Marc García-Elías and Angel Ferreres
DEFINITION
![]() Scapholunate dissociation (SLD) is a symptomatic wrist dysfunction that results from partial or total rupture of the scapholunate ligamentous complex, with or without carpal malalignment.
Scapholunate dissociation (SLD) is a symptomatic wrist dysfunction that results from partial or total rupture of the scapholunate ligamentous complex, with or without carpal malalignment.
![]() It may appear either as an isolated injury, or associated with distal radius fractures or displaced scaphoid fractures. Usually the result of trauma (hyperextension and ulnar deviation injury to the wrist), SLD may also result from a chronic inflammatory arthropathy (rheumatoid arthritis, chondrocalcinosis).
It may appear either as an isolated injury, or associated with distal radius fractures or displaced scaphoid fractures. Usually the result of trauma (hyperextension and ulnar deviation injury to the wrist), SLD may also result from a chronic inflammatory arthropathy (rheumatoid arthritis, chondrocalcinosis).
ANATOMY
![]() Under load the scaphoid is inherently unstable owing to its oblique alignment relative to the direction of axial forces being transmitted across the wrist.6 The amount of instability depends on the following factors:
Under load the scaphoid is inherently unstable owing to its oblique alignment relative to the direction of axial forces being transmitted across the wrist.6 The amount of instability depends on the following factors:
![]() The geometry of the radioscaphoid joint (the deeper the scaphoid fossa, the less unstable)
The geometry of the radioscaphoid joint (the deeper the scaphoid fossa, the less unstable)
![]() The stabilizing efficacy of the periscaphoid ligaments (proximal scapholunate interosseous ligament complex, dorsal scaphotriquetral [STq], palmar scaphocapitate [SC] and lateral scapho-trapezial-trapezoidal [STT] ligaments)7
The stabilizing efficacy of the periscaphoid ligaments (proximal scapholunate interosseous ligament complex, dorsal scaphotriquetral [STq], palmar scaphocapitate [SC] and lateral scapho-trapezial-trapezoidal [STT] ligaments)7
![]() The indirect action of the flexor carpi radialis (FCR) muscle
The indirect action of the flexor carpi radialis (FCR) muscle
![]() The scapholunate interosseous ligament complex consists of three structures: the two scapholunate ligaments (palmar and dorsal) and the proximal fibrocartilaginous membrane.
The scapholunate interosseous ligament complex consists of three structures: the two scapholunate ligaments (palmar and dorsal) and the proximal fibrocartilaginous membrane.
![]() The proximal membrane connects the two adjacent convex borders of the two bones from dorsal to palmar, separating the radiocarpal and midcarpal joint spaces (FIG 1).
The proximal membrane connects the two adjacent convex borders of the two bones from dorsal to palmar, separating the radiocarpal and midcarpal joint spaces (FIG 1).
![]() The dorsal scapholunate ligament is formed by dense, slightly oblique connective fibers that link the dorsal aspects of the scaphoid and lunate bones.
The dorsal scapholunate ligament is formed by dense, slightly oblique connective fibers that link the dorsal aspects of the scaphoid and lunate bones.
![]() The palmar scapholunate ligament has longer, more obliquely oriented fibers, allowing substantial rotation of the scaphoid relative to the lunate.
The palmar scapholunate ligament has longer, more obliquely oriented fibers, allowing substantial rotation of the scaphoid relative to the lunate.
![]() The dorsal scapholunate ligament has the greatest yield strength (260 Newtons [N] on average), followed by the palmar scapholunate ligament (118 N) and the proximal membrane (63 N).2
The dorsal scapholunate ligament has the greatest yield strength (260 Newtons [N] on average), followed by the palmar scapholunate ligament (118 N) and the proximal membrane (63 N).2
![]() The proximal portion of the membrane often appears perforated in middle-aged and older individuals, which does not cause instability.
The proximal portion of the membrane often appears perforated in middle-aged and older individuals, which does not cause instability.
PATHOGENESIS
![]() When axially loaded, the three proximal bones do not react equally in terms of direction of rotation. The scaphoid tends to rotate into flexion and pronation while the triquetrum is pulled into extension by the dorsally subluxing hamate bone (FIG 2A).
When axially loaded, the three proximal bones do not react equally in terms of direction of rotation. The scaphoid tends to rotate into flexion and pronation while the triquetrum is pulled into extension by the dorsally subluxing hamate bone (FIG 2A).
![]() If both the palmar and dorsal scapholunate and lunotriquetral (LTq) ligaments are intact, such differences in reactive motion generate increasing torques at both scapholunate and LTq levels, resulting in an increasing coaptation of these joints. Such an increased coaptation further contributes to the proximal carpal row stability (FIG 2B).
If both the palmar and dorsal scapholunate and lunotriquetral (LTq) ligaments are intact, such differences in reactive motion generate increasing torques at both scapholunate and LTq levels, resulting in an increasing coaptation of these joints. Such an increased coaptation further contributes to the proximal carpal row stability (FIG 2B).
