Achille Gaspardone
Leonardo De Luca
Overview
Definition of Terms
The term, acute coronary syndrome (ACS), describes a spectrum of clinical conditions ranging from ST-segment elevation myocardial infarction (STEMI) to non–ST-segment elevation MI (N–STEMI) and unstable angina (UA) (Fig. 119.1) (1). These manifestations of acute myocardial ischemia may revert to the presymptomatic state or evolve into a non-Q wave (also termed nontransmural) MI or to Q wave (or transmural) MI (Fig. 119.1).
The boundaries between UA, N-STEMI, and STEMI are not always well defined. Indeed, the three entities should be considered as different and dynamic clinical manifestations of a continuous pathogenetic spectrum; N-STE-ACS are represented by UA and N-STEMI.
Unstable Angina (UA)
Anginal pain is the pivotal symptom for the diagnosis of UA, and its intensity, duration, and exercise-related threshold are usually graded according to the Canadian Cardiovascular Society (CCS) classification (Table 119.1) (2). UA may have three clinical presentations (Table 119.2) (3): (1) de novo or new-onset angina of at least CCS III-IV severity in patients without previously diagnosed angina; (2) crescendo, or increasing angina in patients with previously diagnosed angina that has become significantly more frequent, more severe in duration, and with a markedly reduced threshold (CCS Class III-IV); (3) postinfarction angina in patients with an MI within 2 weeks in whom biomarkers of myocardial necrosis have returned within normal range.
In all three clinical presentations of UA, pain may occur at rest and, typically, the low threshold for angina (CCS III and IV) represents an essential clinical feature for the diagnosis of UA. In all three clinical manifestations of UA, the presence of angina at rest is associated with a worse prognosis and a higher rate of events (4). In all cases, of course, it is crucial to exclude extracardiac conditions that can intensify or precipitate myocardial ischemia (secondary UA) such as anemia, fever, infection, hypotension, uncontrolled hypertension, hypoxemia, and thyrotoxicosis. The resting ECG may show ST-segment depression and/or T-wave inversion or transient ST-segment elevation or, rarely, may remain normal. The serum markers (troponin I, troponin T, and CK-MB) may remain within their normal biological ranges or fall between the normal range and the level diagnostic of myocardial infarction, the latter being, according to ACC/AHA recommendations, more than twice the upper normal limit (1). In the absence of release of myocardial markers of necrosis, the diagnosis of UA may be made, whereas if markers of myocardial necrosis have been released, the patient with ACS can be considered to have experienced N-STEMI. In the latter condition, ECG ST-segment or T-wave changes may be persistent, whereas in UA, they may or may not occur and, if they are seen, are usually transient.
A peculiar clinical manifestation of UA was described in 1959 by Prinzmetal and associates detailing an atypical ischemic coronary syndrome characterized by sudden onset angina occurring almost exclusively at rest, particularly in the first hours of the day, associated with ST segment elevation on the ECG (1). Because of its peculiar clinical pattern, this acute coronary syndrome was defined as a variant form of angina. Prinzmetal and colleagues hypothesized that variant angina is caused by a focal spasm of a coronary artery (5); this initial hypothesis has been convincingly demonstrated by coronary angiography. Variant angina may be associated with acute myocardial infarction, severe cardiac arrhythmias—including ventricular tachycardia and fibrillation, and sudden death. Despite these potentially devastating consequences, long term followup of patients with documented coronary vasospasm is not well documented. In a large population of patients with variant angina—i.e. normal or near normal coronary arteries—and treated with calcium channel blockers, the 7.5-year incidence of sudden death and myocardial infarction were 3.6% and 6.5%, respectively (6). Although the clinical presentation of this variant form of angina is also characterized by instability, with evidence of subendocardial and/or transmural myocardial ischemia, the specific pathogenetic mechanisms—i.e. coronary spasm—is completely different from those leading to N-STE-ACS.
Non-ST-Segment Elevation Myocardial Infarction
N-STEMI may have symptoms and a clinical pattern indistinguishable from UA. While the resting ECG more frequently shows ST-segment depression or T-wave inversion (Fig. 119.2), ST-segment elevation, while sometimes observed, is, by definition, never sustained. There will always be a clear-cut rise in the serum biomarkers to levels that are diagnostic for myocardial infarction. Thus, the essential difference between UA and N-STEMI is mainly related to the amount of biomarkers of myocardial injury.
|
|
|
Figure 119.1. The interrelationship of the components of ACS on presentation, during evolution and at final outcome [Adapted from Braunwald E, et al. (1)]. |
Epidemiology of N-STEMI
In the United States, two million patients are admitted annually to cardiac care units with ACS. The number of hospital admissions for patients with UA/N-STEMI is greater than the number with STEMI: 1.4 million and 600,000, respectively (7). The consequences of N-STE-ACS are not benign: among those who reach the hospital alive, approximately 13% of patients will die in the succeeding six months, and 8% will be left with unstable angina (8). The frequency of new stroke ranges between 1.5% and 3%, and rehospitalization for a further episode of ACS ranges between 17% and 20% over the same time interval. Survival data indicate that the risk associated with N-STEMI is greatest during the first 15 to 30 days from symptom presentation.
The Euro Heart Survey–Acute Coronary Syndromes (EHS–ACS) (9) and the Global Registry of Acute Coronary Events (GRACE) studies (8) provided insight into the practice of cardiology in different hospital settings and in different countries. EHS–ACS recorded prospectively 14,271 patients admitted with chest pain, with subsequently documented ACS in 10,484 (73%) of these. GRACE identified, in a prospective or retrospective manner, 11,543 patients with a final diagnosis of myocardial infarction or unstable angina—i.e., an ACS—in 10,709 patients (93%).
|
Table 119.1 Principal Presentations of Unstable Angina |
||||||
|
In both EHS–ACS and GRACE, about half of all patients underwent diagnostic coronary angiography, and percutaneous revascularization (PCI) was performed in 40% of patients admitted with ST elevation and in about a quarter of patients without initial ST elevation. Inpatient medical therapy included aspirin in over 90% of patients, appropriate use of unfractionated or low molecular weight heparin, but low use of glycoprotein IIb/IIIa receptor blockers when compared to guideline recommendations. Therapy at discharge included aspirin and/or ticlopidine/clopidogrel in over 90% of patients, ACE inhibitors (EHS–ACS 56%, GRACE 55%), β-blockers (EHS–ACS 73%, GRACE 71%), and statins (EHS–ACS 53%, GRACE 47%) (8,9). These findings indicate an increasing awareness of the need for preventive medication in most patients with ACS.
|
Table 119.2 Grading of Angina Pectoris According to the Canadian Cardiovascular Society Classification [Modified from reference 1] |
||||||||
|
|
|
|
Figure 119.2. The differentiation of unstable angina/non–ST-segment elevation myocardial infarction from ST-segment elevation myocardial infarction. |
Pathogenesis of N-STE-ACS
N-STE-ACS are usually caused by a sudden reduction of myocardial perfusion resulting from coronary artery narrowing due to a nonocclusive thrombus. The latter, in turn, is a consequence of disruption or erosion of an atherosclerotic coronary artery plaque. Distal microembolization of thrombus and disrupted plaque components may further reduce perfusion of the distal microvasculature. Recent research has focused on the characterization of coronary atherosclerotic plaques more prone to rupture—termed, vulnerable plaque (10). The vulnerable plaque is characterized by a necrotic lipid core infiltrated by inflammatory cells—macrophages and lymphocytes, with evidence of intraplaque hemorrhage and abundant generation of vasa vasorum on the adventitial site, surrounded by a thin fibrous cap (10). The most convincing hypothesis to explain plaque rupture is based on the critical role of inflammatory mediators driving the expression of proteases and proteolytic inhibitors that progressively weaken the fibrous cap, leading to plaque rupture (11).
