Tad Kim and Pierre de Delva
Bullous emphysema is characterized by cystic degeneration of the lung parenchyma. The distribution of bullous emphysema can be focal or diffuse. These cystic airspaces can expand to occupy a significant portion of the pleural cavity and, in the case of focal disease, restrict ventilation of adjacent functional lung tissue. Giant bullae occupy greater than 30% of the chest cavity and can cause significant dyspnea and hypoxia due to compression of functional adjacent lung, air trapping, loss of airway elastic recoil, and impaired diaphragmatic function. It has long been recognized that resection or decompression of giant bulla can improve respiratory mechanics and symptoms in selected patients with giant bullous emphysema.
Bullectomy, performed by thoracoscopy, thoracotomy or sternotomy, is an accepted method of management in patients with significant symptoms. Some patients with giant bullae have limited pulmonary reserve and will not tolerate either single lung ventilation required for thoracoscopy or the pulmonary compromise associated with a transthoracic resection. Furthermore, bullectomy often sacrifices some functional lung tissue and, despite buttressed staple lines, can be complicated by prolonged air leak. In certain situations, drainage of the bulla can achieve similar improvements in respiratory mechanics without the disadvantages of bullectomy.
Intracavitary intubation and suction drainage was initially described by Monaldi in 1938 for decompression of pulmonary abscess cavities with post-tuberculous infection. The procedure was designed as a minimally invasive alternative for patients who would not tolerate resection, thoracoplasty, plombage, or pneumothorax therapy. Monaldi recognized that a pulmonary cavity originates from the destruction of lung tissue, resulting in the formation of the initial pathologic space. The driving force behind the persistence and expansion of the cavity can be due to biologic factors such as persistent infection or, as in the case of giant bullae, mechanical expansion due to the weakened wall of the cyst and pressurization by the communicating bronchus. Crucial to the permanent closure of cystic cavities of the lung by drainage requires control of the infected space, collapse of the cyst, obliteration of the feeding bronchi, and the creation of pleural adhesions to prevent pneumothorax. The original Monaldi procedure and several modified techniques were designed to achieve these goals.
Details of the current technique are to follow, but the original Monaldi procedure was a staged operation designed to manage infected cyst. The cavity was localized by radiographs, needle decompression, and exploration. A small incision was made over the cyst. A limited segment of rib was resected, and the pleura was opened. The wound was packed to induce pleural adhesions. One to two weeks later, a catheter was placed within the cavity for drainage. Monaldi employed a mixture of charcoal, keratin, and collodion to achieve obliteration of the cavity and feeding bronchus. The small bronchocutaneous fistula created by the drainage catheter invariably healed after removal of the catheter.
Several authors have applied the principles of the Monaldi procedure to the management of symptomatic giant bullae. The advantages of intracavitary drainage include a limited incision, short anesthetic time, preservation of lung tissue, and low risk of persistent air leak. Goldstraw and colleagues from the Brompton Hospital in the United Kingdom reported the modification of the Monaldi technique into a single-stage procedure for the management of symptomatic giant bullae. Their results demonstrate subjective symptomatic relief, objective improvement in pulmonary function testing, and reasonable operative mortality. The Brompton technique with slight modifications by other authors represents the modern approach for intracavitary drainage of giant symptomatic bullae.
![]() INDICATIONS/CONTRAINDICATIONS
INDICATIONS/CONTRAINDICATIONS
Historical indications for the Monaldi procedure include decompression of post-tuberculous and pyogenic pulmonary abscess cavities. Image-guided percutaneous drainage has become the treatment of choice for pulmonary abscesses that do not resolve with systemic antibiotics.
The modified Monaldi procedure for giant bullous emphysema (Brompton technique) is currently indicated for patients meeting the following criteria:
1. Dominant, discrete bullous lung disease encompassing 30% or more of the pleural space and with functional surrounding lung parenchyma.
a. The cyst should have a small number of septations to ensure complete drainage with one or two drainage catheters.
