Elizabeth Manias
This chapter will discuss collaborative care in terms of four major areas: (a) definition of collaborative care, (b) the makeup of the critical care team and ancillary health professionals, (c) forms of communication, and (d) team effort. The first examines the meanings associated with collaborative care, with particular reference to the critical care context. The various interdisciplinary health professionals who make up the critical care team, including medical personnel, nurses, pharmacists, respiratory therapists, social workers, occupational therapists, physical therapists, and nutritionists, are described in the second area. The third area considers the forms of communication that take place in critical care settings, including critical care rounds, nursing handover between nurses, and admission and discharge practices. The fourth area focuses on functioning as a team and involves orientation of new team members, patient monitoring and observation, and communication with patients' families.
Meanings Associated with Collaboration
For health professionals to collaborate, it is important to understand how collaborative care is interpreted. Collaborative care involves communicating information, opinions, and feelings; sharing decision making, tasks, and goals; negotiating power to enable more equitable participation and mutual respect; and facilitating the uptake of effective treatment (1,2,3). Henneman et al. (4) described collaborative care as a joint venture with two or more health professionals working together to achieve a common goal. It is a cooperative endeavor in which individuals contribute willingly in planning and organizing patient care. Health professionals offer their expertise and share responsibility for final outcomes while other individuals acknowledge their involvement in the venture. These interpretations of collaborative care assume that professional relations between interacting individuals are equal—that is, power relations are equal.
Balance of Power
However, it is also important to acknowledge that sometimes power relations between individuals may be unequal, thereby affecting the quality of collaboration that takes place (5). Unequal power relations can be influenced by perceived knowledge and expertise attributed to various health professionals, miscommunication, different goals of care developed for patients, and different designated roles or titles. Such an acknowledgment challenges health professionals to critically analyze how they carry out their work to enable greater opportunities for collaboration to occur (3).
Benefits and Aim of Care
The ultimate aim of collaborative care is to produce positive outcomes for patients. Some of the positive outcomes associated with improving collaboration include the following: a decline in nosocomial infections (6), improved patients' quality of life (7), lower mortality rates (8), reduced length of hospital or critical care stay (9,10), reduced cost of care (6,9), and reduced adverse events such as oversedation and readmission to critical care (6). Other outcomes have been related to the effects of collaboration on the health professional, the health care team, and the organization (11,12,13,14). Benefits of collaboration for the health professional include feelings of self-worth, competence, and importance. For the health care team, collaboration is seen to create opportunities for clarification of interactive roles and to enhance respect for, and collegiality between, individuals of various disciplines. For the organization, collaboration is understood to promote productivity, retention, and satisfaction of employees (4).
Members of the Critical Care Team: The Need for Interdependent Working Relationships
The critical care setting is a complex organizational system comprising various health professionals who need to function as an interdependent team (Fig. 7.1). These health professionals have particular roles and functions to bring about high-quality patient care and support. The challenge is to understand how these roles and functions fit with those of other professions, with the aim of developing solid working relationships (15,16). For example, physicians are trained to take charge and assume the role of leadership in health care and responsibility for decisions. For them, learning to share in an interprofessional team is a challenge since they may assume or be expected by other team members to take on the leadership role (13,16). Other health professionals, such as nurses and social workers, may place greater emphasis on patients' and families' accounts of the patient's health, rather than relying on objective data as much as is done by physicians. As a result, physicians may not place much weight on accounts of patients and families provided by nurses and social workers, preferring instead to see numeric data to address a situation. Since expectations about roles and functions are largely unspoken, they create obstacles that are not readily identified by team members who experience difficulties with collaboration. The solution involves ensuring that professional expectations are made apparent to all involved. Success in achieving collaborative care depends on committed interdisciplinary work that is incremental, continuous, and sustained (17,18,19,20).
|
|
|
Figure 7.1. Interrelationships of health professionals involved with providing collaborative care in the critical care unit. |
Health Professionals Within the Critical Care Unit
Various medical professionals have an input in patient care within critical care, including the critical care medical director, critical care unit attending physicians, critical care unit fellows, and critical care unit residents. Medical professionals from outside the critical care unit also play an important role and include consultants, surgical attendings (21,22), residents, and other ancillary personnel.
