Jeffrey C. Posnick
Ramon L. Ruiz
The satisfactory rehabilitation of a child born with cleft lip and palate (CLP) presents unique challenges. Close cooperation is required among the specialists who integrate their talents for the child's overall well-being. A coordinated approach is required to achieve ideal speech, occlusion, facial aesthetics, and individual selfesteem (Adams, 1981; Berry et al, 1997; Broder and Strauss, 1989; Harper, 1995; Richman and Eliason, 1982; Richman et al., 1985). The effective cleft palate (CP) team is patient-, family-, and community-oriented rather than physician-, specialty-, and hospital-centered (Benacerraf and Mulliken, 1993; Slutsky, 1969).
Koop (1987), then the Surgeon General of the United States, issued a report, Children with Special Health Care Needs, that called for a family-centered, community-based, coordinated healthcare delivery system for children with special needs (Christensen and Fogl-Andersen, 1993; Jensen et al., 1983; Jones, 1988; Laatikainen et al., 1996).
The American Cleft Palate-Craniofacial Association (ACPA) (1993) responded by developing parameters of care designed to facilitate the rehabilitation of patients with CLP. The parameters developed by the ACPA support the concept of interdisciplinary care for the CLP patient, encouraging the use of treatment protocols that emphasize the thoughtful timing of interventions (surgery, speech and language therapy, dental and psychosocial treatment) to coincide with the child's physical, cognitive, dental, and psychosocial development (Bowers et al., 1987; Gould, 1990). The parameters of care emphasize the need for the team of cleft specialists to organize for maximum long-term patient benefit, taking into account the child's growth intervals and levels of need in the individual's life.
Whenever surgery is contemplated for the reconstruction of CLP deformities, the benefit-to-risk (and -cost) ratio should be considered (Leonard et al., 1991; Strauss, 1994). Windows of opportunity may exist for maximum advantage (improved benefit-to-risk ratio) at different stages in the patient's growth and development. The goal of the CLP surgeon, orthodontist, speech therapist, and team is to work with the family, carry out periodic reassessments, and make suggestions about the timing and sequencing of care to ensure longterm benefits and to minimize complications and costs (Cohen et al., 1995).
The child born with either a complete unilateral or bilateral CLP (UCLP or BCLP, respectively) or cleft of the palate only (ICP) will face a series of hurdles related to speech, occlusion, facial appearance, and self-development. Reviewing the basic decision-making process of treatment options prospectively provides a reconstructive outline for the family and team members.
Robin Sequence
The French stomatologist Pierre Robin is best known for his description of an anomaly consisting of micrognathia with glossoptosis, CP, and respiratory obstruction (Jeresaty et al., 1969; Perlman and Robin, 1992; Randall et al, 1965; Robin, 1923, 1934) (Fig. 26.1), but the condition had been described earlier by St. Hilaire in 1822 (Dennison, 1965), Fairbairn (1846), and Shukowsky (1911). Birth prevalence estimates of Robin sequence have ranged from 1/200 to 1/30,000 (Bush and Williams, 1983; Carroll et al., 1971; Cohen, 1976). Definitions of this sequence of events also vary, making it difficult to obtain a more precise estimate of the birth prevalence and the ratio of syndromes said to be associated with the Robin sequence (Cohen, 1997). Cohen (1997) indicated that the clinical data are most consistent with etiologic and pathogenetic heterogeneity (Stoll et al., 1992). The most common genetic syndrome associated with Robin sequence is Stickler's syndrome (Turner, 1974). Prompt ophthalmologic assessment of the newborn with Stickler's syndrome is required to detect a myopia because blindness, resulting from retinal detachment, is associated with this syndrome (Turner, 1974; Schreiner et al., 1973; Smith and Stowe, 1961).
|
|
|
FIG. 26.1. A child born with Robin sequence consisting of micrognathia with glossoptosis, clefting the secondary palate, and a degree of respiratory distress. A: Profile view indicating micrognathia. B:Profile view of three-dimensional craniofacial computed tomographic reconstruction indicating micrognathia but with all of the components of the jaw present. For this child, the small mandible is the result of deforming forces during fetal development rather than of a malformation. Catch-up growth of the mandible is anticipated during childhood. (From Posnick, 2000a, with permission.) |
In animal models, intrauterine mandibular constraint with secondary failure of the tongue to descend and resultant CP has been described (Cocke, 1966; Edwards and Newall, 1985). Some instances of Robin sequence have been associated with oligohydramnios. It is thought that reduced amniotic fluid results in compression of the fetal chin against the sternum, restricting mandibular growth and impacting the elevated tongue between the palatal shelves (Poswillo, 1968; Rintala et al., 1984). This deformational cause of Robin sequence has been supported by several authors (Beers and Pruzansky, 1955). Pruzansky (1969) and Pruzansky and Richmond (1954) have shown that mandibular catch-up growth is likely to result in a normal profile by 4 to 6 years of age, when the cause of micrognathia is deformation rather than malformation. Hanson and Smith (1975) found specific syndromes in 25% of their Robin sequence patients, multiple anomalies but no specific syndrome in 35%, and isolated Robin sequence in the remaining 40%. A diversity of specific syndromes and associated malformations have been reported (Bezirdjian and Szucs, 1989; Bruce and Winship, 1993; Carey et al., 1982; Chitayat et al., 1991; Dykes et al., 1985; Glander and Cisneros, 1992; Robinow et al., 1986; Schimke et al., 1993; Schrander-Stumpel et al., 1991; Shprintzen, 1992).
Caouette-Laberge and co-workers (1994) reviewed all children admitted to Montreal Children's Hospital between 1964 and 1991 with the diagnosis of Robin sequence. Each child was placed into one of three groups according to the severity of symptoms: group I comprised children with adequate respiration in the prone position and bottle-feeding (n = 56, 44.8%), group II had adequate respiration in the prone position but feeding difficulties requiring gavage feeding (n = 40, 32%), group III consisted of children with respiratory distress requiring endotracheal intubation and gavage feeding (n = 29, 23.2%). Interestingly, 17 children (13.6%) died during the first year of life. The mortality rate increased with the severity of symptoms (breathing and swallowing), associated anomalies, and the prematurity of the newborn. Among the 108 survivors in the study, 25 presented with psychomotor impairment (23.1%).
The results of Caouette-Laberge and colleagues (1994) contrasts somewhat with those of Lehman and associates (1995). The latter reviewed a consecutive series of Robin sequence newborns presenting over an 18-year period (1972-1990) to their tertiary care pediatric center located in the midwestern United States. Thirty-six patients were included in this study. Only two infants required a tracheostomy, and 34 patients underwent CP repair. At follow-up several years later, only 17.4% of the repaired CP patients required a secondary pharyngoplasty and 11.8% had palatal fistula. No deaths were reported. The discrepancy in these two studies likely reflects differences in referral patterns to each hospital center. Other authors have reported various airway difficulties and have recommended a variety of treatment protocols (Abramson et al., 1997; Argamaso, 1992; Frohberg and Lange, 1993; James and Ma, 1997; LeBlanc and Golding-Kushner, 1992; Moos, 1997; Moyson, 1961; Sher, 1992).
Cleft Lip Repair
A cleft that occurs through at least the lip and alveolus (primary palate) produces distortions in all tissue layers, including skin, muscle, cartilage, mucous membranes, teeth, and bone. With repair of the UCL, e.g., the surgeon is expected to create a structure directly adjacent to its normal mirror image located in the most conspicuous area of the human body (Figs. 26.2,26.3). There are many reasons for the observed differences in the aesthetic results of the repaired CL. Surgeons vary in their ability to achieve a symmetrical and proportionate lip repair. Furthermore, there is a wide variety of presenting cleft malformations and potentials for healing. Although clefts usually follow a pattern, some are narrow while others are wide. There are differences in the severity of distortion of the cupid's bow in UCL and in the amount of philtrum to work with in BCL (Latham, 1993; Mulliken et al., 1993) (Figs. 26.4,26.5). It is an advantage for the surgeon to have experience in CLP care and a broad range of techniques from which to choose.
Timing
Cleft lip repair is generally carried out when the child is 2 to 3 months of age (Thompson, 1912). The general rule is to proceed when the child is approximately 10 weeks of age, weighs 10 Ib, and has achieved a serum hemoglobin of 10 mg/ml. These guidelines have stood the test of time and, in general, place the child at reduced anesthetic risk, ensure successful wound healing, and allow enough time to determine if other malformations are present and to establish comfortable feeding and airway routines for the child and parents (Marsh, 1996).
Some surgeons and cleft teams have advocated other protocols, including “immediate” repair of the cleft, just after birth and prior to discharge from the newborn nursery (Van Boven et al., 1993). Their rationale for doing so is twofold: first, to take advantage of the benefits of “fetal-like” wound healing and, second, to avoid any psychosocial trauma to the parents of having to live with their baby with an unrepaired CL (Marsh, 1996). Unfortunately, the desired long-term facial aesthetic advantages of “neonatal” lip repair with reduced scarring have not been realized (Longaker et al., 1992; Sullivan et al., 1996). Furthermore, studies have failed to show improved bonding between the child and mother when immediate lip repair is performed (Field and Vega-Lahr, 1984). It is therefore difficult to justify the increased anesthetic and surgical risks of neonatal surgery (Eaton et al., 1994).
Techniques
Placing tape or an elastic band across the segmented lip or cheeks to encourage soft tissue lip alignment and alveolar segment remodeling has been performed in preparation for lip repair for centuries. One of the earliest proponents of this procedure was Gaspare Tagliacocci, who in the 16th century described the use of a linen splint with “agglutination” material, under which the approximated prepared (CL) edges could heal with less tension (Gnudi and Webster, 1950). Poole and Farnworth (1994) described their experience with “lip taping” to approximate the segments prior to repair. It is their belief that the soft tissue approximation and bony alignment achieved by lip taping can be as effective as lip adhesion for those who believe that alignment of the lip and alveolar segments prior to repair provides long-term advantages to lip and nose aesthetics.
Controversy continues as to whether it is advantageous to use passive or more aggressive presurgical orthopedic regimens and, if so, to what extent (Ross and MacNamera, 1994; Shaw and Semb, 1990). The purpose of these techniques is to improve the alignment of the maxillary segments and overlying soft tissues prior to lip repair. Ross and MacNamara (1994) reviewed the long-term CL and nasal soft tissue aesthetics in two groups of teenagers who were born with BCLP. The first group underwent presurgical orthopedic procedures (lip taping) prior to lip repair, and the second group did not. When facial photographs were judged by double-blinded impartial observers, no statistical difference in lip or nasal aesthetics between the two groups was found.
|
|
|
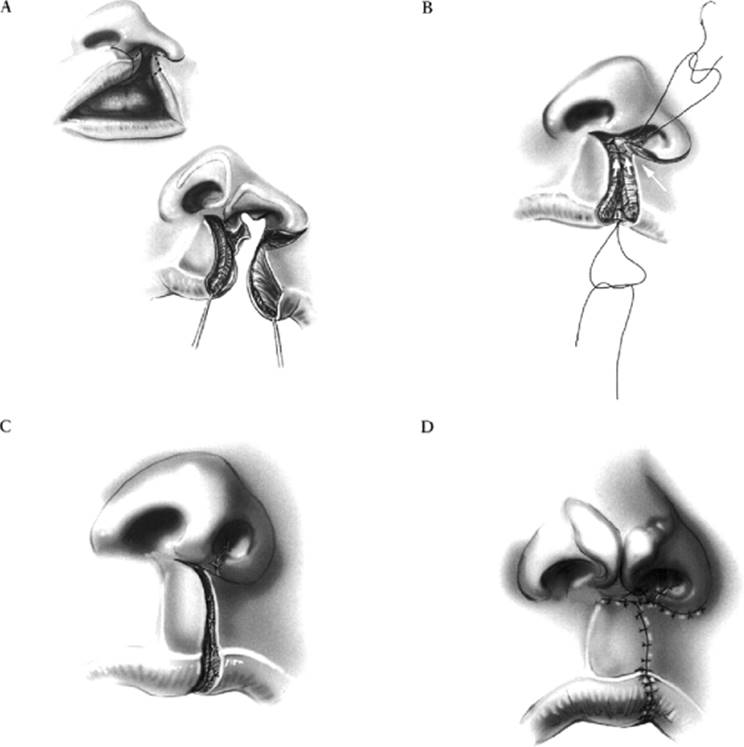
FIG. 26.2. Illustration of the basic components of the Millard rotation and advanced flap technique used by the authors for unilateral cleft lip repair. A: The rotation flap (greater lip segment) and the advancement flap (lesser lip segment) are outlined. Flaps are incised, redundant tissue is excised, and initial flap dissection is completed. The three tissue layers (skin, orbicularis oris muscle, and underlying mucosa) are separated. B: The orbicularis oris muscle, having been released from its abnormal bony attachments, is sutured across the midline and to the base of the columella. The underlying oral mucosa is sutured with reestablishment of a normal intraoral vestibule. C: Once the orbicularis oris muscle has been sutured, the cutaneous flaps approximate without tension for wound closure. The floor of the nose flaps are sutured to establish the nasal sill. D: Precise approximation of anatomic landmarks with fine sutures is undertaken to align the philtral columns, ver-milion-cutaneous junction, and vermilion-mucosa/junction. (From Posnick, 2000a, with permission.) |
A lip adhesion is a partial CL repair that converts a wide, complete cleft into an incomplete one (Millard, 1976a; Randall, 1965). Advocates of lip adhesion suggest that it be used as a first stage only for those patients with very wide clefts where a primary repair might not be possible. A lip adhesion is said to recreate the natural compression forces and can be expected to narrow a wide cleft and to encourage the alignment of the alveolar arches. Those who advocate a lip adhesion usually carry it out when the child is 3 to 4 months of age (Randall, 1965). They then allow 3 to 6 months for the scar tissue of the lip to soften before undertaking definitive lip repair. Lip adhesion has the disadvantage of adding a second operation with additional anesthetic and hospital recovery. Potential complications associated with lip adhesion include wound dehiscence and excess scar formation, which may leave the tissue less supple for the definitive lip repair.