The severity of coronary arterial obstruction and the volume of affected myocardium determine the pattern of clinical presentation. Patients with complete occlusion may manifest with a STEMI if the lesion occludes an artery supplying a substantial volume of myocardium, although the same occlusion in the presence of extensive collateralization may manifest as a N-STEMI or UA.
Early Evaluation and Risk Stratification
Immediate Concerns
ACS constitutes a clinical emergency. Therefore, early recognition and initiation of treatment is mandatory. Every patient with chest pain should be comprehensively evaluated, including a history and clinical examination of the cardiovascular system, the immediate recording of a resting ECG, and urgent evaluation of the serum markers of myocardial injury. Particular attention must be paid to the factors that influence the patient's risk stratification. These factors are found among the clinical features, the magnitude of ECG change, and the elevation of serum markers of myocardial necrosis. Among those without ST elevation on the ECG, an ACS is diagnosed by the presence of a clinical syndrome of acute ischemia with either pain at rest or a crescendo pattern of ischemic pain with minimal exertion, plus electrocardiographic and/or marker evidence of acute ischemic injury. The predictive accuracy of ST elevation for a final diagnosis of MI is very high, but for non-ST elevation MI, less than 50% are suspected as infarction on initial presentation.
Within the spectrum of ACS, N-STEMI represents the most difficult diagnostic challenge. Separation of N-STEMI from UA is based on the biomarker elevation in the former and the absence of detectable marker release in the latter (repeat assay at 6 to 12 hours after presentation is recommended).
Tools for Risk Stratification
Symptoms and Physical Examination
The features of cardiac ischemic chest pain are usually well recognized. The pain may vary in severity from mild compressive discomfort to sharp, severe pain. It may be located in the anterior chest, particularly substernally, or predominantly involve the mandible, neck, shoulders, either or both arms, the back, or epigastrium. It may be associated with shortness of breath, perspiration, palpitations, nausea or vomiting; however, none of these features predicts the severity of the underlying coronary involvement. The pain is generally of short duration but may last longer than 30 minutes without necessarily resulting in myocardial infarction. In ACS, the chest pain is frequently spontaneous in onset and unrelated to the usual stressors known to precipitate stable angina pectoris. It may occur with no—or less than the usual amount of—provocation, and be more severe or more prolonged. Less frequently, ACS may present with little or no chest pain but, instead, with atypical pain, or it can be accompanied by the features of an acute transient reduction in cardiac output—tachycardia, hypotension, and poor peripheral circulation, pulmonary venous congestion, breathlessness or pulmonary edema or, rarely, a potentially lethal ventricular tachyarrhythmia—a rapid heart rate with a weak or nonpalpable pulse (1).
Male gender, age above 50 years and, in women, early menopause, as well as a history of smoking, dyslipidemia, hypertension, diabetes mellitus, and/or a family history of coronary disease all increase the likelihood of ACS in a given patient with chest pain. Repeated attacks of chest pain or ongoing chest pain before admission, or pain which recurs on treatment, is associated with a worse outcome.
Physical examination often fails to contribute to the diagnosis of ACS. There may be no abnormal findings. However, a fourth heart sound, a mitral regurgitant murmur, or signs of pulmonary congestion are suggestive of transient ischemic myocardial dysfunction (1).
Heart failure (HF) is a frequent complication of ACS (12) and significantly worsens the prognosis of patients with ischemic heart disease (13). In a recent subanalysis of the GRACE Registry, HF on hospital admission was associated with an approximately 3- to 4-fold increase in hospital and 6-month death rates (14). HF was also associated with longer hospital stay and higher readmission rates. As in previous studies, the development of HF during hospital stay—as opposed to HF at admission—was associated with an even worse outcome (13,15). Importantly, there was a reduced frequency of PCI and lower β-blocker usage among patients with HF on admission. Notably, given the high mortality rate of patients with HF and ACS, this group would be expected to derive an even greater benefit from revascularization and, indeed, patients with HF who underwent revascularization had lower cumulative 6-month mortality rates than those who did not, even after adjustment for baseline differences (14).
Electrocardiogram
The presence of ECG changes, especially when occurring at rest and associated with angina, are a powerful indicator of higher risk. ST elevation and ST depression are well recognized electrocardiographic markers of risk. It has been demonstrated that when the other elements of baseline risk have been under control, ST deviation conveys the same risk for death whether this deviation is upwards or downwards (16) (Fig. 119.3). New onset T-wave changes—especially T-wave inversion, although less specific—are also important markers of subendocardial ischemia. Clinically, the normalization of ECG alterations and anginal relief are very important within minutes after sublingual nitrate administration; persistence of pain and ECG alterations for more than 20 minutes despite repeated nitrate administration is a marker of increased risk for myocardial infarction (1).
Biochemical Markers
Not all patients presenting with N-STE-ACS have elevated serum markers; at the time of the initial assessment, these markers may be within normal ranges, especially when they have been obtained very shortly after the onset of chest pain. All patients who have normal serum marker results on presentation must have a second assessment 4 to 6 hours later, or 8 to 12 hours after the onset of symptoms, whichever is longer. Elevated levels of creatine kinase (CK), creatine kinase MB iso-enzyme (CK-MB), troponin T or I, and myoglobin are indicators of myocardial injury (Table 119.3).
|
|
|
Figure 119.3. Probability of 30-day mortality among patients with ACS and different ECG patterns at admission [From Savonitto S, et al. (15): Savonitto S, Ardissino D, Granger CB, et al. Prognostic value of the admission electrocardiogram in acute coronary syndromes. JAMA. 1999;281:707–713.] |
Myoglobin is the earliest marker of an infarct event to appear in the serum. Although myoglobin is a very sensitive indicator of infarction, its clinical usefulness as the sole marker of myocardial injury/infarction is limited by the high incidence of false-positive results. CK in conjunction with CK-MB, CK-MB alone (17), and the troponins (18) are all sensitive and specific markers of myocardial injury/infarction that appear within the serum in raised amounts from about 4 hours after the onset of the ischemic event. Whereas CK and CK-MB are cleared from the serum within 2 to 3 days, an elevation of the troponin level may persist for up to 14 days after an event, making the troponins poor markers of early reinfarction.
|
Table 119.3 Advantages and Disadvantages of Biochemical Cardiac Markers for the Evaluation and Management of Patients with Suspected ACS [Modified from Braunwald E, et al. (1)]. |
|||||||||||||||
|
|||||||||||||||
|
|
|||||||||||||||
|
Figure 119.4. Relationship between cardiac troponin levels and risk of mortality in patients with ACS. [From Antman EM, et al. (20): Antman EM, Tanasjevic MJ, Thompson B, et al. Cardiac specific troponin I levels to predict the risk of mortality in patients with acute coronary syndromes. N Engl J Med 1996;335:1342–1349.] |
The bedside use of a “multi-marker strategy” that evaluated CK-MB, troponin I or T, and myoglobin in combination proved much superior to any “single-marker” strategy, and was also better than CK-MB and troponin without myoglobin in reaching an earlier diagnosis and identifying those at higher risk of death or MI by 30 days (19). Elevated levels of troponin T or I (20,21,22) or CK-MB (17) on admission indicate a poorer outcome (Fig. 119.4). The later appearance of an elevated troponin level, suggesting ongoing ischemia, is also associated with higher risk (23).
