Phillip S. LoSavio, M.D.
1 Which of the following statements is true regarding the anatomy of the upper aerodigestive tract?
A The oral tongue lies posterior to the circumvallate papillae.
B The soft palate is a subsite in the oral cavity.
C The supraglottic and glottic regions of the larynx are divided by a transverse plane through the laryngeal ventricles.
D The false vocal cords are a part of the glottic region of the larynx.
E The floor of the mouth contains the openings of the sublingual, submandibular, and parotid glands.
Ref.: 1-3
Comments
The oral tongue lies anterior to the circumvallate papillae. The soft palate is a subsite of the oropharynx, not the oral cavity. The false vocal cords are a part of the supraglottic larynx. The floor of the mouth contains openings for the sublingual (ducts of Rivinus) and submandibular glands (Wharton duct), but not the parotid glands. The ducts for the parotid glands (Stensen duct) exit into the oral cavity adjacent to the upper second molar.
For staging and treatment purposes of head and neck cancer, it is important to understand the anatomic definitions of the different subsites of this region as they are defined by the American Joint Commission for Cancer (AJCC). Oral cavity subsites include the lips, oral tongue (anterior two thirds), buccal mucosa, floor of the mouth, upper and lower alveolar ridge, retromolar trigone, and hard palate. The oral cavity begins at the skin-vermillion junction anteriorly. Posterior boundaries include the circumvallate papillae as it relates to the tongue, the anterior tonsillar pillars, and the junction of the hard and soft palate. Oropharynx subsites include the base of the tongue, tonsils, soft palate, and pharyngeal wall lying between the soft palate and pharyngoepiglottic fold. Hypopharynx subsites include the piriform sinuses, postcricoid region, and posterior pharyngeal wall between the pharyngoepiglottic fold down to the upper esophageal sphincter.
The larynx is divided into three parts: supraglottis, glottis, and subglottis (Figure 15-1). Each has its own lymphatic drainage patterns and pathways of oncologic spread. These differences are a consequence of the different embryologic origins of the supraglottic and glottic larynx. The supraglottic larynx includes the epiglottis, aryepiglottic folds, arytenoids, ventricle, and false vocal cords. The glottis consists of the true vocal cords and the anterior and posterior commissures. It is divided from the supraglottis by a transverse plane passing through the ventricle. The subglottis starts inferior to the glottis and extends to the inferior border of the cricoid cartilage. It has no subsites.

Figure 15-1 Coronal view of the larynx.
Answer
C
2 Which of the following statements is true regarding the anatomy of the salivary glands?
A The paired submandibular glands are the largest of the major salivary glands in the head and neck and are located in the submandibular triangle just inferior to the body of the mandible.
B The retromandibular vein lies deep to the deep lobe of the parotid gland.
C Anatomic landmarks used for identifying the main trunk of the facial nerve during parotid surgery include the tympanomastoid suture line, the tragal pointer, and the posterior belly of the digastric muscle.
D The three major nerves most at risk for direct injury during surgery on the submandibular gland include the hypoglossal nerve, spinal accessory nerve, and lingual nerve.
E Injury to the greater auricular nerve during surgery on the parotid gland may lead to sensory deficits of the lower lip area on the affected side.
Ref.: 1, 2
Comments
The parotid glands, not the submandibular glands, are the largest of the major glands in the head and neck. The retromandibular vein can usually be well visualized as it passes between the superficial and deep lobe of the parotid on computed tomography (CT). The three major nerves most at risk for injury during surgery on the submandibular gland include the hypoglossal, marginal mandibular, and lingual nerves. The parotid gland is encased in a capsule of parotid fascia. The facial nerve (cranial nerve [CN] VII) is identified in reference to various anatomic structures. The tympanomastoid suture line is considered to be a reliable landmark. The main trunk of the nerve is located just deep and medial to this anatomic marker. The nerve also lies about 1 cm deep and inferior in reference to the tragal pointer, although this landmark is less reliable. The posterior belly of the digastric muscle provides a reference regarding the approximate depth of the nerve. As a last option, the nerve could be identified by following the peripheral buccal branches, although this should never be considered the standard approach to dissecting the nerve. The submandibular gland sits in the submandibular triangle of the neck. The marginal mandibular nerve (branch of CN VII) lies just deep to the superficial layer of the deep cervical fascia, which lies below the platysma. The gland wraps around the mylohyoid muscle, which is retracted anteriorly during surgery for exposure. The lingual nerve provides innervation to the gland through the submandibular ganglion. CN XII also lies deep to the gland. The greater auricular nerve supplies sensation to the earlobe, as well as to the preauricular and postauricular skin. The lower chin and lip region receive sensory innervation from the mental nerve, a branch of the third division of the trigeminal nerve (V3).
Answer
C
3 Which statement is most accurate regarding the histology of the head and neck?
A The pharynx is lined exclusively by nonkeratinizing stratified squamous epithelium.
B The minor salivary glands lie in the submucosa of the oral cavity and pharynx.
C The Waldeyer ring consists of only two structures: the palatine tonsils and adenoids.
D The adenoids have crypts lined by stratified squamous epithelium.
E The nasal cavity consists entirely of ciliated respiratory epithelium.
Ref.: 1, 2
Comments
The pharynx is lined by both nonkeratinizing stratified squamous epithelium and ciliated respiratory epithelium. The Waldeyer ring consists of the palatine tonsils, adenoids, and the lingual tonsils, which lie along the base of the tongue. The palatine tonsils have crypts lined by stratified squamous epithelium. The adenoids are covered by pseudostratified ciliated columnar epithelium with surface folds but, unlike the tonsils, do not have crypts. The tonsillar crypts are designed to trap foreign antigens for presentation to the lymphoid follicles. The nasal cavity is composed primarily of respiratory epithelium but also contains specialized sensory olfactory epithelium along the roof. Hundreds of minor salivary glands lie in the submucosa of the oral cavity and pharynx.
Answer
B
4 A 56-year-old man with T2N0M0 squamous cell carcinoma (SCC) of the lateral oral tongue is scheduled for partial glossectomy with selective lymph node neck dissection—levels I, II, and III in the ipsilateral neck. Which of the following statements is true regarding the anatomic classification of cervical lymphatic nodal basins?
A Level IA contains the submandibular gland.
B Tumors of the larynx most commonly metastasize to level I.
C Level II is bounded superiorly by the cricoid cartilage.
D The posterior border of level III is the anterior edge of the sternocleidomastoid (SCM) muscle.
E Level IV is bounded anteriorly by the strap muscles.
Ref.: 1
Comments
Level I is subdivided into two parts (Figures 15-2 and 15-3). Level IA contains mostly fibroadipose/lymphatic tissue with no major neurovascular structures. Level IB contains the submandibular gland. Tumors of the larynx most commonly metastasize to levels II, III, and IV. Level II is bounded superiorly by the skull base and inferiorly by the hyoid bone. Level IV is bounded superiorly by the cricoid cartilage. The posterior border of level III is the posterior edge of the SCM muscle.

Figure 15-2 Diagram of cervical lymph node levels I through V. Level II is divided into regions A and B by the spinal accessory nerve.

Figure 15-3 Diagram of anterior lymph node levels I, VI, and VII. Though large in area, the majority of level VI lymph nodes are confined to the paratracheal region.
Answer
E
5 A 68-year-old woman is evaluated for a 1-month history worsening dyspnea and hoarseness. Fiberoptic laryngoscopy demonstrates left vocal cord paralysis with full mobility of the right true vocal cord. Findings on physical examination are otherwise unremarkable. CT of the chest demonstrates a large mediastinal mass. Which of the following statements is most accurate?
A The left recurrent laryngeal nerve (RLN) branches off of the vagus nerve and passes around the left subclavian artery back to the larynx.
B A nonrecurrent RLN can be associated with a retroesophageal right subclavian artery.
C The RLN supplies all the muscles of the larynx except the posterior cricoarytenoid muscle.
D The vagus nerve exits the skull through the carotid canal.
E The RLN enters the larynx through the thyrohyoid membrane to innervate the larynx.
