Paula A. Ugalde, Jocelyn Grégoire, Yang Zhiguang, Rabah Boultifat, and Jean Deslauriers
Introduction
Although Price Thomas is given credit for having done the first sleeve resection in 1947, the most significant early description of these procedures is that of Paulson and Shaw who, in 1955, reported on 18 patients who had undergone various types of bronchoplasties for benign or malignant disorders of the bronchi and lungs. In that seminal paper, Paulson and Shaw stressed the importance of preserving lung and thus lung function. Since those early days, sleeve resection, once considered to be a compromised operation for lung cancer patients, has become standard of care when tumors can be completely resected by the technique.
In most reported series, including our own, sleeve resections are most commonly done for tumors located in the right upper lobe. Occasionally, however, neoplasms of the left lower lobe (LLL) may be amenable to this type of resection. In those cases, part of the left main bronchus (LMB) is resected in continuity with the LLL and the left upper lobe (LUL) bronchus is reimplanted into the proximal LMB.
![]() INDICATIONS
INDICATIONS
There are several reasons as to why LLL sleeve resections are rarely done when compared to sleeve resections involving other lobes (Table 38.1). The first and most obvious reason is that lung cancers located in the LLL are overall less common than those located in other lobes. Secondly, some surgeons feel that left-sided sleeve resections are technically more difficult than those on the right because there is no bronchus intermedius on the left side. A third argument is that patients with LLL tumors and N1 disease will often have metastatic nodes in the nodal sump area (along the lower border of the LUL bronchus) and that in such cases, sleeve resection may be oncologically less adequate an operation than pneumonectomy. A fourth reason is that left pneumonectomy is well tolerated and, indeed, the operative mortality associated with left pneumonectomy may not be much higher than that observed after lobectomy. The final argument is that some surgeons think, whether it is real or hypothetical, that the left superior pulmonary vein may become kinked during bronchial reconstruction, thus impairing venous return from the LUL.
TABLE 38.1 Possible Arguments as to Why LLL Sleeve Resection is Rarely Done

Although every one of those arguments has some merit, we think that LLL sleeve resection is as valid an operation as that of other types of bronchoplasties when complete resection can be achieved. We also think that left-sided sleeve resections are not more technically difficult than those on the right side and, indeed, they are often easier. Kinking of the superior pulmonary vein is a potential complication, which is more hypothetical than real.
![]() SURGERY
SURGERY
As for tumors located in other lobes, the possibility and feasibility of LLL sleeve resection is usually determined during diagnostic bronchoscopy where the tumor is seen as being located at the origin of the LLL bronchus often extending proximally toward the bifurcation between upper and lower lobes (Fig. 38.1). In such cases, it is generally clear that standard lobectomy will not be able to achieve an R0 status.
The standard operative approach is that of a standard or muscle-sparing thoracotomy done through the fifth intercostal space. After a thorough mobilization of lung and hilum, the final decision to do a LLL sleeve resection can only be made after interlobar, sump, hilar, and mediastinal nodes have been sampled and analyzed by frozen section (FS). If FS is not readily available, visual examination of the nodes is probably sufficient. If any of those nodes are positive for metastatic lung cancer, the surgeon will have to decide if sleeve resection is adequate or if a pneumonectomy would be preferable.
Once the decision to do a bronchoplasty has been reached, the pulmonary arterial branches to the lower lobe and the inferior pulmonary vein are first ligated and divided as they would normally be while doing a standard left lower lobectomy. After the interlobar fissure has been divided anteriorly and posteriorly, we often put tapes around the upper lobe, lower lobe, and main bronchi for the sole purpose of traction. Mobilization of the bronchi must be done gently to avoid devascularization, which fortunately, is uncommon on the left side where there normally are two bronchial arteries as opposed to only one on the right side.
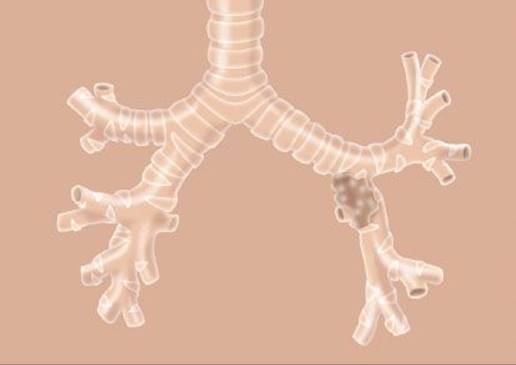
Figure 38.1 Tumor at the origin of the LLL bronchus.
