Derek T. Woodrum
David W. Healy
Presentation
A 65-year-old woman is brought to the emergency department as a level I trauma after being thrown from a horse. At the scene, emergency responders placed the patient in a cervical collar and administered high-flow oxygen via face mask. In the emergency department, her pulse-oximetry saturation is 92% and she has partially obstructed (snoring, noisy) breathing. Due to hypotension and a focused abdominal sonogram positive for free fluid, she is taken directly to the operating room for an exploratory laparotomy. Intravenous and arterial access are already in place.
After rapid sequence induction of anesthesia in the operating room, direct laryngoscopy is performed with in-line cervical stabilization and cricoid pressure after removing the anterior portion of the cervical spine collar. The laryngoscopist is unable to visualize the vocal cords or pass an endotracheal tube into the trachea. The saturations begin to fall into the 80s.
Discussion
An airway emergency is one of the most critical, time-sensitive situations encountered by surgeons and anesthesiologists. This case occurred in the operating room in a “controlled” setting, but a surgeon will very likely be involved in many cases involving airway management during their careers. Smaller hospitals may not have in-hospital 24-hour anesthesia services, and emergency airway management may fall to the surgical team. Even when a full complement of help is available, the surgical team may be the first responder to an airway emergency on rounds, in the trauma bay, or in offsite locations like radiology or in burn debridement rooms. Finally, the surgical team will occasionally be called upon for a surgical airway in the operating room, in settings of trauma or impossible ventilation/impossible intubation.
The purpose of this chapter is to highlight salient points when approaching an airway emergency. It is crucial that the physician has a previously thought-out and well-understood approach to airway management. We discuss preinduction airway evaluation, rapid sequence induction for standard intubation, and what to do when intubation is unsuccessful. Surgical airway management is also reviewed.
Differential Diagnosis
This patient’s hypoxia is likely caused by several factors including hypoventilation from partial airway obstruction, depressed mental status, and opioid administration. Other factors need consideration, including pulmonary contusion, aspiration, pneumothorax or hemothorax associated with rib fractures, depressed cardiac output from cardiac contusion, tamponade, or aortic dissection.
Workup
In an airway emergency, there is very little time for additional workup. A preexisting chest radiograph can diagnose pneumothorax, hemothorax, or widened mediastinum—but the main focus should be on the airway exam. The goal in an urgent situation is to maintain oxygenation while simultaneously identifying predictors of difficult ventilation and intubation. This risk stratification will help guide immediate and subsequent airway management. If a patient is hypoxemic with little or no ventilatory effort, the airway should be supported by chin lift with or without an oral pharyngeal airway while oxygen is applied.
The airway exam is performed to specifically aid in the prediction of three situations: difficult mask ventilation, difficult intubation, and difficult surgical airway. Table 1 lists risk factors for difficulty with each of these three procedures. The ability to mask ventilate is supremely important in maintaining gas exchange and in saving a patient’s life. It may be continued for some time if intubation is unsuccessful. Figure 1 illustrates the Mallampati scoring system, which is a description of how much of the oropharynx can be visualized. A Class III (no visualization of the uvula but the soft palate can be seen) or Class IV (even the soft palate cannot be visualized) Mallampati score alerts to the likelihood of both difficult mask ventilation and intubation with direct laryngoscopy. Alternative airway devices and airway expert consultation should be obtained immediately.
TABLE 1. Risk Factors for Difficult Mask Ventilation, Difficult Intubation, and Difficult Cricothyroidotomy

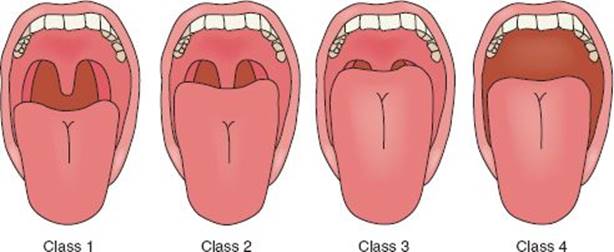
FIGURE 1 • Mallampati score.
The recommended brief airway exam in the emergency setting includes assessment of mouth opening, Mallampati class, and mandibular protrusion (ability to extend the lower teeth anterior to the upper teeth). Presence or absence of teeth is noted, and neck mobility—particularly extension—is assessed if the patient has a cleared cervical spine.
Rapid Sequence Induction
After the airway exam is completed and urgent calls for assistance are made, preoxygenation is performed prior to induction of anesthesia. This is best carried out utilizing a nonrebreathing mask with collapsible air reservoir. In a patient breathing spontaneously, an Ambu bag is not ideal for preoxygenation as it is difficult to draw oxygen from the self-expanding bag. If the airway is partially obstructed but respiratory effort is present, a jaw thrust/chin lift maneuver should be performed. After preoxygenation and application of cricoid pressure, general anesthesia should be induced to optimize intubating conditions. Table 2 lists the common emergency induction agents and muscle relaxants. The comparative advantages and disadvantages are outside the scope of this chapter, but etomidate is used frequently for its property of hemodynamic stability on induction. The use of succinylcholine or rocuronium in the doses listed will provide optimal intubating conditions within 60 seconds. Contraindications to succinylcholine are listed below. Due to these contraindications, rocuronium is frequently used in rapid sequence induction of anesthesia. It will provide approximately 30 to 45 minutes of muscle relaxation. However, the patient will not return to spontaneous ventilation in that time; waking the patient up if intubation is not successful will not be an option.