![]() If the scapholunate ligaments are completely torn, the scaphoid no longer appears constrained by the rest of the proximal row, and tends to collapse into an abnormally flexed and pronated posture (“rotatory subluxation of the scaphoid”).
If the scapholunate ligaments are completely torn, the scaphoid no longer appears constrained by the rest of the proximal row, and tends to collapse into an abnormally flexed and pronated posture (“rotatory subluxation of the scaphoid”).
![]() By contrast, the lunate and triquetrum translate ulnarly while rotating abnormally into extension, a pattern of carpal malalignment known as a dorsal intercalated segment instability (DISI) (FIG 2C).
By contrast, the lunate and triquetrum translate ulnarly while rotating abnormally into extension, a pattern of carpal malalignment known as a dorsal intercalated segment instability (DISI) (FIG 2C).
NATURAL HISTORY
![]() Partial scapholunate ligament injury may not be radiologically demonstrable and may not produce symptoms unless the wrist is overloaded (predynamic instability).
Partial scapholunate ligament injury may not be radiologically demonstrable and may not produce symptoms unless the wrist is overloaded (predynamic instability).
![]() If left untreated, a partial scapholunate tear may progress toward a more complete disruption of all three elements of the scapholunate joint, in which case a symptomatic dysfunction usually appears.
If left untreated, a partial scapholunate tear may progress toward a more complete disruption of all three elements of the scapholunate joint, in which case a symptomatic dysfunction usually appears.
![]() Radiographically, a gap between the scaphoid and lunate may be seen. This, however, is visible only under certain loading conditions (dynamic instability).
Radiographically, a gap between the scaphoid and lunate may be seen. This, however, is visible only under certain loading conditions (dynamic instability).

FIG 1 • Schematic representation of the periscaphoid ligaments seen from a dorsoulnar perspective. Both the lunate and the distal row have been drawn away from the scaphoid to better expose the ligaments.
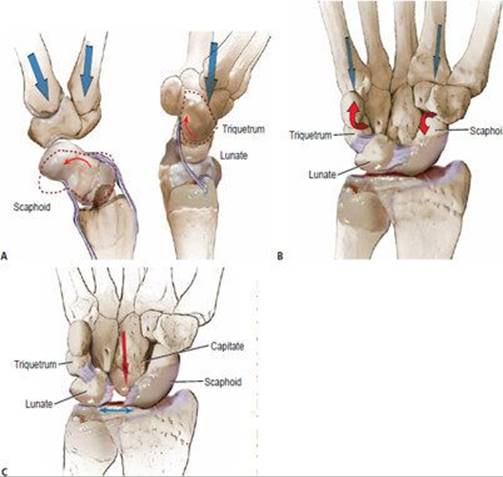
FIG 2 • A. Under axial load (blue arrows) the scaphoid tends to rotate into flexion (red arrows) while the triquetrum tends to extend. B. If both the scapholunate and lunotriquetral ligaments are intact, the two opposite moments counteract each other and a stable equilibrium is reached, allowing force to be transmitted across the proximal row. C. If the scapholunate ligaments fail and the secondary stabilizers do not succeed in maintaining the scaphoid aligned, a diastasis appears between the scaphoid and lunate (red arrow). This gap is formed as the consequence of the capitate edging into that space (blue arrow), forcing the proximal scaphoid to subluxate over the dorsal edge of the distal radius. In such circumstances, the lunate follows the triquetrum into further extension (dorsal intercalated segment instability) and ulnar translation.
![]() With time, the secondary stabilizers (STT and SC ligaments) may stretch out and become inefficient. In such circumstances, the wrist may progress toward permanent malalignment (static instability) (FIG 3A,B).
With time, the secondary stabilizers (STT and SC ligaments) may stretch out and become inefficient. In such circumstances, the wrist may progress toward permanent malalignment (static instability) (FIG 3A,B).
![]() The wrist moves abnormally, with the lunate decreasing its range while progressively adopting an extended position (DISI).
The wrist moves abnormally, with the lunate decreasing its range while progressively adopting an extended position (DISI).
![]() Conversely, the scaphoid adopts a flexed collapsed position, with its proximal pole subluxing dorsoradially over the edge of the radioscaphoid fossa (FIG 3C).
Conversely, the scaphoid adopts a flexed collapsed position, with its proximal pole subluxing dorsoradially over the edge of the radioscaphoid fossa (FIG 3C).
![]() The abnormal joint contact between radius and scaphoid may cause cartilage deterioration of the proximal pole of the scaphoid and the reactive formation of an osteophyte at the tip of the radial styloid. This condition is known as scapholunate advanced collapse (SLAC), stage 1.
The abnormal joint contact between radius and scaphoid may cause cartilage deterioration of the proximal pole of the scaphoid and the reactive formation of an osteophyte at the tip of the radial styloid. This condition is known as scapholunate advanced collapse (SLAC), stage 1.
![]() If untreated, SLAC stage 1 may progress toward a more extended cartilage loss involving the entire scaphoid fossa (SLAC stage 2).
If untreated, SLAC stage 1 may progress toward a more extended cartilage loss involving the entire scaphoid fossa (SLAC stage 2).
