Matthew J. Graczyk, M.D., Anthony W. Kim, M.D.
1 A patient who has remained intubated endotracheally for a prolonged period (>4 weeks) is at risk for the development of tracheal injury. All of the following are true of postintubation tracheal injury except:
A Symptoms usually appear many months after extubation.
B Dyspnea on exertion is the primary symptom.
C It is often misdiagnosed as asthma or bronchitis
D Bronchoscopy is the best mode of evaluation.
E Treatment options include tracheal dilation, laser resection, internal stent placement, and staged reconstruction.
Ref.: 1, 2
Comments
Tracheal injury after endotracheal intubation can occur at the cuff level, as a result of stomal injury, or at the glottic and subglottic areas. It is typically caused by scarring at the site of compression of the tracheal mucosa by the balloon from the endotracheal tube. Symptoms usually appear within 1 to 6 weeks after intubation. Dyspnea on exertion is the primary symptom. The severity usually correlates with the degree of tracheal stenosis. Dilation, laser treatment, and stent placement are most often used as temporizing measures to allow inflammation or the patient’s overall condition to improve. Most functionally significant strictures are best treated by segmental resection and primary anastomosis.
Answer
A
2 Approximately 2 weeks after placement of a tracheostomy, copious bleeding from within and around the tracheostomy develops in a 65-year-old man. Which of the following choices is the best management for this problem?
A Removal of the tracheostomy tube at the bedside
B Replacement of the tracheostomy tube with an endotracheal tube
C Tracheal stent placement
D Resection of the innominate artery
E Arterial wall repair of the innominate artery
Ref.: 1, 2
Comments
A tracheoinnominate artery fistula is a rare, but often fatal complication of intubation or tracheostomy. It has a reported mortality rate of 86%. The most common cause is placement of the tracheostomy too low with subsequent erosion of the anterior tracheal wall into the innominate artery. Massive hemoptysis and episodic hemoptysis are the most common symptoms. Management includes hyperinflation of the tracheal tube cuff, finger compression of the innominate artery, and emergency return to the operating room for control of the airway and operative repair. Following orotracheal intubation, exposure is initially achieved via a collar incision at the stoma with extension into the midline for a sternotomy. The tracheal defect may be closed primarily and covered with soft tissue or be left open to heal by secondary intention if grossly infected. Repair of the innominate artery is associated with a high incidence of failure. Once the vascular defect is identified, the artery is divided proximal and distal to the defect and the divided edges are oversewn. The stumps are then buried under healthy tissue.
Answer
D
3 Hoarseness has developed in a 55-year-old woman following transhiatal esophagectomy. Which of the following is true about her complication?
A It is the result of injury to the superior laryngeal nerve.
B It is the result of injury to the recurrent laryngeal nerve.
C The nerve on the right side is more susceptible to injury.
D Seventy percent of bilateral nerve injuries are related to tracheal surgery.
E The most common mechanism of injury to the nerve is thermal from cautery burn.
Ref.: 1, 2
Comments
Vocal cord paralysis after thoracic surgery procedures has been reported to occur in 4% to 45% of patients. The nerve on the left side is more likely to be injured because of its course around the aortic arch. Seventy percent of bilateral injuries are associated with thyroid surgery. The most common mechanisms of injury to the recurrent laryngeal nerve are traction and division. Treatment is primarily surgical and includes injection, augmentation, and laryngeal framework surgery. Injury can result primarily in hoarseness, but it also can lead to incoordination of swallowing with a predisposition to aspiration.
Answer
B
4 A 53-year-old woman is evaluated for worsening stridor. She also complains of worsening dyspnea. Imaging studies demonstrate no lung pathology but are suggestive of an endotracheal lesion. Bronchoscopy confirms the presence of a primary tracheal tumor. Which of the following statements is true?
A It occurs more frequently in women.
B A tracheal tumor is best treated with radiation therapy to provide the optimal chance for long-term survival.
C The most commonly histology is adenoid cystic and squamous cell.
D It is usually found incidentally.
E Imaging studies allow adequate characterization of tracheal tumors.
Ref.: 1, 2
Comments
Primary tumors of the trachea are rare and account for less than 0.2% of all respiratory tract malignancies in the United States. A male-to-female ratio of 7 : 3 is reported. Patients typically have progressive respiratory symptoms, including cough and hemoptysis. Hoarseness and dysphagia are less common. Although endoscopic resection, radiotherapy, and tracheal resection are all available treatment modalities, surgical resection with airway reconstruction provides the best chance for long-term survival in appropriately select patients. Despite imaging studies visualizing these tumors, bronchoscopic evaluation is extremely important in planning resection.
Answer
C
5 All of the following are true of congenital malformations of the aortic arch system (also known as vascular rings) except:
A Children typically have noisy breathing and varying degrees of respiratory distress.
B Symptoms are usually caused by compression of the trachea or esophagus by the vascular abnormality.
C Symptomatic patients rarely require surgical repair.
D Late complications of unrepaired vascular rings include aortic dissection and aneurysm.
E Contrast-enhanced computed tomography (CT) is the best diagnostic modality.
Ref.: 1, 2
Comments
Congenital malformations of the aortic arch often cause symptomatic compression of the trachea and esophagus. Age at diagnosis and the severity of symptoms depend on the degree of compression. A newborn may exhibit dramatic airway compromise, whereas an adolescent may have subtle swallowing problems. The term dysphagia lusoria is used to describe the symptom occurring as a result of esophageal compression by an anomalous right subclavian artery arising from the thoracic aorta and passing behind the esophagus. Early surgical repair is recommended for symptomatic patients to avoid the complications of severe or recurrent respiratory infections, aortic dissection, and aneurysm formation. CT and magnetic resonance imaging are accurate imaging modalities, but they require sedation, which further jeopardizes the patient’s tenuous respiratory status.
Answer
C
6 A 75-year-old woman is found to have bilious output from her tracheostomy that is associated with subcutaneous air, as well as pneumomediastinum. What is true about her problem?
A Repair can be performed at anytime regardless of the need for ventilator dependence.
B Acquired causes are more common than congenital forms.
C It is best repaired by primary reapproximation of the esophagus and trachea.
D The acquired form is most commonly caused by postintubation injury from endotracheal tube cuff pressure.
E Muscle flap repair should be reserved for defects larger than 6 cm.
Ref.: 1, 2
Comments
A tracheoesophageal fistula (TEF) can occur in two forms: from congenital abnormalities or acquired. Congenital TEF is more common than the acquired forms. There are several different types of congenital TEF, with the most common type being esophageal atresia with a distal TEF. The associated fistula in this type is typically small and is found in the midline of the membranous portion of the trachea proximal to the carina. Acquired TEFs result from destruction of the posterior membranous portion of the trachea. They can be secondary to erosion by malignant tumor or, more commonly, endotracheal tube cuff injury. Repair of an acquired TEF is best performed by segmental tracheal resection, primary closure of the esophagus, and interposition of soft tissue between the trachea and esophagus. The best results are obtained if the patient can be weaned from the ventilator before surgical repair. Endoscopic stents may be used to palliate or treat complications associated with esophageal malignancies causing fistulas.
