Bruce A. Monaghan
DEFINITION
![]() Arthritis between the radial styloid and the distal aspect of the scaphoid can lead to pain, weakness of grip, and limitation of motion. This arthritis can occur in the early stages of a variety of pathologic states of the radiocarpal joint.
Arthritis between the radial styloid and the distal aspect of the scaphoid can lead to pain, weakness of grip, and limitation of motion. This arthritis can occur in the early stages of a variety of pathologic states of the radiocarpal joint.
![]() Radial styloidectomy is a technique that involves resection of the distalmost aspect of the articular surface of the distal radius.
Radial styloidectomy is a technique that involves resection of the distalmost aspect of the articular surface of the distal radius.
![]() A radial styloidectomy can be performed as a distinct procedure via an open incision or by arthroscopic means. It is more commonly undertaken as an adjunct procedure with reconstructive or salvage procedures for scaphoid nonunions, carpal instabilities, Kienböck disease, or posttraumatic arthritis of the radiocarpal joint.9,17
A radial styloidectomy can be performed as a distinct procedure via an open incision or by arthroscopic means. It is more commonly undertaken as an adjunct procedure with reconstructive or salvage procedures for scaphoid nonunions, carpal instabilities, Kienböck disease, or posttraumatic arthritis of the radiocarpal joint.9,17
ANATOMY
![]() The radial styloid is the distalmost projection on the lateral aspect of the terminal end of the radius (FIG 1A,B).
The radial styloid is the distalmost projection on the lateral aspect of the terminal end of the radius (FIG 1A,B).
![]() When viewed from the lateral aspect, the styloid has a gentle slope volarly, placing it below the midcoronal longitudinal axis of the radius.
When viewed from the lateral aspect, the styloid has a gentle slope volarly, placing it below the midcoronal longitudinal axis of the radius.
![]() The intra-articular component of the radial styloid encompasses part of the scaphoid facet.
The intra-articular component of the radial styloid encompasses part of the scaphoid facet.
![]() The extra-articular aspect of the styloid serves as the origin of several dorsal, palmar, and radial extrinsic ligaments that are vital to normal carpal kinematics (FIG 1C).
The extra-articular aspect of the styloid serves as the origin of several dorsal, palmar, and radial extrinsic ligaments that are vital to normal carpal kinematics (FIG 1C).
![]() The palmar radiocarpal ligaments serve as a constraint to radiocarpal pronation, ulnar translation, and distal pole scaphoid stabilization. Global disruption of this complex has been implicated in perilunate dislocation. The palmar radiocarpal ligaments are composed of the following structures:
The palmar radiocarpal ligaments serve as a constraint to radiocarpal pronation, ulnar translation, and distal pole scaphoid stabilization. Global disruption of this complex has been implicated in perilunate dislocation. The palmar radiocarpal ligaments are composed of the following structures:
![]() The radial collateral ligament (RCL) is a thin structure that originates from the tip of the radial styloid and inserts into the waist and distal aspect of the scaphoid. The integrity of the ligament is always sacrificed with a radial styloidectomy, but no untoward effects have been reported.3,4
The radial collateral ligament (RCL) is a thin structure that originates from the tip of the radial styloid and inserts into the waist and distal aspect of the scaphoid. The integrity of the ligament is always sacrificed with a radial styloidectomy, but no untoward effects have been reported.3,4
![]() The radioscaphocapitate (RSC) ligament originates from the palmar cortex of the distal radius coursing distally and ulnarly, attaching to the waist and proximal cortex of the distal pole of the scaphoid and the body of the capitate.3,4
The radioscaphocapitate (RSC) ligament originates from the palmar cortex of the distal radius coursing distally and ulnarly, attaching to the waist and proximal cortex of the distal pole of the scaphoid and the body of the capitate.3,4
![]() The long radiolunate ligament (LRL) originates from the palmar cortical margin of the distal radius immediately adjacent and medial to the RSC ligament. It is separated from the RSC by a distinct sulcus that serves an arthroscopic landmark.3,4
The long radiolunate ligament (LRL) originates from the palmar cortical margin of the distal radius immediately adjacent and medial to the RSC ligament. It is separated from the RSC by a distinct sulcus that serves an arthroscopic landmark.3,4
![]() The dorsal radiocarpal (DRC) ligament originates broadly from the dorsal rim of the distal radius around the tubercle of Lister, coursing ulnarly, distally, and obliquely to insert on the dorsal tubercle of the triquetrum.
The dorsal radiocarpal (DRC) ligament originates broadly from the dorsal rim of the distal radius around the tubercle of Lister, coursing ulnarly, distally, and obliquely to insert on the dorsal tubercle of the triquetrum.
![]() The radialmost fibers of this ligament also insert on the dorsal lunate.
The radialmost fibers of this ligament also insert on the dorsal lunate.