![]() As the lunate becomes fixed in DISI, the dorsally subluxing capitate may present with cartilage deterioration progressing from radial to ulnar until it involves the entire capitolunate joint (SLAC stage 3).
As the lunate becomes fixed in DISI, the dorsally subluxing capitate may present with cartilage deterioration progressing from radial to ulnar until it involves the entire capitolunate joint (SLAC stage 3).

FIG 3 • A. PA radiographic view demonstrating a scapholunate gap and a foreshortened scaphoid with the classic ring sign indicating static scapholunate dissociation. B. Coronal MRI showing the remnants of the disrupted proximal membrane hanging into the scapholunate gap, which is filled with fluid. C. Sagittal MRI showing the abnormal dorsal subluxation of the proximal scaphoid over the edge of the radius.
PATIENT HISTORY AND PHYSICAL FINDINGS
![]() Two clinical situations lead to a diagnosis of SLD. One is the patient who presents following violent trauma, such as a fall from a height or a motorcycle accident, who is likely to have a major carpal derangement. Another is the patient who may not recall specific trauma and yet presents with symptoms.
Two clinical situations lead to a diagnosis of SLD. One is the patient who presents following violent trauma, such as a fall from a height or a motorcycle accident, who is likely to have a major carpal derangement. Another is the patient who may not recall specific trauma and yet presents with symptoms.
![]() In the first case, the diagnosis of a major SLD may be obvious.
In the first case, the diagnosis of a major SLD may be obvious.
![]() In the second case, identification of the true nature of dysfunction may require a high index of suspicion, careful examination, and appropriate diagnostic tools.
In the second case, identification of the true nature of dysfunction may require a high index of suspicion, careful examination, and appropriate diagnostic tools.
![]() Not uncommonly, arthroscopy is the only way to fully assess the extent of ligament derangement (see Chap. HA-41).
Not uncommonly, arthroscopy is the only way to fully assess the extent of ligament derangement (see Chap. HA-41).
![]() In both dynamic and static SLD, swelling may be moderate. In acute cases, range of motion may be limited by pain, whereas it may be normal in chronic cases.
In both dynamic and static SLD, swelling may be moderate. In acute cases, range of motion may be limited by pain, whereas it may be normal in chronic cases.
![]() Scapholunate point tenderness: If sharp pain is elicited by pressing this area, the probability of localized synovitis is high. Not all synovitis represents an injury to the scapholunate joint. Occult ganglia may present with a similar type of pain on palpation.
Scapholunate point tenderness: If sharp pain is elicited by pressing this area, the probability of localized synovitis is high. Not all synovitis represents an injury to the scapholunate joint. Occult ganglia may present with a similar type of pain on palpation.
![]() The resisted finger extension test9 has low specificity but excellent sensitivity. In the presence of scapholunate injury, sharp pain is elicited at the scapholunate area, representing dorsal subluxation of the scaphoid.
The resisted finger extension test9 has low specificity but excellent sensitivity. In the presence of scapholunate injury, sharp pain is elicited at the scapholunate area, representing dorsal subluxation of the scaphoid.
![]() Scaphoid shift test9 : If the scapholunate ligaments are completely torn, the proximal pole may sublux dorsally out of the radius, inducing pain on the dorsoradial aspect of the wrist. This test has low specificity: occult ganglia, hyperlaxity, or radioscaphoid degenerative arthritis may produce similar symptoms.
Scaphoid shift test9 : If the scapholunate ligaments are completely torn, the proximal pole may sublux dorsally out of the radius, inducing pain on the dorsoradial aspect of the wrist. This test has low specificity: occult ganglia, hyperlaxity, or radioscaphoid degenerative arthritis may produce similar symptoms.
IMAGING AND OTHER DIAGNOSTIC STUDIES
![]() Posteroanterior radiographic view of the neutral positioned wrist
Posteroanterior radiographic view of the neutral positioned wrist
![]() Increased scapholunate joint space compared with the contralateral side (Terry Thomas sign) suggests static SLD.
Increased scapholunate joint space compared with the contralateral side (Terry Thomas sign) suggests static SLD.
![]() A foreshortened appearance of the scaphoid with the scaphoid tuberosity projected in the form of a ring over the distal two thirds of the scaphoid (ring sign) indicates rotatory subluxation of the scaphoid. The ring sign is not specific for SLD; it may also be present in static LTq dissociations.
A foreshortened appearance of the scaphoid with the scaphoid tuberosity projected in the form of a ring over the distal two thirds of the scaphoid (ring sign) indicates rotatory subluxation of the scaphoid. The ring sign is not specific for SLD; it may also be present in static LTq dissociations.
![]() Lateral radiographic view
Lateral radiographic view
![]() Increased scapholunate angle compared with the contralateral side. For this to be significant, the wrist needs to be in strict neutral alignment and neutral prono-supination.
Increased scapholunate angle compared with the contralateral side. For this to be significant, the wrist needs to be in strict neutral alignment and neutral prono-supination.
