Shlomo Raz1
(1)
Division of Pelvic Medicine and Reconstructive Surgery, UCLA School of Medicine, Los Angeles, CA, USA
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-1-4939-2941-2_2) contains supplementary material, which is available to authorized users.
Keywords
Stress incontinenceSlingsBladder neck suspensionFascial slingFascia lata slingSpiral sling
2.1 Mechanisms of Normal Continence
Stress urinary incontinence—the involuntary loss of urine through the intact urethra as a result of a sudden increase in intra-abdominal pressure—creates a social problem to the patient. It is the end result of a deficient urinary control system in which the intra-abdominal pressure exceeds the resistance produced by the urethral closure mechanisms. Normal continence in the female results from the delicate balance of several forces, including closing forces of the urethra, a critical functional and anatomical urethral length, the ability of the pelvic floor and the urethra to increase urethral resistance at the time of stress, and the proper anatomical location of the sphincteric unit. We like to organize these factors in what we call the UCLA theory of female continence, in which the U signifies the urethral changes that occur during stress, the C represents the closing function of the urethra, the L is its functional and anatomical length, and A stands for anatomy. These factors are briefly described below.
2.1.1 Closure Forces of the Urethra: The Sphincteric Unit
The urethra is a short elastic tube (3–4 cm long) with a complex anatomical and functional structure. While the woman is resting, walking, or straining, it normally provides a leakproof closure, but during voiding it funnels and opens to permit complete bladder emptying (Fig. 2.1a, b).



Fig. 2.1
(a) Diagram of the lower urinary tract showing the bladder, the bladder neck, and the urethra. The urethra is composed by the inner layer of the mucosa and submucosa, the smooth muscle, and the skeletal musculature (intramural and extramural). (b) Diagram of the sphincteric unit. The bladder neck is the primary mechanism of continence. Longitudinal and circular fibers of the trigone and detrusor muscle provide urethral closure during rest and the ability to open and funnel during micturition. The mucosal and submucosal layers extend along the urethral lumen containing a rich vascular plexus very important for urethral coaptation and continence. (c) Histology of the urethral wall showing the infolded urethral mucosa with a rich submucosal vascular plexus. Surrounding the inner layer is the smooth muscle and the intrinsic skeletal fibers. (d) Axial T2 MRI view of the midurethral area showing the dark fibromuscular envelope enclosing the inner mucosa and submucosal vascular plexus of the urethra. (e) Using a vaginal coil a longitudinal image of the urethral wall and mucosal and submucosal layers are seen with clarity. The urethra is not a muscular tube; rather it is an internal mucosal layer with a rich vascular plexus compressed by the outer muscular layer
The histological structure of the urethra can be seen as a thin, fibromuscular envelope filled with spongy tissue and infolded epithelium surrounded by smooth and skeletal muscle (Fig. 2.1c–e). We can describe three distinct structures: the mucosal sphincter (epithelium and spongy tissue), the smooth muscle and fibroelastic envelope, and the outer skeletal muscular sphincter.
The urethral mucosa is seen as a multilayer, infolded epithelium that meshes like interlocking fingers, to provide an efficient urethral seal. Under the mucosa is a rich, vascular cushion of spongy tissue. This combination, which we call the mucosal urethral sphincter, has a great degree of plasticity and easily deforms under minimal external pressures, providing an efficient seal. The urethra can conform around any inserted object (such as ureteric catheters) while still remaining leakproof. The epithelium and the spongy tissue are under hormonal control, and estrogen deprivation will lead to atrophy of the mucosa, flattening of the epithelium, atrophy of the spongy tissue, and a deficient urethral seal. Trauma of surgery, radiation, neurological conditions, atherosclerosis, and age-related changes may lead to further atrophy of the mucosal sphincter. As in a faucet, a good washer will provide a reliable seal with minimal pressure, but a faucet with a deficient washer will leak. Increasing outside pressure by tightening the faucet will not prevent leakage if the washer is defective. There is no correlation between urethral pressures and continence. Continence depends on the presence of adequate urethral resistance against increases in bladder pressure, and it is clear that the mucosal sphincter plays a very important role in achieving a complete urethral seal.
Around the urethral mucosa is a thin, fibromuscular envelope composed of elastic tissue, smooth muscle, and intrinsic slow-twitch skeletal musculature. This layer compresses the mucosal sphincter, enhancing the urethral resistance. Paralysis, trauma, surgery, radiation, or estrogen deficiency may alter the function of this envelope, inducing a decrease in urethral continence. Autonomic fibers from the sacral spine (S2–S4) and thoracic spine (T9–L1) control the smooth musculature.
The third component of the sphincteric unit with important function in continence is the intramural and extramural skeletal musculature. The extrinsic skeletal musculature is mainly composed of fast-twitch fibers responding to voluntary and involuntary reflexes. Involuntary contraction of the pelvic floor during exercise or a sudden change in abdominal pressures is a protective reflex to prevent incontinence. Another involuntary reflex provides basic tone to the skeletal musculature. The skeletal musculature plays an important role in female continence by its effect on the basic sphincter tone and the reflex and voluntary activity of the sphincter during stress.
2.1.2 Urethral Length
The distance between the bladder neck and the external urethral meatus represents the anatomical length. The urethra can be divided into three segments: proximal, midurethral, and distal. The proximal urethra, the first level of female continence, comprises the bladder neck and intra-abdominal urethra; it is only 1½–2 cm long. A woman will remain continent if the midurethral and distal urethral functions remain intact, even if the proximal urethra and bladder neck are excised (as during total cystectomy), incised (as after a transurethral incision of the bladder neck), or reconfigured (as after Y–V plasty). With fluoroscopy during video urodynamic studies in the standing position, we can observe that the level of continence is at the bladder neck in most women who have normal continence, but in 20–30 % of these women, the bladder neck may be incompetent, confirming that the midurethral segment is the most important secondary area of continence. The midurethral segment is responsible for continence when the bladder neck is incompetent. The pubourethral ligament supports the urethra to the inferior rami of the symphysis. The midurethral area is where the reflex or voluntary contraction to sudden changes of intra-abdominal pressures and the voluntary and involuntary relaxation of the urethra during voiding occurs. The distal centimeter of the urethra does not have sphincteric function and acts as a mere conduit to direct the urinary stream outside the vaginal canal. It can be excised without affecting continence.
2.1.3 Anatomical Support
The anatomical support of the urethra was described in Chap. 1. Following are further details on the impact of the anatomical support for urethral continence.
The urethra is supported by three structures: the close attachment to the vaginal wall and the pubourethral and urethropelvic fasciae or ligaments (Fig. 2.2a).

Fig. 2.2
(a) Diagram of the structures involved in urethral support. The superior support is provided by the pubourethral fascia, the lateral support by the urethropelvic fascia, and the inferior support by the intimate attachment to the urethra to the vaginal wall. (b) Dissection of the anterior vaginal wall shows the lack of a defined cleavage plane between the vaginal and urethral wall. The urethra moves together with the anterior vaginal wall
The urethra moves together with the anterior vaginal wall and is tightly attached to the vaginal wall. Changes in vaginal support will affect urethral support and function (Fig. 2.2b).
The pubourethral fascia attaches the urethra to the inferior ramus of the pubic bone; it is the only connection of the urethra to the pubic bone (Fig. 2.3a, b). During strain, the normally supported urethra rotates a small amount under the pubic bone (minimal mobility), but in patients with deficient pubourethral fascia, the distance of the urethra from the inferior ramus of the symphysis is increased during strain, and the urethra is allowed to rotate considerably under the pubic bone (Fig. 2.3c–e).