![]() The DRC ligament, in concert with the dorsal intercarpal ligament, has a crucial role in maintaining normal carpal kinematics and carpal stability and preventing ulnar translation of the carpus.14,15
The DRC ligament, in concert with the dorsal intercarpal ligament, has a crucial role in maintaining normal carpal kinematics and carpal stability and preventing ulnar translation of the carpus.14,15
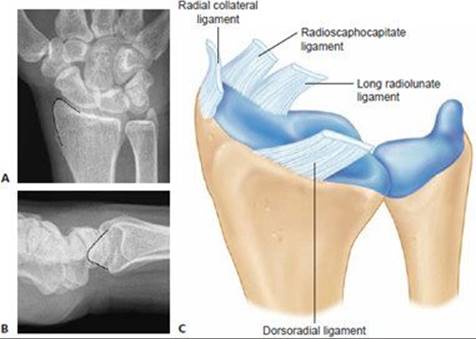
FIG 1 • A,B. The radial styloid outlined on a standard PA and lateral wrist radiograph. C. Palmar and dorsal extrinsic ligaments of the radiocarpal joint. Note the broad origin of the dorsoradial ligament. The radial collateral ligament originates from the tip of the styloid. The radioscaphocapitate and long radiolunate ligaments are separated by a well-defined sulcus readily seen arthroscopically.

FIG 2 • Styloidectomies as described by Nakamura and Siegel and Gelberman.
![]() Siegel and Gelberman13 examined the effect of three different styloidectomy configurations on palmar radiocarpal ligament integrity in a cadaver model (FIG 2).
Siegel and Gelberman13 examined the effect of three different styloidectomy configurations on palmar radiocarpal ligament integrity in a cadaver model (FIG 2).
![]() The most conservative osteotomy (short oblique) removed only 9% of the RSC and none of the LRL ligaments.
The most conservative osteotomy (short oblique) removed only 9% of the RSC and none of the LRL ligaments.
![]() A vertical oblique osteotomy sacrificed 92% of the RSC and 21% of the LRL ligaments.
A vertical oblique osteotomy sacrificed 92% of the RSC and 21% of the LRL ligaments.
![]() A transverse styloidectomy was the most aggressive and resulted in loss of 95% of the RSC and 42% loss of the LRL ligaments.
A transverse styloidectomy was the most aggressive and resulted in loss of 95% of the RSC and 42% loss of the LRL ligaments.
![]() Nakamura et al10 examined the effect of radial styloidectomy on carpal alignment and ulnar translation in cadaveric limbs. They demonstrated that as a larger segment of the radial styloid was resected (FIG 2), a greater tendency toward ulnar translation, as manifested by decreased stiffness, was observed. No frank ulnar translation with axial loading was observed.
Nakamura et al10 examined the effect of radial styloidectomy on carpal alignment and ulnar translation in cadaveric limbs. They demonstrated that as a larger segment of the radial styloid was resected (FIG 2), a greater tendency toward ulnar translation, as manifested by decreased stiffness, was observed. No frank ulnar translation with axial loading was observed.
![]() Based on their analysis, they recommended that no more than 3 to 4 mm of radial styloid should be resected. This correlated with a short oblique styloidectomy as described by Siegel and Gelberman.
Based on their analysis, they recommended that no more than 3 to 4 mm of radial styloid should be resected. This correlated with a short oblique styloidectomy as described by Siegel and Gelberman.
![]() Although ulnar translation is a stated complication of overly vigorous styloidectomy, Viegas et al14 demonstrated in a cadaver model that ulnar translation can occur only with resection of the DRC, RSC, LRL, and SRL ligaments.
Although ulnar translation is a stated complication of overly vigorous styloidectomy, Viegas et al14 demonstrated in a cadaver model that ulnar translation can occur only with resection of the DRC, RSC, LRL, and SRL ligaments.
PATHOGENESIS AND NATURAL HISTORY
Scapholunate Instability
![]() Watson and Ballet16 reviewed radiographs of individuals with scapholunate dissociation to establish the sequential progression of arthritis in the scapholunate advanced collapse (SLAC) wrist (FIG 3).
Watson and Ballet16 reviewed radiographs of individuals with scapholunate dissociation to establish the sequential progression of arthritis in the scapholunate advanced collapse (SLAC) wrist (FIG 3).
![]() SLAC I: Degenerative changes are confined to the radial styloid area.
SLAC I: Degenerative changes are confined to the radial styloid area.
![]() SLAC II: Changes are characterized by joint space narrowing involving the entire radioscaphoid articulation.
SLAC II: Changes are characterized by joint space narrowing involving the entire radioscaphoid articulation.
![]() SLAC III: Changes involve additional arthritis between the capitate and lunate.
SLAC III: Changes involve additional arthritis between the capitate and lunate.
![]() Several authors have examined the mechanics of scapholunate dissociation in cadaver models and have demonstrated that scapholunate instability leads to a shift in the contact pressures from the proximal pole of scaphoid articulation with the radial articular surface toward the distal pole of the scaphoid with the dorsal lip of the radial styloid.6,7 The pathomechanics of these changes can occur even before the frank radiographic appearance of scapholunate diastasis is present (ie, static scapholunate instability). Prolonged exposure to these abnormal contact stresses leads to the predictable arthritic changes described above.
Several authors have examined the mechanics of scapholunate dissociation in cadaver models and have demonstrated that scapholunate instability leads to a shift in the contact pressures from the proximal pole of scaphoid articulation with the radial articular surface toward the distal pole of the scaphoid with the dorsal lip of the radial styloid.6,7 The pathomechanics of these changes can occur even before the frank radiographic appearance of scapholunate diastasis is present (ie, static scapholunate instability). Prolonged exposure to these abnormal contact stresses leads to the predictable arthritic changes described above.
