Sridivya Jaini
Herbert L. DuPont
Diarrhea occurs in close to one occurrence per person per year in the United States. It varies from a short-lasting mild illness to various more serious enteric syndromes that include watery diarrhea with dehydration, febrile dysentery, and gastroenteritis with sepsis.
Although diarrhea may be acquired directly from an infected person, it is usually acquired by exposure to contaminated food, water, or the environment. Foodborne diseases became particularly important during 2006. The foodborne enteric diseases have been estimated to cause approximately 76 million cases of illness, 325,000 hospitalizations, and 5,000 deaths in the United States each year. Known pathogens account for an estimated 14 million cases of illnesses, 60,000 hospitalizations, and 1,800 deaths (1).
Diarrhea has two important definitions:
1. An increase in the normal frequency of stools associated with a decrease in their form, progressing from formed stools to those showing a watery or loose (soft) consistency.
2. Passage of more than 200 gm per day of unformed stool in an adult person on a standard western diet.
Diarrhea may be divided into three stages based on duration: (i) acute (less than or equal to 14 days), (ii) persistent (14 days or more), or (iii) chronic (30 days or more). The cause of the illness is different in the three groups. Viruses, bacteria, and toxins explain most episodes of acute diarrhea (Table 112.1); parasitic agents are more involved in the persistent cases (Table 112.1); and noninfectious causes are characteristically associated with chronic diarrhea. The severity of diarrhea can be determined according to a functional definition:
1. Mild—requires no change in activities
2. Moderate—requires a change in activities but doesn't disable
3. Severe—disables, usually confining the affected person to bed. It is the severe forms of diarrhea that usually lead to hospitalization.
Etiology of Acute Diarrhea in the United States
Community-acquired, acute infectious diarrhea is caused by various micro-organisms including bacteria, viruses, and parasites (Table 112.1). Bacterial causes include the following: Shigella, Salmonella, Campylobacter, Clostridium difficile, and various Escherichia coli species—enterotoxigenic (ETEC), enteroaggregative (EAEC), shigatoxin-producing (STEC) including E. coli O157:H7, enteropathogenic (EPEC), enteroinvasive (EIEC)—and, less commonly, others that include Aeromonas, Plesiomonas, Yersinia species, Vibrio cholerae, and other Vibrios. Important viral causes include rotavirus in infants and noroviruses in all age groups. Protozoan parasitic causes include Giardia, Entamoeba histolytica, Cryptosporidium, Isospora, Cyclospora and Microsporidia.
In the community, the most common causes of diarrhea are viral, with noroviruses being the most important. These cases are usually mild and do not require any specific treatment. The cause of diarrhea may vary depending on the season, with more viral cases in spring and winter and more bacterial cases in summer and spring (2).
The etiology of diarrheal cases presenting to a hospital and hospital-acquired diarrhea is different from the community-based diarrhea. In diarrheal cases presenting to the hospital, the disease is more severe compared to community diarrhea, and the causative agent may be a bacterial (most common), parasitic, or viral agent (rarely). Diarrhea acquired in the hospital may be due to bacteria (Clostridium difficile or Salmonella), viruses (rotavirus, noroviruses), or fungi (Candida albicans), or most commonly to noninfectious agents.
Evaluation of the Patient With Severe Diarrhea
Emergency Department
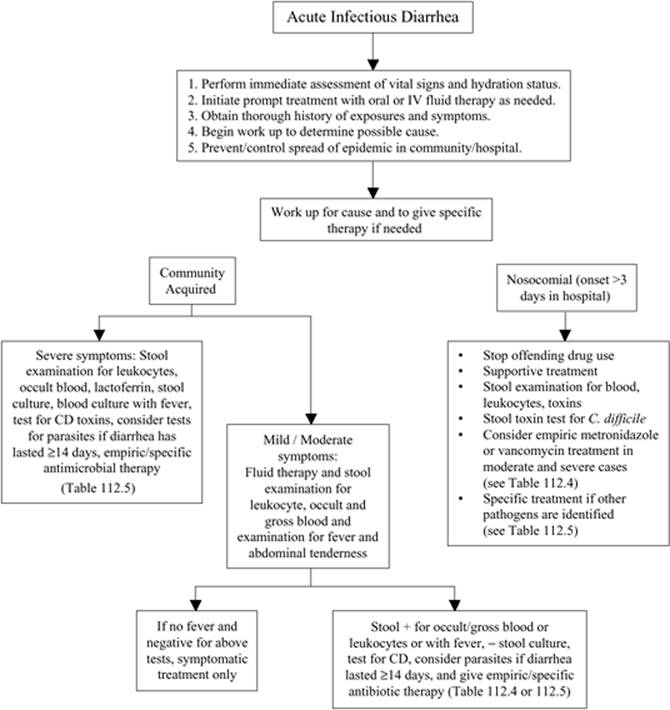
The first priority is to evaluate vital signs and the hydration status of the patient. Second, electrolyte disturbances need to be sought and corrected. The primary concern is to immediately reverse circulatory or organ failure resulting from loss of fluid and salt. Electrolyte imbalances may vary depending on the cause and also on other comorbid conditions. Diagnostic investigations for identifying the causative agent should be done either simultaneously or after stabilization of the patient. Most of the cases requiring hospitalization are due to bacterial causes rather than viral, which tend to be mild. Epidemiologic history and clinical features may provide clues to the diagnosis. Prior travel to an economically developing country suggests a bacterial cause of the diarrhea. Diarrhea in a person receiving antibacterial or chemotherapeutic drugs suggests C. difficile as the etiologic agent. Proctitis in a male with a history of having sex with men suggests sexually transmitted pathogens including Neisseria gonorrhoeae, Chlamydia trachomatis, herpes simplex or Treponema pallidum. In Figure 112.1, an algorithm is provided to help identify important steps in the workup of patients with acute diarrhea.
