Julie Freischlag and Natalia Glebova
![]() INDICATIONS/CONTRAINDICATIONS
INDICATIONS/CONTRAINDICATIONS
Thoracic outlet syndrome (TOS) is a spectrum of disorders resulting from compression of the neurovascular structures within the thoracic outlet. The three subtypes of TOS are identified based on the structures affected: The brachial plexus which is compressed in the most common subtype, neurogenic TOS; the subclavian vein which may be thrombosed in the second most common subtype, venous TOS; and the subclavian artery which may become stenotic or aneurysmal in arterial TOS. Transaxillary approach to first rib resection and anterior scalenectomy is indicated in all three subtypes of TOS unless the subclavian artery needs to be resected and replaced.
The initial treatment of neurogenic TOS is nonoperative with physical therapy, avoidance of inciting activities, and image-guided neuromuscular blockade of the anterior scalene muscle with lidocaine of Botulinum toxin A (Botox). Ample time is allowed for work with physical therapists, at least several months. If no improvement occurs with physical therapy, if the anterior scalene block is positive (the patient obtains temporary symptomatic relief with local anesthetic injection), and if symptoms are truly significant, then an operation is offered.
Transaxillary first rib resection and scalenectomy is indicated for both venous and arterial TOSs as symptoms will recur without this definitive operation even if thrombus is removed via thrombolysis or thrombectomy. Reoperation for residual symptoms after prior supraclavicular first rib resection is also best performed with a transaxillary approach as this avoids scar tissue from the prior operation.
Another indication for this operation is the symptomatic presence of a cervical rib. Cervical ribs, defined as anomalous ribs originating from the seventh cervical vertebrae, are frequently fused to the first rib and may cause symptomatic arterial compression, thrombosis, aneurysm formation, and embolization. Those patients with symptomatic cervical ribs who do not require vascular reconstruction should undergo transaxillary first rib resection, anterior scalenectomy, and cervical rib resection. Patients with this syndrome who require arterial bypass are best served by a supraclavicular approach that allows arterial reconstruction at the time of rib resection.
A contraindication to the transaxillary approach is first rib resection in patients with arterial TOS in whom replacement of the subclavian artery is planned due to aneurysmal changes. These patients are best served with a supraclavicular approach (with sometimes an infraclavicular counterincision) which allows direct arterial reconstruction. Also, preoperative first rib resection in a patient who has had a transaxillary approach should be done using the supraclavicular technique.
![]() PREOPERATIVE PLANNING
PREOPERATIVE PLANNING
Preoperative planning and evaluation vary depending on the type of TOS with which the patient presents.
Patients with suspected neurogenic TOS often present with vague symptoms of arm pain, weakness, or paresthesias. These nonspecific symptoms may result from many other conditions, and thus it is imperative to determine whether such patient have TOS and may benefit from first rib resection. A reliable approach to confirming the diagnosis is neuromuscular blockade of the anterior scalene muscle. The diagnosis is confirmed if an injection of lidocaine into the anterior scalene under ultrasound or computed tomography (CT) guidance produces relief. Nonoperative management should then be attempted, with physical therapy and careful attention to activities that incite symptoms. Botulinum toxin A may also be injected into the anterior scalene muscle for longer duration of relief. If nonoperative management is unsuccessful, first rib resection and anterior scalenectomy is indicated.
Venous TOS typically presents with arm swelling and subclavian vein thrombosis in the setting of exercise or overuse. Thrombosis may be acute or chronic. This disease entity is also known as effort-induced thrombosis of the subclavian vein or Pagett–Schroetter syndrome. Historically, these patients underwent thrombolysis and percutaneous venoplasty. Recent data indicate that preoperative thrombolysis and percutaneous venoplasty are of no benefit for patients with TOS manifested by subacute or chronic venous thrombosis. Preoperatively, these patients should undergo laboratory evaluation for the presence of hypercoagulable disorders such as Factor V Leiden mutation, protein C or S deficiency, antithrombin III deficiency, prothrombin gene mutations, homocysteinemia, activated protein C (APC) resistance, antiphospholipid antibodies, and lupus anticoagulant. Patients with venous TOS should also be anticoagulated, preferably with therapeutic dosing of Lovenox of 1 mg/kg twice a day, which is continued until the operation.
