Mohamed Khereba, Basil S. Nasir, and Moishe Liberman
![]() INDICATIONS/CONTRAINDICATIONS
INDICATIONS/CONTRAINDICATIONS
The trachea traverses the entire neck and enters the chest through the thoracic inlet where it turns posteriorly, eventually occupying a posterior location within the mediastinum. This makes access to the entire trachea through one approach difficult. It is also a rigid tube with very little flexibility; hence, resection of great lengths poses challenges to producing a tension-free reconstruction. However, ensuring a tension-free anastomosis is amongst the most important factor for acceptable postoperative outcome after tracheal resection.
Cantrell and Folse determined a biologic dangerous tension limit of 1,700 g for ensuring the integrity of the tracheal anastomosis. The length of trachea that can be resected using cervicomediastinal mobilization and neck flexion varies with each individual; however, it ranges from 4 to 6 cm, or approximately seven tracheal rings. During certain situations, greater lengths of trachea need to be resected. When such situations arise, mobilization of both tracheal ends through different release maneuvers is employed for ensuring a tension-free anastomosis. Pearson et al. performed pericardial hilar release in 47% of tracheal resections in a series of 32 patients.
While laryngeal release is commonly used in upper tracheal resections, the hilar mobilization through pericardial release maneuvers is more helpful in lower tracheal, carinal, and mainstem bronchial procedures. However, hilar release maneuvers are rarely performed for benign stenotic lesions and are more often reserved for patients with malignant lesions who can tolerate extensive surgery. In the largest series of carinal resections published in 1999, Grillo et al. described 143 cases, performing release maneuvers in 64 patients. These consisted of 49 hilar pericardial releases, 3 laryngeal releases and both maneuvers in 12 cases.
A lengthy midtracheal lesion or extended microscopic disease that was not anticipated preoperatively might necessitate mobilization of both ends of the trachea. In some cases the introduction of a previous tracheostomy might add to the lengthy stenotic segment.
In carinal resections the left mainstem bronchus is usually fixed by the aortic arch and most of mobilization comes from the tracheal side to ensure an end-to-end anastomosis between the trachea and the left mainstem bronchus. In this case, if the gap (resected trachea) exceeds 4 cm, tension will be exerted on the anastomosis even with maximal release maneuvers. In such cases, Grillo et al. demonstrated that hilar release is mandatory, with subsequent anastomosis of the right main bronchus to the trachea and anastomosis of the left main bronchus either to the right mainstem bronchus or the bronchus intermedius.
Contraindications
Contraindications to performing pericardial release maneuvers during tracheal resections are mainly technical. Excessive fibrosis resulting from previous surgery or mediastinitis/pericarditis that obscures the anatomy renders these maneuvers more risky. Excessive inflammation from recently failed tracheal reconstruction can result in a more technically challenging procedure and bleeding can rarely be problematic during hilar release. Some patients will not tolerate more extended morbid incision added solely for the purpose of hilar release. In these patients, a two-staged operation might offer another option. Video-assisted thoracoscopic surgery (VATS) pericardial hilar release is also possible in experienced hands.
![]() PREOPERATIVE PLANNING
PREOPERATIVE PLANNING
Evaluation of the extent of tracheal disease is of enormous value in planning tracheal resection. The decision to proceed with a release maneuver is dependent on the length of trachea to be resected. The length of trachea that is possible to resect using cervicomediastinal mobilization and without extensive release maneuvers is up to 6 cm. This varies depending on factors such as age, body habitus, posture, and previous tracheal surgery. Suprahyoid release techniques add approximately 1 to 2 cm of length that can be resected and are most useful for resections of the upper and midtrachea. Suprahyoid release adds very little to resections of the lower trachea and carina. The technique for suprahyoid release is discussed in Chapter 31. Pericardial hilar release maneuvers can allow additional resection of up to 3 cm during lower tracheal resections. With the aid of release maneuvers, more than half of the trachea can be resected.
Preoperative anticipation for the need for hilar pericardial release is essential during the general planning of tracheal resection. This is typically done with imaging and bronchoscopy. Imaging with computed tomography (CT) is most useful for assessment of the trachea and proximal bronchi. It is also useful as a staging procedure in cases of malignancy. Rigid bronchoscopy is vital in assessing the length of trachea that needs to be resected, and measurements of the length of the tumors, distance from vocal cords, carina, and the length of involvement of the mainstem bronchi are used to plan the resection.
