Tyler Grenda
Jules Lin
Presentation
A 48-year-old male with an unremarkable past medical history presents to his primary care physician with a chief complaint of difficulty swallowing. He describes symptoms of progressive dysphagia to both solids and liquids over several years. He regurgitates undigested food daily and has lost 20 lbs over the past 9 months. He occasionally regurgitates when lying down at night and sometimes wakes up coughing. He denies any nausea, chest, or abdominal pain. His vital signs and physical examination are otherwise unremarkable.
Differential Diagnosis
There are several possible etiologies for this patient’s progressive dysphagia. Painless dysphagia to both solids and liquids with regurgitation of undigested food is suggestive of achalasia. However, pseudoachalasia, with obstruction secondary to a neoplasm in the distal esophagus or extraluminal compression, can present in the same manner and must be considered in the differential. Upper endoscopy is essential to evaluate for a tumor, stricture, or other esophageal or gastric pathology as the cause of his symptoms. The differential includes esophageal dysmotility, esophageal spasm, a peptic stricture, and Zenker’s or epiphrenic diverticulum. Diffuse esophageal spasm results in simultaneous, frequent contractions. However, relaxation of the lower esophageal sphincter (LES) is normal, and patients complain more frequently of chest pain. Surgery is not indicated and is unlikely to resolve the patient’s symptoms. Chagas’ disease is clinically identical to achalasia but is caused by the parasite Trypanosoma cruzi,which destroys the myenteric plexus, and is common in South America.
Workup
The patient underwent a barium swallow, which reveals a dilated esophagus with a “bird’s beak” narrowing at the gastroesophageal junction (Figure 1A). An upper endoscopy is performed, which shows no evidence of a mass or stricture. The esophagus is dilated with retained fluid and food debris. The LES is tight with mild resistance when passing the endoscope. Laboratory values are obtained and are within normal limits. He also undergoes an esophageal manometry, which reveals an aperistaltic esophageal body with incomplete or absent relaxation of the LES on all wet swallows (WS) (Figures 2 and 3).

FIGURE 1 • On barium esophagram (A), the distal esophagus is aperistaltic and mildly dilated. There is a bird’s beak narrowing at the gastroesophageal junction with significant hold-up of contrast consistent with achalasia. Postoperative barium swallow (B) shows no leak and easy passage of contrast through the gastroesophageal junction.

FIGURE 2 • Traditional esophageal manometry (A) and high-resolution manometry (B) show normal peristalsis and relaxation of the lower esophageal sphincter (LES) with each wet swallow (WS). UES, upper esophageal sphincter. (From Jee SR, et al. A high-resolution view of achalasia. J Clin Gastroenterol. 2009;43(7): 646.)

FIGURE 3 • Esophageal manometry (A) and high-resolution manometry (B) show aperistalsis of the esophageal body on all wet swallows (WS) with no relaxation of the lower esophageal sphincter (LES). UES, upper esophageal sphincter.
Discussion
Achalasia is a primary esophageal motility disorder of unknown etiology that is characterized by an aperistaltic esophagus and a LES that fails to relax in response to swallowing. Due to neural degeneration from the dorsal motor nucleus to the myenteric plexus, vagal innervation is lost. Achalasia affects approximately 1 per 100,000 people in the United States and typically presents between the ages of 20 and 50, although it may present at any age. Failure of the LES to relax results in a functional obstruction at the level of the gastroesophageal junction.
Diagnosis and Treatment
Upper endoscopy must be performed to evaluate for pseudoachalasia caused by an esophageal carcinoma or a peptic stricture. Chest CT can also be useful to evaluate for extrinsic compression. A chest radiograph can suggest the diagnosis of achalasia with absence of a gastric air bubble or a dilated esophagus. The diagnosis is often confirmed on a barium swallow showing a dilated esophagus with an air-fluid level and narrowing of the gastroesophageal junction giving the classic “bird’s beak” appearance (Figure 1A). Manometry is an important tool in the diagnosis of achalasia and shows an aperistaltic esophagus and a LES that fails to relax with swallowing (Figure 3). Given the findings present in this patient’s workup, his symptoms are most likely secondary to achalasia.