|
Table 112.1 Potential Etiologic Agents in Patients with Acute Diarrhea |
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
The laboratory will help establish the diagnosis. Finding many fecal leukocytes indicates the patient has diffuse colonic inflammation. Finding occult blood in the stool supports an inflammatory type of diarrhea. Gross blood passed in stool may indicate a dysenteric pathogen including Shigella, Campylobacter, Shigatoxin-producing E. coli (often E. coli O157:H7), and C. difficile. Stool cultures, parasite examination, or stool toxin test for C. difficile may help define the cause of the illness. Some characteristics, when present, that require aggressive and thorough laboratory workup are fever greater than 102°F with systemic findings, suggesting the presence of sepsis; among enteric pathogens, Salmonella is an important cause or an extraintestinal focus of infection such as an intra-abdominal abscess. If associated cases of diarrhea are known to be present, local health department authorities should be notified. In the United States and other economically developed nations, the most important etiologic agent to consider in patients suffering from diarrhea after being admitted to the hospital is C. difficile. Once disease onset, presentation, and progression of associated symptoms are evaluated and immediate laboratory work has been performed, it may be useful to categorize the diarrhea into one of two physiologic classifications. Diarrhea can be divided into noninflammatory and inflammatory (Table 112.2). A subcategory of inflammatory is hemorrhagic or dysenteric diarrhea. Distinction of the specific type of diarrhea is helpful to focus on appropriate empiric management options.
Hospital-Acquired Diarrhea
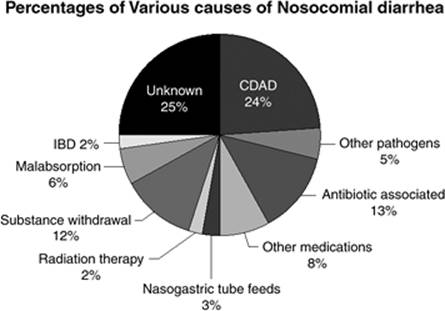
Illness occurring after the expected incubation period of an identified enteric pathogen is considered nosocomial or health care-associated. For practical purposes, diarrhea developing 3 days or longer after admission can be considered health care associated. In Figure 112.2, the relative importance of causes of diarrhea in hospitalized patients in one study is provided. Between 10% and 30% of nosocomial diarrhea is due to C. difficile (3,4). The other important causes of nosocomial diarrhea include antibiotics, chemotherapeutic agents, proton pump inhibitors, tube feedings, laxatives, other drugs, and various iatrogenic and idiopathic conditions (Fig. 112.2).
It is appropriate in all hospital-associated diarrheas, when a patient is receiving antibacterial treatment, to consider C. difficile as the causative agent, and empiric treatment is advisable in the more severe cases while laboratory tests are pending. Rarely, other pathogens can be found in hospital-associated diarrhea, including rotaviruses in pediatric wards, noroviruses, and Salmonella spp.
The International Traveler
The incidence of traveler's diarrhea (TD) ranges from 13.6% to 54.6% in the high-risk regions (5) and approximately 4% in low-risk regions. (6) The various parts of the world have been classified into three different groups: low, intermediate, and high risk, based on the frequency of TD in the traveling public (7).
The important causes of TD are ETEC, EAEC, noroviruses, Campylobacter, Shigella, and Salmonella (7,8,9,10,11,12). Less commonly, the parasitic agents cause TD and should be suspected in persistent illness. The important parasitic pathogens in persistent TD include Giardia, Cryptosporidium, and Cyclospora.
The Immunosuppressed Patient
An immunosuppressed or immune-compromised patient—that is, with congenital or acquired immune deficiency, HIV/AIDS, or receiving immunosuppressive or cancer chemotherapy drugs—will have increased susceptibility to diarrhea. The etiology of diarrheal diseases in immunocompromised hosts is different from that of other populations in that they are at risk of developing infections from various opportunistic organisms in addition to the routine diarrheal pathogens. The use of various chemotherapy drugs or immunomodulators such as cyclosporine, mycophenolate mofetil, tacrolimus, or sirolimus results in drug-induced diarrhea (13). Diarrhea in transplant recipients can also be due to graft versus host disease (GVHD). Various organisms to consider as causes of diarrhea in this group of patients include Clostridium difficile, Salmonella enterica, noroviruses, Cryptosporidium, Isospora, Cyclospora, cytomegalovirus, and Mycobacterium avium intracellulare complex. A thorough and quick evaluation for identifying the causative organism is the key in treating/controlling diarrhea in this patient population. Appropriate rapid diagnostic tests include direct stool examination for ova, cysts, and parasites; stool test for C. difficile toxin; polymerase chain reaction (PCR) for cytomegalovirus or herpesvirus; stool cultures; and blood cultures. If the above tests do not provide a specific diagnosis, endoscopy and mucosal biopsy should be pursued to establish an etiologic diagnosis.
