Rhonda S. Fishel
Jamie Hochman
Case History
November 1, 2005: The patient is a 50-year-old Caucasian female who has had a 3-month history of intermittent left suprapubic pain, nausea, and fever; the episodes last 24 to 48 hours. Her past history is significant for mild hypothyroidism for which she takes levothyroxine. Her last menses was 2 years ago, and she has been followed for a uterine leiomyoma. She does not smoke or drink. The patient is a surgeon and an intensivist. Physical exam is remarkable for a 6-cm uterine mass, which is not fixed. Ultrasonography demonstrates an irregular uterine mass, which does not have increased blood flow. The study is interpreted as a likely growth of a previously benign fibroid. On October 31, 2005, she undergoes a total abdominal hysterectomy and bilateral salpingo-oophorectomy; frozen section shows large areas of uterine necrosis but does not demonstrate malignant cells. On postoperative day 1, the permanent pathology is interpreted as a 9-cm high-grade uterine sarcoma. Her gynecologist, also a colleague, sits at the patient's bedside and delivers this diagnosis. That evening, the patient has a computed tomography (CT) scan of the chest, which shows a pulmonary metastasis. Some months later, the gynecologist reveals to the patient that he was so distraught from giving her bad news that night that he developed laryngitis for the next several days.
Practitioners who choose a career in critical care medicine—or other emergent fields—will soon realize that a significant focus of their practice will be delivering and processing bad news. The excitement of applying bold clinical skills, using advanced technology, and making life-or-death decisions in the most critical patients will be tempered by the need to participate in the most somber of discussions. Giving bad news is not easy, thrilling, or glamorous—but it is essential. Done appropriately, it will provide the patient and family solace in a time of pain; done poorly, it is injury added to illness.
In this chapter, we will consider cultural, professional, and clinical barriers to effective communication. A framework will be provided to help the practitioner who must have these difficult conversations. This will include suggestions and scenarios based on our (RF and JH) experiences—both good and bad—as clinicians for over 25 years. We have learned immensely from our mentors, nurses, respiratory therapists, and social workers; from readings of others' words of wisdom; and from those that we have supervised.
Each country's health system and group of providers are sited in a cultural and social milieu. This siting determines, to a greater or lesser extent, some of the myriad ways with which we respond to the communication difficulties we detail below. As citizens of the United States, we realize that the discussion we bring to bear below is at least partially a result of our social and cultural setting, among other factors. Other of our colleagues, in the west and the east, might approach this issue somewhat differently. This is our approach.
Finally, it is a common misconception among physicians that they are the sole purveyors of the conversations surrounding the delivery of bad news. Nothing could be further from the truth. Physicians may initiate the conversations, but the aftermath is frequently laid on the doorstep of other practitioners—most especially our nurse and social worker colleagues. They must often decipher, interpret, elaborate, and provide emotional support for the patient and family, long after the physician has left.
Barriers to Effective Communication
Influences from American culture and our professional training can be impediments to the effective delivery of bad news (Table 4.1). In the new millennium, communication has become increasingly truncated. Inundation with cell phones, e-mails, and text messaging has generated an ABS (abbreviation-based society), and time is—or at least appears to be—of the essence. We call others when we know that they are not at home, so that we can leave a message on their answering machine. We do not have time for the nuances and articulated detail of spoken or written conversation.
Our society has carried the winner or loser mentality from the battlefield to the gridiron to popular television shows. Contestants must be winners or be banished; there is no middle ground. We watch media coverage and re-enactment of medical miracles, which we accept as expected outcomes. We forget that miracle is defined as an “extraordinary event taken as a sign of divine intervention in human affairs” (Webster's New Explorer Dictionary [published 2000]). In our society, bad events and outcomes must be accompanied by the assessment of blame. “Let bygones be bygones” would not be an apt description of our litigious society. This societal Trifecta, when applied to the medical field, suggests that we are losers if our patients do not get better, and we are to blame. Many intensivists will tell you that in America, the last rites are cardiopulmonary resuscitation. Untoward outcomes from these societal influences may include intimidation of the practitioner, thus preventing a frank conversation with a patient or a family. Perhaps worse, the practitioner comes to see the battle as being between him or her and the disease, with the patient suffering as collateral damage.
