Andrew E. Czeizel
Oral clefts (OCs) are among the most extensively studied congenital abnormalities (CAs) due to their visibility, which frequently causes serious psychological problems, and their common occurrence (1/500-550 births). CAs including OCs represent a distinct category of disorders because of their early (prenatal) onset without a good chance of spontaneous or medically assisted complete recovery. Thus, prevention of OCs is the optimal solution.
Several maternal and environmental factors have been studied in relation to OCs, and some have possible associations (Wyszynszki and Beaty, 1996). Among maternal factors, epilepsy and/or use of antiepileptic drugs such as phenytoin appear to be important. Many studies have proposed an association between acute viral infections and OCs; however, viruses, medications, hyperthermia, and other related factors are questionable. Drugs such as corticosteroids, ampicillin, metrodinazole, and folate antagonists are potential teratogens in the etiology of OCs as well. Maternal cigarette smoking and alcohol consumption may also have a role as co-teratogens through gene-environment interaction. Pesticides/herbicides, water contaminants, and occupational exposures have been cited as possible causes of OCs, but they probably explain only a small portion of cases. Currently, nutritional factors such as folate deficiency appear to be the most relevant, according to the concept of gene-environment interaction, in the etiology of OCs.
This chapter reviews the primary prevention of OCs through the use of folic acid and multivitamin supplements, with emphasis on our Hungarian studies. “Secondary” prevention of OCs (through the use of high-resolution ultrasound scanning or other diagnostic methods for fetal OCs, followed by elective termination of pregnancy) is not acceptable (the manifestation of OCs in holoprosencephaly or other very severe syndromes may be an exception), and this topic is beyond the scope of this chapter. Possible in utero surgical correction or gene therapy of OCs is premature (Zanjani and Anderson, 1999).
Classification of Oral Clefts in Hungary
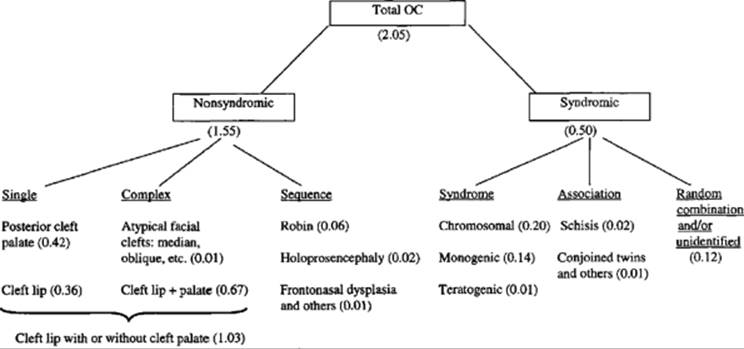
The findings of three Hungarian studies on the primary prevention of OCs will be presented in this chapter, however, before this I summarize our previous Hungarian activities in the research of OCs which explain our classification of OCs. Ascertainment of cases in ad hoc population-based epidemiological studies was based on an active search of all available sources of cases, and on information on the racially homogeneous Hungarian births (Czeizel and Tusnády, 1971, 1972; Czeizel and Nagy, 1986; Czeizel et al., 1986). In addition, the population-based Hungarian Congenital Abnormality Registry, which represents nearly total notification of OC cases thanks to the obligatory reporting system (Czeizel, 1997; Czeizel and Hirschberg, 1997) was used. The classification of OCs and birth prevalences of different OC entities per 1000 total births are shown in Figure 35.1.
|
|
|
FIG. 35.1. Classification of oral clefts (OCs) and birth prevalences of different OC entities per 1000 total births (in parentheses) in Hungary during the 1980s. |
The different origins of posterior cleft palate (CP) and cleft lip with or without cleft palate (CL/P) were shown in the classical work of Fogh-Andersen (1942) and confirmed in our population-based Hungarian epidemiological studies (Table 35.1). Later, it was necessary to differentiate CP and Robin sequence (RS) due to their different origins and clinical manifestations (Table 35.1). A pathogenetic distinction should also be made between isolated, “nonsyndromic” OCs (which are likely due to a localized error of morphogenesis) and multiple, “syndromic” OC (a co-ocurrence of two or more different morphogenetic errors in the same person, i.e., OC not part of a sequence) (Czeizel et al.,1988). The difference between nonsyndromic and syndromic CL/P is clearly illustrated by the epidemiological, clinical, and genetic data (Table 35.2). The syndromic CL/P group comprises chromosomal, mendelian-monogenic, and teratogenic CA-syndromes which include OCs as component element. The origin of nonsyndromic CL/P corresponds to the Gaussian multifactorial threshold model (proportion of heritability 72 ± 14%) (Czeizel and Tusnády, 1984), while that of nonsyndromic CP and RS is also heterogeneous, with a certain proportion of mendelian-monogenic entities (Czeizel and Tusnády, 1972; Czeizel et al., 1986).
The prevalence at birth of OCs in Hungary was 2.05/1000 total births in the 1980s. About three- quarters (1.55/1000, or 76%) were nonsyndromic. The most common categories were CL/P (1.03/1000) and CP (0.42/1000) (Fig. 35.1). These prevalences seem higher than those reported internationally (Tolarova and Cervenka, 1998). This may be due to bias from ascertainment, classification, and certain population characteristics.
|
TABLE 35.1. Different Features of Nonsyndromic Cleft Lip with or without Cleft Palate (CL/P), Posterior Palate (CP), and Robin Sequence (RS) Based on Hungarian Studies (Czeizel, Tusnády, 1971, 1972; Czeizel et al, 1986) |
|||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||
|
TABLE 35.2. Different Features of Nonsyndromic and Syndromic Cleft Lip with or without Palate Based on Hungarian Studies (Czeizel and Tusnády, 1971; Czeizel et al., 1988) |
|||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||
Animal Studies
Treatment of individuals with OCs has improved considerably in recent decades. Nevertheless, the optimal solution is primary prevention. This requires knowledge of causes. The role of dietary deficiencies in the origin of OCs was suggested as early as 1914, when Strauss observed 32 jaguars with CP from one dam by the same sire (Strauss, 1914). When he changed their inadequate diet to fresh meat, no further offspring were born with CP from the same two parents. Pickerill (1914) reported a 99% occurrence of CP in lion cubs born at the zoo. A significant decrease of CP was achieved after the lionesses received a better diet in early pregnancy. In animal studies, the pioneers of teratology (Warkany and Nelson, 1940; Nelson et al., 1952, 1955) induced OCs in more than 90% of rats whose mothers had transitory folk acid deficiency during days 9 through 11 of gestation due to an antimetabolite. Their findings have been confirmed (Lidral et al., 1991). The rate of OCs was reduced in animal experiments by prophylactic vitamins, particularly vitamin B1 (Schinke et al., 1976; Kreybig, 1981). Bienengräber et al. (1997), however, did not confirm these findings. Peer et al. (1958a) reduced the teratogenic effect of cortisone in mice by administering vitamin B6, folic acid, or both. In addition, maternal folate supplementation reduced ethanol teratogenicity in CP-susceptible strains of mice (Sakanashi et al., 1996). Finally, folinic acid (the most stable intermediate of folic acid metabolism) reduced the occurrence of OCs in A/WySN mice (Paros and Beck, 1999).