Critical Care Director
The critical care unit is overseen by a director with demonstrated competence in the provision of critical care services. The director manages the administrative aspects of the unit, including the development and implementation of policies and procedures, review of the appropriate use of critical care resources, and education of unit staff. Together with the nurse manager of the critical care unit, the medical director assumes ultimate responsibility for the safety and appropriateness of services provided in the setting. Consequently, the medical director plays an important role in guiding patient care during unstable clinical situations that require careful titration of therapy, such as multiorgan failure and resuscitation procedures. This responsibility includes the need to communicate regularly with other health professionals and the family about current and future patient goals of treatment. Usually, the medical director has final authority over admission and discharge practices of the critical care unit.
Critical Care Attending Physicians
Critical care attending physicians are primarily accountable for the day-to-day unit and patient management responsibilities. These individuals have expert knowledge in pathophysiology, physiology, pharmacology, and the technical aspects of monitors and invasive equipment, as well as competence in managing critically ill patients. Critical care attending physicians provide a leading role in dealing with the sensitivities associated with dying patients and their families. Also important are attributes related to the latest research and quality improvement activities, as well as facilitating education among health professionals in the unit. In the absence of the medical director, it is the critical care attending physicians who make decisions relating to the admissions and discharges of patients.
Critical Care Fellows
Fellows are required to undertake a specified period of the critical care experience, usually a 1-year fellowship in which they work at least 9 months in a critical care environment (e.g., a neurologic or medical intensive care unit), with the remaining 3 months involving either allocation to a clinical area (e.g., respiratory care or trauma service) or conducting research relevant to critical care. Fellows have comprehensive knowledge about the medical histories, surgical and diagnostic procedures, and laboratory data and medications relating to all patients in the critical care unit. In association with the critical care resident, they provide this information on ward round presentations and in discussions with other health professionals, including consultants, surgeons, and nurses. Fellows are required to review the assessment charts of complicated patients with residents and are expected to guide residents in managing patients with respect to issues such as setting mechanical ventilation parameters, providing hemodynamic support and invasive monitoring, prescribing antibiotics, and managing adverse events. Critical care attending physicians assist fellows in making appropriate patient care decisions and providing them with greater input at the beginning of their training compared to later in the training year, at which point fellows are expected to make more independent decisions.
Critical Care Residents
Residents are junior members of the medical staff who rotate through the critical care unit to learn the fundamental principles of treating critically ill patients. They collaborate with critical care fellows in collecting patient assessment data and formulating a management plan. During their rotation in the critical care unit, they develop beginning level competencies in regard to treating patients with complex health care needs. Residents give patient presentations during ward rounds, where they are provided with feedback on their comprehension and understanding of patient assessment, management, and evaluation of care.
Critical Care Nurses
Critical care nurses provide comprehensive skilled care to critically ill patients by maintaining a continual presence at the bedside. Their extensive knowledge and expertise enable them to recognize changes in patients' clinical manifestations and implement strategies aimed at preventing worsening conditions and minimizing complications. They support patients and families by acting as their advocates and play an integral role in the decision-making process with the health care team. In the United States, critical care nurses may be certified through the American Association of Critical Care Nursing by undertaking specialized education and testing and are recognized as critical care registered nurses (CCRNs). In other countries such as Australia and the United Kingdom, critical care nurses may complete specialized postgraduate critical care qualifications at a university.
A nurse manager of the critical care unit provides clear lines of authority for critical care nurses and is accountable for the delivery of good-quality patient care from the nursing staff. This health professional must have the ability to ensure that critical care nursing practices address key standards of care. Aside from expertise in current advances in the field of critical care nursing, the nurse manager also has experience with health information systems, risk management, and health care economics.
