Jeffrey Kalish
Allen Hamdan
Presentation
A 65-year-old man with a history of hypertension, hyperlipidemia, and non–insulin-dependent diabetes mellitus presents with a 3-day history of pain in his left foot. He reports that his blood sugars, while normally very well controlled, have been very difficult to manage over the past day. His vital signs are normal. On physical examination, he has palpable femoral and popliteal pulses bilaterally but only dopplerable signals in the dorsalis pedis and the posterior tibial arteries. He has redness around the second toe, with a small 5-mm ulcer on the dorsal surface of the toe. The ulcer does not appear to probe deeply.
Differential Diagnosis
The lifetime risk of acquiring foot lesions (ulcers/gangrene) in diabetic patients has been estimated at 15% to 25%, with an annual incidence of approximately 1.0% to 4.1%. The clinical presentation of peripheral arterial disease (PAD) encompasses intermittent claudication, rest pain, and ulcers with or without gangrene. Diabetic patients may exhibit these typical symptoms, but more often they present with a wound that fails to heal or with pain at the site of a callus, pressure point, or other bony prominence. It is imperative to identify the presence of neuropathic ulcers, which arise at points of increased pressure and weight bearing, as well as the characteristic findings of a “Charcot foot.”
Workup
The three pathologic components leading to diabetic foot complications (ischemia, neuropathy, and infection) frequently occur in combination as an etiologic triad. Thorough clinical examination of foot ulcers is necessary to evaluate the depth and extent of involvement, anatomic location, etiology, and presence of ischemia or infection. Diabetic patients typically suffer from tibial and peroneal arterial occlusive disease with relative sparing of the foot arteries, and ischemia results from both atherosclerotic macrovascular disease and microcirculatory dysfunction. Diabetic neuropathy has multiple manifestations in the foot because it encompasses sensory, motor, and autonomic fibers. Because of a blunted neuroinflammatory response, diabetic patients lack a crucial component of the body’s natural first-line defense against pathogens and thus are more susceptible to an ensuing foot infection.
The typical inflammatory signs of infection may be absent or diminished (e.g., erythema, rubor, cellulitis, or tenderness). The usual systemic manifestations of infection (e.g., fever, tachycardia, or elevated white blood cell count) are frequently absent as well. Unexplained hyperglycemia should prompt an aggressive search for a source of infection because the elevated glucose may be the only sign of impending problems. Careful palpation of the foot for areas of tenderness or fluctuance is important in order to detect undrained abscesses in deeper tissue planes. All ulcers must be carefully inspected and probed, and superficial eschar unroofed, to look for potential deep space abscesses. Osteomyelitis occurs after the spread of superficial infection of the soft tissue to the adjacent bone or marrow. Although numerous expensive radiologic techniques are available to diagnose osteomyelitis (e.g., MRI, bone scan, tagged white blood cell scan), a simple sterile metallic probe will usually suffice; if this sterile probe hits bone, then osteomyelitis can be diagnosed with a sensitivity of 66%, a specificity of 85%, and a positive predictive value of 89%. Plain radiographs of the foot should be obtained in every patient with suspected foot infection. X-rays can reveal the presence of a foreign body, gas, osteolysis or joint effusion, as well as delineate anatomy for surgical planning.
A complete vascular exam is imperative in any patient reporting symptoms consistent with claudication or rest pain, and in any patient with extremity ulcers or gangrene. In those cases where the vascular status is unclear, noninvasive vascular laboratory studies (ankle brachial indices/pulse volume recordings [ABI/PVR]) are particularly useful. Patients with severe ischemia usually have ABI of <0.4, but many diabetic patients have noncompressible vessels with resulting artificially elevated ABIs so PVRs are required. Intra-arterial digital subtraction arteriography is the most accurate method to evaluate the lower-extremity arterial circulation. Although magnetic resonance arteriography had been used more frequently during the past decade in patients with marginal renal function, recent reports about nephrogenic systemic fibrosis have shifted clinical practice back to conventional arteriography. A carefully performed arteriogram must show the appropriate inflow source and outflow target artery, and it must incorporate the complete infrapopliteal circulation, including foot vessels.
