Pasquale Giordano1 and Sophia Cashmane1
(1)
Department of Colorectal Surgery, Barts Health NHS Trust, Whipps Cross University Hospital, London, UK
Pasquale Giordano
Email: pasquale.giordano@bartshealth.nhs.uk
Abstract
External pelvic rectal suspension (Express procedure) is a developing operation aimed at restoring the anatomical position of the internal rectal prolapse, while hopefully improving the underlying physiological abnormality. The procedure is carried out transperineally with limited rectal mobilization and, where appropriate, can be combined with surgical correction of a rectocele. The operation consists of “hitching up” the rectum and reinforcement of the rectovaginal wall utilizing a commercially available long-lasting collagen biomaterial (Permacol™; Tissue Science Laboratories plc, Aldershot, UK).
17.1 Introduction
External pelvic rectal suspension (Express procedure) is a developing operation aimed at restoring the anatomical position of the internal rectal prolapse, while hopefully improving the underlying physiological abnormality. The procedure is carried out transperineally with limited rectal mobilization and, where appropriate, can be combined with surgical correction of a rectocele. The operation consists of “hitching up” the rectum and reinforcement of the rectovaginal wall utilizing a commercially available long-lasting collagen biomaterial (Permacol™; Tissue Science Laboratories plc, Aldershot, UK).
17.2 Patient Selection
The procedure is offered to patients with severe rectal evacuatory dysfunction, who have been shown on proctography to have a circumferential, full-thickness intussusception that impedes rectal evacuation. All patients must have tried a course of optimal conservative management and a supervised bowel-retraining program prior to consideration for surgery. An associated rectocele is repaired only if it is greater than 2 cm diameter and contained residual barium after evacuation on proctography.
17.3 Surgical Technique
The patient is prepared with a phosphate enema on the day of the operation, to ensure that the rectum is empty before the procedure. The operation is carried under either general or regional anesthesia, with the patient placed in the Lloyd-Davies position on the operating table. A dose of cefuroxime 750 mg and metronidazole 500 mg is administered at induction and a urinary catheter is inserted in the bladder. After infiltration in the rectovaginal plane with a 1 in 300,000 adrenaline saline solution, a crescent skin incision is made in the perineum midway between the vagina and the anus. The dissection starts in a plane just anterior to the external anal sphincter and extends cranially to enter the rectovaginal plane, taking care not to injure the sphincter complex, the rectum, or the vagina. A Lone Star anal retractor applied to the edges of the wound facilitates the dissection. Meticulous hemostasis is performed, since bleeding from the vaginal venous plexus is common. Once the rectovaginal plane is entered the dissection is extended up to the posterior vaginal fornix to the level of Denonvillier’s fascia. The posterior wall of the vagina is retracted anteriorly and the medial borders of the levator ani muscle exposed. The anterior rectal wall is gently dissected from the puborectalis muscle on both sides to achieve mobilization of the rectum as laterally as possible. Lateral retraction of the puborectalis muscle may help the lateral rectal dissection. This dissection allows access to approximately 12–15 cm of the anterolateral aspect of the distal rectum. In the male patient, a similar dissection is performed extending behind the prostate. Close dissection to the rectal wall is of paramount importance especially at the inferolateral aspect of the prostate to minimize hazard to the pelvic nerves.
Once the perineal dissection is completed, two skin incisions of 2 cm diameter are made just medial and above the level of the pubic tubercle, one on each side. Two 0 polydioxanone sutures (PDS™; Ethicon, Edinburgh, UK) on a J needle are inserted into the periosteum and tendinous insertions overlying the pubis on both sides. These sutures are left long with their needles intact and clipped. The incisions are deepened to gain access to the retropubic space. A purposedesigned tunneller is inserted via the perineal wound lateral to the vagina, upwards anterior to the bladder through the retropubic space of Retzius and behind the pubic bone to emerge through the suprapubic wound (Fig. 17.1a). The plane is delineated by blunt dissection as far as possible from above and below so as to guide the tip of the tunneller as it is advanced upwards so as to prevent injury to the bladder and the vagina.