Aspects of training, particularly of physicians in certain specialties, have encouraged traits that are the antithesis of the compassionate communicator. A majority of practicing physicians have reported having received no formal training in effectively communicating bad news (1). For example, surgeons are taught to be self-reliant, resilient, and tough. Emotions must be checked at the operating room door as surgeons prepare to be the master of the ritual. The sentiment reflected in the admonition given to young residents preparing to begin night duty—“call me if you need me, need me if you call me, and remember, it is a sign of weakness”—is not ambiguous. How do you then get them to flip the switch to something kinder and gentler? Many high-pressure specialties—certainly surgery, critical care medicine, and anesthesiology—attract a personality type that is driven, action-oriented, and without the patience to communicate effectively.
|
Table 4.1 Barriers to effective communication |
||||
|
For those in training and in practice, the efficient use of time is an ongoing challenge. Further, the new work hour limitation for house staff compounds this stress. How does one accomplish all the tasks in the allowable time period? Unfortunately, the delivery of bad news cannot be neatly fit into a schedule, and may be quite time consuming. Finally, if the caregiver is exhausted, it may be hard to muster the energy needed to do this task well. The results from a questionnaire study completed by 167 physicians at the 1999 annual meeting of the American Society of Clinical Oncology noted that a majority of responding physicians felt that they did not have enough time to engage in difficult conversations with patients (2).
Giving patients and families devastating news takes its toll on the sender as well as the recipient. Each practitioner will need to develop two preservation strategies. The first is to have the ability to compartmentalize and be able to move on to a subsequent task. The second is to consider yourself an emotional filter, of which you need to determine the “porosity.” If you are moved to tears and incapacitated every time you deliver bad news, burn-out may be in your near future. On the other hand, if you feel nothing as you give your patient the diagnosis of leukemia, you have lost the reason to be in clinical medicine. Naturally, the “porosity” of our filters will differ with the clinical scenario, and a portion of it will be out of our control.
The Institute for Professionalism and Ethical Practice at Children's Hospital, Boston, developed a workshop named Program to Enhance Relational and Communication Skills (PERCS) to prepare health care professionals for engaging in difficult conversations. The workshop participants commented that to become competent in delivering bad news, one must leave his or her badge at the door, be genuine, invite colleagues from other disciplines into the conversation, and attend to the emotional needs of the patient. It is also important to avoid insensitive and careless terms such as “incompetent cervix” or “harvesting organs” (3).
The Best Way to Give the Worst News
Every practitioner will develop his or her own style of speaking with families and, particularly, a style of how to break bad news. Table 4.2 provides some guidelines for these discussions.
Begin by preparing what you will say. It is very important to consider the context in which the patient/family will be hearing your message. They have or will form an opinion about you that may or may not have merit. You may appear too young, or be of the wrong demographic for them to trust what you say. They may have had a bad experience in your hospital or have emotional dysfunction that impairs their ability to listen to and accept the information you are preparing to present. In these situations, it is good to have another member of the care team with you, both to increase your credibility and to bear witness.
Unlike many communications in our e-mail, text-messaging, sound-bite society, this one must be a conversation. Your goals at the end of this conversation are to have the patient or family understand your message and to feel that you have acted responsibly and professionally. The best ways to accomplish this goal are by paying respect to the situation and by encouraging and watching their responses. Everyone should be sitting, as much as is possible, and pagers and cell phones should be turned off or given to others to hold. Speak directly, make eye contact, and watch the family members'/patient's reaction. Are they listening to you? Are they understanding you? Do you need to slow down, ask if they understand what you say, or repeat some of the information? This advice is simple but crucial to effective communication.
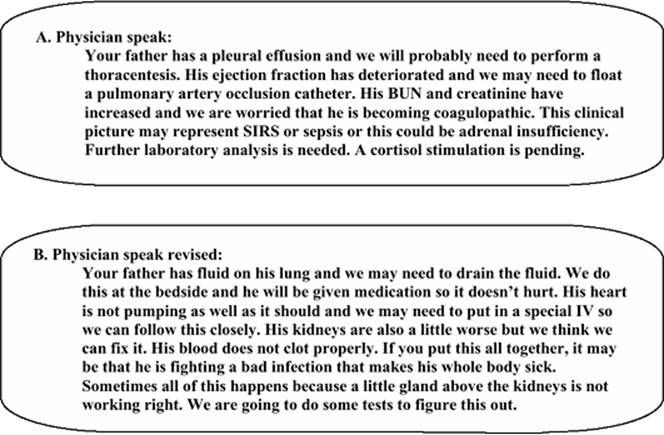
If a patient spoke only Spanish, we would not have a conversation with him in English. In our training, we learned the language of medicine, to which we added common abbreviations and idioms. Whether intentional or not, we speak to our patients in this language, much to their bewilderment. Figure 4.1 provides an example of an intensive care unit (ICU) assessment given to a family in medical language (A) and in English (B).