|
|
|
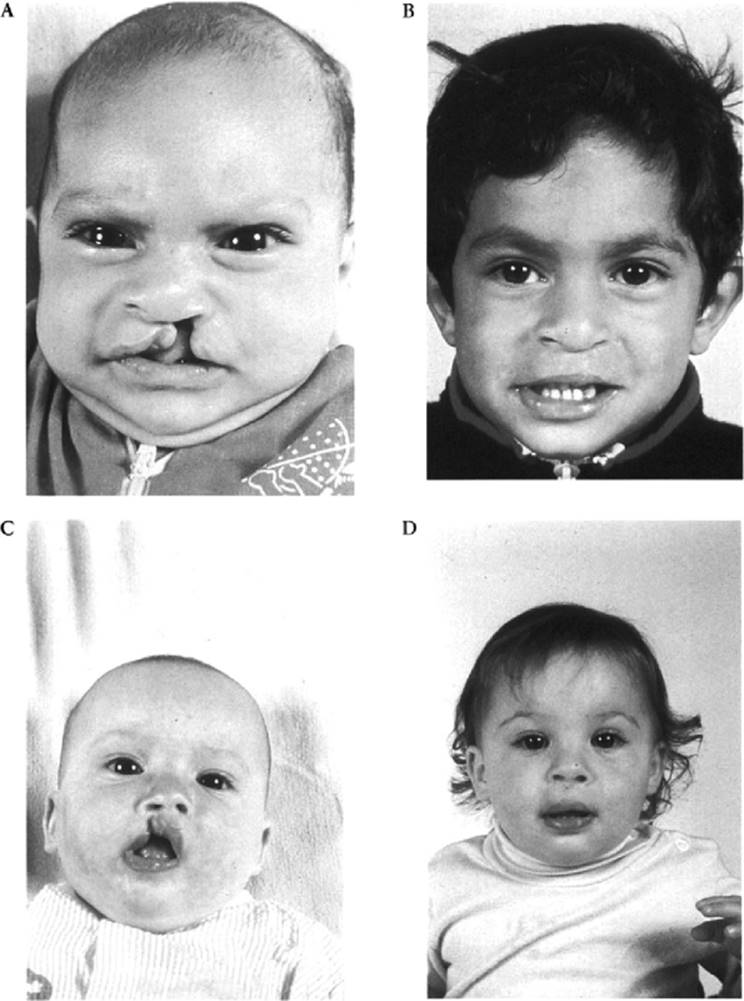
FIG. 26.3. A spectrum of children born with varied degrees of unilateral cleft lip/alveolus and palate (UCLP) before and after initial repairs. A: Child with complete UCLP before surgery. B: Child 2 years later. C: child with incomplete UCL before surgery, D: Child 6 months later. (From Posnick, 2000a, with permission.) |
|
|
|
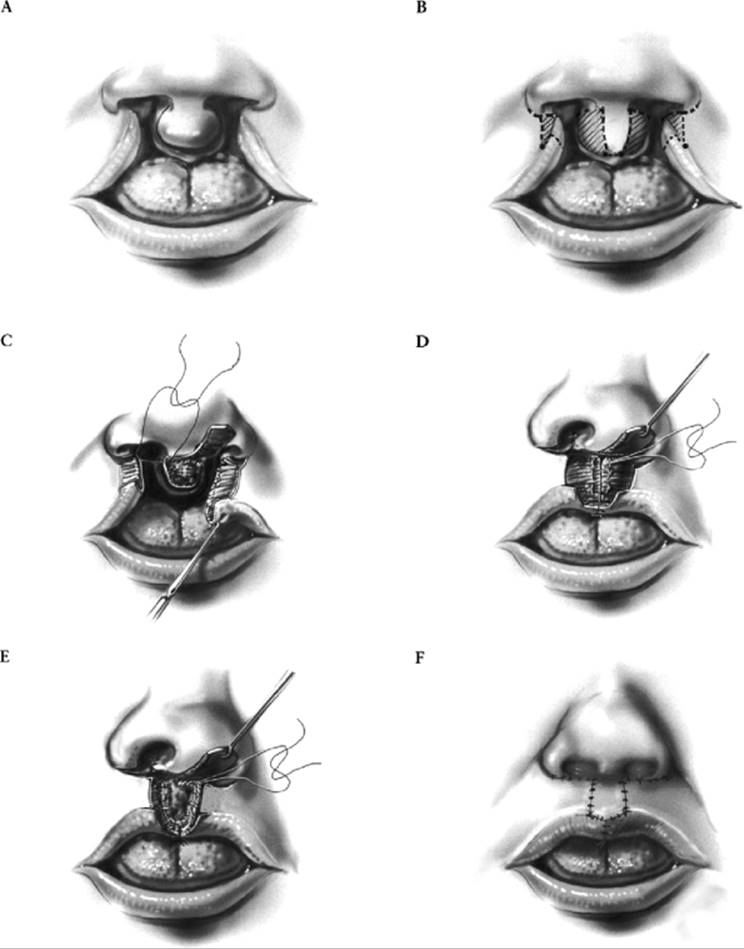
FIG. 26.4. Illustration of the basic components of the Millard technique used by the authors for bilateral cleft lip repair. A: Typical complete bilateral cleft lip deformity. B: Incisions for bilateral cleft lip repair are indicated (dotted lines), with tissue to be excised (diagonal lines). C: The philtral (skin) flap has been elevated, with circulation maintained on its columellar base. Lateral lip flaps have been elevated with addition dissection of lateral vermilion mucosal flaps to be used for reconstruction of the central red lip region. The orbicularis oris muscle has been dissected free of its abnormal bony attachments. D: The anterior portion of the nasal floor has been reconstructed by suturing of the medial and lateral nasal floor flaps. The intraoral mucosa and oral vestibule have been carefully sutured with excision of redundant red lip from the philtral flap. E: The orbicularis oris muscle is approximated across the midline and sutured to the columellar base. F: The vermilion-cutaneous junction is sutured on each side, and the vermilion-mucosal junction is aligned in the midline by approximating the lateral red lip flaps. Lateral cutaneous flaps are advanced and sutured to the columellar base on each side. Philtral columns and nasal sills are sutured. (From Posnick, 2000a, with permission.) |
|
|
|
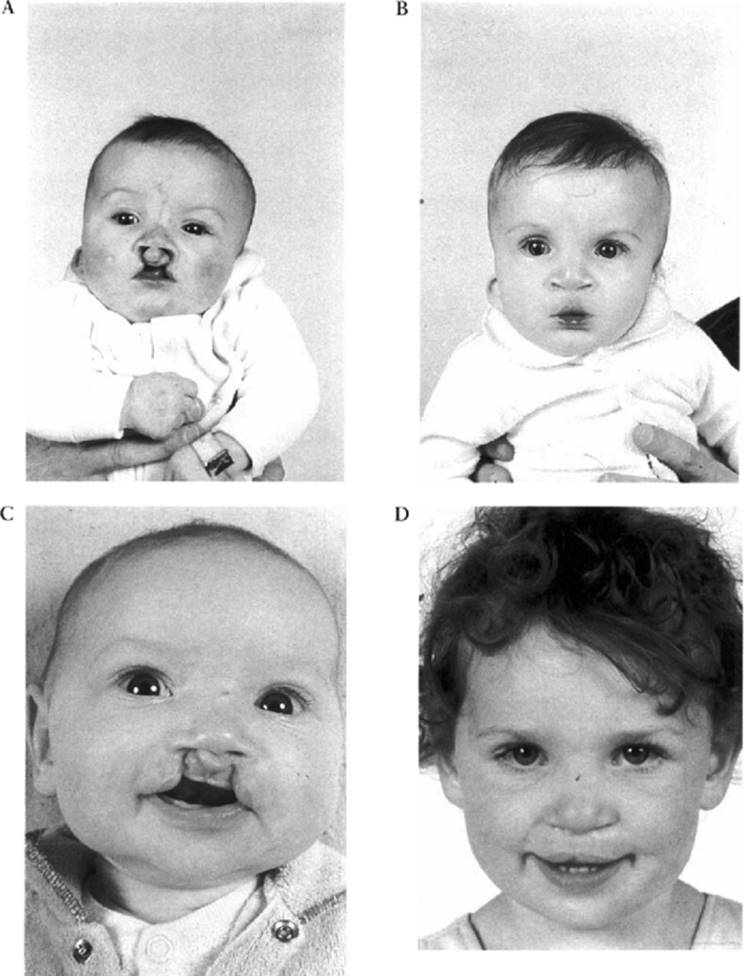
FIG. 26.5. A spectrum of children born with bilateral cleft lip/alveolus and palate (BCLP) before and after initial repairs. A: Child born with multiple malformations, including complete BCLP, before surgery. B: Child 8 months later. C: Child born with BCLP before surgery. D: Child 2 years later. (From Posnick, 2000a, with permission.) |
Every CL surgeon has a favorite technique for repairing the unilateral and bilateral cleft types (Abbe, 1898; Brauer, 1985; Davies, 1966; LeMesurier, 1955; McComb, 1985; Millard, 1960, 1964, 1976b; Mohler, 1987; Skoog, 1969). Refinements in lip repair were presented by LeMesurier (1955), whose approach gave advantages over the previously advocated straight line closure. This was followed by the Tennison (1952) triangular flap technique, the Skoog (1969) high triangular insertion of the lateral lip segment method, and the modifications introduced by Randall (1990) and Brauer (1985). Finally, in the early 1950s, Millard, realized that the popular triangular flap technique often aligned the peak of the cupid's bow in its normal position but violated the natural lines of the philtrum dimple (Millard, 1957). Rather than merely rotating the lower third of the central lip, he conceptualized the high release and subsequent rotation of the whole medial lip segment, thereby returning it to its normal position. The lateral lip segment was then prepared and advanced to meet the leading edge of the rotated medial lip segment. Through the years, Millard and others have added various refinements to his initial technique (Millard, 1960, 1964, 1976a,b). Today, the Millard rotation and advancement flap technique remains the gold standard by which other lip repairs are judged.
Millard's method of UCL repair (the rotation and advancement flap technique) is the most frequently employed method of CL repair in the United States and throughout the world (Fig. 26.2). The rotation and advancement flap repair can be applied to a wide variety of UCL deformities, with flexibility and consistency of results. Other options for CL repair remain the straightline closure (Rose, 1976), the Tennison-Randall triangular flap technique (Randall, 1990), and the LeMesurier (1955) approach. Whichever basic technique is used, the goal is to achieve a symmetrical and proportionate upper lip in repose with dynamic mimetic function.
In unilateral clefts, the alar cartilage is splayed out (laterally) and rotated caudally (downward). The lower border of the lateral crus produces an oblique ridge in the nasal vestibule and the nostril rim droops. The alar dome is pulled laterally and downward, causing irregularity of the nasal tip and shortening of the columella on the cleft side.
At the time of primary CL repair, if the nostril on the cleft side is repositioned without lifting the alar cartilage, a curve is further accentuated in the nostril that may result in the typical flare of the CL nose. Lifting the slumped alar cartilage is thought to be a useful step in limiting this problem. McComb considers the essential features of primary CL nasal repair to be wide undermining of the nasal skin envelope (separating the lower lateral cartilage from the overlying skin) on the side of the cleft, avoidance of incisions in the nasal lining (to limit nostril cicatrization), and placement of sutures to bolster the lower lateral cartilage on the cleft side into its preferred position (McComb, 1985, 1990, 1994; McComb and Coghlan, 1996). The details of surgical technique should be expected to differ from surgeon to surgeon (Takato et al., 1995a; Trier, 1995).
Key elements unique to BCL repair include repairing both cleft sides at one operative sitting, achieving a successful orbicularis oris muscle repair, bringing in adequate vermilion and mucosa from the lateral lip segments to reconstruct the central red lip, reconstructing a relatively small philtrum as it tends to stretch and expand with growth, and restoring a sufficient inner lip vestibule (Figs. 26.4,26.5). Millard's concepts of preserving tissue led him to suggest the “banking of forked flaps” in each nasal sill, to be used later to lengthen the columella in the BCLP patient. It has been the experience of many that, in the short run, the banked forked flaps may obstruct the infant's nasal breathing. In the long run, the flaps contract and are unlikely to provide useful tissue for later nasal reconstruction.
Mulliken (1995) has advanced our understanding of the BCLP patient's nasal deformities and has added several key refinements to BCL repair. He believes that “the bilateral cleft lip nasal deformity is both intrinsic (a primary malformation deficiency) and deformational (extrinsic, secondary to the surgeon's well-intended closure of the lip).” He states that the “malformed alar cartilages are rotated caudally and subluxed from their normal position overlying the upper lateral cartilage. The lower lateral cartilages and alar soft tissues are hypoplastic and widely separated.” Unlike the majority, he believes that early repositioning of the alar cartilage under direct vision through an open technique at the time of primary lip repair is essential to correct BCL nasal deformity. He does not believe that the columella is intrinsically deficient and recommends against lengthening procedures. While the final word is not in, we prefer the McComb approach to nasal reconstruction at the time of lip repair and recommend against columellar (skin) lengthening procedures.
Cleft Palate Repair
While the optimal age of the patient and method of closure of the CP remain unresolved, available information suggests a limited range of acceptable options for timing and technique. A surgical objective of the primary repair is to reconstruct the hard and soft palate with closure of all existing oronasal communication from the incisal foramen back through the uvula. Another goal is the creation of a dynamic soft palate, capable of interfacing with the lateral and posterior pharyngeal walls to achieve sufficient velopharyngeal (VP) closure and, thus, “normal” speech (Broomhead, 1957; Maher, 1977; Ross and Johnstone, 1972).
Timing
Ideally, a decision about the appropriate age for palatal repair should be based on the child's stage of phonemic development or articulation age (language or speech age), as opposed to chronologic age (Copeland, 1990; Dalston, 1992; Denk and Magee, 1996; Evans and Renfrew, 1974; Haapanen and Rantala, 1992; Kemp-Fincham et al., 1990; Randall et al., 1983; Riski and DeLong, 1984). A child with either an unrepaired palate or an inadequately closed palate who approaches a level of phonemic development (articulation age) that requires VP competence will be left vulnerable to the development of compensatory articulations. These maladaptive speech patterns interfere with intelligibility and may be difficult to eliminate once developed (Blijdorp and Muller, 1984; Chapman and Hardin, 1992; Grobbelaar et al., 1995; Harding and Campbell, 1989; Herman, 1995; Riski, 1996; Rohrich et al., 1996).
Most studies indicate that the nonsyndromic normally developing infant who is without hearing impairment or cognitive delay will develop significantly fewer compensatory articulations and maladaptive speech patterns if the palate is repaired before 2 years of age. Furthermore, Dorf and Curtin (1982) reported startlingly different speech results in a group of 21 children whose clefts were closed before 12 months of age compared with a group of 59 children who underwent palatal repair after 12 months of age. In their study, speech was assessed only for the presence or absence of compensatory articulations. Only 10% of children in the early-repair group developed these patterns compared with 86% in the late-repair group. In a later follow-up study of an expanded series of patients, Dorf and Curtin (1990) reported an even greater discrepancy in speech performance between the early-and laterepair groups. The independent studies of Peterson- Falzone (1990,1995) and Dalston (1992) failed to confirm the Dorf and Curtin findings of 12 months being a watershed age for CP repair. While these authors did find an overall prevalence of compensatory articulations in their CP study group similar to that found by Dorf and Curtin, there were no statistical significances when the CP was closed at or before 12 months vs. between 12 and 24 months of age. The two studies did confirm that repair of the palate after 24 months resulted in a much higher prevalence of compensatory articulations than repair at less than 24 months of age. Unfortunately, none of the CP “timing” studies to date have controlled for the variable language or speech age. Riski (1996) and Riski and DeLong (1984) believe that children who develop speech early may be more prone to incorporate maladaptive misarticulations since they attempt pressure consonants even before palatal repair. For most children, CP repair to close down the oronasal opening and establish a competent VP sphincter by 9 to 12 months of age minimizes the development of irreversible pathologic compensatory speech patterns as well as the surgical risks and potential for growth restriction of the upper jaw (Dorf and Curtin, 1990; Devlin, 1990).
Techniques
Options for repositioning the displaced cleft maxillary segments prior to CP repair include no preoperative orthopedic procedures (no active segment repositioning), a conservative preoperative orthopedic treatment (lip taping and a passive palatal plate), or use of the Latham presurgical orthopedic appliance (Bitter, 1992; Georgiade and Latham, 1975; Millard and Latham, 1990; Nguyen and Sullivan, 1993; Pruzansky, 1955, 1964; Ross and MacNamera, 1994). Despite several decades of experience with the Latham appliance and other less aggressive preoperative orthopedic options, no convincing studies have demonstrated long-term comparative benefits in lip or nose aesthetics, arch alignment, or occlusion (Millard, 1980). The potential for morbidity when aggressive preoperative orthopedic options are selected must also be considered.
Berkowitz (1996) compared conservative presurgical orthopedic treatment in complete BCLP patients to use of the Millard-Latham (M-L) method. In the conservatively treated group, external elastic traction was sometimes used to apply gentle pressure to the premaxilla prior to surgical lip closure. The M-L method involves mechanical traction of the protruded premaxilla using the pinned Latham palatal appliances followed by a Millard gingivoperiosteoplasty. In both study groups, the palatal cleft (hard and soft) was closed between 18 and 30 months of age using a modified Langenbeck procedure.
As part of the Berkowitz (1996) study, the children who underwent each regimen were followed similarly into the early teenage years. The conservative presurgical orthopedic group underwent secondary alveolar bone grafting between the ages of 6 and 9 years. Ninety percent of the children in the M-L group demonstrated bony bridging across the alveolar cleft with partial or complete closure of the lateral incisor gap. By 10 to 12 years of age, only two of the 29 patients in the conservatively treated group (6%) demonstrated an anterior crossbite suggestive of maxillary retrusion. All of the patients that underwent the M-L method demonstrated maxillary retrusion by 9 years of age, indicative of maxillary hypoplasia. The results of Berkowitz (1996) confirm that a major disadvantage of using the latham palatal appliance followed by the Millard gingivoperiosteoplasty technique for palatal repair is maxillary growth restriction, with a need for orthognathic surgery in the teenage years anticipated in the majority of patients.
CP centers have advocated earlier protocols for the timing of initial repair (Copeland, 1990; Denk and Magee, 1996). When contemplating early repair of the palate (before 6 months of age), three additional factors are important to consider (Bardach and Salyer, 1991a; Hedrick et al., 1996). First, there is a known potential for maxillary or midfacial growth restriction resulting from surgery carried out in the immature maxilla (Copeland, 1990; Pruzansky, 1964; Bishara, 1973; Canady et al., 1997; Derijcke et al., 1994; Heidbuchel et al., 1994; Kramer et al., 1996; McCance et al., 1993; Motohashi et al., 1994; Roberg and Koblin, 1973; Semb, 1991; Shaw et al., 1992; Trotman and Ross, 1993). Second, the need for blood transfusion at the time of palatal repair and the potential for airway complications are inherently greater when the procedure is carried out at a very young age. Third, for the general CP population, there are no known long-term functional advantages (speech, airway, dental) to carrying out palatal repair before 9 to 12 months of age.
There are three basic surgical options for palatal repair: the modified Langenbeck procedure (von Langenbeck, 1861), the two-flap Bardach technique (Bardach and Salyer, 1991a; Bardach and Nosal, 1987; Bardach et al., 1990), and the Furlow Z-plasty (Furlow, 1986, 1992, 1997; Horswell et al., 1993; Upton, 1993). There are no confirmed inherent advantages of one method over the other, and each has theoretical benefits and technical limitations which the surgeon must understand and master. Other methods of CP repair have been advocated over the years (Kilner, 1937, 1958; Millard et al., 1970; Perko, 1979; Schweckendiek, 1978; Skoog, 1965; Veau, 1931; Wardill, 1928, 1937; Wood et al., 1997). Whichever technique the surgeon prefers, the objectives of primary repair remain the same: achievement of an intact palate (from the anterior incisive foramen through the uvula) without oronasal communication and creation of a dynamic soft palate that is able to achieve VP closure during normal phonation (Abyholm, 1979; Amaratunga, 1988; Emory et al., 1997; Posnick and Getz, 1987). Whenever possible, complete soft tissue closure over the hard palate should be achieved in the operating room without leaving raw lateral bone surfaces open to heal with granulation tissue formation. Healing of the hard palate by secondary intention likely results in increased palatal scarring, maxillary growth restrictions, and the need for orthognathic surgery in the teenage years.
Another often discussed issue related to CP repair is whether to complete a one- or two-stage palatoplasty. The aim of the one-stage palatoplasty (whether using the Langenbeck method, the Bardach two-flap technique, or the Furlow Z-plasty) is straightforward: complete closure of the palatal cleft in one operation, creating adequate conditions for normal speech. There remain some cleft surgeons who continue to advocate a two-stage palatoplasty, in which the velum (soft palate) is repaired first, leaving the hard palate unrepaired for a period ranging from several months to several years. Advocates of the two-stage palatoplasty, a concept presented by Schweckendiek in the late 1930s, believe that this approach achieves two goals simultaneously: creation of a functional soft palate and unrestricted maxillary growth. Advocates of the one-stage palatoplasty believe their approach to be more efficient as it obviates the need for a second palatal procedure and prevents the need to constantly wear a palatal plate, which must be frequently modified to ensure satisfactory speech. Many prominent CP speech pathologists (Morris, Shprintzen, Witzel, and others) report more favorable speech outcomes following the one-stage palatoplasty than following the two-stage approach (Witzel et al., 1984). Interestingly, studies have not documented advantages in maxillary growth with the two-stage technique. The one-stage palatoplasty remains the most frequently performed technique for CP repair throughout the world (Bardach and Salyer, 199la; von Langenbeck, 1861; Bardach et al., 1990; Furlow, 1986, 1992, 1997; Horswell et al., 1993; Upton, 1993).