Answer
D
7 A 32-year-old woman complains of a chronic and recurrent pulmonary infection. Closer evaluation of the CT scan demonstrates an abnormal vessel at the level of the diaphragm that appears to be perfusing a portion of the left lung. Which of the following statements is false regarding her process?
A Intralobar sequestrations have their own pleural covering.
B There are two forms of pulmonary sequestrations: intralobar and extralobar.
C There is no communication between pulmonary sequestrations and the tracheobronchial tree.
D The blood supply to the pulmonary sequestration is from a systemic arterial source.
E Extralobar sequestration is frequently associated with congenital diaphragmatic hernias (CDHs).
Ref.: 1, 2
Comments
Pulmonary sequestration is a congenital abnormality of the lungs. Both intralobar and extralobar types have in common the absence of communication with the tracheobronchial tree, blood supply to the lesion from a systemic source, and venous drainage into either the pulmonary or systemic circulation. The arterial supply is usually derived from the descending thoracic aorta (intralobar) or the abdominal aorta (extralobar). The intercostal arteries are rarely the arterial source. Extralobar sequestration is marked by having its own pleural covering separate from the surrounding normal lung, whereas the intralobar type does not. These lesions are most often located in the lower lung fields. Patients often have recurrent infections in the lungs. Intralobar sequestrations constitute approximately 75% of all the sequestrations. Repeated pulmonary infections and hemoptysis are the most common symptoms. Extralobar sequestrations, in contrast to intralobar sequestrations, are associated with other congenital anomalies, particularly CDH.
Answer
A
8 Indications for an operation in patients with lung abscess include:
A Persistence of an abscess despite adequate therapy
B Empyema associated with a bronchopleural fistula (BPF)
C Inability to exclude a cavitating carcinoma
D Hemoptysis
E All of the above
Ref.: 1, 2
Comments
A lung abscess is a collection of pus contained in a cavity that is formed by the destruction of lung parenchyma. The bacteria responsible are numerous and include many gram positives, gram negatives, and anaerobes that cause pneumonia. The initial symptoms may include cough, fever, chills, fatigue, malaise, weight loss, pleuritic chest pain, dyspnea, and hemoptysis. Initial management consists of antibiotic therapy. Intervention for the aforementioned reasons is best achieved by percutaneous catheter drainage under CT or ultrasound guidance. Bedside tube thoracostomy is indicated for acutely ill patients with rupture of an abscess into the pleural space. Lung abscesses occur on the right side more than on the left side in most instances. Internal drainage with postural techniques and chest physiotherapy is usually sufficient for the management of this problem.
Answer
E
9 Regarding fungal infections of the lungs:
A Histoplasmosis is rarely found in an immunocompetent patient.
B No single staining technique demonstrates all the organisms.
C Coccidioidomycosis is endemic to the Mississippi River Valley.
D Blastomycosis is the most common cause of fibrosing mediastinitis.
E Untreated invasive Aspergillus infections gradually lead to the formation of an aspergilloma.
Ref.: 1, 2
Comments
Mycotic lung infection can be caused by many different organisms. The clinical manifestations vary widely from an asymptomatic patient with subclinical infection to an immunocompromised host with life-threatening opportunistic illness. The overall incidence of histoplasmin sensitivity (indicative of previous infection) in the United States is 20%. The incidence rises to 80% to 90% in the Midwest and Mississippi River Valley, where Histoplasma capsulatum is endemic. Fibrosing mediastinitis is a late complication of the mediastinal granuloma caused by histoplasmosis. Coccidioidomycosis is endemic to the southwestern region of the United States. Immunocompetent patients with no or minimal symptoms and histoplasmosis, coccidioidomycosis, or blastomycosis can be monitored safely without antifungal treatment unless progression of the disease occurs. No single stain demonstrates all of the fungal organisms, but the two best stains to visualize fungal organisms are periodic acid–Schiff and methenamine silver. Aspergillomas are caused by noninvasive Aspergillus infections. They are characterized by a mass of fungal mycelia, sulfur granules, inflammatory cells, mucus, and tissue debris within a preformed lung cavity.
Answer
B
10 A 45-year-old man is admitted to the intensive care unit with septic syndrome and diffuse pulmonary infiltrates. Broad-spectrum antibiotics are initiated after collecting endobronchial specimens for culture and sensitivity. One week later, the patient remains intubated, cultures are negative, but he continues to exhibit a septic picture with negative findings on CT except for diffuse lung infiltrates. Select the most correct statement regarding surgical lung biopsy:
A Is indicated for patients with functional impairment and unexplained lung pathology
B Requires sampling only grossly abnormal lung tissue
C Is indicated to confirm the diagnosis of bacterial pneumonia
D Has diagnostic accuracy similar to that of transbronchial lung biopsy
E Should be placed in formalin and sent to the pathology laboratory for routine processing
Ref.: 1, 2
Comments
Surgical lung biopsy is a helpful diagnostic modality in a patient with unexplained lung pathology. It may be performed to obtain a suspected diagnosis or to assist in excluding other diagnoses that can be made only by histologic evaluation. Lung biopsy should not be used when the clinical diagnosis can be made by less invasive means, such as in the case of bacterial pneumonia. Lung biopsy can be performed by video-assisted thoracoscopic surgery (VATS) or by open thoracotomy. Surgical biopsy has much greater diagnostic accuracy than transbronchial techniques do. Obtaining tissue samples from multiple lobes, even if not grossly abnormal, is critical during diagnostic evaluation for such conditions as idiopathic interstitial pneumonia. Lung specimens should be sent fresh and in a variety of fixatives to maximize the diagnostic yield.
Answer
A
11 A 48-year-old man has a very round 2.5-cm nodule in the lower lobe of his right lung. It has a heterogeneous appearance on CT consistent with some fat within the mass itself. There are no other abnormal findings on CT, and no metabolic activity is seen on positron emission tomography. A benign diagnosis is entertained, and therefore which of the following choices is most accurate about this general category of tumors?
A Are usually symptomatic
B May be diagnosed from the radiographic appearance
C Often double in size within a 2-year period
D Include the histologic subtype bronchoalveolar carcinoma
E Frequently progress to malignant tumors
Ref.: 1, 2
Comments
Benign lung tumors are usually asymptomatic and identified incidentally on imaging performed for other reasons. The radiographic appearance is unreliable in determining whether a lung nodule or mass is benign or malignant. Only specific patterns of calcification or the presence of fat density is considered to be an indicator of benign disease. Lung lesions are often monitored for changes in size over a specific interval to help determine benign versus malignant disease. A lesion that has not increased in size over a 2-year period is generally considered benign. An exception is bronchoalveolar carcinoma, which is a slow-growing malignant lesion with a characteristic ground glass opacity on CT. Malignant degeneration of a benign lung lesion is rare. Hamartomas are the most common benign lung lesions and account for more than 70% of all nonmalignant tumors. The majority of these lesions occur in the periphery.