Advanced practice roles within the critical care unit include acute care nurse practitioners and clinical nurse specialists. Clinical nurse specialists undertake roles that involve education, consultation, research, and management. Acute care nurse practitioners undertake direct patient care activities and research (23), most often in conjunction with the critical care medicine team. Both clinical nurse specialists and acute care nurse practitioners continue to perform many of the interventions involved with conventional nursing practice. They also function autonomously and in collaboration with other health professionals in an effort to produce optimal patient outcomes. Compared to other critical care nurses, those in advanced practice roles require a greater depth and breadth of knowledge and a greater understanding in interpreting patient data and undertaking complex interventions. Clinical nurse specialists and acute care nurse practitioners are also required to have completed additional postgraduate work, usually at a master's level.
Consultants Outside the Critical Care Unit
Consultants of services outside the critical care unit are specialists who provide important information about a particular facet of patient management to the critical care team. Their role is to answer specific questions, as noted by a critical care health professional in the patient's medical record. To ensure time is used appropriately and constructively, the critical care team should discuss the issue of concern beforehand and provide a rational argument in seeking a consultant's referral. It is usually the attending physician's role to write the consultant referral. Any suggestions provided by consultants should be discussed with the critical care team before treatment is implemented.
Surgical Attendings
Surgical attendings are surgeons who play an important role in the management of surgical procedures required by critically ill patients. They interact with patients and their families in relation to preoperative, intraoperative, and postoperative care, as well as long-term follow-up in terms of ensuring optimal recovery from surgery. Although surgical attendings conduct daily rounds in the critical care unit, specific aspects of patient management usually reside with the critical care team. In the context of the surgical team, surgical residents play much the same role as do critical care residents.
Pharmacists
Pharmacists are integral to patient care in a way that extends beyond their traditional role of supplying and distributing medications. With the increasing sophistication of medications available, their role encompasses the education of physicians, nurses, and other health professionals in prescribing, administering, and monitoring the practices and preparation of medications for critical care patients. They have extensive knowledge about pharmacokinetics and pharmacodynamic principles associated with severe illness, poisoning and drug intoxication, sedation practices, pain relief, and antibiotic use.
Pharmacists also make up various medicinal preparations. For critical care units, these preparations commonly include total parenteral nutrition and the incorporation of cytotoxics, antibiotics, potassium, or opioids into intravenous fluids. These preparations are made up in laminar flow cabinets of hospital pharmacy departments under sterile conditions.
One of the most important tasks of pharmacists is to ensure medications are administered in a manner that promotes therapeutic efficacy and minimizes adverse outcomes. More specifically, they help physicians and nurses by coordinating the development, implementation, and evaluation of medication protocols or guidelines. For this reason, pharmacists attend ward rounds and team meetings to familiarize themselves with patients' medical conditions and how these affect medication therapy. The Society of Critical Care Medicine has released a position paper about the scope and practice of critical care pharmacy practice and service (24).
Respiratory Therapists
Respiratory therapists work with physicians and nurses and are involved with maintaining ventilation equipment and monitoring the airway management of critically ill patients. Airway management may include the provision of oxygen therapy, mechanical ventilation, and aerosol medication therapy. They also play a role in titrating ventilation parameters to suit the breathing and hemodynamic patterns of patients, formulating weaning procedures, and providing patient and family education. Although respiratory therapists are well established in North America, they rarely exist in the United Kingdom, Europe, Australia, or Asia, countries or continents in which nurses are responsible for the patients' respiratory equipment and clinical management of respiratory function in collaboration with physician consultation.
Social Workers
Social workers work with the health care team to provide a conduit between management plans for the critical care patient and family members. They possess specialized knowledge about health policies and services, social welfare systems, and community resources. With this information to guide their practice, social workers act as important advocates for critically ill patients and families. Examples of activities conducted by social workers include assisting in the adjudication of family–patient–health care team disagreements, leading team discussions in root cause analyses of ICU-related problems, locating temporary accommodation for family members during patients' stay in hospital, and providing resources to help cover health care costs.
Occupational Therapists
Occupational therapists are educated to conduct a complete evaluation of the impact of illness on the activities of critically ill patients at home, in work situations, and during recreational situations. They work synergistically with other disciplines of the health care team to reduce the physical and psychological disability of patients. Before patients are discharged, occupational therapists often visit the home environment to make comprehensive assessments of the current facilities and changes required to accommodate the patient's needs.
