Michael J. Weyant
![]() INDICATIONS
INDICATIONS
Video-assisted thoracoscopic surgery (VATS) lobectomy is most commonly used to treat conditions of the lung parenchyma requiring resection of an entire lobar section of the lung. The most frequent indications for this approach are either early-stage tumors of the lung, or infectious diseases causing destruction of a significant portion of the lobe. A list of indications for a VATS lobectomy include the following.
Clinical stage I nonsmall cell lung cancer (NSCLC)
Uncharacterized but suspicious pulmonary nodules which are not amenable to wedge resection
Mycetoma contained in the lung parenchyma
Atypical mycobacterial infections causing destruction of the majority of the parenchyma of the lobe intended for resection
Pulmonary sequestration
![]() RELATIVE CONTRAINDICATIONS
RELATIVE CONTRAINDICATIONS
Contraindications to VATS lobectomy are relative based on the experience of the operator. Nearly all forms of surgically treated lung cancer have been reported to be undertaken via a VATS approach with success; however, these approaches may not apply to the general population of thoracic surgeons who do not encounter these cases with great volume. Although concerns over the adequacy of VATS lobectomy have been addressed extensively in treating stage I NSCLC, there is far less data regarding the ability to treat higher stages effectively and should be used with caution unless the operator has significant experience with this approach. In general relative contraindications to a VATS lobectomy include the following.
NSCLC higher than stage I
Tumors invading the chest wall
Tumors invading the hilum
NSCLC with macroscopic lymph node involvement
Failure to progress after a reasonable time with the VATS approach
Aberrant vascular or bronchial anatomy
Complete pleural symphysis
![]() PREOPERATIVE PLANNING
PREOPERATIVE PLANNING
The preoperative planning for a patient undergoing VATS lobectomy is similar for all lobes of the lung and centers mainly around evaluation of a patient’s functional and cardiopulmonary status as well as adequate tumor staging in the event of a malignancy. All patients should have basic spirometry and diffusion capacity measurements as well as a measurement of oxygen saturation during a 6-minute walk test. Quantitative perfusion scanning should be undertaken in patients with more marginal pulmonary function. Cardiac evaluation consists mainly of some form of myocardial stress testing and an echocardiogram to evaluate pulmonary artery pressures, valvular function, and ventricular function. The evaluation of a patient’s physical ability to withstand the operation is much more subjective. In general I am reluctant to perform a VATS lobectomy on wheelchair or bed-bound nonambulatory patients. Demonstrating an ability to independently ambulate as well as strong family support are positive indicators for success. The use of supplemental oxygen should not be an absolute contraindication as its use has increased with the treatment of chronic obstructive pulmonary disease and sleep apnea. Careful history taking can usually help determine whether the use of supplemental oxygen in a particular patient is an actual contraindication. Preoperative physiologic testing prior to a VATS lobectomy may be summarized by the following:
Always:
Spirometry
Diffusion capacity
Myocardial stress test
Echocardiogram
Occasional:
Quantitative perfusion scanning
Six-minute walk
Stair climb
Significant attention should be paid to preoperative imaging studies regarding staging of potential tumors, anatomy of airways and vasculature, and extent of lung destruction in the event of an infectious process. The most helpful imaging study in the preoperative planning of a VATS lobectomy is a contrast-enhanced computed tomography (CT) of the chest. Although intravenous contrast is not often used for lung cancer screening imaging it is extremely helpful in ensuring there is no unusual vascular anatomy or for determining adherence of a lesion to the pulmonary artery. Observation of the relationship of any lesion to the fissure anatomy is very important to determine whether a VATS lobectomy is feasible. 18Flourodeoxyglucose positron emission tomography (FDG-PET) is somewhat useful in predicting nodal disease. This will not be discussed in great detail here; however, the main use of FDG-PET will be to exclude patients from the VATS procedure if there is evidence of significant lymph node involvement or satellite lesions identified. Occasionally, imaging findings can be used to help counsel a patient about the possibility of converting from a VATS to an open procedure based on the above data obtained from a scan.
![]() SURGERY
SURGERY
The discussion of the surgical technique of a VATS lower lobectomy begins below and the specifics of achieving the operation will be discussed. It is important to realize several underlying themes when performing these procedures no matter which lobe is being resected. The key point to all of the techniques described is that they should be as constant and fixed as possible from procedure to procedure. This means that the port placement should be similar for all lobes, ports of access for staplers, although differing according to the type of lobe removed, should not deviate, direction of retraction, and order of transection of tubular structures also should be as consistent as possible from case to case. This rigid adherence may seem counterintuitive given the differences in body habitus and anatomic relationships but one of the most powerful indicators that something is going wrong with a case is the inability to achieve a step of the procedure similar to previous cases. I cannot emphasize enough that when beginning to perform these procedures the failure to achieve a step of the operation as done previously should be an indication to open the patient and figure out why prior to inadvertently transecting or injuring a structure that may not be able to be repaired.
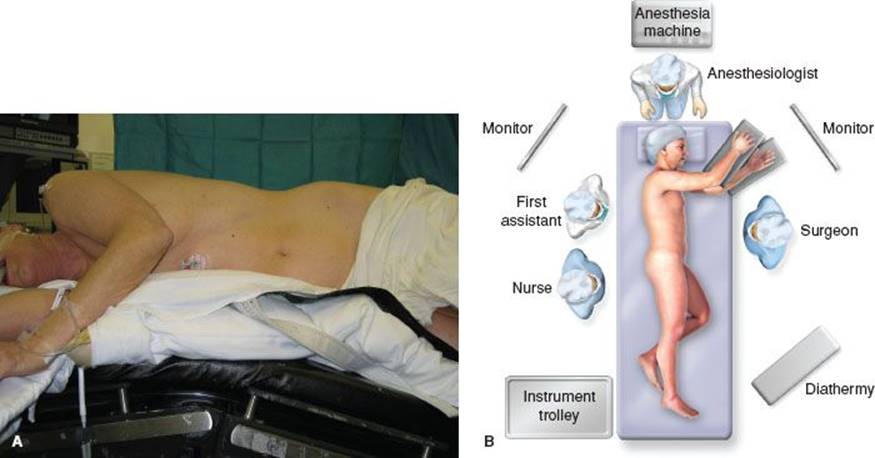
Figure 14.1 A: Standard positioning for VATS pulmonary procedures. B: Schematic description of operating room configuration for most VATS procedures.
Positioning
Positioning for all patients undergoing a VATS lobectomy is the same. The patient is placed in the lateral decubitus position with the bed maximally flexed with the breakpoint just above the superior iliac crest. This reduces the interference caused by the hips and serves to spread the rib spaces as much as possible (Fig. 14.1). Any increase in the space between the ribs will reduce the difficulty of the procedure. A schematic view of the operating room setup is illustrated in (Fig. 14.1).
Port Site Placement
Port site placement is similar for all VATS lobectomies. Many authors have described variations of port placement and number of ports. I will use three ports with one being used as a 4-cm working incision (Fig. 14.2). The camera port is placed first and although markings are made for placement of the other two ports, the final decision on location for the working and retraction port is not made until visualization of the thoracic cavity is undertaken using the camera. The most desirable position for the working incision in a right lower lobectomy is directly over or the superior pulmonary vein. The most important issue with port placement is to become comfortable with accessing all areas of the lung through whatever constellation of ports chosen. The consistency will help establish a routine that will increase the chances of completing the procedure via a VATS approach.