Diagnosis and Treatment
In the absence of deep infection or necrosis, minor infections or ulcers may be managed conservatively with local wound care and/or antibiotics. Topical dressings, typically saline-impregnated gauze, should be aimed at maintaining a moist environment. The ulcer should be protected from excessive pressure by placement of an accommodative pad around the lesion to distribute pressure to surrounding tissues. Patients with limb-threatening infections require immediate hospitalization, immobilization, and intravenous antibiotics. Cultures from the depths of the ulcer should be sent; wound swabs are unreliable and should not be performed. Empiric broad-spectrum antibiotic therapy (dictated by institutional preferences, local resistance patterns, availability, and cost) should be initiated to cover the polymicrobial infections usually seen in diabetic patients. Although various trials have tried to compare various antibiotic regimens, they fail to focus on an inherent weakness of simply using antibiotics alone, that is, the reported “failure rates” in these trials of 11% to 12% for moderate infections and 19% to 30% for severe infections. Furthermore, the presence of PAD predicts a higher failure rate for healing any diabetic foot lesion after 1 year (31% failure vs. 16% failure). Mild infections usually require only 7 to 10 days of antibiotic therapy, whereas moderate and severe infections may require up to 3 weeks of treatment. Traditional therapy for osteomyelitis was accepted as 4 to 6 weeks of intravenous antibiotics, but recent studies have documented a >30% recurrence rate using this modality alone.
Presentation Continued
The patient is admitted to the hospital and placed on an insulin drip. The ulcer and surrounding cellulitis worsen (Figure 1), and he does not respond to the intravenous broad-spectrum antibiotics. An arteriogram shows patency of vessels to the level of the below-knee popliteal but long-segment occlusions in his anterior and posterior tibial vessels with a large reconstituted dorsalis pedis artery (Figure 2).

FIGURE 1 • (A,B) Left second toe ulcer and surrounding cellulitis.

FIGURE 2 • Composite arteriogram of left lower-extremity revealing tibial artery occlusions with reconstitution of dorsalis pedis artery in foot.
Surgical Approach
Debridement/Drainage Procedures
Presentation Continued
The patient undergoes an open second toe amputation, continues on intravenous antibiotics, and has resolution of the surrounding cellulitis. Vein mapping shows adequate ipsilateral greater saphenous vein for a planned below-knee popliteal to dorsalis pedis artery bypass.
Patients with abscess formation or necrotizing fasciitis must undergo prompt incision, drainage, and debridement including partial open toe, ray, or forefoot amputation. Tendon sheaths should be probed as proximally as possible and excised if infected. Despite fears to the contrary, long and extensive drainage incisions will heal when infection is controlled and foot circulation is adequate. It is imperative to make any necessary incision initially, but at the same time to contemplate the implications of those incisions on the potential completion amputation. Wounds should be packed open with saline-moistened gauze, and dressings should be changed two to three times a day. Wounds should be examined daily, and additional bedside or operative debridement should be repeated as needed. Adequate dependent drainage is crucial, and limited incisions with drains (closed-suction or penrose) should be avoided.
Patients with salvageable ischemic foot lesions and concomitant active infection need the infection controlled prior to vascular surgical intervention. In addition to instituting broad-spectrum antibiotics, options include open debridement and drainage or partial foot amputation. A short delay (usually <5 days) before revascularization in order to control active infection is justified; however, longer waits in order to “sterilize wounds” is inappropriate, and may result in further necrosis and a lost opportunity to save the foot.
Lower-Extremity Bypass
From a revascularization perspective, the most important difference in lower-extremity atherosclerosis in the patient with diabetes is the anatomic location or distribution of the arterial lesions. While patients with diabetes who abuse cigarettes may manifest iliac or femoral occlusive disease, diabetic patients typically have significant occlusive disease in the infrapopliteal arteries, while arteries of the foot are spared. This “tibial artery disease” requires a different approach to arterial reconstruction and presents special challenges for the surgeon (Table 1).