Extensive evidence supports the powerful and independent prediction of thrombotic complications, including MI and death, associated with troponin elevation (21). Furthermore, the evidence from trials of PCI revascularization suggests that troponins can be used as one part of the measures to identify higher risk—although it is not the sole arbiter of risk—and the potential for gain from the interventional procedures (24,25). Newer generation troponin assays have higher sensitivity and diagnostic accuracy. With newer generation assays, very minor increases in troponins are noted when as little as 1 gram of myocardium is necrotic. These minor increases do predict a higher risk of cardiac complications and death. In all instances, the risk predictors should complete, rather than replace, clinical judgment.
Certain biomarkers reflect an upregulation of the inflammatory/thrombotic systems—for example, high sensitivity C reactive protein (hsCRP), interleukin 6 (IL-6), CD40 ligand, and platelet–monocyte complexes. These inflammatory markers may be upregulated before the patient's presentation with ACS, but the acute phase reactant biomarkers are also elevated as a consequence of myocyte injury. Elevation of both hsCRP and troponin signifies a substantially higher risk of death—approximately 14% at one year—than either marker alone. In the absence of both markers, the patient is at very low risk of future cardiac events—less than 2%—based on FRISC 2 data (26). Importantly, whereas troponins predict the hazard of acute events, including acute MI and death, hsCRP on presentation does not independently predict the risk of death during hospitalization but is a powerful predictor of death in the following 1 to 2 years. The extent to which these biomarkers add to the predictive accuracy of established risk models remains to be tested (27). Finally, recent investigations demonstrated the association of a single B-type natriuretic peptide (BNP) measured after presentation with an ACS with short-term and long-term risk of death and HF (28). More recently, changes in BNP over time predicted long-term outcomes, thus providing a tool that could be used to tailor therapy after ACS (29).
Imaging Modalities
Echocardiographic ultrasound evaluation may be extremely useful in early evaluation of left ventricular function and to exclude nonischemic causes of chest pain, ECG alterations, and elevated biomarker levels. With increasing emphasis on early reperfusion and prevention of left ventricular remodeling, echocardiography is also assuming a prominent role in the setting of ACS (30). This imaging modality is noninvasive, cheap, and is an ideal portable imaging technique. Newer modalities, including myocardial contrast echocardiography for the assessment of perfusion, also hold promise (31). Other techniques such as single photon emission computed tomography or magnetic resonance imaging can detect wall motion abnormalities in patients with recent or established infarction, but their role remains to be determined.
After clinical stabilization of low-risk ACS patients, exercise stress testing may be appropriate. Early-onset symptoms during exercise, a short exercise time, a fall in blood pressure during exertion, ST-segment elevation, new postexercise ST-segment depression and/or prolonged ST-segment depression are the characteristics of a strongly positive test. Stress echocardiography and/or myocardial perfusion imaging should be reserved for the patient with a particular clinical problem, when such specialized facilities are available locally. If the functional test demonstrates ischemia, investigation by coronary angiography is advised. The more strongly positive the test, the earlier angiography should be undertaken. Angiography defines the nature and extent of the coronary disease and enables the planning of appropriate revascularization.
Estimation of the Level of Risk and Risk Scores
The patient with N-STE-ACS is at risk of major cardiovascular complications and death, and the extent of this risk is dependent upon acute and preexisting risk factors (Table 119.4). These risk factors not only predict the hazards of early cardiac events, but also of future cerebrovascular and peripheral vascular complications. In such patients, early risk stratification plays a central role, as the benefit of newer, more aggressive, and costly treatment strategies seem to be proportional to the risk of adverse clinical events (32,33,34) (Figs. 119.5–119.7). Different scores are now available based on initial clinical history, ECG, and laboratory tests that enable early risk stratification on admission (Table 119.5).
|
Table 119.4 Risk Indicators of a Poor Outcome in ACS |
||||
|
The Thrombolysis In Myocardial Infarction (TIMI) (35) and platelet glycoprotein IIb/IIIa in unstable angina: Receptor Suppression Using Integrilin (PURSUIT) (36) scores were developed with the databases from large clinical trials of N-STE-ACS. The more recent Global Registry of Acute Coronary Events (GRACE) score was developed from the registry (27), with a population of patients across the entire spectrum of ACS. All these scores were developed for short-term prognosis: events in-hospital for the GRACE risk score (RS) (37), at 14 days for the TIMI RS, and at 30 days for the PURSUIT RS. Nevertheless, a significant proportion of adverse events in N-STE-ACS patients occur after the first 30 days, and it is not known whether these RSs can also predict their occurrence. On the other hand, it has been demonstrated that an early invasive strategy has a prognostic benefit long term (38). Recently, the GRACE risk model has been demonstrated to have a good predictive accuracy for death or nonfatal MI at 1 year (37).
Hospital Care and Management Strategies
Early Pharmacologic Treatment
Control of Pain
While analgesics have no influence on the pathophysiological process, narcotic analgesia with IV morphine sulphate and/or sedation with oral benzodiazepines in standard doses may assist in alleviating the patient's pain and anxiety. As morphine may induce nausea and vomiting, it is advisable to premedicate the patient with IV metoclopramide prior to commencing the IV morphine titration. It is important to be aware of other analgesic treatments such as tramadol, a synthetic analogue of codeine, which may have been administered by paramedical staff during transport to the hospital. Adverse interactions might arise if a narcotic analgesic were administered inadvertently shortly thereafter. Intravenous injection of analgesics and other drugs should be preferred, because intramuscular injection may perturb certain serum markers of cardiac injury/infarction (1), have variable absorption, and are, in general, more painful and less humane than IV injections.
Anti-ischemic Drugs
Nitrates, β-adrenergic blockade, and calcium channel blockade have been used to treat patients with ACS. These therapies aim to control symptoms, reduce myocardial ischemia, and prevent the dire complications of this syndrome. The randomized trials that have evaluated the effects of an antianginal agent against placebo therapy or compared one class of antianginal agent with another in ACS are relatively few and fairly small.
Nitrates
Nitrates act by reducing preload and afterload, promoting coronary vasodilation, relieving coronary vasospasm or vasoconstriction, and by putative effects upon platelet aggregability. These effects combine to improve myocardial blood flow and relieve ischemia. Although nitrates effectively relieve cardiac ischemic pain, they have not been found to improve the outcome in ACS (39). They may be administered sublingually, orally, or intravenously in standard doses (Table 119.6).
Beta-blockers
Beta-blockade reduces myocardial oxygen demand and diminishes ischemia. Although there are large trials that have demonstrated the benefit of β-blockade following acute myocardial infarction, there is limited evaluation of this treatment in N-STE-ACS. The effects of β-blockade upon subsequent myocardial infarction and survival are uncertain. The drugs that have been scrutinized in smaller trials or retrospective subgroup analysis are metoprolol (40), propranolol (41), and esmolol (42). Whichever β-blocker is selected, the dose should be titrated to obtain a resting heart rate of 50 to 60 beats per minute, while maintaining an adequate blood pressure and satisfactory peripheral perfusion.