|
|
|
Figure 112.1. Flow chart showing approach to a patient with acute infectious diarrhea. |
The Patient with Extraintestinal Disease
Diagnostic evaluation of patients with diarrhea and systemic symptoms and signs will often take the clinician's focus away from the gut for the diagnosis. Blood cultures, CT of the abdomen, and serology (for Entamoeba histolytica) may help determine the primary cause of the disease. In cases of sepsis, blood cultures and stool studies may provide the diagnosis. Systemic complications are often seen with invasive bacterial and parasitic infections. Systemic complications of enteric infection include hemolytic uremic syndrome (HUS) or thrombotic thrombocytopenic purpura (TTP), Guillain-Barré syndrome, sepsis, infective endocarditis, and abdominal abscesses or localized abscess elsewhere, or pyogenic arthritis (14). In immunocompromised patients with diarrhea, systemic complications can occur with any of the etiologic agents. Antimotility drugs should not be used in inflammatory diarrhea, as they can prolong or complicate the disease (15,16). Amoebiasis, which is uncommon in the United States, shows an extended spectrum of extraintestinal complications including liver abscess and disseminated infection (14,17).
Management of Acute Diarrhea
Dehydration
Dehydration is defined as excess loss of body fluids resulting in fluid and electrolyte abnormalities. In Table 112.3, the classifications of dehydration are provided. Dry skin and dry mucous membranes, sunken eyes, decreased urine output, loss of skin turgor, dizziness/light-headedness are all manifestations of moderate to severe dehydration. Dehydration is the most common serious complication of diarrhea and should be promptly recognized and managed in all patients. Patients in an ICU, with other comorbid conditions and extremes of age, need to be vigorously treated to avoid life-threatening complications of dehydration. Routine testing of electrolytes in patients with severe diarrhea is of proven value in guiding fluid management in the ICU setting (18).
|
Table 112.2 Classification of Acute Diarrhea Based on Findings of Fecal Markers of Inflammation (Leukocytes or Lactoferrin) or Presence of Gross Fecal Blood |
||||||||||||
|
||||||||||||
Rehydration can be done depending on severity of the dehydration either by oral route or intravenous route. Where available, oral rehydration salt (ORS) solution can be used in mild or moderate dehydration, and also for maintenance of hydration after IV fluid administration in severe dehydration. Standard or reduced osmolarity (low-salt) ORS formulations are preferable where available. In dehydration due to cholera, reduced-osmolarity ORS may lead to subclinical reduction of body electrolytes, making standard ORS preferable in this dehydrating form of diarrhea (19). In the United States, ORS is not readily available, but Pedialyte or Ricelyte can be used to maintain hydration and treat minor degrees of dehydration. Specific fluid replacement strategies based on severity are mentioned in Table 112.3.
Dysentery
Dysentery is the diagnosis when subjects are passing grossly bloody stools. The disease has been historically classified as bacillary dysentery (shigellosis) versus amoebic dysentery. Bacillary dysentery is also caused by several invasive pathogens in addition to Shigella spp. including Campylobacter, Clostridium difficile, STEC, and Salmonella. The specific cause of dysentery should be established followed by specific treatment. Empiric and specific antibiotic treatments are provided in Tables 112.4 and 112.5.
|
|
|
Figure 112.2. Relative importance of etiologic agents in hospital-acquired diarrhea. This figure shows the percentage of incidence of each of the common diarrhea-causing bacteria. CDAD, C. difficile–associated disease; IBD, inflammatory bowel disease. (Adapted from McFarland LV. Epidemiology of infectious and iatrogenic nosocomial diarrhea in a cohort of general medicine patients. Am J Infect Control. 1995;23(5):295–305, with permission.) |
Clostridium difficile Diarrhea and Colitis
C. difficile (CD) was first identified as a causative agent of antibiotic-associated diarrhea in the early 1970s and then was associated with clindamycin use (20,21). CD is a Gram-positive, spore-forming anaerobic bacteria that produces an enterotoxin known as toxin A and a cytotoxin called toxin B. There is currently a third type of toxin produced, called binary toxin, which is an actin-specific ADP ribosylating toxin. Toxin A causes necrosis, increased intestinal permeability, and inhibition of protein synthesis. Toxin B is thought to become effective once the gut wall has been damaged (22,23). There has been an increased virulence of CD strains, which is presumably associated with higher levels of toxin production by a fluoroquinolone-resistant CD strain variably classified as PCR ribotype 027, pulsed-field gel electrophoresis (PFGE) type NAP1, restriction endonuclease analysis (REA) type BI, and toxinotype III (24).