TABLE 2. Common Emergency Induction Agents and Muscle Relaxants
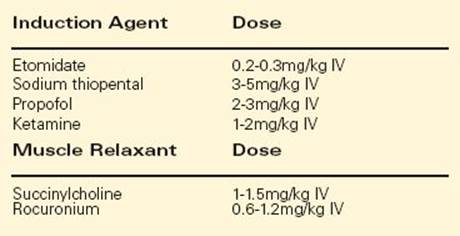
Succinylcholine is a widely used and relatively safe muscle relaxant, but the potential complications should be known. Any provider administering it must be familiar with the absolute contraindications and avoid its use in patients with burns, hyperkalemia, upper motor neuron lesions, neuromuscular disorders, and those with a personal or family history of malignant hyperthermia.
Unable to Ventilate
In the case scenario of this chapter, intubation was not successful after rapid sequence induction and direct laryngoscopy. In this situation, a well thought-out backup plan must be readily instituted. Figure 2illustrates a flow diagram of how to manage an unsuccessful intubation. It is a modification of the American Society of Anesthesiologist’s Difficult Airway Algorithm, focusing on the goals of maintaining gas exchange and oxygen saturation as the airway is managed. Key points are noted in the text following the flow chart.
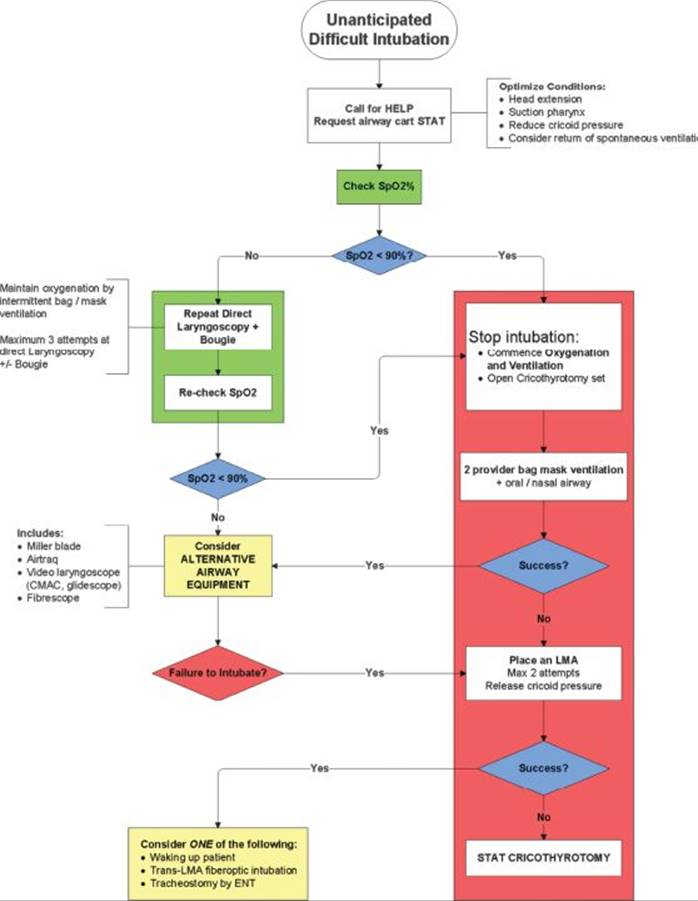
FIGURE 2 • Flow diagram for managing an unsuccessful intubation.
1. If the initial intubation attempt is unsuccessful, the pulse-ox reading should be noted while optimizing intubation conditions for subsequent attempts. If the saturation is already dropping below 90%, further intubation attempts should not be attempted.
2. Oxygenation and ventilation with bag mask should be attempted immediately, while calling for a surgical airway kit and preparing for surgical airway. A surgical airway is not the next step, but parallel preparations should be made.
3. If the bag-mask ventilation is successful, the patient is “re”preoxygenated before subsequent attempts at intubation utilizing alternate airway techniques by an airway expert familiar with alternate devices.
4. If bag-mask ventilation is unsuccessful, a laryngeal mask airway (LMA) should be placed. If LMA placement is successful and ventilation through the LMA is adequate, an airway expert may then consider trans-LMA intubating techniques.
5. If LMA placement is unsuccessful, or inadequate at providing effective oxygenation, a surgical airway should be promptly established (see below).
