Konstantinos Papadakis and Robert C. Shamberger
![]() INDICATIONS/CONTRAINDICATIONS
INDICATIONS/CONTRAINDICATIONS
Pectus excavatum is the most common chest wall deformity in infants, children, and adolescents. Its incidence is estimated between 1 in 400 live births and 7.9 per 1,000 births. There is a male to female ratio of 3:1. The etiology of pectus excavatum is unknown. There is a positive family history of chest wall abnormalities in 37% of cases.
The sternal deformity in pectus excavatum may be either symmetrical or asymmetrical. In the asymmetric deformity, the more severe depression is typically on the right side. In up to 90% of cases, the deformity can be seen within the first year of life.
Children with pectus excavatum may present with symptoms of shortness of breath, dyspnea on exertion, and fatigue. Symptomatic improvement is frequently noted after repair. However, consistent improvement in pulmonary function tests does not follow the repair. Due to the “restrictive” nature of the defect, symptomatic improvement may be due to the relief of anterior compression of the heart, especially on the right ventricle, as well as the release of pulmonary compression. In addition to the physiologic components of the deformity, affected children also can have adverse psychological consequences.
Indications for surgery include both assessments of physiologic and psychological implications of the condition. Parents and patients must both be counseled on the risks and expected benefits of surgical correction.
![]() PREOPERATIVE PLANNING
PREOPERATIVE PLANNING
The most important factor in preoperative consideration is the severity of the deformity, usually quantified by the Haller index. It can be determined from a standard AP and lateral chest radiograph. It is defined as the ratio of the transverse diameter (the horizontal distance of the inside of the thorax) and the anteroposterior diameter (the shortest distance between the anterior aspect of the vertebrae and the posterior aspect of the sternum). A normal Haller index should be about 2.5. Depression of the sternum will increase the index. A Haller index of 3.25 or greater is the usual cutoff for consideration of surgery.
Additional evaluation can include an electrocardiogram, echocardiogram, and/or pulmonary function tests, at the surgeon’s discretion. These evaluations may be required to define the extent of the physiologic abnormality and to exclude other pathologic processes.
Another factor that must be considered is patient age. This may impact both physical and psychological concerns. Correction of pectus excavatum at a young age, before relative skeletal maturity, may lead either to a recurrence of the deformity during the pubertal growth spurt or development of a constricting deformity of the chest wall resulting from impaired chest wall growth. It is recommended to proceed with repair after the onset of puberty to avoid these problems. Psychological maturity must also be evaluated to ensure that the rigors of postoperative pain management, hospital stay, and activity restrictions are understood and adhered to.
![]() SURGERY
SURGERY
The Open “Ravitch” Procedure
The current standard open repair is attributed to Ravitch although his initial description included the resection of the costal cartilage and the perichondrium with anterior fixation of the sternum with Kirschner wires. Welch and Baronofsky in subsequent reports stressed the vital importance of preservation of the perichondrium to achieve optimal regeneration of the costal cartilage after repair.
Positioning
The patient is placed supine on a well-padded table. Lower body Bair Huggers are used to help maintain normothermia.
![]() A transverse incision is made below and between the nipple lines. In females, particular attention is taken to place the incision within the projected inframammary crease thus avoiding complications of breast deformity and development. The pectoralis major muscle is elevated from the sternum along with portions of the pectoralis minor and serratus anterior bundles (Fig. 14.1).
A transverse incision is made below and between the nipple lines. In females, particular attention is taken to place the incision within the projected inframammary crease thus avoiding complications of breast deformity and development. The pectoralis major muscle is elevated from the sternum along with portions of the pectoralis minor and serratus anterior bundles (Fig. 14.1).
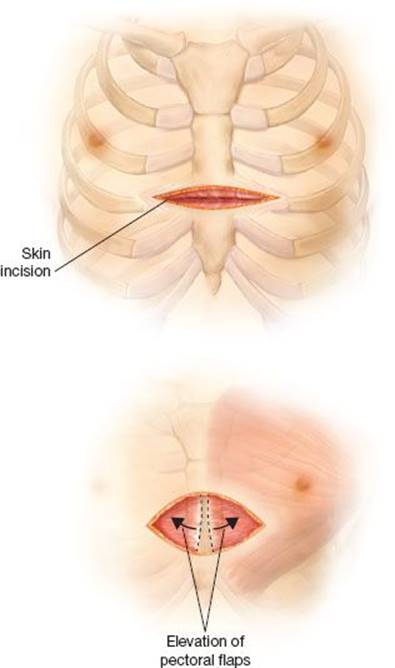
Figure 14.1 Location of the incision and initial mobilization of the pectoral muscle flaps.