|
Table 112.3 Classification of Dehydration in a Patient with Acute Diarrhea |
||||||||||||||||||||
|
||||||||||||||||||||
The incidence of CD acute diarrhea (CDAD) has been rising in recent years due to excess use of antibiotics and emergence of resistant and more virulent strains. According to the Centers for Disease Control and Prevention (CDC) national nosocomial infection surveillance systems data, nosocomial CDAD has been increasing both in the intensive care units of large hospitals and hospital-wide in smaller hospitals (25). This rise has nearly doubled from 1996 to 2003 and has disproportionately increased in the elderly population (26). A conservative estimate of the cost of this disease in the United States is $1.1 billion per year, with a 54% increase in individual adjusted hospital costs and an extension of hospital stay by 3.6 days for each affected person (27). In a study done by our group (4), normal hospital surveillance of CDAD identified only half of the affected patients in our institution. Thus, the real burden of CDAD seems to be much more than estimated.
|
Table 112.4 Empiric Antimicrobial Therapy of Acute Diarrhea |
||||||||||||||||||
|
||||||||||||||||||
Major risk factors for CDAD include antimicrobial use, age older than 65 years, severity of existing health condition, use of other drugs such as chemotherapeutic agents and proton pump inhibitors, renal insufficiency, and gastrointestinal surgery. Our research team recently identified a genetic factor that allows identification of persons at high risk for CDAD (28). In CDAD, advanced age and comorbidity, plus severity of underlying impairment, predict frequency of infection and outcome (29).
When assessing institutionalized individuals, such as nursing home patients with diarrhea, associated risk factors for CDAD should be considered. Some of the risk factors other than antibiotic use and comorbidity are low albumin level (less than 2.5 g/dL), recent admission to a health care institution, and use of proton pump inhibitors (30). In nonhospitalized patients with other predisposing conditions such as cancer, prolonged antibiotic usage—especially with first-generation cephalosporins, fluoroquinolones, or clindamycin—is a recognized risk factor for CDAD (31).
|
Table 112.5 Specific Therapy for Pathogen-Specific Diarrhea, Once Etiologic Diagnosis is Established |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Recurrence is very common in CDAD as, after the first episode, it is estimated that nearly 15% to 30% of patients have recurrent illness after initial treatment (32,33). Recurrences include both re-infections with new strains and relapse of the original infecting strain. In one study, 56% of recurrences were due to re-infection (34). Some of the risk factors for early recurrence of CDAD are renal failure, white blood cell counts greater than 15,000 cells/µL with the initial episode, and community-acquired CDAD with the first episode (35). Failure to mount a serum antibody response to toxin A during an initial episode of CDAD is associated with CD recurrence (36).
Diagnosis of CDAD is based on both clinical and laboratory findings. The customary way to make the diagnosis is to recover a toxigenic strain of CD through microbiologic culture or to detect one or both of the known CD toxins, A and B, in stool samples. The stool toxin studies include a commercial tissue culture cytotoxin assay for toxin B or an enzyme immunoassay (EIA) for one or both of the toxins. In a highly probable clinical case with severe disease or fragile clinical picture, it is often advisable to initiate prompt empiric treatment before stool test results are back or even in the face of negative laboratory tests for the toxins. Colonoscopy should be considered in patients in whom the diagnosis is not obvious, after initial screening, when there are extraintestinal complications, and in those not responding to empiric treatment (37).
Treatment
Prompt diagnosis and treatment are important to successful management of CDAD (Table 112.5). Cessation of causative antibiotic use if possible and initiation of either oral metronidazole (most consider first-line therapy) or oral vancomycin for 10 days is the standard practice in treating symptomatic patients (38,39,40). Vancomycin may be slightly more effective than metronidazole but its widespread use could promote the development of vancomycin resistance in the hospital setting, especially among Enterococcus spp.
Both metronidazole and vancomycin are used in the treatment of recurrent CD diarrhea. Independent predictors of a second recurrence are age and duration of hospitalization after the first recurrence (41). Strategies for treating recurrent CD diarrhea or colitis include repeating antibiotics either with metronidazole or vancomycin, with tapering of the antibiotic dose after a 10-day standard and administering the drug for 2 months or longer; use of probiotics such as Saccharomyces boulardii along with high-dose (500 mg four times a day) vancomycin; and use of intravenous immunoglobulin (IVIG) (42). When Saccharomyces was used in one study, the risk of recurrence was reduced by 50% (43).
If more than one recurrence occurs, various drugs may be used for prolonged therapy including vancomycin, rifaximin, and Saccharomyces. Other microbiologic approaches that may be useful include the restoration of normal colonic flora by fecal enema or by nasogastric tube administration (42). Surgical management of CDAD is done after failure of medical therapy or if life-threatening complications occur, including colonic perforation, peritonitis, or bowel infarction.
Diarrhea Epidemics in the Hospital
Early identification and controlling the spread of rare hospital epidemics of enteric disease are the keys to successful management. Universal protocols of isolation and personal hygiene measures play an important role. Cohorting subjects by putting infected persons in contiguous areas away from uninfected persons and using dedicated hospital personnel for their care is an important strategy. Judicious use of antibiotics in the hospital and prompt discontinuation of possible inciting drugs also can be helpful. Agents showing potential for epidemics in hospitals are C. difficile, Salmonella spp, Shigella, Campylobacter, Vibrio, Aeromonas, Yersinia, noroviruses, and rotavirus. Early therapy of treatable enteric pathogens should occur (Table 112.5). Health care worker and patient education regarding various personal hygiene and isolation procedures could help in stopping the spread within the institution.
