PART VIII
HAND
CHAPTER 85 DUPUYTREN'S DISEASE
CATHERINE M. CURTIN
Dupuytren’s disease is common and surgical treatment can be very satisfying as the surgeon is able to restore function through elegant dissection of complex anatomy. There has been a recent shift in the treatment algorithm toward less invasive treatments. Despite these changes, the surgeon should determine the treatment as the anatomy remains complex and even nonsurgical interventions require a thorough understanding of the hand’s structures. In many instances, medical approaches fail and surgical intervention is required.
EPIDEMIOLOGY
Dupuytren’s disease is a genetic disorder, which is thought to be autosomal dominant with variable penetrance.1 Most patients are older men of European descent, and generally the disease presents in the sixth decade with a male to female ratio of approximately 3 to 1.2 The disease course and response to treatment in patients who do not fit the usual clinical picture can be very challenging. For example, patients with an earlier presentation often have a more aggressive course with high recurrence rates after surgery.3 Women generally have later onset and milder disease. However, women who require surgical intervention often have a higher incidence of postoperative pain complications.4 Beyond genetics, diabetes has been associated with the development of Dupuytren’s disease.5 Diabetic patients are another challenging subgroup because of higher rates of complications after surgery, including hematoma, delayed healing, infection, and skin sloughing.6 Understanding the average patient and those at increased risks for complications will help the surgeon counsel patients on the most appropriate treatment plan.
BASIC SCIENCE
Dupuytren’s disease is a pathologic fibroproliferative process. Although a thorough understanding of the pathologic pathways remains elusive, recent work provides insights into this disorder.7 For example, the β-catenin pathway is altered in Dupuytren’s disease and β-catenin is part of normal wound healing process.8 Also key fibroblast gene expression in people with Dupuytren’s disease is altered. Genes encoding components of the extracellular matrix are downregulated.9 These studies are the first step to the development of targeted molecular interventions.
ANATOMY
Dupuytren’s disease results from deformation of normal anatomic structures (Figure 85.1). The normal anatomy is referred to as a band, whereas diseased tissue is a cord. The surgeon who treats Dupuytren’s contractures must have a thorough knowledge of the normal anatomy to release the deforming cords. In the hand with Dupuytren’s contractures, findings can range from mild skin thickening to severe flexion contractures of all of the finger joints.
Several key anatomic points are emphasized. First, the structure of the proximal interphalangeal joint (PIPJ) and metacarpophalangeal joint (MPJ) impacts treatment outcomes. Metacarpophalangeal (MP) ligaments have a “cam” orientation, which means the center of rotation is eccentric relative to the ligament so that the collateral ligaments are stretched when the joint is flexed. Thus after release of the contracting cords, the collateral ligaments do not tether the joint and MPJs easily return to extension. The PIPJ is designed slightly differently. When the PIPJ is flexed the collateral ligaments and volar plate shorten and thus after Dupuytren’s release the joint may still have an intrinsic flexion contracture. Furthermore, if the proximal interphalangeals (PIPs) have been flexed for years, attempts to fully extend the joint may stretch the neurovascular structures, resulting in further damage to the finger or even loss of the digit.
A second important anatomic consideration is the relationship of the cords with the neurovascular bundles. The “spiral cord” is a continuation of the pretendinous band that merges the spiral band and the lateral digital sheet. As this cord contracts, it pulls the neurovascular bundle medial and superficial putting it at risk for injury (Figure 85.2). The surgeon who operates on a patient with Dupuytren’s disease must take care to identify and protect the neurovascular bundles.
INITIAL CONSULTATION
The initial presentation is often the beginning of a long relationship between the Dupuytren’s patient and his or her surgeon. The first step is to understand the patient’s functional status, their complaints, and goals. This will allow the surgeon to tailor the best treatment for each patient. In the history, complaints such as inability to lay a hand flat on a table should be documented as functional limitations are often used in the decision to authorize interventions.
Physical exam should include careful documentation of the degree of contracture of each finger. In addition, noting the quality of the overlying skin is crucial to help plan intervention and predict the likelihood of leaving the wound open or needing a skin graft. Finally, hand exam should also assess for concomitant issues such as carpal tunnel syndrome. In the initial consultation it is imperative that the patient understands that the disease is part of their genetic makeup and you can only treat the symptoms and that recurrence/progression is expected.

FIGURE 85.1. Anatomy of the palmar and digital fascia. A thorough knowledge of the anatomy of the palmar and digital fascia in the normal palm and finger is essential for an understanding of the patterns of anatomic distortion in the hand with Dupuytren’s contracture.