Ref.: 1
Comments
The left recurrent laryngeal nerve separates from the vagus in the mediastinum, wraps around the aortic arch at the ductus arteriosus, and then ascends back along the tracheoesophageal groove toward the larynx. The right RLN divides off the vagus and passes around the right subclavian artery to travel to the larynx. The RLN supplies all the muscles of the larynx except the cricothyroid muscle, which is innervated by the external branch of the superior laryngeal nerve. The superior laryngeal nerve also has an internal branch that supplies sensation to the larynx above the true vocal cords. The RLN provides sensation below this area. The vagus nerve exits the skull base on both sides through the jugular foramen, not the carotid canal. The internal branch of the superior laryngeal nerve, not the RLN, enters the thyrohyoid membrane. The RLN travels along the tracheoesophageal groove and enters the larynx just superior to the cricoid cartilage. Nonrecurrent nerves occur most commonly on the right side in up to 1% to 2% of patients and can be associated with a retroesophageal right subclavian vein.
Answer
B
6 Which of the following statements is true regarding head and neck carcinogenesis and molecular therapy?
A A synchronous second primary tumor is defined as one developing within 1 year of the initial cancer.
B Human papillomavirus (HPV) has been shown to be a factor in the development of certain head and neck cancers.
C Cetuximab (IMC-C225) is a monoclonal antibody therapy targeted against transforming growth factor-β.
D p53 is commonly underexpressed in head and neck cancer.
E The most frequently mutated tumor suppressor gene in head and neck cancer is cyclin D1.
Ref.: 1, 2
Comments
Head and neck carcinogenesis is a complex process with multiple etiologic factors and a wide variety of genetic alterations that have been identified. The incidence of second primary tumors in head and neck cancer is not insignificant (3% to 7%), and they should be surveyed for in the upper aerodigestive tract, esophagus, and lung at the time of initial diagnosis. Synchronous versus metachronous lesions are defined in relation to the time of diagnosis from initial discovery of the tumor; synchronous lesions are found within 6 months, with metachronous lesion being diagnosed after 6 months. In recent years, human papillomavirus has been identified as an etiologic factor in certain head and neck cancers, specifically the oropharynx. Protooncogenes are genes that produce proteins involved in normal cell regulation and function. Mutation of these genes, including those for epidermal growth factor receptor (EGFR), cyclin D1, and vascular endothelial growth factor (VEGF), occurs in head and neck cancer. Tumor suppressor genes such as p53 and p16-ARF encode proteins that halt tumor growth and carcinogenesis. Cetuximab is novel monoclonal antibody therapy that has been designed to target EGFR. Trials are ongoing regarding its efficacy in combination with standard treatments such as radiotherapy and chemotherapy. Mutated p53 is poorly degraded and therefore commonly overexpressed in head and neck cancer. It is the most commonly altered tumor suppressor gene in human cancers, with p16-ARF being the most commonly altered gene locus in head and neck cancer.
Answer
B
7 A 75-year-old man with a long history of tobacco use comes to the office with a newly discovered tongue mass. A 3-cm ulcerated lesion is noted on the right anterior aspect of the tongue. Biopsy of the lesion demonstrates SCC. CT of the neck with intravenous contrast enhancement shows an enlarged 2-cm lymph node in the level II region on the left side. Findings on chest radiography are clear. How would you stage this patient’s disease?
A T1N1M0
B T2N1M0
C T1N2cM0
D T2N2bM0
E T2N2cM0
Ref.: 1, 3
Comments
The T classification as defined by the AJCC refers to the primary tumor. Carcinoma of the oral cavity is staged according to size. T2 lesions are 2 to 4 cm, as in this patient. Oral cavity T staging is as follows: T1, less than 2 cm; T2, 2 to 4 cm; T3, greater than 4 cm; and T4, invasion of adjacent structures. Clinical staging of the neck has been made more accurate by high-resolution imaging (CT). Had this node been ipsilateral, it would have been staged as N1. However, since it is contralateral to the primary disease, it is classified as N2c. Table 15-1 applies to primary tumors of the oral cavity, oropharynx, hypopharynx, and larynx.
TABLE 15-1 Regional Lymph Nodes (N)
|
NX |
Regional lymph nodes cannot be assessed |
|
N0 |
No regional lymph node metastasis |
|
N1* |
Metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension |
|
N2* |
Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension; or in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension; or in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension |
|
N2a* |
Metastasis in a single ipsilateral lymph node more than 3 cm but not more than 6 cm in greatest dimension |
|
N2b* |
Metastasis in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension |
|
N2c* |
Metastasis in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension |
|
N3* |
Metastasis in a lymph node more than 6 cm in greatest dimension |
* Note: A designation of “U” or “L” maybe used for any N stage to indicate metastasis above the lower border of the cricoids (U) or below the lower border of the cricoids (L). Similarly, clinical/radiological ECS should be recorded as E- or E+, and histopathologic ECS should be designated EN, EM, or Eg.
Used with the permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual, Seventh Edition (2010) published by Springer Science and Business Media LLC, www.springer.com.
Answer
E
8 A 42-year-old nonsmoking man is evaluated at the office because of a new left-sided neck mass. He has no recent history of illness. On examination, he is afebrile with stable vital signs. The mass measures approximately 3 cm, and it is fixed and located on level II. It is nontender and nonpulsatile and does not exhibit any overlying skin changes. The rest of his head and neck examination is unremarkable, including flexible fiberoptic examination of the larynx and hypopharynx. CT of the neck with intravenous contrast enhancement demonstrates an isolated enlarged 3-cm lymph node at level II with no other masses or abnormalities detected. Select the most appropriate next step.
A Bone marrow biopsy to evaluate for suspected lymphoma
B Positron emission tomography (PET)
C Excisional biopsy of the lymph node
D Fine-needle aspiration (FNA) of the lymph node
E Magnetic resonance imaging (MRI) of the neck with and without gadolinium contrast enhancement
Ref.: 1, 2, 4
Comments
A new-onset enlarged cervical lymph node in an adult with no previous history of infection is highly suggestive of metastatic cancer until proved otherwise. The next most appropriate step in diagnosis is to perform a fine-needle aspiration biopsy. This is the most useful diagnostic step in the work-up of a cervical neck mass. Bone marrow biopsy would be useful in staging after establishing the diagnosis of a hematologic malignancy such as lymphoma. The role of PET in head and neck cancer is still being elucidated. It may be useful to assist in searching for the site of an unknown primary lesion. Other current uses of PET include assessment of a patient’s response to treatment and staging and metastatic surveillance. MRI would probably not add any additional useful diagnostic information. Excisional biopsy is not suitable as the initial diagnostic step since it may compromise appropriate definitive therapy such as neck dissection and has been shown to increase local cervical recurrence. Excisional biopsy is indicated when FNA suggests the diagnosis of lymphoma and further subtyping and classification are needed, if initial and repeat FNA biopsies are inconclusive, or if the FNA results are benign but there is high clinical suspicion for malignancy.
Answer
D
9 A 67-year-old man has a 2-month history of a new-onset right level II neck mass. FNA biopsy is performed and demonstrates SCC. Office examination of the head and neck fails to demonstrate a primary tumor site. CT confirms the enlarged node with no additional information. PET also shows increased uptake at the site of the lymph node with no other activity noted. What is the next most appropriate step in management?
A Endoscopy under anesthesia with guided biopsies and bilateral tonsillectomy
B Neck dissection
C Irradiation of the neck and upper aerodigestive tract
D Excisional node biopsy
E Repeated FNA
Ref.: 1, 2
Comments
A large number of patients with metastatic cervical lymphadenopathy of unknown origin will have their primary tumors identified during the office examination. For patients such as this one, in whom the primary site is not apparent, endoscopy of the upper aerodigestive tract under anesthesia should be performed. If no obvious mucosal lesion is detected, one should proceed with directed biopsies of the most likely primary sites. The site of the metastatic node can give some insight into the location of the primary tumor. Oropharyngeal cancers drain to the level II region and would be an area of concern in this patient. Nodes in the lower neck region might raise suspicion for a tumor below the clavicles. The work-up should proceed with a biopsy of the tonsils by tonsillectomy, with additional biopsy samples taken of the base of the tongue, piriform sinuses, and nasopharynx. These are the most common locations for a primary site of an unknown SCC of the head and neck. CT and PET were appropriate but did not add any additional clinical information. Neck dissection or radiation therapy (or both) may be the eventual therapy in this patient, but not before a thorough investigation for the primary site is performed. Excisional node biopsy would be appropriate only if FNA has been inconclusive. Repeated FNA is not needed since the diagnosis has already been established.