Arterial TOS is characterized by chronic thrombosis manifesting as arm claudication, or in the acute form by potentially limb-threatening hand and digit ischemia due to thromboembolism from the subclavian artery secondary to compression. These patients often have a bony abnormality such as a cervical rib. Poststenotic dilatation and aneurysm formation may occur in the subclavian artery in the chronic form of the syndrome. Preoperative planning may include urgent thrombolysis or thrombectomy in the presence of clinically significant distal ischemia. Hypercoagulability studies are conducted as for venous TOS. A plain chest radiograph should be obtained to evaluate for the presence of a cervical rib and other bony abnormalities. A duplex ultrasound should also be performed to evaluate for arterial stenosis and dilatation, as well as to measure arterial velocities. An arteriogram may be helpful in delineating thrombosis or aneurysm formation. It is imperative to determine whether the patient requires arterial reconstruction in addition to first rib resection and scalenectomy, as the transaxillary approach should be reserved for patients not undergoing arterial bypass. The supraclavicular approach is best for patients who require replacement of the subclavian artery.
![]() SURGERY
SURGERY
The operation of first rib resection and anterior scalenectomy is performed under general endotracheal anesthesia. Short acting paralytics are used at the start of the operation, so that their effects wear off and do not interfere with nerve identification during the operation.

Figure 12.1 A: Patient positioning with the operative side facing up and the arm circumferentially prepped (photo courtesy of Holly Grunebach, PA-C). B: Operative side arm is secured in the Machleder retractor prior to incision (photo courtesy of Holly Grunebach, PA-C). C:Incision at inferior aspect of hairline between the borders of pectoralis major and latissimus dorsi muscles. D: Arm raised in the Machleder retractor allowing visualization of axillary structures with supplemental lighting.
Positioning
The patient is positioned on a beanbag in the lateral position with the operative side facing up (Fig. 12.1A). The beanbag is inflated, and ample amounts of padding are used to protect pressure points. The lower leg is slightly bent, and the upper leg is straight and padded with pillows. The axilla is prepped in the standard fashion, and the arm on the operative side is prepped circumferentially. Once the patient is draped, a Machleder retractor is placed on the bed, and the operative arm is extensively padded with Kerlix and towels, and then secured with CoBand to the retractor (Fig. 12.1B).
Technique
The operation commences with an incision in the inferior aspect of the hairline between the posterior border of the pectoralis major muscle and the anterior border of the latissimus dorsi muscle (Fig. 12.1C). The subcutaneous space is entered, and electrocautery is used to dissect down to the chest wall. Lymphatics may be encountered, and if so they are tied. Once the chest wall comes into view, blunt dissection is utilized to sweep the remainder of adipose tissue off the chest wall.
A self-retaining retractor is now placed at the skin level, and the arm is elevated by raising the Machleder retractor (Fig. 12.1D). In order to aid in visualization of deep axillary structures, a Deaver retractor is placed on one side of the incision, and a lighted retractor such as a St. Marks retractor on the other side. As the operation proceeds, frequent breaks are taken and the arm is relaxed into a more neutral position while the wound is packed in order to minimize the amount of stretch on the brachial plexus.
At this time, it is imperative to identify the subclavian vein and artery in order to find the first rib. The artery is revealed by its pulsation. The vein may be difficult to find in patients with venous TOS as it may be quite fibrotic. Nonetheless, the vein is anterior to the artery. Blunt dissection is used to sweep away tissues around these structures in order to identify them and the anterior scalene muscle that lies between them and attaches inferiorly to the first rib. This is done carefully so as not to avulse any small arterial branches. These branches are tied when encountered. The brachial plexus is visible posteriorly to the subclavian artery, and does not need to be dissected (Figs. 12.2A,B).