Calcium Channel Blockers
Calcium channel blockers are a diverse group of compounds that cause smooth muscle relaxation by blocking cellular calcium entry. Their action results in coronary vasodilation and afterload reduction. The dihydropyridine group of calcium channel blockers may increase the resting heart rate, whereas the nondihydropyridine group—diltiazem and verapamil—reduce the resting heart rate, and thus tend to diminish myocardial oxygen demand. The Holland Interuniversity Nifedipine/Metoprolol Trial (40) showed that the short-acting dihydropyridine, nifedipine, was detrimental in comparison with placebo in unstable angina. Calcium channel blockers should be reserved for the control of intractable chest pain or hypertension that cannot be alleviated by other means. Diltiazem is a nondihydropyridine calcium channel blocker that is superior to placebo treatment in reducing reinfarction and postinfarction angina in non-Q wave myocardial infarction (43). Mortality was unaffected in the trial. A trial comparing diltiazem treatment to propranolol found no differences in outcome in groups of patients with unstable angina or Prinzmetal angina (44). In a trial that compared intravenous glyceryl trinitrate with intravenous diltiazem, the combined end point of refractory angina and myocardial infarction was less with diltiazem than with the nitrate (45). Although verapamil has similar effects to diltiazem, its effects in ACS have not been evaluated in any large trial. Dihydropyridines should be used only in combination with β-blockade, as the combination avoids induction of tachycardia. Short-acting dihydropyridine calcium channel blockers should not be used at all. The nondihydropyridine calcium channel blocker, diltiazem, may be used alone as an alternative therapy if it is not possible to use β-blockade. However, β-blockers are preferred in all other patients, as they have marked benefits in those who go on to develop MI. Furthermore, the use of any calcium channel blocker is contraindicated when there is left ventricular dysfunction.
|
|
|
Figure 119.5. Acute ischemia pathway [From Braunwald E, et al. (1): Braunwald E, Antman EM, Beasley JW, et al.; American College of Cardiology; American Heart Association. Committee on the Management of Patients With Unstable Angina. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non–ST-segment elevation myocardial infarction–summary article: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on the Management of Patients With Unstable Angina). J Am Coll Cardiol. 2002;40(7):1366–1374.] |
Antiplatelet Therapy (see Table 119.7)
Aspirin
Aspirin irreversibly inhibits cyclooxygenase-1, thus reducing the generation of thromboxane A2, a potent mediator of platelet aggregation. The most recent update of the Anti-thrombotic Trialists' Collaboration, based upon 287 studies in 13,500 patients, demonstrates a highly significant reduction in the risk of MI/stroke/vascular death as a result of antiplatelet treatment versus control (46). Overall, the event rates were 13.2% in control patients and 10.7% in those treated with antiplatelet therapy, a 22% relative risk reduction (46). In acute MI, and in other high risk patients, the absolute and relative risk reductions were greater: 23 per 1,000 fewer vascular deaths and 13 per 1,000 fewer MIs. Thus, abundant evidence supports the use of aspirin in patients with ACS.
|
|
|
Figure 119.6. Algorithm for the management of NSTE-ACS patients at high-intermediate risk undergoing coronary angiography. |
Additional antiplatelet treatment requires evidence of benefit on top of aspirin, rather than as an alternative to aspirin. Recent data suggest that the bleeding risk doubles for aspirin doses above versus below 160 mg daily, with no improved efficacy (1). Unless there are specific contraindications—intolerance or allergy; active bleeding; hemophilia; severe hypertension; retinal, genitourinary, or gastrointestinal bleeding; active peptic ulcer—aspirin should be given to all patients with N-STE-ACS as soon as possible and continued indefinitely.
Thienopyridines
Thienopyridines (ticlopidine and clopidogrel) inhibit adenosine diphosphate (ADP) mediated platelet aggregation and, although initial studies were conducted with ticlopidine, this has been superseded by clopidogrel due to a much superior safety and more rapid onset of action. The blockade of ADP receptors by thienopyridines is irreversible but relatively slow to became manifest—several days for ticlopidine. Furthermore, recent evidence indicates that a substantial number of individuals appear to be resistant to the antiplatelet action of thienopyridines. For this reason, a high loading dose of 300 to 600 mg of clopidogrel or 500 mg of ticlopidine can be used to obtain a rapid onset of action. As the antiaggregation effects of aspirin and thienopyridines are mediated by different mechanisms, an additive benefit by using both drugs may exist. In N-STE-ACS, the AHA/ACC guidelines recommend approximately nine months treatment with clopidogrel (1). Longer term treatment in higher risk vascular patients awaits the results of the large scale CHARISMA trial. The association of aspirin and clopidogrel increases the risk of bleeding during major surgery and coronary surgery (CABG), thus clopidogrel should be interrupted 5 to 7 days before elective surgery. If early diagnostic catheterization is scheduled within 24 to 36 hours, clopidogrel administration can be initiated after coronary angiography when it is clear that CABG will not be undertaken; in the case of immediate percutaneous revascularization, the therapy can be initiated with a loading dose immediately.
|
|
|||||||||
|
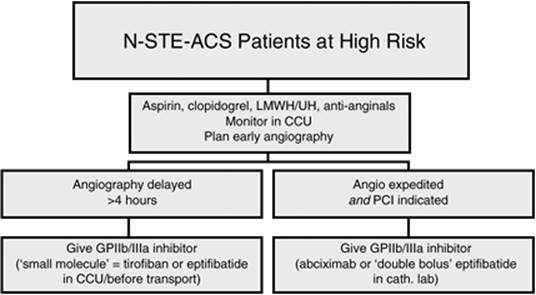
Figure 119.7. Algorithm for the treatment of high risk patients with unstable angina/non–ST-segment elevation myocardial infarction. |
|||||||||
|
Table 119.5 Risk Scores for N-STE-ACS |
|||||||||
|
Thienopyridines reduce the risk of stent thrombotic occlusion and are now part of standard treatment for at least four weeks in all patients undergoing elective PCI. With drug eluting stents, at least six months and perhaps 12 months of clopidogrel and aspirin are required (1). The CURE trial tested clopidogrel in 12,562 N-STE-ACS patients on top of background treatment and aspirin (47). A 2.1% absolute risk reduction (20% relative risk reduction, p <0.0001) occurred in the frequency of nonfatal MI, stroke, or cardiovascular death (47). The treatment effect was evident within the first 24 hours of starting therapy and, although the absolute benefits were greatest in the first three months of treatment, the relative risk reduction was the same beyond three months. Approximately 1% more patients experienced major bleeding, but there was no significant excess of life-threatening bleeding or hemorrhagic strokes (47). Nevertheless, in view of the irreversible nature of the ADP antagonism, current guidelines suggest that clopidogrel should be withheld for five days before CABG surgery. In candidates for very urgent CABG, a small molecule Gp IIb/IIIa inhibitor—eptifibatide or tirofiban—can be used before surgery.
Three new antiplatelet drugs are in phase III clinical trials, including a potent, fast-acting thienopyridine (prasugrel [48]), a reversible oral PGY12 inhibitor (AZD6140, a cyclopentyltriazolopyridimidine [49]), and a potent, short-acting intravenous PGY12 inhibitor (cangrelor [50]). In patients with N-STE-ACS, preliminary data from the DISPERSE 2 (Safety, Tolerability and Preliminary Efficacy of AZD6140, the First Oral Reversible ADP Receptor Antagonist, Compared with Clopidogrel in Patients with Non-ST-Segment Elevation Acute Coronary Syndrome) trial comparing AZD6140 with placebo demonstrated that AZD6140, 180 mg twice daily, achieved greater and more consistent platelet inhibition, and showed favorable effects on clinical outcomes without an increase in major bleeding (51).
Glycoprotein IIb/IIIa Receptor Antagonists
Platelet aggregation involves the GP IIb/IIIa receptor linked to fibrinogen or von Willebrand factor. Intravenous GP IIb/IIIa receptor antagonists have been extensively tested in patients with ACS and, in a meta-analysis of all the major randomized trials, the absolute risk reduction for death or MI at 30 days was 1% (11.8% control vs. 10.8% with Gp IIb/IIIa) (52). The absolute treatment benefit was largest in high risk patients—in particular, those with evidence of troponin release or those undergoing acute PCI (52). Among those without troponin elevation or PCI, no significant benefits were observed with Gp IIb/IIIa administration.
