this purpose, various sources can be used. We can exemplify this with childhood asthma. Some studies have used hospital discharge registers to identify such disease, sometimes also diagnoses from outpatient clinics. Other studies have used registers of filled prescriptions and regarded at least repeated filling of prescriptions for anti-asthmatics as evidence for asthma in the child (Källén et al. 2013b). In selected populations (often from selected strata of the population), data from medical insurance systems have been used. There are weaknesses with all methods. Hospital discharge diagnoses have a tendency to identify severe cases which have needed hospitalization. Outpatient information may be biased if maternal characteristics affect the probability that a child with perhaps light asthma is taken to medical care. This will also affect the results of studies based on prescription registers where the problem also exists that anti-asthmatics may have been prescribed for other conditions than asthma.
In studies of mental retardation or other severe neuropsychiatric conditions, health registers have been much used, for instance the Danish psychiatric register (Sørensen et al. 2013). Prescription registers can be used to identify children with conditions when specific drugs are used for the conditions. An example is the use of methylphenidate or similar drugs at ADHD (Källén et al. 2013c). In some populations it is possible to study school results, e.g., at the end of compulsory school, based on national registers of school marks (Forsberg et al. 2011).
Other health registers may exist which make it possible to study specific long-term outcomes. One example is cancer registers which give good information on the occurrence of malignant tumors.
In order to follow the children through life, valid identification is necessary. Notably in the Scandinavian countries, this is easily done with the help of the personal identification number every person living in the country gets at or immediately after birth. Such numbers are widely used in society and in all health care. In order to protect patient privacy, the identification number can be changed to other, neutral numbers, but that has to be done in a similar way in all health registers to be useful. In many populations probability linkage between registers has to be made which is more complex and uncertain than the use of individual identification numbers.
All studies of prenatal effects of drug use on long-time development of the child have complications. A genetic component in the disease for which the drug was taken can transfer susceptibility for the disease to the child. The situation during the child’s early life may also be affected by the maternal disease and cause disturbances in the child’s development.
We can exemplify this problem with studies on maternal use of antibiotics during pregnancy and childhood asthma. Many studies have shown that such an association exists, but as maternal asthma is associated with antibiotic use and a genetic component for asthma exists, the association could be spurious. This was recently shown in a large study by Örtqvist et al. (2014) where a sibling analysis seemed to remove the association completely. In this case, about one-third of the material was eligible for sibling analyses.
Permanent life-long impairment of the child’s function is perhaps of greater importance than many congenital malformations which can easily be corrected.
References
Almgren M, Källén B, Lavebratt C (2009) Population based study of antiepileptic drug exposure in utero – influence on head circumference in the newborn. Seizure 18:672–675CrossRefPubMed
Casey BM, McIntire DD, Leveno KJ (2001) The continuing value of the Apgar score for the assessment of newborn infants. N Engl J Med 344:467–471CrossRefPubMed
Fejzo MS, Magtira A, Schoenberg FP, MacGibbon K, Mullin P, Romero R et al (2013) Antihistamines and other prognostic factors for adverse outcome in hyperemesis gravidarum. Eur J Obst Gynecol Reprod Biol 170:71–76CrossRef