Once these structures are identified, dissection of the first rib begins. A sharp periosteal elevator is used to clear intercostal muscles off the inferior aspect of the first rib. One is careful to push precisely along the rib edge so as not to enter the pleural space or injure intercostal vessels. Once the inferior edge of the first rib is freed of intercostal muscle attachments both anteriorly and posteriorly, a small blunt periosteal elevator is used underneath the first rib to push pleura off the rib inferiorly. One is careful not to enter the pleural space at this point. The first rib is mobilized from the subclavian vein anteriorly to the brachial plexus posteriorly.
Next, the subclavius muscle located at the anterior aspect of the first rib next to the subclavian vein is sharply divided. Care is taken to divide the muscle right on top of the rib edge, without injuring the vein. The anterior scalene muscle between the artery and the vein is then divided sharply. A right angle clamp is used to lift muscle fibers up and away from the subclavian artery, and the muscle is divided with scissors leaving as much muscle as possible on the first rib (Fig. 12.2C). This is done in stages, by lifting subsequent portions of the anterior scalene muscle, so that one does not cut the artery.
A right angle clamp is then placed underneath the first rib to check the extent of mobilization. The middle scalene muscle may at this time be pushed away from the first rib if necessary. This is done with a periosteal elevator hugging the rib so as not to injure the long thoracic nerve. With the first rib sufficiently mobilized, a bone cutter is placed anteriorly, and the first rib divided next to the subclavian vein. The first rib is then divided posteriorly, with great care taken not to injure the brachial plexus. Due to the extensive mobilization described above, one can pull the rib inferiorly to visualize the nerve root. The rib is divided anterior to the plexus and removed from the field (Fig. 12.2D).
A rongeur is then used to remove any remaining bony edges until they are smooth and appear to be away from the neurovascular structures. The field is then inspected for hemostasis and pleural tears. Next, the axillary space is filled with saline, and the patient is given several positive pressure breaths to evaluate for a pneumothorax manifested as air bubbles in the saline. If a pneumothorax is present, a 12-French chest tube is placed in the second intercostal space through a separate incision. The wound is then closed in layers and a sterile dressing is applied. The chest tube is connected to a Pleuravac at –20 cm water.