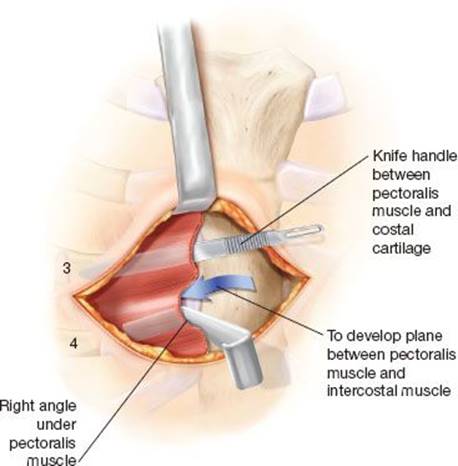
Figure 14.2 Creation of a plane between the pectoral muscle flaps and the chest wall.
![]() The correct plane of dissection of the pectoralis muscle flap is defined by passing an empty knife handle directly anterior to a costal cartilage after the medial aspect of the muscle has been elevated with electrocautery. The knife handle is then replaced with a right-angle retractor, which is pulled anteriorly. The process is then repeated anterior to an adjoining costal cartilage. Anterior distraction of the pectoral muscle during the dissection facilitates identification of the avascular areolar plane and avoids entry into the intercostal muscle bundles (Fig. 14.2).
The correct plane of dissection of the pectoralis muscle flap is defined by passing an empty knife handle directly anterior to a costal cartilage after the medial aspect of the muscle has been elevated with electrocautery. The knife handle is then replaced with a right-angle retractor, which is pulled anteriorly. The process is then repeated anterior to an adjoining costal cartilage. Anterior distraction of the pectoral muscle during the dissection facilitates identification of the avascular areolar plane and avoids entry into the intercostal muscle bundles (Fig. 14.2).
![]() Elevation of the pectoral muscle flaps is extended bilaterally to the costochondral junctions of the third to fifth ribs and a comparable distance for ribs six and seven or to the lateral extent of the deformity.
Elevation of the pectoral muscle flaps is extended bilaterally to the costochondral junctions of the third to fifth ribs and a comparable distance for ribs six and seven or to the lateral extent of the deformity.
![]() Subperichondrial resection of the costal cartilage. The objective of this step is the removal of the costal cartilage connecting the ribs to the sternum, while leaving the perichondrial sheath in place. The cartilage removal will allow mobilization of the sternum, and the remaining sheath will act as a conduit for rib regeneration after the repair. The resection is achieved by incising the perichondrium anteriorly between the intercostal muscles (Fig. 14.3). The perichondrium is then dissected away from the costal cartilages in the bloodless plane between perichondrium and the costal cartilage. Cutting back the perichondrium 90 degrees in each direction at its junction with the sternum facilitates visualization of the back wall of the costal cartilage (Fig. 14.3).
Subperichondrial resection of the costal cartilage. The objective of this step is the removal of the costal cartilage connecting the ribs to the sternum, while leaving the perichondrial sheath in place. The cartilage removal will allow mobilization of the sternum, and the remaining sheath will act as a conduit for rib regeneration after the repair. The resection is achieved by incising the perichondrium anteriorly between the intercostal muscles (Fig. 14.3). The perichondrium is then dissected away from the costal cartilages in the bloodless plane between perichondrium and the costal cartilage. Cutting back the perichondrium 90 degrees in each direction at its junction with the sternum facilitates visualization of the back wall of the costal cartilage (Fig. 14.3).
![]() The cartilages are sharply divided at their junction with the sternum as a Welch perichondrial elevator is held posteriorly to elevate the cartilage and protect the mediastinum (Fig. 14.4). The divided cartilage can then be held with an Allis clamp and elevated. The costochondral junction is preserved by leaving a segment of costal cartilage on the osseous ribs by incising the cartilage with a scalpel. Costal cartilages three through seven are generally resected, but occasionally the second cartilages must be removed as well. Segments of the sixth and seventh costal cartilages are resected to the point where they flatten to join the costal arch. Familiarity with the cross-sectional shape of the medial ends of the costal cartilages facilitates their removal. The second and third cartilages are broad and flat, the fourth and fifth are circular, and the sixth and seventh are narrow and deep.