Answer
A
10 Which of the following has not been shown to be a risk factor for the development of head and neck cancer?
A Tobacco use
B Alcohol abuse
C Inhalation of heavy metal dust
D Plummer-Vinson syndrome
E High-fat diet
Ref.: 1, 3
Comments
The two largest risk factors for the development of squamous cell carcinoma of the head and neck are tobacco and alcohol abuse. Occupational exposure to heavy metals and wood dust has been shown in some studies to increase the risk for sinonasal cancers. Exposure to ultraviolet light is associated with an increased risk for cutaneous malignancies of the head and neck, as well as lip cancer. Intake of salted fish and exposure to Epstein-Barr virus (EBV) have been associated with the development of nasopharyngeal carcinoma. Dietary and nutritional factors have a link with certain head and neck malignancies. Iron deficiency, as seen in Plummer-Vinson syndrome, has been linked to an increased risk for oral cavity and hypopharyngeal carcinoma. Although there may be a connection between fat intake and head and neck cancer, such an association has yet to be shown in any evidence-based medical studies. HPV infection has been studied extensively in regard to its relationship with cervical cancer. Recently, there has been great interest in its association with head and neck cancers, especially oropharyngeal cancer, as well as oral cavity and laryngeal cancers.
Answer
E
11 A 75-year-old man with T2N0M0 SCC of the lower lip undergoes primary resection of the tumor, with full-thickness resection resulting in a defect involving about 55% of the central lower lip but not involving the oral commissure. Which of the following is the best option for reconstruction of the defect?
A Primary closure
B Abbe two-stage cross-lip transfer flap
C Radial forearm free flap transfer
D Nasolabial transposition flap
E Estlander flap
Ref.: 1, 2
Comments
The lip begins at the vermillion border and is a subsite of the oral cavity. Risk factors for lip carcinoma include sun exposure and tobacco use. The lower lip is by far the most common site of tumor development, with squamous cell carcinoma being the most common pathology. Basal cell carcinoma is the most frequent pathology found on diagnosis for upper lip cancers. Initial evaluation should include testing for mental nerve involvement, evaluation for mandibular invasion, and examination of the cervical lymphatics. CT can be useful, especially in staging the mandible and cervical nodes.
Treatment of early-stage disease can consist of either primary external beam radiation or surgical resection. Primary excision is typically the favored treatment. Elective lymph node neck dissection for a clinically negative neck is performed in patients with advanced T stage disease or in the setting of deep tumor invasion in which the risk for occult cervical lymph node disease is elevated. Therapeutic neck dissection is appropriate in patients with positive nodal disease. Indications for postoperative irradiation include advanced T stage, positive margins, perineural/perivascular invasion, multiple or bulky nodal disease, and invasion of bone. Fortunately, given its location, many lip cancers are detected early and can be treated with a high success rate. Stage I and II lesions have a 90% 5-year survival rate. The survival rate drops to about 50% in patients with cervical lymph node involvement.
Reconstructive options following excision of carcinoma of the lip generally depend on the location of the lesion (medial versus lateral with involvement of the oral commissure) and the size of the defect. Smaller lesions that involve less than a third to half of the lip can be closed primarily with local advancement of the tissue. Larger defects involving between half and two thirds of the lip will probably require donated tissue such as a pedicled two-stage cross-lip transfer flap. An Abbe flap is used for central defects, whereas Estlander-style flaps are used for lateral defects. Larger defects can be repaired with local advancement techniques, local rotational flaps, or distal free flaps.
Answer
B
12 A 55-year-old male smoker, otherwise healthy, has a 3-cm ulcer on the left lateral border of the anterior aspect of his tongue with no involvement of the floor of the mouth or mandible. Biopsy demonstrates SCC with a 6-mm depth of tumor invasion. CT of his neck shows no evidence of cervical lymphadenopathy. His remaining metastatic work-up is negative. Which of the following choices is the best option for treatment?
A Concomitant chemotherapy and external beam radiation
B Partial glossectomy with left supraomohyoid neck dissection
C Total glossectomy with left supraomohyoid neck dissection
D Primary chemotherapy with 5-fluorouracil and cisplatin
E Total glossectomy with bilateral modified radical neck dissection
Ref.: 1, 3
Comments
The oral tongue is the most common site for cancer of the oral cavity. Most tongue cancers develop on the lateral border, as in this example. SCC is by far the most common pathology, but other malignancies may also occur. Verrucous carcinoma is a variant of SCC; it is described as having pushing borders with a very low propensity toward metastasis. Other nonepidermoid malignancies can include adenoid cystic carcinoma, Kaposi sarcoma, lymphoma, and melanoma. Cancer of the tongue is staged according to the same system as used for other oral cavity malignancies: T1, less than 2 cm; T2, 2 to 4 cm; T3, greater than 4 cm; and T4, invasion of adjacent structures.
Treatment of the primary site for early-stage (T1/T2) tongue cancer can consist of either primary surgical excision or radiation therapy. Advanced cancers are generally treated with multimodality therapy involving surgery and postoperative radiotherapy with or without chemotherapy. Chemotherapy alone has very poor results and is not a standard option for care. Primary excision with partial glossectomy or hemiglossectomy leaves a defect that requires some type of reconstruction. Smaller defects can usually be repaired by either primary closure or secondary intention. Larger defects may require a split-thickness skin graft. Large resection involving a majority of the tongue may need a regional (e.g., pectoralis major) or distant flap (e.g., radial forearm). Postoperative radiation therapy is indicated for patients with positive margins, advanced-stage tumors, extracapsular nodal spread, perineural/perivascular invasion, bulky or multiple nodal involvement, and deep muscular/bone invasion.
Therapeutic neck dissection is indicated for grossly positive nodal disease. Since patients with oral tongue cancer have a high rate of occult cervical metastases, even in a clinically N0 neck, elective neck dissection may be indicated for early-stage T1 tumors. Rates higher than 20% have led to a recommendation for limited supraomohyoid dissection—levels I, II, and III—in almost all patients. Factors that increase the risk for occult metastases include the depth of invasion, with depths greater than 4 to 5 mm showing an increased risk for occult metastatic disease. Sentinel lymph node biopsy is currently under investigation for its role in the treatment of N0 stage necks in patients with cancer of the oral cavity.
Answer
B
13 A T4N0M0 SCC in the midline anterior floor of the mouth is recently diagnosed in a 72-year-old man. The tumor is approximately 2.3 cm in diameter but is invading anteriorly into the cortical bone of the mandible. What is the best option for treatment in this patient?
A Local resection with curettage of involved bone
B Composite tumor resection with total mandibulectomy and bilateral radical neck dissection
C Primary external beam radiation therapy
D Composite tumor resection with segmental mandibulectomy and bilateral selective neck dissection
E Primary chemotherapy
Ref.: 1, 3
Comments
The floor of the mouth is a subsite of the oral cavity. The staging system used is the same as for all other cancers of the oral cavity. In this patient, although the size (2 to 4 cm) would stage it as a T2 cancer, invasion into cortical bone qualifies as T4 disease. The floor of the mouth is defined anatomically as extending from the lower alveolar ridge to the ventral surface of the tongue. Posteriorly, it is bounded by the anterior tonsillar pillars. Overall, treatment of cancer in the floor of the mouth is primarily surgical. Radiation therapy is less effective in patients with deep invasion of bone or muscle, as in the patient in this example. Primary radiation treatment of the mandible also carries the risk of osteoradionecrosis. All patients undergoing radiation therapy that will encompass the oral cavity should receive a pretreatment dental evaluation so that any carious teeth that would predispose to this complication can be removed. In regard to surgical treatment of the floor of the mouth, primary composite resection of the involved area with 1-cm margins is usually appropriate. In oral cavity cancers, the mandible can prevent surgical access to the tumor, or it may be involved by tumor. For surgical access, mandibular osteotomy or visor flaps may be needed. When tumor approaches the bone but does not directly invade it, marginal resection of the inner or outer cortex of the bone can be done. The periosteum itself serves as a barrier to tumor invasion and can be considered a margin of resection. When direct cortical invasion has occurred, en bloc segmental resection is required. Surgical resection involving the floor of the mouth, tongue, and mandible is classically referred to as a “composite” or “commando” resection. The neck is treated similar to that for other tumors of the oral cavity. Grossly positive metastatic disease is treated by therapeutic modified radical neck dissection. Elective neck dissections are recommended for clinical N0 disease in most tumors, especially if advanced stage or deeply infiltrative. Radiotherapy as a primary treatment can be used when there is a significant contraindication to surgery. It is also used in the postoperative adjuvant setting for advanced-stage disease. Overall survival rates range anywhere from 64% to 95% for stage I disease to 6% to 52% for stage IV cancer. This patient has significant involvement of bone with direct invasion and requires a composite resection. The neck is clinically negative (N0) for metastatic disease, so bilateral elective supraomohyoid neck dissection is indicated for treatment. Radical neck dissection would be performed in the case of bulky metastatic cervical disease. External beam radiation can be used for early-stage tumors but is probably not the favored option, especially in light of the deep bone invasion. Primary chemotherapy has not been shown to be effective in treating cancer of the floor of the mouth.