![]() Arthroscopy is the gold standard technique in the diagnosis of SLD. It is also useful in describing the degree of injury to the interosseous ligaments.4
Arthroscopy is the gold standard technique in the diagnosis of SLD. It is also useful in describing the degree of injury to the interosseous ligaments.4
![]() Magnetic resonance imaging may provide useful information regarding ligament integrity, bone vascularity, presence of local synovitis, and other soft tissue status.
Magnetic resonance imaging may provide useful information regarding ligament integrity, bone vascularity, presence of local synovitis, and other soft tissue status.
Staging
![]() SLD stage 1: Partial scapholunate ligament injury. Normal wrist alignment. Usually diagnosed by arthroscopy. No abnormal scapholunate gap (Table 1).4,5
SLD stage 1: Partial scapholunate ligament injury. Normal wrist alignment. Usually diagnosed by arthroscopy. No abnormal scapholunate gap (Table 1).4,5

![]() SLD stage 2: Complete scapholunate ligament injury, reparable. Complete disruption of scapholunate ligaments, the dorsal one being still reparable, with good healing potential. Normal wrist alignment.
SLD stage 2: Complete scapholunate ligament injury, reparable. Complete disruption of scapholunate ligaments, the dorsal one being still reparable, with good healing potential. Normal wrist alignment.
![]() SLD stage 3: Complete scapholunate ligament injury, nonreparable, normally aligned scaphoid. Dorsal scapholunate ligament with poor healing capability. Normal carpal alignment.
SLD stage 3: Complete scapholunate ligament injury, nonreparable, normally aligned scaphoid. Dorsal scapholunate ligament with poor healing capability. Normal carpal alignment.
![]() SLD stage 4: Complete scapholunate ligament injury, nonreparable, reducible rotary subluxation of the scaphoid. Complete SLD plus detachment of the dorsal STq ligament off the distal margin of the lunate, plus insufficiency of the distal scaphoid stabilizers (STT and SC ligaments). Rotary subluxation of the scaphoid. Radioscaphoid angle greater than 45 degrees. The lunate may appear abnormally ulnarly translated and in DISI.
SLD stage 4: Complete scapholunate ligament injury, nonreparable, reducible rotary subluxation of the scaphoid. Complete SLD plus detachment of the dorsal STq ligament off the distal margin of the lunate, plus insufficiency of the distal scaphoid stabilizers (STT and SC ligaments). Rotary subluxation of the scaphoid. Radioscaphoid angle greater than 45 degrees. The lunate may appear abnormally ulnarly translated and in DISI.
![]() SLD stage 5: Complete scapholunate ligament injury with irreducible malalignment, but normal cartilage. Fixed, irreducible long-lasting malalignment, without cartilage degeneration.
SLD stage 5: Complete scapholunate ligament injury with irreducible malalignment, but normal cartilage. Fixed, irreducible long-lasting malalignment, without cartilage degeneration.
![]() SLD stage 6: Complete scapholunate ligament injury with irreducible malalignment and cartilage degeneration. Chronic dysfunctional wrists with cartilage degeneration (SLAC).
SLD stage 6: Complete scapholunate ligament injury with irreducible malalignment and cartilage degeneration. Chronic dysfunctional wrists with cartilage degeneration (SLAC).
NONOPERATIVE MANAGEMENT
![]() Acute, minimally dysfunctional SLD, stage 1, may respond well to a period of 3 to 5 weeks of wrist immobilization, anti-inflammatory medication, and subsequent physical rehabilitation.
Acute, minimally dysfunctional SLD, stage 1, may respond well to a period of 3 to 5 weeks of wrist immobilization, anti-inflammatory medication, and subsequent physical rehabilitation.
![]() Re-education of the dynamic scaphoid stabilizing capability of the FCR muscle may be helpful in minimal scapholunate dysfunctions. The FCR uses the scaphoid tuberosity as a hinge toward its distal insertion into the second metacarpal base. Its contraction generates a dorsally directed vector to the unstable scaphoid that prevents its collapse into flexion. Optimization of the time response of the FCR muscle to wrist loading may prevent progression of scapholunate ligament disruption (FIG 4).4
Re-education of the dynamic scaphoid stabilizing capability of the FCR muscle may be helpful in minimal scapholunate dysfunctions. The FCR uses the scaphoid tuberosity as a hinge toward its distal insertion into the second metacarpal base. Its contraction generates a dorsally directed vector to the unstable scaphoid that prevents its collapse into flexion. Optimization of the time response of the FCR muscle to wrist loading may prevent progression of scapholunate ligament disruption (FIG 4).4
SURGICAL MANAGEMENT
![]() Partial ligament injuries may create discomfort from joint irritation by the ligament remnants. Arthroscopic débridement of these fragments may solve this problem.
Partial ligament injuries may create discomfort from joint irritation by the ligament remnants. Arthroscopic débridement of these fragments may solve this problem.