The cartilages are sharply divided at their junction with the sternum as a Welch perichondrial elevator is held posteriorly to elevate the cartilage and protect the mediastinum (Fig. 14.4). The divided cartilage can then be held with an Allis clamp and elevated. The costochondral junction is preserved by leaving a segment of costal cartilage on the osseous ribs by incising the cartilage with a scalpel. Costal cartilages three through seven are generally resected, but occasionally the second cartilages must be removed as well. Segments of the sixth and seventh costal cartilages are resected to the point where they flatten to join the costal arch. Familiarity with the cross-sectional shape of the medial ends of the costal cartilages facilitates their removal. The second and third cartilages are broad and flat, the fourth and fifth are circular, and the sixth and seventh are narrow and deep.
![]() Once the costal cartilages are all separated from the sternum, a sternal osteotomy is created at the level of the posterior angulation of the sternum (Fig. 14.5). Generally, this is at the level of the third cartilage. Two transverse sternal osteotomies are created through the anterior cortex with a Hall air drill 3 to 5 mm apart, and the wedge of bone is partially mobilized. The base of the sternum and the rectus muscle are elevated with two towel clips and the posterior plate of the sternum at the osteotomy is fractured. The xiphoid can be divided from the sternum if its anterior angulation produces an unsightly bump below the sternum when it is elevated into its corrected position. The insertion of the rectus muscle into the sternum can generally be preserved by dividing the xiphoid with electrocautery through a lateral approach. Preservation of the attachment of the perichondrial sheaths and xiphoid to the sternum, avoids an unsightly depression that can occur below it.
Once the costal cartilages are all separated from the sternum, a sternal osteotomy is created at the level of the posterior angulation of the sternum (Fig. 14.5). Generally, this is at the level of the third cartilage. Two transverse sternal osteotomies are created through the anterior cortex with a Hall air drill 3 to 5 mm apart, and the wedge of bone is partially mobilized. The base of the sternum and the rectus muscle are elevated with two towel clips and the posterior plate of the sternum at the osteotomy is fractured. The xiphoid can be divided from the sternum if its anterior angulation produces an unsightly bump below the sternum when it is elevated into its corrected position. The insertion of the rectus muscle into the sternum can generally be preserved by dividing the xiphoid with electrocautery through a lateral approach. Preservation of the attachment of the perichondrial sheaths and xiphoid to the sternum, avoids an unsightly depression that can occur below it.

Figure 14.3 Omission of the perichondrial for resection of the costal cartilages.
![]() A retrosternal strut is placed behind the sternum and is secured to the rib ends laterally to prevent migration (Fig. 14.6).
A retrosternal strut is placed behind the sternum and is secured to the rib ends laterally to prevent migration (Fig. 14.6).
![]() The perichondrial sheath to either the fourth or fifth rib is divided from its junction with the sternum to allow passage of the strut behind the sternum. It is secured with two pericostal sutures at each end to prevent migration (Fig. 14.6). The wound is then flooded with warm saline and antibiotic solution to remove clots and inspect for pleural entry. A single-limb medium Hemovac drain is brought through the inferior skin flap and placed in a parasternal position.
The perichondrial sheath to either the fourth or fifth rib is divided from its junction with the sternum to allow passage of the strut behind the sternum. It is secured with two pericostal sutures at each end to prevent migration (Fig. 14.6). The wound is then flooded with warm saline and antibiotic solution to remove clots and inspect for pleural entry. A single-limb medium Hemovac drain is brought through the inferior skin flap and placed in a parasternal position.
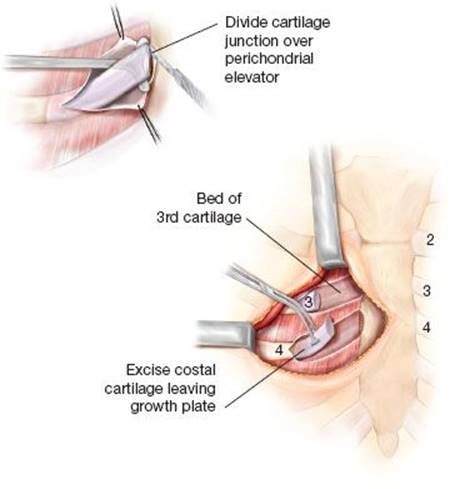
Figure 14.4 Division of the medial and lateral extent of the costal cartilages.