Fig. 2.3
(a) A suprameatal incision was made and the distal anterior aspect of the urethra is seen. Pubourethral fascia is detached from the inferior rami of the pubic bone. The urethropelvic fascia supports the urethra to the inferior rami of the pubic bone. (b) A lateral distal vaginal incision was made and the retropubic space is entered. The forceps separates the urethropelvic fascia from the arcus tendineus fascia pelvis. At the superior aspect of the incision we can see the pubourethral fascia. Inserting a finger into the retropubic space and pointing it toward allow us to palpate the pubourethral fascia under the pubic symphysis. (c) Lateral T2 MRI image of the pelvis with strain showing the downward rotation of the urethra under the inferior rami of the pubic bone. The pubourethral fascia is the only connection of the urethra to the inferior aspect of the pubic bone. (d) Lateral T2 image of the pelvis under strain in a patient with stress incontinence. The urethra further rotates under the pubic bone and funneling of the bladder neck is seen
The urethropelvic fascia comprises the endopelvic and periurethral fascia attaching the urethra to the lateral pelvic wall, the levator muscle, and the arcus tendineus fascia pelvis. It is the only connection of the urethra to the levator. Contraction of the levator muscles will increase the tension of the urethropelvic fascia, stabilizing the urethra and increasing urethral resistance. Weakened urethropelvic fascia leads to urethral hypermobility and deficient compensatory response of the urethra during stress (Fig. 2.4a–e).


Fig. 2.4
(a) T2 MRI image of the urethra. Using a vaginal coil, the vaginal distension allows us to see the urethra supported like two wings laterally to the levator muscle. The urethropelvic fascia is composed by the periurethral fascia in the vaginal side and the endopelvic fascia in the abdominal side. The levator inserts on a condensation of the obturator muscle. ATFP, arcus tendineus fascia pelvis; ATLA, arcus tendineus levator ani. (b) Diagram of the abdominal view of the bladder support and urethra. The endopelvic fascia (the abdominal segment of the urethropelvic fascia) inserts laterally into the levator muscle (arcus tendineus fascia pelvis) inferior to the arcus tendineus levator ani. (c) Diagram of the lateral urethral support. The urethropelvic fascia is composed by the endopelvic and periurethral fascia. Both cover the sphincteric unit extending laterally to insert into the levator musculature (arcus tendineus fascia pelvis). The urethropelvic fascia is the only structure connecting the urethra to the lateral pelvic wall. (d) Diagram of the deficient urethropelvic fascia. The fascia can be attenuated or detached from the lateral levator musculature producing proximal urethral mobility and descent of the sphincteric unit. Poor levator function or relaxation will produce a similar effect. (e) During surgery a lateral incision of the anterior vaginal wall was performed, and the retropubic space was entered with scissors exposing the lateral margin of the urethropelvic fascia that was detached from the arcus tendineus fascia pelvis
2.1.4 Urethral Changes During Stress: Compensatory Mechanisms
Sudden changes in intra-abdominal pressure have a marked effect on urethral function. Three changes seem to be of primary importance: (1) the backboard effect of urethral support, (2) the valvular effect at the bladder neck, and (3) the voluntary and reflex contraction of the pelvic floor.
The proximal urethra is an intra-abdominal structure, so any sudden increase of pressures will lead to a concomitant increase in urethral resistance and closure in the proximal urethra. A poorly supported urethra in a low, dependent position will mechanically tend to funnel and open during sudden increases of abdominal pressure (Fig. 2.5a). A properly supported urethra will respond to sudden changes in abdominal pressures with an increased urethral resistance as it is compressed against a strong posterior support (backboard effect); surgeries like a sling prevent the downward rotation of the urethra and create and hammock against which the urethra can be compressed during a sudden increase in abdominal pressure. A midurethral sling should support the urethra, increasing urethral resistance without direct increase in urethral pressures.

Fig. 2.5
(a) Diagram of the lateral support of the sphincteric unit. During sudden increase of abdominal pressure, there is a compensatory contraction of the levators (stress reflex). Levator contraction will increase the tensile forces of the urethropelvic fascia producing an increase of urethral resistance and protecting the urethra against leakage. Voluntary contraction of the levator as in pelvic floor exercises will have a similar effect. (b) When the urethropelvic fascia is detached or attenuated or the levator function is deficient, increase of abdominal pressures will not produce the reflex increase in urethral resistance that occurs in normal supported patients. Pelvic exercise in patients with significant deficient levator musculature will not produce any effect on urethral resistance or improve continence (c). Videourodynamic images of a patient with stress incontinence showing loss of urine per urethra (flow) in a patient with sudden changes of abdominal and vesical pressures without a change in the true detrusor pressures. Loss of urine during stress may or may not be associated with urethral mobility. Stress incontinence occurs due to a deficient sphincteric urine with a loss of the normal compensatory mechanism during stress
The normally supported urethra is superior to the bladder base and trigone creating an angulation of 90° with the bladder neck. This anatomical relation produces a valvular effect at the bladder neck. Sudden increases of abdominal pressure will increase this valvular effect in a well-supported urethra, protecting against incontinence. After a successful Burch colposuspension for stress incontinence, we very often can reproduce stress incontinence by elevating the bladder base in patients who were perfectly cured by the operation. This valvular effect also plays a significant role in the appearance of outlet obstruction in patients who undergo anti-incontinence procedures and had a cystocele before surgery or later develop a secondary cystocele.
The skeletal musculature has fast-twitch fibers providing a rapid pelvic floor response to acute events and slow-twitch fibers responsible for the basic skeletal muscle tone. In the resting state, the basic tone of the skeletal musculature increases with bladder filling. During sudden changes of intra-abdominal pressures, a reflex response of the fast-twitch fibers increases urethral closure and resistance. In patients with pelvic floor relaxation due to trauma of delivery, neuropathy of the pudendal nerve, hormonal changes, age, or multiple surgeries, this compensatory mechanism fails. The urethral resistance will not increase with changes in abdominal pressure, so a tendency for stress incontinence will ensue.
The skeletal musculature has a direct and indirect impact on urethral function. The only attachment of the urethra to the levator muscle is the urethropelvic ligaments. Voluntary or involuntary (cough reflex) contraction of the levators tenses the urethropelvic ligaments, providing support and increasing resistance. Elongated or detached urethropelvic ligaments or poor levator function will result in poor urethral compensation during sudden changes in abdominal pressures (Fig. 2.5). The extramural fibers of the urethra are poorly defined and may play a compensatory role in continence and urethral compensation. The intramural skeletal musculature surrounds the urethra. With aging, there is progressive denervation, atrophy, and loss of neuronal mass, further impacting urethral closure.
2.2 Clinical Correlates
Normally, anatomical support of the bladder neck and proximal urethra allows for thorough transmission of intra-abdominal pressure increases to this area of continence. Together with an intact sphincteric unit, with its coapting mucosal surface, and the reflex pelvic contraction at the time of cough or strain, a leakproof sphincter is achieved. Failure of one of the components of this delicate balance will not invariably produce stress incontinence because of the compensatory effect of the other factors. This effect also may explain the phenomenon whereby many patients with urethral hypermobility can be totally asymptomatic; only a small percentage of these patients have stress incontinence (Fig. 2.6). Although obstetric trauma and the resulting anatomical displacements tend to occur when the woman is in her 20s or 30s, symptomatic stress incontinence is found mainly around menopause, suggesting that hormonal changes (atrophy of urethral tissue) superimposed on the anatomical defect facilitate the loss of urine during stress. Stress incontinence seems therefore to occur as a result of a failure of compensatory mechanisms when one factor such as anatomy is abnormal. There is no doubt that the underlying anatomy is of great importance, as stress urinary incontinence is corrected by a surgery that usually also corrects the anatomy. But it is important to remember that anatomical defects alone are not causing stress incontinence; they are only one of the factors in a complex mechanism of pelvic floor relaxation. The actual anatomic basis of these pathophysiologic concepts is an area of both confusion and controversy, yet it is only through a clear conceptual understanding of the anatomy involved that rational treatment can be given.