Answer
B
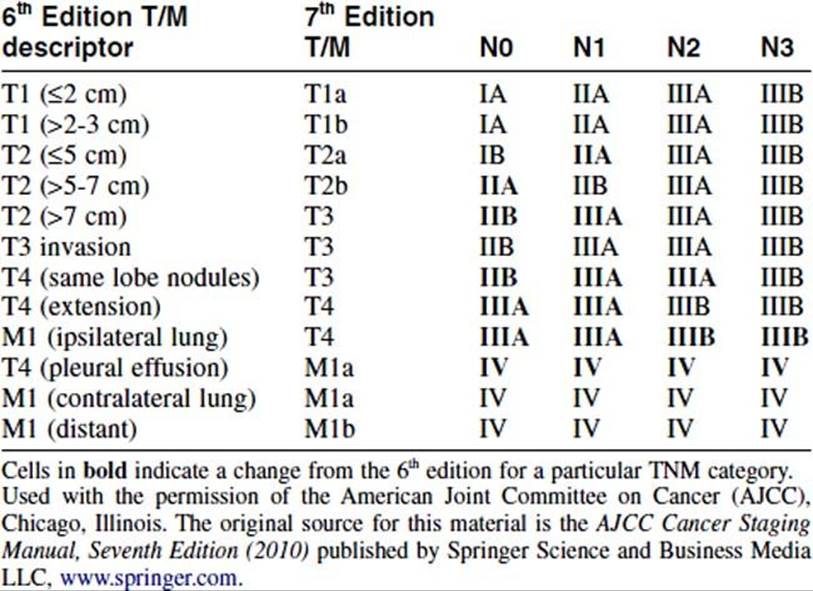
12 A 3-cm right upper lobe parenchymal mass and ipsilateral positive mediastinal lymph nodes (N2 disease) place a patient in which stage according to the new 7th edition of the American Joint Committee on Cancer (AJCC) staging system?
A IB
B IIA
C IIB
D IIIA
E IIIB
Ref.: 1-3
Comments
Staging of lung tumors is based on individual descriptors and their grouping. Stage IIIA disease in the new (seventh edition) staging system of the AJCC encompasses a range of disease from T1-3N2 to T4N0-1. Tables 29-1 and 29-2 delineate the individual T, N, and M descriptors and show the grouping of T, N, and M into their stages. The T designation typically refers to the status of the primary tumor in terms of size, location, visceral pleural involvement, and other factors. The N designation refers to the level of lymph node involvement. The M descriptor refers to the presence of metastasis.
TABLE 29-1 Definitions of TNM
|
Primary Tumor (T) |
|
|
TX |
Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but no visualized by imaging or bronchoscopy |
|
T0 |
No evidence of primary tumor |
|
Tis |
Carcinoma in situ |
|
T1 |
Tumor 3 cm or less in greatest dimension, surrounded by lung or visceral pleura, without bronchoscopic evidence of invasion more proximal than the lobar bronchus (i.e., not in the main bronchus)a |
|
T1a |
Tumor 2 cm or less in greatest dimension |
|
T1b |
Tumor more than 2 cm but 3 cm or less in greates dimension |
|
T2 |
Tumor more than 3 cm but 7 cm or less or tumor with any of the following features (T2 tumors with these features are classified T2a if 5 cm or less); Involves main bronchus, 2 cm or more distal to the carina; Invades visceral pleura (PL1 or PL2); Associated with atelectasis or obstructive pneumonitis that extends to the hilar region but does not involve the entire lung |
|
T2a |
Tumor more than 3 cm but 5 cm or less in greatest dimension |
|
T2b |
Tumor more than 5 cm but 7 cm or less in greatest dimension |
|
T3 |
Tumor more than 7 cm or one that directly invades any of the following: parietal pleural (PL3) chest wall (including superior sulcus tumors), diaphragm, phrenic nerve, mediastinal pleura, parietal pericardium; or tumor in the main bronchus (less than 2 cm distal to the carinaa but without involvement of the carina; or associated atelectasis or obstructive pneumonitis of the entire lung or separate tumor nodule(s) in the same lobe |
|
T4 |
Tumor of any size that invades any of the following: mediastinum, heart, great vessels, trachea, recurrent laryngeal nerve, esophagus, vertebral body, carina, separate tumor nodule(s) in a different ipsilateral lobe |
|
Regional Lymph Nodes (N) |
|
|
NX |
Regional lymph nodes cannot be assessed |
|
N0 |
No regional lymph node metastases |
|
N1 |
Metastasis in ipsilateral peribronchial and/or ipsilateral hilar lymph nodes and intrapulmonary nodes, including involvement by direct extension |
|
N2 |
Metastasis in ipsilateral mediastinal and/or subcarinal lymph node(s) |
|
N3 |
Metastasis in contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph node(s) |
|
Distant Metastasis (M) |
|
|
MX |
Distant metastasis cannot be assessed |
|
M0 |
No distant metastasis |
|
M1 |
Distant metastasis |
|
M1a |
Separate tumor nodule(s) in a contralateral lobe; tumor with pleural nodules or malignant pleural (or pericardial) effusionb |
|
M1b |
Distant metastasis (in extrathoracic organs) |
a The uncommon superficial spreading tumor of any size with its invasive component limited to the bronchial wall, which may extend proximally to the main bronchus, is also classified as T1.
b Most pleural (and pericardial) effusions with lung cancer are due to tumor. In a few patients, however, multiple cytopathologic examinations of pleural (pericardial) fluid are negative for tumor, and the fluid is nonbloody and is not an exudate. Where these elements and clinical judgment dictate that the effusion is not related to the tumor, the effusion should be excluded as a staging element and the patient should be classified as T1, T2, T3, or T4.
Used with the permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual, Seventh Edition (2010) published by Springer Science and Business Media LLC, www.springer.com.
TABLE 29-2 Stage Grouping Comparisons: 6th Edition vs. 7th Edition Descriptors, T and M Categories, and Stage Groupings
Answer
D
13 A 56-year-old man has what appears to be early-stage non–small cell lung cancer and therefore resection is planned. Which of the following statements is most accurate in the treatment of this patient’s problem?
A Cannot be performed with VATS
B Does not need to include mediastinal lymph node sampling or dissection
C Includes lobectomy and pneumonectomy only
D Should not be performed in conjunction with chemotherapy or radiation therapy given either preoperatively or postoperatively
E Is possible only in a minority of patients initially seen with lung cancer
Ref.: 1, 2
Comments
Although most patients in whom non–small cell lung cancer is diagnosed eventually die of their disease, surgical resection is the most effective means of controlling the primary tumor and provides the best chance for cure. Because patients are often initially seen with advanced disease, only 20% to 35% of patients with non–small cell lung cancer are candidates for surgery. Presuming that the appropriate stage is assigned, the majority of this group typically represents those with stages I and II disease. Resection can include the removal of an entire lung, a lobe, or a portion/segment of a lobe of the lung. Surgery can be performed by video-assisted thoracoscopic surgery or thoracotomy with good results. Sampling or removal of mediastinal lymph nodes (or both) is paramount for complete pathologic staging. Complete and accurate staging determines whether a patient may receive adjuvant therapy in addition to surgical resection, such as chemotherapy, radiation therapy, or both. These adjuncts can be given before or after surgical resection, depending on tumor stage.
Answer
E
14 Which of the following is not a criterion for resection of pulmonary metastases?
A The primary tumor is not controllable.
B More than one other extrapulmonary site of tumor exists.
C No better method or proven treatment is available.
D Complete resection of the metastatic focus is possible.