Human Studies of Recurrence
The data of previous human intervention studies on the efficacy of vitamins in the reduction of recurrent OCs are summarized in Table 35.3. Conway (1958) used B vitamins together with vitamins A, C, and D. Of 87 women who had already had one child with an OC, 48 received no vitamin supplementation during their 78 subsequent pregnancies and four cases with OC (two CL/P and two CP) were seen among their children. The 39 remaining women were supplemented with the above vitamins during the first trimester of 59 subsequent pregnancies and no recurrent OCs were found (p = 0.078). Peer et al. (1958b, 1964) gave 5 mg of folic acid, 10 mg of vitamin B6, or both to mothers who had previously given birth to children with CL/P at the first suspicion of pregnancy through the fourth month. Of 176 women with this supplementation, four (2.3%) had children with CL/P compared with 19 of 418 women (4.5%) without vitamin supplementation [relative risk 0.5, 95% confidence interval (CI) 0.2-1.4]. Briggs (1976) supplemented 348 pregnancies of 228 women who had already had a child with CL/P using a multivitamin including 0.5 mg of folic acid, and 11 (3.2%) cases of recurrent CL/P were found. Among the control group of 417 women who also had a CL/P child but did not take supplemental vitamins during their subsequent pregnancies, the recurrent CL/P rate was 4.8% (p = 0.30). Tolarova (1982) highlighted the possible primary prevention of CL/P by folic acid and other vitamins in a prospective study of healthy women living mainly in Bohemia who had had one child with unilateral CL/P. These women were encouraged to take three tablets of a multivitamin (Table 35.4) and 10 mg of folic acid per day for at least 3 months before conception and to continue taking these tablets at least until the end of the first trimester of pregnancy. Most of the women also received supplemental iron (75 mg/day of ferrum II fumaricum) and additional vitamin B6 (1 mg/day). Among 84 pregnancies of 80 fully supplemented women, one (1.2%) recurrence was reported compared with 15 recurrences among 206 pregnancies of 202 women without supplementation (7.4%) (p = 0.023). The supplemented and unsupplemented groups also experienced one and six miscarriages, respectively, not included in the data. The frequency of CL/P in the control group, however, was higher than the 4.1% risk for uni-or bilateral CL/P calculated from 2487 sibships in the total Bohemian data set. Tolarova (1987) reported cumulative findings (including data from the 1982 study) that continued to show a significant reduction of recurrent CL/P associated with use of a multivitamin and a very high dose of folic acid supplementation during the periconceptional period. Later, the data set of all subtypes of CL/P, collected from 1970 through 1982, was re-evaluated by Tolarova and Harris (1995). From a group of 2115 women with one previous child with nonsyndromic CL/P, 214 pregnancies were supplemented and three (1.4%) recurrent CL/P cases occurred. However, of 1901 pregnancies without supplementation, 77 (4.1%) ended again with the birth of infants with CL/P (p = 0.03). When the supplemented group was divided according to sex and severity, the biggest reduction was found in the group of male probands with unilateral CL (this subgroup had the lowest heritability value and, thus, the largest proportion of environmental factors).
|
TABLE 35.3. Data of Intervention Studies to Check the Efficacy of Vitamins Including Folic Acid in Early Pregnancy for the Reduction of Recurrent Oral Clefts (OC) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
TABLE 35.4. Component of Multivitamin Spofavit® Used in the Studies of Tolarova (1982, 1987) and Tolarova and Harris (1995) in Addition to Components of Elevit Pronatal® Used in the Hungarian Intervention Studies |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
These studies, however, were not randomized, and the possible effect of folic acid could not be distinguished from the possible effect of other vitamins. In addition, both the dose (0.5-10.0 mg) and the design (prospective or retrospective) were different. In general, the observed protective effect did not reach statistical significance (except in the Bohemian data set), but the trend was similar. However, starting vitamins before conception could just as easily be a marker for general health consciousness. Thus, there were two significant goals for further studies. First, it was necessary to organize a double-blind randomized controlled trial (RCT). Second, the reduction of recurrent OCs is important from the aspect of these families, but about 95% of OCs manifested as a first occurrence; therefore, the reduction of first occurrences would be of great public health benefit.
The Hungarian Randomized Controlled Trial
One of the major objectives of the Hungarian RCT of periconceptional folic acid-containing multivitamin supplementation (PFMS) was to evaluate whether multi vitamins including 0.8 mg of folic acid can reduce the first occurrence of nonsydromic CL/P and CP. The RCT was based on the periconceptional care program in Hungary (Czeizel et al., 1998; Czeizel, 1999), established in 1984. To be eligible to participate, women planning a pregnancy had to satisfy the following criteria: no infertility, no current pregnancy, and voluntary appearance. Qualified nurses supervised the three steps: checkup of reproductive health, a 3-month preparation period for conception, and better protection of early pregnancy before the usual prenatal care. Supplementation was part of the periconceptional care.