The basic principles of the Bardach two-flap palatoplasty technique include (1) complete closure of the entire palatal cleft as a one-stage procedure; (2) two-layer closure (nasal and oral layers) of the hard palate and three-layer closure (nasal mucosa, soft palatal muscles, and oral mucosa) of the soft palate; (3) release of the muscles of the soft palate from the posterior edge of the hard palate and from the periosteum on the nasal side, allowing creation of a more physiologic soft palate muscle sling; and (4) in wide clefts, when an area of bare bone must be left exposed on the hard palate, covering of the open areas with Avitene (microfibrillar collagen) Hemostat to limit healing time and scar formation (Bardach and Salyer, 199la; Bardach and Nosal, 1987; Bardach et al., 1990) (Fig. 26.6).
The Furlow Z-plasty is also a one-stage palatoplasty (Furlow, 1986, 1992, 1997; Horswell et al., 1993). The Furlow technique provides for closure of the hard palate in one procedure without push-back or lateral relaxing incisions and repair of the soft palate with mirror-image Z-plasties to retroposition and overlap the soft palatal muscles, forming a muscle sling (Fig. 26.7). Furlow believes that if there is some lengthening of the soft palate it is by the Z-plasties, which do not take tissue from the hard palate. If the Z-plasties in fact lengthen the palate, they do so at the expense of palatal tissue, which would otherwise be used for approximation at the junction of the hard and soft palate. This may be the reason for the reported increased incidence of oronasal fistulae when using the Furlow technique.
|
|
|
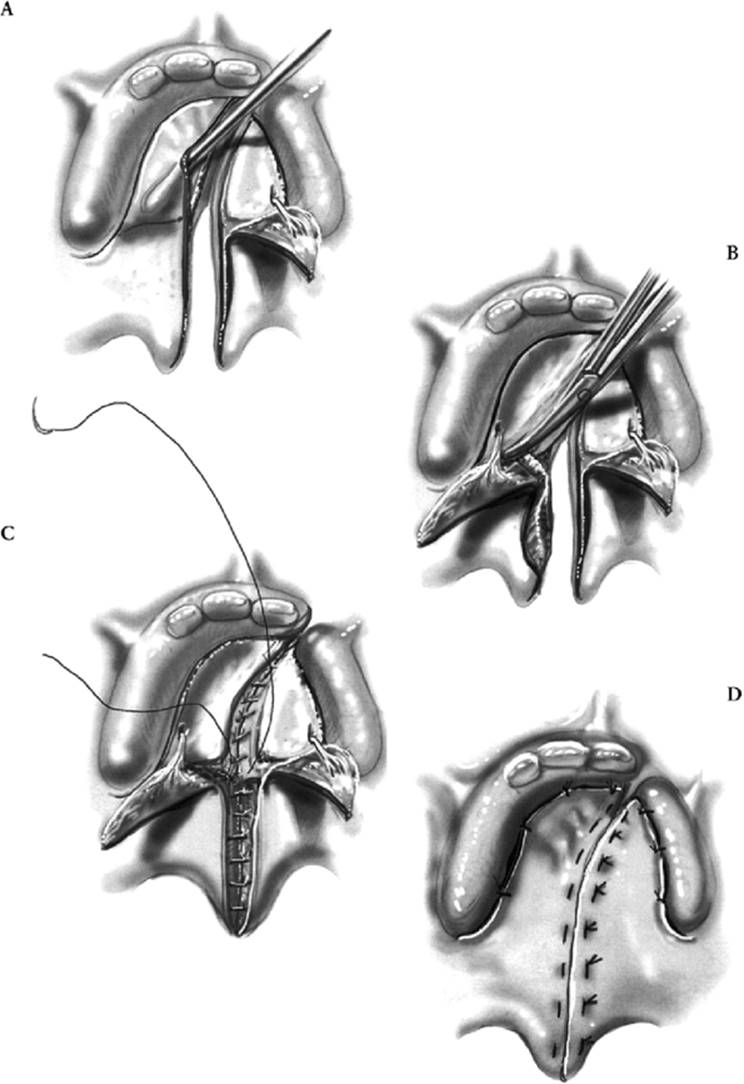
FIG. 26.6. Illustration of the basic technique of the Bardach two-flap palatal repair. A: Oral and nasal mucosae are incised and separated from the uvula forward to the incisal foramen on each side of the cleft. A second incision is completed on each palatal shelf to allow for flap elevation. The second set of incisions is from the anterior extent of the previous incision, continuing posteriorly at the junction of the palatal mucosa and alveolar mucosa. Relaxing incisions are made behind each maxillary tuberosity. Each full-thickness mucoperiosteal flap is elevated, with care taken to preserve the greater palatine vascular pedicle within each flap. B: With each full-thickness flap elevated and the greater palatine vessels preserved, the soft palatal musculature is taken off its abnormal attachments to the posterior palatine bones. C: Nasal mucosa is sutured for a water-tight closure from the incisal foramen to the junction of the hard and soft palate. The nasal side of the soft palate is then closed from the uvula forward to the junction of the hard and soft palate. The soft palatal musculature is also sutured across the midline. D: Oral mucosa is closed from the uvula forward to the incisal foramen. Finally, each mucoperiosteal flap is sutured back to its original location, limiting exposed bone whenever feasible. (From Posnick, 2000a, with permission.) |
|
|
|
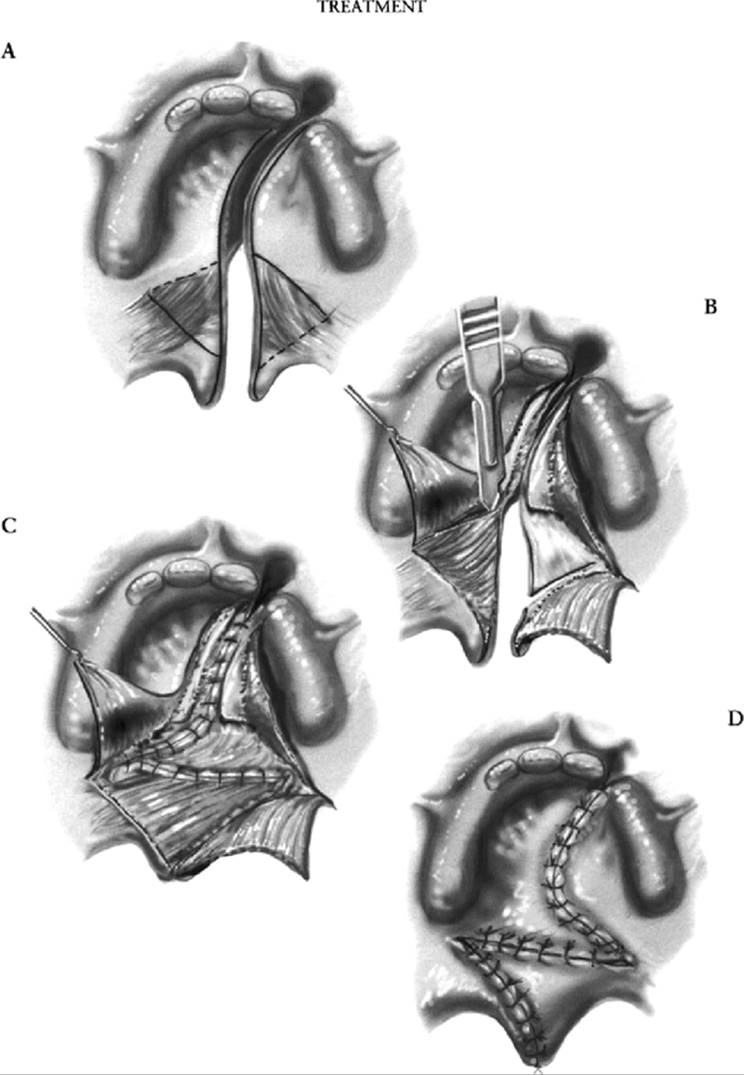
FIG. 26.7. Illustration of the basic technique of the Furlow double-opposing Z-plasty palatal repair. A: Location of planned incisions. B: Flaps are elevated. C: Nasal side closure is achieved using opposing Z-plasty flaps in the soft palate and nasal flap closure over the hard palate. D: Oral side closure of hard and soft palate is completed. (From Posnick, 2000a, with permission.) |
The Langenbeck palatoplasty calls for elevation of two bipedicled mucoperiosteal flaps, one off of each palatal shelf (von Langenbeck, 1861) (Fig. 26.8). The theoretical advantage is the maintenance of an anterior pedicle for improved flap circulation. Unfortunately, with maintenance of the anterior pedicle, direct visualization for nasal side closure is limited. In addition, flap elevation and relaxation for advancement to the midline to close the cleft at the junction of the hard and soft palate may be difficult.
|
|
|
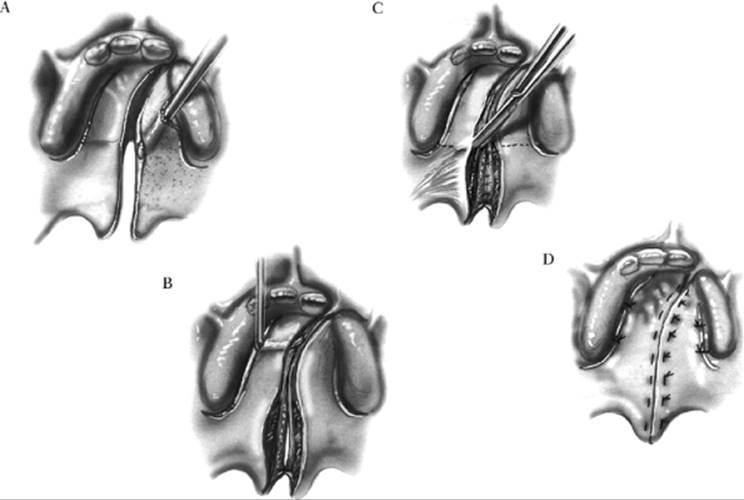
FIG. 26.8. Illustration of the basic technique of Langenbeck's cleft palate repair. A, B: Incisions and initial elevation of bipedicled, full-thickness mucoperiosteal palatal flaps. C: After separation of nasal and oral mucosae, nasal side closure is achieved from the incisal foramen back to the uvula. Release of the soft palatal musculature off of its abnormal attachment to the palatine bones is completed, and the soft palatal musculature is approximated in the midline with sutures. D: Oral side closure is completed with interrupted sutures from the incisal foramen back through the uvula. Laterally, the palatal flaps are sutured back to their origin. This prevents exposed bone, which would then have to heal by secondary intention. (From Posnick, 2000a, with permission.) |
Secondary Cleft Palate Procedures for Management of Velopharyngeal Dysfunction
Velopharyngeal dysfunction (VPD) is one of the most complex secondary problems related to CP treatment. It affects the ability of the patient to communicate coherently with others and may be considered more debilitating than many other secondary lip, nose, and dental deformities that primarily affect physical appearance.
When carrying out initial CP repair, the surgeon will try to restore the palatal anatomy for optimal VP closure and eventual normal speech production (Cutting et al., 1995; Morris, 1973). Unfortunately, present knowledge does not allow prediction of the eventual speech outcome in individual patients after initial palatal repair (Ainoda et al., 1985; Hartzel et al., 1994; Morris et al., 1989; Peterson-Falzone, 1995; Riski, 1995). It must be remembered that all aspects of VP valve function are not based solely on the palate. The CP itself is only one factor contributing to VP function, and even this single aspect cannot be managed optimally in every patient because of the varying degrees of severity of cleft and hypoplasia as well as differences in surgical techniques used, surgeon expertise, and individual factors related to the local wound-healing process (McCance et al., 1993; Ren and Wang, 1993).
Timing
Additional surgical intervention is recommended after initial palatal repair when VP dysfunction is consistent and determined to be related to an anatomic problem (Henningsson and Isberg, 1986; Isberg and Henningsson, 1987; Lohmander-Agerskov et al., 1996). In patients 2.5 to 4 years of age, it is difficult for the surgeon, but occasionally possible for the speech and language pathologist, to draw definitive conclusions about VP function or dysfunction. Riski (1997a,b)believes that many children who suffer marked VP dysfunction after CP repair can be critically assessed at 3 years of age. According to Shprintzen and Bardach (1995a) and Shprintzen and Golding-Kushner et al., (1989), this judgment generally cannot be made until the child is 4 to 5 years of age. They specify several reasons for delaying surgery until this age, including the child's language and articulation development, the ability to accurately assess VP function, and patient compliance. All agree that preoperative diagnostic accuracy is critical to achieving a good clinical outcome. Secondary palatal surgery should not be planned until reliable and consistent assessment of the patient's speech is possible (Riski, 1997b; D'Antonio et al., 1989; Golding-Kushner et al., 1990; Siegel-Sardewitz and Shprintzen, 1986; Warren, 1975, 1994; Warren et al., 1994). Pharyngeal flap surgery is reportedly successful approximately 80% of the time when applied randomly to repaired CP patients with subjective hypernasality who have not undergone advanced preoperative diagnostic tests (i.e., nasopharyngoscopy or multiview videofluoroscopy) (Argamaso et al., 1994; Shprintzen et al., 1979). However, a success rate of 97% was reported when the same surgeons applied their operations based on the preoperative diagnostic information provided by nasendoscopy, multiview videofluoroscopy, and discussion with the evaluating speech therapist (Argamaso et al., 1994; Shprintzen et al., 1979). The major advantage of nasendoscopy is the ability to dynamically observe the internal anatomy of the nose, pharynx, and larynx in detail. Decisions regarding the advisability of surgery, the choice of operation, and treatment alternatives are influenced by observations of the VP valve and surrounding structures and are best made after discussion with the speech pathologist (Argamaso et al., 1994; Croft et al., 1981; Peat et al., 1994; Riski et al., 1984; Shprintzen, 1990; Shprintzen and Bardach, 1995b).
Techniques
Various pharyngoplasty techniques have been designed to improve VP function following initial CP repair (Bardach and Salyer, 1991b; Barone et al., 1994; Blocksma, 1963; Bluestone et al., 1968; Brauer et al., 1990; Chen et al., 1994; Denny et al., 1993; Graivier et al., 1992; Hogan, 1973; Jackson, 1990; Morris et al., 1995; Orticochea, 1968, 1984; Witt et al., 1995, 1997; Wolford et al., 1989). The basic goal of any pharyngoplasty is to allow complete VP sphincter closure with specific speech sounds, eliminating hypernasality. At present, there are only limited clinical data to support any one surgical technique as the optimal choice for a particular form of VP dysfunction (Riski, 1979; Riski et al., 1984, 1989, 1992a,b; Witt et al., 1997; Witzel et al., 1989). The basic techniques of pharyngoplasty include the inferiorly based pharyngeal flap, the superiorly based pharyngeal flap, the sphincter pharyngoplasty, and augmentation of the posterior pharyngeal wall.
The custom-designed, superiorly based pharyngeal flap remains the standard for the surgical resolution of VP dysfunction after initial palatal repair (Argamaso et al., 1994; Shprintzen et al., 1979) (Fig. 26.9). With the superiorly based flap technique, a long flap can be designed to ensure a tension-free insertion and fixation of the flap into a bed created in the soft palate. The width of the flap is varied to accommodate individual VP needs (Argamaso et al., 1994). Proper elevation of the pharyngeal flap to place its base at a level higher than the posterior edge of the soft palate is preferred, to avoid a downward pull on the soft palate. This problem is avoided with a superiorly based flap but occurs frequently when an inferiorly based flap is used. Randall and others in the 1970s (Randall et al., 1978) documented greater morbidity without improved speech outcomes when using the inferiorly based flap compared with the superiorly based flap. For this reason, the inferiorly based flap is rarely used. Using a tailored approach to the elevation and insertion of the superiorly based flap designed to accommodate individual patient needs, Argamaso and colleagues (1994) described effective resolution of VPI in 97% of their patients. Bardach and Salyer (1991b) reported the use of a superiorly based pharyngeal flap tailored according to preoperative objective findings and demonstrated a 95% success rate.
The so-called dynamic sphincter pharyngoplasty is another option (Jackson, 1990; Jackson and Silverton, 1977). Its aim is to substitute the two lateral ports that would be created by a superiorly based pharyngeal flap with one central port with improved VP valve function. This is achieved by elevating and inserting mucomuscular flaps into the lateral walls, to create a functional sphincter. The dynamic sphincteroplasty technique has no proven advantage over the superiorly based flap in the elimination of VP dysfunction but may be the preferred method to prevent the postoperative airway obstruction and mucus trapping sometimes seen with the latter (Croft et al., 1981; Brouilette et al., 1984; Caouette-Laberge et al., 1992; Gray, 1990; Guilleminault and Stoohs, 1990; Shprintzen et al., 1987; Sirois et al., 1994; Witt et al., 1996; Ysunza et al., 1993).