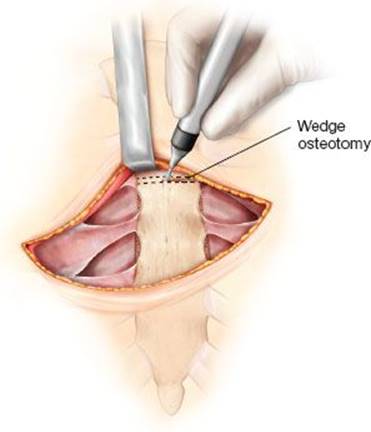
Figure 14.5 Creation of sternal osteotomy to allow anterior displacement of the sternum.
![]() The pectoral muscle flaps are secured to the midline of the sternum, advancing the flaps inferiorly to obtain complete coverage of the entire sternum (Fig. 14.7). The rectus muscle fascia is then joined to the pectoral muscle flaps, closing the mediastinum.
The pectoral muscle flaps are secured to the midline of the sternum, advancing the flaps inferiorly to obtain complete coverage of the entire sternum (Fig. 14.7). The rectus muscle fascia is then joined to the pectoral muscle flaps, closing the mediastinum.
![]() The incision is meticulously closed in layers to prevent traction on the wound. Steri-strips and an occlusive dressing are applied.
The incision is meticulously closed in layers to prevent traction on the wound. Steri-strips and an occlusive dressing are applied.

Figure 14.6 Location of the retrosternal strut which is passed through a tunnel created posterior to the anterior and anterior to the pericardium.
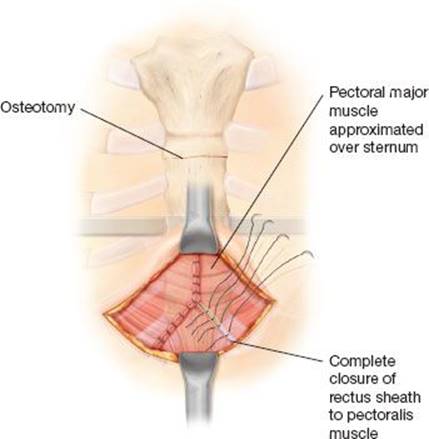
Figure 14.7 Closure of the pectoral muscle flaps which are advanced inferiorly to cover the previously bone sternum. The flaps are secured to both the sternum and to the rectus sheath.
![]() POSTOPERATIVE MANAGEMENT
POSTOPERATIVE MANAGEMENT
Postoperative antibiotics are given for one dose. Pain control is managed by a variety of techniques, which may include an epidural catheter, transpleural catheters, or intravenous narcotics in the immediate postoperative period. A multidisciplinary strategy to optimize postoperative pain may be very beneficial to the patient. Postoperative care should also include a bowel regimen, pulmonary toilet, and early ambulation. The Hemovac drain is removed when there is less than 15 mL drainage for an 8-hour shift. The average length of stay for the Ravitch procedure is 3 to 5 days. Retrosternal struts are removed a minimum of 6 months after repair to allow solid fusion of the sternum fracture and complete regeneration of the costal cartilages. The retrosternal struts are removed via a small incision over one end of the strut as an ambulatory procedure.
![]() COMPLICATIONS
COMPLICATIONS
Complications of the procedure include wound infection and pneumothorax. Wound infection can be treated with oral or intravenous antibiotics, in severe cases. Most patients with pneumothorax can be observed unless the pneumothorax is large enough to cause pulmonary impairment. Excessive blood loss that requires transfusion is rare.
Recurrence of the defect is a well-documented occurrence. The use of strut fixation optimizes early results. Delay of the repair until the patient has begun the pubertal growth spurt and achieved much of the ultimate chest wall size will decrease the amount of chest remodeling that occurs with continued growth. The risk of recurrence in large series with adequate follow-up is approximately 5% to 15%. There can be progressive deterioration of the repair over time, but once full stature is achieved, chest wall configuration is generally quite stable. Rigid strut fixation is commonly applied to patients with Marfan syndrome because of their well-recognized high risk of recurrence.
Limited postoperative rib growth has been noted to occur in children after operative repair at an early age. It results in limited growth of the ribs after resection of the costal cartilages, and produces a band-like narrowing of the midchest. This may be related to a growth plate injury at the costochondral junction, which is the longitudinal growth center for the ribs.
Serious complications regarding strut bar migration have been identified. Intracardiac migration, with resultant aorto-ventricular fistula, has been reported. Strut migration is more common in struts that have been left in place for a prolonged postoperative period. Close postoperative follow-up and routine bar removal is recommended to prevent this type of serious, yet remote complication.