We should not assume that our patients will question what they do not understand. They may not want to appear ignorant in our “temple.” It is more important to sound intelligible than intelligent. One should avoid “inadvertent disempowering behavior” (Caroline Pace, personal communication, 2006), where the patient or family members, already at a disadvantage because of illness, now must feel inadequate because they do not understand the communication.
|
Table 4.2 Guidelines for effective conversations |
|
|
|
|
|
|
|
Figure 4.1. An intensive care unit assessment given to a family in medical language (A) and in English (B). |
It is not necessary to feel sorry for patients, but it is crucial to have empathy for their situations. Though perhaps irrational, upon the receipt of bad news, there is a sense of isolation from others not afflicted. Patients hope that you can acknowledge, if not relate, to their feelings. There are practitioners—some of you reading these words now—young or fortunate enough not to have experienced loss or tragedy. Empathy is a quality of humanity and is not well faked. It has been said that “empathy is my pain in your heart” (4).
We may become frustrated when a family member or a patient seems slow to grasp what is so obvious to us as health care providers. For example, we may view a patient with a ruptured cerebral aneurysm, approaching brain death, as a straightforward fatality. However, the family members, seeing a relatively healthy-looking patient on the ventilator, may wonder when he will wake up. Remember, they lack your perspective and may have only had a few hours or a few days to process their family tragedy.
The traditional relationship between physician and patient has often been patriarchal. The physician was held on a pedestal (at least outwardly) by the remainder of the care team, so there was a natural comfort in surrendering one's fate to an omnipotent healer. Dr. Rachel Remen, in My Grandfather's Blessing, challenged this paradigm. Dr. Remen, who has struggled with the complications of Crohn disease since her late teens, counsels those with chronic or terminal illness, as well as the physicians and nurses who care for those patients. Her book suggests that the relationship between caregiver and patient is that of equals, with each bringing their strengths and weaknesses to the fore. This defines the important concept of service, which she describes with the comment:
I have served impeccably with parts of myself of which I am ashamed.
Implicit in this admission is the acknowledgment that weaknesses may be strengths in difficult settings. However, she warns that the stress of caring for chronically ill and dying patients will take its toll on the provider, particularly if that stress is not recognized and defused (5).
Baile and Buckman described a simple mnemonic to help practitioners convey bad news (6) (Table 4.3). The SPIKES protocol emphasizes the critical features of this type of communication. A small, laminated copy of this protocol may be a good addition to the stethoscope and penlight in the ICU house officer's armamentarium.
|
Table 4.3 Spikes protocol |
||
|
Clinical Scenarios
There are many specific scenarios in which bad news is given. In the critical care setting, these consist primarily of sudden catastrophic events and end-of-life issues.
Sudden Catastrophic Events
A sudden catastrophic event is usually the unexpected death of a family member, but may also include situations where the patient or family member has sustained an adverse, life-changing event, such as a traumatic injury with quadriplegia, a massive myocardial infarction, or severe stroke. Seasoned health care professionals are easily able to identify clinical scenarios that result in poor outcomes. “Just as medications need to be dispensed with consideration for choice, dosage, and timing, so, too, should clinical information be communicated with regard to the choice of what to communicate, the degree of detail that is preferred by the family, and at a time that is most appropriate to the family's needs” (7). As you enter the room, remember the suggestions listed above. Have another member of the team with you, sit down, turn off cell phones and pagers, and introduce the members of your team.
You have the solemn task of giving information that in some cases will change the listeners' lives forever. Give the news directly, particularly when the patient has died, and get to the point within a few sentences:
Your son was in a head-on collision. He had massive injuries; we tried everything we could to save his life, but I am sorry to tell you that he died.
It is unkind to put the family through the ups and downs of what transpired during an hour-long resuscitation. Use the term dead or died; the message should not have more than one possible interpretation. One should not be cruel but, rather than stating that the patient has “moved on” or “passed away,” one should state that he or she is dead. As that news is heard, the family will react, sometimes verbally, sometimes physically, and sometimes in silence. During this time, your input will not be heard. When the family members return their gaze in your direction, you can give more information or ask if there are further questions. Occasionally, families will turn their anger toward you and imply that the patient would still be alive if he or she had received competent care. Stay calm and reiterate that the injuries were severe—perhaps with some detail—and that everything possible was done for the patient. End by giving your condolences. Provide the family members a means by which they can contact the team if they have questions a day, a week, or a month later, and leave a team member behind to answer any questions that they may not have wanted to ask you. In addition, the family may need to ask another person to verify and thus validate your comments.