![]() Electrothermal shrinkage of stretched scapholunate ligaments has been shown to be beneficial in selected cases of dynamic instability. Careful control of intra-articular fluid temperature is mandatory. Burns are not rare if lasers are carelessly applied.4
Electrothermal shrinkage of stretched scapholunate ligaments has been shown to be beneficial in selected cases of dynamic instability. Careful control of intra-articular fluid temperature is mandatory. Burns are not rare if lasers are carelessly applied.4

FIG 4 • The flexor carpi radialis (FCR) tendon is in close relationship to the scaphoid tuberosity. Based on this, the scaphoid flexion tendency that appears when the bone is unstable can be effectively compensated by the dynamic action of the FCR muscle. Indeed, proprioception re-education of this muscle may be useful in stage 1 scapholunate dissociation.
![]() Tendon reconstruction of the scapholunate linkage is recommended only in SLD stages 3 or 4—that is, when there is a nonreparable complete scapholunate ligament injury causing carpal malalignment. For this to be successful, however, it is very important that:
Tendon reconstruction of the scapholunate linkage is recommended only in SLD stages 3 or 4—that is, when there is a nonreparable complete scapholunate ligament injury causing carpal malalignment. For this to be successful, however, it is very important that:
![]() The malalignment is easily reducible, and
The malalignment is easily reducible, and
![]() The periscaphoid cartilages are completely normal
The periscaphoid cartilages are completely normal
![]() No soft tissue reconstruction can achieve effective carpal stability if the malalignment cannot be reduced with minimal force.
No soft tissue reconstruction can achieve effective carpal stability if the malalignment cannot be reduced with minimal force.
![]() Intra-articular fibrosis is the most common cause of irreducibility.
Intra-articular fibrosis is the most common cause of irreducibility.
![]() Heavy manual workers are not good candidates for this treatment modality; they may require a more solid form of stabilization, such as a partial fusion.
Heavy manual workers are not good candidates for this treatment modality; they may require a more solid form of stabilization, such as a partial fusion.
![]() Tendon reconstruction cannot solve the loss of protective capsular proprioception, and therefore tenodeses are likely to deteriorate with time if chronically overstressed.
Tendon reconstruction cannot solve the loss of protective capsular proprioception, and therefore tenodeses are likely to deteriorate with time if chronically overstressed.
Preoperative Planning
![]() A complete set of plain radiographic views and stress views are mandatory.
A complete set of plain radiographic views and stress views are mandatory.
![]() Arthroscans (tomograms taken after three-compartment injection of dye) are very useful to assess cartilage status.
Arthroscans (tomograms taken after three-compartment injection of dye) are very useful to assess cartilage status.
![]() Best-quality magnetic resonance imaging may provide useful accessory information regarding bone vascularity, synovitis effects, and soft tissue status.
Best-quality magnetic resonance imaging may provide useful accessory information regarding bone vascularity, synovitis effects, and soft tissue status.
![]() Arthroscopy is by far the best tool for preoperative planning.
Arthroscopy is by far the best tool for preoperative planning.
Positioning
![]() An axillary block is used. The patient is in the supine position. The arm is exsanguinated.
An axillary block is used. The patient is in the supine position. The arm is exsanguinated.
Approach
![]() An 8-cm dorsal zigzag, lazy S, or longitudinal incision of the skin and subcutaneous tissue is centered on the tubercle of Lister.
An 8-cm dorsal zigzag, lazy S, or longitudinal incision of the skin and subcutaneous tissue is centered on the tubercle of Lister.
![]() The dorsal sensory branches of the radial and ulnar nerves are identified and protected.
The dorsal sensory branches of the radial and ulnar nerves are identified and protected.
![]() The extensor retinaculum is divided along the third compartment and the extensor pollicis longus tendon is retracted radially.
The extensor retinaculum is divided along the third compartment and the extensor pollicis longus tendon is retracted radially.
![]() The retinacular septa between compartments II and V are sectioned and the two retinacular flaps so created are retracted. Most septa contain intraseptal vertical vessels that need to be carefully coagulated (FIG 5).
The retinacular septa between compartments II and V are sectioned and the two retinacular flaps so created are retracted. Most septa contain intraseptal vertical vessels that need to be carefully coagulated (FIG 5).

FIG 5 • Dorsal approach to the wrist through a longitudinal incision. The extensor retinaculum has been divided along the third compartment and retracted in the form of two flaps, radial and ulnar. Extensor tendons are uncovered.
TECHNIQUES
DORSAL LIGAMENT-SPLITTING CAPSULOTOMY (BERGER ET AL 1)
![]() The first incision is made along the dorsal rim of the radius to the center of the lunate fossa.
The first incision is made along the dorsal rim of the radius to the center of the lunate fossa.
![]() The second incision is made from the end of the first incision following the fibers of the dorsal radiotriquetral ligament to its distal insertion onto the dorsal ridge of the triquetrum (TECH FIG 1A).
The second incision is made from the end of the first incision following the fibers of the dorsal radiotriquetral ligament to its distal insertion onto the dorsal ridge of the triquetrum (TECH FIG 1A).
![]() The third incision is made from the STT joint progressing medially along the dorsal intercarpal ligament to its insertion onto the dorsum of the triquetrum.
The third incision is made from the STT joint progressing medially along the dorsal intercarpal ligament to its insertion onto the dorsum of the triquetrum.