Fig. 2.6
(a) Lateral cystogram in a patient with significant urethral mobility. During straining, the urethra is moved away from its normal close proximity to the inferior ramus of the symphysis into a low position, owing to weakness of the pubourethral and urethropelvic fascia. Most patients with this anatomical defect do not lose urine unless there is an intrinsic sphincter defect. (b) Lateral T2 MRI of the pelvis in a patient with stress incontinence. In the relax films, the urethra is seen in a low position, still in close proximity to the inferior rami of the pubic bone (pubourethral fascia). (c) During strain there is downward rotation of the urethra under the inferior rami of the pubic bone, descent and funneling of the bladder neck, and an open urethra
We can now make a clinical correlate between the different anatomical defects of the anterior vaginal wall. We must highlight the importance of the insertion of the urethropelvic ligament to the lateral pelvic wall (arcus tendineus fascia pelvis). It is the only connection of the urethra to the levator muscle. The urethra is seen supported to the lateral pelvic wall and enclosed like a sandwich (between endopelvic and periurethral fasciae) by this fascial extension with both strength and elasticity, so as to rise and fall with changes in intra-abdominal pressure and with contraction or relaxation of the levator musculature.
As mentioned above, the pubourethral ligaments divide the urethra into three areas of continence: the intrapelvic, intra-abdominal proximal third (1.5 cm in length); a mid third, which includes the pubourethral ligaments; and a distal third, which serves only as a conduit for urine, without continence activity. Passive continence (resting involuntary control of continence) depends on the integrity, coaptation, and support of the proximal third of the urethra, but this area can be incised or excised, and the patient can remain continent because the mid third will take over as a secondary mechanism for passive continence. In some patients with significant stress urinary incontinence, the bladder neck is open and incompetent; in these cases, the midurethra is responsible for passive continence.
In a woman with normal continence, a complex compensatory mechanism is standing by to improve the seal effect of the urethra during any stress such as coughing, straining, or walking. The midurethral complex is not only a secondary mechanism for passive continence but is the area most responsible for active continence (voluntary control of urine by contraction of pelvic musculature). The area just distal to the pubourethral ligaments is outside the realm of the intra-abdominal forces, and it is the area of “high pressures” when urethral pressure studies are performed. There seems to be no relationship between urethral pressure and continence or incontinence. Urethral pressures are not changed after incontinence is cured or improved by a sling procedure or injection of a bulking agent. Voluntary contraction of the skeletal pelvic musculature is able to stop the urinary stream during voiding and increase urethral resistance during increases in abdominal pressure. During cough, strain, or any other sudden increase of abdominal pressures, there is a reflex involuntary contraction of the pelvic floor that increases urethra resistance and protects against any loss of urine. With age, multiple deliveries, and pelvic floor relaxation, the levator function becomes deficient, diminishing the reflex and voluntary activity of the pelvic floor as a protective mechanism against incontinence.
Other factors also participate to protect the urethra against involuntary loss of urine. A mild posterior bladder rotation against a well-supported urethra will increase the valvular effect of the bladder neck. In fact, many patients cured by a bladder suspension or sling procedure can have incontinence demonstrated by elevation of the bladder base at the time of strain. Voluntary or reflex contraction of the levator and obturator muscles will increase tension on the urethropelvic ligaments, thereby elevating and compressing the proximal urethra. Direct transmission of intra-abdominal forces to a well-supported proximal urethra will increase its closing mechanism. This backboard effect explains the curative effects of the sling procedures in which a hammock is created against which the urethra can be compressed during changes in abdominal pressure.
Pelvic floor relaxation and weakening of the urethropelvic and pubourethral ligaments will produce posterior and downward rotation of the proximal urethra and bladder neck. The compensatory mechanisms and the improved seal of the proximal urethra against sudden changes in abdominal pressures are impaired. Urethral hypermobility will transfer the bladder neck area to a dependent position in the pelvis, where sudden increases in intra-abdominal pressures will facilitate its funneling and opening, as the valvular effect is lost. A weak levator will not efficiently increase resistance during stress. The intra-abdominal forces are not transmitted efficiently to the proximal urethra. Nevertheless, a hypermobile urethra alone will not lead to incontinence unless the intrinsic sphincter function is impaired (urethral seal) (Fig. 2.7).

Fig. 2.7
(a) Lateral cystogram in a patient with stress incontinence. In the relax position, the bladder neck is at the level of the inferior rami of the pubic bone appearing to be incompetent (funneled). (b) With strain there is downward rotational descent of the urethra with further funneling of the bladder neck. (c) With further strain the urethra and bladder neck are totally open. It is now inferior to the pubic bone and the distance of the urethra to the inferior pubic bone has increased (weakness of pubourethral fascia). The urethra is open and the patient is leaking urine
Surgical transfer of the proximal urethra to a more supported position will restore some of the urethral compensatory mechanisms against sudden changes in abdominal pressures (Fig. 2.8). Sling procedures provide dynamic support of the urethra without increasing urethra pressures (Fig. 2.9).

Fig. 2.8
Lateral cystogram in a patient after a successful sling procedure. Sling procedures prevent the sequence of funneling and downward rotation of the urethra. It is not only an anatomical correction that occurs after a sling but an important functional change. Slings allow proper transmission of abdominal pressures during strain. They create a hammock under the urethra (without compression) so increase abdominal pressures can increase urethral resistance during stress. The normal compensatory mechanism of the urethra is restored including the increase of urethral resistance by the levator contraction. The urethral elevation above the bladder level may also create a valvular effect improving continence (Burch procedure)