Answer
D
14 A 62-year-old woman is seen in your office with a 1-cm painless mass involving the hard palate. You develop a differential diagnosis. Which of the following diagnoses is least likely in this location?
A SCC
B Granular cell tumor
C Necrotizing sialometaplasia
D Adenoid cystic carcinoma
E Lipoma
Ref.: 1, 3
Comments
There is no fat pad in this subsite of the oral cavity, unlike the buccal space and other areas of the head and neck, and therefore a lipoma should not be on the differential diagnosis. All the other diseases listed commonly occur in this area and should be considered when confronted with a mass in this area. Biopsy is usually warranted for diagnosis. Many benign lesions can mimic cancer of the hard palate. Necrotizing sialometaplasia is a self-limited inflammatory disease of the minor salivary glands that can be mistaken for carcinoma given its ulcerative appearance. No treatment is required. The palate is the most common site of Kaposi sarcoma in the oral cavity and should be considered in any patient with immunosuppression. Minor salivary gland tumors and SCC are both common malignancies in this region. Cancer at this site is rare in the United States, where it accounts for 0.5% of oral cavity malignancies. It is much more common in India because of the high incidence of betel nut chewing. Treatment of cancer of the hard palate usually involves local resection. Typically, surgery is favored over radiation therapy for early-stage lesions given the risk for osteoradionecrosis. More advanced tumors may require partial or total maxillectomy. It is generally thought that the incidence of occult metastatic cervical disease is low with hard palate tumors, so elective neck dissection is not indicated in most cases. Advanced-stage tumors generally receive combined-modality therapy consisting of surgery and adjuvant radiation therapy.
Answer
E
15 Which of the following statements is true regarding cancer of the oropharynx?
A HPV is a risk factor.
B Oropharyngeal cancer commonly metastasizes to level I of the neck.
C Concurrent treatment with chemotherapy and radiation therapy has little role in the management of advanced-stage oropharyngeal cancer.
D Subsites of the oropharynx include the base of the tongue, tonsils, soft palate, and adenoids.
E Extensive resection of the base of the tongue increases the possibility of postoperative velopharyngeal insufficiency.
Ref.: 1, 3, 5
Comments
The oropharynx consists of several subsites, including the base of the tongue, tonsils, soft palate, and posterior pharyngeal wall. The adenoids are located in the nasopharynx. The oropharynx serves an important functional role in speech and swallowing. Extensive surgical resection in this area can lead to severe deficits. Besides the universal risk factors of tobacco and alcohol use, recent evidence has begun to suggest a role for HPV in the development of some oropharyngeal carcinomas. Most tumors of the oropharynx are SCC, but lymphoma and salivary gland neoplasms can also arise in this region. Cancers of the oropharynx most commonly metastasize to levels II, III, and IV of the neck, as well as the retropharyngeal nodes. Bilateral metastases are common, especially with lesions on the base of the tongue and palate. Many patients with oropharyngeal cancer may initially have a neck mass from an unknown primary site. Especially if this node is located in the level II region, the base of the tongue and tonsil should be highly suspected as the primary site. Cystic neck masses in an adult should always arouse concern for a possible metastatic oropharyngeal cancer and not be assumed to be a branchial cleft anomaly. Treatment of oropharyngeal cancer has evolved over the years. Traditional surgical approaches have included transcervical, transpharyngeal, and transmandibular routes for advanced tumors. More recently, transoral laser microsurgery has been introduced as a treatment option and has shown some promising early results. Concurrent treatment with chemotherapy and radiotherapy has been used as primary management of advanced disease with good results. There are no conclusive data to date regarding the superiority of surgery with postoperative radiation therapy over concurrent chemotherapy and radiation therapy. This is especially true in light of the rapidly advancing field of transoral laser surgery. Patients who do undergo more traditional surgical approaches can have large surgical defects requiring advanced reconstruction, including regional and distal flaps. In addition, external beam radiation can cause changes in the tissue and musculature that leave the patient with permanent oropharyngeal dysphagia. The soft palate is important in preventing regurgitation of food and liquids into the nose, as well as in contributing to normal speech that does not sound hypernasal. Patients who undergo resection of the soft palate can be fitted with a prosthesis called an obturator to allow improved velopharyngeal function.
Answer
A
16 Which of the following statements is most accurate regarding treatment of SCC of the larynx?
A The most common location of carcinoma in the larynx is the subglottis.
B Advanced-stage bulky tumors are best treated with transoral laser microscopic surgery.
C Vocal cord fixation qualifies a tumor as a T4 carcinoma.
D Patients undergoing open conservation laryngeal surgery should be assessed preoperatively for adequate pulmonary function.
E T2 cancers of the glottis are most commonly treated with multimodality therapy.
Ref.: 1, 3
Comments
Laryngeal carcinoma is an extensive topic with a complex set of treatment approaches. It is the second most common noncutaneous head and neck cancer after cancer of the oral cavity. Glottic cancer is the most frequent, followed by supraglottic, with subglottic cancers being relatively uncommon. Hoarseness and otalgia are common initial symptoms. The diagnosis is made by flexible laryngoscopy in the office, with confirmatory biopsy of the tumor usually done in the operating room (OR). CT of the neck assists in staging, in addition to evaluation of the chest with either CT or bronchoscopy. The lungs are the most common site of distant metastases. Nodal metastases are much more common in supraglottic than in glottic cancer. The most frequent areas of spread are levels II, III, and IV. Elective neck dissection is usually recommended for T3 glottic and T2 supraglottic cancers. T staging of laryngeal tumors is complex. A general overview is as follows: T1, limited to one subsite; T2, extends to a second subsite; T3, vocal cord fixation; and T4, extralaryngeal spread. Squamous cell carcinoma is the most common pathology, as with other sites in the head and neck. Malignancies can arise from any type of tissue origin in the larynx, including salivary, cartilage, neuroendocrine, and lymphoid tissue. Verrucous carcinoma differs from invasive SCC in that it has pushing rather than invasive margins. The larynx is the second most common site after the oral cavity. It has an extremely low propensity for spread to the cervical lymphatics. Treatment of the primary site in laryngeal cancer is based on the subsite involved, extent of tumor involvement, and individual patient factors. Early-stage tumors (T1 and T2) are treated in most cases with single-modality therapy consisting of either surgery or radiation therapy. Advanced lesions (T3 and T4) are treated with multimodality therapy, with the two main options being either chemoradiation therapy or surgery with postoperative radiation therapy. In regard to early-stage lesions, the decision to proceed with radiation therapy versus surgery is based on multiple factors, including patient preference, medical stability for surgery, anticipated voice quality after surgery, and the patient’s ability to comply with a 6-week course of radiation therapy. Early-stage tumors are commonly treated today with endoscopic transoral laser techniques. Laser excision of early-stage glottic lesions has a high cure rate, with reports in the 80% to 100% range for T1 and T2 lesions. Traditionally, advanced cancer of the larynx was treated by total laryngectomy with postoperative radiation therapy. Given the profound disability, social stigmatization, and negative psychological impact of this operation, laryngeal preservation with maintenance of the three functions of the larynx (respiration, phonation, and airway protection) is preferred. Conservation laryngeal surgery consists of both endoscopic and open techniques. Candidates for open conservation laryngeal surgery need to undergo a thorough preoperative evaluation of their pulmonary and cardiac function since these procedures will place the patient at an increased risk for aspiration. Traditional open conservative treatment of supraglottic cancers consists of a horizontal partial laryngectomy. Organ preservation in patients with advanced tumors is possible with nonsurgical therapy without any difference in survival. Total laryngectomy is indicated for patients with bulky advanced T4 disease, as salvage for failed conservative therapy, and in patients with a benign nonfunctional larynx after conservative treatment with repeated severe aspiration.