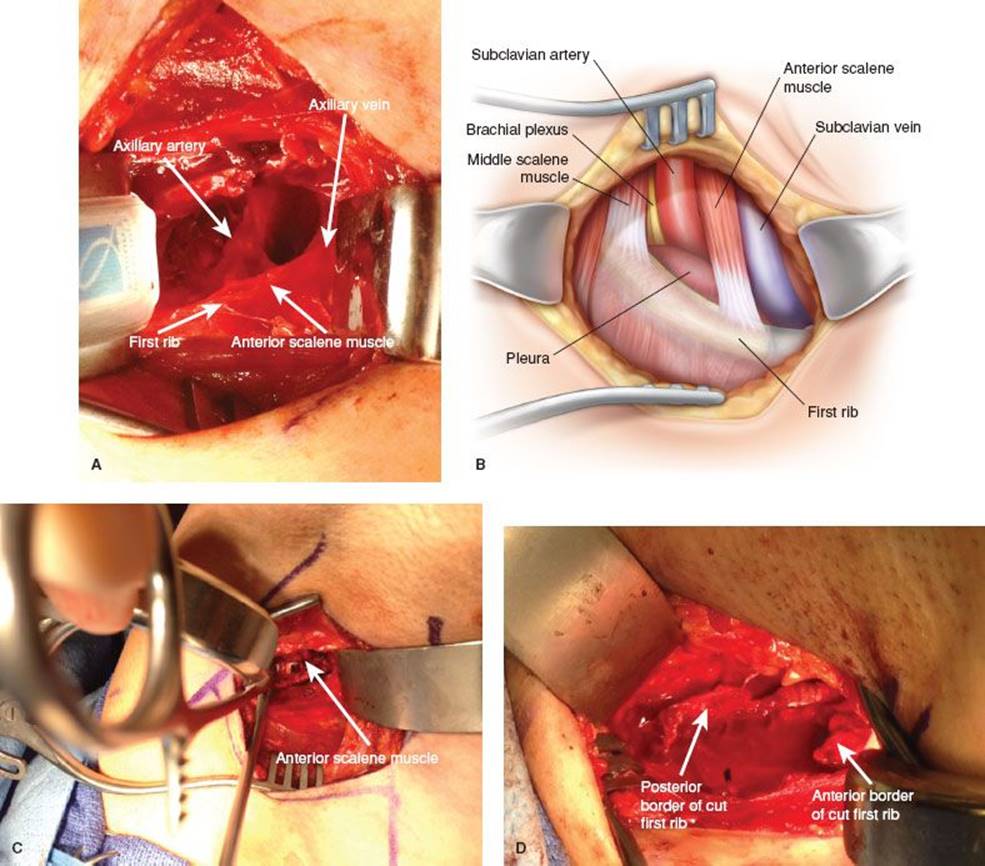
Figure 12.2 A: Axillary structures prior to rib resection. B: Schematic depiction of axillary structures. C: Anterior scalene muscle being presented between tines of a right angle clamp for division. D: Appearance of the axilla after rib removal. Please note the empty space between the borders of the removed rib.
![]() POSTOPERATIVE MANAGEMENT
POSTOPERATIVE MANAGEMENT
Postoperatively, the patient is admitted overnight for observation. A plain chest radiograph is obtained in the postoperative recovery area to evaluate for pneumothorax or confirm position of the chest tube. If a pneumothorax is present, it is usually small and does not require placement of a chest tube postoperatively. Pain is controlled with PCA overnight, and diet is advanced as tolerated. No toradol or NSAIDs are given due to risk of bleeding. An arm sling is used for comfort. On postoperative day 1, intravenous pain control is discontinued and parenteral narcotics and muscle relaxants such as soma are started. Most patients are discharged home on postoperative day 1.
Patients with venous TOS restart anticoagulation with Lovenox 72 hours after surgery. They undergo a venogram 2 weeks after rib resection. If no stenosis is present at this time, anticoagulation is stopped. If there is persistent subclavian vein stenosis, the patient undergoes gentle percutaneous venoplasty, and anticoagulation is continued for 1 to 2 months, at which time vein patency is checked with duplex ultrasound. If there is vein occlusion, anticoagulation is continued for a maximum of 6 months. These patients are checked with serial ultrasounds every 2 months to evaluate vein patency. Once the vein is patent, anticoagulation is stopped. It is stopped regardless of patency at 6 months. Patients with arterial TOS undergo duplex evaluation at 6 months and 1 year after operation. All patients receive physical therapy starting 2 weeks after the operation, focusing on posture training and muscles in the shoulder, chest, and neck area, and eventually progressing to mimicking work-related activities.
![]() COMPLICATIONS
COMPLICATIONS
The complication rate of transaxillary first rib resection and scalenectomy is low. The most common complication is pneumothorax, occurring at a rate of approximately 10%. Bleeding and infection of the wound are rare. Injuries to nerves such as the brachial plexus or the long thoracic nerve occur in less than 1% of cases. Symptom recurrence or failure of symptom resolution occurs in about 10% of patients with neurogenic TOS, and management of these patients presents several challenges beyond the scope of this chapter.