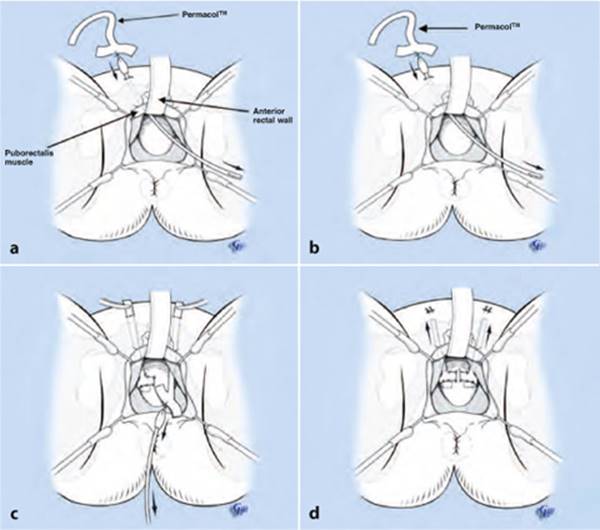
Fig. 17.1
Express procedure for intussusception. a A purpose-designed tunneller is inserted via the perineal wound (lateral to the vagina) upwards behind the pubic bone to emerge through the suprapubic wound taking great care to prevent injury to the bladder. b The sharp point of the tunneller is replaced by a plastic olive, which has attached to it a T-shaped strip of Permacol™. c The Permacol™ strip is drawn down to the perineal wound and positioned so the transverse part of the strip lies on the anterolateral wall of the rectum at approximately 8 cm above the superior border of the sphincter complex. The second strip is similarly placed on the opposite side. d After gentle upward traction on the Permacol™ strips, they are sutured to the periosteum of the pubic bone. (Reproduced from [1], with permission)
The sharp point of the tunneller is replaced by a plastic olive which has attached to it a T-shaped strip of Permacol™ (Fig. 17.1b). This strip is then drawn down to the perineal wound and its transverse part, measuring 2 cm in width, is sutured to the anterolateral rectal wall with two 0 PDS™ sutures with its lower edge at approximately 6–8 cm above the superior border of the sphincter complex (Fig. 17.1c). The vertical part of the strip is left emerging from the suprapubic wound with an artery forceps attached. This maneuver is repeated on the opposite side. Once in place, vertical traction is exerted on the strips via the suprapubic wounds. Once firm but not excessive traction of the rectal wall is achieved, the proximal parts of the T-shaped strips of Permacol™ are sutured to the periosteum of the pubic bone with the two interrupted 0 PDS™ sutures previously placed (Fig. 17.1d). If a rectocele is also present, it can be repaired at the same time using a patch of Permacol™. The patch is shaped 5 ± 5 cm in size with two extensions on the lateral sides. The patch is sutured over the anterior rectal wall with interrupted 2.0 PDS™ sutures (Fig. 17.2). The lateral wings are routed behind the puborectalis and sutured to the periosteum overlying the medial aspect of the ischium in line with the rectocele on either side with two sutures of 0 PDS™ on a J needle. This is performed from within the perineal wound, the rationale being to reinforce the rectovagianal septum and at the same time limit the anterior protrusion and ballooning effect of the anterior rectal wall causing the rectocele.
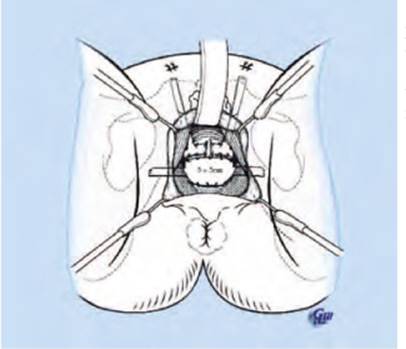
Fig. 17.2
Concomitant rectocele repair. A patch of Permacol™ is sutured over the defect in the rectovaginal septum and the wings are sutured to the ischial tuberosities. (Reproduced from [1], with permission)
17.4 Results
Our initial experience with this procedure included 17 patients [1]. Thirteen patients (all female) had a concomitant rectocoele repair. Clinical details are summarized in Table 17.1. The median follow-up period was 12 months (range 6–20 months).
Table 17.1
Demographics and symptoms for patients with rectal intussusception (n = 17)
|
Patient characteristics and symptoms |
|
|
Age (years) |
47 (20–67) |
|
Gender (M:F) |
4:13 |
|
Symptom duration (months) |
36 (5–400) |
|
Previous pelvic surgery (n) |
9 (2 gracilis neosphincter, 4 colposuspension, 3 hysterectomy) |
|
Parity |
3 (0–5) |
|
Symptom: |
|
|
Obstructed defecation |
16 |
|
Straining |
13 |
|
Anorectal pain |
8 |
|
Prolapse |
7 |
|
Bleeding per rectum |
7 |
|
Toilet revisiting |
7 |
|
Mucus per rectum |
6 |
|
Fecal incontinence |
5 |
|
Urinary incontinence |
5 |
For age, parity, and symptom duration values represent median (range). The frequency of each symptom is represented by the number of patients (of 17) reporting that symptom
There were no major intraoperative complications. One patient, in whom the anterior rectal wall was injured and repaired at the time of the operation, subsequently developed sepsis in the rectovaginal plane, which required drainage and a defunctioning stoma. Two further patients developed local sepsis, one requiring surgical drainage. Despite the sepsis, none of the patients required removal of the Permacol™. Postoperative complications also included neuralgic pain (n = 3), which resolved in all cases during follow-up. No patient reported any changes in sexual function, and in particular none of the women reported dyspareunia.