Of critical importance is the immediate call for help from experienced providers if the initial attempt at intubation is unsuccessful. The goal is oxygenation and gas exchange, and this should be accomplished with bag-mask ventilation if intubation is not successful. We recommend against the use of advanced alternative airway devices (video laryngoscope, intubating supraglottic airways, fiberoptic intubations, etc.) by inexperienced providers. Just as an anesthesiologist is unlikely to safely perform an appendectomy (even after observing the procedure hundreds of times), it is unlikely that a surgical team member will be successful in using advanced, alternative airway devices in a critical situation. The strong focus should remain on oxygen delivery and airway patency—this is the reason for LMA placement if intubation and bag-mask ventilation are unsuccessful.
Surgical Approach
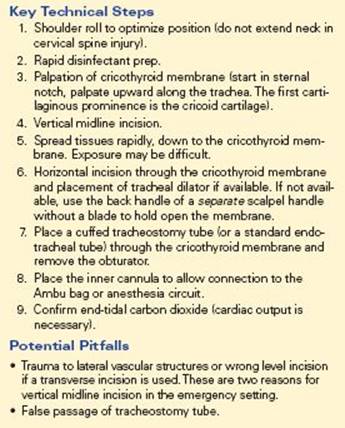
If intubation is unsuccessful and mask ventilation is inadequate to permit additional attempts by alternate airway methods, a surgical airway should be performed without delay. Two methods are commonly employed: kit-based wire-guided cricothyroidotomy (Figure 3 and Table 3) and open cricothyroidotomy (Table 4). Wire-guided technique utilizing a Melker cricothyrotomy kit is very common and is widely available. Benefits to the kit-based technique include wide availability, provider familiarity, and rapid placement. The open approach may take longer to perform and involves more dissection time.
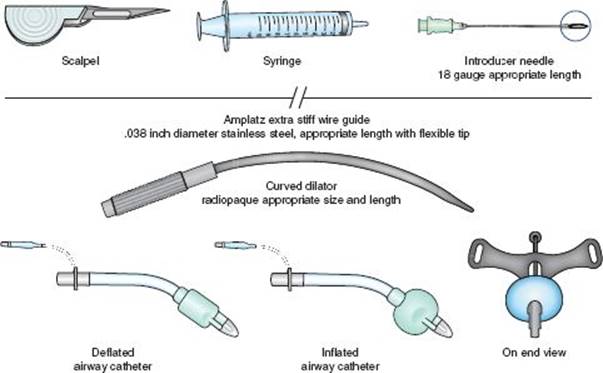
FIGURE 3 • Melker cricothyrotomy kit.
TABLE 3. Steps When Using the Melker Cricothyrotomy Kit
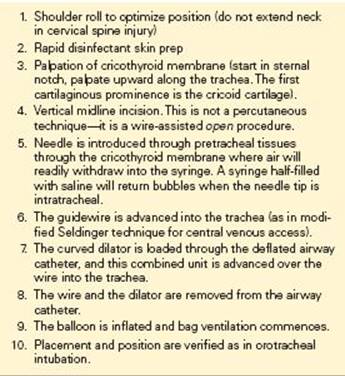
TABLE 4. Key Technical Steps and Potential Pitfalls in Open Cricothyroidotomy
Postoperative Management
After establishing a definitive airway—that is, a cuffed tube in the trachea—placement is confirmed by listening for bilateral breath sounds and checking for return of end-tidal CO2. The latter is accomplished either by observing color change on an in-line device, or by return of CO2 to a gas analyzer on an anesthesia machine. However, blood must be flowing to the lungs in order for CO2 delivery. In the setting of very low cardiac output (exsanguination, massive MI, or PE) or in cardiac arrest without CPR, CO2 will not be detected even if the airway is correctly positioned. Pulse oximetry and arterial blood gas sampling are used in an adjunctive manner. A chest x-ray (CXR) should be ordered to confirm position and to check for adequate inflation of all lung lobes (an emergency operation should not be delayed for a CXR, of course).
TAKE HOME POINTS
· Immediate consultation with an airway management expert gives the greatest chance for successful outcome in emergency airway management.
· Rapid sequence induction followed by direct laryngoscopy (accompanied by in-line cervical stabilization if cervical spine stability is uncertain) is the current standard of care.
· An understanding of the failed airway algorithm (memorized!) is crucial for logical, safe, and sequential handling of the emergency airway.
· Alternative airway devices beyond a standard LMA require previous experience for successful placement. Their use is not recommended in an emergency without prior familiarity.
SUGGESTED READINGS
Hung O, Murphy M. Context sensitive airway management. Anesth Analg. 2010;110(4):982–983.
Kheterpal S, et al. Incidence and predictors of difficult and impossible mask ventilation. Anesthesiology. 2006;105(5):885–891.
Melker JS, Gabrielli A. Melker cricothyrotomy kit: an alternative to the surgical technique. Ann Otol Rhinol Laryngol. 2005;114(7):525–528.
Melker kit video. http://www.cookmedical.com/cc/resources.do?id=4813. Accessed 10/1/2010.