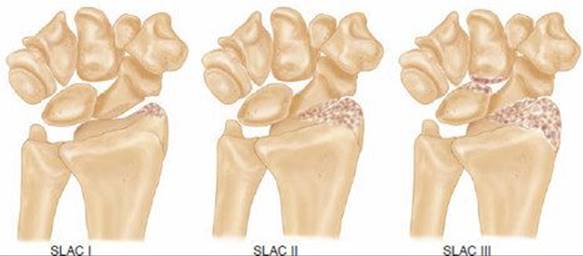
FIG 3 • Stages of arthritis with scapholunate advanced collapse (SLAC). SLAC I: degenerative changes are confined to the radial styloid. SLAC II: joint space narrowing of the entire radioscaphoid articulation. SLAC III: chondral changes in the radioscaphoid and capitolunate joint.
![]() Scaphoid nonunion
Scaphoid nonunion
![]() With an unstable scaphoid fracture, the proximal pole of the scaphoid remains firmly fixed to and extends with the lunate through an intact scapholunate interosseous ligament. The distal pole adopts a flexed posture, which can then impinge upon the radial styloid, leading to abnormal contact stresses and arthritic changes.
With an unstable scaphoid fracture, the proximal pole of the scaphoid remains firmly fixed to and extends with the lunate through an intact scapholunate interosseous ligament. The distal pole adopts a flexed posture, which can then impinge upon the radial styloid, leading to abnormal contact stresses and arthritic changes.
![]() The natural history of scaphoid nonunion has not been established by rigorous prospective analysis. Nonetheless, most surgeons believe that unstable scaphoid fractures result in abnormal carpal kinematics with a dorsal intercalated segment instability (DISI) deformity and subsequent arthritis (scaphoid nonunion advanced collapse [SNAC] wrist).
The natural history of scaphoid nonunion has not been established by rigorous prospective analysis. Nonetheless, most surgeons believe that unstable scaphoid fractures result in abnormal carpal kinematics with a dorsal intercalated segment instability (DISI) deformity and subsequent arthritis (scaphoid nonunion advanced collapse [SNAC] wrist).
![]() Inoue and Sakuma8 reviewed 102 patients with scaphoid nonunions clinically and radiographically; they found that arthritis initially developed at the scaphoid–radial styloid articulation and subsequently the midcarpal joint. All patients had radiographic arthritis within 10 years of injury. They also demonstrated that although radiographic progression did not correlate with wrist pain, it did correlate with a decrease in grip strength and range of motion.
Inoue and Sakuma8 reviewed 102 patients with scaphoid nonunions clinically and radiographically; they found that arthritis initially developed at the scaphoid–radial styloid articulation and subsequently the midcarpal joint. All patients had radiographic arthritis within 10 years of injury. They also demonstrated that although radiographic progression did not correlate with wrist pain, it did correlate with a decrease in grip strength and range of motion.
![]() Impingement after triscaphe (scaphoid-trapezoid-trapezium) fusion
Impingement after triscaphe (scaphoid-trapezoid-trapezium) fusion
![]() Rogers and Watson12 reviewed 93 patients after triscaphe fusion and found a 33% incidence of painful impingement between the fusion mass and the radial styloid that resolved after limited radial styloidectomy. They hypothesized that the fixed scaphoid could no longer be accommodated in the fossa and impacted upon the radial styloid.
Rogers and Watson12 reviewed 93 patients after triscaphe fusion and found a 33% incidence of painful impingement between the fusion mass and the radial styloid that resolved after limited radial styloidectomy. They hypothesized that the fixed scaphoid could no longer be accommodated in the fossa and impacted upon the radial styloid.
![]() Proximal row carpectomy
Proximal row carpectomy
![]() Although not all surgeons routinely perform a radial styloidectomy in the setting of a proximal row carpectomy, a recent cadaveric study demonstrated that radial deviation after proximal-row carpectomy was limited by impingement of the trapezoid on the radial styloid.5
Although not all surgeons routinely perform a radial styloidectomy in the setting of a proximal row carpectomy, a recent cadaveric study demonstrated that radial deviation after proximal-row carpectomy was limited by impingement of the trapezoid on the radial styloid.5
PATIENT HISTORY AND PHYSICAL FINDINGS
![]() Patients with clinically significant radial styloid arthritis or impingement frequently complain of pain along the dorsal radial aspect of the wrist that is exacerbated by extension of the wrist or gripping activities. They may also note focal swelling or a decrease in the range of motion.
Patients with clinically significant radial styloid arthritis or impingement frequently complain of pain along the dorsal radial aspect of the wrist that is exacerbated by extension of the wrist or gripping activities. They may also note focal swelling or a decrease in the range of motion.
![]() A complete physical examination of the radiocarpal, the midcarpal, and the first carpometacarpal joints is necessary to assess for associated conditions and to rule out alternative diagnoses.
A complete physical examination of the radiocarpal, the midcarpal, and the first carpometacarpal joints is necessary to assess for associated conditions and to rule out alternative diagnoses.
![]() Styloid impingement typically causes radial-sided wrist pain that is exacerbated by radial deviation, extension, and loading of the wrist.
Styloid impingement typically causes radial-sided wrist pain that is exacerbated by radial deviation, extension, and loading of the wrist.
![]() Physical findings of styloid impingement are centered around the anatomic snuffbox (FIG 4).
Physical findings of styloid impingement are centered around the anatomic snuffbox (FIG 4).
![]() The anatomic snuffbox is triangular, with its radial border formed by the extensor pollicis brevis tendon, its ulnar border by the extensor pollicis longus tendon, and its proximal border by the dorsal rim of the distal radius at the level of the styloid. The waist of the scaphoid and a small segment of the trapezium are palpable in the floor of the snuffbox, more readily with ulnar deviation.