TABLE 1. Key Technical Steps and Potential Pitfalls to a Lower-extremity Bypass
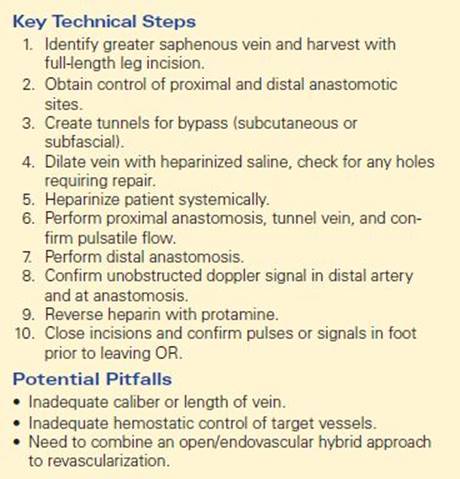
Each operation must be individualized, based on the patient’s available venous conduit and arterial anatomy. In 10% of cases a foot artery, usually the dorsalis pedis artery, is the only suitable outflow vessel; in an additional 15% of patients, the dorsalis pedis artery will appear to be the best target vessel in comparison to other patent but diseased tibial vessels. Although pedal bypass represents the most “extreme” type of distal arterial reconstruction, it is almost always possible, particularly when the surgeon is flexible in terms of venous conduit and location of proximal anastomosis. Primary patency, secondary patency, and limb salvage rates approach 57%, 63%, and 78% at 5 years and 38%, 42%, and 58% at 10 years.
Endovascular Therapy
Although surgical reconstruction has traditionally been the gold standard for diabetic foot revascularization, endovascular intervention has become a viable alternative. With the potential pitfalls accompanying traditional surgical approaches to limb salvage, as well as the overall poor health and life expectancy of patients with PAD, less invasive endovascular therapy can represent an attractive option. Balloon angioplasty and stenting are well suited to focal, short-segment iliac stenoses or occlusions, which exist in 10% to 20% of diabetic patients. With regard to outflow procedures, the morbidity of open surgery can be quite significant, and not simply limited to local wound complications or myocardial infarctions. Readmissions to the hospital, reoperations, slow time to healing, and time spent in rehabilitation must be factored into the risk-benefit analysis. In fact, the ideal outcome (patent graft, healed wound, no additional operations in a fully ambulatory patient who can sustain independent living) may only be obtainable up to 20% of the time. Although patency rates of bypass grafts have been shown to be equivalent in diabetics and nondiabetic patients, endovascular interventions may be associated with worse patency rates in diabetics due to their higher prevalence of limb-threatening ischemia as the presenting symptom.
The best scientific attempt to compare primary open and endovascular interventions was the bypass versus angioplasty in severe ischemia of the leg trial. Perioperative (30-day) morbidity was higher with surgery; all-cause mortality trended higher with surgery for the first 6 months but then trended lower for the next 6 months; amputation-free survival was similar in both groups. Two-year post hoc analysis revealed that surgery was associated with a reduced risk of future amputation and/or death. The trialists concluded that although the strategies are roughly equivalent at medium-term follow-up with regard to mortality and amputation-free survival, angioplasty should be used first for patients with significant comorbidities and with a life expectancy of <1 to 2 years. Moreover, longer-term results favor surgery over angioplasty if there is a “good” vein and a medically fit patient. More recent reviews have shown that after 2 years, tibial angioplasty requires repeat endovascular intervention in up to one-third of patients, and another 15% of patients go on to have a surgical bypass.
Amputation
The last alternative remains amputation. Closed minor amputations (toes or transmetatarsal) are practical following infection control and revascularization, and typically leave the patient with a functional foot for walking (Figure 3). In situations involving extensive tissue loss precluding a functional foot, when there are nonhealing wounds in the setting of patent grafts, and for control of sepsis, amputation below the knee is necessary. Surgeons should strive to preserve the knee joint because of its functional significance for rehabilitation. Above-knee amputations are reserved for debilitated patients with severe tissue loss or with no capacity to ambulate. Because of modern advances in prostheses coupled with aggressive approaches to rehabilitation, amputation should be viewed as an acceptable modality to treat diabetic foot complications and not as a treatment failure.