2. Disabling dyspnea.
Absolute contraindications for a modified Monaldi procedure include:
1. No viable or functional lung surrounding the bulla.
2. Diffuse, nonparaseptal emphysema.
Relative contraindications include:
1. Mild symptoms
2. FEV1 less than 350 mL (due to higher mortality risk)
![]() PREOPERATIVE PLANNING
PREOPERATIVE PLANNING
Evaluation includes history and physical examination, documentation of severity of dyspnea and pulmonary impairment and smoking cessation. Pulmonary rehabilitation for up to 6 weeks with deep breathing exercises, coughing exercises, incentive spirometry, and out-of-bed activity has been shown to be beneficial in preoperative patients with advanced emphysema.
Preoperative workup includes:
1. Chest radiograph
2. CT scan of the chest
3. Pulmonary function tests (including lung volumes by whole body plethysmography, spirometry, and diffusion capacity)
4. Arterial blood gas
The most important aspect of the preoperative plan is selecting the appropriate patients based on severity of symptoms and CT imaging. Patients with dominant giant bulla with limited septations and compressed functional lung tissue are the ideal candidates for this procedure (Fig. 8.1).

Figure 8.1 Sagittal and coronal computed tomography images of the chest demonstrating a giant bulla compressing the right lower lobe and flattening the diaphragm.
![]() SURGERY
SURGERY
The airway strategy is flexible with the modified Monaldi procedure and depends on the ability of the patient to tolerate single lung ventilation. Airway management strategies include:
1. Spontaneous breathing with local anesthetic
2. Double lung ventilation via single-lumen tube
3. Double lung ventilation via single-lumen tube with intermittent apnea
4. Single lung ventilation via double-lumen tube or bronchial blocker
Fiberoptic bronchoscopy may be performed to assess the anatomy of the tracheobronchial tree and obtain cultures.
Positioning
The patient is placed in the optimal position to provide access to the bulla. The location of the incision is based on CT imaging and can be landmarked by the specific interspace or rib overlying the bulla.
Technique of the Modified Monaldi Procedure
The operative steps for the single-stage modified Monaldi procedure for decompression of giant bullae are:
1. A small incision is made directly over the most dependent portion of the bulla as determined by preoperative imaging or with assistance of thoracoscopy (Fig. 8.2).
a. Thoracoscopy of the pleural space can aid in selecting a site for drainage of the incision and free up the lung from pleural adhesions.
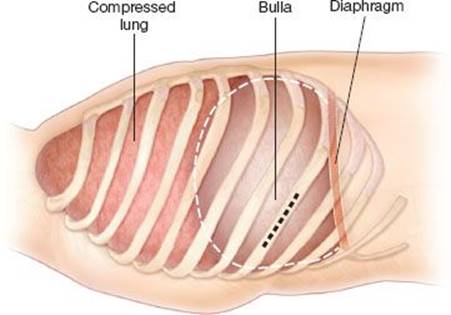
Figure 8.2 Sagittal view of the chest wall demonstrating localization of the incision based on a rib overlying a dependent portion of the giant bulla (light gray).
2. Subperiosteal excision of a limited segment of rib to allow visualization and adequate exposure of the underlying pleura (Fig. 8.3).
3. The parietal pleura and bulla are incised.
4. A 3-0 polypropylene purse-string suture is placed in the bleb itself or, if the tissue is too friable, reinforced by incorporating the parietal pleura in the purse-string suture (Fig. 8.4).
5. A finger may be inserted to lyse septations within the dominant bulla.
b. Insertion of a 5-mm thoracoscope into the cyst cavity can aid in full exploration of the bulla. This can be accomplished by securing a thoracoport through the purse-string incision and inserting the camera inside the cavity. Thin thoracoscopic instruments can be used to lyse intracavitary septations.