![]() RESULTS
RESULTS
Deformity of the chest wall led many early authors to attribute the symptomatic improvement in patients after pectus surgery to improvement in pulmonary function. Brown and Cook performed respiratory studies on patients before and after surgical repair. Vital capacity was normal in these patients, but maximal breathing capacity (MBC) was markedly diminished in the majority of cases. MBC increased an average of 31% after surgical repair. Orzalesi and Cook performed studies in 12 children with severe pectus excavatum. The group showed a significant decrease in vital capacity, total lung capacity, and MBC from height-matched normal children. When lung volumes were measured, absolute lung volumes increased only in postoperative patients who had grown in height after surgery.
Cahill et al. performed preoperative and postoperative studies in pectus excavatum patients. The pectus excavatum patients demonstrated low normal vital capacities unchanged by operation, but a small improvement in their total lung capacity and a significant improvement in the maximal voluntary ventilation. Exercise tolerance was also improved in patients after surgery as determined by both total exercise time and the maximal oxygen consumption although both of these factors would clearly be effort related.
Derveaux et al. studied pre- and postoperative PFTs in cases that involved extensive chest wall dissection. The postoperative values for FEV1 and vital capacity were decreased in all groups when expressed as a percent of predicted. Those with less than 75% of predicted function had improved function after surgery whereas results were worse after surgery if the preoperative values were greater than 75% of predicted. These physiologic results were in contrast to the subjective improvement in symptoms from the subjects and the improved chest wall configuration. The decline in pulmonary function in postoperative studies was attributed to the surgery because the defect appeared stable regardless of the age of the initial repair. Further studies suggested that the increased restrictive defect was produced by extrapulmonary rather than pulmonary factors or that surgery produced increased rigidity of the chest wall.
Wynn et al. showed that cardiac output and stroke volume increased appropriately with exercise before and after operation in both groups, and operation was thought to have produced no physiologically significant effect on the response to exercise.
Kelly et al. in a large prospective, multicenter study, reviewed pre- and postoperative pulmonary function tests after surgical pectus correction using both the open and “Nuss technique.” A separate cohort was subjected to both static and exercise pulmonary function testing after 1 year. All groups demonstrated a significant improvement in lung function at rest in VO2 max and O2 pulse following surgical correction. However, the cohorts who underwent exercise testing early and at 1-year post correction, failed to show significant improvement after repair. There is significant improvement in CT index following surgery, but there is no significant improvement in exercise pulmonary functions when measured.
Overall, the studies of pulmonary function have failed to document consistent improvement in pulmonary function resulting from surgical repair. Studies have indeed demonstrated deterioration in pulmonary function at long-term evaluation attributable to increased chest wall rigidity after surgery. Despite these findings, studies have shown improvement in exercise tolerance after repair.
Depression of the sternum can deform the underlying heart, particularly producing anterior indentation of the right ventricle. Exercise studies have shown that increased cardiac output can be achieved primarily by increased heart rate as the stroke volume is limited. Intracardiac pressures are normal at rest and with exercise despite the apparent limitation of ventricular volume. Postoperative studies have shown an increase in cardiac index on average of 38%. An enhanced stroke volume response was responsible for this increase as heart rate at maximal exercise was not higher after surgery.
The degree of symptoms cannot be correlated with the severity of the anatomic defect. Peterson et al. documented a marked decrease in symptoms after surgical correction of pectus excavatum in a regulated exercise protocol, substantiating anecdotal reports regarding symptomatic improvement after repair.
![]() CONCLUSIONS
CONCLUSIONS
![]() The open “Ravitch” procedure for pectus excavatum is well tolerated.
The open “Ravitch” procedure for pectus excavatum is well tolerated.
![]() It has excellent structural results.
It has excellent structural results.
![]() It has a low complication rate.
It has a low complication rate.
![]() For optimal results, it should be performed after the patient has begun or completed their pubertal growth spurt.
For optimal results, it should be performed after the patient has begun or completed their pubertal growth spurt.
![]() In cases of patients with connective tissue disorders, the struts will need to be left in for a longer period of time to minimize the risk for recurrence.
In cases of patients with connective tissue disorders, the struts will need to be left in for a longer period of time to minimize the risk for recurrence.
![]() Preoperative severity of the defect does not correlate with functional limitations.
Preoperative severity of the defect does not correlate with functional limitations.