E Nonanatomic resection may be required.
Ref.: 1, 2
Comments
Many patients with lung metastases from sarcomas and germ cell tumors may be candidates for metastasectomy, but with most cancers of epithelial origin, only 1% to 2% of patients may be treated in this manner because these patients often have concurrent distant metastases in other organs. The general criteria for pulmonary metastasectomy are outlined in the answers. In general, patients being considered should satisfy all these criteria. In very general terms, the survival rate with complete metastasectomy is 36% at 5 years, 26% at 10 years, and 22% at 15 years. These figures can obviously vary depending on the site of origin. The median survival after lung resection for metastatic disease is 35 months. It is not uncommon for anatomic resections (segmentectomy, lobectomy, and pneumonectomy) to be performed in the appropriate circumstances.
Answer
B
15 A 20-year-old tall, thin man experiences spontaneous pneumothorax. On further questioning and examination, it is revealed that approximately 1 year earlier he was hospitalized and had a right chest tube placed for a similar problem. What is the optimal treatment option for this patient at this time?
A Observation and discharge
B Repeated tube thoracostomy maintained until resolution
C Needle aspiration and discharge
D Lobectomy and hospitalization
E Thoracoscopic resection
Ref.: 1, 2
Comments
Primary spontaneous pneumothorax occurs in young patients without significant lung disease, whereas secondary spontaneous pneumothorax occurs in patients with chronic obstructive pulmonary disease. The most common cause of primary spontaneous pneumothorax is rupture of small apical blebs. In the United States, tube thoracostomy with water seal drainage is the usual first-line treatment of a moderate to large pneumothorax in a patient with a first-time occurrence. Needle aspiration of air from the pleural space is more commonly done in Europe. Patients with small first-time pneumothoraces can be safely observed. Approximately 20% to 30% of patients will have a recurrence within 2 years of the first episode. After three or more episodes of spontaneous pneumothorax, the rate of recurrence rises to 50% to 70% within the following 2 years. It is for this reason that surgery is indicated if there is a recurrence. Operative intervention may be considered after a first episode of spontaneous pneumothorax in patients with previous pneumonectomy, a history of untreated bilateral pneumothorax, or an occupation that poses an elevated risk for the development of pneumothorax, such as an airline pilot or underwater diver.
Answer
E
16 The location of the thoracic duct at the level of the diaphragm is best described as:
A Extrapleural along the right anterior surface of the vertebral bodies, posterior to the esophagus, between the aorta and azygous vein
B Extrapleural along the left anterior surface of the vertebral bodies, posterior to the esophagus, between the aorta and azygous vein
C Intrapleural along the right anterior surface of the vertebral bodies, posterior to the esophagus, between the aorta and azygous vein
D Intrapleural along the left anterior surface of the vertebral bodies, posterior to the esophagus, between the aorta and azygous vein
E Extrapleural along the right anterior surface of the vertebral bodies, anterior to the esophagus, between the aorta and azygous vein
Ref.: 1, 2
Comments
See Question 17.
Answer
A
17 Management of chylothorax includes all of the following except:
A Drainage of the pleural space
B Fluid, electrolyte, and nutritional support
C External beam radiation therapy
D Surgical ligation of the thoracic duct
E Reduction of chyle production
Ref.: 1, 2
Comments
Chylothorax is the accumulation of excess lymphatic fluid in the pleural space. It is usually a result of injury to the thoracic duct or one of its major branches and occasionally results from obstruction of the duct. The thoracic duct at the level of the diaphragm runs extrapleurally along the left anterior surface of the vertebral bodies, posterior to the esophagus, between the aorta and azygous vein. A triglyceride level of 110 mg/dL has a 99% likelihood of being chylous versus 5% when the drainage is 50 mg/dL. The most common causes are trauma, neoplasms, tuberculosis, and venous thrombosis. Treatment options are divided into operative and nonoperative categories. Drainage of the pleural space is the basic treatment of any significant accumulation of fluid. Prevention of dehydration and malnutrition and correction of electrolyte imbalance are important for higher-output chyle leaks. The most effective means of reducing chyle production is limitation or elimination of oral intake and institution of total parenteral nutrition. Somatostatin, octreotide, etilefrine, mechanical ventilation with positive end-expiratory pressure, and embolization of the thoracic duct have been used with variable success. In general, 25% to 50% of chyle leaks will close spontaneously within 2 weeks of nonoperative treatment. Surgical treatment is recommended for persistent leaks and can be performed with a variety of described techniques. Successful operative management relies on anatomic understanding of the course of the thoracic duct. Prolonged drainage only results in dehydration, malnutrition, and immunologic compromise secondary to the loss of fluid, fats, proteins, and T lymphocytes.
Answer
C
18 A 60-year-old former smoker and plumber is being evaluated for progressive dyspnea and is found to have a large left-sided effusion. Work-up reveals that his effusion is secondary to a malignant pleural mesothelioma of sarcomatoid histology. Which of the following is true regarding his diagnosis?
A Only approximately 20% of malignant pleural mesotheliomas are not asbestos related.
B It is related to infection with Histoplasma.
C Its incidence is decreasing.
D Malignant pleural mesothelioma cannot be treated with surgery.
E It has a 5- to 10-year latency period after exposure to asbestos.
Ref.: 1, 2
Comments
Malignant mesothelioma is a rare tumor of the pleura. It is classified histologically into three subtypes: epithelioid, sarcomatoid, and mixed. The incidence is believed to be related to the industrial use of asbestos, particularly in occupations that expose individuals to the amphibole fibers of asbestos. Approximately 80% of malignant pleural mesotheliomas are secondary to asbestos exposure. Other factors that may contribute to the development of malignant pleural mesothelioma include radiation, non–asbestos-containing mineral fibers, organic chemicals, viruses, genetic predisposition, pleural scarring, and chronic inflammation. Despite governmental regulations on asbestos exposure in the second half of the 20th century, the incidence of malignant pleural mesothelioma has been rising in the United States since 1980. The latency period between exposure to asbestos and disease is 20 to 50 years. Twenty percent of cases are not related to asbestos exposure. Overall survival is grim. The best overall survival appears to be achieved with multimodality therapy consisting of combinations of surgery, chemotherapy, and radiation therapy. In appropriately selected patients, surgical treatment options include pleurectomy with decortication and extrapleural pneumonectomy. Controversy exists regarding which procedure is best.
Answer
A
19 A 64-year-old woman has recurrent malignant pleural effusion that is not responding to repeated thoracentesis. She underwent mastectomy for stage II carcinoma of the breast 10 years earlier. In managing this malignant pleural effusion, the most effective agent for chemical pleurodesis is which one of the following?