If significant bleeding is encountered during the operation, the imperative is to obtain timely proximal and distal control. One may be able to repair venous injury without further exposure by applying pressure proximally and distally on the vein to allow time for repair. With arterial injury, distal control is obtainable via the existing exposure. Proximal control will likely require additional exposure. A supraclavicular incision will allow proximal subclavian control rapidly and without the need for patient repositioning. One must keep in mind the important structures with this approach, including the phrenic nerve and the thoracic duct (on the left side). Packing of the operative field to temporize bleeding will allow time for systematic exposure. Arterial repair is accomplished once proximal and distal control is obtained. Postoperative bleeding, namely significant hematoma, is usually managed via the existing axillary incision.
![]() RESULTS
RESULTS
The results of transaxillary first rib resection and scalenectomy are best measured by resolution of symptoms, return to work and daily activities, and effects on quality of life. In neurogenic TOS, this operation has been shown to result in significant improvements in patients’ quality of life. Furthermore, long-term follow-up (mean 44.7 months) of patients after surgical decompression for neurogenic TOS reveals that the improvement in quality of life continues over time. Poorer outcomes are associated with coexisting chronic pain syndromes, neck and/or shoulder disease, other systemic diseases, smoking, age >40 years, and opioid use. Successful symptom resolution has also been shown in patients with venous TOS who undergo transaxillary first rib resection and scalenectomy with close postoperative follow-up based on several algorithms.
![]() CONCLUSIONS
CONCLUSIONS
Transaxillary first rib resection and scalenectomy is a safe and effective operation for neurogenic, venous, and arterial TOSs. With careful patient selection, meticulous surgical technique, and attention to postoperative management, this operation improves the quality of life in patients with TOS.
Recommended References and Readings
Call D, Grunebach HL, Freischlag JA. Role of the Noninvasive Vascular Laboratory in Thoracic Outlet Syndrome. AbuRahma AF, eds. Noninvasive Vascular Diagnosis. London: Springer-Verlag; 2013:499–504.
Chang DC, Lidor AO, Matsen SL, et al. Reported in-hospital complications following rib resections for neurogenic thoracic outlet syndrome. Abb Vasc Surg. 2007;21(5):564–570.
Chang DC, Rotellini-Coltvet LA, Mukherjee D, et al. Surgical interventions for thoracic outlet syndrome improves patients’ quality of live. J Vasc Surg. 2009;49:630–635.
Chang KZ, Likes K, Demos J, et al. Routine venography following transaxillary first rib resection and scalenectomy (FRRS) for chronic subclavian vein thrombosis ensures excellent outcomes and vein patency. Vasc Endovascular Surg. 2012;46(1):15–20.
Chang KZ, Likes K, Demos J, et al. The significance of cervical ribs in thoracic outlet syndrome. J Vasc Surg. 2013;57(3):771–775.
Christo PJ, Christo DK, Carinci AJ, et al. Single CT-guided chemodenervation of the anterior scalene muscle with botulinum toxin for neurogenic thoracic outlet syndrome. Pain Med. 2010; 11(4):504–511.
DeLeon RA, Chang DC, Hassoun HT, et al. Multiple treatment algorithms for successful outcomesin venous thoracic outlet syndrome. Surgery. 2009;145:500–507.
Guzzo JL, Chang K, Demos J, et al. Preoperative thrombolysis and venoplasty affords no benefit in patency following first rib resection and scalenectomy for subacute and chronic subclavian vein thrombosis. J Vasc Surg.2010;52(3):658–662.
Lum YW, Brooke BS, Likes K, et al. Impact of anterior scalene lidocaine blocks on predicting surgical success in older patients with neurogenic thoracic outlet syndrome. J Vasc Surg. 2012; 55(5):1370–1375.
Rochlin DH, Gilson MM, Likes KC, et al. Quality-of-life scores in neurogenic thoracic outlet syndrome in patients undergoing first rib resection and scalenectomy. J Vasc Surg. 2013;57(2):436–443.
Rochlin DH, Likes KC, Gilson MM, et al. Management of unresolved, recurrent, and/or contralateral neurogenic symptoms in patients following first rib resection and scalenectomy. J Vasc Surg.2012;56(4):1061–1067.