The RCT took place between February 1, 1984, and April 30, 1992. At the first periconceptional care visit, the criteria for eligibility were reviewed. Eligible women were informed about the purpose of the RCT and asked whether they agreed to be randomly assigned to receive a multivitamin pill or a placebo-like trace element pill. The women were then asked to provide written, informed consent and to stop taking any other vitamins. The women entering the RCT were randomly assigned to receive a multivitamin (Elevit Prenatal®; Roche, Switzerland) (Table 35.4) or a trace element supplement as a single tablet each day for at least 1 month before the planned conception. They were asked to record daily their pill taking on a form used to record their basal body temperature and to leave unused tablets in the box. At the second visit, 3 months later, women were supplied with tablets for the next 3 months, advised to attempt conception within this period, and asked to return immediately after the first missed menstrual period. The purpose of the third visit was to confirm pregnancy if a menstrual period had been missed and to supply tablets until the end of the third month of gestation. If a woman did not conceive within this 3-month period, she was given an additional 3-month supply of supplement until the end of 1 year. Compliance in taking the supplement was verified by interview, checking records of basal body temperature, and counting unused tablets. Compliance was categorized as full, partial, or none (Smithells et al., 1980). However, the intention-to-treat analysis was used to evaluate the primary end point of the RCT (Czeizel and Dudás, 1992). Each participant had a certificate with a page including the pregnancy outcome data (date and type of pregnancy outcome, sex, weight, gestational age of singletons or twins, and particularly any defects of the fetuses or newborn infants) filled in by mothers and confirmed by physicians (documented by signature), and women were asked to mail this certificate after the end of pregnancy. When a woman did not mail the certificate, considerable effort was expended to obtain information about her pregnancy outcome. This effort resulted in only 49 of 4753 (1%) confirmed pregnancies with unknown pregnancy outcomes (Czeizel et al., 1994). Informative offspring (fetuses with prenatally diagnosed conditions aborted after the week 12 of gestation, stillborn fetuses, and liveborn infants) were evaluated with particular attention to the appropriate diagnosis or description of the CA.
The data from the Hungarian RCT showed a significant reduction in the first occurrence of neural tube defects and some other CAs (Czeizel and Dudás, 1992; Czeizel, 1993a, 1996). However, the study did not show a reduction in the occurrence of nonsyndromic CL/P and CP (Table 35.5), though the statistical power of these results was small for these defects (it could detect incidence differences only on the order of 50%).
Other Human Studies of Occurrence
Khoury et al. (1989) analyzed the data of the Atlanta Birth Defects Case-Control Study. Mothers who consumed vitamins during pregnancy were at lower risk of having a child with CL/P than mothers who did not take vitamins [odds ratio (OR) 0.74, 95% CI 0.56-0.98], but a statistically significant difference was not found in the CP group (OR 0.93, 95% CI 0.62-1.40). Other studies did not find any association between vitamin use and OCs (Eraser and Warburton, 1964; Saxen, 1975; Hill et al., 1988).
Shaw et al. (1995) investigated whether use of multivitamins containing folk acid from 1 month before through 2 months after conception reduced the risk of OCs in a population-based case-control study in California, 1987–1989. The risk of nonsyndromic CL/P was reduced by half (OR 0.50, 95% CI 0.36-0.68). For CP, this reduction was smaller and not statistically significant (OR 0.73, 95% CI 0.35-1.2). However, the crude ORs for syndromic CL/P (0.61, 95% CI 0.35-1.1) and CP (0.64, 95% CI 0.35-1.2) were also lower, though not significantly. This is surprising because, as mentioned above, syndromic OCs have a different origin. Hayes et al. (1996), in a hospital-based case-control study, compared folic acid supplementation in cases with CL/P (n = 195), CP (n = 108), and 1167 patient controls with other CAs (e.g., other than OCs, such as neural tube defects and other midline defects). The adjusted relative risks for daily folic acid supplementation during the periconceptional period were 1.32 (95% CI 0.82-2.12) for CL/P and 0.89 (95% CI 0.51-1.58) for CP. However, Werler (1999), from the same research group and using the same approach with “normal” and “affected” controls, found ORs below 1.0 in both CL/P and CP groups regardless of control type. In addition, there was a statistically significant reduction in the occurrence of CP due to multivitamin use after the periconceptional period.
|
TABLE 35.5. Results of the Randomized Controlled Trial (RCT) and Two Cohort Controlled Study (TCS) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In summary, the results of studies using low doses folic acid (in general, 0.4 mg) are puzzling since they provide different findings despite using similar approaches. Thus, the effects of confounders (such as lifestyle) and other indirect causal factors should not be excluded.
The Hungarian two Cohort Controlled Study
The results of previous studies were controversial; nevertheless, the Hungarian RCT was discontinued due to ethical reasons. A two cohort controlled study (TCS) was therefore launched on May 1, 1993, and closed on April 30, 1996 (Czeizel et al., 1999). Cases were recruited from the participants with PFMS of the Hungarian periconceptional care centers after confirmation of pregnancy. They were also supplemented with Elevit Prenatal® (Table 35.4) during the same periconceptional period and using the same criteria of compliance as in the RCT. However, if a woman was pregnant at the start of PFMS, she was excluded from the TCS and referred to regional prenatal care. Matched controls were recruited during prenatal care, which is mandatory in Hungary for pregnant women. All pregnant women after the first visit between weeks 8 and 12 of gestation were informed about the purpose of the TCS and invited to take part in the region where cases were recruited. Eligibility of controls was based on three criteria: (1) no multivitamin and/or folic acid supplementation in the periconceptional period; (2) appropriate matching of age (±1 year), socioeconomic status, and residence of supplemented pregnant women; (3) voluntary participation. If unsupplemented pregnant women were eligible for the TCS and agreed to participate, they were asked to sign an informed consent form and to personally deliver or mail their completed pregnancy certificate to the regional prenatal care center after the end of pregnancy. Each supplemented pregnant woman was matched to two unsupplemented pregnant women, the second of whom was enrolled if the first dropped out of the study.
|
TABLE 35.6. Data of Liveborn Cases with Nonsyndromic Oral Clefts from the Randomized Controlled Trial (RCT) and the Two Cohort Controlled Study (TCS) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The data of CAs including OCs were evaluated in 3056 case-control matched pairs. Birth order was lower in the supplemented group (1.2 ± 0.6) due to the larger proportion of women planning first pregnancies compared with the unsupplemented group (1.4 ± 0.7) because primiparous females preferred to take part in periconceptional care. Fetal deaths, infant deaths, and CAs in previous pregnancies were more common among supplemented than unsupplemented women. These differences can be explained by the expected higher medical standard of periconceptional care in couples with previous unsuccessful pregnancy outcomes. Of 172 malformed offspring in the previous pregnancies of supplemented women, six had OCs, while of four previous malformed offspring in the unsupplemented group, none had an OC. In addition, of 3056 case and control mothers, one and none, respectively, had an OC, while of 3056 case and control fathers, three and one, respectively, had OCs. Thus, a higher potential recurrence risk for OCs must be considered in the supplemented group than in the unsupplemented group. All OCs occurred in liveborn infants. The occurrence of CL/P and CP did not show a difference between the supplemented and unsupplemented groups (Table 35.5). One unsupplemented twin infant had RS, but in general this CA entity is included in the CP group; the other twin was healthy. There was one recurrent case of cleft lip and CP (CLP) in a newborn infant; his brother also had CLP.