Physical Therapists
Physical therapists assess and treat critically ill patients with a temporary or permanent physical disability, with the aim of achieving the highest degree of recovery. Treatment modalities used by physical therapists include exercise, mobilization and manipulation, massage, splinting, the application of hot and cold compresses, suctioning of respiratory secretions, and electrical stimulation. Conditions treated include birth deformities, fractures, back strain, spinal injuries, strokes, and multiple sclerosis. Rehabilitation after surgery, such as open heart, orthopedic, and abdominal surgery, is another area of responsibility.
Nutritionists
Qualified nutritionists are a vital part of the health care team who consult with physicians, nurses, pharmacists, and family members in the critical care unit. The aim of nutritionists is to improve the nutritional health and promote the recovery of the critical care patient. Nutritionists possess detailed knowledge of the food principles that apply to health and disease states; the biochemical properties of food; the mechanisms underlying food absorption, metabolism, digestion, and elimination; and the indications for nutritional support. They also have an in-depth understanding of the interactions of particular food products with medications commonly used in critical care.
Nutritionists play an important role in the decision to introduce parenteral or enteral feeding or other forms of nutrient supplementation for critically ill patients. Critically ill patients are susceptible to malnutrition as they undergo invasive procedures and diagnostic tests, and disease states may alter the digestive process of nutrients. In collaboration with physicians and nurses, nutritionists determine the precise requirements for energy, protein, vitamins, minerals, essential fatty acids, electrolytes, and water to be administered through parenteral or enteral feeding. Enteral feeds are usually made in a hospital diet kitchen, the process of which is supervised by nutritionists. Conversely, critical care pharmacists prepare parenteral nutrition solutions using sterile laminar flow environments.
Forms of Communication
Health professionals interact with each other using different forms of communication, depending on the intended purpose. These forms of communication include critical care ward rounds, nursing handovers, and communication concerning admission to and discharge of patients from critical care units. The effective collaboration within these forms of communication is essential to the overall function of critical care units, which significantly affects the patient's risk-adjusted mortality and length of stay (25,26,27).
Critical Care Ward Rounds
Critical care ward rounds are recognized as an important forum for various health professionals to come together and discuss the daily goals of care. The goals of care serve various functions, which include recognizing patient problems, sharing information, initiating treatment, evaluating the effectiveness of changes in treatment, and increasing learning opportunities for the critical care staff (28). Ineffective patient care and decision making can occur if the goals of care are not communicated clearly, leading to increased costs and the possibility of medical errors (27).
Critical care rounds should be multidisciplinary and include various personnel in addition to the critical care physicians: the nurse unit manager, the specific nurse assigned to each patient, the pharmacist, the respiratory therapist, and others such as the social worker and dietitian. Although some part of the ward round may be undertaken away from the bedside to prevent interruptions adversely affecting decision making, the health care team must also be present at the bedside, since direct patient assessment is integral to identifying problems. Such problems may include inappropriate ventilation settings, patient agitation and confusion, an incorrectly positioned endotracheal tube, and pain as shown by abdominal guarding and inappropriate breathing.
Usually, it is the role of the critical care fellow to present each patient with feedback provided by the critical care attending physician. In this manner, the ward round provides a formalized process of education and training for less experienced medical personnel. It is also an opportunity for other health professionals to provide their feedback on various perspectives of the patients' care, including wound management, nutrition, and medication management. The critical care physician is then able to direct discussions and debates for the planning of patient care (5).
The ward round should be a structured process occurring at a formally designated time each day. Scheduled ward rounds allow physicians, nurses, and other health professionals to plan their attendance despite unexpected situations that can occur. Organizing the ward round as a haphazard process, where it is conducted at different times of day, may mean that certain health professionals will not be able to attend (29). A lack of representation at ward rounds by particular disciplines may adversely affect the range of opinions and possible therapies for patients. A well-organized ward round is more likely to become a creative space in which health professionals of different disciplines can contribute to developing strategic plans for patient care and to sharing openly their clinical activities with other individuals.
