Sedative/Hypnotic
PREGNANCY RECOMMENDATION: Limited Human Data—No Relevant Animal Data
BREASTFEEDING RECOMMENDATION: No Human Data—Potential Toxicity
PREGNANCY SUMMARY
Although the data are limited, there is evidence of structural anomalies in newborns exposed to amobarbital during organogenesis. The absolute risk is unknown but may be low. The drug also is eliminated slowly in newborns. If possible, the drug should be avoided during organogenesis and near delivery.
FETAL RISK SUMMARY
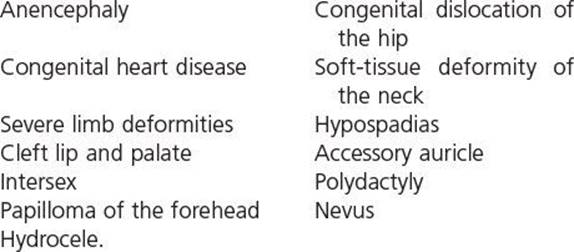
Amobarbital is a member of the barbiturate class. The drug crosses the placenta, achieving levels in the cord serum similar to those in the maternal serum (1,2). Single or continuous dosing of the mother near term does not induce amobarbital hydroxylation in the fetus as demonstrated by the prolonged elimination of the drug in the newborn (half-life 2.5 times maternal). An increase in the incidence of congenital defects in infants exposed in utero to amobarbital has been reported (3,4, pp. 336, 344). In one survey of 1369 patients exposed to multiple drugs, 273 received amobarbital during the 1st trimester (3). Ninety-five of the exposed mothers delivered infants with major or minor abnormalities. Malformations associated with barbiturates, in general, were as follows:
The Collaborative Perinatal Project monitored 50,282 mother–child pairs, 298 of whom had 1st trimester exposure to amobarbital (4, pp. 336, 344). For use anytime during pregnancy, 867 exposures were recorded (4, p. 438). A possible association was found between the use of the drug in the 1st trimester and the following: cardiovascular malformations (7 cases), polydactyly in blacks (2 cases in 29 blacks), genitourinary malformations other than hypospadias (3 cases), inguinal hernia (9 cases), and clubfoot (4 cases).
In contrast to the above reports, a 1964 survey of 187 pregnant patients who had received various neuroleptics, including amobarbital, found a 3.1% incidence of malformations in the offspring (5). This is approximately the expected incidence of abnormalities in a nonexposed population. Arthrogryposis and multiple defects were reported in an infant exposed to amobarbital during the 1st trimester (6). The defects were attributed to immobilization of the limbs at the time of joint formation, multiple drug use, and active tetanus.
BREASTFEEDING SUMMARY
No reports describing the use of amobarbital during lactation have been located. Similar to other barbiturates, the drug probably is excreted into breast milk. The effects of this exposure are unknown, but toxicity is possible (e.g., see Phenobarbital).
References
1.Kraver B, Draffan GH, Williams FM, Calre RA, Dollery CT, Hawkins DF. Elimination kinetics of amobarbital in mothers and newborn infants. Clin Pharmacol Ther 1973;14:442–7.
2.Draffan GH, Dollery CT, Davies DS, Krauer B, Williams FM, Clare RA, Trudinger BJ, Darling M, Sertel H, Hawkins DF. Maternal and neonatal elimination of amobarbital after treatment of the mother with barbiturates during late pregnancy. Clin Pharmacol Ther 1976;19:271–5.
3.Nelson MM, Forfar JO. Associations between drugs administered during pregnancy and congenital abnormalities of the fetus. Br Med J 1971;1:523–7.
4.Heinonen OP, Slone D, Shapiro S. Birth Defects and Drugs in Pregnancy. Littleton, MA: Publishing Sciences Group, 1977.
5.Favre-Tissot M. An original clinical study of the pharmacologic-teratogenic relationship. Ann Med Psychol (Paris) 1964;1:389.
6.Jago RH. Arthrogryposis following treatment of maternal tetanus with muscle relaxants. Arch Dis Child 1970;45:277–9.