Fig. 2.9
Diagram to explain the impact of suburethral support on urethral function. Support alone can improve continence without direct impact on urethral pressures. (a) If a garden hose is placed under a strong surface, minimal superior compression is required to prevent the stream of water. (b) If the surface under the garden hose is soft and giving, higher forces are required to stop the stream of water. (c) If the garden hose is elevated without any direct compression, less superior pressure will be required to interrupt the flow of water
2.3 Surgical Correlates
Armed with this better understanding of the anatomy of stress incontinence, what surgical correlates can be drawn? First of all, a clinician who has a conceptual picture of the structures involved in support of the bladder neck and proximal urethra gains a better understanding of what actually occurs when surgical therapy is used. The various types of sling or suspension procedures provide dynamic support to the bladder neck and urethra, an increase in urethra resistance, and improved urethral coaptation without creation of an obstruction or urethral compression. In suspension procedures (like Burch or bladder neck suspensions), the vaginal wall is the supporting structure of the urethra; it does not have a suburethral component. Sling procedures have a suburethral component. The importance of this suburethral segment is unclear, as the incision of this suburethral segment of a sling after obstruction usually does not result in recurrence of the stress incontinence. These procedures increase urethral resistance during changes in abdominal pressure by a combination of factors: by creating a hammock against which the urethra is compressed, by allowing better transmission of intra-abdominal pressures, by allowing better compensation of urethral function during stress, or by creating a valvular effect.
As one gains a clearer view of the anatomy, it becomes apparent which structures are important for urethral support and, perhaps more importantly, where and how urethral surgery should be performed to avoid complications. The anatomical placement of sutures or sling material has a major impact on the eventual outcome. When performing a sling or vaginal suspension, placing the sutures or the sling material too close to the urethral wall creates a danger of obstruction and iatrogenic urethral damage. When a sling is done proximal to the bladder neck, there will be no impact on the continence mechanism. A sling procedure that is too tight or penetrates deeply into the periurethral fascia can result in urethral obstruction or erosion. Using translabial ultrasound and studying the final location of midurethral slings, we have found that 50 % are actually not in the midurethra. Urethral location of the mesh appears to have no impact on the clinical outcome of the surgery.
2.4 Treatment of Stress Incontinence
The remainder of this chapter describes various procedures in the treatment of stress incontinence. All the procedures in this section share similar indications, preoperative and postoperative care, and complications. The techniques given represent our own surgical technique. Even as most procedures for the treatment of stress incontinence are done with the mesh, we have nearly abandoned the use of the mesh for treatment of incontinence and pelvic prolapse. Though these days most patients request surgery without some elect to have these procedures and take the risk of short- and long-term mesh complications like pain or extrusion. We describe only one surgery using mesh: a sling procedure (distal urethral polypropylene sling) for simple stress incontinence. We now perform the spiral sling using autologous fascia.
2.4.1 Indications for Surgery
Indications for surgery are mainly stress incontinence or mixed incontinence with a primary component of stress. The degree of incontinence, prior surgeries or radiation, the quality of the vaginal tissues, and medical comorbidities are all factors dictating the type of surgery. For the patient with mild stress incontinence, a well-performed bladder neck suspension will produce a good outcome, but for the patient with multiple failed surgeries, severe incontinence, or incontinence after mesh removal, we will prefer an autologous fascial sling or spiral sling.
2.5 Bladder Neck Suspension (Raz Procedure)
2.5.1 Indications
The bladder neck suspension procedure was designed for the treatment of mild to moderate stress incontinence. The concept is to create a vaginal wall sling. It is not indicated for the patient with multiple failed surgeries and severe incontinence with minimal activity, for the patient after radiation, or in patients with a fixed open urethra. The bladder neck suspension (BNS) is similar to the Burch procedure but is performed transvaginally. The surgery aims at creating a hammock that supports the urethra during changes in intra-abdominal pressure while preventing urethral displacement and allowing proper transmission of abdominal pressures to the urethra and increase in urethral resistance during stress (hammock effect). The anatomical structures involved in the bladder neck suspension include the vaginal wall (excluding the epithelium), the periurethral and perivesical fascia at the level of the bladder neck and urethra, and the urethropelvic fascia that attaches the urethra to the levator muscles (arcus tendineus).
The clinical presentation of stress incontinence depends on the degree of severity of the urethral incompetence. Stress incontinence can manifest as only activity related, or it can be combined with urinary urgency. A history of prior failed surgical procedures, urethral trauma, or irradiation should be noted since a bladder neck suspension is not indicated on these patients. The patient may complain of urinary leakage during straining maneuvers in both the upright and supine positions. On physical examination, different degrees of anterior vaginal wall prolapse can be demonstrated, and stress incontinence can be confirmed during coughing or straining with the patient in the supine or standing position, with leakage demonstrated only at the time of stress. Cystourethroscopy can demonstrate a funneled bladder neck during straining that returns to normal when the stress is relieved. Important preoperative considerations include the degree of anterior vaginal wall prolapse (minimal, moderate, or severe), the degree of incontinence (minimal, moderate, or severe), and other anatomical abnormalities that require concomitant repair, such as uterine prolapse, enterocele, or cystocele.
2.5.2 Preoperative Considerations
A severely shortened and deformed urethra is a contraindication to a vaginal sling procedure. Urethral reconstruction, elongation procedures, and a fascial sling procedure may be better choices in these cases. Another contraindication is senile atrophic vaginitis, as the vaginal wall may not have sufficient integrity and tensile strength to be used as a sling. If recognized early, this problem can be circumvented with the preoperative administration of vaginal estrogen. Radiation or the patients with severe sphincteric damage after mesh removal are not candidates to the procedure.
2.5.3 Surgical Technique
The patient is placed in the dorsal lithotomy position. The lower abdomen and vagina are prepped and draped in a sterile fashion. A Foley catheter is inserted, and the bladder is emptied. A weighted vaginal speculum and a ring retractor with hooks are placed. One dose of prophylactic antibiotics is given.
Figure 2.10 illustrates the anterior vaginal wall, in which two oblique incisions are made in the distal vaginal area.

Fig. 2.10
(a) Two oblique incisions are made in the anterior vaginal wall, extending a few centimeters proximal to the bladder neck. The incision is made 1 cm from the lateral vaginal wall. (b) Two Allis clamps are placed on each side at the apex of the incisions (arrows) for traction and improved exposure
Figure 2.11 depicts the lateral dissection of the vaginal wall over the perivesical fascia to enter the retropubic space. The urethropelvic fascia is detached from the arcus tendineus of the levator muscle, and a window is made in the retropubic space. Any adhesions in the retropubic space are freed using sharp and blunt dissection.

Fig. 2.11
(a, b) To enter the retropubic space, curved scissors are placed parallel to the urethra, under the pubic bone and in an upward direction, abutting the pubic bone at all times
A finger in the retropubic space exposes the lateral edge of the urethropelvic fascia that was detached from the arcus tendineus. This fascia is the only connection of the urethra to the levator muscle (Fig. 2.12).

Fig. 2.12
A finger is placed in the retropubic space, exposing the lateral edge of the urethropelvic ligament
Figure 2.13 demonstrates the placement of the suspension sutures. These sutures incorporate the periurethral fascia at the level of the mid- and proximal urethra and the perivesical fascia at the bladder neck. In a second pass, the free edge of the urethropelvic fascia is included. The suture extends medially to incorporate a large segment of the periurethral fascia. With forceps in the retropubic space, medial retraction of the vaginal incision allows the exposure of the margin of the urethropelvic fascia (Fig. 2.14).

Fig. 2.13
Placement of the bladder neck suspension sutures used to create the suspension

Fig. 2.14
The sutures are initially applied at the level of the bladder neck, incorporating the vaginal wall (excluding the epithelium)
The sutures must incorporate the urethropelvic ligament (Fig. 2.15). Since a bladder neck suspension is not indicated on these patients.

Fig. 2.15
A #0 monofilament nonabsorbable suture is used to incorporate the lateral margin of urethropelvic fascia. Care should be taken not to insert the needle deeply, to avoid penetrating the wall of the bladder or urethra
Medial traction is applied to the vaginal wall, and the perivesical fascia at the bladder neck and the periurethral fascia at the proximal and midurethra are incorporated. The passage is extended medially in order to create a strong hammock of the anterior vaginal wall and the monofilament sutures, acting like a sling under the urethra. The same maneuver is done at least twice and the end traction is applied to the sutures to confirm a strong anchor (Fig. 2.16).

Fig. 2.16
The periurethral and perivesical fasciae are also included
The perivesical and periurethral fascia are incorporated in a similar fashion on the contralateral side. The suture passage is extended medially in order to create a stronger suburethral hammock (Fig. 2.17).

Fig. 2.17
(a, b) The same procedure is performed again on the contralateral side
Traction of the sutures confirms the strong anchor of the vaginal wall and urethropelvic fascia (Fig. 2.18).

Fig. 2.18
By applying traction on the sutures, strong anchoring of the vaginal wall and periurethral tissues is confirmed
A small puncture is performed in the suprapubic area. We perform only a midline puncture to avoid any lateral placement of sutures that can impact the inguinal innervation and cause suprapubic pain (Fig. 2.19).

Fig. 2.19
A small puncture is performed just above the symphysis of the pubic bone. The puncture in the suprapubic abdominal wall is done as close as possible to the upper margin of the pubic bone to prevent suprapubic pain due to traction of the rectus musculature
Under finger control in the retropubic space, a double-pronged needle passer is used to transfer the sutures from the vagina to the suprapubic area. The distance between the tips of the double passer is 1 cm (Fig. 2.20).

Fig. 2.20
A double-pronged ligature carrier (Raz needle passer) is used to transfer each of the Prolene® sutures from the vagina to the suprapubic region. Under finger control, the tips of the passer are transferred from the suprapubic incision to the vaginal incisions
The tips of the suture passer are exposed in the vaginal incision, and the sutures are transferred through the eyes of the needle for a distance of 10 cm to prevent dislodgement during the passage of the passer to the suprapubic area (Fig. 2.21).

Fig. 2.21
The sutures are transferred through the eyes of the needle and retracted to the suprapubic area
The sutures have been transferred to the suprapubic puncture area (Fig. 2.22). The vaginal wall is closed with delayed absorbable sutures and all retraction is removed.