Forsberg L, Wide K, Källén B (2011) School performance at age 16 in children exposed to antiepileptic drugs in utero – a population-based study. Epilepsia 52:364–369PubMed
Hemels ME, Einarson A, Koren G, Lanctot G, Einarson TR (2005) Antidepressant use during pregnancy and the rates of spontaneous abortions: a meta-analysis. Ann Pharmacother 39:803–809CrossRefPubMed
Källén B (1995) A birth weight for gestational age standard based on data in the Swedish Medical Birth Register. Eur J Epidemiol 11:601–605
Källén B (2012) Chapter 26. Human studies – epidemiologic techniques in developmental and reproductive toxicology. In: Hood R (ed) Developmental and reproductive toxicology. A practical approach, 3rd edn., Informa Healthcare, London, pp 645–647
Källén B, Finnström O, Nygren K-G, Otterblad Olausson P (2013a) Maternal and fetal factors which affect fetometry: use of in vitro fertilization and birth register data. Europ J Obstet Gynecol Reprod Biol 170:372–375CrossRef
Källén B, Finnström O, Nygren K-G, Otterblad Olausson P (2013b) Maternal drug use during pregnancy and asthma risk among children. Paed Allergy Immunol 24:28–32CrossRef
Källén B, Borg N, Reiss M (2013c) The use of central nervous system active drugs during pregnancy. Pharmaceuticals 6:1221–1286CrossRefPubMedPubMedCentral
Kullander S, Källén B (1976) A prospective study on drugs and pregnancy. I Psychopharmaca Acta Obstet Gynecol Scand 55:25–33CrossRefPubMed
Marsál K, Persson PH, Larsen T, Lilja H, Selbing A, Sultan B (1996) Intrauterine growth curves based on ultrasonically estimated foetal weights. Acta Paediatr 85:843–848CrossRefPubMed
Nakhai-Pour HR, Broy P, Bérard A (2010) Use of antidepressants during pregnancy and the risk of spontaneous abortion. CMAJ 182:1031–1037CrossRefPubMedPubMedCentral
Örtqvist AK, Lundholm C, Kieler H, Ludvigsson JF, Fall T, Ye W et al (2014) Antibiotics in fetal and early life and subsequent childhood asthma: nationwide population based study with sibling analysis. BMJ 349:g6979. doi:10.1136/bmj.g6979CrossRefPubMedPubMedCentral
Palmsten K, Huiybrechts KF, Michels KB, Williams PL, Mogun H, Setogushi S et al (2013) Antidepressant use and risk for preeclampsia. Epidemiology 24:682–691CrossRefPubMedPubMedCentral
Pucci M, Sarween N, Knox ED, Lipkin G, Martin U (2015) Angotensin-converting enzyme inhibitors and angiotensin//receptor blockers in women of childbearing age: risk versus benefits. Expert Rev Clin Parmacol 8:221–231CrossRef
Reis M, Källen B (2010) Delivery outcome after maternal use of antidepressant drugs in pregnancy: an update using Swedish data. Psychol Med 11:1723–1733CrossRef
Smith LK, Draper ES, Evans TA, Field DI, Johnson SJ, Manktelow BN et al (2015) Associations between late and moderately late preterm birth and smoking, alcohol, drug use and diet: a population-based case-cohort study. Arch Dis Child Fetal Neonatol Ed 100:F486–F91. doi:10.1136/archdischild-2014-207265CrossRef
Sørensen MJ, Grenborg TK, Christensen J, Parner ET, Vestergaard M, Schendel D et al (2013) Antidepressant exposure in pregnancy and risk of autism spectrum disorders. Clin Epidemiol 5:449–459CrossRefPubMedPubMedCentral
Stuart A, Otterblad Olausson P, Källén K (2011) Apgar scores at 5 minutes after birth in relation to school performance at 16 years of age. Obstet Gynecol 118:201–208CrossRefPubMed
Susser E (1983) Spontaneous abortion and induced abortion: an adjustment for the presence of induced abortion when estimating the rate of spontaneous abortion from cross-sectional studies. Am J Epidemiol 117:305–308PubMed
Tweed EJ, Mackay DF, Nelson SM, Cooper S-A, Pell JP (2015) Five-minute Apgar score and educational outcomes: retrospective cohort study of 751 369 children. Arch Dis Child Feral Neonatal Ed 101:F121–F126. doi:10.1136/archdischild-2015-308483CrossRef
Vest AR, Cho LS (2014) Hypertension in pregnancy. Curr Atheroscel Rep 16:395. doi:10.1007/s11883-013-0395-8CrossRef