Augmentation of the posterior pharyngeal wall represents another option in the treatment of VPI recognized in the child after first-stage palatal repair. (Blocksma, 1963; Bluestone et al., 1968; Brauer 1990; Witt et al., 1997). When successful, this procedure moves the posterior pharyngeal wall forward so that the mobile but poorly functioning palate can more easily make contact with the posterior wall to prevent nasal air escape with certain speech sounds. Unfortunately, the ideal material to use for augmentation of the posterior pharyngeal wall has not been found. Homologous or autologous cartilage, Silastic implants, Teflon injections, and Dacron-wrapped silicone gel implants have been tried but without reliable long-term success. Outcome studies demonstrating the long-term efficacy of these augmentation techniques have not been forthcoming.
|
|
|
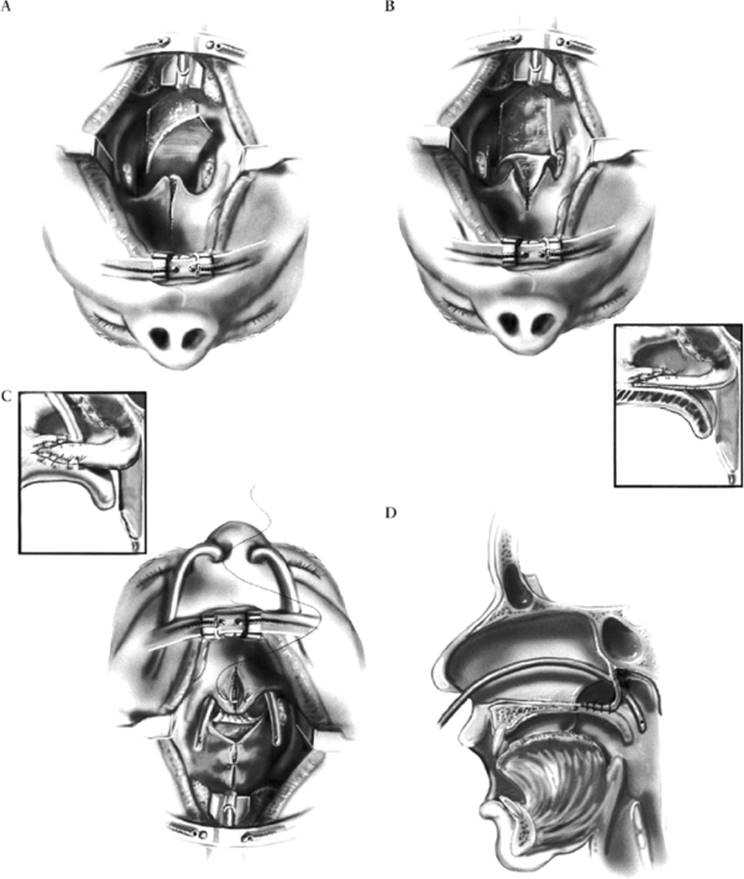
FIG. 26.9. Illustration of the basic technique of elevation and inset of a superiorly based pharyngeal flap for management of velopharyngeal insufficiency. A: Intraoperative view of soft palate and posterior pharyngeal wall with Dingman mouth gag in place. The soft palate is incised in the sagittal midline from the uvula forward to the junction of the hard and soft palate. The superiorly based pharyngeal flap is elevated off the prevertebral fascia. B: The superiorly based pharyngeal flap is inset to the soft palate and sutured to the nasal side of the soft palate with interrupted sutures. This is also demonstrated in the cross-sectional view (inset). C: The pharyngeal wall donor site is partially closed with 2-0 Vicryl interrupted sutures. Nasopharyngeal airways are placed through each lateral pharyngeal port for sizing and for postoperative airway support as needed. With the flap inset and the nasal side closed, the soft palatal musculature is further dissected and approximated as indicated. The oral side of the soft palate is then closed with interrupted sutures. A cross-sectional view (inset) demonstrates the separate oral and nasal side closure of the soft palate. D: Cross-sectional sagittal view of the face indicates the location of the nasopharyngeal airway in relationship to the soft palate and inset pharyngeal flap. (From Posnick, 2000a, with permission.) |
Witt and co-workers (1996) reported on the use of autogenous posterior pharyngeal wall augmentation using a “rolled superiorly based pharyngeal myomucosal flap.” This procedure was originally described by Wardill (1928). Witt and colleagues (1996) used this technique on a series of 14 consecutive patients who had VP dysfunction not responsive to speech therapy and a less than 20% coronal gap on VP nasendoscopy. All patients were evaluated preoperatively and 3 months postoperatively with recorded (audiovisual tape) perceptual, nasendoscopic, and fluoroscopic standardized speech and airway tests. Preoperatively, the majority of these patients had nasal turbulence and all had variable degrees of hypernasality ranging from intermittent to pervasive. Unfortunately, there were no statistically significant tendencies for patients' speech to be rated as closer to normal after the augmentation procedure than before it. The authors concluded that autogenous posterior pharyngeal wall augmentation by the techniques selected does not result in speech improvement.
In another attempt to resolve the problem of VPI, Marsh and Wray (1980) reported the results of 34 children, aged 3 to 13 years, who were randomized to manage their VPI with either a speech bulb (n = 12) or superiorly based pharyngeal flap (n = 22). The speech bulb was effective in 11 of 12 and the pharyngeal flap in 20 of 22 cases. All patients randomized to surgery complied, while 29% of the prosthesis patients did not. In addition, 33% of patients randomized to the speech prosthesis later had a pharyngeal flap placed. For a variety of reasons (e.g., cost, time, expertise, compliance, and family preference for surgery), use of a speech bulb to solve the problem of VPI is almost always a secondary choice (Ross et al., 1996).
Our clinical impression is in agreement with the objective findings of Shprintzen et al. (1979), Argamaso et al. (1994), and Salyer and others. For the majority of patients, a superiorly based pharyngeal flap tailored in both height and width according to the preoperative findings gives the most reliable results with an acceptable degree of morbidity.
Management of Alveolar and Palatal (Cleft) Skeletal Defects and Residual Oronasal Fistula
When the congenital cleft runs through the alveolar ridge, as it does in 75% of CLP patients, a residual perialveolar oronasal fistula and bony defect through the alveolar ridge, floor of the nose, and hard palate will remain despite satisfactory lip and palatal repair (Millard, 1980). In addition, by early childhood there will be a variable degree of collapse of the two maxillary segments in the UCLP patient and of the lateral and premaxillary segments in the BCLP patient, resulting in lateral crossbites and the potential for a negative overjet at the incisors (Preuzansky, 1964; Derijcke et al., 1994; Jolleys, 1954; Jolleys and Robertson, 1972; Lebert, 1962; McCance et al., 1993; Nelson et al., 1988; Nylen et al., 1974; Rehrmann, 1971; Robertson and Jolleys, 1968).
Timing
The most efficient way to achieve the objectives of eruption of the (permanent) canine tooth through the grafted cleft with normal alveolar ridge development, improved skeletal support for the base of the nose, effective closure of all residual labial and palatal oronasal fistulae, and unity of the cleft maxillary segments is through properly sequenced and timed interceptive orthodontic treatment and secondary alveolar and palatal skeletal and soft tissue surgery (Pruzansky, 1964; Abyholm et al., 1981; Assuncao, 1993; Bergland et al., 1986; Bertz, 1981; Boyne, 1970, 1974, 1985; Boyne and Sands, 1972,1976; Correa Normando et al., 1992; El Deeb et al., 1982; Hall and Posnick, 1984; Henderson and Jackson, 1975; Koberg, 1973; Nique et al., 1987; Posnick, 1991; Rosenstein et al., 1982, 1991a,b; Rudman, 1997; Sindet-Pedersen and Enemark, 1990; Troxell et al., 1982; Turvey et al., 1984; Waite and Kersten, 1980). There are two advantages to waiting until the eruption of the permanent maxillary first molars before proceeding. First, reliable and efficient orthodontic anchorage is achieved for rapid arch expansion just prior to the surgical procedure. Second, waiting allows maximal transverse (posterior) growth of the maxilla prior to bone grafting. The preferred age at treatment is therefore dependent on dental age rather than chronologic age (Abyholm et al., 1981; Hall and Posnick, 1984).
It is important to remember that in the CLP patient the maxillary dental eruption pattern is often delayed.
Techniques
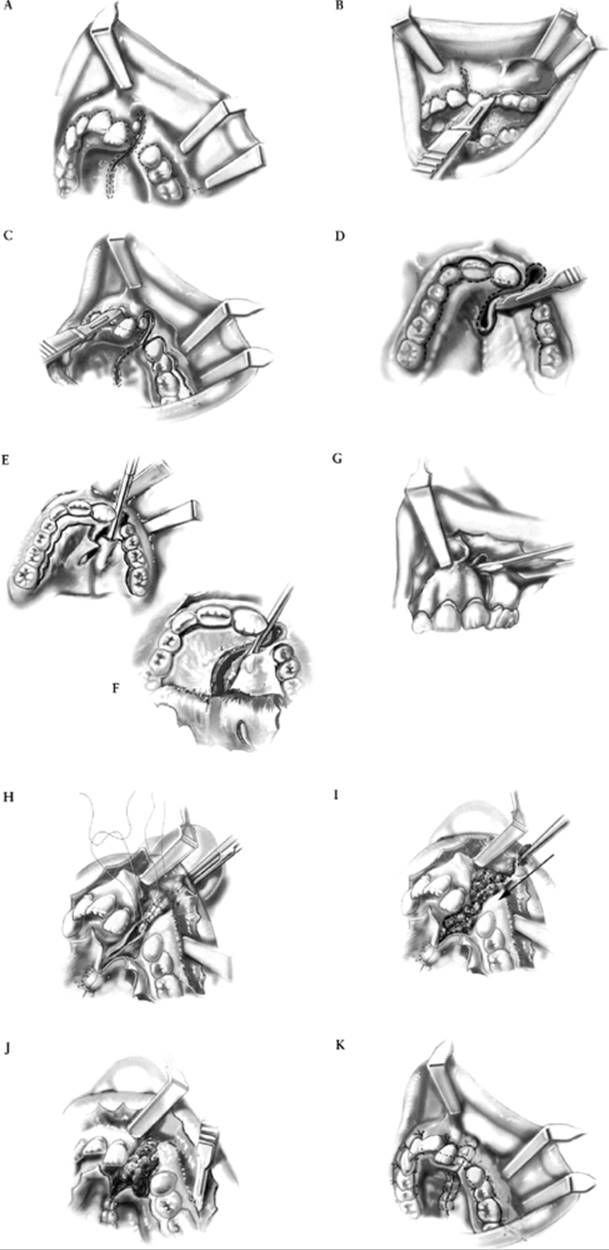
The interceptive phase of orthodontic treatment will achieve expansion of the posterior arch width in both BCLP and UCLP patients and will reposition the premaxilla in BCLP patients. Once these orthodontic objectives are completed, surgery is carried out to place the patient's own cancellous iliac (hip) bone within the skeletal defects in the hard palate, alveolar ridge, and nasal floor with closure of all residual labial and palatal oronasal fistulae (Canady et al., 1993; Catone et al., 1992; Fonseca, 1997; Posnick, 2000a,b) (Figs. 26.10,26.11 and 26.12). While some CLP teams believe that placement of the bone graft within the skeletal defect prior to eruption of the permanent central or lateral incisors at the cleft site is an advantage, all agree that a successful graft is best placed prior to eruption of the permanent canine tooth through the cleft (Abyholm et al., 1981; Hall and Posnick, 1984).
There is no long-term advantage to achieving orthodontic expansion of the cleft segments until just prior to grafting. Arch expansion is generally achieved with a Quadhelix or Hyrax appliance over a 3- to 6-month period. Approximately 6 to 8 weeks following bone grafting, the orthodontist may proceed with additional segment repositioning and tooth movement in and around the grafted area. Only rarely will the rudimentary lateral incisor tooth at the cleft site have long-term value (Abyholm et al., 1981; Hall and Posnick, 1984). Even if the (lateral incisor) crown is sufficient to hold a restoration, its root length and volume are generally insufficient to warrant its preservation. The decision of whether to retain or extract the lateral incisor tooth must be made early in the mixed dentition, with extraction carried out prior to or at the time of bone grafting.
|
|
|
FIG. 26.10. Illustrations of techniques for bone grafting and management of residual oronasal fistula in the patient with unilateral cleft lip and palate. A: Location of planned left and right labial and bilateral palatal incisions prior to flap elevation. B: Close-up view of left labial mucogingival incision in progress. C: Left labial mucogingival incision completed and right labial incision in progress. D:Attention is turned to the palate for elevation of the palatal flaps and separation of the oral and nasal mucosae at the site of the fistula. E: Subperiosteal elevation of palatal flaps. F: With palatal flaps elevated, the nasal mucosa is separated from the floor of the nose on each side for later closure. G: Left and right labial flaps have been elevated. The nasal mucosa is further separated from its bony surface along the distal aspect of the central incision for later suturing. H: Suturing of nasal flaps for water-tight closure. A hemostat is placed through the left nostril to demonstrate the sutured nasal floor. I: Once the nasal flaps are sutured, lilac cancellous bone graft is packed into palatal, alveolar, and floor-of-thenose skeletal defects. J: The left labial flap is scored at the periosteum to allow advancement for wound closure over the cleft site. K: Left and right labial flaps and palatal flaps are closed for water-tight seal. By advancing the left labial mucogingival flap, keratinized tissue has been placed over the alveolar ridge where the permanent canine tooth will eventually erupt. (From Posnick, 2000b, with permission.) |
|
|
|
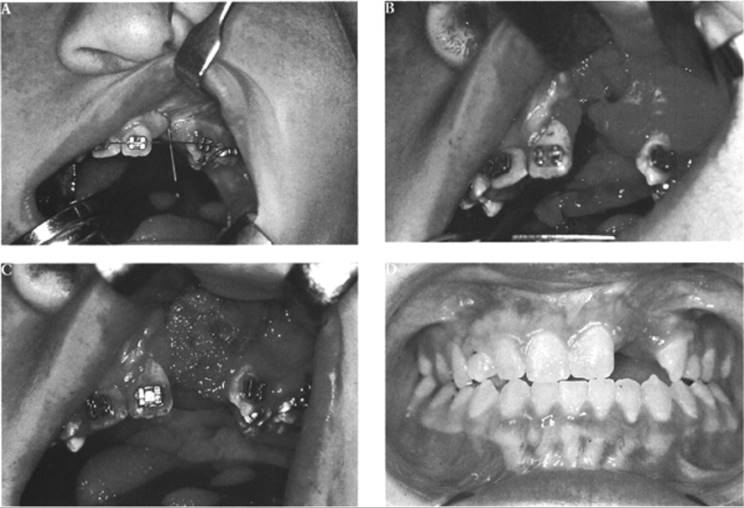
FIG. 26.11. A child in the mixed dentition born with unilateral cleft lip and palate who underwent lip and palatal repair in infancy and early childhood. He presented in the mixed (transitional) dentition with an alveolar/palatal defect and residual labial and palatal oronasal fistulae. He underwent interceptive orthodontic treatment to expand the maxillary arch width, followed by autogenous lilac bone grafting and fistula closure. A: Intraoperative close-up view with nasolacrimal probe placed through the floor of the nose into the oral cavity, demonstrating oronasal fistula. B: Close-up view of skeletal defect after flap elevation. C: Same view with cancellous (lilac) bone graft packed into defect. D: Occlusal view after bone grafting and completion of interceptive orthodontic treatment. (From Posnick, 2000b, with permission.) |
An important aspect of the surgical procedure is management of the intraoral soft tissue as part of the oronasal fistula closure. A labial mucogingival flap is elevated and advanced anteriorly, bringing keratinized mucosa to the cleft site, where the permanent canine tooth will erupt (Adell, 1974). It is important to elevate and advance the flap to achieve closure of the fistula without destruction of the vestibular architecture, as would occur if a buccal (cheek) flap were used. The erupted canine tooth is then surrounded by gingiva and develops a normal periodontal sulcus.
Orthognathic Deformities in Cleft Lip and Palate
Unfortunately, one long-term negative effect of CP repair is a 25% incidence of maxillary growth restriction that produces secondary deformities of the jaws and occlusion, which will also have a negative impact on speech and self-esteem to the extent that further skeletal surgery will be required (Harper, 1995; Correa Normando et al., 1992; Bardach et al., 1994; Kapp-Simon, 1995).
The maxillary hypoplasia is the result of surgical intervention and is not attributable to the congenital clefting. Jaw reconstruction is needed for these patients, which must be coordinated with the final phase of orthodontic treatment. Jaw surgery, if required, is preferably carried out at the time of skeletal maturity of the patient (age 14-16 in girls and 16-18 in boys).
|
|
|
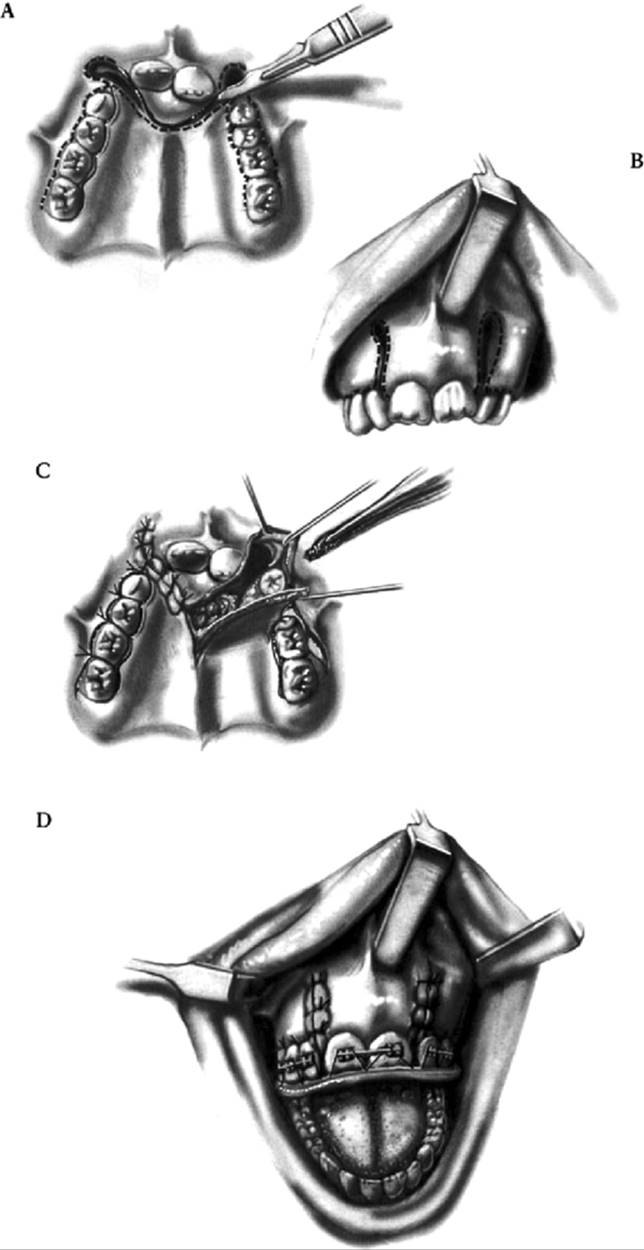
FIG. 26.12. Illustration of the technique modifications for bone graft and management of the residual oronasal fistula in the patient with bilateral cleft lip and palate. A: Palatal view indicating location and extent of planned incisions for secondary bone grafting and fistula closure. B: Frontal view indicating location and extent of planned labial incisions. Note the importance of maintaining the integrity of the labial mucosa to the premaxillary bone. Without doing so, the circulation requirements to the premaxilla would be compromised. C: After nasal side closure and bone graft placement, the oral wounds are closed. View of palate indicating final placement of bone graft prior to closure. D: Frontal view of patient at end of bone grafting procedure. A prefabricated acrylic splint is used to secure the three maxillary segments to one another to allow for bone graft healing. (From Posnick, 2000b, with permission.) |
Unfortunately, there remains a subgroup of adolescents who present with a jaw deformity requiring orthognathic surgery as well as residual CLP, alveolar and palatal defects, oronasal fistulae, and dental gaps of the maxilla. For these patients, modification of the standard Le Fort I osteotomy allows for independent repositioning of the cleft maxillary segments according to the type of presenting cleft (UCLP or BCLP), the specific residual deformities, and individual variation (Hall and Posnick, 1984; Posnick, 1991, 2000c, 2000d; Proffitt, 1991). These unique anatomic abnormalities should be seen as technical challenges rather than obstacles to the satisfactory rehabilitation of the patient. For either the isolated CP patient or the UCLP or BCLP patients who achieved a successful bone graft in the mixed dentition, a more standard Le Fort I type osteotomy provides the desired skeletal reconstruction of the maxilla and dental rehabilitation.