6. A 32-Fr Foley catheter (the “intracavitary drain”) is inserted and the cavity insufflated with talc via the Foley, and then the purse string is secured down with the balloon of the Foley flush against the chest wall (Fig. 8.5).
7. A dependent intrapleural tube thoracostomy is placed to decompress the pleural space (Fig. 8.6). Talc may be applied to the pleural space intraoperatively or in the postoperative period if there is concern for the total dosage of talc given to the patient in one setting.
8. The Foley catheter may be brought out through the incision or through a short tunnel adjacent to the incision.
9. Both the intracavitary drain and the pleural chest tube are placed to suction.
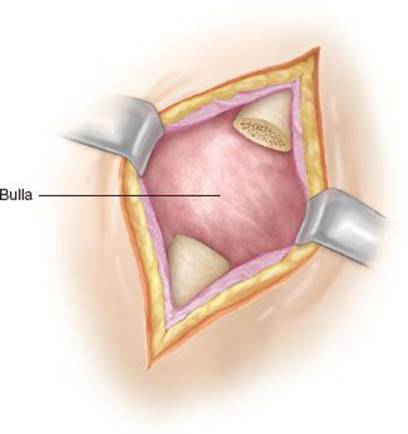
Figure 8.3 Skin incision and subperiosteal excision of a small portion of the rib overlying the bulla.
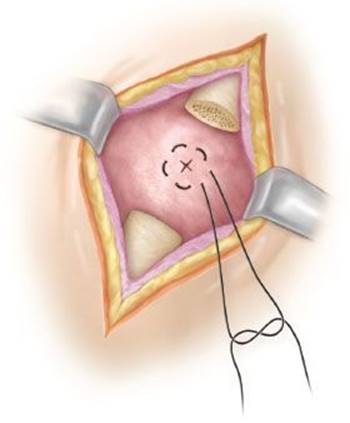
Figure 8.4 Placement of the purse-string suture and incision of the bulla.
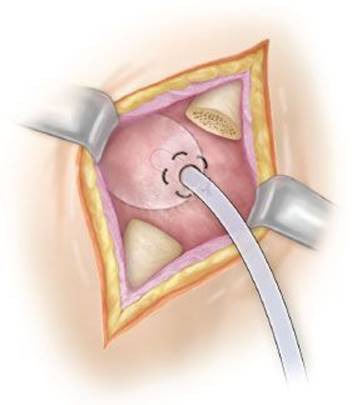
Figure 8.5 Intracavitary Foley catheter inserted into the bulla and secured with the purse-string suture.
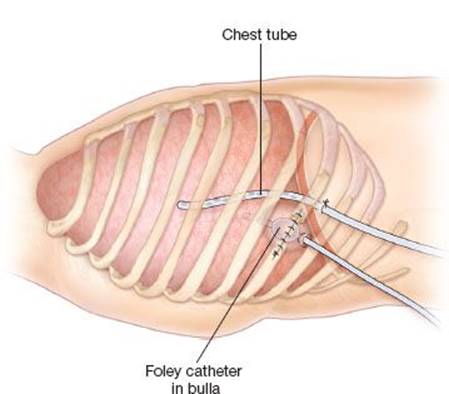
Figure 8.6 Sagittal view of the chest wall demonstrates placement of the intracavitary and pleural drains.
![]() POSTOPERATIVE MANAGEMENT
POSTOPERATIVE MANAGEMENT
Postoperatively, the intrapleural drain is kept on 20 cm suction for 2 days and then removed when the air leak has stopped. The intracavitary drain is kept on suction for 2 days but may be water sealed with a persistent air leak if the cavity is collapsed on imaging. Once the patient is ambulating with adequate pain control, the patient can be discharged with the intracavitary drain (Foley) on a one-way valve container (i.e., Heimlich valve) for 1 to 2 weeks—allowing for formation of a controlled bronchocutaneous fistula. The intracavitary drain can be removed after 7 to 14 days, irrespective of residual air leak. The bronchocutaneous fistula usually closes within 24 to 48 hours.