Figure 14.2 A,B: Illustration of standard port site placements for VATS pulmonary procedures.
Identification of Lesion
Once the operator becomes comfortable with the port site placement nearly all surfaces of the lung can be palpated with the index finger using countertraction from a gentle lung clamp. Despite the confidence given by locating lesion via CT scan preoperatively there is no substitute for reconfirming that the target lesion is present in the lobe it was thought to be.
Pulmonary Vein Dissection
The lower lobe pulmonary vein is dissected first in all right lower lobectomies. This can be accomplished first by incising the inferior pulmonary ligament with electrocautery (Fig. 14.3). Often a lymph node will reside in the inferior pulmonary ligament immediately adjacent to the inferior pulmonary vein and can be used as an indicator that the vein is near. Blunt dissection with a pediatric suction device and large blunt right-angled clamps effectively encircle the inferior pulmonary vein (Fig. 14.3). It is extremely important to identify the middle lobe pulmonary vein before transecting the lower lobe pulmonary vein as it can occasionally drain into the inferior pulmonary vein. The inferior vein is then transected by introducing the endovascular stapler through the working incision (Fig. 14.3).
Pulmonary Artery Dissection
The order of transection of tubular structures of the right lower lobe is somewhat variable and depends on the anatomy of the fissure. If the fissure is complete and the pulmonary artery is visible at the base of the fissure it is very reasonable to dissect the pulmonary artery to the lower lobe as a next step. The anterior portion of the major fissure can be transected similar to the technique mentioned in the VATS middle lobe chapter in this text and the pulmonary artery can be completely dissected as described in Figure 14.4. When the occasion arises that the major fissure is entirely incomplete and offers no easy access to the pulmonary artery it is then appropriate to dissect and transect the pulmonary artery from an inferior approach after the bronchus is dissected and transected. Particular to the right lower lobe, developing comfort with both of the potential methods to transect the tubular structures will help the surgeon complete more VATS lobes successfully. Regardless of how the pulmonary artery is dissected it is transected by introducing the endovascular stapler through the working incision.