A Tetracycline
B Talc
C Bleomycin
D Doxycycline
E Erythromycin
Ref.: 1, 2
Comments
Malignant pleural effusion is a common clinical problem that can lead to significant morbidity and reduction in quality of life in patients with advanced cancer. Lung cancer and breast cancer are the most common underlying primary malignancies. Relief of shortness of breath and improvement in quality of life are the mainstays of treatment. The diagnosis is usually made by cytologic evaluation of pleural fluid obtained via thoracentesis or thoracoscopy. Treatment options include repeated thoracentesis, tube thoracostomy with bedside pleurodesis, and placement of an indwelling pleural catheter. The most effective agent for achieving pleurodesis is talc. Talc can be instilled via closed tube thoracostomy as a “slurry” in solution or as an aerosol “poudrage” delivered at the time of thoracoscopy. Talc has been shown to control malignant pleural effusions in more than 90% of patients, generally with a success rate of between 85% and 96%. Although other series have reported high success rates with other agents, on average, the success rates are not as consistent as with talc pleurodesis. The other sclerosing agents listed are associated with success rates of 50% to 75%. It is important to point out that pleurodesis can be achieved only if the lung is not trapped and can re-expand to allow apposition of the visceral and parietal pleural surfaces. For patients with trapped lung associated with a malignant pleural effusion, an indwelling pleural catheter is a good option for ongoing drainage of the pleural space and control of symptoms. Erythromycin has no current role in pleurodesis.
Answer
B
20 Two months following right-sided pneumonectomy, empyema develops in a 60-year-old man. Conservative measures followed by lesser invasive measures to address this problem are not successful. Therefore, the patient is scheduled for open drainage of his empyema. Which of the following is true?
A Is typically used in any patient able to tolerate general anesthesia
B Is best suited if the underlying lung will re-expand after drainage and is not well adherent to the surrounding chest wall
C Particularly useful if a BPF is present
D Cannot be used in the setting of a BPF
E Can be considered as an alternative first-line therapy in lieu of a chest tube
Ref.: 1, 2
Comments
Empyema is defined as a purulent pleural effusion. The most common source of infection is the lung, but bacteria may enter the pleural space through the chest wall, from below the diaphragm, or through the mediastinum. The mainstays of treatment are antibiotics and drainage of the pleural space. Diagnostic thoracentesis is often performed, but definitive pleural drainage must be undertaken to control the infection. This can be performed by closed tube thoracostomy, pigtail catheter, VATS, or open thoracotomy. Open drainage of an empyema is best suited for chronic empyema with fixed underlying lung parenchyma that will not reexpand. Open drainage is particularly useful if a bronchopleural fistula is present. The drainage technique of open-window thoracostomy is credited to Dr. Leo Eloesser. In 1935 he described an open thoracic window for tuberculous empyemas in which a U-shaped flap of skin and subcutaneous tissue was created and sewn to the most dependent portion of the empyema cavity after removing two to three underlying ribs and intercostal muscles. The Eloesser flap is performed with a thoracotomy incision over the empyema, rib resection, and marsupialization of the skin edges to the parietal pleura to prevent closure of the incision. The Clagett procedure can be used if a BPF is not present and consists of open pleural drainage, serial operative débridement, and eventual chest closure after filling the chest cavity with antibiotic solution. It is most often used for an infected pneumonectomy space.
Answer
C
21 A 14-year-old boy has an anterior chest wall deformity that includes a depression in the body of the sternum, as well as in the lower costal cartilage. Which of the following statements regarding his chest wall deformity is accurate?
A There is a 4 : 1 male-to-female preponderance.
B Occurrence on the left side is more common than on the right side.
C There is a high incidence of spontaneous resolution.
D There is an association with Marfan syndrome in more than 10% of patients.
E It is frequently associated with syndactyly.
Ref.: 1, 2
Comments
Pectus excavatum and carinatum are the most common chest wall deformities. Carinatum is anterior angulation of the sternum, whereas excavatum is posterior angulation. Asymmetry of the depression can occur, such as the right side being more involved than the left side. It is usually present at birth but may worsen significantly during adolescence because of rapid growth of the individual. Pectus excavatum occurs four times more commonly in males than in females and is rarely seen in the African-American or Hispanic population. Although rare cases of spontaneous resolution occur, the majority of children have deformities that persist or worsen with time, especially during rapid growth periods. Approximately 65% of patients with Marfan syndrome have chest wall deformities, with pectus excavatum being the most common. However, only 2% of all patients with pectus excavatum have Marfan syndrome. Poland syndrome is a congenital anomaly characterized by absence of the sternal head of the pectoralis major and minor muscles. It is associated with anomalies, including hypoplasia of the breast/nipple complex, rib aplasia, lung hernia, small and elevated scapula (Sprengel deformity), cervical vertebral fusion (Klippel-Feil syndrome), syndactyly, and renal anomalies. Malignancies such as leukemia, lymphoma, cervical cancer, and lung cancer have also been associated.
Answer
A
22 A 45-year-old man is being evaluated for a painful right chest wall mass emanating from the ribs. Work-up suggests that this is a primary lesion of the chest wall. What is the most common primary malignant chest wall neoplasm in an adult?
A Osteosarcoma
B Soft tissue sarcoma
C Ewing sarcoma
D Chondrosarcoma
E Plasmacytoma
Ref.: 1, 2
Comments
Most primary chest wall tumors are benign, whereas most malignant chest wall neoplasms are metastatic. The most common primary malignant chest wall mass in adults is chondrosarcoma. It accounts for 50% of malignant chest wall tumors and 25% of all primary chest wall masses. Eighty percent of chondrosarcomas occur in the ribs and 20% in the sternum. Surgical resection is the best treatment of chondrosarcoma because these tumors are extremely resistant to radiation therapy and chemotherapy. Wide resection is typically curative. If left untreated, metastases typically occur late. Ewing sarcoma and primitive neuroectodermal tumors are the most common primary chest mall malignancies in children. These tumors are best treated by resection and radiation therapy. Chemotherapy can be used to control distant disease. Plasmacytoma is a local manifestation of multiple myeloma that is often manifested as a rib lesion in older men. Osteosarcomas have a bimodal distribution; they occur between the ages of 10 and 25 then again after the age of 40, often in association with many other diseases. Primary soft tissue sarcomas of the chest wall are uncommon.
Answer
D
23 A 49-year-old woman after bilateral mastectomies for advanced cancer of the breast has a soft tissue skin metastasis in the midsternal region. After radiation therapy, a 5-cm, indolent, extremely painful necrotic ulcer develops. Following appropriate work-up, the patient is offered full-thickness resection of the chest wall. Which of the following is the most common soft tissue pedicled flap used for chest wall reconstruction?
A Transverse rectus abdominis muscle (TRAM)
B Serratus anterior
C Omentum
D Latissimus dorsi
E Trapezius
Ref.: 1, 2
Comments
Chest wall reconstruction is often necessary after chest wall resection. Soft tissue reconstruction of the chest wall can be done with any of the flaps listed. They can be used either as free tissue flaps with microvascular anastomoses or, more commonly, as pedicled flaps using the native blood supply. The choice of flap is dictated by the location and size of the defect to be covered. The latissimus dorsi muscle is the most versatile and most common choice for chest wall reconstruction. However, the thoracodorsal vessels may have been compromised by the previous therapy, in which case a transverse rectus abdominis muscle flap can be used. It may be used as an isolated muscular flap or taken with the overlying paddle of skin and used as a myocutaneous flap. It the most commonly used flap because it has an extensive arc of rotation when the pedicle is based on the thoracodorsal neurovascular bundle. When used in such a manner, the latissimus dorsi flap can cover defects on the anterior, posterior, and lateral chest wall.
Answer
D
24 Regarding the diagnosis and management of thoracic outlet syndrome:
A An operation is the primary treatment.