Answer
D
17 Which of the following statements is most accurate regarding the management of SCC of the hypopharynx?
A Hypopharyngeal carcinoma is most commonly initially seen at an early stage.
B The hypopharynx includes the piriform sinuses, posterior pharyngeal wall, and arytenoid cartilages.
C Ten percent of patients with hypopharyngeal carcinoma have palpable lymphadenopathy.
D Surgical therapy for advanced-staged hypopharyngeal carcinoma usually consists of total laryngopharyngectomy.
E Overall survival rates for patients with hypopharyngeal carcinoma compare favorably with those in patients with carcinoma of the glottis.
Ref.: 1, 3, 6
Comments
Hypopharyngeal cancers have a poor prognosis overall in comparison to other head and neck cancers. These cancers tend to initially be seen at later stages with early lymphatic spread. About 70% to 80% of patients have cervical metastatic disease. The subsites of the hypopharynx include the piriform sinus, posterior pharyngeal wall, and postcricoid region. Staging is similar to larynx cancer: T1, one subsite; T2, more than one subsite; T3, hemilarynx fixation; and T4, invasion of adjacent structures. Risk factors besides tobacco use include iron deficiency anemia, as seen in Plummer-Vinson syndrome. Conservation surgery—partial pharyngectomy without laryngectomy—is indicated in the absence of cartilage invasion and extension to the piriform apex in patients with a mobile vocal cord. Any further involvement is an indication for either partial or total laryngectomy, in addition to pharyngectomy. Transoral laser microsurgery shows promising results. However, total open laryngopharyngectomy with bilateral neck dissection is still indicated in many cases as treatment given the advanced stage in most patients. Routine assessment of esophageal involvement is mandatory. Organ preservation with chemoradiation therapy is also commonly used at many institutions as a first line of therapy.
Answer
D
18 A 47-year-old male immigrant from southern China has a complaint of right-sided hearing loss for the past 3 weeks. He has no history of a recent upper respiratory infection or chronic ear disease. His clinical history is otherwise unremarkable. Serous otitis media is noted in his right ear. In addition, a 1.5-cm level V lymph node is palpated in the left side of the neck. The rest of the physical examination is within normal limits. What is the next step in management?
A Treatment with amoxicillin for 10 days
B Flexible nasopharyngoscopic examination
C Ototopical antibiotic drops
D Oral and topical decongestants for 2 weeks with reexamination
E Observation with follow-up in 2 weeks if the symptoms do not resolve
Ref.: 1-3, 7
Comments
Any adult patient with a new onset of unilateral middle ear effusion and no related history of recent upper respiratory illness should undergo evaluation of the nasopharynx. Another clinical clue in this patient is the presence of a level V node, which is a common location for cervical metastasis from nasopharyngeal cancer. This is especially true in this patient given his history of a southern Chinese background. This area, particularly the Guangdong Province, has an increased incidence of nasopharyngeal carcinoma. The etiologic factors are multifactorial and include genetic and environmental factors. Infection with Epstein-Barr virus has been shown to have an etiologic role. In addition, dietary factors, including the intake of salted fish, have a strong association with the development of this disease. Nasopharyngeal carcinoma is divided by the World Health Organization into two groups, keratinizing versus nonkeratinizing carcinoma, with the second group including both differentiated and undifferentiated subtypes. The diagnosis of nasopharyngeal carcinoma is done by nasopharyngoscopy and biopsy. High serologic levels of IgA to EBV viral capsid antigen and early antigen are seen in patients with this disease. It has been advocated as a screening tool in high-risk populations based on a study showing a 5.4% diagnosis rate of subclinical nasopharyngeal cancer in patients with elevated IgA levels to EBV who live in the Guangdong Province. Treatment consists mainly of chemotherapy and radiation therapy. Surgery has a limited role in treating nasopharyngeal cancer in patients with limited primary site recurrence and nodal recurrence.
Answer
B
19 Which of the following statements is true regarding salivary gland tumors?
A Approximately 80% of submandibular gland tumors are malignant.
B The most common location for adenoid cystic carcinoma is the parotid gland.
C Treatment of a pleomorphic adenoma of the parotid gland usually involves radical parotidectomy.
D Adenoid cystic carcinoma has a high rate of lymphatic spread.
E The most common malignant salivary gland neoplasm is mucoepidermoid carcinoma.
Ref.: 1, 3
Comments
The study of salivary gland neoplasms begins with a review of anatomy. The salivary glands consist of major and minor glands. The major glands include the parotid, submandibular, and sublingual glands. Minor glands are scattered throughout the upper aerodigestive tract. The majority of neoplasms (70% to 80%) overall arise in the parotid gland, followed by the submandibular and minor glands. Nearly 80% of parotid tumors are benign. There is an approximately equal distribution of submandibular tumors, with minor gland tumors having an opposite distribution consisting of about 80% being malignant. Initial diagnosis of a salivary gland neoplasm can involve FNA biopsy and CT, although some advocate proceeding directly with excision. Warning signs of a possible malignancy include pain, rapid growth, nodal enlargement, and facial nerve paralysis.
The most common neoplasm overall in the parotid gland is a pleomorphic adenoma. It represents about two thirds of all salivary gland neoplasms. Treatment consists of resection via parotidectomy. Most lesions arise in the tail of the parotid, and lateral lobe parotidectomy is typically required for treatment. A Warthin tumor (papillary cystadenoma lymphomatosum) is the second most common benign tumor that arises in the parotid gland. Up to 10% of tumors are bilateral, with smoking shown to be a risk factor for the development of these lesions. They are noted to concentrate technetium-99m, which can aid in diagnosis. The most frequent malignant tumor overall is mucoepidermoid carcinoma, and it is the most common malignancy in the parotid gland. It is graded from low to high, with higher-grade lesions behaving very aggressively, similar to SCC. Treatment consists of total parotidectomy. Radical parotidectomy with resection of the facial nerve is typically indicated only in patients with gross nerve invasion and loss of function. Elective treatment of the neck is advocated in patients with advanced T stage or high-grade disease. Adenoid cystic carcinoma is the malignancy found most frequently in the submandibular and minor salivary glands. Its most common primary location is the oral cavity. These tumors are notorious for perineural spread, and they also commonly metastasize to the lung. Because these distant metastases can develop decades in the future, a yearly chest radiograph is recommended. Treatment consists of excision, but elective treatment of the neck is unnecessary given the low incidence of cervical spread.
Answer
E
20 Which of the following statement is most accurate regarding the use of chemoradiation therapy for head and neck cancer?
A Chemotherapy can be used as single-modality primary therapy with intent to cure in many head and neck cancers.
B Induction chemotherapy plus radiation therapy had superior overall survival results when compared with surgery plus radiation therapy for the treatment of advanced-stage laryngeal cancer.
C Postoperative concomitant chemotherapy with radiation therapy improves overall survival in comparison to postoperative radiation therapy alone in high-risk locally advanced head and neck cancer.
D Chemotherapy has no role in the palliative setting for metastatic head and neck cancer.
E Chemotherapy in the postoperative adjuvant setting in conjunction with radiation therapy has the advantage of improving survival while not increasing mucosal toxicity.