The primary goal of treatment is palliation of the patient’s symptoms by alleviating the distal esophageal obstruction present at the LES. None of the available treatments will return the esophagus to normal, and the esophageal body remains aperistaltic. In addition, a careful balance must be achieved between alleviating the Obstruction And Creating Gastroesophageal reflux.
Pharmacologic therapies, such as calcium channel blockers and nitrates, cause smooth muscle relaxation and decrease LES pressure. The effectiveness of these treatments is short-lived and often causes significant side effects. As a result, these should be reserved for temporizing therapy and for patients that are poor surgical candidates.
Endoscopic injection of botulinum toxin (Botox) into the LES relaxes the smooth muscle fibers. While this treatment can improve dysphagia, its effects often last <6 months and require repeat injections for continued relief of symptoms. Botox injections can also cause an inflammatory reaction, which can make a future myotomy more difficult. Therefore, Botox should be reserved for individuals that are poor candidates for endoscopy or surgery.
Pneumatic dilation disrupts the smooth muscle fibers of the LES and is successful in relieving dysphagia in 60% to 75% of patients after a single dilation and in up to 85% after multiple dilations. The risk of perforation associated with this procedure is approximately 3% to 5%. It is typically considered to be less effective in younger patients. Pneumatic dilation should be reserved for patients that are unable to undergo a laparoscopic esophageal myotomy.
Myotomy is the treatment of choice, particularly in patients younger than 40 years. Given this patient’s degree of symptoms, findings consistent with achalasia, and limited comorbidities, a laparoscopic esophageal (Heller) myotomy with a Dor fundoplication would be the most appropriate treatment. While esophageal myotomy was performed through a thoracotomy or laparotomy in the past, it is now most commonly performed laparoscopically since the angle for the myotomy is easier and allows the addition of a fundoplication to prevent reflux. Laparoscopic myotomy relieves symptoms in 90% of patients and is more effective in providing prolonged symptom relief than endoscopic therapy with a low morbidity (6.3%) and mortality (0.1%). A partial fundoplication should be performed at the time of myotomy to reduce the incidence of gastroesophageal reflux (8.8% vs. 31.5%).
Since the esophagus remains aperistaltic, patients with a megaesophagus or a sigmoid esophagus with significant tortuosity or angulation (Figure 4) will continue to have poor emptying despite a myotomy and should undergo a transhiatal esophagectomy. In addition, patients who have had a previous myotomy should undergo esophagectomy unless there is concern that the previous myotomy was incomplete.

FIGURE 4 • Barium esophagram demonstrates end-stage achalasia with a grossly dilated megaesophagus up to 12 cm with minimal flow through the gastroesophageal junction 20 years after a previous esophageal myotomy.
Surgical Approach
The patient is restricted to a clear liquid diet for 2 days prior to the operation. Since the dilated esophagus may contain large amounts of fluid and retained food, decompression with a nasogastric tube prior to induction of general anesthesia is critical to prevent aspiration. The patient is then placed in the supine position. A camera port is placed above the umbilicus, and pneumoperitoneum is established to 15 mm Hg. Four additional ports are placed under direct vision with two 5-mm working ports in the epigastrium. A 5-mm port is placed laterally on the right for the liver retractor and a 5-mm port in the left abdomen to retract the stomach. The gastrohepatic ligament is opened, and the right crus is identified. The anterior aspect of the esophagus is bluntly dissected while the posterior planes are left intact unless there is a hiatal hernia.
The gastroesophageal fat pad is removed exposing the gastroesophageal junction. Care is taken to identify and preserve the anterior vagus nerve. The myotomy is started just above the gastroesophageal junction using the hook cautery. The longitudinal and circular muscle fibers are divided 6 cm onto the esophagus and 2 cm onto the stomach. The edges of the myotomy are bluntly separated from the mucosa for half of the esophageal circumference. The integrity of the esophageal mucosa is then tested with insufflation through the endoscope with the myotomy submerged under water. The location of the gastroesophageal junction is confirmed endoscopically to ensure that the myotomy extends at least 2 cm onto the stomach.