Cleft-Orthognathic Surgery: Unilateral Cleft Lip and Palate
Residual deformities in the adolescent born with unilateral cleft lip and palate
The prevalence of residual clefting deformities in adolescents born with UCLP who present with a jaw discrepancy varies widely, depending on the center's philosophy in regard to the staging of reconstruction and its available surgical expertise. In addition, despite a center's preferred method of management in infancy, childhood, and early adolescence, a subgroup of UCLP patients presenting with multiple clefting problems includes the following:
1. Maxillary hypoplasia. The maxilla is often vertically short, resulting in an edentulous look, and the occlusal plane is often canted (up on the cleft side). Arch width deficiency resulting in crossbite may be present in the transverse plane. The maxillary dental midline may be shifted off the facial midline, usually toward the cleft side. The hypoplastic maxilla is retruded in the horizontal plane, resulting in a concave midfacial profile, Angle class III malocclusion, and negative overjet. Greater and lesser maxillary segments vary in degree of dysplasia, making it difficult to achieve a satisfactory appearance by repositioning the maxilla in one unit rather than with segmental osteotomies.
2. Residual oronasal fistula. Despite the general preference for oronasal fistula closure and bone grafting in the mixed dentition, the UCLP candidate for orthognathic surgery will often have residual labial and palatal fistulae. Previous attempts at closure may have failed. Furthermore, buccal mucosa may have been placed over the cleft site, resulting in a lack of attached gingiva in the tooth-bearing surface region and loss of vestibular depth.
3. Residual bony defects. In the UCLP patient who has not been successfully bone-grafted in the mixed dentition, there remain significant bony defects, not just at the alveolus but throughout the palate and floor of the nose along the cleft site. This results in an inferiorly and posteriorly displaced floor of the nose and nasal sill.
4. Cleft-dental gap. The lateral incisor is frequently congenitally absent at the cleft site. A hypoplastic tooth may be present but with inadequate root development or bony impaction in the cleft. Orthodontic closure of this gap with movement of the canine tooth into the bone-grafted lateral incisor location is the preferred approach in the mixed dentition. Unfortunately, this is not always accomplished and often there is mesial angulation of the canine tooth into a nongrafted cleft site. The result is often a dental gap at the cleft site between the central incisor and canine teeth.
5. Chin dysplasia. The UCLP patient will frequently be a mouth-breather with the resulting open-mouth posture. Addition of a pharyngeal flap in childhood may increase this tendency. The result is a vertically long and retrognathic chin.
6. Mandibular dysplasia. True mandibular prognathism is uncommon in the UCLP patient. The need for mandibular osteotomies should be limited to facial asymmetries, occlusal plane canting, and the occasional true anteroposterior discrepancy (Laspos et al., 1997).
Technique
We have described modifications of the Le Fort I osteotomy for the UCLP deformity, placing the soft tissue incisions to permit direct exposure for dissection, osteotomies, disimpaction, fistula closure, bone graft, and application of plate-and-screw fixation but without risk of circulation injury to the dento-osseous-musculo-mucosal flaps (Posnick, 2000c; Posnick and Tompson, 1992). The increased visibility provided by these incisions makes it possible to incorporate routine surgical closure of the cleft-dental gap through differential maxillary segmental repositioning (Figs. 26.13,26.14). This method of approximating the gap in the maxillary segments also closes the cleft dead space and brings together the labial and palatal flaps to permit closure of recalcitrant oronasal fistulae without tension.
|
|
|
FIG. 26.13. Illustrations of modified Le Fort I osteotomy, performed in two segments, in a patient with unilateral cleft lip and palate. A: Lateral view of maxillofacial skeleton before and just after osteotomies and fixation of modified Le Fort I osteotomy. B: Illustration of downfractured Le Fort I osteotomy in two segments after submucous resection of septum, reduction of inferior turbinate through the nasal mucosa opening, and watertight nasal side closure. C: Palatal view of bony segments before and after repositioning. D: Oral-side wound closure on both labial and palatal aspects after differential segmental repositioning. (From Posnick, 1991b, with permission.) |
Cleft-Orthognctthic Surgery: Bilateral Cleft Lip and Palate Deformity
Residual deformities in the adolescent born with bilateral cleft lip and palate
The BCLP adolescent presenting with a jaw discrepancy may have several or all of the following residual clefting problems (Posnick, 2000d). These deformities, when present, must be addressed to achieve improved facial aesthetics, function, and dental rehabilitation.
1. Maxillary hypoplasia. The premaxilla may be either vertically long, resulting in a gummy smile, or vertically short, with an edentulous look. There may be a negative overjet, indicating horizontal deficiency. The arch width of the lateral segments is generally deficient in the transverse plane, with bilateral posterior crossbites and a degree of horizontal deficiency, with an Angle class III malocclusion.
2. Residual oronasal fistula. Despite a preference for fistula closure and bone grafting in the mixed dentition, the BCLP candidate for orthognathic surgery will often have residual labial and palatal fistulae with loss of fluid through the nose while drinking and air leakage while speaking. Previous attempts at fistula closure may have failed because of inadequate available soft tissue for wound closure.
3. Cleft-dental gaps. Lateral incisors are most frequently absent at the cleft site. Rudimentary teeth may also be impacted within the cleft and, if so, are of no functional value. If hypoplastic lateral incisors do erupt in the lateral segments, they rarely have adequate root support for long-term functioning. The result is often a dental gap at the cleft site between the central incisor and canine teeth on each side.
4. Residual bony defects. Significant residual bony defects through the alveolus, floor of the nose, and palate are frequent, resulting in a mobile premaxilla secured only to the nasal septum.
5. Chin dysplasia. The BCLP patient will frequently be a mouth-breather with the resulting open-mouth posture. The result is a vertically long and retrognathic chin.
6. Mandibular dysplasia. True manidular prognathism in the BCLP patient is uncommon. The need for mandibular osteotomy should be limited to facial asymmetries, occlusal plane canting, and actual anteroposterior discrepancy.
|
|
|
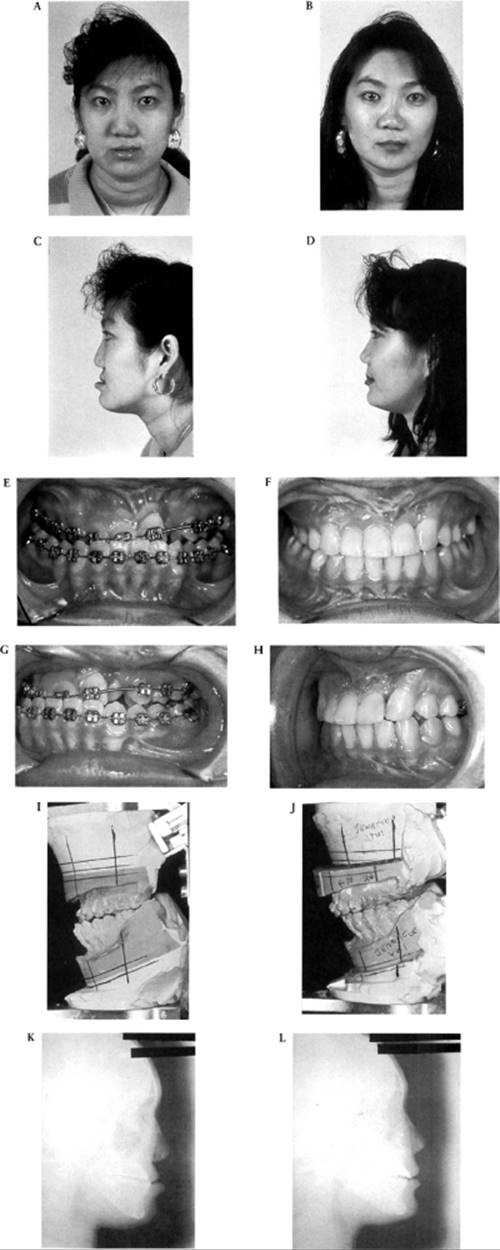
FIG. 26.14. A 16-year-old girl born with unilateral cleft lip and palate underwent a combined orthodontic and orthognathic surgical approach including a modified Le Fort I osteotomy in two segments (differential repositioning of the segments, correction of occlusal canting, and closure of oronasal fistula, alveolar defect, and cleft-dental gap), bilateral sagittal split osteotomies of the mandible (correction of asymmetry), and osteoplastic genioplasty (vertical reduction and horizontal advancement). Stabilization was accomplished with iliac graft and miniplate and screw fixation. A: Frontal view in repose before surgery. B: Frontal view in repose after reconstruction. C: Profile view before surgery. D: Profile view after reconstruction. E: Occlusal view before surgery. F: Occlusal view after reconstruction. G: Oblique occlusal view before surgery. H: Oblique occlusal view after reconstruction. I: Lateral view of articulated dental casts before surgery. J: Lateral view of articulated dental casts after model surgery. K: Lateral cephalometric radiograph before surgery. L: Lateral cephalometric radiograph after reconstruction. (From Posnick and Tompson, 1995, with permission.) |
|
|
|
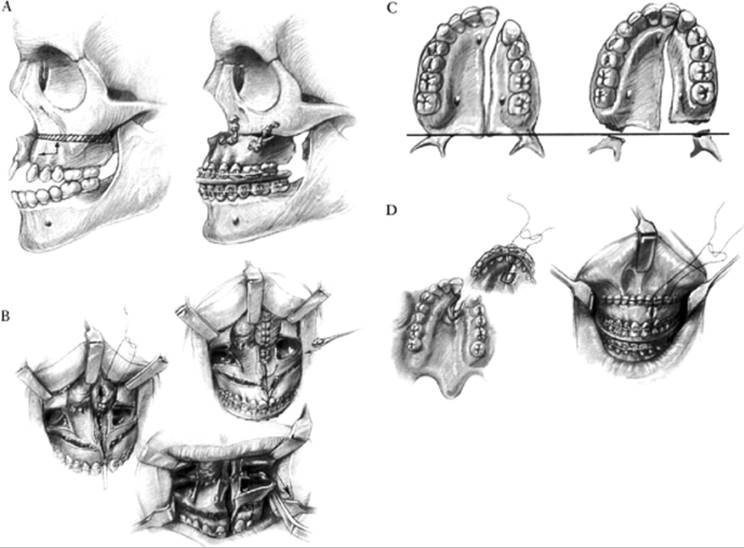
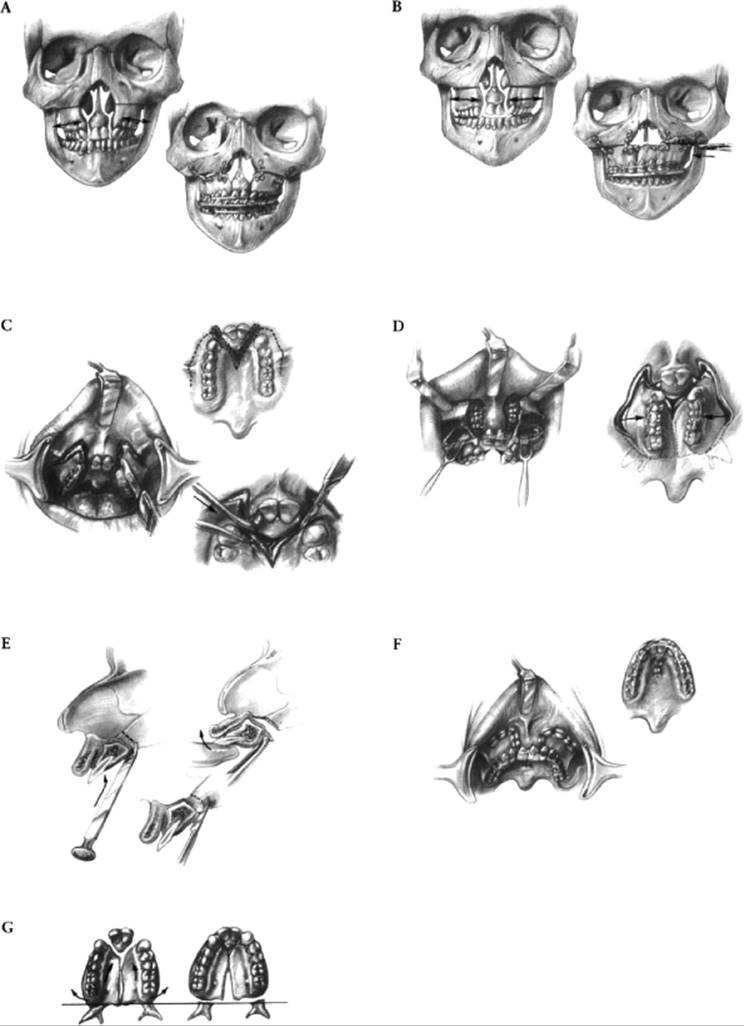
FIG. 26.15. Illustrations of modified Le Fort I osteotomy in two or three segments. A: Patient with bilateral cleft lip and palate before (left) and after (right) lateral segmental osteotomies and repositioning. B: Illustrations before (left) and after (right) three-part maxillary osteotomies with repositioning of the segments. C: Incisions for modified Le Fort I in three segments. D: Downfractured lateral segments demonstrating exposure of nasal-side closure of oronasal fistula and additional view of oral mucosal incisions. E: Premaxillary osteotomy from palatal side using either a chisel, a rongeur, or a reciprocating saw. F: Oral wounds sutured at end of procedure. G: Palatal view of bone segments before (left) and after (right) repositioning for closure of cleft-dental gaps. (From Posnick, 1991b, with permission.) |
|
FIG. 26.16. An 18-year-old boy born with bilateral cleft lip and palate underwent a combined orthodontic and orthognathic surgical approach including a modified Le Fort I osteotomy in three segments (differential repositioning of segments; closure of oronasal fistula, alveolar defects, and cleft-dental gaps; and stabilization of premaxilla), bilateral sagittal split osteotomies of the mandible (correction of asymmetry), and an osteoplastic genioplasty (vertical reduction and horizontal advancement). Stabilization was accomplished with iliac bone graft and miniplate and screw fixation. A: Frontal view prior to cleft lip and palate repair. B: Profile view in the mixed dentition developmental stage. C: Occlusal view early in the mixed dentition stage. D: Occlusal view later in the mixed dentition stage. E: Frontal view with smile before surgery. F: Frontal view with smile after reconstruction. G: Profile view before surgery. H: Profile view after reconstruction. I: Occlusal view before surgery. J: Occlusal view after reconstruction. K, L: Lateral views of articulated dental casts after model surgery. M: Lateral cephalometric radiographs before surgery. N: Lateral cephalometric radiograph after reconstruction. (From Posnick and Tompson, 1993, with permission.) |
Technique
Precise incision placement is critical in the modified Le Fort I osteotomy for midfacial advancement in the BCLP patient (Posnick, 2000d; Posnick and Tompson, 1993) (Figs. 26.15,26.16). Buccal incisions are made in the depth of the vestibules and extend from the zygomatic buttress forward to the location of the residual labial oronasal fistula on each side. The premaxillary segment labial incisions are placed adjacent to the distal line angle of the central incisor on each side to separate the oral and nasal mucosae. Care is required to prevent any disruption of, or incision into, the mucosa on the labial vestibule of the premaxilla. It is imperative that the labial vestibule mucosa in the premaxilla remain connected to its underlying periosteum and the bone since blood flows through this pedicle into the premaxillary bone and teeth. The nasal and oral mucosae are also sharply incised and separated on the palatal aspect of the premaxilla and on each lateral segment.
A subperiosteal soft tissue dissection provides direct exposure of the anterolateral maxilla on each (lateral segment) side. Routine Le Fort I osteotomies are then performed through the lateral, anterior, and medial maxillary walls with a reciprocating saw. The pterygomaxillary sutures are separated with a mallet and osteotome. The lateral segments are downfractured with finger pressure, then disimpacted with Tessier hooks to release scar tissue for three-dimensional repositioning. The vomer may be attached to the lateral segments. If it is, an osteotomy is also required before the downfracture. The lateral maxillary segments are advanced and ligated into the prefabricated acrylic occlusal splint, along with the premaxillary segment. Through this procedure, the cleft-dental gap on each side and the dead space associated with the bony clefts are closed. All three segments are placed into a prefabricated acrylic splint, and the desired horizontal advancement is achieved. The ideal vertical dimension, determined preoperatively, is achieved at the maxillary osteotomy sites to improve the lip-to-tooth relationship and the appearance of the smile.