The anatomic snuffbox is triangular, with its radial border formed by the extensor pollicis brevis tendon, its ulnar border by the extensor pollicis longus tendon, and its proximal border by the dorsal rim of the distal radius at the level of the styloid. The waist of the scaphoid and a small segment of the trapezium are palpable in the floor of the snuffbox, more readily with ulnar deviation.
![]() Focal tenderness and synovitis along the proximal edge of the snuffbox made worse by forced radial deviation and extension may be indicative of styloid impingement.
Focal tenderness and synovitis along the proximal edge of the snuffbox made worse by forced radial deviation and extension may be indicative of styloid impingement.
![]() More diffuse tenderness, synovitis, and global limitations of motion may be indicative of a more advanced stage of posttraumatic arthritis or an inflammatory process (rheumatoid arthritis), which would preclude the success of a radial styloidectomy.
More diffuse tenderness, synovitis, and global limitations of motion may be indicative of a more advanced stage of posttraumatic arthritis or an inflammatory process (rheumatoid arthritis), which would preclude the success of a radial styloidectomy.
IMAGING AND OTHER DIAGNOSTIC STUDIES
![]() Plain radiographs of the wrist
Plain radiographs of the wrist
![]() To diagnosis and stage SNAC and SLAC (FIG 5)
To diagnosis and stage SNAC and SLAC (FIG 5)
![]() To rule out scaphoid fracture or other acute injury
To rule out scaphoid fracture or other acute injury
![]() Stress radiographs (clenched fist and radial–ulnar deviation posteroanterior) of the wrist can yield information concerning dynamic impingement between the scaphoid and the radial styloid.
Stress radiographs (clenched fist and radial–ulnar deviation posteroanterior) of the wrist can yield information concerning dynamic impingement between the scaphoid and the radial styloid.
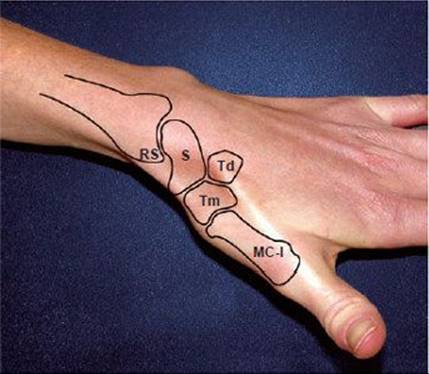
FIG 4 • Meticulous and systematic physical examination of this region can rule out diagnoses other than radial styloid impingement. RS, radial styloid; S, scaphoid; Tm, trapezium; Td, trapezoid; MC-I, thumb metacarpal.

FIG 5 • Impingement of the flexed distal pole of the scaphoid nonunion against the radial styloid leading to arthritic changes.
DIFFERENTIAL DIAGNOSIS
![]() DeQuervain stenosing tenosynovitis: Tenderness usually extends along the extra-articular component of the radial styloid, proximally and radially over the first dorsal compartment. A positive Finkelstein test is highly suggestive of this disorder.
DeQuervain stenosing tenosynovitis: Tenderness usually extends along the extra-articular component of the radial styloid, proximally and radially over the first dorsal compartment. A positive Finkelstein test is highly suggestive of this disorder.
![]() Scapho-trapezoid-trapezial arthritis: focal tenderness in the distal-ulnar aspect of the snuffbox under the extensor pollicis long tendon along the axis of the second metacarpal
Scapho-trapezoid-trapezial arthritis: focal tenderness in the distal-ulnar aspect of the snuffbox under the extensor pollicis long tendon along the axis of the second metacarpal
![]() Thumb carpometacarpal instability or arthritis: tenderness distal to the anatomic snuffbox that is worsened by loading of the thumb ray (CMC grind test)
Thumb carpometacarpal instability or arthritis: tenderness distal to the anatomic snuffbox that is worsened by loading of the thumb ray (CMC grind test)
![]() Scaphoid fracture: After an acute injury, special imaging (bone scan or MRI) may be required to rule out an acute scaphoid fracture.
Scaphoid fracture: After an acute injury, special imaging (bone scan or MRI) may be required to rule out an acute scaphoid fracture.
![]() Preiser disease
Preiser disease
![]() Inflammatory arthritis (ie, rheumatoid)
Inflammatory arthritis (ie, rheumatoid)
![]() Radial sensory neuritis or neuroma
Radial sensory neuritis or neuroma
![]() Tenosynovitis of the extensor carpi radialis longus and brevis
Tenosynovitis of the extensor carpi radialis longus and brevis
![]() Not uncommonly, styloid impingement coexists with other diagnoses, especially basilar thumb arthritis and De Quervain stenosing tenosynovitis.
Not uncommonly, styloid impingement coexists with other diagnoses, especially basilar thumb arthritis and De Quervain stenosing tenosynovitis.
NONOPERATIVE MANAGEMENT
![]() Individuals with chronic SLAC or SNAC wrist arthritis frequently present with acute pain after a recent injury. After obtaining an accurate medical history of prior injury and radiographic assessment, the chronicity of the problem is usually evident.
Individuals with chronic SLAC or SNAC wrist arthritis frequently present with acute pain after a recent injury. After obtaining an accurate medical history of prior injury and radiographic assessment, the chronicity of the problem is usually evident.
![]() In this situation, a course of conservative treatment with activity modification, nonsteroidal anti-inflammatory drugs, rest in a forearm-based thumb spica splint, and selective corticosteroid injection in the radial styloid area is appropriate.