The data on all infants with nonsyndromic OCs in the RCT and TCS are shown in Table 35.6. The major methodological factors were similar in the two Hungarian intervention studies (Table 35.7); however, there was a significant difference in design: the RCT was randomized among participants in the coordinating center of periconceptional care, while the TCS was nonrandomized and supplemented women were recruited in all (n = 32) periconceptional centers, while unsupplemented controls enrolled in the regional prenatal care clinics. Combination of the data from the RCT and TCS offers an opportunity to estimate the efficacy of PFMS in the reduction of the first occurrence of non-syndromic CL/P and CP (Table 35.8). (One infant in the trace element group of the RCT who had a father with CLP and one infant and his brothers who had CLP in the supplemented group of the RCT were excluded from the analysis. In addition, ten and one newborn infants with OC who had parents or previous sibs affected with OCs in the supplemented and unsupplemented groups of the TCS, respectively, were also excluded from the denominators due to a 50-fold higher recurrence risk.) There were seven and four CL/P infants in the supplemented and unsupplemented groups, respectively. In addition, there were one and three children with CP in the supplemented and unsupplemented groups, respectively. Crude ORs did not show a difference between the two groups. In addition, there was no significant difference in the first occurrence of non-syndromic CL/P (p = 0.47) and CP (p = 0.35) between the supplemented and unsupplemented groups. Thus, the data of 5516 supplemented and 5445 unsupplemented women do not indicate a protective effect of PFMS, including a physiological dose (<1 mg) of folic acid, for nonsyndromic OC.
|
TABLE 35.7. Comparison of Major Methodological Factors of the Randomized Controlled Trial (RCT) and the Two Cohort Controlled Study (TCS) |
|||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||
The so-called syndromic OCs were also evaluated (Table 35.5). There were three and two syndromic OCs in the PFMS and placebo-like trace element groups of the RCT, respectively. One and two fetuses had Edwards' or Patau's syndrome including OCs in the PFMS and placebo-like groups, respectively. Of two unidentified multimalformed cases after PFMS, one newborn was affected with RS (CP + micrognathia) and rib agenesia, while another had bilateral CLP, bilateral congenital structural talipes equinovarus, and spina bifida occulta. There were one and five syndromic OCs in the supplemented and unsupplemented groups of the TCS, respectively. Both chromosomal OCs occurred in Edwards' syndrome. In addition, four unidentified multimalformed infants were found in the unsupplemented group of the TCS: left CLP and polycystic kidney disease type IV causing hydronephrosis (Meckel syndrome?); bilateral CL + ventricular septal defect + cholecyst agenesia + mesenterium commune (one member of a triplet); CP + facial dysmorphism + syndactyly in left hand (II-V fingers) and in right hand (II-IV fingers); RS and bilateral congenital structural talipes equinovarus (the father had micrognathia and high arched palate). The limited number of syndromic OCs does not allow any conclusion; however, these findings do not appear to confirm the observation of Shaw et al. (2000) that women who used PFMS had an elevated risk of delivering a fetus or infant with multiple CAs.
|
TABLE 35.8. First Occurrence of Nonsyndromic Cleft Lip with or without Cleft Palate (CL/P) and Posterior Cleft Palate (CP) in the Previous Hungarian Randomized Double-Blind Controlled Trial (RCT) and the Two Cohort Controlled Study (TCS) with (Supplemented) or without (Unsupplemented) Folic Acid-Containing (0.8 mg) Multivitamin during the Periconceptional Period |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In conclusion, data from the two Hungarian intervention studies do not support a protective effect against nonsyndromic OCs of multivitamins including folic acid (<1 mg).
The Hungarian Case-Control Surveillance of Congenital Abnormalities
The association between oral supplement use and CA occurrence was also evaluated using a case-control approach in the population-based data from the Hungarian Case-Control Surveillance of Congenital Abnormalities (HCCSCA) between 1980 and 1991 (Czeizel et al., 1996) and between 1980 and 1996 (Czeizel et al., 1999). Cases with nonsyndromic CAs (except for congenital dislocation of the hip, congenital inguinal hernia, and hemangiomas) and multiple CAs reported to the Hungarian Congenital Abnormality Registry in the first 3 months after birth or termination of pregnancy were selected for the HCCSCA. Babies with Down syndrome were used as patient controls. The methods and data set of the above registry have been described elsewhere (Czeizel et al., 2001). Population controls were ascertained from the National Birth Registry of the Central Statistical Office. Two population controls without CAs were matched to every case according to sex, date of birth (within 1 week), and parent's residence (district).
Data on use of vitamins were obtained from three sources. First, a postpaid questionnaire with an explanatory letter and a list of drugs and diseases was mailed to parents immediately after the selection of cases and controls. The questionnaire requested information on drug intake and use of pregnancy supplements, pregnancy complications, and maternal diseases during pregnancy according to gestational month. To standardize the answers, mothers were asked to read a set of lists as a memory aid before they replied. These were lists of medications, including pregnancy supplements such as folic acid, and diseases. The mean return time of completed questionnaires was 1.6 and 3.5 months after birth for the case and population controls, respectively. Second, mothers were requested to send us the prenatal care logbook and all medical records concerning their diseases during pregnancy and the child's CA. Third, regional nurses were asked to visit and to question nonresponding families in the group of cases. Thus, information was available on 79% (69% from reply, 10% from visit) of cases. The response rate for population controls was 64%, but district nurses did not visit nonresponding population control families because the ethical committee considered this follow-up to be disturbing to the parents of these healthy children. If a case had two population controls, one was randomly excluded. If a case had no population control, another one was selected from the 38,151 population controls on the basis of matching criteria.
Folic acid intake was evaluated according to (1) source of information (maternal self-reported, medically recorded, or both), (2) type of treatment (folic acid alone or folic acid plus other drugs; multivitamins including 0.1-1.0 mg folic acid were excluded due to the small number of pregnant women in the two groups of OC), (3) dose (only one kind of folic acid tablet, 3 mg, was available during the study period, and obstetricians prescribed daily 1-3, but in general 2, tablets, i.e., 6 mg for pregnant women), (4) duration of treatment (after the start of folic acid use, it was generally continued until the end, but at least until the fourth month, of pregnancy), (5) gestational age [calculated from the first day of the last menstrual period, and three time intervals were considered: first month of pregnancy as a continuation of preconceptional treatment; the critical period for primary palatal development, i.e., 49-64 gestational (35-50 postconceptional) days in CL/P, and for secondary palatal development, i.e., 70-98 gestational (56-84 postconceptional) days in CP (Canick, 1954); gestational months after the critical period of orofacial clefts], (6) potential confounding factors (e.g., maternal age, birth order, acute and chronic maternal disorders, and use of other drugs).