Figure 14.3 A: Exposure of the inferior pulmonary ligament and incisures with electrocaurtery. B: Demonstration of identification of inferior pulmonary vein after dissection of pulmonary ligament. C: Blunt dissection of inferior pulmonary vein. D: Transection of inferior pulmonary vein using an endovascular stapler placed via the working port.
Bronchus Dissection
The right lower lobe bronchus is located immediately behind the pulmonary vein. It can be dissected and encircled bluntly as well. More caution should be used when bluntly dissecting behind the bronchus as the lower lobe pulmonary artery is located immediately deep to it (Fig. 14.5). Particular to the right lower lobe, it is imperative to thoroughly evaluate the placement of the endoscopic GIA stapler in regard to the middle lobe bronchus. It is quite easy to close the stapler and encroach on the right middle lobe bronchial orifice so much so that the middle lobe is nonfunctional. This is avoided by testing the inflation of the lower lobe while the stapler is closed across the right lower lobe bronchus. The stapler here is also introduced through the working incision.

Figure 14.4 A: Identification of the pulmonary artery in the major fissure using blunt dissection. B,C: Encircling of the pulmonary artery to the lower lobe using blunt dissection. D: Transection of the pulmonary artery to the lower lobe using an endovascular stapler placed via the working incision.
Fissure
The fissure between the lower and upper lobes is then divided by placing an endoscopic GIA stapler in the working incision (Fig. 14.6).
Intercostal Nerve Block
Before placing a chest tube and closing the incisions an intercostal nerve block is performed. This is done by using 0.25% Marcaine with epinephrine and instilled next to the intercostal nerves using an angled mediastinoscopy needle (Fig. 14.7).
![]() POSTOPERATIVE MANAGEMENT
POSTOPERATIVE MANAGEMENT
The postoperative management of a VATS lobectomy patient is consistent for all lobes. All patients receive aggressive pulmonary toilet with early ambulation, patient-controlled analgesia, and incentive spirometry. The thoracostomy tube placed in the operating room is removed when all air leaks subside and the drainage of pleural fluid is below 300 to 400 cc. I will have the chest tube placed on −20 cm H2O overnight and then to water seal. Realizing that tube management postoperatively is not uniform among thoracic surgeons I will summarize by saying that the tube is removed when the air leak stops and the surgeon is comfortable with the amount of pleural drainage. The use and amount of suction is entirely based on surgeon’s preference. Multiple studies have suggested that pleural drainage volumes of as high as 400 cc per day can be effectively used as indicators that a tube is ready to be removed.

Figure 14.5 A,B: Dissection of the bronchus to the lower lobe using blunt technique. C: Transection of the right lower lobe bronchus using an endoscopic GIA stapler placed through the working incision.

Figure 14.6 A,B: Transection of the remaining portion of the major fissure using endoscopic GIA staplers placed through the working incision.

Figure 14.7 A,B: Intrathoracic intercostal nerve block is placed using a standard mediastinoscopy needle and 0.25% Marcaine with additional epinephrine.
![]() COMPLICATIONS
COMPLICATIONS
The complications of a VATS lobectomy are similar to open lobectomy and can be discussed separately in intraoperative and postoperative settings. Intraoperatively, airway and vascular injuries can occur and are more unsetting to the surgeon in the VATS approach due to the perceived lack of control and access to the injury. The wariness of dealing with these problems during the operation can be mitigated by proper planning. In addition to marking the expected port placement for the VATS lobectomy I will always mark an incision line for a thoracotomy on every VATS lobectomy case. In the event that urgent conversion to thoracotomy is needed, guessing where to make the incision only increases the stress. I suggest that when converting to an open thoracotomy in either a nonemergent or emergent situation that a standard thoracotomy be used rather than trying to extend the working incision which you will find does not afford significant access to deal with the problem you are opening for and only serves to transect the long thoracic nerve. When dealing with significant hemorrhage it is almost always possible to place a sponge stick through the working incision to apply pressure to control the bleeding while a thoracotomy is made. Airway injuries intraoperatively are uncommon but can be evaluated by placing a small amount of irrigation in the chest and inflating the lung while looking for significant leakage of air.
Postoperative complications mainly are the result of poor pulmonary toilet and manifest usually as a pneumonia. Prolonged air leak (>7 days) can occur and are usually managed by observation with rare reoperation. Patience and the use of small portable pleurovacs can help discharge patients safely while waiting for any prolonged air leak to heal.
![]() RESULTS
RESULTS
VATS lobectomy has been reported to have significant benefit over open lobectomy for early-stage lung cancer. These benefits include shorter hospital stay, shorter chest tube duration, decreased production of inflammatory mediators, and less perioperative pain. This is all coupled with a large body of literature documenting comparable safety when compared to the open procedure. In addition, many authors have reported equivalent oncologic effectiveness for early-stage lung cancer. Despite these findings the adoption of VATS lobectomy has been slow with approximately only a third of patients undergoing lobectomy having a VATS approach. The salient debates and controversies that have arisen during the development of VATS lobectomy techniques include safety outcomes of the procedure, comparison with open lobectomy, oncologic effectiveness, ability to stage lymph nodes in stage I lung cancer, and biologic benefits of VATS lobectomy (Table 14.1). Each controversy outlined in Table 14.1 has an illustrative modern reference described to help address these controversies realizing that there is a multitude of literature that is not referenced here.
TABLE 14.1 Representative Literature Regarding the Controversies of VATS Lobectomy