Prevention of Diarrhea in the Hospital
Appropriate use of antibiotics in hospitalized patients, along with use of the narrowest-spectrum antibiotics safely possible to minimize the disruption of gut flora should prevent cases of CDAD. Additionally, at least in a research setting, Saccharomyces has been used to prevent CDAD (44). Enteric isolation practices for patients with known enteric infection in the hospital will help prevent the spread of diarrhea and lower its incidence. Effective and widespread hand washing with soap and water—note that alcohol-based hand cleaners are not effective against C. difficile—by patients and health care workers, using disposable thermometers for recording temperature, and meticulous environmental cleaning with chlorine-based bleach products in clinical settings where C. difficile-infected patients have been housed are proven to prevent spread of infections in the hospital (45,46,47).
References
1. Mead PS, Slutsker L, Dietz V, et al. Food-related illness and death in the United States. Emerg Infect Dis. 1999;5(5):607–625.
2. Denno DM, Stapp JR, Boster DR, et al. Etiology of diarrhea in pediatric outpatient settings. Pediatr Infect Dis J. 2005;24(2):142–148.
3. McFarland LV. Epidemiology of infectious and iatrogenic nosocomial diarrhea in a cohort of general medicine patients. Am J Infect Control. 1995;23(5):295–305.
4. Garey KW, Graham G, Gerard L, et al. Prevalence of diarrhea at a university hospital and association with modifiable risk factors. Ann Pharmacother. 2006;40(6):1030–1034.
5. Steffen R, Tornieporth N, Clemens SA, et al. Epidemiology of travelers' diarrhea: details of a global survey. J Travel Med. 2004;11(4):231–238.
6. Steffen R. Epidemiologic studies of travelers' diarrhea, severe gastrointestinal infections, and cholera. Rev Infect Dis. 1986;8(Suppl 2):S122–130.
7. DuPont HL, Ericsson CD. Prevention and treatment of traveler's diarrhea. N Engl J Med. 1993;328(25):1821–1827.
8. Ko G, Garcia C, Jiang ZD, et al. Noroviruses as a cause of traveler's diarrhea among students from the United States visiting Mexico. J Clin Microbiol. 2005;43(12):6126–6129.
9. Bouckenooghe AR, Jiang ZD, De La Cabada FJ, et al. Enterotoxigenic Escherichia coli as cause of diarrhea among Mexican adults and US travelers in Mexico. J Travel Med. 2002;9(3):137–140.
10. Adachi JA, Ericsson CD, Jiang ZD, et al. Natural history of enteroaggregative and enterotoxigenic Escherichia coli infection among US travelers to Guadalajara, Mexico. J Infect Dis. 2002;185(11):1681–1683.
11. Gallardo F, Gascon J, Ruiz J, et al. Campylobacter jejuni as a cause of traveler's diarrhea: clinical features and antimicrobial susceptibility. J Travel Med. 1998;5(1):23–26.
12. Adachi JA, Jiang ZD, Mathewson JJ, et al. Enteroaggregative Escherichia coli as a major etiologic agent in traveler's diarrhea in 3 regions of the world. Clin Infect Dis. 2001;32(12):1706–1709.
13. Ginsburg PM, Thuluvath PJ. Diarrhea in liver transplant recipients: etiology and management. Liver Transpl. 2005;11(8):881–890.
14. Rees JR, Pannier MA, McNees A, et al. Persistent diarrhea, arthritis, and other complications of enteric infections: a pilot survey based on California FoodNet surveillance, 1998–1999. Clin Infect Dis. 2004;38(Suppl 3):S311–317.
15. Cimolai N, Basalyga S, Mah DG, et al. A continuing assessment of risk factors for the development of Escherichia coli O157:H7-associated hemolytic uremic syndrome. Clin Nephrol. 1994;42(2):85–89.
16. DuPont HL, Hornick RB. Adverse effect of Lomotil therapy in shigellosis. JAMA. 1973;226(13):1525–1528.
17. Landzberg BR, Connor BA. Persistent diarrhea in the returning traveler: think beyond persistent infection. Scand J Gastroenterol. 2005;40(1):112–114.
18. Wathen JE, MacKenzie T, Bothner JP. Usefulness of the serum electrolyte panel in the management of pediatric dehydration treated with intravenously administered fluids. Pediatrics. 2004;114(5):1227–1234.
19. Murphy C, Hahn S, Volmink J. Reduced osmolarity oral rehydration solution for treating cholera. In: Murphy C, Hahn S, Volmink J. Reduced osmolarity oral rehydration solution for treating cholera. Cochrane Database Syst Rev. 2004 Oct 18;(4):CD003754.
20. Tedesco FJ, Barton RW, Alpers DH. Clindamycin-associated colitis. A prospective study. Ann Intern Med. 1974;81(4):429–433.
21. Bartlett JG, Chang TW, Gurwith M, et al. Antibiotic-associated pseudomembranous colitis due to toxin-producing Clostridia. N Engl J Med. 1978;298(10):531–534.
22. Poxton IR, McCoubrey J, Blair G. The pathogenicity of Clostridium difficile. Clin Microbiol Infect. 2001;7(8):421–427.