The patient presentation should be concise and clear without redundant and irrelevant information, such as unrelated details about the patients' past medical history or superfluous explanations of daily activities. There are several steps that should be followed to ensure the patient presentation functions smoothly (Table 7.1).
|
Table 7.1 Steps to Take for an Effective Ward Round |
|
|
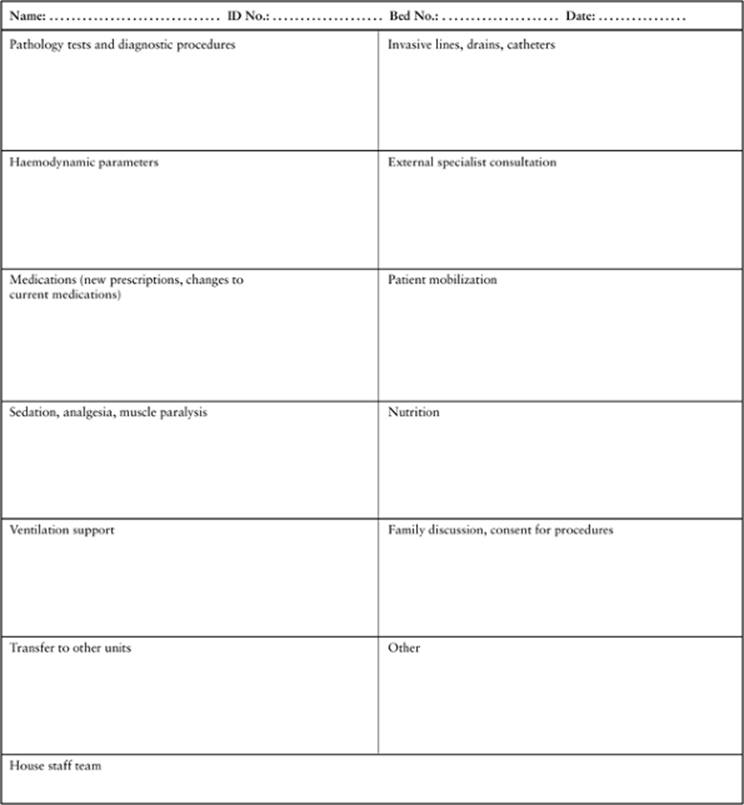
To improve the quality of care, a daily goals sheet can be used during ward rounds, with input from nurses, physicians, and other health professionals. A daily goals sheet is a document that is completed during ward rounds and posted at the bedside of each patient. It summarizes the plan of prioritized activities for a patient during the course of a day. Information recorded on the goals sheet depends on specific characteristics of the unit (Table 7.2). Because each sheet is a work in progress, it is usually discarded the day after use and not included in the patient's medical record. Information contained in the goals sheet can serve as a guide to assist physicians, nurses, and other health professionals in documenting their progress. Past research has shown a significant reduction in the length of intensive care stay of patients from 6.4 days to 4.3 days after introduction of a daily goals sheet. The understanding of the goals of care by nurses and physicians, as well as communication between them, had also improved (27).
Nursing Handover Between Nurses
The nursing handover is a verbal form of communication involving nurses from one working shift communicating with those of the oncoming working shift. The purpose of the handover is to ensure continuity of patient care between nurses. Beyond its use as a mode of transferring information about patients, the handover is a complex form of communication that encompasses social and environmental contexts (30,31).
|
|
|
Table 7.2 Sample Daily Goals Sheet |
Manias and Street (30) conducted an observational study of handover practices in a critical care unit through the use of participant observation, individual interviews, focus groups, and professional journaling. In their study, the charge nurse of the previous shift gave a “global” handover of all patients to oncoming nurses of the next shift. Oncoming nurses then proceeded to a bedside handover, where bedside nurses from the previous shift focused on a patient's individual needs. The global handover functioned mainly as a form of communication between charge nurses of the oncoming and previous shifts. During this time, the charge nurses often directed comments to each other and did not involve other oncoming nurses in their discussions. At the bedside handover, nurses from the previous shift regarded requests from oncoming nurses for patient information as a form of criticism of their own clinical practices, and they sometimes expressed fear and anxiety about the process. Nurses from the previous shift were concerned with demonstrating that they were in control of their environment, as evidenced by a tidy bedside area, a patient whose vital signs were stable, and the completion of all set tasks. They needed to fit into the expected norm of a busy, efficient, and effective nurse—essentially, a nurse who was in control of the bedside area. This need to maintain control impeded effective communication during the nursing handover.