B It is recognized in approximately 2% of the population.
C Neurogenic symptoms primarily result from compression of the phrenic nerve between the anterior and middle scalene muscles.
D Patients may have primarily neurogenic symptoms, vascular symptoms, or a combination of both.
E Decreased nerve conduction velocity of the median nerve at the elbow is strongly suggestive.
Ref.: 1, 2
Comments
Thoracic outlet syndrome is compression of the subclavian vessels or the brachial plexus (or both) as these structures exit the chest at the junction of the scalene muscles and the bony thorax. Most of the compression occurs at the first rib. It is present in approximately 8% of the population. Patients may have neurologic symptoms, signs of vascular compression, or a combination of both. Although the phrenic nerve lies on the anterior scalene muscle, neurogenic symptoms occur from compression of the brachial plexus between the scalene triangle and the bony thorax. Pain and paresthesia symptoms predominate, particularly in the ulnar nerve distribution. The initial treatment of most patients with thoracic outlet syndrome is nonoperative and consists of patient education on positioning, behavior modification, and physical therapy. Surgery is usually reserved for the 5% of patients with persistent symptoms despite nonoperative treatment. Delayed nerve conduction velocity across the thoracic outlet is consistent with thoracic outlet syndrome, and decreased velocity around the elbow is indicative of ulnar nerve entrapment or neuropathy.
Answer
D
25 A minor league pitcher arrives at the hospital with complaints of edema, discoloration, and distention of the superficial veins in his throwing arm the day after he pitched for an extended period. What is true about his current condition?
A Is the result of a hypercoagulable state
B Is best treated with catheter-directed thrombolytic agents followed by surgical decompression of the thoracic outlet
C Is best treated with rest, elevation, and long-term warfarin therapy
D Is best treated with balloon angioplasty and intravascular stent placement
E Is not associated with occupational risk factors
Ref.: 1, 2
Comments
Effort thrombosis of the axillary subclavian vein is known as Paget-Schroetter syndrome. It is usually caused by unusual or excessive use of the arm in association with some element of anatomic compression as described in thoracic outlet syndrome. Repetitive muscular activity such as that observed in professional athletes, painters, and beauticians can predispose the individual to this condition. It is not a direct result of a hypercoagulable state, although increased thrombogenicity can increase the incidence and exacerbate the symptoms. Treatment consisting of rest, elevation, and anticoagulation therapy was once the mainstay of management but has been shown to be associated with significant morbidity, including deep venous thrombosis, pulmonary embolism, and subsequent need for thrombectomy. The best treatment is catheter-directed lytic therapy combined with prompt surgical decompression of the thoracic outlet.
Answer
B
26 Risk factors for poststernotomy mediastinitis include all of the following except:
A Male gender
B Advanced age (>75)
C Obesity (body mass index >30 kg/m2)
D Diabetes with glucose levels higher than 200 mg/dL
E Smoking
Ref.: 1, 2, 4
Comments
The incidence of post-sternotomy mediastinitis is reported be between 0.7% and 1.5%. The mortality rate can be significant but averages between 4% and 10%. A number of risk factors are associated with this problem and are classified as modifiable versus unmodifiable or as preexisting, intraoperative, and postoperative. All of the risk factors listed are associated with an increased incidence of post-sternotomy mediastinitis except male gender. Female gender is an associated risk factor. The duration of cardiopulmonary bypass has also been shown to be a strong predictor of post-sternotomy mediastinitis. The principles of management for sternal wound infections are to (1) gain control the infectious process in the shortest amount of time and (2) ensure sternal stability.
Answer
A
27 During the performance of trisegmentectomy in a patient with colorectal metastasis to the right lobe of the liver, a brisk venous-like type of bleeding arises posterior to the liver. The surgeon decides to extend the incision through a median sternotomy. The best location to take down and repair the diaphragm so that the phrenic nerve is not injured is:
A Centrally along the middle of the diaphragm, beginning medially at the central tendon and moving laterally toward the chest wall
B Along the posterior third between the aorta and esophagus
C Circumferentially at the periphery of the diaphragm
D Centrally along the middle of the diaphragm in a vertical line from anterior to posterior
E Medially in linear fashion at the junction of the diaphragm and mediastinal pleura
Ref.: 1, 2
Comments
The diaphragm is innervated by the phrenic nerves. Arising from cervical roots C3, C4, and C5, the nerves originate at the superior border of the thyroid cartilage, pass along the anterior scalene muscles bilaterally, and descend through the mediastinum along the middle of the pericardium anterior to the hilum of the lungs. The right phrenic nerve reaches the diaphragm just lateral to the inferior vena cava. The left phrenic nerve enters the diaphragm lateral to the left border of the heart. Both nerves divide at the level of the diaphragm or just above it into several branches. There are three main muscular branches on the surface of the diaphragm. One is directed anteromedially toward the sternum, another is directed anterolaterally toward the central tendon, and the third is directed posteriorly. When taking down the diaphragm for surgical exposure it is of paramount importance to avoid injury to these branches. The best approach to divide the diaphragm is along the peripheral circumference with just enough muscle left on the chest wall for sturdy reapproximation. Generally, it is advised that one stay at least 5 cm lateral to the edge of the central tendon to avoid the posterolateral and anterolateral branches of the phrenic nerve.
Answer
C
28 Bochdalek CDH:
A Is right sided 90% of the time
B Is located anterior at the sternocostal junction
C Usually has a hernia sac with associated abdominal contents
D Is related to failure of development or fusion of the pleuroperitoneal membranes
E Is associated with other congenital anomalies in less than 10% of patients
Ref.: 1, 2
Comments
Congenital diaphragmatic hernias are divided into two subtypes, Bochdalek and Morgagni. Both types occur as a result of abnormalities during embryogenesis, specifically failure of development or fusion of the pleuroperitoneal membranes that usually make up the diaphragm between the fourth and eighth weeks of gestation. In Morgagni hernias, the defect occurs at the sternocostal hiatus through which the superior epigastric vessels pass from the abdomen to the retrosternal area. Bochdalek hernias occur in the posterolateral portion of the diaphragm and are left sided in 90% of cases. Most are found incidentally or are recognized after organ incarceration or volvulus. All Morgagni hernias have a sac that usually contains omentum and may also contain stomach, small bowel, or colon. Most (90%) Bochdalek hernias do not have a sac. CDH is associated with other congenital abnormalities in 45% to 50% of live births.
Answer
D
29 A newborn infant begins to experience respiratory distress approximately 4 hours after delivery. On examination, the newborn is tachypneic, with sternal, subcostal, and supraclavicular retractions. Decreased breath sounds are noted, and bowel sounds are present in the left side of the chest. The abdomen is scaphoid. Which of the following is not part of the management of this newborn?