End-of-life Issues
On television and in the movies, characters will be critically ill or sustain horrific trauma. They must either die or be well by the end of the show. Unfortunately, this fantasy forms the perception of most of the public, and thus presents a constant challenge for the critical care provider, who must guide patients and families through the process of illness and—in some cases—dying. We believe that the most important priorities are the care and advocacy for the patient and the relationship with the family. The clinical aspects of care are well represented in this textbook and will not be covered here.
|
Table 4.4 The initial intensive care unit family meeting |
|
|
As early as possible in the patient's ICU course, the critical care provider should meet with the family (Table 4.4). If the patients are coherent and competent, they should be included in the conversation, as they are the decision makers. However, in the ICU, patients with end-of-life issues are often not sufficiently awake to participate in this discussion. Determine if the patient has a living will or advanced directive, and the identity of the decision maker. This accomplished, the clinical discussion should begin with a review of the patient's illness, as well as the important topic of the patient's pre-existing state of health. The influence of comorbidities on the outcome of illness needs to be emphasized. If the prognosis is particularly dismal, one should “hang crepe,” that is, set the stage for the likelihood of further bad news. Be leery of giving statistics; make sure that the family and patient understand that statistics are primarily of predictive value and may not deal with their particular situation. Inquire about the family's level of religious and/or spiritual beliefs. This can be a powerful source of comfort in a time of crisis and loss. Many faiths believe that life does not end with death, which can facilitate acceptance. Whether or not the critical care provider's beliefs match those of the patient and family is not relevant in these discussions. It is important for all concerned to remember that there are aspects of the patient's course that we cannot control. Finally, the provider should outline what the goals of treatment will be, and how we measure whether the patient is meeting those goals.
If the information includes unexpected and catastrophic news, such as a patient who went to the operating room for an elective colon resection and is found to have extensive metastatic disease, it should be delivered similarly to news of a sudden death. The recipient will need to process this information and may be unresponsive, or even turn pale for a moment. Judge when to continue the discussion, but remember that you are unlikely to successfully convey important details during this conversation. Speak broadly, offer a later detailed discussion, and give the patient hope to recover from the acute phase of this disease. Patients want the truth to be balanced with hope. Specifically, oncology patients wish for information to be presented honestly, but not too bluntly as to destroy hope. Physicians need to emphasize what can be done, not focus on concerns that cannot be fixed (8).
As the patient's ICU stay continues, members of the care team should give regular progress reports. A feature of the daily rounds should be an assessment of the patient's condition. All viewpoints must be heard, but in the end, the team should decide on a uniform message for the patient and the family. Their situation is stressful and confusing enough without receiving mixed messages, as might occur in a large teaching institution with several services caring for the patient. Further, dysfunctional or suspicious families may use discordant assessments as verification of their belief that “one hand doesn't know what the other hand is doing.” The report given to the family will include how the patient is doing in relation to the goals that were set. The daily or regular meetings give the family and the patient time to adjust to the situation. Critical care providers will often encounter family denial of clinical deterioration. While we tend to view denial disparagingly, it can also be a circuit breaker (or surge protector) from the overwhelming effect of the message. In these instances, give the information incrementally. Emily Dickinson understood this phenomenon:
Tell all the Truth but tell it slant—
Success in circuit lies
Too bright for our Infirm Delight
The Truth's superb surprise
As Lightning to the Children eased
With explanation kind
The Truth must dazzle gradually
Or every man be blind
--Emily Dickinson
In addition to the daily assessment of the condition of the patient, the team should consider if care has become futile. If the patient's clinical course continues to decline or fails to improve—with little hope that it will—it is likely time for a conversation about withdrawal of care. Occasionally, families request to withdraw care from a patient, but generally this topic is broached by the critical care team. If possible, have members of the multidisciplinary team present; again, it provides cohesion of message. Review the patient's course up to this point and how goals have not been met. Although we express that our purpose in the ICU is to prolong life, there comes a point when we are actually prolonging death. That point may not be clear as we approach it, but is recognized after we pass it. The conundrum of ICU care in the new millennium is that there are patients whom we can keep alive but cannot make well.