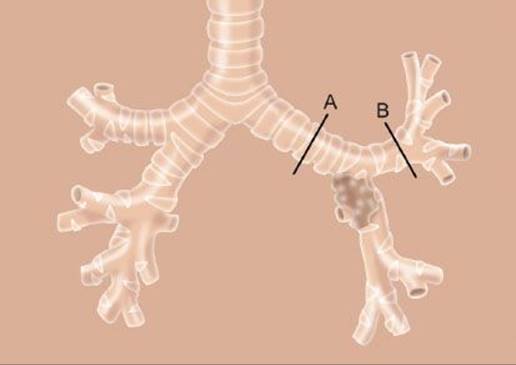
Figure 38.2 Sites of bronchial division. Also note division of left main bronchus (A), and division of left upper lobe bronchus (B).
The LMB is then divided perpendicular to its long axis approximately 2 cm proximal to the origin of the LUL bronchus and, likewise, the upper lobe bronchus is divided a few millimeters before it bifurcates into culmen and lingular segments (Fig. 38.2). Once both bronchial margins have been confirmed to be free of tumor by FS analysis (a most important feature of the operation), the anastomosis can be carried out in a standard fashion by using interrupted 3-0 and 4-0 resorbable suture material (Vicryl), knots being tied outside the lumen. Usually, three to four stitches are first placed over the right and anterior portion of the anastomosis and these are tied (Fig. 38.3). The remaining sutures are then inserted and tied once they have all been placed. Sutures are usually placed at 2-mm intervals and size discrepancy is corrected by uneven suture spacing. Once the anastomosis is completed (Fig. 38.4), it is checked for air tightness by asking the anesthetist to inflate the lung at pressures of approximately 30 to 40 cm of water.
Unless the bronchi are at risk of poor healing (older patients with osseous degenerescence of bronchial cartilages, irradiated bronchi, induction chemotherapy, redo surgery), covering the anastomosis with autogenous tissue is probably unnecessary. Ideally, a bronchoscopy should be done before the patient leaves the operating room not only to check the anastomosis but also to suction blood or other debris that may have accumulated in the reimplanted lobe.
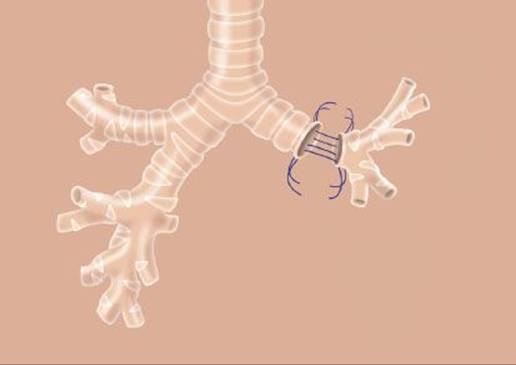
Figure 38.3 Back wall of anastomosis.
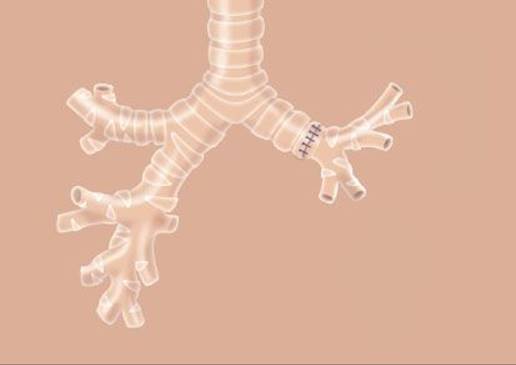
Figure 38.4 Anastomosis complete.
![]() POSTOPERATIVE CARE
POSTOPERATIVE CARE
The postoperative care of patients having had a LLL sleeve resection is essentially the same as for patients who have had any other type of bronchoplasty. It involves optimal pain control, maintenance of adequate fluid balance, and aggressive physiotherapy. Complications are rare and operative mortality is in the range of 2%.
![]() CONCLUSION
CONCLUSION
LLL sleeve resection should be part of the armamentarium of every thoracic surgeon doing lung cancer operations. The technique is fairly straightforward and short- as well as long-term results are similar to those associated with bronchoplasties of other lobes.
Recommended References and Readings
Paulson DL, Shaw RR. Bronchial anastomosis and bronchoplastic procedures in the interest of preservation of lung tissue. J Thorac Surg. 1955;29:238–259.
Thomas CP. Conservative resection of the bronchial tree. J R Coll Surg Edinb. 1956;1:169–186.
Tronc F, Grégoire J, Rouleau J, et al. Long-term results of sleeve lobectomy for lung cancer. Eur J Cardiothoracic Surg. 2000;17:550–556.