![]() CONCLUSIONS
CONCLUSIONS
VATS lobectomy has been proven to be a safe and effective modality to treat early-stage lung cancer and other diseases requiring resection of a lobe of the lung. Thorough preoperative planning regarding physiologic and imaging evaluations of the patient will reduce complications and lead to more frequent successful completion of VATS procedures. Maintaining a consistent stepwise plan in performing VATS lobectomies will reduce the incidence of intraoperative catastrophe and alert the operator to an impending irreversible problem during the procedure.
Recommended References and Readings
Allen MS, Darling GE, Pechet TT, et al. Morbidity and mortality of major pulmonary resections in patients with early-stage lung cancer: Initial results of the randomized, prospective ACOSOG Z0030 trial. Ann Thorac Surg.2006;81:1013–1019; discussion: 1019–1020.
Boffa DJ, Kosinski AS, Paul S, et al. Lymph node evaluation by open or video-assisted approaches in 11,500 anatomic lung cancer resections. Ann Thorac Surg. 2012;94:347–353.
Craig SR, Leaver HA, Yap PL, et al. Acute phase responses following minimal access and conventional thoracic surgery. Eur J Cardiothorac Surg. 2001;20(3):455–463.
Farjah F, Wood DE, Mulligan MS, et al. Safety and efficacy of video-assisted versus conventional lung resection for lung cancer. J Thorac Cardiovasc Surg. 2009;137:1415–1421.
Flores RM, Ihekweazu UN, Rizk N, et al. Patterns of recurrence and incidence of second primary tumors after lobectomy by means of video-assisted thoracoscopic surgery (VATS) versus thoracotomy for lung cancer. J Thorac Cardiovasc Surg. 2011; 141:59–64.
McKenna RJ Jr, Houck W, Fuller CB. Video-assisted thoracic surgery lobectomy: Experience with 1,100 cases. AnnThorac Surg. 2006;81:421–425; discussion: 425–426.
Onaitis MW, Petersen RP, Balderson SS, et al. Thoracoscopic lobectomy is a safe and versatile procedure: Experience with five hundred consecutive patients. Ann Surg. 2006;244:420–425.
Paul S, Altorki NK, Sheng S, et al. Thoracoscopic lobectomy is associated with lower morbidity than open lobectomy: A propensity-matched analysis from the STS database. J Thorac Cardiovasc Surg.2010;139:366–378.
Roviaro G, Varoli F, Vergani C, et al. Long-term survival after videothoracoscopic lobectomy for stage I lung cancer. Chest. 2004;126:725–732.
Swanson SJ, Herndon JE, D’Amico TA, et al. Video- assisted thoracic surgery lobectomy: Report of CALGB thirty-nine thousand eight hundred and two—a prospective, multi-institution feasibility study. J Clin Oncol.2007;25:4993–4997.
Walker WS, Codispoti M, Soon SY, et al. Long-term outcomes following VATS lobectomy for non-small cell bronchogenic carcinoma. Eur J Cardiothorac Surg. 2003;23:397–402.
Whitson BA, Groth SS, Duval SJ, et al. Surgery for early-stage non-small cell lung cancer: A systematic review of video-assisted thoracoscopic surgery versus thoracotomy approaches to lobectomy. Ann Thorac Surg. 2008;86:2008–2016.