When asking families to agree to withdrawal of care or comfort care orders, the provider should consider his or her choice of words very carefully. Family members should not be made to feel like the executioner of their loved one. We prefer an approach such as the following:
You know your father much better than we do. Oftentimes, as people get older or have suffered for a long time with a chronic illness, they are not as afraid of death as they are of the prolonged process of dying. As much as you want him to remain alive, he has counted on you to convey his wishes. Our best attempts to battle his illness have failed; we cannot save him, but I promise that we can make him comfortable.
Lautrette et al. emphasized several other aspects of a good end-of-life discussion with the family. Repeat back what families have said; do not present treatment options as equally practical; and learn to tolerate periods of silence. Most importantly, make sure the family understands that good care will be given, even if all possible treatments are not applied (9).
|
Table 4.5 Progression of hope |
||
|
Sometimes various members of the family will have differing opinions on withdrawal of care. Good communication during frequent family meetings was found to result in less psychological stress, anxiety, and depression for families dealing with the loss of a loved one (10). Though decision making usually rests with only one person, achieving a consensus is desirable to prevent subsequent recriminations.
Conclusion
As critical care providers, we are on a first-name basis with death, tragedy, and sorrow. On a daily basis, we must find the balance to serve and stay true to our values. Irrespective of your belief in a higher power—even if you do not have such a belief—consider the insightful words of the Serenity Prayer:
The Serenity Prayer
God grant me the serenity
to accept the things I cannot change;
courage to change the things I can;
and wisdom to know the difference.
--Reinhold Niebuhr
Dunn described the stages of hope (Table 4.5), which illustrate the importance of perspective (11). We must remember that a death with dignity is not a failure. In the end, the words of Dr. Edward Livingstone Trudeau ring true:
To cure sometimes, to relieve often, to comfort always (12).
Case History (Continued)
The patient undergoes resection of the lung metastasis. Six weeks later, she has numerous metastatic lesions in both lungs. She begins weekly treatment consisting of chemotherapy and biologic agents. Unable to operate during that time, the patient and her friend develop a lecture entitled “Giving and Receiving Bad News—Lessons I Learn” to educate her audiences by sharing her experiences as both a clinician and as a patient. A positron emission tomography/CT scan obtained 4 months later shows that her tumor is in remission. She returns to patient care and remains in remission 14 months later.
The patient (RF) and the friend (JH) are the authors of this chapter.
References
1. Rosenbaum M, Ferguson K, Lobas J. Teaching medical students and residents skills for delivering bad news: a review of strategies. Acad Med. 2004;79(2):107–115.
2. Baile W, Lenzi R, Parker RB, et al. Oncologist's attitudes toward and practices in giving bad news: an exploratory study. J Clin Oncol. 2002;20(8):2189–2196.
3. Browning D, Meyer E, Truog R, et al. Difficult conversations in health care: cultivating relational learning to address the hidden curriculum. Acad Med. 2007;82(9):905–912.
4. Komarnicki JW, ed. How to Teach Towards Character Development. Conshohocken, PA: Infinity Publisher; 2004:101.
5. Remen N. My Grandfather's Blessing. New York: The Berkley Publishing Group; 2000.
6. Baile WF, Kudelka AP, Beale EA, et al. Communication skills training in oncology: description and preliminary outcomes of workshops on breaking bad news and managing patient reactions to illness. Cancer. 1999;86:887–897. Baile et al.'s protocol was adapted from Buckman R. How to Break Bad News: A Guide For Health care Professionals. Baltimore: Johns Hopkins University Press; 1992.
7. Truog R, Christ G, Browning D, et al. Sudden traumatic death in children “We did everything, but your child didn't survive.” JAMA. 2006;295(22):2646–2654.
8. Evans W, Tulsky J, Back A, et al. Communication at times of transitions: how to help patients cope with loss and re-define hope. Cancer J. 2006;12(5):417–424.
9. Lautrette A, Ciroldi M, Ksibi H, et al. End of life conferences: rooted in the evidence. Crit Care Med. 2006;43(11 Suppl):s364–s372.
10. Cordts G, Grant M, Sevransky J. Palliative care in the intensive care unit. Contemp Crit Care. 2007;4(12):1–12.
11. Dunn G. What in the world is comfort care? Presented at the American College of Surgeons Meeting, New Orleans, October 9, 2007.
12. Strauss MB. Anonymous: Familiar Medical Quotations. Boston: Little Brown and Company; 1968:410.