In this situation, a course of conservative treatment with activity modification, nonsteroidal anti-inflammatory drugs, rest in a forearm-based thumb spica splint, and selective corticosteroid injection in the radial styloid area is appropriate.
![]() If the arthritic changes are truly isolated to the area of articulation between the scaphoid and the styloid, the surgeon may elect earlier operative intervention with the theoretical goal of slowing or preventing progressive arthrosis and the need for a more extensive reconstructive procedure.
If the arthritic changes are truly isolated to the area of articulation between the scaphoid and the styloid, the surgeon may elect earlier operative intervention with the theoretical goal of slowing or preventing progressive arthrosis and the need for a more extensive reconstructive procedure.
SURGICAL MANAGEMENT
![]() Isolated radial styloidectomy is a limited procedure to treat the early stage of progressive posttraumatic arthritis.
Isolated radial styloidectomy is a limited procedure to treat the early stage of progressive posttraumatic arthritis.
![]() It cannot be expected to prevent its pathologic progression.
It cannot be expected to prevent its pathologic progression.
![]() It can also be employed as a temporizing solution in a low-demand individual or in a patient unfit or unwilling to undertake a more extensive procedure and postoperative rehabilitative course.
It can also be employed as a temporizing solution in a low-demand individual or in a patient unfit or unwilling to undertake a more extensive procedure and postoperative rehabilitative course.
![]() In that instance, patient expectations with respect to motion and pain relief must be assiduously managed.
In that instance, patient expectations with respect to motion and pain relief must be assiduously managed.
![]() Arthroscopic radial styloidectomy has the theoretical advantages of being minimally invasive and allowing more precise control of the level of bony resection to minimize injury to the palmar radiocarpal ligaments. In addition, arthroscopic evaluation of the radiocarpal and midcarpal joints can allow for diagnosis and treatment of concomitant intra-articular pathology.17
Arthroscopic radial styloidectomy has the theoretical advantages of being minimally invasive and allowing more precise control of the level of bony resection to minimize injury to the palmar radiocarpal ligaments. In addition, arthroscopic evaluation of the radiocarpal and midcarpal joints can allow for diagnosis and treatment of concomitant intra-articular pathology.17
Preoperative Planning
![]() Precise radiographic assessment and patient selection are critical in ensuring a good outcome. The surgeon must review all radiographic studies and the severity, characteristics, and nature of the patient’s symptoms and physical findings.
Precise radiographic assessment and patient selection are critical in ensuring a good outcome. The surgeon must review all radiographic studies and the severity, characteristics, and nature of the patient’s symptoms and physical findings.
![]() In some cases, final staging of the severity of articular degeneration can be made only by direct visualization with diagnostic wrist arthroscopy (FIG 6). An isolated radial styloidectomy or a more extensive reconstructive procedure can be done at the time of arthroscopy or at a later time, after the implications of the arthroscopic findings are discussed with the patient.
In some cases, final staging of the severity of articular degeneration can be made only by direct visualization with diagnostic wrist arthroscopy (FIG 6). An isolated radial styloidectomy or a more extensive reconstructive procedure can be done at the time of arthroscopy or at a later time, after the implications of the arthroscopic findings are discussed with the patient.
Positioning
![]() The patient is positioned supine on a stretcher with an attached hand table and the arm centered on the hand table with the shoulder abducted 90 degrees. A mini-fluoroscopy unit is draped in a sterile fashion and placed in a plane perpendicular to the hand table.
The patient is positioned supine on a stretcher with an attached hand table and the arm centered on the hand table with the shoulder abducted 90 degrees. A mini-fluoroscopy unit is draped in a sterile fashion and placed in a plane perpendicular to the hand table.
![]() For arthroscopic procedures, the arm is stabilized to the hand table with a strap that allows countertraction.
For arthroscopic procedures, the arm is stabilized to the hand table with a strap that allows countertraction.
![]() The shoulder is abducted 90 degrees, the elbow is flexed 90 degrees, and finger traps are placed on the index and middle fingers.
The shoulder is abducted 90 degrees, the elbow is flexed 90 degrees, and finger traps are placed on the index and middle fingers.
![]() The forearm is suspended in a standard wrist traction tower with 8 to 12 pounds of traction employed.
The forearm is suspended in a standard wrist traction tower with 8 to 12 pounds of traction employed.
![]() A mini-fluoroscopy unit is draped in a sterile fashion and placed in a plane parallel to and above the hand table.
A mini-fluoroscopy unit is draped in a sterile fashion and placed in a plane parallel to and above the hand table.
![]() Alternatively, the hand can be suspended via finger traps using a nonsterile overhead traction boom (ie, an arthroscopic shoulder holder); in this case, the wrist traction tower will not be an impediment to intraoperative fluoroscopic assessment.
Alternatively, the hand can be suspended via finger traps using a nonsterile overhead traction boom (ie, an arthroscopic shoulder holder); in this case, the wrist traction tower will not be an impediment to intraoperative fluoroscopic assessment.
Approach
![]() A radial styloidectomy can be performed in conjunction with other reconstructive procedures such as proximal-row carpectomy, intercarpal fusion, or bone grafting for a scaphoid nonunion.
A radial styloidectomy can be performed in conjunction with other reconstructive procedures such as proximal-row carpectomy, intercarpal fusion, or bone grafting for a scaphoid nonunion.
![]() In these instances, the primary procedure usually requires wide exposure through a standard dorsal approach to the wrist.