Assessment of the patient’s general condition, cardiorespiratory functions and anatomy is vital. A decision needs to be made about the patient’s ability to tolerate the addition of sternotomy, unilateral or bilateral thoracotomy, or VATS procedure(s). Knowledge of previous thoracic procedures and complications that occurred is of critical value to decide the feasibility and risk of performing pericardial release. Previous tracheal resections, lung resections, sternotomy, or mediastinitis can greatly influence the technical feasibility or the benefit from pericardial release.
![]() SURGERY
SURGERY
Positioning and Incisions
Patient positioning and incision planning is critical. The patient should be positioned and prepared for a possible median sternotomy with a T incision through the left fourth intercostal space, right thoracotomy up to the axillary fold or even in rare cases bilateral thoracotomy or thoracoscopy. Bilateral submammary incisions can be performed in cases where bilateral intrapericardial release is anticipated.
In cases where resection is performed via cervicomediastinal approach or median sternotomy, the patient is positioned supine with both arms tucked. If access to one of the arms is required for venous access of invasive arterial monitoring, then the arm could be abducted on an arm board. If a unilateral pericardial release is anticipated, then a rolled support is placed longitudinally beneath the upper back, parallel to the spine, off the midline toward the side of the anticipated thoracotomy. The ipsilateral shoulder is partially abducted and the elbow is partially flexed. This elevates the thorax slightly and exposes it all the way to the posterior axillary line, making an extension via an ispilateral anterior thoracotomy much more feasible.
For patients who undergo resection via a right thoracotomy, the position is just as that for a standard right thoracotomy with the patient in left lateral decubitus position.
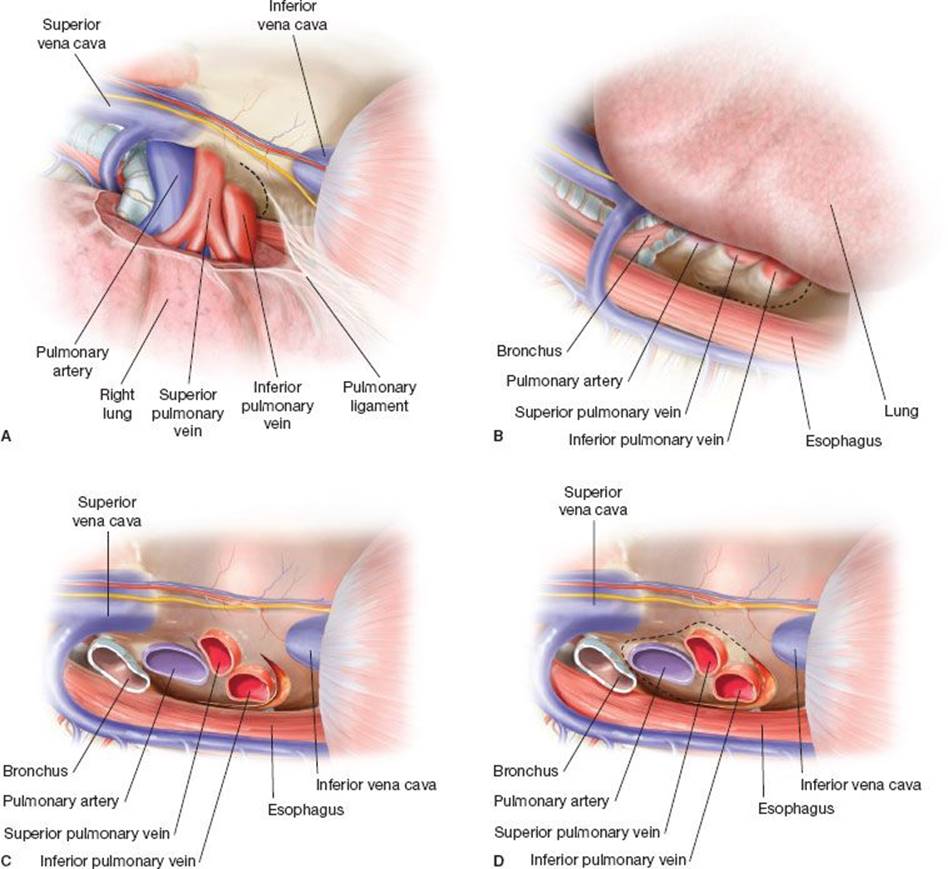
Figure 32.1 Right pericardial release (transpleural). A: After division of the pulmonary ligament, a U-shaped incision (dotted line) is performed in the right pericardium anterior and inferior to the inferior pulmonary vein. B: Completion of the pericardial incision posterior to the inferior pulmonary vein. C:Sagittal view of the right hilum from the intrapericardial side. D: Extension of the pericardial incision anteriorly and posteriorly until the superior aspect of the pulmonary artery is reached with complete encircling of the hilum increases hilar mobilization.