FIGURE 85.2. Spiral cord displacement of digital nerve. Note how the neurovascular bundle has been pushed medially by a spiral cord. The clamp is pulling on the cord, which is pushing the neurovascular bundle.
TREATMENT
No Finger Contracture/No Pain
Many patients present with a mass in the hand, skin pits, or for a feeling of “tightness” in the fingers but have no contractures. For these patients, the treatment consists of an explanation of the disease, reassurance, and clear instructions on when to consider intervention. Intervention is generally not considered until the MPJ has contracture of at least 30° or there is any contracture of the PIPJ.
Painful Palmar Nodules
Some patients with early active Dupuytren’s disease will complain of painful nodules in their palms. The conventional wisdom has been not to excise these because of the theoretical risk of flare of the disease. There is some evidence that injecting these nodules with steroids can provide some symptomatic relief and potentially soften and flatten the nodules.10
Dorsal Dupuytren’s Disease
“Knuckle pads” are generally seen in patients with a strong Dupuytren’s diathesis. These fibromatous masses on the dorsum of the PIPJs can be quite bothersome to patients but generally do not cause tethering to the extensor apparatus. The nodules can be monitored or excised depending upon the patient’s preference.
Contracted Fingers
Treatment for Dupuytren’s contractures has been evolving over the last few years. Many more options are available to the surgeon, which allows the ability to refine the approach to each cord, each hand, and each patient. The following outlines the available interventions:
1. Needle aponeurotomy (NA): This less invasive treatment for Dupuytren’s disease has been popularized in France and is gaining acceptance internationally. The premise is that the cord is weakened by percutaneous needle insertions into the cord after which the finger is manipulated to rupture the cord. Foucher reviewed 211 patients who had 261 hands treated with NA. Their study included 311 MPJs and PIPJs. The mean preoperative contracture was 65° and the mean postoperative contracture was 15°. NA was more effective for MPJs when compared with PIPJ contractures. The major complications included neuropraxia of digital nerves with one digital nerve requiring repair.11 Recurrence rate is difficult to define in Dupuytren’s research because there can be progression of old disease as well as the development of new disease. For NA, there was increased Dupuytren’s disease (both progression and new disease) in 69% of the patients at 3 years.11 Theoretically, one would expect a higher recurrence rate after these procedures given that no diseased tissue is removed, but at this time large trials assessing the recurrence after NA are lacking (Figure 85.3).
Technique: Dr. Eaton12 has published a thorough review of the technique. The following is a technique summary. The skin is prepped with an alcohol swab and a small weal of lidocaine is placed over the cord to be treated. The lidocaine is localized in the subcutaneous tissue just above the cord. This prevents the digital nerve from being anesthetized, which allow a patient to alert the surgeon about parasthesias indicating that the needle is close to the nerve. The targeted cord is then prepped. A 25G needle is used to perforate the volar aspect of the cord in multiple areas of the cord along an area of approximately 5 mm2. (This perforating technique is more an up and down maneuver less sawing). The needle never passes more than bevel deep. Depending on the complexity of the cord, it may require perforation at several points along its longitudinal axis to achieve full release. The shallow penetration of the needle minimizes the risk of nerve injury. After the cord has been perforated, manipulation is performed. This MPJ is stabilized and the contracted finger is smoothly but forcefully extended. A crack is heard when the cord ruptures. After release, the contracted finger is re-palpated with applied traction to feel for any residual cords that require additional NA.
Pros: This is a minimally invasive technique that can be performed under local anesthesia in a clinical setting. It is effective especially for MP cords. There are no incisions.

FIGURE 85.3. Needle aponeurotomy—A 25G needle perforating the cord.
Cons: It is a blind approach (nerve injury about 1%). The disease is not removed, which may translate into a high recurrence rate.
Pearls: Digital nerve sensation is monitored and the patients are instructed to alert the surgeon if they experience any “electric shocks” during the procedure. Patients are counseled that skin tears can occur. It is recommended that the surgeon start with a simple well-formed MP cord to get the feeling of the interface of the cord and the needle.
2. Collagenase: Collagenase is a recently approved medical treatment for Dupuytren’s disease.13 This technique uses collagenase enzyme from Clostridium histolyticum to soften the cord and allow for rupture with manipulation. In the clinic, 203 primary cords were treated with collagenase and 64% reached the primary end point of a residual contracture of less than 5°. Like NA, collagenase is more effective for MPJ contractures: 77% MPJs had less than 5° residual contracture versus PIPJ contractures in which only 40% made that end point. The majority of patients had local side effects related to the injection, including bruising and swelling. In this study of 308 patients, there were two flexor tendon ruptures after the treatment of small finger PIPJ contractures, both necessitating surgery.