FIGURE 3 • Transmetatarsal amputation.
Special Intraoperative Considerations
Several unexpected findings may be encountered during a lower-extremity revascularization procedure. If an artery is found to be too heavily calcified or does not have an adequate lumen, then the surgeon must reevaluate the preoperative arteriogram to find a more suitable target. If the venous conduit is not of suitable quality or length to perform the planned bypass, then the surgeon must consider splicing the greater saphenous vein with alternative venous conduits or using an alternative conduit altogether (such as contralateral greater saphenous vein, ipsilateral or contralateral lesser saphenous vein, basilic or cephalic arm veins, or even a composite sequential bypass with prosthetic and vein). Another current option involves hybrid procedures to achieve revascularization; this involves the combination of a shorter bypass with either an inflow or outflow endovascular procedure (such as a superficial femoral artery angioplasty/stent coupled with a popliteal to distal bypass, or a prosthetic femoral to popliteal bypass coupled with a tibial angioplasty/stent). Vascular surgeons have many tools and technologies available, and these should all be used in the efforts to achieve limb salvage.
Postoperative Management
Patients should be observed in a monitored setting overnight following lower-extremity revascularization, and neurovascular checks should be performed every 1 to 2 hours. Arterial lines and foley catheters can usually be discontinued after 1 to 2 days once blood pressures have stabilized, and urine output has been adequate. Patients should get out of bed to chair by postoperative day 1 and typically can ambulate on postoperative day 2. Physical therapy consults should be involved early in order to facilitate a patient’s transition home or to rehabilitation. Because these vascular surgery patients typically have significant comorbidities, practitioners must be vigilant for postoperative complications such as myocardial infarction, pneumonia, wound infection, hematoma, etc.
Surveillance studies should typically be done on both lower-extremity bypass grafts and endovascular interventions in order to monitor for recurrent stenoses or impending failure. Exact algorithms are debatable, but the basic premise relies on surveillance duplex ultra-sounds in regular intervals (such as every 3 months for 1 year, then every 6 months for 1 year, then yearly) in order to identify grafts that are at risk for failure. This allows for certain patients to undergo arteriograms to identify and treat potential areas of intimal hyperplasia or new atherosclerotic lesions.
Case Conclusion
The patient undergoes a successful bypass and is discharged to rehabilitation on postoperative day 5. His wound improves with local wound care, and he eventually granulates the wound and heals secondarily. Surveillance duplex shows a patent bypass graft with no areas of elevated velocities.
TAKE HOME POINTS
· The three pathologic components leading to diabetic foot complications (ischemia, neuropathy, and infection) frequently occur in combination as an etiologic triad.
· The typical inflammatory signs and systemic manifestations of infection may be absent or diminished in diabetic patients, and unexplained hyperglycemia may be the only indicator of a foot infection.
· Patients with salvageable ischemic foot lesions and concomitant active infection need the infection controlled for a short period (usually no more than 5 days) prior to vascular surgical intervention.
· Each lower-extremity bypass operation must be individualized, based on the patient’s available venous conduit and arterial anatomy, with diabetic patients typically manifesting tibioperoneal disease with sparing of foot arteries.
· Although surgical reconstruction is the current gold standard for diabetic foot revascularization, endovascular intervention has become a viable alternative.
SUGGESTED READINGS
Adam DJ, Beard JD, Cleveland T, et al. BASIL trial participants. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet. 2005;366(9501):1925–1934.
Gibbons GW, Eliopoulos GM. Infection of the diabetic foot. In: Kozak GP, Campbell DR, Frykberg RG, et al., eds. Management of Diabetic Foot Problems. 2nd ed. Philadelphia, PA: WB Saunders, 1995:121–129.
Mills JL, Armstrong DG, Andros G. Strategies to prevent and heal diabetic foot ulcers: building a partnership for amputation prevention. J Vasc Surg. 2010;52(3 suppl):1S–103S.
Pomposelli FB, Kansal N, Hamdan AD, et al. A decade of experience with dorsalis pedis artery bypass: analysis of outcome in more than 1000 cases. J Vasc Surg. 2003;37:307–315.