Technique
Release maneuvers should be ideally anticipated and accomplished before tracheal incision and resection. Access to right hilar mobilization by pericardial release can be accomplished through right thoracotomy in the fourth intercostal space or right VATS. If median sternotomy is already performed, the right pleura can be incised and mobilization of the right hilum performed although it might be technically more challenging. We have preferred a right VATS procedure for right hilar release in patients undergoing resection and reconstruction through median sternotomy. The right hilar release can also be achieved transpericardially through extended anterior pericardiotomy giving access to the right pulmonary veins. However, the transpleural route is simpler and safer as the access to the right inferior pulmonary vein is difficult because of the presence of inferior vena cava and right atrium.
After identifying and preserving the phrenic nerve, the inferior pulmonary ligament is divided to give access to the pericardium over the inferior pulmonary vein. A U-shaped incision in the pericardium is then performed anterior, inferior, and posterior to the inferior pulmonary vein. The phrenic nerve lies anterior to the plane of the pericardial incision. The intrapericardial longitudinal raphe between the inferior pulmonary vein and inferior vena cava attaching the pericardium to the epicardium is freed above to the entry of the inferior pulmonary vein into the atrium. To gain even more hilar mobility, an extension of the pericardial incision posteriorly and anteriorly directed superiorly above the pulmonary artery is performed rendering the pericardium completely incised around the hilum.
Right pericardial release (Fig. 32.1) can add 1 to 2 cm to right hilar mobility to secure a tension-free anastomosis. Care must be taken not to injure the phrenic nerve anterior to the pulmonary vessels. Preservation of mediastinal tissue around the hilum especially posterior to the pericardium and inferior to the main bronchus will aid the preservation of bronchial blood supply and posterior pulmonary lymphatics. Closure of pericardium is not necessary after pericardial hilar release.
Left hilar release (Figs. 32.2 and 32.3) through pericardial incision is mostly indicated in cases of left main bronchial sleeve resection and as a part of bilateral hilar release in extensive tracheal resections and carinal resections. As in right hilar release, it can be achieved transpleurally or from the intrapericardial route. Access to the left transpleural release can be achieved through T sternotomy to the left fourth intercostal space, through left posterolateral thoracotomy or left VATS. Transpleural left hilar release is performed in the same technique as right hilar release. Some authors suggest dividing the ductus arteriosus to allow the left hilum to shift upward.
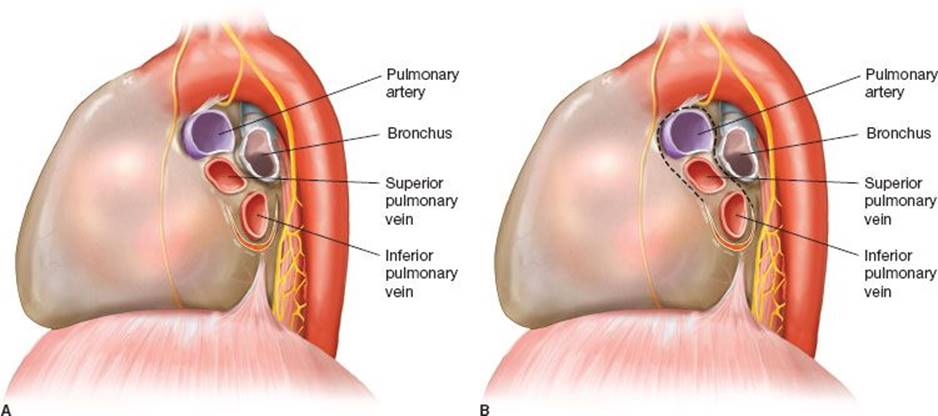
Figure 32.2 Left hilar release (transpleural). A: U-shaped incision is performed in the pericardium anterior, inferior, and posterior to the inferior pulmonary vein. B: Extension of the pericardial incision to encircle the left hilum with division of the ductus arteriosus. Care should be taken not to injure the left recurrent laryngeal nerve while dissecting the ductus.