The CREDO (Clopidogrel for the Reduction of Events During Observation) trial has helped to resolve the question of whether clopidogrel plus GP IIb/IIIa receptor antagonists may be required in patients undergoing PCI (53). Approximately half of the patients received GP IIb/IIIa antagonists (a non-randomized subset) and two thirds had presented with an ACS. The frequency of MI, stroke, or death at one year was reduced with clopidogrel from 11.5% to 8.5% (p = 0.02), with similar risk ratios in the presence or absence of GP IIb/IIIa inhibitors (53). In the ISAR-REACT 2 (Abciximab in Patients with Acute Coronary Syndromes Undergoing Percutaneous Coronary Intervention After Clopidogrel Pre-treatment) trial, abciximab reduced the composite of death, MI, or urgent target vessel revascularization within 30 days compared with placebo by 25% among 2,022 patients with N-STE-ACS, all of whom received clopidogrel, 600 mg, at least 2 h before PCI (54). However, the benefit of abciximab was observed only in patients with N-STEMI (54).
|
Table 119.6 Dosages of NTG and Nitrates in Angina [Modified from Braunwald et al. (1).] |
|||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||
|
Table 119.7 Commonly Used Antiplatelet and Anticoagulant Agents in Unstable Angina and N-STEMI — Drug Doses and Special Precautions |
|||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||
The EVEREST (Randomized Comparison of Upstream Tirofiban versus Downstream High Bolus Dose Tirofiban or Abciximab on Tissue-Level Perfusion and Troponin Release in High-Risk Acute Coronary Syndromes Treated with Percutaneous Coronary Interventions) trial of 93 patients with high risk N-STE-ACS compared upstream tirofiban given in the CCU several hours before coronary angiography to downstream (immediately after coronary angiography) high bolus-dose tirofiban and downstream abciximab given 10 min before PCI (55). Upstream tirofiban improved TIMI myocardial perfusion before and after PCI, achieved a higher myocardial contrast echocardiographic score, and resulted in lower rates of postprocedure troponin elevation (55). Results from the open-label ACUITY (Acute Catheterization and Urgent Intervention Triage strategy) timing trial in 9,207 patients randomized to upstream GP IIb/IIIa inhibitors administered, on average, 6 hours before PCI compared with downstream use begun in the catheterization laboratory demonstrated that a downstream strategy was noninferior for a quaternary net clinical benefit end point—death, myocardial infarction, unplanned revascularization for ischemia, major bleeding—but did not satisfy the noninferiority criterion for the triple ischemic end point (56). A cost-effective analysis using data from the TACTICS–TIMI-18 (Prognostic Implications of Elevated Troponin in Patients with Suspected Acute Coronary Syndrome but no Critical Epicardial Coronary Disease–Thrombolysis In Myocardial Infarction-18) trial concluded that the upstream use of tirofiban was superior to selective use and was cost-effective in moderate to high risk patients (57). Taken together, these studies suggest that upstream GPI therapy may be more effective than downstream use in moderate to high risk patients managed with an invasive strategy in whom immediate catheterization is not planned. The EARLY ACS (Early Glycoprotein IIb/IIIa Inhibition in Non-ST-Segment Elevation Acute Coronary Syndrome) study (58) is an ongoing randomized, double-blind, clinical trial comparing upstream double-bolus eptifibatide to downstream selective use in high risk patients with N-STE-ACS who are not undergoing PCI in the first 12 hours, and should help shed further light on this issue.
Anticoagulation Therapy
Thrombin (Factor IIa) is a highly potent stimulus not only of the generation of fibrin, but also platelet activation. In addition, it leads to monocyte chemotaxis, mitogenesis, increased permeability of the vascular wall, and secretion of cytokines and growth factors from smooth muscle cells. Effective antithrombotic treatment requires the inhibition of both platelet function and thrombin.
Unfractionated heparin has been widely used, but suffers from practical difficulties in maintaining antithrombin activity within the therapeutic range, which are influenced by acute phase proteins and binding to antithrombins. Nevertheless, there is clear evidence that a form of heparin, either unfractionated or low molecular weight heparin (LMWH), is superior to placebo in patients with ACS. The meta-analysis of trials demonstrates a reduction in absolute rates of death or MI from 7.4% to 4.5% (odds ratio 0.53, 95% CI 0.38 to 0.73) (59).
Direct antithrombins may provide significant advantages over the indirect inhibitors (unfractionated and LMWH). Combined analysis of the hirudin studies suggests a relative risk reduction compared to unfractionated heparin. At this point in time, hirudin has only been approved for patients with heparin-induced thrombocytopenia, and none of the hirudins are licensed for ACS. LMWHs partially inhibit factor Xa of the coagulation cascade, but newer specific inhibitors of Xa have been developed—for example, bivaliridin and fondaparinux. Such agents inhibit thrombin generation as distinct from thrombin activity. In the recently published ACUITY trial, 13,819 patients with moderate to high risk N-STE-ACS were randomized to 1 of 3 arms: (1) heparin + GP IIb/IIIa inhibitors (standard), (2) bivalirudin + GP IIb/IIIa inhibitors (combination), or (3) bivalirudin alone (monotherapy) (56). Combination therapy was noninferior to the standard (neither arm was superior), while monotherapy was superior to standard therapy, driven by a reduction in bleeding with bivalirudin monotherapy (56). A common theme among the studies evaluating bivalirudin is the marked reduction in bleeding observed when GP IIb/IIIa inhibitors are not routinely administered.
Direct comparisons with LMWH did not show advantages for fondaparinux over enoxaparin in reducing the risk of ischemic events at nine days, but it substantially reduces major bleeding and improves long term mortality and morbidity (60). The results of a randomized, double-blind trial of fondaparinux versus enoxaparin in 20,000 patients with unstable angina or non-STEMI are pending (OASIS 5) (61).
An alternative approach involves an orally administered, direct thrombin antagonist, ximelagatran. It is converted to melagatran in the circulation and directly binds with the active site of the thrombin molecule. Ximelagatran does not require anticoagulation monitoring, and is administered as a fixed dose. In a phase II trial, it reduced the frequency of death, nonfatal MI, and severe recurrent ischemia compared to placebo treatment (hazard ratio 0.76, 95% CI 0.59 to 0.98) (62). Ximelagatran has also been used as an alternative to warfarin in the management of atrial fibrillation (SPORTIF trials), and demonstrates similar efficacy but less bleeding than warfarin. A potential hazard of ximelagatran involves alterations in liver enzymes: 6% to 10% of patients experience a rise in alanine aminotransferase to at least three times the upper limit of normal (62). This appears to resolve with or without cessation of drug treatment. Widespread application of ximelagatran as an alternative to other antithrombins in ACS requires large scale safety and efficacy studies.
HMG-CoA Reductase Inhibitors
In the past year, ancillary analyses from randomized trials of intensive statin therapy and mechanistic studies provided new insights into the role of lowering lipids in patients with ACS. The case for intensive statin therapy after N-STE-ACS was strengthened by a meta-analysis of 6 randomized controlled trials demonstrating that intensive, but not moderate, statin treatment reduces early recurrent ischemic events and stroke (63). A detailed comparison of two trials comparing intensive to moderate statin therapy emphasized the importance of intensive therapy beginning in the early post-ACS phase, and suggested that the early benefit may be associated with a more profound reduction in CRP achieved with earlier intensive therapy (64).
These results have been rapidly reflected in subsequent changes in the particular statin and dose prescribed. A trend-over-time analysis in Ontario, Canada, documented a greater than two-fold increase in the use of atorvastatin, 80 mg, within months after publication of the PROVE IT–TIMI-22 (Pravastatin or Atorvastatin Evaluation and Infection Therapy Thrombolysis In Myocardial Infarction-22) and REVERSAL (Reversing Atherosclerosis With Aggressive Lipid Lowering) studies (65).