Technique: The patient is counseled that the hand will be swollen and bruised the day after the injection (Figure 85.4). The medication is reconstituted according to the package insert. Three small aliquots of the medication are injected into the substance of the cord according to the training module (https://www.xiaflex.com/hcp/REMS_statement.jsp) (Figure 85.5). Care is taken to avoid injection into the structures deep to the cord and special precautions are taken when injecting PIPJ cord. In general, if faced with a small finger PIPJ contracture the surgeon should be cautious and select only those with a clearly palpable and discrete cord. The patient returns and the finger is manipulated to rupture the cord. The timing of manipulation is 24 hours after injection per the packet insert. However, we are finding nice results with manipulation 1 week after injection. A lidocaine block is given before the manipulation, which seems to produce better results. Skin tears are not infrequent and patients are counseled accordingly. The patient is splinted at night for 3 months.
Pros: Minimally invasive and effective for the release of straightforward Dupuytren’s cords. Potentially lower recurrence rates than NA because of the chemical denaturing of the collagen cords.
Cons: Only one cord can be treated at each setting. Requires the patient to have two visits. The medication is costly.

FIGURE 85.4. Bruising of a hand after receiving a collagenase injection.

FIGURE 85.5. Recommended technique for injecting collagenase into cord (no deeper).
Pearls: Make sure the patients understand that their hand will be bruised and swollen. If the patient has no reaction, the medication may not be effective. Plan to use local anesthesia for the manipulation.
3. Limited fasciectomy: Surgical excision of the disease is still the standard for the treatment of Dupuytren’s disease. The amount of surgery can also be tailored to each individual patient based on his or her disease, health state, and ultimate functional demands. Limited fasciectomy is the most common approach with removal of a section of the cord. The amount of cord removed can be individualized to each patient, but the prevailing wisdom is that the more the diseased tissue removed the lower the recurrence rate. The surgeon balances the desire for the most extensive removal of the disease with the need to limit risks to the patient. The magnitude of limited fasciectomy varies tremendously. For example, a first web space cord that is adducting the thumb can be excised quickly under local anesthesia. On the opposite extreme, a limited fasciectomy can include the removal of multiple cords across multiple fingers requiring a full 2-hour tourniquet time and intense postoperative hand therapy to maximize functional return. Postoperative care depends on the degree of the surgical excision. For most cases, the hand is splinted until suture removal and then nighttime splinting is prescribed.
Dias performed a survey of over a thousand patients who had surgical treatment of Dupuytren’s contracture with an average follow-up of 27 months. Fifteen percent of participants had recurrence or persistence of deformity and recurrence was higher in patients with more severe preoperative disease. Forty-six percent of patients reported at least one complication from surgical site infection to persistent numbness. Complications were more common in patients with more severe disease.14
Pros: Surgery removes the disease, which limits recurrence and provides the most durable outcomes.
Cons: There are surgical risks (nerve injury, wound healing delay, etc.). Extensive surgical release can result in limited flexion. The rehabilitative process requires several weeks.
Pearls: Incisions are carefully planned to allow for final skin rearrangement and limit eventual scar contraction across the joint. The most common skin incisions are a Brunners-type incision or a straight line over the cord that is supplemented with Z-plasties at the flexion crease after the disease has been removed (Figure 85.6).
4. Dermatofasciectomy/skin graft: Some patients require a more aggressive surgical approach, such as those with severe disease of PIP with extensive skin involvement, revisional surgery, or for young patients with a very strong diathesis. In this technique, the disease as well as the overlying skin is excised and a full-thickness skin graft is used to resurface the defect. The theory is that the skin graft will act as a barrier and prevent recurrence of the disease.15 However, recent studies suggest that recurrence is not prevented by skin graft.16 Skin grafting remains a useful tool for resurfacing areas that are scarred or with extensive disease involvement.
Pros: There is complete excision of the diseased tissue to resurface scarred and fibrotic skin.
Cons: Long rehabilitation and potential loss of skin graft.
Pearls: Do not skimp on the skin graft. If you choose these techniques then fully resurface the involved area. Use a bolster, as there is risk of graft loss in this mobile area (Figure 85.7).
5. Soft tissue distraction: Distraction of the soft tissue is not a new technique for the treatment of severe PIPJ contractures. Distraction is attractive because it will stretch the shortened soft tissue, such as neurovascular bundles and collateral ligaments. Distraction devices, such as the digit widget, use skeletally anchored hardware to provide soft tissue distraction of the PIPJ. These devices allow the surgeon to pre-distract the soft tissue fully straightening the finger. Afterward, a limited fasciectomy or dermatofasciectomy can be performed. The device is easily placed with a digital block and we have found that most patients reach full extension at about 5 weeks. We then remove the device and excise the Dupuytren’s disease at a second procedure. The advantage of this staging is that the removal of this disease is facilitated now that the finger is not severely contracted. At the end of the distraction, the finger is straight but the disease must still be removed because without fasciectomy the contracture will quickly reoccur17 (Figure 85.8).