At the evaluation of the HCCSCA data set between 1980 and 1996, the study period covered 2,146,574 total births in Hungary; hence, the 38,151 population controls represented 1.8% of Hungarian births. Of 22,834 cases with CA, 1377 and 600 with non-syndromic CL/P and CP, respectively, were evaluated in the case-control matched pair analysis.
Data on maternal age, birth order, pregnancy complications, maternal disorders, and use of other drugs are shown in Table 35.9. Influenza/common cold and epilepsy were more frequent in cases with CL/P or CP compared with their matched controls, while excessive nausea/vomiting was less frequent.
Pregnant women rarely (13.9%-14.8%) used folic acid alone in the two groups. Thus, folic acid alone and with other drugs were evaluated together (Table 35.10) because most other drugs, including other pregnancy supplements (other vitamins, irons, calcium derivatives), had similar occurrence rates in cases and controls. Mothers of newborn infants with CL/P had a significantly lower use of folic acid (49.4%) than mothers of matched controls (54.7%). This was the case in the CP group (47.7%) as well compared with their matched controls (55.2%). The proportion of medically recorded folic acid supplementation was similar in the combined control (65.6%) and case (64.2%) groups (X2 = 5.1, p = 0.25). However, it is worth evaluating the start of folic acid supplementation according to gestational month (Table 35.10). Folic acid was used only in a small proportion of women in the first month of gestation, which corresponded to the preconceptional supplementation. The increase of folic acid use in the second month of gestation may reflect the early visits to the prenatal care or voluntary folic acid supplementation after the recognition of pregnancy. The maximum rate was seen in the third month of gestation, at the usual time of the first visit to prenatal care. The later start of folic acid supplementation can be explained by a postponed visit to prenatal care or a delay in folic acid use. The major point is the use of folic acid before and during the time of primary and secondary palatal development. Thus, the cumulative number of pregnant women with high-dose folic acid supplementation was calculated during the critical period of CL/P and CP. However, the critical period of primary palatal development (CL/P) includes the last week of the second and the first week of the third gestational months, while secondary palatal development (i.e., CP-forming period) overlaps the last 2 weeks of the third and the first 2 weeks of the fourth gestational months. This explains why there were two estimates for the protective effect of folic acid. (The adjusted OR in case-control pairs was estimated by a conditional logistic regression model for confounding factors.) At the evaluation of primary palatal development, there was a significantly higher rate of supplementation with a high dose (in general, 6 mg/day) of folic acid during the first and second months of gestation in the matched population control group (11.7% vs. 9.0% in the case group), which may indicate a protective effect for CL/P. This was also the case at the evaluation of folic acid supplementation in the first 4 months of gestation (40.2% in matched population controls and 32.6% in cases) in the CP group. There was no difference in the use of folic acid supplementation after the critical period of these two kinds of OC between cases and matched population controls (Table 35.10).
|
TABLE 35.9. Some Variables of Total, Cleft Lip with or without Palate (CL/P), and Posterior (CP) Cases, in Addition to Comparative Values of Total, Matched CL/P, and CP Controls the Hungarian Case-Control Surveillance of Congenital Abnormalities between 1980 and 1996 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
TABLE 35.10. High-Dose (in General Daily 6 mg) Folic Acid Supplementation in Case-Control Pairs of Nonsyndromic Cleft Lip with or without Cleft Palate (CL/P) and Posterior Cleft Palate (CP) in Addition to Distribution of Gestational Months According to Start of Folic Acid Supplementation and Cumulative Number of Pregnant Women during the Critical Period of CL/P (i.e., 49–64 Gestational Days) and of CP (i.e., 70–98 Gestational Days) and Adjusted Odds Ratio (OR) with 95% Confidence Interval (CI) for Confounding Factors |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The strengths and weaknesses of the HCCSCA have been discussed previously (Czeizel et al., 2001). However, the HCCSCA is the largest case-control data set of its type in the world, and population-based sampling makes risk-benefit assessment possible. A significant reduction was found in the rate of nonsyndromic CL/P and CP due to the pharmacological doses (in general, 6 mg/day) of folic acid supplementation during the crifical period of these OC entities in pregnant women. This finding is in agreement with the previously mentioned results of Tolarova (1982, 1987) and Tolarova and Harris (1995)because 10 mg of folic acid was used. The question is whether the reduction of nonsyndromic OCs associated with folic acid supplementation is real or confounded by other factors (e.g., lifestyle). That the effect may be real is supported by the finding that a reduction was seen after the use of folic acid during the critical period of OC development, but not after development of the primary and secondary palate.
Some data of both the TCS and the HCCSCA were published previously (Czeizel et al., 1999); however, the data set of the TCS was complemented by supplemented and unsupplemented pregnant women of three other regional periconceptional care centers, while that of the HCCSCA was modified after the cleaning of multiple CAs and the decision to use one case-one control matched pairs.
In conclusion, folate/folic acid deficiency may play a role in the origin of OCs, and it can be neutralized by supplementation of high-dose folic acid during the critical period of primary and secondary palatal development. According to our study, only high doses (about 6 mg) of folic acid daily during the critical period of OC development reduce the first occurrence of nonsyndromic CL/P and CP. About 30% of first occurrences can be prevented by this method. Our findings agree with the results of Tolarova (1982, 1987), which indicated a reduction of recurrent CL/P after the periconceptional use of 10 mg of folic acid. Thus, the protective effect of folic acid seems to be dose-dependent because only high-dose folic acid supplementation was effective at reducing first and recurrent cases of non-syndromic CL/P and CP.
Biological Plausibility and Practical Implications of the Dose-Dependent Protective Effect of Folic Acid
Berry et al. (1999), in a study in China, showed that the preventive efficacy of folic acid depends on the birth prevalence of neural tube defects. This rule may be valid for nonsyndromic OCs as well. In addition, the population differences in genetic background (ethnicity), lifestyle (e.g., diet), and demographic features (e.g., advanced maternal age) may influence not only on the occurrence of OCs but also on the possible preventive effect of folic acid. These findings demonstrate that here state-of-the-art OC prevention is based mainly on the homogeneous white Hungarian population.