|
Table 7.3 Steps to Ensure an Effective Nursing Handover |
|
|
Charge nurses of working shifts need to acknowledge the interests of all oncoming nurses when presenting patient information in the global handover. The global handover needs to be perceived as an opportunity for all nurses to openly discuss the care plans of various patients, rather than merely as a forum in which only charge nurses communicate with each other. Nurses should not expect themselves to fit into an expected norm of a busy and tidy nurse who is always in control of the bedside area. Instead, an appreciation of the inherent messiness of a critical care setting will help facilitate supportive and collaborative communication during the nursing handover. The nursing handover is then more likely to be a time in which nurses can develop strategic plans for patient care and can share their clinical activities openly. Several steps (Table 7.3) should be followed to ensure that the nursing handover process functions smoothly and effectively (32).
Admission and Discharge Practices of Critical Care Units
Consensus guidelines have been developed to provide general information about criteria and procedures for admission and discharge practices (33,34). These guidelines detail objective clinical parameters to assist health professionals in their decision making about patient flow to and from the unit. Aside from consensus guidelines, organizational factors, which are closely linked to collaborative care, have drawn attention and been examined for associations between admission and discharge practices of critical care settings and patient mortality.
Open and Closed Systems
An organizational factor that has been examined in terms of admission and discharge practices is the open or closed system of care (22). In the open system, various health professionals are present in the unit, but physicians directing patient care have obligations at a site separate from the critical care setting, such as the operating room or inpatient or outpatient areas. A physician with expertise in critical care may or may not be involved to assist with management of care in an open system arrangement. In a closed system, care is provided by a critical care–based team of physicians, nurses, pharmacists, respiratory therapists, and other health professionals.
In a prospective cohort study, the effect of changing from an open to a closed critical care unit was examined in terms of clinical outcomes (35). A consecutive sample of 124 patients admitted under an open system was compared to that of 121 patients admitted after changing to a closed system. In the closed system, the ratio of actual mortality (31.4%) to predicted mortality (40.1%) was 0.78. In the open system, the ratio of actual mortality (22.6%) to predicted mortality (25.2%) was 0.90. Notably, 52% of house staff in the closed system rated their level of experience in managing critically ill patients as “very experienced” compared with 15% in the open system. Nurses commented that they were very confident about the clinical decisions made by physicians in the closed system compared to the open system (41% vs. 7%, p <0.01). The authors suggested the results may be an indication of the improved communication between physicians and nurses in the closed system.
Time of Day
Another organizational factor identified as being important in relation to admission and discharge practices is time of day, with specific attention to weekdays versus weekends and daytime versus nighttime. A cohort study of all 23,134 emergency admissions over a 3 1/2-year period showed that weekend critical care admissions were associated with an increased adjusted mortality compared with weekday admissions (odds ratio [OR] 1.20, 95% confidence interval [CI] 1.01–1.43) (36). The adjusted mortality was similar for admissions made after business hours compared with those made during business hours (OR 0.98, CI 0.85–1.13). On the other hand, the adjusted risk of death was higher after business hours as compared with during business hours (OR 6.89, CI 5.96–7.96). The time of discharge from the critical care unit was not associated with additional hospital mortality. These findings provide evidence of the importance played by the organization of critical care services. It is also possible that there are more opportunities for collaborative care in planning and managing patient flow during times when there are greater numbers of health professionals and greater availability of more experienced staff (35).
Functioning as a Team
The integral functioning of a critical care team goes beyond the interactions of health professionals during the specified forums of communication elucidated previously. It also involves developing an understanding of unpredictable events that can lead to clinical crises. Providing support for new team members, monitoring and observing patients for changes in clinical outcomes, and facilitating the involvement of family members are crucial facets for the foundation of a successful collaborative unit.