![]() Surgical correction of the pectus excavatum often leads to subjective improvement in exercise tolerance.
Surgical correction of the pectus excavatum often leads to subjective improvement in exercise tolerance.
![]() Cardiac function may improve after repair with improvement in oxygen consumption and cardiac index.
Cardiac function may improve after repair with improvement in oxygen consumption and cardiac index.
![]() Objective recurrence rate is low.
Objective recurrence rate is low.
Recommended References and Readings
Aydemir B, Sokullo O, Hastaoglu O, et al. Aorto-to-right ventricular fistula due to pectus migration. Thorac Cardiovasc Surg. 2011;59:51–52.
Bevegard S. Postural circulatory changes at rest and during exercise in patients with funnel chest, with special reference to factory affecting the stroke volume. Acta Med Scand. 1962;171:695–713.
Borgeskov S, Raahove D. Long-term result after operative correction of funnel chest. Thorax. 1971;26:74–76.
Brown AL, Cook O. Cardio-respiratory studies in pre and post operative funnel chest (pectus excavatum). Dis Chest. 1951;20:378–391.
Cahill JL, Lees GM, Robertson HT. A summary of preoperative and postoperative cardiorespiratory performance in patients undergoing pectus excavatum and carinatum repair. J Pediatr Surg. 1984;19:430–433.
Colborn GL, Weidman TA, Mirilas P, et al. Chapter 2. Thoracic wall and pleurae. In: Skandalakis JE, ed. Surgical Anatomy: The Embryologic and Anatomic Basis of Modern Surgery. Athens, Greece: PMP; 2004:117–146.
Derveaux L, Clarysse I, Ivanoff I, et al. Preoperative and postoperative abnormalities in chest x-ray indices and in lung function in pectus deformities. Chest. 1989;95;850–856.
Derveaux L, Ivanoff I, Rochette F, et al. Mechanism of pulmonary function changes after surgical correction for funnel chest. Eur Respir J. 1988;1:823–825.
Haller JA, Kramer SS, Lietman A. Use of CT scans in selection of patients for pectus excavatum surgery: A preliminary report. J Pediatr Surg. 1987;22:904–906.
Humphreys GH II, Jaretzki A III. Pectus excavatum: Late results with and without operation. J Thoracic Cardiovasc Surg. 1980; 80:686–695.
Kelly RE Jr, Mellins RB, Shamberger RC, et al. Multicenter study of pectus excavatum, final report: Complications, static/exercise pulmonary function, and anatomic outcomes. J Am Coll Surg.2013;217(6):1080–1089.
Morshuis WJ, Mulder H, Wapperom G, et al. Pectus excavatum: A clinical study with long-term postoperative follow-up. Eur J Cardiothoracic Surg. 1992;6:318–329.
Orzalesi MM, Cook CD. Pulmonary function in children with pectus excavatum. J Pediatr. 1965;66:898–900.
Papadakis K, Shamberger RC. Congenital thoracic deformities. In: Prem Puri, ed. Newborn Surgery. 3rd ed. London, Great Britain: Hodder Arnold; 2011:297–304.
Peterson RJ, Young WG Jr, Godwin JD, et al. Noninvasive assessment of exercise cardiac function before and after pectus excavatum repair. J Thorac Cardiovasc Surg. 1985;90:251–260.
Prevot J. Treatment of sternocostal wall malformations of the child: A series of 210 surgical correnctions since 1975. Eur J Pediatr Surg. 1994;4:131–136.
Ravitch MM. Operative treatment of congenital deformities of the chest. Am J Surg. 1961;101:588–597.
Ravitch MM. The operative treatment of pectus excavatum. Ann Surg. 1949;129:429–444.
Shamberger RC, Welch KJ. Surgical repair of pectus excavatum. J Pediatr Surg. 1988;23:615–622.
Shamberger RC. Congenital chest wall deformities. Curr Probl Surg. 1996;33:469–542.
Scherer LR, Arn PH, Dressel DA, et al. Surgical management of children and young adults with Marfan syndrome and pectus excavatum. J Pediatr Surg. 1988;23:1169–1172.
Wynn SR, Driscoll DJ, Ostrom NK, et al. Exercise cardiorespiratory function in adolescents with pectus excavatum. J Thorac Cardiovasc Surg. 1990;99:41–47.
Zhang R, Hagl C, Bobylev D, et al. Intrapericardial migration of dislodged sternal struts as late complication of open pectus excavatum repairs. J Cardiothoracic Surg. 2011;6:40–44.