Pros: This technique allows for gentle stretching of the contracted soft tissue of the severely contracted PIPJ.
Cons: This is a two-stage procedure and the patient must tolerate the device for several weeks. There is a risk of hardware complications such as infection.
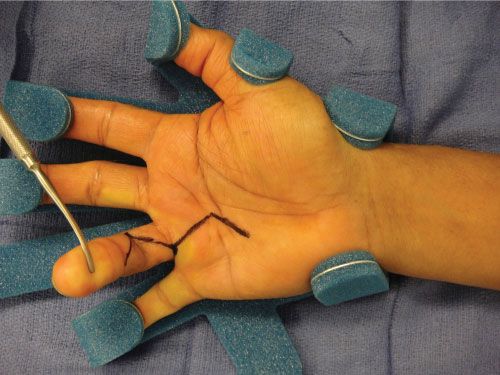
FIGURE 85.6. Incision design—Bruener incisions are a common technique. If straight line incisions are used, z-plasties are added when closure is performed.

FIGURE 85.7. Full-thickness skin graft to resurface the proximal segment of the finger.
Pearls: It is important to make sure that there is enough space between the device and the skin to prevent rubbing, as the finger swells postoperatively. Partnering with hand therapists to follow the patients will help ensure a smooth postoperative course.
CLINICAL DILEMMAS
1. Pale finger at the end of the case—After release of a severely contracted digit, occasionally the finger will remain pale after the tourniquet is released. This is usually related to vasospasm and the finger will soon “pink up.” If the finger remains white then any bandages are released, the finger is flexed and irrigated with warm saline. The finger is observed for several minutes.18 If the finger remains white, the vessels are explored for injury. If no injury is identified, vasodilators may be employed (sometimes 20 minutes can pass before the finger will have return of circulation). If injury is noted, a microvascular repair is performed.

FIGURE 85.8. Soft tissue distractor applied to a finger.
2. Dupuytren’s disease is excised but full extension of the PIPJ is lacking—This is a common situation and the surgeon must decide whether to proceed with release of the joint. First, it is paramount that the patient understands before surgery that there is always a possibility that full release on a severely contracted PIPJ may not be possible. Intraoperatively, the surgeon must balance the risks of traumatizing the PIPJ versus accepting less than complete release of PIPJ. On the one hand, the residual contracture is known to predispose the patient to recurrence of the original contracture.19 On the other hand, manipulation of the joint will induce swelling and put the patient at risk for increased stiffness. Though release of the joint remains controversial, it appears that cautious release of the checkrein and accessory ligaments may improve the final results without excess risk.20
3. The patient has both Dupuytren’s contracture and carpal tunnel syndrome—There has been concern that simultaneous carpal tunnel release and palmar fasciectomy puts patients at increased risk for a postoperative pain reaction. Lilly and Stern21 reviewed 70 patients who had both procedures performed at the same setting and found no increase in the rates of complications when compared with controls who had either fasciectomy or carpal tunnel.
OUTCOMES
The outcomes after the treatment of Dupuytren’s are variable depending on the severity of disease, treatment type, and joint affected. A few facts are absolute. First, MPJ contractures respond better than PIPJ contractures for all types of treatment. Second, the more severe the preopative disease the higher the risk of complications, incomplete release, and recurrent disease. Finally, no treatment changes the presence of the disease and recurrence/progression is expected.
Release of the contracted fingers does improve function and lessen disability. Patients do appreciate the ability to shake hands and put hands in their pockets. Engstrand et al.22 evaluated 60 patients who had surgical correction for Dupuytren’s disease and their median disability score on the Disability Arm Shoulder and Hand instrument improved after surgery.
With the advent of new techniques, a comparison of these techniques would be extremely helpful. Unfortunately, at this time well-done comparative studies between treatment types are lacking.
FUTURE DIRECTIONS
The new directions for the treatment of Dupuytren’s disease are focused on prevention of contractures. Radiation is being investigated for prevention of Dupuytren’s disease progression. Betz followed 208 hands that had been treated with radiotherapy. At 13-year median follow-up 69% had no progression of their disease with no major long-term side effects.23
References
1. Hu FZ, Nystrom A, Ahmed A, et al. Mapping of an autosomal dominant gene for Dupuytren’s contracture to chromosome 16q in a Swedish family. Clin Genet. 2005 November;68(5):424-429.