A major proportion of first-occurrence neural tube defects can be prevented by folic acid (Berry et al., 1999) or PFMS (Czeizel and Dudás, 1992). The origins of neural tube defects and OCs may have some similarities. In the early embryo, the neural folds are largely comprised of epithelial cells of the neural plate. After elevation of the neural folds, cells adjacent to the neural plate undergo mesenchymal differentiation and migrate into underlying regions. These neuroepithelial cells, cranial neural crest cells, represent the major cell population that contributes to the formation of, among others, the frontonasal processes and palatal shelves. Thus, closure of the neural tube and development of the face and palate have a common origin, with the same or a similar genetic background (Thorogood and Tickle, 1988). They may share potential candidate genes in folate/folic acid metabolism, providing a plausible biological link between the prevention of neural tube defects and OCs by maternal folate/folic acid supplementation during the critical period for these CAs.
Analysis of the population-based data of multimalformed cases in the Hungarian Congenital Abnormality Registry indicated that the so-called schisis-type CAs, i.e., neural tube defects, OCs, CAs of the midline abdominal region, and diaphragmatic CAs, associated with one another far more frequently than at the expected random combination rates. Their combination with other CAs did not exceed the expected rate. Combinations of two or more schisis-type CAs without other CAs therefore were managed as a provisional entity, named schisis association (Czeizel, 1981) or midline defect (Opitz and Gilbert, 1982). Later, the causal association of schisis-type CAs was confirmed by familial clustering (Fraser et al., 1982). However, there are also differences between these two CA groups; e.g., studies have shown an association between homozygosity for a variant form of the C677T genotype, nor in the methylenetetrahydrofolate reductase (MTHFR) gene and risk of neural tube defects (van der Put et al., 1995; Kirke et al., 1996), while Shaw et al. (1998a, 1999) did not indicate increased risk for CL/P and CP among infants homozygous for the C677T genotype nor an interaction between infant C677T genotype and maternal multivitamin use on the occurrence of these OCs in the United States. However, Wyszynszki and Diehl (2000) reanalyzed the data of Shaw et al. (1999) and concluded that multivitamin supplementation before and during the early weeks of pregnancy may protect against CL/P. Mills et al. (1999) found that the thermolabile variant of MTHFR (TT) was associated with a significantly higher risk for nonsyndromic CP in the Irish population. Thus, ethnic origin may be important. The point is that a multivitamin including a physiological dose of folic acid is appropriate (Czeizel and Dudás, 1992) and that flour-bread fortification with folic acid, vitamin B6, and vitamin B12 (Czeizel and Merhala, 1998) may be effective at reducing neural tube defects but not for OCs because the latter requires a high dose of folic acid.
The available findings about the possible protective effect of folic acid against OCs are conflicting. The data of our Hungarian studies, however, may be appropriate to generate the dose-dependent effect of folic acid hypothesis because this theory is based on the following evidence.
1. It was possible to induce OCs in animal experiments by drastic folate deficiencies (Nelson et al., 1952, 1955), and an association was suggested between antifolate agents and OCs (Hernandes-Dias at al., 2000).
2. There is no evidence of an obvious socioeconomic dependence in the occurrence of nonsyndromic CL/P and CP that may be connected with dietary differences (Czeizel and Tusnády, 1971). Dietary folate intake was not able to reduce the occurrence of OCs (Bower and Stanley, 1992). The usual daily intake of folate is about 0.18 to 0.20 mg, and it is difficult to achieve the necessary two-to threefold increase in folate intake, which would need about 15 servings of broccoli or brussel sprouts. In addition, this dose would not be enough to prevent OCs. Finally, Cuskelly et al. (1996) showed that an extreme increase in consumption of extra folate from natural food is relatively ineffective at increasing folate status.
3. The teratogenic, particularly OC-inducing, effect of anticonvulsant medications, smoking, and alcohol may be related to the reduction of folate that is available to the developing embryo. The teratogenic effect of most anticonvulsants is mediated through folate deficiency (Wegner and Nau, 1992). Smoking can lower serum folate in pregnant women (Houdayer and Bahuau, 1998). Shaw et al. (1996) demonstrated a strong association between periconceptional maternal cigarette smoking, transforming growth factor-α (TGFa) genotype of infants, and risk of OCs. Shaw et al. (1998b) compared infants with the common TGFa genotype whose mothers used PFMS to infants with the A2 genotype (homo-and heterozygous) whose mothers did not use multivitamins and found increased OC risk (for nonsyndromic CL/P, OR = 3.0, 95% CI 1.4-6.6; for syndromic CL/P, OR = 2.4, 95% CI 0.7-11.6; for nonsyndromic CP, OR = 2.6, 95% CI 1.0-7.7; for syndromic CP, OR = 4.2, 95% CI 1.3-16.2; for other known syndromic OCs, OR = 8.1, 95% CI 2.6-27.7). Other candidate genes for nonsyndromic OC and maternal smoking and alcohol consumption were also detected (Romitti et al., 1999). Thus, a gene-environment interaction may play an important role in the origin of OCs.
4. Only the very high dose (6-10 mg) of folic acid reduced both occurrence (Czeizel et al., 1996, 1999) and recurrence (Peer et al., 1964; Tolarova, 1982, 1987; Tolarova and Harris, 1995) of nonsyndromic CL/P and CP in intervention studies.
5. The protective effect of high-dose folic acid is probably different from its reduction of neural tube defects. There is little evidence for a defect in folate metabolism in infants with OCs or their mothers (Mills, 1999). However, the natural polyglutamate folate and the synthetic monoglutamate folic acid (i.e., two forms of the same vitamin, which is called recently as vitamin B11 as a twin to vitamin B12) are pluripotent (Little, 1995). For example, folates also play a role in cell proliferation, and the absence of an adequate level of folates in the embryo leading to less epithelial activity may cause a fusing defect in the craniofacial processes. However, the importance of folic acid/folate in the production of the methyl group needed in the remethylation (i.e., detoxification) of homocysteine should also be considered (Cooper, 1984).
The major question is related to practical use of our knowledge. A higher dose (about 6 mg) of folic acid should be recommended for the reduction of recurrent OCs early during the postconceptional period under medical control (Czeizel et al., 1999). The question is whether it is appropriate to recommend the use of a high dose of folic acid supplementation before conception or after the early diagnosis of pregnancy in all women to reduce the first occurrence of nonsyndromic CL/P and CP. The pharmacological dose of folic acid may have some side effects, e.g., in women with pernicious anemia or epilepsy (ErŐs et al., 1998). It is reasonable to foresee that, in the future, women will be targeted with high doses of folic acid supplementation based on their genetic composition. Then, primary prevention through pharmacogenetics will be a reality.