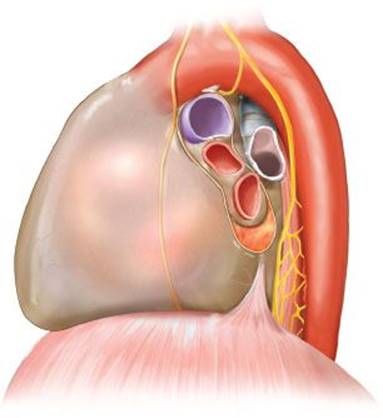
Figure 32.3 Left-sided pericardial hilar release after sleeve resection. Release incision marked by yellow line.
Most patients will not tolerate cardiac retraction for proper left hilar exposure and pericardial release transpleurally. Through sternotomy, CD Wright described a left hilar release maneuver from the intrapericardial side through a wide anterior pericardiotomy. This technique is well tolerated and is associated with less morbidity as it does not necessitate thoracotomy. From inside the pericardium, a transpericardial incision is performed anterior, inferior, and posterior to the inferior pulmonary vein. The incision anterior to the pulmonary vein should be very close to the vein to avoid the phrenic nerve anteriorly. As visualization of the phrenic nerve through the pericardium is impossible, the nerve can be visualized by dissecting between the outer surface of the pericardium and the left mediastinal pleura.
Adding another thoracotomy, sternotomy, or left VATS to the right thoracotomy solely for left hilar release is excessive in most cases, however, sometimes necessary. Limited blunt dissection of the anterior surface of the left main bronchus aids in left hilar release from the fixed aortic arch. However, care must be taken to preserve the bronchial blood supply and pulmonary lymphatics.
![]() COMPLICATIONS
COMPLICATIONS
There were no significant intraoperative or postoperative complications related to pericardial release maneuvers in the few series published in the literature. Vascular complications might be the most dangerous ones during release close to pulmonary main vessels and left atrium. The risk increases after previous operations or if there is excessive inflammation due to infection in the area.
Risk of phrenic nerve injury should always be considered and avoided by proper identification of the nerve during transpleural pericardial release. Although the nerve cannot be visualized from intrapericardial side, keeping the incision as close as possible to the inferior pulmonary vein anteriorly can help avoid phrenic nerve injury.
Cardiac arrhythmia may complicate manipulations and heart retraction during pericardial release, especially on the left side. Supraventricular tachycardia and atrial fibrillation are the most commonly encountered arrhythmias. Patients with enlarged left atrium are at increased risk.
Excessive dissection of mediastinal hilar tissues might also compromise the bronchial vascular and lymphatic supply to the hilum. Care should be taken to preserve normal mediastinal tissue as much as possible.
Recommended References and Readings
Grillo HC. Surgery of the Trachea and Bronchi. Hamilton, Ontario: BC Decker Inc; 2004.
Liberman M, Mathisen DJ. Surgical anatomy of the trachea and techniques of resection and reconstruction. In: Shields TW, Locicero J, Reed CE, et al., eds. General Thoracic Surgery. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:955–965.
Maziak DE, Todd TR, Keshavjee SH, et al. Adenoid cystic carcinoma of the airway: Thirty-two-year experience. J Thorac Cardiovasc Surg. 1996;112:1522–1532.
Mitchell JD, Mathisen DJ, Wright CD, et al. Clinical experience with carinal resection. J Thorac Cardiovasc Surg. 1999;117:39–53.
Mulliken JB, Grillo HC. The limits of tracheal resection with primary anastomosis: Further anatomical studies in man. J Thorac Cardiovasc Surg. 1968;55:418–421.