![]() By connecting the last two incisions, a radially based capsular flap is created. This flap is carefully elevated by sectioning its connections to the dorsal edge of the three bones of the proximal row (TECH FIG 1B).
By connecting the last two incisions, a radially based capsular flap is created. This flap is carefully elevated by sectioning its connections to the dorsal edge of the three bones of the proximal row (TECH FIG 1B).
![]() It is important to leave enough dorsal RTq ligament attached to the triquetrum in order to facilitate later tensioning of the tendon reconstruction.
It is important to leave enough dorsal RTq ligament attached to the triquetrum in order to facilitate later tensioning of the tendon reconstruction.
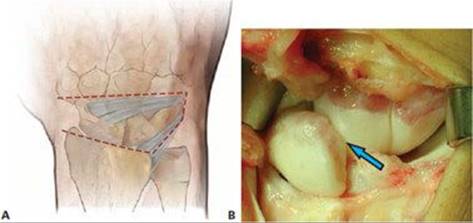
TECH FIG 1 • A. A radially based capsular flap is created by incising the dorsal capsule along the fibers of both the dorsal radiotriquetral ligament and the dorsal intercarpal ligament. B. Once the capsular flap is retracted radially, the scapholunate injury can be inspected (arrow) and a final therapeutic decision can be made.
PALMAR SCAPHOTRAPEZOID PLUS DORSAL RADIOSCAPHOID TENODESIS (BRUNELLI AND BRUNELLI 3)
![]() Beginning at the level of the distal pole of the scaphoid, using small transverse palmar incisions along the course of the FCR, a strip of the FCR tendon is obtained.
Beginning at the level of the distal pole of the scaphoid, using small transverse palmar incisions along the course of the FCR, a strip of the FCR tendon is obtained.
![]() The strip is incised at the musculotendinous junction and left attached distally.
The strip is incised at the musculotendinous junction and left attached distally.
![]() The size of graft harvested depends on the size of the scaphoid and bone tunnel created.
The size of graft harvested depends on the size of the scaphoid and bone tunnel created.
![]() A 2.7to 3.2-mm drill hole is started volarly at the distal pole of the scaphoid, entering at the front of the scaphoid tuberosity to emerge dorsally at the level of the scaphoid neck.
A 2.7to 3.2-mm drill hole is started volarly at the distal pole of the scaphoid, entering at the front of the scaphoid tuberosity to emerge dorsally at the level of the scaphoid neck.
![]() Using a tendon passer or a wire loop, the tendon strip is passed through the bone tunnel.
Using a tendon passer or a wire loop, the tendon strip is passed through the bone tunnel.
![]() While maintaining the proximal pole of the scaphoid reduced on its fossa, two Kirschner wires are passed across the scaphocapitate joint.
While maintaining the proximal pole of the scaphoid reduced on its fossa, two Kirschner wires are passed across the scaphocapitate joint.
![]() Fluoroscopic assessment of reduction is important. Slight overreduction (radioscaphoid angle of about 60 degrees) is recommended.
Fluoroscopic assessment of reduction is important. Slight overreduction (radioscaphoid angle of about 60 degrees) is recommended.
![]() Later stretch of the tenodesis is likely, in which case the scaphoid will recover its ideal alignment of 45 degrees.
Later stretch of the tenodesis is likely, in which case the scaphoid will recover its ideal alignment of 45 degrees.
![]() While the wrist is maintained in neutral position, the tendon is tightly anchored to the area of the tubercle of Lister using transosseous nonabsorbable sutures or metal suture anchors (TECH FIG 2).
While the wrist is maintained in neutral position, the tendon is tightly anchored to the area of the tubercle of Lister using transosseous nonabsorbable sutures or metal suture anchors (TECH FIG 2).
![]() The capsular flap is passed underneath the tenodesis and reattached to its origins by absorbable sutures.
The capsular flap is passed underneath the tenodesis and reattached to its origins by absorbable sutures.
![]() The extensor retinaculum is repaired, leaving subretinacular drains. The extensor pollicis longus is usually left superficial to the extensor retinaculum.
The extensor retinaculum is repaired, leaving subretinacular drains. The extensor pollicis longus is usually left superficial to the extensor retinaculum.

TECH FIG 2 • Schematic representation of the palmar scaphotrapezoid plus dorsal radioscaphoid tenodesis (Brunelli and Brunelli’s technique) as seen from a lateral view. Note the location and direction of the bone tunnel as well as the placement of the suture anchor.
THREE-LIGAMENT TENODESIS (MODIFIED BRUNELLI'S TENODESIS 5,8)
![]() The transscaphoid tunnel is not transverse across the distal scaphoid (as detailed above), but oblique along the longitudinal axis of bone, from dorsal to palmar, entering at the level of the original insertion site of the dorsal scapholunate ligament, aiming at the palmar tuberosity (TECH FIG 3A).
The transscaphoid tunnel is not transverse across the distal scaphoid (as detailed above), but oblique along the longitudinal axis of bone, from dorsal to palmar, entering at the level of the original insertion site of the dorsal scapholunate ligament, aiming at the palmar tuberosity (TECH FIG 3A).