References
Berry, RJ, Li, Z, Erickson, D, et al. (1999). Prevention of neural-tube defects with folic acid in China. N Engl J Med 341: 1485–1490.
Bienengräber, V, Fanghänel, J, Malek, TA, Kundt, G (1997). Application of thiamine in preventing malformations, specifically cleft alveolus and palate, during the intrauterine development of rats. Cleft Palate Craniofac J 34: 318–324.
Bower, C, Stanley, FJ (1992). Dietary folate and nonneural midline birth defects. No evidence of an association from a case-control study in Western Australia. Am J Med Genet 44: 647–650.
Briggs, RM (1976). Vitamin supplements as a possible factor decreasing the incidence of cleft lip/palate deformities in humans. Clin Plast Surg 3: 647–652.
Canick, ML (1954). Cleft lip and cleft palate. A review of embryology, pathologic anatomy and etiology. Plast Reconstr Surg 14: 30–52.
Conway, H (1958). Effect of supplemental vitamin therapy on the limitation of incidence of the cleft lip and palate in humans. Plast Reconstr Surg 22: 450–453.
Cooper, BA (1984). Folate, its metabolism and utilization. Clin Biochem 17: 95–98.
Cuskelly, GJ, McNulty, H, Scott, JM (1996). Effect of increasing dietary folate on red-cell folate: implications for prevention of neural tube defects. Lancet 347: 657–659.
Czeizel, AE (1981). Schisis association. Am J Med Genet 10: 25–35.
Czeizel, AE (1993a). Prevention of congenital abnormalities by periconceptional multivitamin supplementation. BMJ 306: 1645–1648.
Czeizel, AE (1993b). Epidemiological studies of congenital abnormalities in Hungary. Issues Rev Teratol 6: 83–124.
Czeizel, AE (1996). Reduction of urinary tract and cardiovascular defects by periconceptional multivitamin supplementation. Am J Med Genet 62: 179–183.
Czeizel, AE (1997). First 25 years of the Hungarian Congenital Abnormality Registry. Teratology 55: 299–305.
Czeizel, AE (1999). Ten years of experiences in periconceptional care. Eur J Obstet Gynecol Reprod Biol 84: 43–49.
Czeizel, AE, Dobó, M, Dudás, I, et al. (1998). The Hungarian Periconceptional Service as a model for community genetics. Community Genet 1: 252–259.
Czeizel, AE, Dudás, I (1992). Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. N Engl J Med 327: 1832–1835.
Czeizel, AE, Dudás, I, Métneki, J (1994). Pregnancy outcomes in a randomized controlled trial of periconceptional multivitamin supplementation. Final report. Arch Gynecol Obstet 255: 131–139.
Czeizel, AE, Hirschberg, J (1997). Orofacial clefting in Hungary. Folia Phoniatr Logop 49: 111–116.
Czeizel, AE, Hirschberg, J, Tary, E (1986). Etiological study on the Robin sequence [in Hungarian]. Gyermekgyógyászat 37: 157–171.
Czeizel, AE, Merhala, Z (1998). Bread fortification with folic acid, vitamin B12 and vitamin B6 in Hungary. Lancet 352: 1225.
Czeizel, AE, Nagy, E (1986). Recent aetiological study on facial clefting in Hungary. Acta Paediatr Hung 27: 145–166.
Czeizel, AE, Rockenbauer, M, Siffel, C, Varga, E (2001). Description and mission evaluation of the Hungarian Case-Control Surveillance of Congenital Abnormalities, 1980–1996. Teratology 63: 176–185.
Czeizel, AE, Telegdi, L, Tusnády, G (1988). Multiple Congenital Abnormalities. Budapest: Akadémiai Kiadó.
Czeizel, AE, Tímár, L, Sárközi, E (1999). Dose-dependent effect of folic acid on the prevention of orofacial clefts. Pediatrics 204: e66.
Czeizel, AE, Tóth, M, Rockenbauer, M (1996). Population-based case-control study of folic acid supplementation during pregnancy. Teratology 53: 345–351.
Czeizel, AE, Tusnády, G (1971). An epidemiological study of cleft lip with or without cleft palate and posterior cleft palate in Hungary. Hum Hered 21: 17–38.
Czeizel, AE, Tusnády, G (1972). A family study on cleft lip with or without cleft palate and posterior cleft palate in Hungary. Hum Hered 22: 405–416.
Czeizel, AE, Tusnády, G (1984). Aetiological Studies of Isolated Common Congenital Abnormalities in Hungary. Budapest: Akadémiai Könyvkiadó.
ErŐs, E, Géher, P, Gömör, B, Czeizel, AE (1998). Epileptogenic activity of folic acid after drug induced SLE. Folic acid and epilepsy. Eur J Obstet Gynecol Reprod Biol 80: 75–78.
Fogh-Andersen, P (1942). Inheritance of Harelip and Cleft Palate. Copenhagen: Arnold Busck.
Fraser, FC, Czeizel, AE, Hanson, C (1982). Increased frequency of neural tube defects in sibs of children with other malformations. Lancet 2: 144–145.
Fraser, FC, Warburton, D (1964). No association of emotional stress or vitamin supplement during pregnancy to cleft lip or palate in man. Plast Reconstr Surg 33: 394–395.
Hayes, C, Werler, MM, Willett, WC, Mitchell, AA (1996). Case-control study of periconceptional folic acid supplementation and oral clefts. Am J Epidemiol 143: 1229–1234.
Hernandes-Dias, S, Werler, MM, Walker, AM, Mitchell, AA (2000). Folic acid antagonists during pregnancy and the risk of birth defects. N Engl J Med 343: 1608–1614.
Hill, L, Murphy, M, McDowall, M, Paul, AH (1988). Maternal drug histories and congenital malformations: limb reduction defects and oral clefts. J Epidemiol Community Health 42: 1–7.
Houdayer, CI, Bahuau, M (1998). Orofacial cleft defects: inference from nature and nurture. Ann Genet 41: 89–117.
Khoury, MJ, Gomez-Farias, M, Mulinare, J (1989). Does maternal cigarette smoking during pregnancy cause cleft lip and palate in offspring? Am J Dis Child 243: 333–337.
Kirke, PN, Mills, JL, Whitehead, AS (1996). Methylene-tetrahydro-folate reductase mutation and neural tube defects. Lancet 348: 1037–1038.
Kreybig, TV (1981). Erweiterung der Lippen-Kiefer-Gaumen-spalten-Prävention zur Verkütung anderer Fehlbildungs formen. Munch Med Wochenschr 123: 1151–1154.