Ref.: 1, 8-12
Comments
Chemotherapy has developed an increasing role over the past two decades in the treatment of head and neck SCC. For early-stage patients, treatment consists of either radiation therapy or surgery, with chemotherapy having little to no role in treatment. It is never used as a primary single-modality treatment for head and neck cancer with intent to cure. For patients with advanced metastatic or recurrent disease, chemotherapy can be used in the palliative setting to inhibit tumor growth for a limited effective period. Its main role is in the treatment of locoregionally advanced stage III/IV cancer. A second role in this group of patients is for organ preservation. Patients with advanced primary T stage are best served by total laryngectomy. For advanced-stage unresectable tumors, concurrent chemoradiation therapy, in comparison to radiation therapy alone, has shown improved locoregional control with questionable overall survival benefit.
Answer
C
21 A 34-year-old woman is seen in the office with a 3-month history of a left-sided neck mass and pain with mastication. On examination, a 3-cm nontender mass is present at level II; it moves laterally but not in the craniocaudal direction. CT with intravenous contrast enhancement demonstrates a 3.5-cm mass at the carotid bifurcation. A follow-up angiogram is obtained:
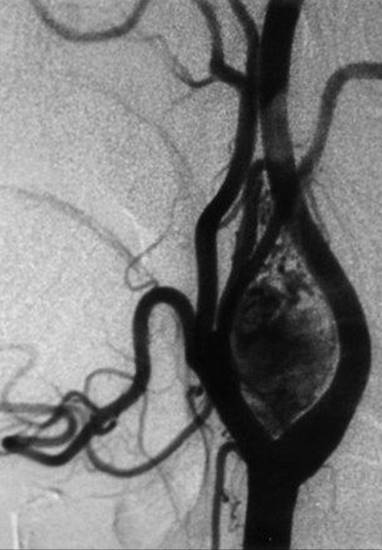
Which of the following statements is most accurate regarding this case?
A It represents the most common paraganglioma in the head and neck.
B The rate of malignancy is about 30%.
C The majority of these lesions show functional secretion of catecholamines.
D FNA biopsy is indicated to rule out malignancy.
E Radiation therapy is the most effective treatment of these lesions.
Ref.: 1, 2
Comments
A carotid body tumor is the most common paraganglioma in the head and neck. Other paragangliomas that occur in this region include the vagal and jugulotympanic types. The majority of paragangliomas are solitary and nonfamilial. Multicentricity is reported in about 10% of cases, with about a 6% rate of malignancy. Only about 1% to 3% of them are considered functional and can be evaluated with a 24-hour urine collection for analysis of catecholamines. The “Fontaine sign” refers to mobility in only the lateral direction on palpation, whereas pain occurring with chewing is called “first-bite syndrome.” Histopathologic evaluation of this tumor demonstrates two types of cells: type I, chief cells/granular cells; and type II, sustentacular supporting cells. Unlike most head and neck tumors, malignancy is not diagnosed by the presence of dysplastic changes in the primary tumor. The presence of metastatic disease either to the regional cervical lymphatics or to distant sites is the only diagnostic criteria. Imaging is the major modality for primary diagnosis since needle biopsy is contraindicated. CT will show a hypervascular mass at the carotid bifurcation, with MRI demonstrating a classic “salt and pepper” appearance on T2-weighted sequences because of hemorrhage and flow voids. On angiography, the internal and external carotid arteries will be bowed apart, a finding referred to as a “lyre sign.” These tumors are best treated surgically, and vascular reconstruction may be necessary. Radiation therapy can stop the growth of these lesions but not shrink their size. Patients should be aware of the potential risk of injury to the vagus.
Answer
A
22 A 66-year-old man with T3N2bM0 SCC on the base of the tongue undergoes concomitant chemotherapy and external beam irradiation for a total of 6 weeks. At the end of treatment he is noted to have a persistently enlarged, left neck level II lymph node about 5 cm in size, for which salvage surgical therapy and standard radical neck dissection are planned. Which of the following is true?
A The phrenic nerve is commonly injured during surgery.
B Radical neck dissection includes removing the internal jugular vein, SCM muscle, and vagus nerve.
C The patient will probably need postoperative physical therapy for his shoulder.
D Resection of the internal carotid artery is a common component of this surgery.
E Level VI is part of a radical neck dissection.
Ref.: 1, 2, 13
Comments
Neck dissection involves removal of the cervical lymphatic tissue and related structures for the treatment of head and neck cancer. Radical neck dissection involves removing all of the cervical lymphatic tissue in neck levels I through V, in addition to removing the internal jugular vein, SCM muscle, and spinal accessory nerve. A modified radical neck dissection is performed for the same clinical indications as a radical neck dissection. The differentiating feature is that it preserves at least one of the following: the internal jugular vein, SCM muscle, or spinal accessory nerve. Level I through V lymph nodes are removed as for a traditional radical neck dissection. However, it is frequently possible to preserve one of the major structures just listed, especially when it is not involved with tumor. Particularly in the case of the spinal accessory nerve, this is preferable to prevent postoperative shoulder dysfunction from denervation of the trapezius muscle. The patient in this scenario will most certainly need postoperative physical therapy because of sacrifice of CN XII with his surgery.
Selective neck dissection is used for removing a limited number of lymph node levels, as opposed to resecting levels I through V. Furthermore, the internal jugular vein, SCM muscle, and CN XII are preserved. The philosophy behind performing this type of dissection is to remove the clinically uninvolved lymphatic groups thought to be most at risk for future metastatic disease. Therefore, the type of dissection is predicated on where the primary tumor is located. Oral cavity cancers typically metastasize to levels I, II, and III. These levels would be included in what is termed a supraomohyoid selective neck dissection. Laryngeal, hypopharyngeal, and oropharyngeal cancers commonly spread to levels II, III, and IV, which would be incorporated into a lateral selective neck dissection. Posterolateral neck dissection (levels II, III, IV, and V) is most commonly used in the setting of cutaneous malignancies involving the posterior region of the scalp.
Sentinel lymph node biopsy is under investigation for its efficacy in SCC of the head and neck. It is currently used in the management of cutaneous melanoma of the head and neck. The internal carotid artery, however, is not considered a standard part of routine neck dissection, and there is controversy regarding the utility and benefit of resection. The phrenic nerve is at risk when dissecting along the floor of the neck. A level VI or central compartment dissection is not part of a standard radical neck dissection. It is typically used in patients with thyroid tumors, tracheal tumors, or laryngeal cancers with extensive subglottic extension.
Therapeutic neck dissection has been used to treat positive metastatic cervical disease (N+) through either a radical or a modified radical neck dissection. Currently, some surgeons are beginning to advocate for the use of more limited selective neck dissection if the patient has limited N1 disease. In addition to being used as primary treatment, it also can be used as salvage treatment after failed nonsurgical therapy, such as external beam radiation. For patients with clinically negative disease in the neck (N0), elective neck dissection can be performed to target the most likely sites of metastatic drainage. Such dissection is based on the primary site of the tumor. Sentinel lymph node biopsy in the treatment of SCC of the head and neck is currently under investigation and not yet advocated widely as a proven standard of care.
Answer
C
23 A 65-year-old man is seen in the emergency department with angioedema of the tongue. Flexible laryngoscopy demonstrates a severely edematous larynx with no visible glottic space. Worsening stridor, severe agitation, and panic develop, and the patient begins to desaturate with a nasal trumpet in place and a 100% O2 nonrebreather mask. What is the next step in management?
A Emergency beside tracheostomy or cricothyrotomy
B Transfer of the patient immediately to the OR for urgent tracheostomy
C Mild sedation of the patient with midazolam, an attempt at direct laryngoscopy with intubation, and if unsuccessful, proceeding with tracheostomy at the bedside
D Flexible fiberoptic intubation
E Racemic epinephrine nebulizer treatment
Ref.: 1
Comments
Creation of a surgical airway or “tracheostomy” is one of the most fundamental skills in the management of upper airway pathology. There are three major indications for a tracheostomy: upper airway obstruction, chronic respiratory failure, and management of poor pulmonary toilet. The timing of a tracheostomy can be categorized into three groups. Emergency tracheostomy or cricothyrotomy is required in patients with imminent airway obstruction, as in this example. A cricothyrotomy is the most rapid form of surgical airway control but does require conversion to a formal tracheostomy because of the high risk of subglottic stenosis developing. This patient has no evidence of an identifiable airway on fiberoptic examination and therefore cannot be intubated fiberoptically, but he is beginning to desaturate secondary to his airway obstruction and will probably decompensate at any moment; therefore, there is no time to make arrangements in the OR. An urgent tracheostomy done in the OR setting is always preferable if possible. Sedating the patient will inhibit spontaneous ventilation, promote further upper airway collapse, and worsen an already precarious airway scenario. Direct intubation will also probably be unsuccessful because of the patient’s tongue edema. Racemic epinephrine can decrease laryngeal/subglottic edema but will be of little immediate help in this setting.