23. Rupnik M, Grabnar M, Geric B. Binary toxin producing Clostridium difficile strains. Anaerobe. 2003;9(6):289–294.
24. Kuijper EJ, Coignard B, Tull P, et al. Emergence of Clostridium difficile-associated disease in North America and Europe. Clin Microbiol Infect. 2006;12(Suppl 6):2–18.
25. Archibald LK, Banerjee SN, Jarvis WR. Secular trends in hospital-acquired Clostridium difficile disease in the United States, 1987-2001. J Infect Dis. 2004;189(9):1585–1589.
26. McDonald LC, Owings M, Jernigan DB. Clostridium difficile infection in patients discharged from US short-stay hospitals, 1996-2003. Emerg Infect Dis. 2006;12(3):409–415.
27. Kyne L, Hamel MB, Polavaram R, et al. Health care costs and mortality associated with nosocomial diarrhea due to Clostridium difficile. Clin Infect Dis. 2002;34(3):346–353.
28. Jiang ZD, DuPont HL, Garey K, et al. A common polymorphism in the interleukin 8 gene promoter is associated with Clostridium difficile diarrhea. Am J Gastroenterol. 2006;101(5):1112–1116.
29. Andrews CN, Raboud J, Kassen BO, et al. Clostridium difficile-associated diarrhea: predictors of severity in patients presenting to the emergency department. Can J Gastroenterol. 2003;17(6):369–373.
30. Al-Tureihi FI, Hassoun A, Wolf-Klein G, et al. Albumin, length of stay, and proton pump inhibitors: key factors in Clostridium difficile-associated disease in nursing home patients. J Am Med Dir Assoc. 2005;6(2):105–108.
31. Palmore TN, Sohn S, Malak SF, et al. Risk factors for acquisition of Clostridium difficile-associated diarrhea among outpatients at a cancer hospital. Infect Control Hosp Epidemiol. 2005;26(8):680–684.
32. Fekety R, McFarland LV, Surawicz CM, et al. Recurrent Clostridium difficile diarrhea: characteristics of and risk factors for patients enrolled in a prospective, randomized, double-blinded trial. Clin Infect Dis. 1997;24(3):324–333.
33. McFarland LV, Surawicz CM, Rubin M, et al. Recurrent Clostridium difficile disease: epidemiology and clinical characteristics. Infect Control Hosp Epidemiol. 1999;20(1):43–50.
34. Wilcox MH, Fawley WN, Settle CD, et al. Recurrence of symptoms in Clostridium difficile infection–relapse or reinfection? J Hosp Infect. 1998;38(2):93–100.
35. Do AN, Fridkin SK, Yechouron A, et al. Risk factors for early recurrent Clostridium difficile-associated diarrhea. Clin Infect Dis. 1998;26(4):954–959.
36. Kyne L, Warny M, Qamar A, et al. Association between antibody response to toxin A and protection against recurrent Clostridium difficile diarrhoea. Lancet, 2001;357(9251):189–193.
37. Bauer TM, Lalvani A, Fehrenbach J, et al. Derivation and validation of guidelines for stool cultures for enteropathogenic bacteria other than Clostridium difficile in hospitalized adults. JAMA. 2001;285(3):313–319.
38. Aslam S, Musher DM. An update on diagnosis, treatment, and prevention of Clostridium difficile-associated disease. Gastroenterol Clin North Am. 2006;35(2):315–335.
39. Bergogne-Berezin E. Treatment and prevention of antibiotic associated diarrhea. Int J Antimicrob Agents. 2000;16(4):521–526.
40. Bricker E, Garg R, Nelson R, et al. Antibiotic treatment for Clostridium difficile-associated diarrhea in adults. Cochrane Database Syst Rev. 2005 Jan 25;(1):004610.
41. Pepin J, Routhier S, Gagnon S, et al. Management and outcomes of a first recurrence of Clostridium difficile-associated disease in Quebec, Canada. Clin Infect Dis. 2006;42(6):758–764.
42. Surawicz CM. Treatment of recurrent Clostridium difficile-associated disease. Nature Clin Practice Gastroenterol Hepatol. 2004;1(1):32–38.
43. Surawicz CM, McFarland LV, Greenberg RN, et al. The search for a better treatment for recurrent Clostridium difficile disease: use of high-dose vancomycin combined with Saccharomyces boulardii. Clin Infect Dis. 2000;31(4):1012–1017.
44. McFarland LV. Meta-analysis of probiotics for the prevention of antibiotic associated diarrhea and the treatment of Clostridium difficile disease. Am J Gastroenterol. 2006;101(4):812–822.
45. Jernigan JA, Siegman-Igra Y, Guerrant RC, et al. A randomized crossover study of disposable thermometers for prevention of Clostridium difficile and other nosocomial infections. Infect Control Hospital Epidemiol. 1998;19(7):494–499.
46. Worsley MA. Infection control and prevention of Clostridium difficile infection. J Antimicrob Chemother. 1998;41(Suppl C):59–66.
47. Robinson B. Be alert to an avoidable problem. Management and prevention of antibiotic-acquired diarrhoea. Prof Nurse. 1993;8(8):510–512.
48. Duggan C, Santosham M, Glass RI. The management of acute diarrhea in children: oral rehydration, maintenance, and nutritional therapy. Centers for Disease Control and Prevention. MMWR Recomm Rep. 1992;41(RR-16):1–20.