The benefit of atorvastatin, 80 mg, compared with pravastatin, 40 mg, occurred within 30 days in the PROVE IT–TIMI-22 trial (28% reduction in the hazard ratio of death, myocardial infarction, or rehospitalization for recurrent ACS) consistent with greater early pleiotropic effects (66). A number of potential early benefits of statins independent of LDL have been postulated and include favorable effects on inflammation, endothelial function, and the coagulation cascade (67). In a secondary analysis from the PROVE IT–TIMI-22 trial, randomization to intensive statin therapy was associated with a lower CRP level, irrespective of the presence of a single or multiple uncontrolled cardiovascular risk factors (68). Endothelium-dependent, flow-mediated dilation increased between one and four months after initiating either atorvastatin, 80 mg, or pravastatin, 40 mg, in the BRAVER (Intensity of Lipid Lowering with Statins and Brachial Artery Vascular Endothelium Reactivity After Acute Coronary Syndromes) trial, independent of reductions in LDL and CRP (69).
Two important observations regarding the safety of statins were reported during the past year. An analysis of 15,693 patients from the GRACE (Global Registry of Acute Coronary Events) registry demonstrated that, in general, patients receiving the combination of clopidogrel and a statin did not have an increase in clinical events, thus suggesting no adverse interaction exists between these two therapies. Indeed, even after adjustment for differences in baseline variables and bias in treatment allocation, an analysis of patients administered aspirin with or without clopidogrel and with or without statin revealed that the group taking all 3 drugs had the lowest mortality (70). In an analysis of patients who achieved very low LDL concentrations in the PROVE IT–TIMI-22 trial, there was no adverse safety signal, while clinical efficacy improved as the LDL was lowered to less than 40 mg/dL (71), thus suggesting that downward adjustment of the statin dose is not required in patients who achieve very low LDL concentrations. Despite such favorable results with high intensity statins, only 44% of patients randomized to atorvastatin, 80 mg, with baseline total cholesterol less than 240 mg/dL (average LDL 106 mg/dL) achieved the dual goals of LDL less than 70 mg/dL and CRP less than 2 mg/L (72). Better control of traditional risk factors (68) and even more potent pharmacologic therapy are necessary to achieve these ambitious targets that have been associated with relatively lower rates of death and recurrent ischemic complications (73).
Invasive Strategies
The Role of Coronary Angiography
Presently, coronary angiography represents the only reliable tool for the assessment of coronary anatomy in patients with N-STE-ACS. Patients with high risk coronary lesions—left main disease, three vessel disease, and proximal left anterior descending coronary artery disease—represent about 50% of all patients with N-STE-ACS (74,75) and, despite the use of risk scores and biomarkers of myocardial damage, it is frequently impossible to correctly identify these high risk patients who are most likely to benefit from revascularization both in terms of survival and symptom improvement (Table 119.8). Thus, the concept of low and high risk patients suggested by the various scores derived by investigational studies and registry is rather relative. According to the TIMI risk score, about 50% of patients with N-STE-ACS are in the low risk subgroup (below score 3); nevertheless about 25% of these patients develop a major event—death, nonfatal MI, or urgent revascularization—within 14 days from hospitalization. Thus, as the predictive accuracy of these risk scores is rather low, all patients with N-STE-ACS should be regarded at risk to develop major coronary events. In this context, the early knowledge of coronary anatomy and the possibility to promptly restore myocardial perfusion appear to have important therapeutic and prognostic implications.
|
Table 119.8 High Risk Features Favoring an Early Invasive Strategy |
|
|
Early Conservative versus Invasive Strategies
Studies comparing head-to-head early conservative versus an early invasive strategy are flawed by the substantial rate of crossover patients originally randomized into the conservative arm who were treated invasively because of unstable symptoms. Indeed, when the difference in revascularization rate between the treatment arms is large, the benefit of revascularization strategy is evident. According to a recently published meta-analysis, managing N-STE-ACS by early invasive approach improves long-term survival and reduces late nonfatal myocardial infarction and rehospitalization for symptoms recurrence (76,77,78). Thus the issue is not whether but when a patient with N-STE-ACS should undergo coronary angiography and eventually revascularization. Combined data from seven large randomized trials indicate that the goal in patients with N-STE-ACS should be to perform early invasive therapy within 48 hours from hospital admission (76,77) (Fig. 119.8).
Obviously, coronary angiography should be anticipated if clinical instability occurs. This time interval is also supported by the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines) registry data, indicating that a delay of 46 hours is not associated with increased adverse events compared with a delay of only 23 hours (79). As clinical stabilization can be obtained pharmacologically in about 90% of patients with N-STE-ACS, this time delay appears reasonably applicable in the majority of cardiology centers. The best revascularization strategy (PCI or CABG) should be evaluated for each case according to coronary anatomy, clinical symptoms, and associated diseases.
|
|
|
Figure 119.8. Odds of non-fatal myocardial infarction (MI) from randomization to end of follow-up in a meta-analysis of 7 trials of routine versus selective invasive management of acute coronary syndromes (77). P = 0.51 for heterogeneity across the trials. CI = confidence interval; OR = odds ratio. |
References
1. Braunwald E, Antman EM, Beasley JW, et al.; American College of Cardiology; American Heart Association. Committee on the Management of Patients with Unstable Angina. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non–ST-segment elevation myocardial infarction–summary article: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on the Management of Patients with Unstable Angina). J Am Coll Cardiol. 2002;40(7):1366–1374.
2. Myler RK, Shaw RE, Stertzer SH, et al. Unstable angina and coronary angioplasty. Circulation. 1990;82(3 Suppl):II88–95.
3. Maseri A, Liuzzo G, Biasucci LM. Pathogenic mechanisms in unstable angina. Heart. 1999 Sep;82(Suppl 1):I2–4.
4. Giugliano RP, Braunwald E. The year in non-ST-segment elevation acute coronary syndromes. J Am Coll Cardiol. 2006;48(2):386–395.
5. Haywood LJ, Khan AH, de Guzman M. Prinzmetal angina. Normal arteries and multifocal electrocardiographic changes. JAMA. 1976;235(1):53–56.
6. Bory M, Pierron F, Panagides D, et al. Coronary artery spasm in patients with normal or near normal coronary arteries. Long-term follow-up of 277 patients. Eur Heart J. 1996;17:1015–1021.
7. National Center for Health Statistics. Detailed diagnoses and procedures: national hospital discharge survey, 1996. Hyattsville, MD: National Center for Health Statistics; 1998:13. Data from Vital and Health Statistics.
8. Fox KAA, Goodman SG, Klein W, et al; for the GRACE Investigators. Management of acute coronary syndromes. Variations in practice and outcome; findings from the Global Registry of Acute Coronary Events (GRACE). Eur Heart J. 2002;23:1177–1189.
9. Hasdai D, Behar S, Wallentin L, et al. A prospective survey of the characteristics, treatments and outcomes of patients with acute coronary syndromes in Europe and the Mediterranean Basin; the Euro Heart Survey of acute coronary syndromes (Euro Heart Survey ACS). Eur Heart J. 2002;23:1190–1201.
10. Virmani R, Burke AP, Farb A, et al. Pathology of the vulnerable plaque. J Am Coll Cardiol. 2006;47(Suppl C):C13–18.
11. Libby P. Act local, act global: inflammation and the multiplicity of “vulnerable” coronary plaques. J Am Coll Cardiol. 2005;45:1600–1602.
12. Steg PG, Goldberg RJ, Gore JM, et al. Baseline characteristics, management practices, and in-hospital outcomes of patients hospitalized with acute coronary syndromes in the Global Registry of Acute Coronary Events (GRACE). Am J Cardiol. 2002;90:358–363.
13. Bart BA, Shaw LK, McCants CB Jr, et al. Clinical determinants of mortality in patients with angiographically diagnosed ischemic or nonischemic cardiomyopathy. J Am Coll Cardiol. 1997;30:1002–1008.