When reviewed at 6 months, all patients reported a significant improvement in symptoms related to prolapse and evacuatory function. Incontinence did not deteriorate in any of the patients. Quality of life also significantly improved. Anorectal physiology demonstrated a significant reduction in maximum tolerable volume and pelvic floor descent. All other measurements remained unchanged. Fourteen patients underwent postoperative proctographic evaluation. In ten of these patients the intussusception appeared improved by surgery. Furthermore, 11 of the 14 patients who underwent postoperative proctography had undergone a rectocele repair. Eight of these had no evidence of rectocele on postoperative proctography. In the remaining three patients who all presented with very large rectocoeles (8 cm, 8 cm, and 6.5 cm), the size of the rectocele was markedly reduced postoperatively (3 cm, 2.5 cm, and 2.5 cm, respectively).
The postoperative functional outcome did not significantly differ in patients, with or without postoperative radiological improvement.
17.5 Discussion
Patients with rectal evacuatory dysfunction may present with a variety of symptoms, often nonspecific and with very variable impact on quality of life. In these patients defecography is used to demonstrate possible morphological abnormality. However similar morphological abnormalities can also be identified in normal subjects [2], and therefore cannot be used on their own as an indication for surgery. Furthermore, as confirmed in our experience, improvement of symptoms following surgical intervention does not necessarily correlate with improved anatomical appearance on postoperative evacuatory proctography. Nevertheless, it is our belief that in patients without pelvic floor dyssynergia in whom severe symptoms have failed to respond to optimal conservative treatments, gross anatomical abnormalities revealed on evacuatory proctography may contribute to their symptoms. Notwithstanding these limitations, the basis of this new technique was to correct the anatomical abnormalities in a way that is less invasive and more effective than traditional approaches.
Rectal intussusception is normally initiated by an anterior take-off point at approximately 6–8 cm from the anorectal junction [3, 4]. Our aim was to fix this area to prevent the process of intussusception. To reach this area via an abdominal approach, rectal mobilization to the pelvic floor is necessary. Such mobilization carries potential hazard to the pelvic autonomic nerves and may contribute to postoperative constipation [5]. Furthermore, incomplete rectal mobilization during abdominal rectopexy may result in inadequate fixation and lead to unsatisfactory results. The Express procedure through the perineal approach allows relatively easy access to the crucial area of the take-off point without violation of the peritoneal cavity and hopefully with less hazard to the pelvic nerves. In our experience it is not associated with worsening incontinence. The insertion of strips of Permacol™ to the anterior rectal wall to prevent the initial take-off of the rectal wall also provides structural support to the entire pelvic floor, as confirmed by a significant reduction in pelvic floor descent. Further the Permacol™ patch in the rectovaginal plane, with its lateral attachments to the ischium, buttresses the anterior rectal wall and successfully corrects the associated rectocele as demonstrated on proctographic postoperatively.
Dissection of the rectovaginal plane required with the Express procedure can be challenging and perforation of the vagina or rectum may occur. Despite repair of such defects it was feared that the presence of foreign material would impair healing and result in extrusion, as has been the case with synthetic meshes in rectocele repair (unpublished observations). In the authors’ experience even when local sepsis developed, extrusion or erosion of the implants never occurred and the Permacol™ never had to be removed [1, 6].
References
1.
Williams NS, Dvorkin LS, Giordano P et al (2005) EXternal Pelvic REctal SuSpension (Express procedure) for rectal intussusception, with and without rectocele repair. Br J Surg 92:598–604PubMedCrossRef
2.
Pomerri F, Zuliani M, Mazza C et al (2001) Defecographic measurements of rectal intussusception and prolapse in patients and in asymptomatic subjects. Am J Roentgenol 176:641–645CrossRef
3.
Brodén B, Snellman B (1968) Procidentia of the rectum studied with cineradiography. A contribution to the discussion of causative mechanism. Dis Colon Rectum 11:330–347PubMedCrossRef
4.
Ihre T (1990) Intussusception of the rectum and the solitary ulcer syndrome. Ann Med 22:419–423PubMedCrossRef
5.
Huber FT, Stein H, Siewert JR (1995) Functional results after treatment of rectal prolapse with rectopexy and sigmoid resection. World J Surg 19:138–143PubMedCrossRef
6.
Williams NS, Giordano P, Dvorkin LS et al (2005) External Pelvic Rectal Suspension (The Express Procedure) for Full-Thickness Rectal Prolapse: Evolution of a New Technique. Dis Colon Rectum 48:307–316PubMedCrossRef