![]() So as not to damage the medial or lateral articular surfaces of the scaphoid, we recommend using a 2.7to 3.2-mm cannulated drill over a Kirschner wire preset under fluoroscopy control.
So as not to damage the medial or lateral articular surfaces of the scaphoid, we recommend using a 2.7to 3.2-mm cannulated drill over a Kirschner wire preset under fluoroscopy control.
![]() The FCR tendon strip is passed through the oblique scaphoid tunnel using a wire loop or a tendon passer (TECH FIG 3B).
The FCR tendon strip is passed through the oblique scaphoid tunnel using a wire loop or a tendon passer (TECH FIG 3B).
![]() A transverse trough or channel is then made over the dorsum of the lunate with a rongeur. This trough needs to uncover cancellous bone, the only tissue able to generate proper healing of the tendon into bone (TECH FIG 3C).
A transverse trough or channel is then made over the dorsum of the lunate with a rongeur. This trough needs to uncover cancellous bone, the only tissue able to generate proper healing of the tendon into bone (TECH FIG 3C).
![]() To obtain intimate contact between the tendon strip and the lunate cancellous bone, a small anchor suture is placed into the floor of the trough.
To obtain intimate contact between the tendon strip and the lunate cancellous bone, a small anchor suture is placed into the floor of the trough.
![]() The distal end of the dorsal radiotriquetral ligament is then localized. By its insertion on the bone, a slit is created through which the tendon strip is passed volar to dorsal (TECH FIG 3D).
The distal end of the dorsal radiotriquetral ligament is then localized. By its insertion on the bone, a slit is created through which the tendon strip is passed volar to dorsal (TECH FIG 3D).
![]() The dorsal radiotriquetral ligament is used as a pulley to tension the ligament strip.
The dorsal radiotriquetral ligament is used as a pulley to tension the ligament strip.
![]() The scaphoid, lunate, and capitate are reduced and stabilized with two 1.5-mm Kirschner wires prior to tensioning the tendon graft. One wire is placed across the scapholunate joint and one across the SC joint.
The scaphoid, lunate, and capitate are reduced and stabilized with two 1.5-mm Kirschner wires prior to tensioning the tendon graft. One wire is placed across the scapholunate joint and one across the SC joint.
![]() It is critical to ensure reduction of the scaphoid and the lunate, elimination of any DISI deformity, and proper placement of the wires using fluoroscopy.
It is critical to ensure reduction of the scaphoid and the lunate, elimination of any DISI deformity, and proper placement of the wires using fluoroscopy.
![]() Radially directed tension is applied to the tendon graft already placed around and through the dorsal radiotriquetral ligament (TECH FIG 3E).
Radially directed tension is applied to the tendon graft already placed around and through the dorsal radiotriquetral ligament (TECH FIG 3E).
![]() The tendon graft is secured tightly into the cancellous bone channel created in the lunate using the suture anchor (TECH FIG 3F).
The tendon graft is secured tightly into the cancellous bone channel created in the lunate using the suture anchor (TECH FIG 3F).
![]() The end of the tendon strip is sutured onto itself with nonabsorbable 3–0 sutures (TECH FIG 3G,H).
The end of the tendon strip is sutured onto itself with nonabsorbable 3–0 sutures (TECH FIG 3G,H).
![]() The capsular flap is brought back, over the tendon reconstruction, to its original position by suturing side-byside the split fibers of the two ligaments involved in the capsulotomy. Some sutures are also placed connecting the capsule and the tendon loop to re-establish the normal capsular attachment to the dorsum of the scapholunate joint.
The capsular flap is brought back, over the tendon reconstruction, to its original position by suturing side-byside the split fibers of the two ligaments involved in the capsulotomy. Some sutures are also placed connecting the capsule and the tendon loop to re-establish the normal capsular attachment to the dorsum of the scapholunate joint.
![]() The extensor retinaculum is finally reconstructed, drains are placed, and the skin is closed.
The extensor retinaculum is finally reconstructed, drains are placed, and the skin is closed.


TECH FIG 3 • A. A 2.7-mm drill is used to create an oblique tunnel that enters the scaphoid beginning at the site where the dorsal scapholunate ligament originally inserted. The drill exits the scaphoid at the palmar scaphoid tubercle. B. With a tendon passer or a wire loop, the strip of FCR tendon is brought through the bone tunnel exiting dorsally. C. The strip of FCR tendon has been passed through the scaphoid tunnel. A trough has been carved onto the dorsal cortex of the lunate and a suture anchor inserted at that location. A slit has been developed along the fibers of the dorsal radiotriquetral ligament. D. The strip of FCR tendon has been passed through the ligament rent created along the fibers of the dorsal radiotriquetral ligament. E. The strip of FCR tendon is tensioned in a radial direction using the dorsal radiotriquetral ligament as a pulley. F. Lateral depiction of the tendon graft secured to the dorsal lunate utilizing the suture anchor. G. After stabilization of the scaphoid, lunate, and capitate with two Kirschner wires, tensioning of the graft, and suturing of the graft into the lunate trough, the strip of FCR tendon is sutured back to itself. H. Final clinical appearance of the tenodesis.