![]() COMPLICATIONS
COMPLICATIONS
Complications of the Monaldi procedure include mortality (due to the high-risk nature of these patients with such poor preoperative pulmonary function), pulmonary complications such as pneumonia or pleural space infection, and recurrence of pneumothorax due to additional bullae. Future pneumothoraces due to residual bullae can be managed with percutaneous pigtail catheter drainage, as the intrapleural talc administration at the index operation should promote adhesion formation and decrease the likelihood of lung collapse.
![]() RESULTS
RESULTS
Operative mortality with the modified Monaldi procedure ranges from 6.5% to 15%.
This procedure is associated with radiographic improvement in 97%. Objective improvement in pulmonary function (FEV1 and vital capacity) has been observed in 83% of cases. More importantly, symptomatic relief can be expected in well-selected patients. Shah et al. updated the results with the Brompton technique in 1994 and reported symptomatic relief in 90% of patients; average FEV1 increased by 28%, and average total lung capacity increased by 12%. Venn et al. demonstrated operative mortality of 3 of 20 (15%) due primarily to low preoperative FEV1 (median 350 mL). Symptomatic improvement was reported in 16 of the remaining 17 surviving patients (94%) with 22% median improvement in FEV1, 11% median reduction in total lung capacity, and 26% median reduction in residual volume.
![]() CONCLUSIONS
CONCLUSIONS
Due to the high morbidity (up to 50%) with bullectomy or resectional procedures in patients with poor pulmonary reserve, the Monaldi procedure is an excellent minimally invasive option for patients with large, dominant bulla and disabling dyspnea. The current Brompton modification of the Monaldi procedure is a safe and effective alternative to achieve successful and complete decompression of giant bullous cavities with subsequent expansion of adjacent lung and symptomatic improvement.
Recommended References and Readings
Cope JH. Monaldi procedure. Calif Med. 1950;73:563–564.
Froeschle P, Krishnadas R, Berrisford R. Video-assisted approach combined with the open Brompton technique for intracavitary drainage of giant bullae. Thorac Cardiovasc Surg. 2012;60:164–166.
Greenberg JA, Singhal S, Kaiser LR. Giant bullous lung disease: Evaluation, selection, techniques, and outcomes. Chest Surg Clin N Am. 2003;13:631–649.
Head JR. Intracavitary (Monaldi) suction. J Thorac Surg. 1946;15:153–161.
Kelley WO, Pecora DV. The Monaldi procedure; a report of thirty cases. Am Rev Tuberc. 1952;65:83–87.
MacArthur AM, Fountain SW. Intracavitary suction and drainage in the treatment of emphysematous bullae. Thorax. 1977;32:668–672.
Monaldi V. Endocavitary aspiration; its practical application. Tubercle. 1946;28:223–228.
Monaldi V. Endocavitary aspiration in the treatment of lung abscess. Dis Chest. 1956;29:193–201.
Shah SS, Goldstraw P. Surgical treatment of bullous emphysema: Experience with the Brompton technique. Ann Thorac Surg. 1994;58:1452–1456.
Suzuki C. Treatment of pulmonary tuberculosis by Monaldi transthoracic cavity suction drainage with thoracoplasty. Tohoku J Exp Med. 1950;52:77–86.
Venn GE, Williams PR, Goldstraw P. Intracavitary drainage for bullous, emphysematous lung disease: Experience with the Brompton technique. Thorax. 1988;43:998–1002.
Vergeret J, Dabadie P, Dupon M, et al. Endocavitary drainage (Monaldi’s technique) in the treatment of pulmonary abscess. Rev Fr Mal Respir. 1983;11:201–207.
Wang H, Xu Z, Gao W. A modified Brompton technique for the treatment of giant bulla in patients with diffuse emphysema. Thorac Cardiovasc Surg. 2012;60:161–163.