Cleft-Orthognathic Surgery: Isolated Cleft Palate Deformity
Residual deformities in the adolescent born with an isolated cleft palate
The isolated CP adolescent presenting with a jaw discrepancy may have one or more of the following residual maxillofacial deformities (Posnick, 2000e).
1. Maxillary dysplasia. When maxillary dysplasia occurs, it generally follows one of two patterns. The first and most frequently seen is horizontal maxillary retrusion, generally with a degree of vertical hypoplasia. The second is vertical maxillary excess with a degree of horizontal retrusion. The latter tends to occur in mouth-breathers, especially if a pharyngeal flap was placed in childhood.
2. Residual oronasal (palatal) fistula. There may be a residual midline palatal fistula located in the region between the incisal foramen and the soft palate.
3. Residual bony defects. The alveolus is not cleft, but generally there are bony defects of the hard palate.
4. Chin dysplasia. The isolated CP patient will frequently be a mouth-breather with the resulting open-mouth posture. The end result is a vertically long and retrognathic chin. If Robin sequence is present, retrogenia is also expected.
5. Mandibular dysplasia. True mandibular prognathism is rare. Mandibular retrognathism may be part of a Robin sequence but is rarely seen in the adolescent. The need for mandibular osteotomies in addition to maxillary osteotomy is limited, but each patient's unique jaw deformities must be evaluated independently.
Revision of the Cleft Lip Scar and Correction of the Nasal Deformity
Cleft Nasal Reconstruction
A congenital cleft, either unilateral or bilateral, extending through the lip, nasal base, and alveolar ridge results in a significant nasal malformation affecting both function and appearance (McComb, 1990, 1994; Horswell and Pospisil, 1995; Sandham and Murray, 1993). Despite effective initial CL repair with or without primary nasal maneuvers, a significant functional and displeasing nasal malformation or deformation frequently persists, which, for psychological reasons, will benefit from further reconstruction.
Some surgeons take an aggressive posture to correction of both the nasal dysfunction and less-than-ideal facial aesthetics, carrying out additional surgery once the problem is recognized, regardless of the child's age. Others take a long-range approach and selected a preferred window of opportunity to achieve maximal longterm nasal function and facial aesthetics, with the creation of minimal scar tissue and a limited need for additional procedures.
The final (secondary) nasal reconstruction will likely be carried out through an open (columella-splitting) technique to achieve maximal exposure of the nasal dorsum, tip, and septum. Through this approach, nasal osteotomies, dorsal reduction, lower lateral cartilage repositioning or sculpting, and harvesting of septal cartilage for augmentation of the nasal tip to improve nasal symmetry and projection can be performed under direct vision (Gubiscla, 1990; Takato et al., 1995b). If the need for orthognathic surgery seems likely, then it is best to postpone the final rhinoplasty until after the jaw reconstruction. The cleft surgeon must remember that cartilage grafting is an essential component of the final rhinoplasty and that septal cartilage provides the best source and will be available in sufficient quantity only one time. The use of ear or rib cartilage is another option.
Standard thinking holds that the columella in the BCL patient is short and requires secondary lengthening. The teaching is that there are two ways to accomplish this goal: using banked forked flaps (Millard, 1967; van der Meulin, 1992) and lengthening the columella with medial rotation of the bilateral nasal floor and alar flaps (Cronin, 1958). Unfortunately, these techniques result in an unnatural, sharp columellarlabial angle, excessive columellar length, a broad nasal tip, further deformity to the nostrils, and a wide and scarred columella. Trier (1995), agreeing with Mulliken (1995), abandoned the secondary columellar lengthening procedures as unsightly and cosmetically counterproductive. We prefer to reshape and augment the lower lateral cartilage of the nose with a septal cartilage strut graft secured to the caudal portion of the septum under direct vision via the open technique. By doing this, a stretching of the overlying soft tissue envelope rather than a direct lengthening of the skin of the columella is possible.
Cleft Lip Scar Revision
The majority of children who undergo initial CL repair in infancy will require at least one lip scar revision in childhood or adolescence (Harper, 1995; Cohen et al., 1995). The extent of revision required is dependent on the success of the primary CL repair and the degree to which subsequent growth has affected the initial results (Chen et al., 1995; Randall, 1995). Cleft lip revision will often require a complete takedown with excision of scar tissue (skin, vermilion, and mucosa), removal of redundant and residual hypoplastic tissue, and reapproximation of the obicularis oris muscle. It may also require reapproximation of key anatomic landmarks, including the vermilion-cutaneous junction and the vermilion-mucosal junction. Additional objectives include leveling of the lip lengths (philtral columns) and establishment of a normal upper lip oral vestibule. Ideally, only one major lip scar revision will be required, and it is best accomplished when the child is between 5 and 15 years of age, with psychosocial needs taken into account. The exact age at revision is dependent on the family's and patients' preference, the extent of the deformity, and the potential for surgical improvements.
Conclusions
The successful rehabilitation of a child born with CLP requires close cooperation among the specialists that make up the CLP team. Each specialist has a level of involvement at different stages of the patient's growth and development. A coordinated approach is essential to help the child achieve ideal speech, occlusion, facial appearance, and self-esteem. Unnecessary, unproductive, and unproven interventions, whether speech therapy, orthodontic or prosthetic treatment, or surgical procedures, should be avoided as they exhaust the patient, family, and healthcare system, produce unfulfilled expectations, and often introduce secondary deformities which may limit the eventual success of rehabilitation. Maximizing the patient's ability to pursue and achieve personal success in his or her life without special regard to the original CLP malformation is the ultimate objective.
References
Abbe, R (1898). A new plastic operation for the relief of deformity due to double hare lip. Med Rec 53: 477.
Abramson, DL, Marrinan, EM, Muiilken, JB (1997). Robin sequence: obstructive sleep apnea following pharyngeal flap. Cleft Palate Craniofac J 34: 256.
Abyholm, F, Bergland, O, Semb, G (1981). Secondary bone grafting of alveolar clefts. Scand J Plast Reconstr Surg 15: 127.
Abyholm, FE (1979). Palatal fistulae following cleft palate surgery. Scand J Plast Reconstr Surg 13: 295.
Adams, GR (1981). The effects of physical attractiveness on the socialization process. In: Lucker GW, Psychological Aspects of Facial Form. Craniofacial Growth Series 11, edited by GW Lucker, KA Ribbens, and JA McNamara. Ann Arbor: University of Michigan Press, pp. 25–47.
Adell, R (1974). Regeneration of the periodontium. Scand J Plast Reconstr Surg Hand Surg Suppl 11: 1–177.
Ainoda, N, Yamashita, Y, Tsukada, S (1985). Articulation at age 4 in children with early repair of cleft palate. Ann Plast Surg IS: 415.
Amaratunga, NA (1988). Occurrence of oronasal fistulas in operated cleft palate patients. J Oral Maxillofac Surg 46: 834.
American Cleft Palate-Craniofacial Association (1993). Parameters for the evaluation and treatment of patients with cleft lip/palate or other craniofacial anomalies. Cleft Palate Craniofac J 30(Suppl 1): 4.
Argamaso, RV (1992). Glossopexy for upper airway obstruction in Robin sequence. Cleft Palate Craniofac J 29: 232.
Argamaso, RV, Levandowski, G, Golding-Kushner, KJ, et al. (1994). Treatment of asymmetric velopharyngeal insufficiency with skewed pharnygeal flap. Cleft Palate Craniofac J 31: 287.
Assuncao, AGA (1993). The design of tongue flaps for the closure of palatal fistulas. Plast Reconstr Surg 91: 806.
Bardach, J, et al. (1990). The Iowa-Hamburg project. In: Multidisciplinary Management of Cleft Lip and Palate, edited by J Bardach and HL Morris. Philadelphia: WB Saunders, pp. 98–112.
Bardach, J, Kelly, KM, Salyer, KE (1994). Relationship between the sequence of lip and palate repair and maxillary growth: an experimental study in beagles. Plast Reconstr Surg 93: 269.
Bardach, J, Nosal, P (1987). Geometry of the two-flap palatoplasty. In: Surgical Techniques in Cleft Lip and Palate, edited by J Bardach and K Salyer. St. Louis: Mosby Year Book, pp. 192–197.
Bardach, J, Salyer, K (1991a). Surgical Techniques in Cleft Lip and Palate, 2nd ed. St. Louis: Mosby Year Book.
Bardach, J, Salyer, K (1991b). Pharyngoplasty. In: Surgical Techniques in Cleft Lip and Palate, 2nd ed., edited by J Bardach and K Salyer. St. Louis: Mosby Year Book.
Barone, CM, Shprintzen, RJ, Strauch, B, et al. (1994). Pharyngeal flap revisions: flap elevation from a scarred posterior pharynx. Plast Reconstr Surg 93: 279.
Beers, MD, Pruzansky, S (1955). The growth of the head of an infant with mandibular micrognathia: glossoptosis and cleft palate following the Beverly Douglas operation. Plast Reconstr Surg 16: 189.
Benacerraf, BR, Mulliken, JB (1993). Fetal cleft lip and palate: sonographic diagnosis and postnatal outcome. Plast Reconstr Surg 92: 1045.
Bergland, O, Semb, G, Abyholm, FE, et al. (1986). Elimination of the residual alveolar cleft by bone graft and subsequent orthodontic treatment. Cleft Palate J 23: 175.
Berkowitz, S (1996). The comparison of treatment results in complete cleft lip/palate using conservative approach vs Millard- Latham PSOT procedure. Semin Orthod 2: 169.
Berry, LA, Witt, PD, Marsh, JL, et al. (1997). Personality attributions based on speech samples of children with repaired cleft palates. Cleft Palate Craniofac J 34: 385–9.
Bertz, JE (1981). Bone grafting of alveolar clefts. J Oral Surg 39: 874.
Bezirdjian, DR, Szucs, R (1989). Sickle-shaped scapulae in a patient with the Pierre Robin syndrome. Br J Radiol 62: 171.
Bishara, SE (1973). Cephalometric evaluation of facial growth in operated and unoperated individuals with isolated clefts of the palate. Cleft Palate J 10: 239.
Bitter, K (1992). Latham's appliance for presurgical repositioning of the protruded premaxilla in bilateral cleft lip and palate. J Craniomaxillofac Surg 20: 99.
Blijdorp, P, Muller, H (1984). The influence of the age at which the palate is closed on speech in the adult cleft patient. J Maxillofac Surg 12: 239.
Blocksma, R (1963). Correction of velopharyngeal insufficiency by Silastic pharyngeal implants. Plast Reconstr Surg 31: 268.
Bluestone, CD, Musgrave, RH, McWilliams, BJ (1968). Teflon injection pharyngoplasty: status 1968. Laryngoscope 78: 558.
Bowers, EJ, Mayro, RF, Whitaker, LA, et al. (1987). General body growth in children with clefts of the lip, palate and craniofacial structure. Scand J Plast Reconstr Surg 21: 7.
Boyne, PJ (1970). Autogenous cancellous bone and marrow transplants. Clin Orthop 73: 199.
Boyne, PJ (1974). Use of marrow-cancellous bone grafts in maxillary alveolar and palatal clefts. J Dent Res 53: 821.
Boyne, PJ (1985). Correction of dentofacial deformities associated with residual alveolar and palatal clefts. In: Surgical Correction of Dentofacial Deformities, Vol. 3, edited by WH Bell. Philadelphia: WB Saunders, pp. 560–591.
Boyne, PJ, Sands, NR (1972). Secondary bone grafting of residual alveolar and palatal clefts. J Oral Surg 30: 87.
Boyne, PJ, Sands, NR (1976). Combined orthodontic-surgical management of residual palatoalveolar cleft defects. Am J Orthod 70: 21.
Brauer, RO (1985). Repair of unilateral cleft lip: triangular flap repairs. Clin Plast Surg 12: 595.
Brauer, RO, Fox, DR, Humphreys, D. (1990). Augmentation of the posterior pharyngeal wall. In: Multidisciplinary Management of Cleft Lip and Palate, edited by J Bardach and HL Morris. Philadelphia: WB Saunders.
Broder, H, Strauss, RP (1989). Self-concept of early primary school age children with visible or invisible defects. Cleft Palate J 26: 114.
Broen, PA, Doyle, SS, Bacon, CK (1993). The velopharyngeally inadequate child: phonologic change with intervention. Cleft Palate Craniofac J 30: 500.
Broomhead, I (1957). The nerve supply of the soft palate. Br J Plast Surg 10: 81.
Brouilette, R, Hanson, D, David, R, et al. (1984). A diagnostic approach to suspected obstructive sleep apnea in children. J Pediatr 105: 10.
Bruce, A, Winship, I (1993). Radial ray defect and Robin sequence: a new syndrome? Clin Dysmorphol 2:241.
Bush, PG, Williams, AJ (1983). Incidence of the Robin anomalad (Pierre Robin syndrome). Br J Plast Surg 36: 434.
Canaday, JW, Thompson, SA, Colburn, A (1997). Craniofacial growth after iatrogenic cleft palate repair in a fetal ovine model. Cleft Palate Craniofac J 34: 69.
Canady, JW, Zeitler, DP, Thompson, SA, et al. (1993). Suitability of the iliac crest as a site for harvest of autogenous bone grafts. Cleft Palate Craniofac J 30: 579.
Caouette-Laberge, L, Bayet, B, Larocque, Y (1994). The Pierre Robin sequence: review of 125 cases and evolution of treatment modalities. Plast Reconstr Surg 93: 934.
Caouette-Laberge, L, Egerszegi, EP, de Remont, A-M, et al. (1992). Long-term follow-up after division of a pharyngeal flap for severe nasal obstruction. Cleft Palate Craniofac J 29: 27.
Carey, JC, Fineman, RM, Ziter, FA (1982). The Robin sequence as a consequence of malformation, dysplasia, and neuromuscular syndromes. J Pediatr 101: 858.
Carroll, DB, Peterson, RA, Worton, EW, Birnbaum, LM (1971). Hereditary factors in the Pierre Robin syndrome. Br J Plast Surg 24: 43.
Catone, GA, Reimer, BL, McNeir, D, et al. (1992). Tibial autogenous cancellous bone as an alternative donor site in maxillofacial surgery. J Oral Maxillofacial Surg 50: 1258.
Chapman, KL, Hardin, MA (1992). Phonetic and phonologic skills of 2-year-olds with cleft palate. Cleft Palate Craniofac J 29: 435.
Chen, KT, Noordhoff, MS, Chen, Y-R, et al. (1995). Augmentation of the free border of the lip in cleft lip patients using temporoparietal fascia. Plast Reconstr Surg 95: 781.
Chen, PK-T, Wu, JTH, Chen, Y-R, et al. (1994). Correction of secondary velopharyngeal insufficiency in cleft palate patients with the Furlow palatoplasty. Plast Reconstr Surg 94: 933.
Chitayat, D, Meunier, CM, Hodgkinson, KA, et al. (1991). Robin sequence with facial and digital anomalies in two half-brothers by the same mother. Am J Med Genet 40: 1167.
Christensen, K, Fogh-Andersen, P (1993). Isolated cleft palate in Danish multiple births, 1970–1990. Cleft Palate Craniofac J 30: 469.
Cocke, WJ (1966). Experimental production of micrognathia and glossoptosis associated with cleft palate (Pierre Robin syndrome). Plast Reconstr Surg 38: 395.
Cohen, MM, Jr (1976). The Robin anomalad—its nonspecificity and associated syndromes. J Oral Surg 34: 587.
Cohen, MM, Jr (1997). Need for velopharyngeal management following palatoplasty: an outcome analysis of syndromic and nonsyndromic patients with Pierre Robin. Plast Reconstr Surg 99: 1530.
Cohen, SR, Corrigan, M, Wilmot, J, et al. (1995). Cumulative operative procedures in patients aged 14 years and older with unilateral or bilateral cleft lip and palate. Plast Reconstr Surg 96: 267.
Copeland, M (1990). The effect of very early palatal repair on speech. Br J Plast Surg 43: 676.
Correa Normando, AD, da Silva Filho, OG, Capelozza Filho, L (1992). Influence of surgery on maxillary growth in cleft lip and/or palate patients. J Craniomaxillofac Surg 20: 111.
Croft, CB, Shprintzen, RJ, Ruben, RJ (1981). Hypernasal speech following adenotonsillectomy. Otolaryngol Head Neck Surg 89: 179.
Cronin, TD (1958). Lengthening columella by use of skin from nasal floor and alae. Plast Reconstr Surg 21: 417.
Cutting, CB, Rosenbaum, J, Rovati, L (1995). The technique of muscle repair in the cleft soft palate. Operative Tech Plast Reconstr Surg 2: 215.
Dalston, RM (1992). Timing of cleft palate repair: a speech pathologist's viewpoint. In: Problems of Plastic Surgery in Cleft Palate Surgery, edited by JA Lehman. Philadelphia: JB Lippincott, pp. 30–38.
D'Antonio, L, Marsh, JL, Province, M, et al. (1989). Reliability of flexible fiberoptic nasopharyngoscopy for evaluation of velopharyngeal function in a clinical population. Cleft Palate J 26: 217.
Davies, D (1966). The one-stage repair of unilateral cleft lip and palate: a preliminary report. Plast Reconstr Surg 38: 129.
Denk, MJ, Magee, WP, Jr (1996). Cleft palate closure in the neonate: preliminary report. Cleft Palate Craniofac J 33: 57.
Dennison, WM (1965). The Pierre Robin syndrome. Pediatrics 36: 336.
Denny, AD, Marks, SM, Oliff-Carneol, S (1993). Correction of velopharyngeal insufficiency by pharyngeal augmentation using autologous cartilage: a preliminary report. Cleft Palate Craniofac J 30: 46.