49. King CK, Glass R, Bresee JS, et al. Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep. 2003;52(RR-16):1–16.
50. Adachi JA, Ostrosky-Zeichner L, DuPont HL, et al. Empirical antimicrobial therapy for traveler's diarrhea. Clin Infect Dis. 2000;31(4):1079–1083.
51. Adachi JA, Ericsson CD, Jiang ZD, et al. Azithromycin found to be comparable to levofloxacin for the treatment of US travelers with acute diarrhea acquired in Mexico. Clin Infect Dis. 2003;37(9):1165–1171.
52. Kuschner RA, Trofa AF, Thomas RJ, et al. Use of azithromycin for the treatment of Campylobacter enteritis in travelers to Thailand, an area where ciprofloxacin resistance is prevalent. Clin Infect Dis. 1995;21(3):536–541.
53. DuPont HL. Use of quinolones in the treatment of gastrointestinal infections. Europ J Clin Microbiol Infect Dis. 1991;10(4):325–329.
54. Salam I, Katelaris P, Leigh-Smith S, et al. Randomised trial of single-dose ciprofloxacin for travellers' diarrhoea. Lancet. 1994;344(8936):1537–1539.
55. Ericsson CD, DuPont HL, Mathewson JJ. Optimal dosing of ofloxacin with loperamide in the treatment of non-dysenteric travelers' diarrhea. J Travel Med. 2001;8(4):207–209.
56. DuPont HL, Jiang ZD, Ericsson CD, et al. Rifaximin versus ciprofloxacin for the treatment of traveler's diarrhea: a randomized, double-blind clinical trial. Clin Infect Dis. 2001;33(11):1807–1815.
57. DuPont HL, Ericsson CD, Mathewson JJ, et al. Rifaximin: a nonabsorbed antimicrobial in the therapy of travelers' diarrhea. Digestion. 1998;59(6):708–714.
58. Musher DM, Logan N, Hamill RJ, et al. Nitazoxanide for the treatment of Clostridium difficile colitis. Clin Infect Dis. 2006;43(4):421–427.
59. Wenisch C, Parschalk B, Hasenhundl M, et al. Comparison of vancomycin, teicoplanin, metronidazole, and fusidic acid for the treatment of Clostridium difficile-associated diarrhea. Clin Infect Dis. 1996;22(5):813–818.
60. Wullt M, Odenholt I. A double-blind randomized controlled trial of fusidic acid and metronidazole for treatment of an initial episode of Clostridium difficile-associated diarrhoea. J Antimicrob Chemother. 2004;54(1):211–216.
61. DuPont HL. Guidelines on acute infectious diarrhea in adults. the practice parameters committee of the American College of Gastroenterology. Am J Gastroenterol. 1997;92(11):1962–1975.
62. Guerrant RL, Van Gilder T, Steiner TS, et al. Practice guidelines for the management of infectious diarrhea. Clin Infect Dis. 2001;32(3):331–351.
63. Soe GB, Overturf GD. Treatment of typhoid fever and other systemic salmonelloses with cefotaxime, ceftriaxone, cefoperazone, and other newer cephalosporins. Rev Infect Dis. 1987;9(4):719–736.
64. Khan WA, Seas C, Dhar U, et al. Treatment of shigellosis, V: comparison of azithromycin and ciprofloxacin. A double-blind, randomized, controlled trial. Ann Intern Med. 1997;126(9):697–703.
65. Bhattacharya SK, Bhattacharya MK, Dutta P, et al. Randomized clinical trial of norfloxacin for shigellosis. Am J Trop Med Hyg. 1991;45(6):683–687.
66. Salam MA, Bennish ML. Antimicrobial therapy for shigellosis. Rev Infect Dis. 1991;13(Suppl 4):S332–341.
67. Pai CH, Gillis F, Tuomanen E, et al. Erythromycin in treatment of Campylobacter enteritis in children. Am J Dis Child. 1983;137(3):286–288.
68. Mandal BK, Ellis ME, Dunbar EM, et al. Double-blind placebo-controlled trial of erythromycin in the treatment of clinical Campylobacter infection. J Antimicrob Chemother. 1984;13(6):619–23.
69. Endtz HP, Ruijs GJ, van Klingeren B, et al. Quinolone resistance in Campylobacter isolated from man and poultry following the introduction of fluoroquinolones in veterinary medicine. J Antimicrob Chemother. 1991;27(2):199–208.
70. Wong CS, Jelacic S, Habeeb RL, et al. The risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med. 2000;342(26):1930–1936.
71. O'Ryan M, Prado V. Risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med. 2000;343(17):1271.
72. Aragon T, Fernyak S, Reiter R. Risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med. 2000;343(17):1271–1272.
73. Cimolai N, Carter JE, Morrison BJ, et al. Risk factors for the progression of Escherichia coli O157:H7 enteritis to hemolytic-uremic syndrome. J Pediatr. 1990;116(4):589–592.
74. DuPont HL, Reves RR, Galindo E, et al. Treatment of travelers' diarrhea with trimethoprim/sulfamethoxazole and with trimethoprim alone. N Engl J Med. 1982;307(14):841–844.
75. Hossain MS, Salam MA, Rabbani GH, et al. Tetracycline in the treatment of severe cholera due to Vibrio cholerae O139 Bengal. J Health Popul Nutr. 2002;20(1):18–25.