In these instances, the primary procedure usually requires wide exposure through a standard dorsal approach to the wrist.
![]() An isolated styloidectomy can be performed through a limited radial incision.
An isolated styloidectomy can be performed through a limited radial incision.
![]() An arthroscopic styloidectomy can be performed through standard arthroscopic portals.
An arthroscopic styloidectomy can be performed through standard arthroscopic portals.

FIG 6 • Arthroscopic findings of full-thickness cartilage loss in the entire scaphoid facet (dashed line) and proximal pole of the scaphoid as viewed from the dorsal 3-4 portal. These degenerative changes were not readily apparent on plain radiographs. An isolated radial styloidectomy cannot be expected to confer pain relief in this instance.
TECHNIQUES
OPEN RADIAL STYLOIDECTOMY
![]() Expose the radial styloid by sharp dissection (TECH FIG 1C).
Expose the radial styloid by sharp dissection (TECH FIG 1C).
![]() Using a sharp osteotome, remove the distal 3 to 4 mm of radial styloid. The plane of the cut should be perpendicular to the articular surface (TECH FIG 1D).
Using a sharp osteotome, remove the distal 3 to 4 mm of radial styloid. The plane of the cut should be perpendicular to the articular surface (TECH FIG 1D).
![]() Fluoroscopic imaging of the level of resection can be useful at this point in the procedure.
Fluoroscopic imaging of the level of resection can be useful at this point in the procedure.
![]() A narrow malleable retractor can be placed in the radiocarpal joint to prevent damage to the scaphoid as the styloid is being resected (TECH FIG 1E).
A narrow malleable retractor can be placed in the radiocarpal joint to prevent damage to the scaphoid as the styloid is being resected (TECH FIG 1E).
![]() After styloidectomy, fluoroscopic examination with the wrist in radial and ulnar deviation to assess for impingement confirms adequacy of the resection level (TECH FIG 1F,G).
After styloidectomy, fluoroscopic examination with the wrist in radial and ulnar deviation to assess for impingement confirms adequacy of the resection level (TECH FIG 1F,G).
![]() Loosely reapproximate the periosteum with resorbable suture, allow the extensor compartments to fall back into their anatomic position, and suture the skin. A bulky dressing and volar splint holding the wrist is applied.
Loosely reapproximate the periosteum with resorbable suture, allow the extensor compartments to fall back into their anatomic position, and suture the skin. A bulky dressing and volar splint holding the wrist is applied.
![]() Palpate the distalmost aspect of the radial styloid on the volar radial aspect of the wrist. Make an incision from that point for 2 or 3 cm proximally and obliquely between the first and second extensor compartments (TECH FIG 1A).
Palpate the distalmost aspect of the radial styloid on the volar radial aspect of the wrist. Make an incision from that point for 2 or 3 cm proximally and obliquely between the first and second extensor compartments (TECH FIG 1A).
![]() Alternatively, a transverse incision may provide a more cosmetically pleasing scar but also may limit exposure.
Alternatively, a transverse incision may provide a more cosmetically pleasing scar but also may limit exposure.
![]() At this level, there will be arborization of the terminal branches of the radial sensory and lateral antebrachial cutaneous nerves in the subcutaneous tissue.2 Use blunt dissection and gentle retraction to expose the first and second compartments.
At this level, there will be arborization of the terminal branches of the radial sensory and lateral antebrachial cutaneous nerves in the subcutaneous tissue.2 Use blunt dissection and gentle retraction to expose the first and second compartments.
![]() Distal placement of the incision may place the dorsal branch of the radial artery at risk and should be recognized.
Distal placement of the incision may place the dorsal branch of the radial artery at risk and should be recognized.
![]() Incise the extensor retinaculum in the 1–2 interval and expose the radial styloid by subperiosteal dissection. Alternatively, the radius can be approached through the floor of the first compartment (TECH FIG 1B).
Incise the extensor retinaculum in the 1–2 interval and expose the radial styloid by subperiosteal dissection. Alternatively, the radius can be approached through the floor of the first compartment (TECH FIG 1B).
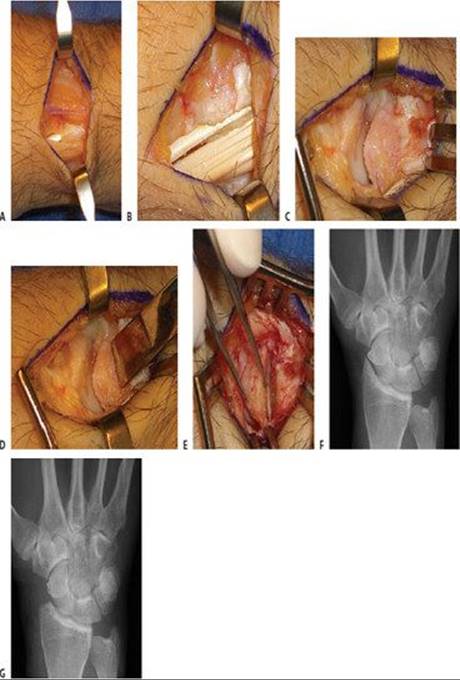
TECH FIG 1 • Open radial styloidectomy. A. A 2to 3-cm oblique skin incision is made between the first and second extensor compartments. Note the branches of the radial sensory and lateral antebrachial cutaneous nerves. B. The first dorsal compartment is then opened. C. The radial styloid is extraperiosteally exposed by sharp dissection. D. An osteotome is used to resect the distal 3 to 4 mm of radial styloid. The osteotome should be angled perpendicular to the joint surface. E. The resected radial styloid is removed. F,G. Preoperative and postoperative PA radiographs of the wrist with early scaphoid nonunion advanced collapse [SNAC] undergoing open radial styloidectomy. (Courtesy of Dr. John J. Fernandez.)