Fig. 2.22
The sutures are transferred to the suprapubic puncture area. The double-pronged carrier will permit the sutures to be tied over a 1-cm segment of the rectus fascia
Cystoscopy is performed to rule out any bladder or urethral injury (Fig. 2.23). Keeping the sheet of the cystoscope in a 45° angulation, each of the sutures is tied individually without tension. Because there is a 1-cm space between the double needles, the tie of the sutures will be supported by the abdominal wall for this distance.

Fig. 2.23
In order to prevent undue tension on the sutures and urinary obstruction from the suspension, the cystoscope is inserted in the bladder and positioned at a 45° angle with the horizontal. The suprapubic sutures are tied individually over the rectus fascia, with the cystoscope sheath in place
2.5.4 Intraoperative Complications
Potential complications at the time of surgery are similar to those of other vaginal procedures and are discussed in another chapter. The most common potential complications are bleeding, urethral or bladder perforation during dissection, and urethral obstruction by the suspension sutures.
2.5.5 Postoperative Care
The procedure can be performed as an outpatient surgery. The vaginal packing is removed 2 h after surgery. The patient is discharged home with a Foley catheter that the patient will remove a few days later. The patient is discharged home after recovering from anesthesia, usually 2–3 h after surgery. Oral antibiotics when indicated, stool softeners, and pain medication are prescribed. There is minimal pain after surgery. Postoperatively, the patient is allowed to engage in normal activities like walking, driving, and performing simple chores. The patient is instructed to avoid high-impact exercise and sexual relations for 1 month.
2.5.6 Postoperative Complications
Risks of any sling procedure include delayed voiding, obstructive urinary symptoms, and even permanent urinary retention, but in our experience, no patient with non-neurogenic urethral incompetence has suffered from permanent retention. De novo overactive bladder without obstruction usually responds to anticholinergic medications. Vaginal shortening is another potential risk, although we have not yet found this to be a problem. Suprapubic wound infections are very rare and may require antibiotics, drainage, or both.
2.6 Distal Urethral Polypropylene Sling (DUPS)
2.6.1 Indications
The distal urethral polypropylene sling (DUPS) procedure for the treatment of stress incontinence is indicated in patients with mild to severe stress incontinence. After distal vaginal incisions are made bilaterally, a tunnel is made in the anterior vaginal wall between the two incisions, 2 cm from the external meatus. A segment of soft polypropylene mesh (10 × 1 cm) is prepared and a #0 delayed absorbable suture is applied at each end. The mesh is transferred through the vaginal tunnel. The sutures will be transferred under finger control in the retropubic space to a small suprapubic puncture. The mesh will be infiltrated by fibrous tissue, providing stability and support to the urethra and anterior vaginal wall during changes in abdominal pressure.
The diagnosis and preoperative considerations are the same as those for bladder neck suspension, discussed previously. We have encountered some patients who present with late complications due to the use of the mesh (erosions, exposure, and pelvic pain) even 7–10 years later. At this time, we will use this procedure very rarely.
2.6.2 Surgical Technique
The patient is placed in the dorsal lithotomy position. The lower abdomen and vagina are prepped and draped in a sterile fashion. If required, the labia are retracted laterally with stay sutures. A Foley catheter is inserted into the urethra, and the bladder is emptied. A weighted vaginal speculum is placed.
Figures 2.24, 2.25, 2.26, 2.27, 2.28, 2.29, 2.30, 2.31, 2.32, 2.33, 2.34, 2.35, 2.36, and 2.37 depict the sequence of steps in the placement of a Prolene® sling. At the end of the procedure, the vaginal wall is closed with multiple absorbable sutures, with extra care not to include the mesh during closure. Vaginal packing soaked in antibiotic cream is inserted in the vagina.

Fig. 2.24
Two oblique incisions are made in the anterior vaginal wall

Fig. 2.25
(a) Allis clamps are used to grasp the anterior vaginal wall just proximal to the urethral meatus for traction. The oblique incision is dissected further to expose the periurethral fascia. (b) The vaginal wall is dissected laterally along the glistening white periurethral fascia toward the ipsilateral shoulder. With a curved scissors parallel to the urethra and pointing superiorly under the inferior pubic bone, the attachment of the urethropelvic fascia to the arcus tendineus fascia pelvis is entered. A small window is made in the retropubic space. The pubic bone can be palpated to confirm proper entrance into the retropubic space. All adhesions from prior surgeries are freed

Fig. 2.26
A segment of soft polypropylene mesh measuring 10 × 1 cm is used. A #0 delayed absorbable suture is passed several times through the end of the sling to provide a strong anchor to the mesh. The mesh is kept soaked in antibiotic solution

Fig. 2.27
Using a right-angle clamp, a tunnel connecting the two incisions is made under the vaginal wall, between the mid- and distal urethra

Fig. 2.28
Using a right-angle clamp, the mesh is transferred beneath the tunnel and positioned at the center of the incisions

Fig. 2.29
A puncture is made in the suprapubic area just above the superior margin of the pubic bone

Fig. 2.30
A hemostatic clamp is used to create a pocket in the suprapubic area down to the rectus fascia, just superior to the symphysis of the pubic bone

Fig. 2.31
The small incision over the suprapubic area is seen

Fig. 2.32
A double-pronged ligature carrier is used to transfer the delayed absorbable sutures (DAS) from the vagina to the suprapubic region. Under finger control, the tips of the passer are transferred from the suprapubic to the vaginal area. Finger guidance in the retropubic space prevents inadvertent penetration of the bladder or urethra

Fig. 2.33
The tips of the double-pronged passer are seen in the vaginal area after being transferred from the suprapubic area

Fig. 2.34
The absorbable sutures are transferred through the eyes of the needle for a distance of 10 cm

Fig. 2.35
The double-pronged passer is pulled up and retracted from the suprapubic area, allowing the retrieval of the sutures. The sutures are seen in the suprapubic wound

Fig. 2.36
Cystourethroscopy is performed to ensure that the bladder and urethra were not inadvertently injured

Fig. 2.37
Two Allis clamps are placed vaginally at each side of the mesh to prevent migration of the sling. The suprapubic delayed absorbable sutures (DAS) are tied individually, and the mesh is kept under slight traction to prevent excessive tensioning of the sling and urethral obstruction
The intraoperative complications and postoperative care are the same as those for bladder neck suspension, discussed previously.
2.6.3 Postoperative Complications
The complications of this procedure are similar to those of other anti-incontinence procedures. The potential for urethral obstruction with this technique may be higher because the mesh may shrink 20–30 % from its original size. The mesh should therefore lie loosely beneath the vaginal wall. Slight countertraction of the sling at the time of the tying of the suprapubic sutures will prevent excessive tensioning of the sling against the urethral wall. With the use of absorbable sutures, the potential for suprapubic infection is nearly eliminated. Infection of the sling or urethral perforation requires removal of the sling.
2.7 Abdominal Autologous Fascial Slings (Pubovaginal Sling)
Three types of autologous fascial sling procedures are described in this chapter: the classic U-shaped pubovaginal sling (Fig. 2.38), the omega shaped fascial sling (Fig. 2.39) and the spiral sling. While our original description of the spiral sling (Fig. 2.40) used mesh we currently have abandoned mesh and use exclusively autologous fascia lata.