Lidral, AC, Johnston, MC, Switzer, R (1991). The relationship between vitamins and the prevalence of cleft lip in mice [abstract]. J Dent Res 68: 524.
Little, J (1995). Is folic acid pluripotent? A review of the associations with congenital anomalies, cancer and other diseases. In: Drugs, diet and disease. Mechanistic Approaches to Cancer, Vol. 1, edited by DFV Lewis. New York: Ellis Horwood, pp. 259–308.
Mills, JL (1999). Folate and oral clefts: where do we go from here? New Dir Oral Clefts Res 60: 251–252.
Mills, JL, Kirke, PN, Molloy, AM, et al. (1999). Methylenetetrahydrofolate reductase thermolabile variant and oral clefts. Am J Med Genet 86: 71–74.
Nelson, MM, Asling, CW, Evans, HM (1952). Production of multiple congenital abnormalities in young by maternal pteroylglutamic acid deficiency during gestation. J Nutr 48: 61–79.
Nelson, MM, Wright, HV, Asling, CW, Evans, HM (1955). Multiple congenital abnormalities resulting from transitory deficiency of pteroylglutamic acid during gestation in rat. J Nutr 56: 349–369.
Opitz, JM, Gilbert, EF (1982). CNS anomalies and the midline as a developmental fields. Am J Med Genet 12: 443–455.
Paros, A, Beck, SL (1999). Folinic acid reduces cleft lip [CL(P)] in A/WySn mice. Teratology 60: 344–347.
Peer, LA, Bryan, WH, Strean, LP (1958a). Induction of cleft palate in mice by cortisone and its reduction by vitamins. J Int Coll Surg 30: 249.
Peer, LA, Gordon, HW, Bernhard, WG (1964). Effect of vitamins on human teratology. Plast Reconstr Surg 34: 358–363.
Peer, LA, Strean, LP, Walker, JC, et al. (1958b). Study of 400 pregnancies with birth of cleft lip-palate infants: protective effect of folic acid and vitamin B6 therapy. Plast Reconstr Surg 22: 422–429.
Pickerill, HP (1914). The anatomy and physiology of cleft palate and a new method of treatment. In: Transactions of the 6th International Dental Congress, London: pp. 453–469.
Romitti, PA, Lidval, AC, Munger, RG, et al. (1999). Candidate genes for nonsyndromic cleft lip and palate and maternal cigarette smoking and alcohol consumption: evaluation of genotype-environment interaction from a population-based case-control study of orofacial clefts. Teratology 59: 39–50.
Sakanashi, TM, Rogers, JM, Fu, SS, et al. (1996). Influence of maternal folate status on the developmental toxicity of methanol in the CD-I mouse. Teratology 54: 198–206.
Saxen, I (1975). Association between oral clefts and drugs taken during pregnancy. Int J Epidemiol 4: 37–44.
Schinke, G, Sikapa, R, Kreybig, TV (1976). Beeinflussung der Teratogenitat von Hydroxamsäuren durch Thiamin (Vitamin BI) bei der Ratte. Z Kinderchir 19: 333–344.
Shaw, GM, Croen, LA, Todoroff, K, Tolarova, MM (2000). Periconceptional intake of vitamin supplements and risk of multiple congenital anomalies. Am J Med Genet 93: 188–193.
Shaw, GM, Finnell, RH, Todoroff, K, et al. (1999). Maternal vitamin use, infant C677T mutation in MTHFR and isolated cleft palate risk. Am J Med Genet 85: 84–85.
Shaw, GM, Lammer, EJ, Wasserman, CR, et al. (1995). Risks of orofacial clefts in children born to women using multivitamins containing folic acid periconceptionally. Lancet 346: 393–396.
Shaw, GM, Rozen, R, Finnel, RH, et al. (1998a). Infant C677T mutation in MTHFR, maternal periconceptional vitamin use, and cleft lip. Am J Med Genet 80: 196–198.
Shaw, GM, Wasserman, CR, Lammer, EJ, et al. (1996). Orofacial clefts, parental cigarette smoking and transforming growth factor alpha gene variants. Am J Hum Genet 58: 551–561.
Shaw, GM, Wasserman, CR, Murray, JC, Lammer, EJ (1998b). Infant's TGF-alpha genotype, orofacial clefts and maternal periconceptional multivitamin use. Cleft Palate Craniofac J 35: 366–370.
Smithells, RW, Sheppard, S, Schorah, CJ, et al. (1980). Possible prevention of neural tube defects by periconceptional vitamin supplementation. Lancet 1: 339–340.
Strauss, OA (1914). Predisposing causes of cleft palate and harelip. In: Transactions of the 6th International Dental Congress. London: pp. 470–471.
Thorogood, P, Tickle, C (1988). Craniofacial development. Development 103: 1–257.
Tolarova, M (1982). Periconceptional supplementation with vitamins and folic acid to prevent recurrence of cleft lip. Lancet 1: 217.
Tolarova, M (1987). Orofacial clefts in Czechoslovakia. Incidence, genetics and prevention of cleft lip and palate over a 19-year period. Scand J Plast Reconstr Surg 21: 19–25.
Tolarova, M, Harris, T (1995). Reduced recurrence of orofacial clefts after periconceptional supplementation with high dose folic acid and multivitamin. Teratology 51: 71–78.
Tolarova, MM, Cervenka, J (1998). Classification and birth prevalence of orofacial clefts. Am J Med Genet 75: 126–137.
Van der Put, NM, Steegers-Theunissen, RP, Frosst, P, et al. (1995). Mutated methylenetetrahydrofolate reductase as a risk factor for spina bifida. Lancet 346: 1070–1071.
Warkany, J, Nelson, RC (1940). Appearance of skeletal abnormalities in the offspring of rats reared on a deficient diet. Science 92: 383–384.
Wegner, C, Nau, H (1992). Alteration of embryonic folate metabolism by valproic acid during organogenesis: implications for mechanism of teratogenesis. Neurology 42(Suppl 5): 17–24.
Werler, MM (1999). Multivitamin supplementation and risk of birth defect. Am J Epidemiol 150: 675–682.
Wyszynski, DF, Beaty, TH (1996). Review of the role of potential teratogens in the origin of human nonsyndromic oral clefts. Teratology 53: 309–317.
Wyszynski, DF, Diehl, SR (2000). Infant C677T mutation in MTHFR, maternal periconceptional vitamin use, and risk of nonsyndromic cleft lip. Am J Med Genet 92: 79–80.
Zanjani, ED, Anderson, WF (1999). Prospects for in utero human gene therapy. Science 285: 2084–2088.