ARTHROSCOPIC STYLOIDECTOMY
![]() After patient positioning as previously described, insufflate the joint with 5 to 10 mL of sterile saline and establish the 3-4 portal. Outflow is achieved by placing an 18-gauge needle in the 6U interval. Perform a complete arthroscopic evaluation of the radiocarpal joint.
After patient positioning as previously described, insufflate the joint with 5 to 10 mL of sterile saline and establish the 3-4 portal. Outflow is achieved by placing an 18-gauge needle in the 6U interval. Perform a complete arthroscopic evaluation of the radiocarpal joint.
![]() Establish the radial and ulnar midcarpal portals and perform an arthroscopic evaluation to confirm capitolunate joint preservation.
Establish the radial and ulnar midcarpal portals and perform an arthroscopic evaluation to confirm capitolunate joint preservation.
![]() Place a localization needle into the styloscaphoid joint space, in the interval between the first and second compartments.
Place a localization needle into the styloscaphoid joint space, in the interval between the first and second compartments.
![]() Confirm the adequacy of the position of this working portal by arthroscopic evaluation from the 3–4 interval.
Confirm the adequacy of the position of this working portal by arthroscopic evaluation from the 3–4 interval.
![]() Develop the portal by sharp dissection through skin only and blunt dissection in the subcutaneous tissues to the capsule to prevent damage to the radial sensory nerve, the lateral antebrachial cutaneous nerve, and the radial artery.
Develop the portal by sharp dissection through skin only and blunt dissection in the subcutaneous tissues to the capsule to prevent damage to the radial sensory nerve, the lateral antebrachial cutaneous nerve, and the radial artery.
![]() Resect the radial styloid with a 2.9-mm full-radius resector, an arthroscopic covered burr, or both (TECH FIG 2A). This is initiated at the radial margin of the radioscaphocapitate ligament and carried radially. The diameter of the burr can be used as a gauge for the amount of bone being resected.
Resect the radial styloid with a 2.9-mm full-radius resector, an arthroscopic covered burr, or both (TECH FIG 2A). This is initiated at the radial margin of the radioscaphocapitate ligament and carried radially. The diameter of the burr can be used as a gauge for the amount of bone being resected.
![]() Intraoperative fluoroscopy is critical in the assessment of the resection level (TECH FIG 2B).
Intraoperative fluoroscopy is critical in the assessment of the resection level (TECH FIG 2B).
![]() After completing the styloidectomy, remove the arthroscopic instruments and suture the portals. Apply a sterile bulky dressing and volar splint to the wrist and forearm.
After completing the styloidectomy, remove the arthroscopic instruments and suture the portals. Apply a sterile bulky dressing and volar splint to the wrist and forearm.
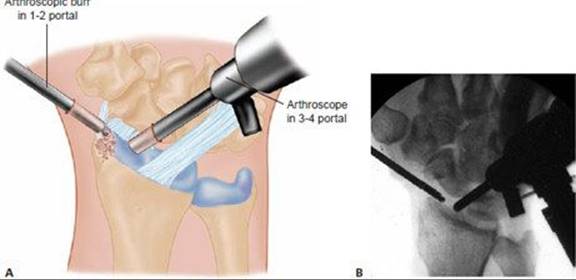
TECH FIG 2 • Arthroscopic radial styloidectomy. A. The arthroscopic burr is in the 1,2 portal and the arthroscope is in the 3,4 portal. B. Fluoroscopic image obtained during arthroscopic radial styloidectomy for scapholunate instability and secondary degeneration. Note the disruption of the line of Gilula in the proximal carpal row.

POSTOPERATIVE CARE
![]() If the radial styloidectomy is performed concomitantly with another reconstructive procedure (PRC, four-corner arthrodesis, scaphoid bone grafting and fixation), the rehabilitation is dictated by the requirements of that additional procedure.
If the radial styloidectomy is performed concomitantly with another reconstructive procedure (PRC, four-corner arthrodesis, scaphoid bone grafting and fixation), the rehabilitation is dictated by the requirements of that additional procedure.
![]() After either open or arthroscopic radial styloidectomy, the postoperative dressing and sutures are removed in 7 to 10 days. Early active, active-assisted, and passive motion is initiated under the guidance of a hand therapist. Usually a removable splint is used initially for patient comfort. As the patient’s symptoms permit, graded strengthening and unrestricted activities are allowed.
After either open or arthroscopic radial styloidectomy, the postoperative dressing and sutures are removed in 7 to 10 days. Early active, active-assisted, and passive motion is initiated under the guidance of a hand therapist. Usually a removable splint is used initially for patient comfort. As the patient’s symptoms permit, graded strengthening and unrestricted activities are allowed.