76. Alam AN, Alam NH, Ahmed T, et al. Randomised double blind trial of single dose doxycycline for treating cholera in adults. BMJ. 1990;300(6740):1619–1621.
77. Holmberg SD, Farmer JJ 3rd. Aeromonas hydrophila and Plesiomonas shigelloides as causes of intestinal infections. Rev Infect Dis. 1984;6(5):633–639.
78. Kain KC, Kelly MT. Clinical features, epidemiology, and treatment of Plesiomonas shigelloides diarrhea. J Clin Microbiol. 1989;27(5):998–1001.
79. Nathwani D, Laing RB, Harvey G, et al. Treatment of symptomatic enteric Aeromonas hydrophila infection with ciprofloxacin. Scand J Infect Dis. 1991;23(5):653–654.
80. Abdel-Haq NM, Papadopol R, Asmar BI, et al. Antibiotic susceptibilities of Yersinia enterocolitica recovered from children over a 12-year period. Int J Antimicrob Agents. 2006;27(5):449–452.
81. Hoogkamp-Korstanje JA, Moesker H, Bruyn GA. Ciprofloxacin vs. placebo for treatment of Yersinia enterocolitica triggered reactive arthritis. Ann Rheum Dis. 2000;59(11):914–917.
82. Pai CH, Gillis F, Tuomanen E, et al. Placebo-controlled double-blind evaluation of trimethoprim-sulfamethoxazole treatment of Yersinia enterocolitica gastroenteritis. J Pediatr. 1984;104(2):308–311.
83. Levi GC, de Avila CA, Amato Neto V. Efficacy of various drugs for treatment of giardiasis. A comparative study. Amer J Trop Med Hyg. 1977;26(3):564–565.
84. Penggabean M, Norhayati, Oothuman P, et al. Efficacy of albendazole in the treatment of Trichuris trichiura and Giardia intestinalis infection in rural Malay communities. Med J Malaysia. 1998;53(4):408–412.
85. Carr A, Marriott D, Field A, et al. Treatment of HIV-1-associated microsporidiosis and cryptosporidiosis with combination antiretroviral therapy. Lancet. 1998;351(9098):256–261.
86. Fichtenbaum CJ, Ritchie DJ, Powderly WG. Use of paromomycin for treatment of cryptosporidiosis in patients with AIDS. Clin Infect Dis. 1993;16(2):298–300.
87. Foudraine NA, Weverling GJ, van Gool T, et al. Improvement of chronic diarrhoea in patients with advanced HIV-1 infection during potent antiretroviral therapy. AIDS. 1998;12(1):35–41.
88. Portnoy D, Whiteside ME, Buckley E 3rd, et al. Treatment of intestinal cryptosporidiosis with spiramycin. Ann Intern Med. 1984;101(2):202–204.
89. Rossignol JF, Ayoub A, Ayers MS. Treatment of diarrhea caused by Cryptosporidium parvum: a prospective randomized, double-blind, placebo-controlled study of nitazoxanide. J Infect Dis. 2001;184(1):103–106.
90. Rossignol JF, Hidalgo H, Feregrino M, et al. A double-‘blind’ placebo-controlled study of nitazoxanide in the treatment of cryptosporidial diarrhoea in AIDS patients in Mexico. Trans R Soc Trop Med Hyg. 1998;92(6):663–666.
91. Rossignol J. Nitazoxanide in the treatment of acquired immune deficiency syndrome-related cryptosporidiosis: results of the United States compassionate use program in 365 patients. Aliment Pharmacol Ther. 2006;24(5):887–894.
92. Hoge CW, Shlim DR, Ghimire M, et al. Placebo-controlled trial of co-trimoxazole for Cyclospora infections among travellers and foreign residents in Nepal. Lancet. 1995;345(8951):691–693.
93. Verdier RI, Fitzgerald DW, Johnson WD Jr, et al. Trimethoprim-sulfamethoxazole compared with ciprofloxacin for treatment and prophylaxis of Isospora belli and Cyclospora cayetanensis infection in HIV-infected patients. A randomized, controlled trial. Ann Intern Med. 2000;132(11):885–888.
94. Blanshard C, Ellis DS, Tovey DG, et al. Treatment of intestinal microsporidiosis with albendazole in patients with AIDS. AIDS. 1992;6(3):311–313.
95. Tremoulet AH, Avila-Aguero ML, París MM, et al. Albendazole therapy for Microsporidia diarrhea in immunocompetent Costa Rican children. Pediatr Infect Dis J. 2004;23(10):915–918.
96. Farthing MJ. Treatment options for the eradication of intestinal protozoa. Nature Clin Pract Gastroenterol Hepatol. 2006;3(8):436–445.
97. Dieterich DT, Kotler DP, Busch DF, et al. Ganciclovir treatment of cytomegalovirus colitis in AIDS: a randomized, double-blind, placebo-controlled multicenter study. J Infect Dis. 1993;167(2):278–282.
98. Mayoral JL, Loeffler CM, Fasola CG, et al. Diagnosis and treatment of cytomegalovirus disease in transplant patients based on gastrointestinal tract manifestations. Arch Surg. 1991;126(2):202–206.