14. Steg PG, Dabbous OH, Feldman LJ, et al. Determinants and prognostic impact of heart failure complicating acute coronary syndrome: observations from the Global Registry of Acute Coronary Events (GRACE). Circulation. 2004;109:494–499.
15. Spencer FA, Meyer TE, Gore JM, et al. Heterogeneity in the management and outcomes of patients with acute myocardial infarction complicated by heart failure: the National Registry of Myocardial Infarction. Circulation. 2002;105:2605–2610.
16. Savonitto S, Ardissino D, Granger CB, et al. Prognostic value of the admission electrocardiogram in acute coronary syndromes. JAMA. 1999;281:707–713.
17. Lloyd-Jones DM, Camargo CA, Giugliano RP, et al. Characteristics and prognosis of patients with suspected acute myocardial infarction and elevated MB relative index but normal total creatine kinase. Am J Cardiol. 1999;84:957–962.
18. Hamm CW, Goldmann BU, Heeschen C, et al. Emergency room triage of patients with acute chest pain by means of rapid testing for cardiac troponin T or troponin I. N Engl J Med. 1997;337:1648–1653.
19. Newby LK, Storrow AB, Gibler WB, et al. Bedside multimarker testing for risk stratification in chest pain units: the Chest Pain Evaluation by Creatine Kinase-MB, Myoglobin and Troponin I (CHECKMATE) Study. Circulation. 2001;103:1832–1837.
20. Ohman EM, Armstrong PW, Christenson RH, et al. Cardiac troponin T levels for risk stratification in acute myocardial ischaemia. N Engl J Med. 1996;335:1333–1341.
21. Antman EM, Tanasjevic MJ, Thompson B, et al. Cardiac specific troponin I levels to predict the risk of mortality in patients with acute coronary syndromes. N Engl J Med. 1996;335:1342–1349.
22. Heeschen C, Goldmann BU, Terres W, et al. Cardiovascular risk and therapeutic benefit of coronary intervention for patients with unstable angina according to the troponin T status. Eur Heart J. 2000;21:1159–1166.
23. Newby LK, Christenson RH, Ohman M, et al. Value of serial troponin T measures for early and late risk stratification in patients with acute coronary syndromes. Circulation. 1998;98:1853–1859.
24. Wallentin L, Lagerqvist B, Husted S, et al. Outcome at 1 year after an invasive compared with a non-invasive strategy in unstable coronary-artery disease: the FRISC II invasive randomised trial. Lancet. 2000;356:9–16.
25. Cannon CP, Weintraub WS, Demopoulos LA, et al. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879–1887.
26. Lindahl B, Toss H, Siegbahn A, et al. Markers of myocardial damage and inflammation in relation to long-term mortality in unstable coronary artery disease. N Engl J Med. 2000;343:1139–1147.
27. Granger CB, Goldberg RJ, Dabbous O, for the Global Registry of Acute Coronary Events Investigators, et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med. 2003;163:2345–2353.
28. Pfeffer MA, Pfeffer JM, Lamas GA. Development and prevention of congestive heart failure following myocardial infarction. Circulation. 1993;87(Suppl IV):IV-120–IV-125.
29. Stevenson LW, Perloff JK. The limited reliability of physical signs for estimating hemodynamics in chronic heart failure. JAMA. 1989;261:884–888.
30. Greaves SC. Role of echocardiography in acute coronary syndromes. Heart. 2002;88(4):419–425.
31. Greaves SC. Role of echocardiography in acute coronary syndromes. Heart. 2002;88(4):419–425.
32. Cannon CP, Weintraub WS, Demopoulos LA, et al. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879–1887.
33. Antman EM, Cohen M, McCabe C, et al. Enoxaparin is superior to unfractionated heparin for preventing clinical events at 1-year follow-up of TIMI 11B and ESSENCE. Eur Heart J. 2002;23:308–314.
34. Morrow DA, Antman EM, Snapinn SM, et al. An integrated clinical approach to predicting the benefit of tirofiban in non-ST elevation acute coronary syndromes. Application of the TIMI risk score for UA/NSTEMI in PRISM-PLUS. Eur Heart J. 2002;23:223–229.
35. Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-ST elevation MI. JAMA. 2000;284:835–842.
36. Boersma E, Pieper KS, Steyerberg EW, et al., for the PURSUIT Investigators. Predictors of outcome in patients with acute coronary syndromes without persistent ST-segment elevation. Results from an international trial of 9461 patients. Circulation. 2000;101:2557–2567.
37. de Araùjo Gonçalves P, Ferreira J, Aguiar C, et al. TIMI, PURSUIT, and GRACE risk scores: sustained prognostic value and interaction with revascularization in NSTE-ACS. Eur Heart J. 2005;26:865–872.
38. Fragmin and Fast Revascularization during Instability in Coronary artery disease (FRISC II) Investigators. Invasive compared with non-invasive treatment in unstable coronary artery disease: FRISC II prospective randomised multicentre study. Lancet. 1999;354:708–715.
39. Curfman GD, Heinsimer JA, Lozner EC, et al. Intravenous nitroglycerin in the treatment of spontaneous angina pectoris: a prospective randomized trial. Circulation. 1983;67:276–282.
40. HINT Group. Early treatment of unstable angina in the coronary care unit: a randomised double-blind, placebo controlled comparison of recurrent ischaemia in patients treated with nifedipine, metoprolol or both. Report of the Holland Interuniversity Nifedipine/Metoprolol Trial (HINT) Research Group. Br Heart J. 1986;56:400–413.
41. Gheorghiade M, Schultz L, Tilley B, et al. Effects of propranolol in non-Q wave acute myocardial infarction in the beta blocker heart attack trial. Am J Cardiol. 1990;66:129–133.
42. Hohnloser SH, Meinertz T, Kingenheben T, et al. Usefulness of esmolol in unstable angina pectoris. European Esmolol Study Group. Am J Cardiol. 1991;67:1319–1323.
43. Gibson RS, Boden WE, Theroux P, et al. Diltiazem and reinfarction in patients with non-Q wave myocardial infarction: results of a double-blind, randomized, multicenter trial. N Engl J Med. 1986;315:423–429.
44. Theroux P, Taeymans Y, Morissette D, et al. A randomized trial comparing propanolol and diltiazem in the treatment of unstable angina. J Am Coll Cardiol. 1985;5:717–722.
45. Gobel EJAM, Hautvast RWM, van Gilst WH, et al. Randomised, double blind trial of intravenous diltiazem versus glyceryl trinitrate for unstable angina pectoris. Lancet. 1995;346:1653–1657.
46. Antithrombotic Trialists' Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324:71–86.
47. The Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345:494–502.
48. Wiviott SD, Antman EM, Gibson CM, et al. Evaluation of prasugrel compared to clopidogrel in patients with acute coronary syndromes: design and rationale for the TRial to assess Improvement in Therapeutic Outcomes by optimizing platelet inhibition with prasugrel (TRITON-TIMI 38). Am Heart J. 2006;152:627–635.
49. Husted S, Emanuelsson H, Heptinstall S, et al. Pharmacodynamics, pharmacokinetics, and safety of the oral reversible P2Y12 antagonist AZD6140 with aspirin in patients with atherosclerosis: a double-blind comparison to clopidogrel with aspirin. Eur Heart J. 2006;27:1038–1047.
50. Greenbaum AB, Grines CL, Bittl JA, et al. Initial experience with an intravenous P2Y12 platelet receptor antagonist in patients undergoing percutaneous coronary intervention: results from a 2-part, phase II, multicenter, randomized, placebo- and active-controlled trial. Am Heart J. 2006;151:e1–689.