An elective tracheostomy is commonly done for chronic respiratory failure and for improving pulmonary toilet. In patients with chronic respiratory failure, a tracheostomy decreases anatomic dead space ventilation, allows improved pulmonary toilet, and decreases the risk for laryngeal stenosis and the formation of granulation tissue from pressure by the endotracheal tube. Percutaneous tracheostomy has become an alternative to conventional tracheostomy in carefully selected patients. Bronchoscopic monitoring augments the safety of the procedure, which is frequently done in the intensive care unit. A smaller incision and the use of a dilator facilitate introduction of the cannula. Many surgeons still prefer an open traditional tracheostomy in all cases. Once the patient’s medical status has stabilized and the initial indication for tracheostomy is resolved, decannulation can be considered after evaluation of the larynx to confirm good function of the vocal cords and a patent airway.
Answer
A
24 A 68-year-old woman with chronic respiratory failure underwent a tracheostomy for long-term ventilator support. The procedure went uneventfully and the patient was discharged to a long-term care facility after an initial tracheostomy tube change 1 week later. The patient is readmitted 2 weeks later with a report at the nursing facility of a 1-minute episode of brisk bright red bleeding from the tracheostomy site that resolved without intervention. Her hemoglobin concentration is 10.2 g/dL, and coagulation studies are normal. What is the most likely diagnosis?
A Pneumonia
B Tracheitis
C Bleeding of granulation tissue in the stoma
D Tracheoinnominate fistula
E Bleeding from the anterior jugular vein
Ref.: 1, 2
Comments
This is a case of classic “sentinel” bleeding that occurs before full rupture of the innominate artery. It can occur with a low tracheostomy or high innominate artery with erosion of the anterior tracheal wall as a result of pressure necrosis. Fiberoptic examination of the area should be performed to evaluate the situation. If there is obvious evidence of erosion, the patient might need a sternotomy and mediastinal exploration. If the index of suspicion is lower or the examination is inconclusive, diagnostic imaging with high-resolution CT or angiography (or both) may be appropriate. This complication carries an extremely high mortality rate if blowout occurs. Attempts to control active bleeding can consist of direct digital pressure or inflation of a cuffed tube directly over the area for tamponade. Any of the other choices would not cause rapid-onset bright red bleeding. Bleeding from the anterior jugular veins usually occurs immediately in the postoperative setting if they were not ligated adequately during surgery. Other complications of tracheostomy in the early period include infection, pneumothorax, bleeding, and tube obstruction. Later complications can include wound breakdown, formation of granulation tissue, tracheal stenosis, tracheoesophageal fistula, and tracheoinnominate fistula, as just described.
Answer
D
25 A 61-year-old man with T3N2cM0 SCC of the supraglottic larynx undergoes total laryngectomy with left radical neck dissection/right modified radical neck dissection and primary pharyngeal closure without any intraoperative complications. Tube feeding is started on postoperative day 2. On day 3 the patient is noted to have increasingly high output of yellow/cloudy fluid from the left neck drain recorded to be 400 mL over the past 24 hours. The hemoglobin concentration and white blood cell count are stable. The patient is afebrile with no signs of infection at the surgical site. What is the next most appropriate step in management?
A Immediate reexploration and closure of the pharyngeal fistula
B Thoracotomy with clamping of the thoracic duct
C Closed wound drainage, pressure dressings, and tube feeding consisting of medium-chain triglycerides
D Continuation of the current postoperative management
E Removal of the left neck drain with a pressure dressing applied to the wound
Ref.: 2
Comments
This patient has a chylous fistula. The initiation of tube feeding provided lipids to the lymphatic system, which increased the volume of chyle flow. Pharyngeal fistulas do not generally develop this early in the postoperative course and do not usually have such extremely high drain output. However, it is always something to consider after a pharyngeal repair. Chylous fistulas typically occur in the left side of the neck during radical neck dissections when dissecting low in the level IV/V region. The incidence is about 1% to 2%. If recognized at the time of surgery, they should be repaired immediately with ligature. If they occur in delayed fashion, such as in this patient, they can usually be initially managed conservatively, as stated in choice C. The rationale for using medium-chain triglycerides is that they are absorbed directly through the portal circulation and not the lymphatic system. Another nutritional alternative in more severe cases is the use of total parenteral nutrition. In regard to deciding on surgical management, a general guideline accepted by many physicians is greater than 600 mL of output over a 24-hour period. Reexploration with control of the leak can be very difficult given the delicate nature of lymphatic tissue.
Answer
C
26 A 71-year-old female tobacco user undergoes a salvage total laryngectomy with bilateral radical neck dissection and primary closure of her pharynx. This was performed after failed treatment with primary concurrent chemotherapy and external beam radiation. On postoperative day 6, breakdown of the wound occurs with a resulting 1- by 2-cm defect, just lateral to the stoma, and salivary drainage from the wound. Initial treatment consists of culture-directed intravenous antibiotic therapy, local wound care, and use of a Penrose drain for control of the drainage. Later on that same day, bright red blood is noticed on the wound dressing. Which of the following factors is most important in the development of these complications?
A Age of the patient
B Tobacco use
C Bilateral versus unilateral neck dissection
D Previous radiation therapy
E Carotid injury during dissection of the neck
Ref.: 2
Comments
A postoperative pharyngocutaneous fistula has developed in this patient, along with probably carotid artery rupture secondary to local infection and breakdown of the vessel wall. Although age and tobacco use are important factors in wound healing, a previous history of external beam radiation therapy in a patient undergoing total laryngectomy places that individual at much higher risk for a postoperative pharyngocutaneous fistula. Rates of postoperative fistula formation have been reported to be anywhere from 30% to 60% in patients with a history of radiation therapy. The general medical status of the patient needs to be evaluated in regard to nutrition and underlying medical problems such as diabetes so that these factors can be optimized as much as possible before surgery. A vascularized tissue flap should be considered in these patients. Carotid blowout is a deadly and feared complication of neck dissection. A salivary fistula with wound infection is a strong predisposing factor. Again, the use of vascularized tissue flaps can aid in preventing fistulas. This clinical scenario is highly suggestive of an evolving carotid blowout. Immediate management includes the application of direct pressure to the wound, administration of fluids and blood products as needed, and surgical exploration. In the case of a large infected field, a segment of the carotid artery may need to be resected.
Answer
D
27 A 55-year-old man with advanced-stage SCC of the larynx is undergoing total laryngectomy with bilateral modified radical neck dissection. While dissecting on the right side you inadvertently enter the internal jugular vein and proceed to clamp the vessel with the intention of ligating it for hemostatic control. Shortly thereafter, the patient is noted to be hypotensive. Bilateral breath sounds are auscultated, but a mill wheel murmur is heard over the precordium. What is the next step in management?
A Place the patient in the left lateral decubitus position and insert a central venous catheter.
B Place the patient in the right lateral decubitus position and insert a central venous catheter.
C Place the patient in the reverse Trendelenburg position.
D Call for an intraoperative chest radiograph.
E Pack the wound and place the patient in the prone position.
Ref.: 14
Comments
This patient has venous air embolism as a result of the internal jugular vein being inadvertently opened. With all surgeries above the heart there is a risk for air embolism. This is especially true in neurosurgical procedures, where there is significant elevation of the wound relative to the heart. In head and neck surgery, patients are typically placed in the reverse Trendelenburg position, which places them at additional risk for entrance of air into the venous system. A “mill wheel murmur” is the traditional finding on cardiac examination and may be detected on precordial Doppler ultrasound. The clinical manifestations can include cardiovascular, pulmonary, and neurologic findings. Cardiac findings can include tachyarrhythmias, right-sided heart strain, and myocardial ischemia. Pulmonary findings can include hypercapnia with decreased O2 saturation. Decreased cardiac output results in decreased cerebral perfusion, but direct air embolism to the central nervous system can occur through a patent foramen ovale. Initial treatment involves placing the patient in the left lateral decubitus position (Durant position) to try to force the air to stay in the right side of the heart in an attempt to prevent it from traveling into the pulmonary circulation. Placement of a central venous catheter with aspiration of air from the right atrium can also be attempted. Other supportive efforts may need to include cardiopulmonary resuscitation if the situation deteriorates. Hyperbaric oxygen therapy has been shown to be of benefit in some studies.