Derijcke, A, Kuijpers-Jagtman, AM, Lekkas, C, et al. (1994). Dental arch dimensions in unoperated adult cleft palate patients: an analysis of 37 cases. J Craniofac Genet Dev Biol 14: 69.
Devlin, HB (1990). Audit and the quality of clinical care. Ann R Coll Surg Engl 72(Suppl 1): 3.
Dorf, DS, Curtin, JW (1982). Early cleft palate repair and speech outcome. Plast Reconstr Surg 70: 74.
Dorf, DS, Curtin, JW (1990). Early cleft palate repair and speech outcome: a ten year experience. In: Multidisdplinary Management of Cleft Lip and Palate, edited by J Bardach and HL Morris. Philadelphia: WB Saunders, pp. 341–348.
Dykes, EH, Raine, PA, Arthur, DS (1985). Pierre Robin syndrome and pulmonary hypertension. Pediatr Surg 20: 49.
Eaton, AC, Marsh, JL, Pilgram, TK (1994). Does reduced hospital stay affect morbidity and mortality rates following cleft lip and palate repair in infancy? Plast Reconstr Surg 94: 911.
Edwards, JRG, Newall, DR (1985). The Pierre Robin syndrome reassessed in the light of recent research. Br J Plast Surg 38: 339.
El Deeb, M, Messer, LB, Lehnert, MW, et al. (1982). Canine eruption into grafted bone in maxillary alveolar cleft defects. Cleft Palate J 19: 9.
Emory, RE, Jr, Clay, RP, Bite, U, et al. (1997). Fistula formation and repair after palatal closure: an institutional perspective. Plast Reconstr Surg 99: 1535.
Evans, D, Renfrew, C (1974). The timing of primary cleft palate repair. Scand J Plast Surg 8: 153.
Fairbairn, P (1846). Suffocation in an infant from retraction of the base of the tongue, connected with defect of the frenum. Monthly J Med Sci 6: 280.
Field, TM, Vega-Lahr, N (1984). Early interactions between infants with craniofacial anomalies and their mothers. Infant Behav Dev 7:527.
Fonseca, RJ (1997). Prospective evaluation of morbidity associated with iliac crest harvest for alveolar cleft grafting. J Oral Maxillofac Surg 55: 223.
Frohberg, U, Lange, R-T (1993). Surgical treatment of Robin sequence and sleep apnea syndrome: case report and review of the literature. J Oral Maxillofac Surg 51: 1274.
Furlow, LT (1986). Cleft palate repair by double opposing Z-plasty. Plast Reconstr Surg 78: 724.
Furlow, LT (1992). The double opposing Z-plasty for palate closure. Part I. In: Recent Advances in Plastic Surgery, edited by I Jackson and B Sommerlad. Edinburgh: Churchill Livingstone, pp. 29–42.
Furlow, LT (1997). Bilateral buccal flaps with double opposing Z-plasty for wider palatal clefts. Plast Reconstr Surg 300: 1144.
Georgiade, NG, Latham, RA (1975). Maxillary arch alignment in the bilateral cleft lip and palate infant, using the pinned coaxial screw appliance. Plast Reconstr Surg 52: 52.
Glander, K II, Cisneros, GJ (1992). Comparison of the craniofacial characteristics of two syndromes associated with the Pierre Robin sequence. Cleft Palate Craniofac J 3: 210.
Gnudi, MT, Webster, JP (1950). The Life and Times of Gaspare Tagliococci: Surgeon of Bologna. New York: Herbert Reichner, 1950.
Golding-Kushner, KJ, Argamaso RV, Cotton, RT, et al. (1990). Standardization for the reporting of nasopharyngoscopy and multiview videofluoroscopy: a report from an international working group. Cleft Palate J 27: 337.
Gould, HJ (1990). Hearing loss and cleft palate: the perspective of time. Cleft Palate J 27:36.
Graivier, MH, Cohen, SR, Kawamoto, HK, et al. (1992). A new operation for velopharyngeal insufficiency: the palatoglossus myomucosal pharyngoplasty. Plast Reconstr Surg 90: 707.
Gray, S (1990). Airway obstruction and apnea in cleft palate patients. In: Multidisdplinary Management of Cleft Lip and Palate, edited by J Bardach and HL Morris. Philadelphia: WB Saunders.
Grobbelaar, AO, Hudson, DA, Fernandes, DB, et al. (1995). Speech results after repair of the cleft soft palate. Plast Reconstr Surg 95: 1150.
Gubiscla, W (1990). How to obtain symmetries in a unilaterally cleft nose. Eur J Plast Surg 13: 241.
Guilleminault, C, Stoohs, R (1990). Chronic snoring and obstructive sleep apnea syndrome in children. Lung 168(Suppl): 912.
Haapanen, ML, Rantala, SL (1992). Correlation between the age at repair and speech outcome in patients with isolated cleft palate. Scand J Plast Reconstr Surg Hand Surg 26: 71.
Hall, HD, Posnick, JC (1984). Early results of secondary bone grafts in 106 alveolar clefts. J Oral Maxillofac Surg 41: 289.
Hanson, J, Smith, DW (1975). U-shaped palatal defect in the Robin anomaly: developmental and clinical relevance. J Pediatr 87: 30.
Harding, A, Campbell, RC (1989). A comparison of the speech results after early and delayed hard palate closure: a preliminary report. Br J Plast Surg 42: 187.
Harper, DC (1995). Children's attitudes to physical differences among youth from Western and non-Western cultures. Cleft Palate Craniofac J 32: 114.
Hartel, J, Gundlach, KKH, Ruickoldt, K (1994). Incidence of velopharyngoplasty following various techniques of palatoplasty. J Craniomaxillofac Surg 22: 272.
Hedrick, MH, Rice, HE, Vander Wall, KJ, et al. (1996). Delayed in utero repair of surgically created fetal cleft lip and palate. Plast Reconstr Surg 97: 900.
Heidbuchel, KLWM, Kuijpers-Jagtman, AM, Freihofer, HPM (1994). Facial growth in patients with bilateral cleft lip and palate. A cephalometric study. Cleft Palate Craniofac J 31: 210.
Henderson, D, Jackson, IT (1975). Combined cleft lip revision, anterior fistula closure and maxillary osteotomy: a one-stage procedure. Br J Oral Surg 13: 33.
Henningsson, G, Isberg, A (1986). Velopharyngeal movements in patients alternating between oral and glottal articulation: a clinical and cineradiographical study. Cleft Palate J 23: 1.
Herman, LT (1995). An evaluation of verlopharyngeal ring ligation in cleft palate repair. J Oral Maxillofac Surg 53: 655.
Hogan, VM (1973). A clarification of the surgical goals in cleft palate speech and the introduction of the lateral port control (LPC) pharyngeal flap. Cleft Palate J 10: 331.
Horswell, BB, Castiglione, CL, Poole, AE, et al. (1993). The doublereversing Z-plasty in primary palatoplasty: operative experience and early results. J Oral Maxillofac Surg 51: 145.
Horswell, BB, Pospisil, OA (1995). Nasal symmetry after primary cleft lip repair: comparison between Delaire cheilorhinoplasty and modified rotation-advancement. J Oral Maxillofac Surg 53: 1025.
Isberg, A, Henningsson, G (1987). Influence of palatal fistula on velopharyngeal movements: a cineradiographic study. Plast Reconstr Surg 79: 525.
Jackson, IT (1990). Pharyngoplasty: Jackson technique. In: Multidisciplinary Management of Cleft Lip and Palate, edited by J Bardach and HL Morris. Philadelphia: WB Saunders.
Jackson, IT, Silverton, JS (1977). The sphincter pharyngoplasty as a secondary procedure in cleft palates. Plast Reconstr Surg 59: 518.
James, D, Ma, L (1997). Mandibular reconstruction in children with obstructive sleep apnea due to micrognathia. Plast Reconstr Surg 100: 1131.
Jensen, BL, Dahl, E, Kreiborg, S (1983). Longitudinal study of body height, radius length and skeletal maturity in Danish boys with cleft lip and palate. Scand J Dent Res 91: 473.
Jeresaty, RM, Huszar, RJ, Basu, S (1969). Pierre Robin syndrome. Am JDis Child 117:710.
Jolleys, A (1954). A review of the results of operations on cleft palates with reference to maxillary growth and speech function. Br J Plast Surg 7: 229.
Jolleys, A, Roberston, NR (1972). A study of the effects of early bone grafting in complete clefts of the lip and palate: five year study. Plast Reconstr Surg 25: 229.
Jones, WB (1988). Weight gain and feeding in the neonate with cleft: a three-center study. Cleft Palate J 25: 379.
Kapp-Simon, KA (1995). Psychological interventions for the adolescent with cleft lip and palate. Cleft Palate Craniofac J 32: 104.
Kemp-Fincham, SI, Kuehn, DP, Trost-Cardamone, JE (1990). Speech development and the timing of primary palatoplasty. In: Bardach J, Morris HL (eds): Multidisciplinary Management of Cleft Lip and Palate, edited by J Bardach and HL Morris. Philadelphia: WB Saunders.
Kilner, TP (1937). Cleft lip and palate repair techniques. St Thomas Hosp Rep 2: 127.
Kilner, TP (1958). The management of the patient with cleft lip and/or palate. Am J Surg 93: 204.
Koberg, WR (1973). Present view on bone grafting in cleft palate. J Maxillofac Surg 1: 185.
Koop, CE (1987). Surgeon General's Report: Children with Special Health Care Needs, 184-020/65654. Washington, DC: Government Printing Office.
Kramer, GJC, Hoeksma, JB, Prahl-Andersen, B (1996). Prediction of early palatal growth and development in children with cleft lip and palates. Cleft Palate Craniofac J 33: 112.
Laatikainen, T, Ranta, R, Nordstrom, R (1996). Craniofacial morphology in twins with cleft lip and palate. Cleft Palate Craniofac J 33: 96.
Laspos, CP, Kyrkanides, S, Moss, ME, et al. (1997). Mandibular and maxillary asymmetry in individuals with unilateral cleft lip and palate. Cleft Palate Craniofac J 34: 232.
Latham, FA (1993). The anatomy of cupid's bow in normal and cleft lip. Plast Reconstr Surg 92: 404.
Lebert, L (1962). Growth change of the palate. J Dent Res 41: 1391.
LeBlanc, SM, Golding-Kushner, KJ (1992). Effect of glossopexy on speech sound production in Robin sequence. Cleft Palate Craniofac J 29: 239.
Lehman, JA, Fishman, JRA, Neiman, GS (1995). Treatment of cleft palate associated with Robin sequence: appraisal of risk factors. Cleft Palate Craniofac J 32: 25.
LeMesurier, AB (1955). Quadrilateral Mirault flap operation. Plast Reconstr Surg 16: 425.
Leonard, BJ, Brust, JD, Abrahams, G, et al. (1991). Self-concept of children and adolescents with cleft lip and/or palate. Cleft Palate Craniofac J 28: 347.
Lohmander-Agerskov, A, Dotevall, H, Lith, A, et al. (1996). Speech and velopharyngeal function in children with an open residual cleft in the hard palate, and the influence of temporary covering. Cleft Palate Craniofac J 33: 324.
Longaker, MT, Stern, M, Lorenz, HP, et al. (1992). A model for fetal cleft lip repair in lambs. Plast Reconstr Surg 90: 750.
Maher, W (1977). Distribution of palatal and other arteries in cleft and non-cleft human palates. Cleft Palate J 14: 1.
Marsh, JL (1996). Craniofacial surgery: the experiment on the experiment of nature. Cleft Palate Craniofac J 33: 1.
Marsh, JL, Wray, RC (1980). Speech prosthesis versus pharyngeal flap: a randomized evaluation of the management of velopharyngeal incompetence. Plast Reconstr Surg 65: 592.
McCance, A, Roberts-Harry, D, Sherriff, M, et al. (1993). Sri Lankan cleft lip and palate study model analysis: clefts of the secondary palate. Cleft Palate Craniofac J 30: 227.
McComb, H (1985). Primary correction of unilateral cleft lip nasal deformity: a 10-year review. Plast Reconstr Surg 75: 791.
McComb, H (1990). The nasal deformity in clefts. In: Kernahan DA, Rosenstein SW (eds): Cleft Lip and Palate: A System of Management, edited by DA Kernahan and SW Rosenstein. Baltimore: Williams and Wilkins, pp. 68–73.
McComb, H (1994). Primary repair of the bilateral cleft lip nose: a 4-year review. Plast Reconstr Surg 94: 37.
McComb, HK, Coghlan, BA (1996). Primary repair of the unilateral cleft lip nose: completion of a longitudinal study. Cleft Palate Craniofac J 33: 23.
Millard, DR, Jr (1957). A primary camouflage in the unilateral harelip. In: Transactions of the International Congress of Plastic Surgeons. Baltimore: Williams and Wilkins, p. 160.
Millard, DR, Jr (1960). Complete unilateral clefts of the lip. Plast Reconstr Surg 25: 595.
Millard, DR, Jr (1964). Refinements in rotation-advancement cleft lip technique. Plast Reconstr Surg 33: 26.
Millard, DR (1967). Bilateral cleft lip and a primary forked flap: a preliminary report. Plast Reconstr Surg 30: 50.
Millard, DR, Jr (1976a). A preliminary adhesion. In: Cleft Craft. The Unilateral Deformity, Vol. 1, edited by DR Millard. Boston: Little, Brown, pp 17–51.
Millard, DR, Jr (1976b). How to rotate and advance in a complete cleft. In: Cleft Craft. The Unilateral Deformity, Vol. 1, edited by DR Millard. Boston: Little, Brown, pp. 449–486.
Millard, DR, Jr (1980). Cleft Craft: The Evolution of Its Surgery. Alveolar and Palatal Deformities, Vol. 3. Boston: Little, Brown.
Millard, DR, Jr, Batstone, J, Heycock, M, et al. (1970). Ten years with the palatal island flap. Plast Reconstr Surg 46: 540.
Millard, DR, Jr, Latham, RA (1990). Improved surgical and dental treatment of clefts. Plast Reconstr Surg 86: 856.
Mohler, LR (1987). Unilateral cleft lip repair. Plast Reconstr Surg 80: 511.
Moos, KF (1997). Mandibular reconstruction in children with obstructive sleep apnea due to micrognathia. Plast Reconstr Surg 100: 1138.
Morris, H, Bardach, J, VanDermark, D, et al. (1989). Results of twoflap palatoplasty with regard to speech production. Eur J Plast Surg 12: 19.
Morris, HL (1973). Velopharyngeal competence and primary cleft palate surgery, 1960-1971: a critical review. Cleft Palate J 10: 62.
Morris, HL, Bardach, J, Jones, D, et al. (1995). Clinical results of pharyngeal flap surgery: the Iowa experience. Plast Reconstr Surg 95: 652.
Motohashi, N, Kuroda, T, Filho, LC, et al. (1994). P-A cephalometric analysis of non-operated adult cleft lip and palate. Cleft Palate Craniofac J 31: 193.
Moyson, F (1961). A plea against tracheotomy in the Pierre Robin's syndrome. Br J Plast Surg 14: 187.
Mulliken, JB (1995). Bilateral complete cleft lip and nasal deformity: an anthropometric analysis of staged to synchronous repair. Plast Reconstr Surg 96: 9.
Mulliken, JB, Pensler, JM, Kozakewich, HPW (1993). The anatomy of cupid's bow in normal and cleft lip. Plast Reconstr Surg 92: 395.
Nelson, CL, Chemello, PD, Jones, JE, et al. (1988). The effect of primary alveolar cleft bone grafting on facial growth. J Oral Maxillofac Surg 46: 33.
Nguyen, PN, Sullivan, PK (1993). Issues and controversies in the management of cleft palate. Clin Plast Surg 20: 671.
Nique, T, Fonseca, RJ, Upton, LG, et al. (1987). Particulate allogeneic bone grafts into maxillary alveolar clefts in humans: a preliminary report. J Oral Maxillofac Surg 45: 386.
Nylen, B, Korlof, B, Arnander, C, et al. (1974). Primary, early bone grafting in complete clefts of the lip and palate. Scand J Plast Reconstr Surg 8: 79.
Orticochea, M (1968). Construction of a dynamic muscle sphincter in cleft palate. Plast Reconstr Surg 41: 323.
Orticochea, M (1984). A rationale for modifying the site of insertion of the Orticochea pharyngoplasty. Plast Reconstr Surg 73: 892.
Peat, BG, Albery, EH, Jones, K, et al. (1994). Tailoring velopharyngeal surgery. The influence of etiology and type of operation. Plast Reconstr Surg 93: 948.
Perko, MA (1979). Two-stage closure of cleft palate. J Maxillofac Surg 7: 76.
Perlman, C, Robin, P (1992). A personal diary. Cleft Palate Craniofac J 29: 201.
Peterson-Falzone, SJ (1990). A cross-sectional analysis of speech results following palatal closure. In: Multidisciplinary Management of Cleft Lip and Palate, edited by J Bardach and HL Morris. Philadelphia: WB Saunders, pp. 750–757.
Peterson-Falzone, SJ (1995). Speech outcomes in adolescents with cleft lip and palate. Cleft Palate Craniofac J 32: 125.
Pigott, RW (1974). The results of nasopharyngoscopic assessment of pharyngoplasty. Scand J Plast Reconstr Surg 8: 148.
Poole, R, Farnworth, TK (1994). Preoperative lip taping in the cleft lip. Ann Plast Surg 32: 243.
Posnick, JC (1991a). Orthognathic surgery in cleft patients treated by early bone grafting. Plast Reconstr Surg 87: 840.
Posnick, JC (1991b). Orthognathic surgery in the cleft patient. In: Instructional Courses. Plastic Surgery Education Foundation, Vol. 4, edited by RC Russel. St. Louis: Mosby-Year Book, pp. 129–157.