51. Cannon CP, Husted S, Storey RF, et al. The DISPERSE 2 trial: safety, tolerability and preliminary efficacy of AZD6140, the first oral reversible ADP receptor antagonist, compared with clopidogrel in patients with non-ST segment elevation acute coronary syndrome [Abstract]. Circulation. 2005;112:II615.
52. Boersma E, Harrington RA, Moliterno DJ, et al. Platelet glycoprotein IIb/IIIa inhibitors in acute coronary syndromes: a meta-analysis of all major randomised clinical trials. Lancet. 2002;359:189–198.
53. Steinhubl SR, Berger PB, Mann JT 3rd, et al., for the CREDO Investigators. Clopidogrel for the Reduction of Events During Observation. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;288:2411–2420.
54. Kastrati A, Mehilli J, Neumann FJ, et al. Abciximab in patients with acute coronary syndromes undergoing percutaneous coronary intervention after clopidogrel pretreatment: the ISAR-REACT 2 randomized trial. JAMA. 2006;295:1531–1538.
55. Bolognese L, Falsini G, Liistro F, et al. Randomized comparison of upstream tirofiban versus downstream high bolus dose tirofiban or abciximab on tissue-level perfusion and troponin release in high-risk acute coronary syndromes treated with percutaneous coronary interventions: the EVEREST trial. J Am Coll Cardiol. 2006;47:522–528.
56. Stone GW, McLaurin BT, Cox DA, et al.; ACUITY Investigators. Bivalirudin for patients with acute coronary syndromes. N Engl J Med. 2006;355:2203–2016.
57. Glaser R, Glick HA, Herrmann HC, et al. The role of risk stratification in the decision to provide upstream versus selective glycoprotein IIb/IIIa inhibitors for acute coronary syndromes: a cost-effectiveness analysis. J Am Coll Cardiol. 2006;47:529–537.
58. Giugliano RP, Newby LK, Harrington RA, et al. The early glycoprotein IIb/IIIa inhibition in non-ST-segment elevation acute coronary syndrome (EARLY ACS) trial: a randomized placebo-controlled trial evaluating the clinical benefits of early front-loaded eptifibatide in the treatment of patients with non-ST-segment elevation acute coronary syndrome-study design and rationale. Am Heart J. 2005;149:994–1002.
59. Eikelboom JW, Anand SS, Malmberg K, et al. Unfractionated heparin and low-molecular-weight heparin in acute coronary syndrome without ST elevation: a meta-analysis. Lancet. 2000;355:1936–1942.
60. Fifth Organization to Assess Strategies in Acute Ischemic Syndromes Investigators; Yusuf S, Mehta SR, Chrolavicius S, et al. Comparison of fondaparinux and enoxaparin in acute coronary syndromes. N Engl J Med. 2006;354:14641476.
61. MICHELANGELO OASIS 5 Steering Committee. Design and rationale of the MICHELANGELO Organization to Assess Strategies in Acute Ischemic Syndromes (OASIS)-5 trial program evaluating fondaparinux, a synthetic factor Xa inhibitor, in patients with non-ST-segment elevation acute coronary syndromes. Am Heart J. 2005;150:1107.
62. Wallentin L, Wilcox RG, Weaver WD, et al. Oral ximelagatran for secondary prophylaxis after myocardial infarction: the ESTEEM randomised controlled trial. Lancet. 2003;362:789–797.
63. Schwartz GG, Olsson AG. The case for intensive statin therapy after acute coronary syndromes. Am J Cardiol. 2005;96:45F–53F.
64. Wiviott SD, de Lemos JA, Cannon CP, et al. A tale of two trials: a comparison of the post-acute coronary syndrome lipid-lowering trials A to Z and PROVE IT-TIMI 22. Circulation. 2006;113:1406–1414.
65. Austin PC, Mamdani MM. Impact of the pravastatin or atorvastatin evaluation and infection therapy-thrombolysis in myocardial infarction 22/Reversal of Atherosclerosis with Aggressive Lipid Lowering trials on trends in intensive versus moderate statin therapy in Ontario, Canada. Circulation. 2005;112:1296–1300.
66. Ray KK, Cannon CP, McCabe CH, et al. Early and late benefits of high-dose atorvastatin in patients with acute coronary syndromes: results from the PROVE IT-TIMI 22 trial. J Am Coll Cardiol. 2005;46:1405–1410.
67. Ray KK, Cannon CP. The potential relevance of the multiple lipid-independent (pleiotropic) effects of statins in the management of acute coronary syndromes. J Am Coll Cardiol. 2005;46:1425–1433.
68. Ray KK, Cannon CP, Cairns R, et al. Relationship between uncontrolled risk factors and C-reactive protein levels in patients receiving standard or intensive statin therapy for acute coronary syndromes in the PROVE IT-TIMI 22 trial. J Am Coll Cardiol. 2005;46:1417–1424.
69. Dupuis J, Tardif JC, Rouleau JL, et al. Intensity of lipid lowering with statins and brachial artery vascular endothelium reactivity after acute coronary syndromes (from the BRAVER trial). Am J Cardiol. 2005;96:1207–1213.
70. Lim MJ, Spencer FA, Gore JM, et al. Impact of combined pharmacologic treatment with clopidogrel and a statin on outcomes of patients with non-ST-segment elevation acute coronary syndromes: perspectives from a large multinational registry. Eur Heart J. 2005;26:1063–1069.
71. Wiviott SD, Cannon CP, Morrow DA, et al. Can low-density lipoprotein be too low? The safety and efficacy of achieving very low low-density lipoprotein with intensive statin therapy: a PROVE IT-TIMI 22 substudy. J Am Coll Cardiol. 2005;46:1411–1416.
72. Ridker PM, Morrow DA, Rose LM, et al. Relative efficacy of atorvastatin 80 mg and pravastatin 40 mg in achieving the dual goals of low-density lipoprotein cholesterol <70 mg/dL and C-reactive protein <2 mg/L: an analysis of the PROVE-IT TIMI-22 trial. J Am Coll Cardiol. 2005;45:1644–1648.
73. Ridker PM, Cannon CP, Morrow D, et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med. 2005;352:20–28.
74. Fox KA, Anderson FA, Dabbous OH, et al. Intervention in acute coronary syndromes: do patients undergo intervention on the basis of their risk characteristics? The global registry of acute coronary events (GRACE). Heart. 2007 Feb;93(2):177–182. Epub 2006 Jun 6.
75. Heras M, Bueno H, Bardaji A, et al; DESCARTES Investigators. Magnitude and consequences of undertreatment of high-risk patients with non-ST segment elevation acute coronary syndromes: insights from the DESCARTES Registry. Heart. 2006;92:1571–1576.
76. Mehta SR, Cannon CP, Fox KAA, et al. Routine versus selective invasive strategies in patients with acute coronary syndromes: a collaborative meta-analysis of the randomized trials. JAMA. 2005;293:2908–2917.
77. Bavry AA, Kumbhani DJ, Rassi AN, et al. Benefit of early invasive therapy in acute coronary syndromes: a meta-analysis of contemporary randomized clinical trials. J Am Coll Cardiol. 2006;48:1319–1325.
78. Bavry AA, Kumbhani DJ, Quiroz R, et al. Invasive therapy along with glycoprotein IIb/IIIa inhibitors and intracoronary stents improves survival in non-ST-segment elevation acute coronary syndromes: a meta-analysis and review of the literature. Am J Cardiol. 2004;93:830–835.
79. Ryan JW, Peterson ED, Chen AY, et al.; CRUSADE Investigators. Optimal timing of intervention in non-ST-segment elevation acute coronary syndromes: insights from the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines) Registry. Circulation. 2005;112:3049–3057.