Fig. 2.38
Diagram of a U-shaped fascial sling: the fascial segment is placed in a U shape under the urethra. The sling is generally 10–12 cm long and is anchored to a small puncture in the suprapubic area

Fig. 2.39
Diagram of the omega-shaped fascial sling: the fascial strip is crossed in the retropubic space anterior to the urethra

Fig. 2.40
Diagram of the spiral fascial sling: the sling surrounds the urethra in a circular fashion, providing the best possible urethral compression
2.7.1 Indications
The indications for this type of surgery include moderate to severe stress incontinence, failed prior surgeries, incontinence after mesh removal, or refusal of a mesh sling by a patient with stress incontinence. Most times, it is a secondary procedure.
2.7.2 Surgical Technique: Autologous Fascia Pubovaginal Sling
Figures 2.41, 2.42, 2.43, 2.44, 2.45, 2.46, 2.47, 2.48, 2.49, 2.50, 2.51, 2.52, 2.53, 2.54, 2.55, 2.56, and 2.57 illustrate the procedure for placement of a classic, U-shaped pubovaginal sling. For the classic fascial sling, a segment of autologous fascia is retrieved that is 2 cm wide and 10–12 cm in length. The segment of the fascia is usually obtained from the suprapubic area; rarely, it may come from other areas of the abdominal wall. It is not necessary to retrieve a long segment of the fascia, as the cure rate is the same with short segments, therefore diminishing the morbidity after surgery. At the end of the fascial strip, a #1 delayed absorbable suture is applied. The fascial strip is transferred under the tunnel and then passed toward a small suprapubic incision, using a double-pronged suture passer.

Fig. 2.41
The patient is placed in the dorsal lithotomy position. The lower abdomen and vagina are prepped and draped in a sterile fashion. A Foley catheter is inserted into the urethra, and the bladder is emptied. A weighted vaginal speculum is placed and a ring retractor with hooks is used to expose the anterior vaginal wall

Fig. 2.42
Diagram depicting the oblique incisions that are made in the anterior vaginal wall. In a similar maneuver as described for bladder neck suspension surgery, dissection is carried out over the glistening surface of the periurethral fascia. A small window is made in the retropubic space to allow passage of a finger. All adhesions are freed

Fig. 2.43
Using a right-angle clamp, a tunnel is made under the vaginal wall, connecting the two incisions

Fig. 2.44
Exposure of the lower abdomen is seen. The line of incision for fascial retrieval is marked

Fig. 2.45
Suprapubic exposure marking the area of fascial retrieval

Fig. 2.46
The skin and subcutaneous are exposed. Two parallel incisions are made over the anterior abdominal wall fascia, 2 cm apart

Fig. 2.47
A right-angle clamp is used to free underlying adhesions of the fascia to the anterior wall musculature
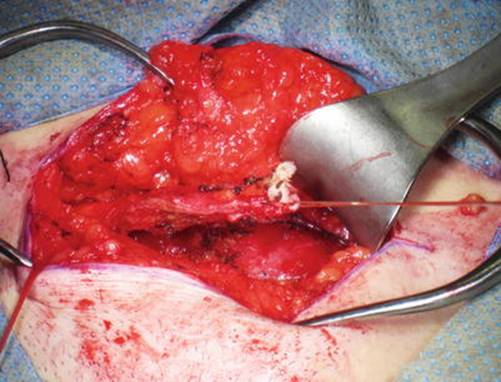
Fig. 2.48
The left side of the fascial strip has been detached from the lateral margin of the incision and multiple passes of a #1 delayed absorbable suture are applied to the end of the fascial strip

Fig. 2.49
The strip of abdominal wall is dissected toward the right side of the incision and freed from the abdominal musculature

Fig. 2.50
The strip of abdominal wall fascia, measuring 2 × 12 cm, with multiple passes of #1 delayed absorbable at the end of the strip

Fig. 2.51
The abdominal wall fascia is closed with multiple figure-of-eight sutures, using #1 delayed absorbable sutures

Fig. 2.52
The sling is transferred under the vaginal tunnel

Fig. 2.53
The fascial strip is anchored to the periurethral fascia on the right side only, to prevent displacement during the tying of the sutures in the suprapubic area

Fig. 2.54
A small suprapubic puncture is performed in the midline, just above the superior margin of the pubic bone. A clamp will be used to dissect a pocket down to the rectus muscle just above the pubic bone

Fig. 2.55
Diagram of the passage of a double-pronged passer (ligature carrier) under finger control in the retropubic space

Fig. 2.56
The double-pronged passer is transferred to the vaginal area. The absorbable sutures at the end of the fascial strip are transferred through the eyes of the passer. The passer is retracted up and removed through the suprapubic incision, bringing with it the sutures attached to the sling. Proper positioning of the sling in the retropubic space must be confirmed, as outlined in the text

Fig. 2.57
After cystoscopy, the anterior vaginal wall is closed with multiple interrupted absorbable sutures
To prevent undue tension on the sutures and urinary obstruction from the suspension, two Allis clamps are used to keep the sling in an horizantal plane while the sutures are tied. We use two Allis clamps the sling can be maintained in an horizontal plane to prevent undo tensioning of the sutures. Once the cystoscope is removed, the urethral Foley catheter is replaced.
2.7.3 Surgical Technique: Omega-Shaped Autologous Fascial Sling
This fascial sling modification is used for patients with severe sphincteric damage with poor coaptation and severe incontinence. Instead of providing a U-shaped sling for urethral compression and support, the omega sling crosses anterior to the urethra (see Fig. 2.39), providing a more extended circular compression to the urethral wall. The technique is similar to the technique for placement of the classic fascial sling, but the difference is in the technique of passage of the fascial strip in the retropubic space (Figs. 2.58, 2.59, 2.60, 2.61, 2.62, 2.63, 2.64, and 2.65). After entering the retropubic space, all adhesions of the bladder and urethra to the posterior aspect of the pubic bone must be completely free in order to allow the crossover of the sling. Two punctures are performed in the suprapubic area. The double passer is transferred from the right suprapubic puncture to the left vaginal incision to capture the sutures attached to the sling. In the left suprapubic puncture, the passer is transferred through the retropubic space to the right vaginal incision, lateral to the urethra. The ends of the sling sutures are transferred to the suprapubic area. In the retropubic space, the sling is crossed anterior to the urethra, forming an omega-shaped compression.

Fig. 2.58
A strip of anterior abdominal wall fascia (2 × 12 cm) is excised. At each end of the fascial strip, we apply #1 delayed absorbable sutures

Fig. 2.59
A tunnel is made under the vaginal wall at the midurethral area

Fig. 2.60
The sling is transferred under the tunnel of the anterior vaginal wall at the midurethral level

Fig. 2.61
Two punctures are performed in the suprapubic area, 10 cm apart. A clamp is used to create a subcutaneous pocket

Fig. 2.62
A finger is inserted in the left vaginal incision and through the retropubic space. A double-pronged passer is inserted in the right suprapubic puncture, and the passer will be transferred under finger control to the left periurethral incision

Fig. 2.63
The tips of the double passer are transferred to the left vaginal incision. The eyes of the needle are seen. The ends of the sling sutures are transferred through the eyes of the double passer for a distance of 10 cm. The same maneuver is performed on the contralateral side, transferring the passer from the left suprapubic puncture to the right vaginal incision. The sutures at the end of the right side of the sling are transferred to the left suprapubic area

Fig. 2.64
The suprapubic area is seen after the sutures have been transferred. The suture in the right puncture anchors the left side of the sling, and the suture in the left puncture anchors the right side of the sling, creating the omega-shaped retropubic compression. The arrows indicate the direction of the double passer and the supporting sutures in the retropubic space

Fig. 2.65
Cystoscopy is performed to rule out any urethral or bladder injury. The suprapubic sutures are tied without tension
In some patients with neurogenic incontinence, the sutures may be tied more tightly, to close an open urethra and create intentional urinary retention.
2.8 Fascia Lata Autologous Fascial Sling
2.8.1 Autologous Fascial Sling Using Fascia Lata
Although most surgeons used abdominal fascia for autologous fascial sling, we strongly prefer an old technique of fascial retrieval from the lateral thigh (iliotibial band of the tensor fascia lata) (Fig. 2.66). The technique is minimally invasive and is particularly useful in obese patients and patients with multiple abdominal surgeries. The tensor fascia lata and the gluteal muscle form a tendinous extension to the tibia called the iliotibial band. This strong tendon of the fascia lata extends lateral to the thigh inserting into the superior lateral tibial bone. A segment of 10–12 cm by 1–2 cm is retrieved, at the end of which we apply #0 or #1 delayed absorbable sutures. A tunnel is made under the vaginal wall and the sling material is transferred under the tunnel. Using a double-pronged passer, the sutures are transferred under finger control in the retropubic space from the vagina to the suprapubic area.