An anterior (Dor) or a posterior (Toupet) fundoplication is then performed after the myotomy is completed. The Dor fundoplication has the added benefit of buttressing the myotomy site and is constructed by placing two sutures on either side of the hiatus passing through the fundus, the divided esophageal muscle, and the crus.
Special Considerations
In separating the muscle fibers from the underlying mucosa, an esophageal perforation may occur particularly if there is scarring from previous Botox treatments. The procedure should be converted to a laparotomy if the surgeon is not facile at intracorporeal suturing. The mucosal perforation should be repaired with a 4-0 absorbable suture and the overlying myotomy closed with interrupted sutures to buttress the repair. A myotomy should then be performed on the contralateral aspect of the esophagus.
Postoperative Management
On postoperative day 1, an esophagram is obtained to evaluate for perforation (Figure 1B). If no evidence of perforation is present, a clear liquid diet is started, and the patient is discharged home. Patients are typically advanced to a mechanical soft diet, which is maintained for 3 weeks, on postoperative day 3. Mild recurrent symptoms of dysphagia, heartburn, and regurgitation may occur in up to 40% to 50% of patients. However, few of these patients will require additional intervention other than initiation of a proton pump inhibitor or dietary modifications.
Case Conclusion
The patient successfully underwent a laparoscopic Heller myotomy with a Dor fundoplication. On postoperative day 1, his esophagram showed no evidence of leak with significant improvement in esophageal emptying. He is advanced to a clear liquid diet and discharged home. At his 6-month follow-up appointment, he is tolerating a regular diet without any symptoms of dysphagia or heartburn (Table 1).
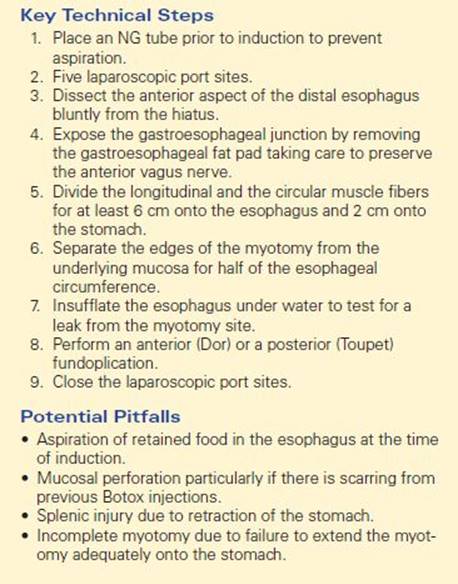
TABLE 1. Key Technical Steps and Potential Pitfalls to a Laparoscopic Heller Myotomy with a Dor Fundoplication
TAKE HOME POINTS
· Pseudoachalasia due to a carcinoma must be ruled out by upper endoscopy in a patient that presents with progressive dysphagia.
· Typical findings on esophageal manometry include an aperistaltic esophageal body with absent or incomplete relaxation of the LES.
· Botulinum toxin injection and pneumatic dilation are typically reserved for patients who are poor surgical candidates.
· Laparoscopic Heller myotomy is the standard surgical therapy for achalasia and is combined with a partial fundoplication to prevent reflux.
· Patients with megaesophagus and significant angulation or tortuosity of the esophagus should undergo a transhiatal esophagectomy.
SUGGESTED READINGS
Campos GM, Vittinghoff E, Rabl C, et al. Endoscopic and surgical treatments for achalasia: a systematic review and meta-analysis. Ann Surg. 2009;1:45–57.
Devaney EJ, Iannettoni MD, Orringer MB, et al. Esophagectomy for achalasia: patient selection and clinical experience. Ann Thorac Surg. 2001;72:854–858.
SSAT patient care guidelines. Esophageal achalasia. J Gastrointest Surg. 2007;11:1210–1212.
Williams VA, Peters JH. Achalasia of the esophagus: a surgical disease. J Am Coll Surg. 2009;208:151–162.