Answer
A
28 A 22-year-old man is brought to the emergency department by ambulance with a 2-day history of lower tooth pain and neck swelling. He was prescribed antibiotics by his primary care physician yesterday, but his condition had not improved overnight. This morning he felt his “throat beginning to close” and called the emergency medical service. He is febrile at 102° F with a heart rate of 105 beats/min, blood pressure of 110/70 mm Hg, and respiratory rate of 20 breaths/min. His white blood cell count is 38,000/mm3. On examination he is noted to have firm tender swelling of the submental region with skin erythema. In addition, severe edema of the floor of the mouth and tongue is present. His SaO2 is 100% on 40% O2 by face tent, and the patient is ventilating well, anxious, and sitting forward drooling. Flexible laryngoscopy shows no laryngeal edema. What is the next appropriate step in management?
A Intravenous antibiotics and steroids with close observation of the airway in the intensive care unit
B High-resolution CT of the neck with dye
C Immediate cricothyrotomy in the emergency department under local anesthesia
D Immediate transfer to the OR for awake fiberoptic intubation and be prepared for tracheostomy if needed
E Incision and drainage of a suspected neck abscess at the bedside
Ref.: 2
Comments
This patient has Ludwig angina, probably secondary to an odontogenic infection given the history of tooth pain. This condition involves a rapidly evolving soft tissue cellulitis that spreads through the fascial planes of the sublingual space, submandibular space, and anterior aspect of the neck. It can cause severe swelling of the floor of the mouth and tongue and possibly airway obstruction. Initial management in this patient should involve securing his airway. Emergency cricothyrotomy would be appropriate in the emergency department if the patient was currently decompensating and exhibiting obstruction and needed an airway immediately. He is ventilating well but drooling and posturing forward. This patient should be taken to the OR expediently to perform fiberoptic intubation and possible tracheostomy under controlled circumstances. At that point CT could be performed to evaluate for an abscess collection. Exploration of the neck at the bedside, especially without securing the airway, is unsafe and not appropriate. Tonsillitis is the most frequent cause of deep tissue neck infections in children with odontogenic sources, and intravenous drug injection is a more common cause in adults. Peritonsillar abscessesare the most commonly encountered. Classic signs and symptoms include drooling, hot potato voice, otalgia (from irritation of CN IX), and unilateral swelling of the soft palate with uvular deviation to the opposite side. Treatment includes drainage by transoral needle aspiration or incision and drainage with a scalpel blade. A parapharyngeal space abscess can be manifested in similar fashion to a peritonsillar abscess as severe throat and neck pain but without the appearance of soft palate/peritonsillar swelling. The tonsil may appear deviated medially. It is adjacent to many of the other spaces and can allow spread along the carotid sheath (“Lincoln Highway of the neck”) or damage to CNs IX to XII. Drainage is generally performed in a transcervical fashion if necessary. Retropharyngeal space abscesses are more common in young children and require some clinical suspicion to detect. Initial signs may include fever, lack of appetite, cervical adenopathy, and torticollis. This area can usually be approached transorally if the infection is limited but may require transcervical drainage. CT is mandatory to define its extent and to aid in planning access. The retropharyngeal space extends from the skull base to the mediastinum. The retropharyngeal space has a midline raphe that causes unilateral shifting, whereas the prevertebral space does not, with these collections appearing more midline.
Answer
D
29 A 15-year-old boy is taken to the emergency department with a 1-month history of recurrent right-sided epistaxis. He has had almost daily episodes, with some noted to be very difficult to stop with local pressure. He is currently bleeding from his right nostril and coughing up blood clots. The bleeding is able to be controlled with an 8-cm nasal pack. His vital signs are stable, he is resting comfortably, and blood is drawn for a complete blood count, which shows a hemoglobin level of 8.0 g/dL. What is the next step in management?
A Discharge the boy home with follow-up in 2 to 3 days for removal of the packing.
B Transfuse 2 units of packed red blood cells given the concern for possible further bleeding.
C Remove the packing, perform diagnostic nasal endoscopy, and cauterize the bleeding site in the emergency department.
D Admit overnight and remove the packing at the bedside in the morning.
E Perform CT of the sinuses with or without intravenous infusion.
Ref.: 2
Comments
Severe new-onset unilateral epistaxis in an adolescent boy should always raise suspicion for a juvenile nasal angiofibroma. This is a benign neoplasm arising around the region of the pterygopalatine fossa. It is almost exclusively found in adolescent boys. Treatment includes mainly surgery via either open or endoscopic approaches. Radiation therapy is used in only limited circumstances, especially since this is a benign lesion. The patient’s bleeding is currently controlled, and although his hemoglobin content is lowered, he is not showing any signs indicating a need for transfusion such as tachycardia or hypotension. The packing should remain in place until further diagnostic testing is performed given the suspicion for a possible neoplasm. In this case, CT of the sinuses with or without intravenous infusion is the next appropriate step given the suspicion for an underlying angiofibroma.
Epistaxis most commonly occurs from the Kiesselbach space along the anterior nasal septum. Bleeding from this site does not usually require more than simple pressure applied to the area or a small amount of anterior nasal packing. Cauterization can be done in the office setting under direct visualization if needed. Bleeding from the posterior nasal cavity typically arises from the sphenopalatine artery; it is less common but can be more severe. It may require control with posterior nasal packing, which can include a balloon device for tamponade. Any patient with such posterior packing in place should be monitored in the hospital because posterior packing has been shown to cause alterations in oxygen saturation. This is especially true in elderly patients and those with cardiopulmonary disease.
Answer
E
References
1 Lorenz RR, Netterville JL, Burkey BB. Head and neck. In Townsend CM, Beauchamp RD, Evers BM, et al, editors: Sabiston textbook of surgery: the biological basis of modern surgical practice, ed 18, Philadelphia: WB Saunders, 2008.
2 Cummings CW, Haughey BH, Thomas JR, et al. Cummings otolaryngology: head and neck surgery, ed 4. Philadelphia: CV Mosby; 2005.
3 Myers EN, Suen JY, Myers JN, et al. Cancer of the head and neck, ed 4. Philadelphia: WB Saunders; 2003.
4 McGuirt WF, McCabe BF. Significance of node biopsy before definitive treatment of cervical metastatic carcinoma. Laryngoscope. 1978;88:594-597.
5 Camp AA, Fundakowski C, Petruzzelli GJ, et al. Functional and oncologic results following transoral laser microsurgical excision of base of tongue carcinoma. Otolaryngol Head Neck Surg. 2009;141:66-69.
6 Steiner W, Ambrosch P, Hess CF, et al. Organ preservation by transoral laser microsurgery in piriform sinus carcinoma. Otolaryngol Head Neck Surg. 2001;124:58-67.
7 Al-Sarraf M, LeBlanc M, Giri PG, et al. Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal cancer: phase III randomized Intergroup Study 0099. J Clin Oncol. 1998;16:1310-1317.
8 The Department of Veterans Affairs Laryngeal Cancer Study Group. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. N Engl J Med. 1991;324:1685-1690.
9 Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003;349:2091-2098.
10 Bernier J, Domenge C, Ozsahin M, et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med. 2004;350:1945-1952.
11 Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med. 2004;350:1937-1944.
12 Bailey BJ, Johnson JT, Newlands SD. Head and neck surgery: otolaryngology, ed 4. Philadelphia: Lippincott Williams & Wilkins; 2006.
13 Patel RS, Clark JR, Gao K, et al. Effectiveness of selective neck dissection in the treatment of the clinically positive neck. Head Neck. 2008;30:1231-1236.
14 Mirski MA, Lele AV, Fitzsimmons L, et al. Diagnosis and treatment of vascular air embolism. Anesthesiology. 2007;106:164-177.