A Immediate operative repair
B Extracorporeal membrane oxygenation (ECMO)
C High-frequency oscillatory ventilation
D Inhaled nitric oxide
E Inotropic and vasopressor support
Ref.: 1, 2
Comments
Treatment of congenital diaphragm hernias often begins with a prenatal diagnosis via ultrasound. If a prenatal diagnosis is made, delivery should take place in a center capable of delivering advanced neonatal and pediatric surgical care with reasonable experience in dealing with CDH. Stabilization of the patient and delayed surgical repair are the standard of care for newborns with CDH. Stabilization begins with respiratory support, including immediate intubation. Additional measures of support, including ECMO, oscillatory ventilation, inhaled nitric oxide, and hemodynamic support, can be used as the clinical condition warrants. Immediate surgical repair before stabilization and support is associated with significant morbidity and mortality. Tube thoracostomy is not routinely described as an adjunct in the preoperative care of patients with CDH, presumably because of the presence of herniated abdominal contents in the ipsilateral side of the chest and the absence of a true pneumothorax. The respiratory distress and hypoxia that are present are usually secondary to pulmonary hypoplasia. Finally, a tube thoracostomy is not typically used after repair because of concern for negative intrapleural pressure causing barotrauma and alveolocapillary membrane damage.
Answer
A
30 A 40-year-old man is evaluated for unremitting fevers and chills following a recent history of having a dental abscess. He neck is tender, and flexion and extension of the neck result in pain. What best characterizes this process?
A Arises commonly from a postoperative surgical site infection
B Is best treated by percutaneous drainage
C Can usually be treated in a single-stage operation
D Is a chronic, indolent disease process
E Is best diagnosed by CT of the neck and chest
Ref.: 1, 2
Comments
Acute descending necrotizing mediastinitis is a destructive, life-threatening condition similar to necrotizing fasciitis and acute necrotizing pancreatitis. Infection usually stems from an oropharyngeal source, with cultures yielding a polymicrobial mix of aerobic and anaerobic bacteria. The bacteria progress to the mediastinum via the pretracheal and retrovisceral spaces or along the carotid sheath. Although the diagnosis is often delayed, it is best made by early contrast-enhanced CT of the neck and chest. The principles of treatment are immediate parenteral broad-spectrum antibiotics and aggressive surgical treatment of both the neck and mediastinum. In most cases a cervical approach is sufficient, but a thoracic approach may need to be performed on occasion. Serial operations are often required. The best results are achieved with a multidisciplinary approach that includes thoracic surgeons, otolaryngologists, and oral maxillofacial surgeons when appropriate.
Answer
E
31 A stage I thymoma has been diagnosed in a 41-year-old woman. Through which of the following surgical approaches should a thymectomy not be performed?
A Transcervical collar incision
B Median sternotomy
C Partial sternal split
D VATS
E Posterolateral thoracotomy through the sixth intercostal space
Ref.: 1, 2
Comments
Thymectomy is performed most commonly for patients with myasthenia gravis. Indications for thymectomy include the presence of thymoma and a diagnosis of myasthenia without thymoma in patients whose disease is refractory to medical therapy or who cannot tolerate or are noncompliant with medical treatment. Thymectomy is also indicated for patients with other less common thymic neoplasms such as thymic carcinoma and thymic carcinoid tumors. Various surgical techniques for thymectomy have been advocated and include all of the approaches listed. The debate regarding which technique has the best results has not been resolved. A posterolateral thoracotomy through the sixth intercostal space would be too low and provide suboptimal exposure.
Answer
E
32 All of the following mediastinal tumors are found in the anterior mediastinum except:
A Thymoma
B Thyroid mass
C Lymphoma
D Teratoma
E Ganglioneuroma
Ref.: 1, 2
Comments
Mediastinal masses are characterized by their location in the three compartments of the mediastinum: anterior, middle, and posterior. The anterior mediastinum extends vertically from the thoracic inlet to the diaphragm and is bounded anteriorly by the sternum and posteriorly by the brachiocephalic vessels, aorta, and pericardium. The middle mediastinum is defined as the space that contains the heart and pericardium. The posterior mediastinal compartment is defined anteriorly by the heart and trachea, laterally by the mediastinal pleura, and posteriorly by the vertebrae. The differential diagnosis of an anterior mediastinal mass includes thymoma, thyroid, lymphoma, and teratoma as the most common tumors. Neurogenic tumors, of which ganglioneuromas are one, are most often located in the posterior mediastinum.
Answer
E
33 A 58-year-old former heavily smoking man with a history of ethanol abuse recently ceased drinking and experienced a severe episode of ethanol withdrawal while hospitalized. Shortly after this episode he was noted to have pneumomediastinum on a chest radiograph. Which of the following is most likely the result of pneumomediastinum in the patient presented?
A Esophageal perforation
B Tracheobronchial injury
C Rupture of terminal alveoli from pressure generated by coughing or straining against a closed glottis
D Extension of a pneumothorax
E Penetrating trauma
Ref.: 1, 2
Comments
Pneumomediastinum refers to the presence of air in the mediastinal space. The most common source is rupture of terminal alveoli generated by coughing or straining against a closed glottis. The air escapes the distal lung tissue, but the visceral pleura remains intact. The air then courses along the perivascular or peribronchial space into the mediastinum. This process is rarely clinically significant and almost always requires no intervention except reassurance and a brief period of observation. Pneumomediastinum may also arise from more significant injury to the tracheobronchial tree or from esophageal perforation. Tracheobronchial injuries should be evaluated with bronchoscopy. An esophagogram with or without esophagoscopy can be performed to evaluate for esophageal injury. Rarely, gas extension from the neck, usually secondary to trauma or surgical procedures, or from the abdominal cavity, usually after perforation of retroperitoneal hollow viscera, may result in pneumomediastinum.
Answer
A
34 A 23-year-old man is taken to the trauma department following a snowmobile accident in which his neck was injured in a “clothesline” fashion. In the field, he exhibited respiratory distress and was intubated. What is true about the laryngeal trauma that this patient experienced?
A It is graded on a four-point descriptive scale according to the severity of injury.
B Management begins with stabilizing the neck because of associated injuries.
C Minor injuries can be evaluated with endoscopy and managed nonoperatively.
D Early-stage blunt trauma classically causes symptoms.
E CT is not a sensitive diagnostic test for identifying traumatic laryngeal injury.
Ref.: 1, 2
Comments
Because of the protected position of the larynx in the neck, external laryngeal trauma is rare. However, the mortality rates associated with these injuries can as high as 40% from blunt injury and 20% from penetrating injury. Death most often results from asphyxia secondary to laryngospasm, hemorrhage from an associated vascular injury, or laryngeal concussion. The signs and symptoms may be overt, with findings of subcutaneous emphysema, an expanding neck hematoma, hemoptysis, hematemesis, or a neurologic deficit. Alternatively, the clinical findings may be more subtle and consist of changes in voice, dyspnea, neck pain, dysphagia, coughing, or aspiration suggesting possible injury. CT is a sensitive diagnostic test for traumatic laryngeal injury and may be indicated despite normal findings on flexible laryngoscopy or bronchoscopy. Laryngeal injuries are graded on a five-point descriptive scale according to the severity of injury. Management, as with all trauma victims, begins with obtaining a stable airway. Minor injuries may be managed nonoperatively after careful and thorough endoscopic evaluation. Major injuries to the larynx require surgical exploration, with repair and reconstruction dictated by the extent of the injury.