Fig. 2.66
The gluteal and tensor fascia lata muscles form the iliotibial band, the inserts in the lateral aspect of the tibial bone. A lateral view of the knee joint shows the insertion of the iliotibial band into the lateral aspect of the tibial bone. The band is well defined in most patients
2.8.2 Surgical Technique
The first part of the surgery is the retrieval of the fascial segment. The patient is placed in the tort position with elevation of the thigh and knee over a pillow. The inferior part of the lateral thigh and knee is prepared and draped (Fig. 2.67).

Fig. 2.67
The first part of the surgery is the retrieval of the fascial segment. The patient is placed in the tort position with elevation of the thigh and knee over a pillow. The inferior part of the lateral thigh and knee is prepared and draped
A horizontal incision is made on the lateral thigh 8–10 cm above the knee joint. Dissection is carried out of the subcutaneous tissues to expose the tendineus segment of the fascia lata (iliotibial band). The fascia is in general thick and different from the rest of the fascia covering the lateral musculature. The proper segment should be selected. Two parallel incisions are made 1–2 cm apart (Fig. 2.68).

Fig. 2.68
A vertical is made on the lateral thigh 3–4 cm above the knee joint. Dissection is carried out of the subcutaneous tissues to expose the tendineus segment of the fascia lata muscle. The fascia is in general thick and different from the rest of the fascia covering the lateral musculature. The proper segment should be selected. Two parallel incisions are made 1–2 cm apart
A right-angle clamp is used to isolate the strip of the fascia from the underlying musculature (Fig. 2.69).

Fig. 2.69
A right-angle clamp is used to isolate the strip of fascia from the underlying musculature
The fascia is transected inferiorly and #1 delayed absorbable sutures are applied to the free end of the fascial strip. Multiple passes of the needle are required to obtain a strong anchoring effect (Fig. 2.70).

Fig. 2.70
The fascia is transected inferiorly and #1 delayed absorbable sutures are applied to the free end of the fascial strip. Multiple passes of the needle are required to obtain a strong anchoring effect
Sharp and blunt dissection is used superior to the fascia to separate the fascia from the subcutaneous tissues for a distance of 10 cm. The fascia is also dissected sharply and bluntly from the underlying lateral musculature to facilitate the fascial incision (Fig. 2.71).

Fig. 2.71
Sharp and blunt dissection is used superior to the fascia to separate the fascia from the subcutaneous tissues for a distance of 10 cm. The fascia is also dissected sharply and bluntly from the underlying lateral musculature to facilitate the fascial incision
The Crawford fascial stripper is used. The device consists of two sliding elements with a rotational circular plate (arrow) that prevents the advancement of the cutting blade. The inner segment contains a cutting blade that transects the fascial strip when activated (Fig. 2.72).

Fig. 2.72
The Crawford fascial stripper is used. The device consists of two sliding elements with a circular plate (arrow) that prevents the advancement of the cutting blade. The inner segment contains a cutting blade that will transect the fascial strip when activated
The inner segment is retracted to show the cutting blade (arrow). Advancement of this segment will transect the sling at the desired point (Fig. 2.73).

Fig. 2.73
Close view of the distal segment of the fascial stripper. The inner segment is retracted to show the cutting blade (arrow). Advancement of this segment will transect the sling at the desired point
The sutures applied at the end of the fascia are transferred through the tip of the fascial stripper, and the end of the fascia will also be transferred for a distance of 4–5 cm (Fig. 2.74).

Fig. 2.74
The sutures applied at the end of fascia are transferred through the tip of the fascial stripper, and the end of the fascia will also be transferred for a distance of 4–5 cm
A clamp is applied to the end of the fascial segment to provide countertraction at the time of the advancement of the stripper (Fig. 2.75).

Fig. 2.75
A clamp is applied to the end of the fascial segment to provide countertraction at the time of the advancement of the stripper
The stripper is advanced in the subcutaneous tissues in the direction of the fascia lata fibers for the desired distance, in general 10–12 cm. The device is activated. The fascial strip is transected and retrieved from the incision (Fig. 2.76).

Fig. 2.76
The stripper is advanced in the subcutaneous tissues in the direction of the fascia lata fibers for the desired distance, in general 10–12 cm. The device is activated. The fascial strip is transected and retrieved from the incision
The fascial strip is removed and another #1 delayed absorbable suture is applied to the free end. The fascia lata segment is placed in antibiotic solution. The wound is closed in two layers of #2-0 delayed absorbable sutures in the subcutaneous and #4-0 in the skin (Fig. 2.77).

Fig. 2.77
The fascial strip is removed and another #1 delayed absorbable suture is applied to the free end. The fascia lata segment is placed in antibiotic solution. The wound is closed in two layers of #2-0 delayed absorbable sutures in the subcutaneous and #4-0 in the skin
Pneumatic stocking is applied to the lower extremities, the patient is placed in lithotomy position, and the vaginal wall is prepared and draped.
Exposure of the anterior vaginal wall is obtained after insertion of a Foley catheter (Fig. 2.78).

Fig. 2.78
Exposure of the anterior vaginal wall is obtained after insertion of a Foley catheter
Two oblique incisions are made in the distal lateral vagina. The retropubic is entered in each side and all adhesions are freed. A tunnel is made under the vaginal wall, 2 cm from the external meatus (Fig. 2.79).

Fig. 2.79
Two oblique incisions are made in the distal lateral vagina. The retropubic is entered in each side and all adhesions are freed. A tunnel is made under the vaginal wall, 2 cm from the external meatus
The strip of fascia is transferred under the tunnel. A delayed absorbable suture is applied to the periurethral fascia and the fascial sling in one side, to prevent displacement (Fig. 2.80).

Fig. 2.80
A small incision is made in the suprapubic area. Using a double-pronged passer, under finger control in the retropubic space, the sutures are transferred from the vagina to the suprapubic puncture area
A small incision is made in the suprapubic area. Using a double-pronged passer, under finger control in the retropubic space, the sutures are transferred from the vagina to the suprapubic puncture area (Fig. 2.81).

Fig. 2.81
The anterior vaginal wall is closed with interrupted figure-of-eight sutures
The anterior vaginal wall is closed with interrupted figure-of-eight sutures after the cystoscopy and the tying of the sprapubic sutures (Fig. 2.82).

Fig. 2.82
After the cystoscopy, the sheet of the cystoscope is kept in a 45° angulation and the suprapubic sutures are tied without tension. A vaginal packing soaked with antibiotics will be inserted in the vagina. The patient is discharged home the same day or after 24-h observation
After the cystoscopy, cystocopy is performed to rule out intravesical lesions. Two Allis clamps are kept the horizontal plane and the suprapubic sutures tied without tension (Fig. 2.83).