2. Geoghegan JM, Forbes J, Clark DI, Smith C, Hubbard R. Dupuytren’s disease risk factors. J Hand Surg Br. 2004 October;29(5):423-426.
3. Hueston JT. Unsatisfactory results in Dupuytren’s contracture. Philosophies of Dr. J. T. Hueston. Hand Clin. 1991 November;7(4):759-763.
4. Sennwald GR. Fasciectomy for treatment of Dupuytren’s disease and early complications. J Hand Surg Am. 1990 September;15(5):755-761.
5. Burke FD, Proud G, Lawson IJ, et al. An assessment of the effects of exposure to vibration, smoking, alcohol and diabetes on the prevalence of Dupuytren’s disease in 97,537 miners. J Hand Surg Eur. 2007 August;32(4):400-406.
6. Bayat A, Cunliffe EJ, McGrouther DA. Assessment of clinical severity in Dupuytren’s disease. Br J Hosp Med (Lond). 2007 November;68(11): 604-609.
7. Ojwang JO, Adrianto I, Gray-McGuire C, et al. Genome-wide association scan of Dupuytren’s disease. Hand Surg Am. 2010 December;35(12): 2039-2045.
8. Mosakhani N, Guled M, Lahti L, et al. Unique microRNA profile in Dupuytren’s contracture supports deregulation of β-catenin pathway. Mod Pathol. 2010 November;23(11):1544-1552.
9. Satish L, LaFramboise WA, O’Gorman DB, et al. Identification of differentially expressed genes in fibroblasts derived from patients with Dupuytren’s contracture. BMC Med Genomics. 2008 April 23;1:10.
10. Ketchum LD, Donahue TK. The injection of nodules of Dupuytren’s disease with triamcinolone acetonide. Hand Surg Am. 2000 November;25(6): 1157-1162.
11. Foucher G, Medina J, Navarro R. Percutaneous needle aponeurotomy: complications and results. J Hand Surg Br. 2003 October;28(5):427-431.
12. Eaton C. Percutaneous fasciotomy for Dupuytren’s contracture. J Hand Surg Am. 2011 May;36(5):910-915.
13. Hurst LC, Badalamente MA, Hentz VR, et al. Injectable collagenase clostridium histolyticum for Dupuytren’s contracture. N Engl J Med. 2009 September 3;361(10):968-979.
14. Dias JJ, Braybrooke J. Dupuytren’s contracture: an audit of the outcomes of surgery. J Hand Surg Br. 2006 October;31(5):514-521.
15. Villani F, Choughri H, Pelissier P. Importance of skin graft in preventing recurrence of Dupuytren’s contracture. Chir Main. Dec 2009;28(6): 349-351.
16. Ullah AS, Dias JJ, Bhowal B. Does a ‘firebreak’ full-thickness skin graft prevent recurrence after surgery for Dupuytren’s contracture?: a prospective, randomised trial. J Bone Joint Surg Br. 2009 March;91(3): 374-378.
17. Hodgkinson PD. The use of skeletal traction to correct the flexed PIP joint in Dupuytren’s disease. A pilot study to assess the use of the Pipster. J Hand Surg Br. 1994 August;19(4):534-547.
18. Nancarrow JD. Avoidance of critical ischemia in the surgery of Dupuytren’s disease. J Hand Surg Am. 2002 November;27(6):1109-1110.
19. Misra A, Jain A, Ghazanfar R, Johnston T, Nanchahal J. Predicting the outcome of surgery for the proximal interphalangeal joint in Dupuytren’s disease. J Hand Surg Am. 2007 February;32(2):240-245.
20. Beyermann K, Prommersberger KJ, Jacobs C, Lanz UB. Severe contracture of the proximal interphalangeal joint in Dupuytren’s disease: does capsuloligamentous release improve outcome? J Hand Surg Br. 2004 June;29(3):240-243.
21. Lilly SI, Stern PJ. Simultaneous carpal tunnel release and Dupuytren’s fasciectomy. J Hand Surg Am. 2010 May;35(5):754-759.
22. Engstrand C, Borén L, Liedberg GM. Evaluation of activity limitation and digital extension in Dupuytren’s contracture three months after fasciectomy and hand therapy interventions. J Hand Ther. 2009 January-March;22(1):21-26; quiz 27.
23. Betz N, Ott OJ, Adamietz B, Sauer R, Fietkau R, Keilholz L. Radiotherapy in early-stage Dupuytren’s contracture. Long-term results after 13 years. Strahlenther Onkol. 2010 February;186(2):82-90.