Answer
C
35 A 24-year-old woman is a passenger in motor vehicle collision. On arrival to the trauma bay, a chest radiograph is suggestive of a left hemothorax. A tube thoracostomy is performed and a copious amount of bloody effusion is evacuated. Blood continues to be drained from her chest. In blunt chest trauma with hemothorax, what is an indication for surgical exploration that is listed among the following choices?
A Initial chest tube output exceeding 1500 mL
B Hourly chest tube output of up to 100 mL for 3 consecutive hours
C Declining hemoglobin or hematocrit
D Increasing opacities on chest radiography
E Presence of pneumothorax
Ref.: 1, 2
Comments
Blunt injury to the thorax often results in varying degrees of hemothorax, pneumothorax, or both. Tube thoracostomy is the initial management of all injuries, both blunt and penetrating, to the thoracic cavity that result in hemothorax or pneumothorax. Many such injuries can be managed with tube thoracostomy alone. With regard to hemothorax, two metrics are generally accepted as indications for thoracotomy: (1) volume of initial drainage after tube thoracostomy of 1500 mL or more or (2) ongoing bloody chest tube output of greater than 200 mL/h. A drop in hemoglobin or hematocrit is often associated with a multiply injured trauma victim and is not by itself an indication for thoracotomy. Opacities on a chest radiograph in trauma patients are relatively nonspecific and may represent lung contusion, atelectasis, pneumonia, pleural effusion, or retained hemothorax. Their presence, although important to ongoing care of the patient, is not an indication for surgical exploration. Most pneumothoraces from trauma will resolve with tube thoracostomy.
Answer
A
36 A 26-year-old man was the driver in a high-speed motor vehicle collision in which the side of his car was hit in a lateral fashion (“T-boned”), and he sustained left-sided blunt chest wall injury. On evaluation, his primary survey is intact. He does have some left lateral rib fractures on the lower aspect of the left side of his chest. His chest radiograph shows an elevation in the costophrenic angle with air-fluid levels in the chest. Before undergoing chest CT, a nasogastric tube is placed, and during confirmatory radiographs, diagnosis of the injury is made. Which of the following is true regarding this patient’s injury?
A Must be repaired with a patch
B Can be readily identified on radiographs or CT
C Heals spontaneously
D Is best identified and repaired via laparotomy
E Requires full excision of the diaphragm with prosthetic repair
Ref.: 1, 2
Comments
Injury to the diaphragm accounts for only 3% of all trauma-related injuries, with the majority occurring on the left side rather than the right side. Blunt injuries usually occur secondary to high-speed motor vehicle crashes. A lateral impact is more likely to cause the injury than a frontal impact. Initial chest radiographic findings are normal in 50% of patients, and pneumothorax or hemothorax is seen in the remaining 50% of patients with diaphragmatic injury. CT, though helpful in the evaluation for other injuries to the thorax and abdomen, will aid in the diagnosis of a diaphragm injury only if abdominal viscera herniate into the pleural space. This is less common in the acute setting. The diagnosis of a diaphragm injury is best made with a high index of clinical suspicion based on the mechanism of injury and an injury pattern that is confirmed by thorough exploration via laparotomy. Recently, laparoscopic exploration of the abdomen has been used in the diagnosis of diaphragmatic injuries. Almost all trauma-related diaphragm injuries in the acute setting can be repaired primarily with a continuous monofilament suture 1-0 or larger in size. In general, in the acute setting a transabdominal approach is preferred, although some have advocated a right thoracic approach for right-sided injuries regardless of the time from injury. Classically, a thoracic approach is reserved for injuries seen in delayed fashion.
Answer
D
37 A 29-year-old man sustains a stab wound to the right side of his chest in approximately the sixth intercostal space in the anterior axillary line. He is found to have hemopneumothorax. In the management of penetrating injury to the lung, all of the following are appropriate except:
A Tube thoracostomy
B Oversewing of small lung lacerations
C Wedge resection
D Anatomic lung resection
E Placement on continuous ECMO within hours of evaluation
Ref.: 1, 2
Comments
Penetrating injury to the lungs results in varying degrees of hemothorax, pneumothorax, or both. Tube thoracostomy is the initial management of all injuries, both blunt and penetrating, to the thoracic cavity that result in hemothorax or pneumothorax. Most injuries can be managed by tube thoracostomy alone. Drainage of the pleural space with reestablishment of pleural apposition is usually sufficient to tapenade the low-pressure venous bleeding and serves to seal the air leak. Indications for early thoracotomy are massive hemothorax and massive air leak (only after the level of tracheobronchial injury, if present, has been identified by bronchoscopy). With regard to hemothorax, two metrics are generally accepted as indications for thoracotomy: (1) volume of initial drainage after tube thoracostomy of 1500 mL or greater or (2) ongoing bloody chest tube output greater than 200 to 250 mL/h for 3 to 4 consecutive hours after tube thoracostomy. All of the methods listed can be used to definitively control injury, depending on the extent of involved lung and associated blood vessels. Surgical exploration in a trauma patient should be expeditious and focused. Because anatomic lung resection may be time-consuming, other measures of controlling injury to the lung should be well known to the surgeon exploring the thorax in the setting of trauma. If surgical exploration is performed, some bronchial stump coverage is important because of contamination of the pleural space. Lung injury alone is not an indication for ECMO.
Answer
E
38 A 31-year-old man is brought to the trauma department 10 minutes after a gunshot wound to the left side of his chest. On arrival, he loses his vitals signs. He is already intubated with endotracheal tube placement confirmed, and an ongoing resuscitation effort is maintained. In preparing for emergency thoracotomy, which of the following best characterizes the necessary incision and position of the patient?
A Posterolateral incision through the fourth intercostal space and the patient in the lateral decubitus position
B Anterior incision through the second intercostal space and the patient supine
C Anterolateral incision through the fourth or fifth intercostal space and the patient supine
D Vertical incision along the anterior axillary line through the sixth intercostal space and the patient supine
E Anterolateral incision through the sixth intercostal space and patient in the lateral decubitus position
Ref.: 1, 2
Comments
The most common emergency thoracotomy incision is an anterolateral incision. It allows quick access to the thoracic cavity for control of life-threatening hemorrhage. This is performed with the patient supine and begins along the inframammary fold. The incision is turned superiorly along the medial aspect after crossing the midclavicular line so that if extension across the sternum is required, the incision will not be too low. The pericardium, lungs, pulmonary hilum, and descending thoracic aorta from the left side are readily accessible through this incision. If on entering the chest, high apical bleeding is encountered consistent with injury to a great vessel, the apex of the chest should be packed and the appropriate counterincision made. All of the other incisions listed are used in thoracic surgery for various exposures but are not generally indicated for trauma.
Answer
C
References
1 Patterson GA, Cooper JD, Deslauriers J, et al, editors. Pearson’s thoracic and esophageal surgery, ed 3, Philadelphia: Churchill Livingstone, 2008.
2 Sellke FW, del Nido PJ, Swanson SJ, editors. Sabiston and Spencer surgery of the chest, ed 7, Philadelphia: WB Saunders, 2005.
3 Detterbeck FC, Boffa DJ, Tanoue LT. The new lung cancer staging system. Chest. 2009;136:260-271.
4 Shields TW, Locicero J, Reed CE, et al, editors. General thoracic surgery, ed 7, Philadelphia: Lippincott Williams & Wilkins, 2009.