Fig. 2.83
Diagram of the exposure of the anterior vaginal wall, with two oblique incisions in the distal vagina
A vaginal packing soaked with antibiotics will be inserted in the vagina. The patient is discharged home the same day or after a 24-h observation.
2.8.3 Postoperative Care
This is similar to other sling procedures.
2.9 Spiral Slings
2.9.1 Indications-Surgical Technique
The spiral sling procedure is designed for the treatment of patients with severe stress incontinence. The patient is placed in the dorsal lithotomy position. The lower abdomen and vagina are prepped and draped in a sterile fashion. If required the labia are retracted laterally with stay sutures. A Foley catheter is inserted into the urethra and the bladder is emptied. A weighted vaginal speculum and a ring retractor with hooks are used (Figs. 2.84, 2.85, 2.86, 2.87, 2.88, 2.89, 2.90, 2.91, 2.92, 2.93, and 2.94). After distal vaginal incisions are made bilaterally, a tunnel is made in the anterior vaginal wall between the two incisions, 2 cm from the external meatus. A complete urethrolysis is performed, and all adhesions of the urethra and bladder to the posterior aspect of the pubic bone are freed. A segment of 15 × 1 cm of fascia lata segment is prepared and, at each end, a #1 delayed absorbable suture is applied. A Derra or other sharp angulated clamp is inserted into the retropubic space in one side of the vaginal incision and brought to the contralateral incision. The graft is transferred through the retropubic space. A right-angle clamp is passed under the vaginal tunnel from the left to the right side of the vaginal tunnel, and the end of the fascial strip is transferred to the left side of the vaginal incision. From the right side, the mesh is transferred from the left side of the vaginal incision to the right. On completion of the transfer, we have created a complete circle around the urethra. The sutures at the end of the fascial strip will be transferred to the suprapubic area and tied after a cystoscopy has been performed.

Fig. 2.84
Two oblique incisions are made in the anterior vaginal wall. The retropubic space is entered and all adhesions of the bladder and urethra are freed

Fig. 2.85
A curved clamp is seen lateral to the vaginal incision

Fig. 2.86
Under finger control in the retropubic space just anterior and distal to the urethra, the clamp is transferred through the retropubic space from the left vaginal incision to the right side

Fig. 2.87
(a) A 15 × 1 cm segment of fascia lata is prepared. At each end, a #1 delayed absorbable suture is applied. (b) The fascia is transferred through the retropubic space between the urethra and the pubic bone

Fig. 2.88
A tunnel is made under the vaginal wall at the midurethral level

Fig. 2.89
The right side of the fascia is transferred under the vaginal tunnel to the left side

Fig. 2.90
The left side of the fascial segment will be transferred to the right side of the tunnel

Fig. 2.91
Both ends of the fascial segment have been transferred, completing the circle around the urethra

Fig. 2.92
A small suprapubic puncture is performed. A double-pronged passer is transferred, under finger control in the retropubic space, from the suprapubic to the vaginal area

Fig. 2.93
The absorbable sutures are transferred through the needle holes of the passer for a distance of 10 cm. The passer is pulled to the suprapubic area, carrying the delayed absorbable sutures

Fig. 2.94
(a) The suprapubic incision and sutures are seen. (b) Cystoscopy will be performed, the sutures will be tied using two Allis clamps to keep the sling in an horizontal plane and the anterior vaginal wall will be closed with several delayed absorbable sutures
2.9.2 Surgical Technique
A vaginal packing soak with antibiotics will be inserted.
2.9.3 Postoperative Complications
The complications are similar to those of other anti-incontinence procedures. The use of this technique in patients with significant sphincteric damage increases the potential for temporary obstruction. Attention should be paid to tie the suprapubic sutures loosely. Light countertraction of the sling at the time of suprapubic suture tying will prevent excessive tensioning of the sling against the urethral wall. In case of urinary retention, the patient is instructed on self-catheterization. If retention continues after 6–8 weeks, a limited sling incision may be required.
Suggested Reading
Agur W, Riad M, Secco S, Litman H, Madhuvrata P, Novara G, et al. Surgical treatment of recurrent stress urinary incontinence in women: a systematic review and meta-analysis of randomized controlled trials. Eur Urol. 2013;64(2):323–36.CrossRefPubMed
Albo ME, Richter HE, Brubaker L, Norton P, Kraus SR, Zimmern PE, Urinary Incontinence Treatment Network, et al. Burch colposuspension versus fascial sling to reduce urinary stress incontinence. N Engl J Med. 2007;356:2143–55.CrossRefPubMed
Banakhar MA, Al-Shaiji TF, Hassouna MM. Pathophysiology of overactive bladder. Int Urogynecol J. 2012;23:975–82.CrossRefPubMed
Brubaker L, Richter HE, Norton PA, Albo M, Zyczynski HM, Chai TC, Urinary Incontinence Treatment Network, et al. 5-year continence rates, satisfaction and adverse events of burch urethropexy and fascial sling surgery for urinary incontinence. J Urol. 2012;187(4):1324–30.CrossRefPubMedPubMedCentral
Chapple CR, Monassero F. Pathophysiology of stress incontinence. In: Raz S, Rodriguez L, editors. Female urology. 3rd ed. Philadelphia: Saunders-Elsevier; 2008. p. 301.CrossRef
Committee Opinion No. 603: Evaluation of uncomplicated stress urinary incontinence in women before surgical treatment. Obstet Gynecol. 2014;123(6):1403–7.
Delancey J. What causes stress incontinence: fallacies, fascias and facts. Can Urol Assoc J. 2012;6(5 Suppl 2):S114–5.PubMedPubMedCentral
deTayrac R, Deffieux X, Droupy S, Chauveaud-Lambling A, Calvanèse-Benamour L, Fernandez H. A prospective randomized trial comparing tension-free vaginal tape and transobturator suburethral tape for surgical treatment of stress urinary incontinence. Am J Obstet Gynecol. 2004;190:602–8.CrossRefPubMed
Glazener CM, Cooper K. Bladder neck needle suspension for urinary incontinence in women. Cochrane Database Syst Rev. 2014;(12):CD003636. doi:10.1002/14651858.CD003636.pub3.
Leach GE, Dmochowski RR, Appell RA, Blaivas JG, Hadley HR, Luber KM, et al. Female Stress Urinary Incontinence Clinical Guidelines Panel summary report on surgical management of female stress urinary incontinence. The American Urological Association. J Urol. 1997;158:875–80.CrossRefPubMed
Mansoor A, Vedrine N, Darcq C. Surgery of female urinary incontinence using trans-obturator tape (TOT): a prospective randomized comparative study with TVT. Neurourol Urodyn. 2003;22:488–9.
Nambiar A, Cody JD, Jeffery ST. Single-incision sling operations for urinary incontinence in women. Cochrane Database Syst Rev. 2014;(6):CD008709. doi:10.1002/14651858.CD008709.pub2.
Nilsson C, Falconer C, Rezapour M. Seven-year follow-up of the tension- free vaginal tape procedure for treatment of urinary incontinence. Obstet Gynecol. 2004;104:1259–62.CrossRefPubMed
Petros P, Ulmsten U. An integral theory and its method for the diagnosis and management of female urinary incontinence. Scand J Urol Nephrol Suppl. 1993;153:1–93.PubMed
Porena M, Constantini E, Frea B, et al. Tension-free vaginal tape versus transobturator tape as surgery for stress urinary incontinence: results of a multicentre randomized trial. Eur Urol. 2007;52:1481–91.CrossRefPubMed
Rehman H, Bezerra CC, Bruschini H, Cody JD. Traditional suburethral sling operations for urinary incontinence in women. Cochrane Database Syst Rev. 2011;(1):CD001754. doi:10.1002/14651858.CD001754.pub3.
Rodriguez LV, Raz S. Polypropylene sling for the treatment of stress urinary incontinence. Urology. 2001;58:783–5.CrossRefPubMed
Tamussino KF, Hanzal E, Kölle D, Ralph G, Riss PA, Austrian Urogynecology Working Group. Tension-free vaginal tape operation: results of the Austrian registry. Obstet Gynecol. 2001;98:732–6.PubMed
Thor KB, de Groat WC. Neural control of the female urethral and anal rhabdosphincters and pelvic floor muscles. Am J Physiol Regul Integr Comp Physiol. 2010;299(2):R416–38.CrossRefPubMedPubMedCentral
Ward K, Hilton P. Tension-free vaginal tape versus colposuspension for primary urodynamic stress incontinence: 5-year follow-up. Br J Obstet Gynaecol. 2008;115:226–33.CrossRef