Posnick, JC (2000a). The staging of cleft lip and palate reconstruction: infancy through adolescence. In: Craniofacial and Maxillofacial Surgery in Children and Young Adults, edited by JC Posnick. Philadelphia: WB Saunders.
Posnick, JC (2000b). Cleft lip and palate: bone grafting and management of the residual oronasal fistula. In: Craniofacial and Maxillofacial Surgery in Children and Young Adults, edited by JC Posnick. Philadelphia: WB Saunders.
Posnick, JC (2000c). Cleft-orthognathic surgery: the unilateral cleft lip and palate deformity. In: Craniofacial and Maxillofacial Surgery in Children and Young Adults, edited by JC Posnick. Philadelphia: WB Saunders.
Posnick, JC (2000d). Cleft-orthognathic surgery: the bilateral cleft lip and palate deformity. In: Craniofacial and Maxillofacial Surgery in Children and Young Adults, edited by JC Posnick. Philadelphia: WB Saunders. pp. 908–950.
Posnick, JC (2000e). Cleft-orthognathic surgery: the isolated cleft palate deformity. In: Craniofacial and Maxillofacial Surgery in Children and Young Adults, edited by JC Posnick. Philadelphia: WB Saunders. pp. 951–980.
Posnick, JC, Getz, SB, Jr (1987). Surgical closure of end-stage palatal fistulas using anteriorly-based dorsal tongue flaps. J Oral Maxillofac Surg 45: 907.
Posnick, JC, Tompson, B (1992). Modification of the maxillary Le Fort I osteotomy in cleft-orthognathic surgery: the unilateral cleft lip and palate deformity. J Oral Maxillofac Surg 50: 666.
Posnick, JC, Tompson, B (1993). Modification of the maxillary Le Fort I osteotomy in cleft-orthognathic surgery: the bilateral cleft lip and palate deformity. J Oral Maxillofac Surg 51: 2.
Poswillo, D (1968). The aetiology and surgery of cleft palate with micrognathia. Ann R Coll Surg Engl 43: 61.
Proffitt, WR (1991). Orthodontic treatment of clefts: yesterday, today and tomorrow. In: Proceedings of the 48th Annual Meeting, American Cleft Palate-Craniofacial Association, Hilton Head, South Carolina, March 1991, p. 32.
Pruzansky, S (1955). Factors determining arch form in cleft of the lip and palate. Am J Orthod 41: 827.
Pruzansky, S (1964). Pre-surgical orthopaedics and bone grafting for infants with cleft lip and palate: a dissent. Cleft Palate J 1: 154.
Pruzansky, S (1969). Not all dwarfed mandibles are alike. Birth Defects 5: 120.
Pruzansky, S, Richmond, JB (1954). Growth of the mandible in infants with micrognathia. Am J Dis Child 88: 29.
Randall, P (1965). A lip adhesion operation in cleft lip surgery. Plast Reconstr Surg 35: 371.
Randall, P, Whitaker, LA, Noone RB, Jones, WD. The case for the inferiorly based pharyngeal flap. Cleft Palate Craniofac J. 1978; 15(3):262-5.
Randall, P (1990). Long-term results with the triangular flap technique for unilateral cleft lip repair. In: Multidisciplinary Management of Cleft Lip and Palate, edited by J Bardach and H Morris. Philadelphia: WB Saunders, p. 173.
Randall, P (1995). Augmentation of the free border of the lip in cleft patients using temporoparietal fascia. Plast Reconstr Surg 95: 789.
Randall, P (1965). Pierre Robin and the syndrome that bears his name. Cleft Palate J 2: 237.
Randall, P, Larossa, DD, Fakhraee, SM, et al. (1983). Cleft palate closure at 3 to 7 months of age: a preliminary report. Plast Reconstr Surg 71: 624.
Rehrmann, AH (1971). The effects of early bone grafting on the growth of the upper jaw in cleft lip and palate children: a computer evaluation. Minerva Chir 26: 874.
Ren, Y-F, Wang, G-H (1993). A modified palatopharyngeous flap operation and its application in the correction of velopharyngeal incompetence. Plast Reconstr Surg 91: 612.
Richman, LC, Eliason, M (1982). Psychological characteristics of children with cleft lip and palate: intellectual achievement, behavioral and personality variables. Cleft Palate J 19: 249.
Richman, LC, Holmes, CS, Eliason, MJ (1985). Adolescents with cleft lip and palate: self-perceptions of appearance and behavior related to personality adjustment. Cleft Palate J 22: 93.
Rintala, A, Ranta, R, Stegars, T (1984). On the pathogenesis of cleft palate in the Pierre Robin syndrome. Scand J Plast Reconstr Surg 18: 237.
Riski, JE (1979). Articulation skills and oral—nasal resonance in children with pharyngeal flaps. Cleft Palate J 16: 421.
Riski, JE (1995). Speech assessment of adolescents. Cleft Palate J 32: 109.
Riski, JE (1996). Speech outcome following palatoplasty in primary school children: do lay peer observers agree with speech pathologists? Plast Reconstr Surg 98: 966.
Riski, JE (1997a). Principles of speech pathology in the cleft lip and palate child. In: Georgiade Plastic, Maxillofacial and Reconstructive Surgery, 3rd ed., edited by GS Georgiade, R Riefkohl and LS Levin. Philadelphia: JB Lippincott.
Riski, JE (1997b). Secondary surgical procedures to correct postoperative velopharyngeal incompetencies found after primary palatoplasties. In: Communicative Disorders Related to Cleft Lip and Palate, 4th ed., edited by KR Bzoch. Austin, TX: Pro-Ed, p. 121.
Riski, JE, DeLong, E (1984). Articulation development in children with cleft lip/palate. Cleft Palate J 21: 57.
Riski, JE, Hoke, JA, Dolan, EA (1989). The role of pressure flow and endoscopic assessment in successful palatal obturator revision. Cleft Palate J 26: 56.
Riski, JE, Ruff, GL, Georgiade, GS, et al. (1992a). Evaluation of failed sphincter pharyngoplasties. Ann Plast Surg 28: 545.
Riski, JE, Ruff, GL, Georgiade, GS, et al. (1992b). Evaluation of the sphincter pharyngoplasty. Cleft Palate Craniofac J 29: 254.
Riski, JE, Serafin, D, Rictkohl, R, et al. (1984). A rationale for modifying the site of insertion of the Orticochea pharyngoplasty. Plast Reconstr Surg 73: 882.
Roberg, W, Koblin, I (1973). Speech development and maxillary growth in relation to technique and timing of palatoplasty. J Maxillofac Surg 1: 44.
Robertson, NR, Jolleys, A (1968). Effects of early bone grafting in complete clefts of the lip and palate. Plast Reconstr Surg 42: 414.
Robin, P (1923). La chute de la base de la langue consideree comme une nouvelle cause de gene dans la respiration naso-pharyngienne. Bull Acad Med (Paris) 89: 37.
Robin, P (1934). Glossoptosis due to atresia and hypotrophy of the mandible. Am J Dis Child 48:541.
Robinow, M, Johnson, GF, Apesos, J (1986). Robin sequence and oligodactyly in mother and son. Am J Med Genet 25: 293.
Rohrich, RJ, Rowsell, AR, Johns, DF, et al. (1996). Timing of hard palatal closure: a critical long-term analysis. Plast Reconstr Surg 98: 236.
Rose, W (1976). Harelip and Cleft Palate. London: HK Lewis.
Rosenstein, S, Dado, DV, Kernahan, D, et al. (1991a). The case for early bone grafting in cleft lip and palate: a second report. Plast Reconstr Surg 87: 644.
Rosenstein, SW, Kernahan, D, Dado, D, et al. (1991b). Orthognathic surgery in cleft patients treated by early bone grafting. Plast Reconstr Surg 87: 835.
Rosenstein, SW, Monroe, CW, Kernahan, DA, et al. (1982). The case for early bone grafting in cleft lip and cleft palate patients. Plast Reconstr Surg 70: 297.
Ross, RB, Johnston, MC (1972). Cleft Lip and Palate. Baltimore: William and Wilkins.
Ross, RB, MacNamera, MC (1994). Effect of presurgical infant orthopedics on facial esthetics in complete bilateral cleft lip and palate. Cleft Palate Craniofac J 31: 68.
Ross, DA, Witzel, MA, Armstrong, DC, et al. (1996). Is pharyngoplasty a risk in velocardiofacial syndrome? An assessment of medially displaced carotid arteries. Plast Reconstr Surg 98: 1182.
Rudman, RA (1997). Prospective evaluation of morbidity associated with iliac crest harvest for alveolar cleft grafting. J Oral Maxillofac Surg 55: 219.
Sandham, A, Murray, JAM (1993). Nasal septal deformity in unilateral cleft lip and palate. Cleft Palate Craniofac J 30: 222.
Schimke, RN, Collins, DL, Hiebert, JM (1993). Congenital nonprogressive myopathy with Mobius and Robin sequence: the Carey- Fineman-Ziter syndrome. A confirmatory report. Am J Med Genet 46: 721.
Schrander-Stumpel, C, Fryns, JP, Beemer, FA, et al. (1991). Association of distal arthrogryposis, mental retardation, whistling face, and Pierre Robin sequence: evidence for nosologic heterogeneity. Am J Med Genet 38: 557.
Schreiner, RL, McAlister, WH, Marshall, RE, Shearer, WT (1973). Stickler syndrome in a pedigree of the Pierre Robin syndrome. Am J Dis Child 126: 86.
Schweckendiek, W (1978). Primary veloplasty: long-term results without maxillary deformity. A twenty-five year report. Cleft Palate J 15: 268.
Semb, G (1991). A study of facial growth in patients with bilateral cleft lip and palate treated by the Oslo CLP team. Cleft Palate Craniofac J 28: 22.
Shaw, WC, Asher-McDade, C, Brattshrtom, V, et al. (1992). The RPS: a six-centre international study of treatment outcome in patients with clefts of the lip and palate: Part 5. General discussion and conclusions. Cleft Palate Craniofac J 29: 413.
Shaw, WC, Semb, G (1990). Current approaches to the orthodontic management of cleft lip and palate. J R Soc Med 83: 30.
Sher, AE (1992). Mechanisms of airway obstruction in Robin sequence: implications for treatment. Cleft Palate Craniofac J 3: 224.
Shprintzen, RJ (1992). The implications of the diagnosis of Robin sequence. Cleft Palate Craniofac J 3: 205.
Shprintzen, RJ (1990). Conceptual framework for pharyngeal flap surgery. In: Multidisciplinary Management of Cleft Lip and Palate, edited by J Bardach and HL Morris. Philadelphia: WB Saunders.
Shprintzen, RJ, Bardach, J (1995a). Communicative impairment associated with clefting. In: Cleft Palate Speech Management: A Multidisciplinary Approach. St. Louis: Mosby Year Book, p. 137.
Shprintzen, RJ, Bardach, J (1995b). The use of information obtained from speech and instrumental evaluations in treatment planning for velopharyngeal insufficiency. In: Cleft Palate Speech Management: A Multidisciplinary Approach. St. Louis: Mosby Year Book, p 257.
Shprintzen, RJ, Golding-Kushner, K (1989). Evaluation of velopharyngeal insufficiency. Otolaryngol Clin North Am 22: 519.
Shprintzen, RJ, Lewin, ML, Croft, CB, et al. (1979). A comprehensive study of pharyngeal flap surgery: tailor-made flaps. Cleft Palate J 16:46.
Shprintzen, RJ, Sher, AE, Croft, CB (1987). Hypernasal speech caused by hypertrophic tonsils. J Pediatr Otorhinolaryngol 14: 45.
Shukowsky, WP (1911). Zur Atiologie des Stridor inspiratorius congenitus. Z Kinderheilkd 73: 459.
Siegel-Sardewitz, VL, Shprintzen, RJ (1986). Changes in velopharyngeal valving with age. Int J Pediatr Otorhinolaryngol 11: 171.
Sindet-Pedersen, S, Enemark, H (1990). Reconstruction of alveolar clefts with mandibular or iliac crest bone graft: a comparative study. J Oral Maxillofac Surg 48: 554.
Sirois, M, Caouette-Laberge, L, Spier, S, et al. (1994). Sleep apnea following a pharyngeal flap: a feared complication. Plast Reconstr Surg 93: 943.
Skoog, T (1965). The use of periosteal flaps in the repair of the primary palate. Cleft Palate J 2: 332.
Skoog, T (1969). Repair of unilateral cleft lip deformity. Maxilla, nose and lip. Scand J Plast Reconstr Surg 3: 109.
Slutsky, H (1969). Maternal reaction and adjustment to birth and care of cleft palate child. Cleft Palate J 6: 425.
Smith, JL, Stowe, FR (1961). The Pierre Robin syndrome (glossoptosis, micrognathia, cleft palate): a review of 39 cases with emphasis on associated ocular lesions. Pediatrics 27: 128.
Stoll, C, Kieny, JR, Dott, B, et al. (1992). Ventricular extrasystoles with syncopal episodes, perodactyly, and Robin sequence in three generations: a new inherited MCA syndrome? Am J Med Genet 42: 480.
Strauss, RP (1994). Health policy and craniofacial care: issues in resource allocation. Cleft Palate Craniofac J 31: 78.
Sullivan, WG, Hedrick, MH, Rice, HE, et al. (1996). Delayed in utero repair of surgically created fetal cleft lip and palate. Plast Reconstr Surg 97; 906.
Takato, T, Yonehara, Y, Mori, Y, et al. (1995a). Early correction of the nose in unilateral cleft lip patients using an open method: a 10-year review. J Oral Maxillofac Surg 53: 28.
Takato, T, Yonehara, Y, Mori, Y, et al. (1995b). Columella lengthening using a cartilage graft in the bilateral cleft lip-associated nose: choice of cartilage according to age. J Oral Maxillofac Surg 53: 149.
Tennison, C (1952). The repair of the unilateral cleft lip by the stencil method. Plast Reconstr Surg 9: 115.
Thompson, JE (1912). An artistic and mathematically accurate method of repairing the defect in cases of harelip. Surg Gynecol Obstet 14: 498.
Trier, WC (1995). Bilateral complete cleft lip and nasal deformity: an anthropometric analysis of staged to synchronous repair. Plast Reconstr Surg 96: 24.
Trotman, C-A, Ross, RB (1993). Craniofacial growth in bilateral cleft lip and palate: ages six years to adulthood. Cleft Palate Craniofac J 30: 261.
Troxell, JB, Fonseca, RJ, Osbon, DB (1982). A retrospective study of alveolar cleft grafting. J Oral Maxillofac Surg 40: 721.
Turner, G (1974). The Stickler syndrome in a family with the Pierre Robin syndrome and severe myopia. Aust Paediatr J 10: 103.
Turvey, TA, Vig, K, Moriarty, J, et al. (1984). Delayed bone grafting in the cleft maxilla and palate: a retrospective multidisciplinary analysis. Am J Orthod 86:244.
Upton, LG (1993). The double-reversing Z-plasty in primary palatoplasty: operative experience and early results. J Oral Maxillofac Surg 51: 149.
Van Boven, MJ, Pendeville, PE, Veyckemans, F, et al. (1993). Neonatal cleft lip repair: the anesthesiologist's point of view. Cleft Palate Craniofac J 30: 574.
van der Meulin, JC (1992). Columellar elongation in bilateral cleft lip repair: early results. Plast Reconstr Surg 59: 6.
Veau, V (1931). Division Palatine. Paris: Masson, pp. 6-8, 51–53.
von Langenbeck, B (1861). Operation der angeborenen totalen Spaltung des harten Gaumens nach einer neuen Methode. Dtsch Klin 8: 231.
Waite, DE, Kersten, RB (1980). Residual alveolar and palatal clefts. In: Surgical Correction of Dentofacial Deformities, edited by WH Bell, WR Proffit, and RP White Jr. Philadelphia: WB Saunders, p. 1335.
Wardill, W (1937). The technique of operation for cleft palate. Br J Surg 25: 117.
Wardill, WFM (1928). Cleft palate: results of operation for cleft palate. Br J Plast Surg 16: 127.
Warren, DW (1975). The determination of velopharyngeal incompetency by aerodynamic and acoustical techniques. Clin Plast Surg 2: 299–304.
Warren, DW (1994). Should velopharyngoplasty and tonsillectomy in the cleft palate child be performed simultaneously? J Oral Maxillofac Surg 52: 930.
Warren, DW, Dalston, RM, Mayo, R (1994). Hypernasality and velopharyngeal impairment. Cleft Palate Craniofac J 31: 257.
Witt, PD, Marsh, JL, Marty-Grames, L, et al. (1995). Management of the hypodynamic velopharynx. Cleft Palate Craniofac J 32: 179.
Witt, PD, Marsh, JL, Muntz, HR, et al. (1996). Acute obstructive sleep apnea as a complication of sphincter pharyngoplasty. Cleft Palate Craniofac J 33: 183.
Witt, PD, O'Daniel, TG, Marsh, JL, et al. (1997). Surgical management of velopharyngeal dysfunction: outcome analysis of autogenous posterior pharyngeal wall augmentation. Plast Reconstr Surg 99: 1287.
Witzel, MA, Salyer, KE, Ross, RB (1984). Delayed hard palate closure: the philosophy revisited. Cleft Palate J 21: 263.
Witzel, MA, Tobe, J, Salyer, KE (1989). The use of videonasopharyngoscopy for biofeedback therapy in adults after pharyngeal flap surgery. Cleft Palate J 26: 129.
Wolford, LM, Oelschlaeger, M, Deal, R (1989). Proplast as a pharyngeal wall implant to correct velopharyngeal insufficiency. Cleft Palate J 26: 119.
Wood, RJ, Grayson, BH, Cutting, CB (1997). Gingivoperiosteoplasty and midfacial growth. Cleft Palate Craniofac J 34: 17.
Ysunza, A, Garcia-Velasco, M, Garcia-Garcia, M, et al. (1993). Obstructive sleep apnea secondary to surgery for velopharyngeal insufficiency. Cleft Palate Craniofac J 30: 387.