POSTOPERATIVE CARE
![]() The wrist is immobilized in a well-padded splint including the metacarpophalangeal joint of the thumb for 10 days.
The wrist is immobilized in a well-padded splint including the metacarpophalangeal joint of the thumb for 10 days.
![]() After stitch removal, the wrist is maintained in a short-arm thumb spica cast for 5 more weeks.
After stitch removal, the wrist is maintained in a short-arm thumb spica cast for 5 more weeks.
![]() A protective removable splint is then fabricated. This will allow resting the joint between sessions of supervised physiotherapy. The splint is used for an additional 4 weeks.
A protective removable splint is then fabricated. This will allow resting the joint between sessions of supervised physiotherapy. The splint is used for an additional 4 weeks.
![]() Before wire removal, at 8 weeks, therapy consists of only gentle radiocarpal mobilization. After pin removal, global active mobilization is emphasized. Aggressive passive mobilization is never recommended.
Before wire removal, at 8 weeks, therapy consists of only gentle radiocarpal mobilization. After pin removal, global active mobilization is emphasized. Aggressive passive mobilization is never recommended.
![]() Muscle strengthening exercises are not initiated until 10 weeks after surgery.
Muscle strengthening exercises are not initiated until 10 weeks after surgery.
![]() Contact sports are to be avoided for 6 months after surgery.
Contact sports are to be avoided for 6 months after surgery.
OUTCOMES
![]() A recently published review of 38 patients with a symptomatic SLD who had a three-ligament tenodesis procedure, with a mean follow-up of 46 months, showed an average range of motion of about 75% of the contralateral side.5Average grip strength was 65%. Pain relief at rest was obtained in 28 patients, with 8 complaining of mild discomfort during strenuous activity, and 2 having pain in most activities of daily life. Twenty-nine resumed their normal occupationalvocational activities. There were no signs of scaphoid necrosis. Recurrence of carpal collapse occurred in only two wrists. Nine patients showed mild signs of degenerative osteoarthritis at the tip of the radial styloid, but none had substantial symptoms.
A recently published review of 38 patients with a symptomatic SLD who had a three-ligament tenodesis procedure, with a mean follow-up of 46 months, showed an average range of motion of about 75% of the contralateral side.5Average grip strength was 65%. Pain relief at rest was obtained in 28 patients, with 8 complaining of mild discomfort during strenuous activity, and 2 having pain in most activities of daily life. Twenty-nine resumed their normal occupationalvocational activities. There were no signs of scaphoid necrosis. Recurrence of carpal collapse occurred in only two wrists. Nine patients showed mild signs of degenerative osteoarthritis at the tip of the radial styloid, but none had substantial symptoms.
COMPLICATIONS
![]() Recurrence of the malalignment and subsequent development of degenerative arthritis is common when the technique is used inappropriately, in cases with a poorly reducible SLD (stage 5), or when cartilage deterioration is already present (SLAC).
Recurrence of the malalignment and subsequent development of degenerative arthritis is common when the technique is used inappropriately, in cases with a poorly reducible SLD (stage 5), or when cartilage deterioration is already present (SLAC).
![]() When reducibility is in doubt, a more aggressive treatment (partial fusion or proximal row carpectomy) is recommended.
When reducibility is in doubt, a more aggressive treatment (partial fusion or proximal row carpectomy) is recommended.
REFERENCES
1. Berger RA, Bishop AT, Bettinger PC. New dorsal capsulotomy for the surgical exposure of the wrist. Ann Plast Surg 1995;35:54–59.
2. Berger RA, Imaeda T, Berglund L, et al. Constraint and material properties of the subregions of the scapholunate interosseous ligament. J Hand Surg Am 1999;24A:953–962.
3. Brunelli GA, Brunelli GR. A new technique to correct carpal instability with scaphoid rotary subluxation: a preliminary report. J Hand Surg Am 1995;20A:S82–S85.
4. Garcia-Elias M, Geissler WB. Carpal instabilities. In: Green DP, Hotchkiss RN, Pederson WC, et al, eds. Green’s Operative Hand Surgery, 5th ed. Philadelphia: Elsevier-Churchill Livingstone, 2005:535–604.
5. Garcia-Elias M, Lluch A, Stanley KJ. Three-ligament tenodesis for the treatment of scapholunate dissociation: indications and surgical technique. J Hand Surg Am 2006;31A:125–134.
6. Linscheid RL, Dobyns JH, Beabout JW, et al. Traumatic instability of the wrist: diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54A:1612–1632.
7. Short WH, Werner FW, Green JK, et al. Biomechanical evaluation of ligamentous stabilizers of the scaphoid and lunate. J Hand Surg Am 2002;27A:991–1002.
8. Van Den Abbeele KLS, Loh YC, Stanley JK, et al. Early results of a modified Brunelli procedure for scapholunate instability. J Hand Surg Br 1998;23B:258–261.
9. Watson HK, Ashmead D IV, Makhlouf MV. Examination of the scaphoid. J Hand Surg Am 1988;13A:657–660.