OUTCOMES
![]() Stubbins and Barnard1 first described a radial styloidectomy as part of an operative treatment strategy for scaphoid nonunion in 14 patients in 1948. They thought that the styloidectomy removed impingement, enhanced exposure of the scaphoid, and provided material for bone grafting from the same operative field. Since that time there have been no series of outcomes in the indexed English literature for outcomes after isolated open radial styloidectomy. Several reports of radial styloidectomy performed with open reduction and internal fixation of scaphoid nonunion or with triscaphe fusion have demonstrated good pain relief but no significant improvement in range of motion.12,16
Stubbins and Barnard1 first described a radial styloidectomy as part of an operative treatment strategy for scaphoid nonunion in 14 patients in 1948. They thought that the styloidectomy removed impingement, enhanced exposure of the scaphoid, and provided material for bone grafting from the same operative field. Since that time there have been no series of outcomes in the indexed English literature for outcomes after isolated open radial styloidectomy. Several reports of radial styloidectomy performed with open reduction and internal fixation of scaphoid nonunion or with triscaphe fusion have demonstrated good pain relief but no significant improvement in range of motion.12,16
![]() Page et al11 presented their experience with the arthroscopic technique in 22 patients to the European Federation of National Associations of Orthopaedics and Traumatology in 2003. In short-term follow-up, they reported 75% good and satisfactory results.
Page et al11 presented their experience with the arthroscopic technique in 22 patients to the European Federation of National Associations of Orthopaedics and Traumatology in 2003. In short-term follow-up, they reported 75% good and satisfactory results.
![]() Radial styloidectomy is most often performed as a limited procedure to address posttraumatic arthritis of the wrist early in its pathogenesis. While it can provide long-lasting symptomatic relief, it cannot be expected to halt the progression of the arthritis. A successful radial styloidectomy could be one in which a more extensive reconstructive procedure was delayed by several years.
Radial styloidectomy is most often performed as a limited procedure to address posttraumatic arthritis of the wrist early in its pathogenesis. While it can provide long-lasting symptomatic relief, it cannot be expected to halt the progression of the arthritis. A successful radial styloidectomy could be one in which a more extensive reconstructive procedure was delayed by several years.
COMPLICATIONS
![]() Incomplete resection leading to persistent pain
Incomplete resection leading to persistent pain
![]() Excessive resection leading to extrinsic ligament incompetence and wrist instability with ulnar translation
Excessive resection leading to extrinsic ligament incompetence and wrist instability with ulnar translation
![]() Nerve injury to the terminal branches of the radial sensory nerve or lateral antebrachial cutaneous nerve
Nerve injury to the terminal branches of the radial sensory nerve or lateral antebrachial cutaneous nerve
![]() Arthrofibrosis
Arthrofibrosis
![]() Infection
Infection
![]() Complex regional pain syndrome
Complex regional pain syndrome
REFERENCES
1. Barnard L, Stubbins SG. Styloidectomy of the radius in the surgical treatment of non-union of the carpal navicular: a preliminary report. J Bone Joint Surg Am 1948;30A:98–102.
2. Beldner S, Zlotolow DA, Melone CP, et al. Anatomy of the lateral antebrachial cutaneous and superficial radial nerve in the forearm: a cadaver and clinical study. J Hand Surg Am 2005;30A: 1226–1230.
3. Berger RA, Landsmeer JMF. The palmar radiocarpal ligaments: a study of adult and fetal human wrist joints. J Hand Surg Am 1990;15A:847–854.
4. Berger RA. The ligaments of the wrist: a current overview of anatomy with considerations of their potential functions. Hand Clin 1997;13:63–82.
5. Blankenhorn BD, Pfaeffle HJ, Tang P, et al. Carpal kinematics after proximal row carpectomy. J Hand Surg Am 2007;32A:37–46.
6. Blevens AD, Light TR, Jablonsky WS, et al. Radiocarpal articular contact characteristics with scaphoid instability. J Hand Surg Am 1989;14A:781–790.
7. Burgess RC. The effect of rotatory subluxation of the scaphoid on radio-scaphoid contact. J Hand Surg Am 1987;12A:771–774.
8. Inoue G, Sakuma M. The natural history of scaphoid non-union: radiologic and clinical analysis in 102 cases. Arch Orthop Trauma Surg 1996;115:1–4.
9. Kalainov DM, Cohen MS, Sweet S. Radial styloidectomy. In: Geissler WB, ed. Wrist Arthroscopy. New York: Springer-Verlag, 2005: 134–138.
10. Nakamura T, Cooney WP, Lui W, et al. Radial styloidectomy: a biomechanical study on the stability of the wrist. J Hand Surg Am 2001;26A:85–93.
11. Page RS, Waseem M, Stanley JK. Clinical outcome of arthroscopic radial styloidectomy. J Bone Joint Surg Br 2004;86B:280.
12. Rogers WD, Watson HK. Radial styloid impingement after triscaphe fusion. J Hand Surg Am 1989;14A:297–301.
13. Siegel DB, Gelberman RH. Radial styloidectomy: an anatomical study with special reference to radiocarpal intracapsular ligamentous morphology. J Hand Surg Am 1991;16A:40–44.
14. Viegas SF, Patterson RM, Ward, K. Extrinsic wrist ligaments in the pathomechanics of ulnar translation instability. J Hand Surg Am 1995;20A:312–318.
15. Viegas SF, Yamaguchi S, Boyd NL, et al. The dorsal ligaments of the wrist: anatomy, mechanical properties and function. J Hand Surg Am 1999;24A:456–468.
16. Watson HK, Ballet FL. The SLAC wrist: scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984; 9A:358–365.
17. Yao J, Osterman AL. Arthroscopic techniques for wrist arthritis (radial styloidectomy and proximal pole hamate excision). Hand Clin 2005;21:519–526.