New Team Members
Specialized health care requires a tailored form of orientation for health professionals entering the critical care setting. Experienced clinicians in critical care are faced with the challenge of how to deliver important information to new team members to facilitate effective learning. This challenge is compounded by the difficulty associated with a shortage of appropriately trained nurses and physicians. Comprehensive preparation through orientation programs has been shown to be a vital component for retaining health professionals (37). In a recent survey of the American Association of Critical Care Nurses, the nurse managers of 300 critical care units (52.1% response rate) provided information about staffing, professional advancement, staff satisfaction, orientation, and quality indicators (38). Eighty percent of responding nurse managers had a standardized orientation program. The responding nurse managers also indicated that graduate nurses were actively employed and trained to work in the critical care setting.
Orientation of newly employed health professionals to critical care departments should be viewed as a shared responsibility among senior health professionals, educators, and new staff members. The sharing of responsibilities improves the effectiveness of the orientation process because it allows more efficient completion of activities associated with the orientation, promotes collegial relationships, and links knowledge with practice. Orientation should occur through a structured program with defined goals that are agreed on by all individuals concerned.
The new staff member needs to be matched with a primary mentor and a secondary mentor, based on their discipline backgrounds, past experiences, attitudes, and learning styles. This matching process should be a strategic rather than a random choice to stimulate critical thinking, encourage open communication, and stimulate further professional development. The designation of a mentor based on random choice often leads to the use of multiple mentors, leading to inconsistent and confusing messages being conveyed (39).
Learning opportunities should be structured using a combined learner-led, theoretical, and clinical program (37). Such a model facilitates the transfer of knowledge to the practice setting. Theoretical reference material provided to the new staff member should include information about unit policies and protocols, roles and responsibilities of various members of the health care team, and the pathophysiology, assessment, and treatment relating to common patient conditions observed in the unit.
Although new staff members are very likely to have a rich array of experiences, experienced mentors are also influenced by the critical care culture in which they are positioned. As a result, new staff members and experienced mentors could be accustomed to performing activities their own way, which may lead to conflict. New staff members may feel that their learning needs and past experiences are not adequately recognized while mentors may feel that their advice is being ignored. By identifying potential problems from the outset, the orientation process can be more individually adapted to the team member's specific needs, the focus of which is becoming part of the unit. Developing a sense of belonging can help to solidify collaboration between the new staff member and other health professionals.
Monitoring and Observation of Critically Ill Patients
Most patients in critical care require constant monitoring and observation, such as patients with multisystem organ failure, multiple trauma, and adult respiratory distress syndrome. The nurse:patient ratio in many parts of the world is generally 1:2 (21). However, in Australia, the nurse:patient ratio for carrying out nursing activities in critical care units is 1:1. As nurses maintain a constant presence at the bedside, they play a critical role in undertaking regular monitoring of patients, assist in the early diagnosis of impending problems, and recommend appropriate interventions to be administered.
Patients in critical care require clinical parameters to be measured hourly or more frequently if these parameters change quickly. Also important is the close observation of patients through physical methods of inspection, palpation, percussion, and auscultation. Comprehensive judgment should be used in interpreting the significance of information obtained to avoid the complacency that could occur with repetitious documentation of clinical parameters and observations.
Nurses' knowledge in conducting patient monitoring and observation is largely constructed by their ongoing experiences and education in the critical care context. On the other hand, medical residents and critical care fellows who work in critical care for a limited period have to rely on past experiences and knowledge as their major sources of information, which may not necessarily be compatible with the types of decisions required in critical care. As an illustration, in an ethnographic study on professional relationships (5), a critical care fellow with previous experience in anesthetics was confronted by a situation involving a patient who had gone to the operating room for a duodenal ulcer repair and returned to the critical care setting. Within an hour of the patient's return, the bedside nurse, who was a clinical nurse specialist, reported to the fellow that the patient was restless, cold, and not breathing well with the ventilator. Based on his past anesthetic experience, the fellow advised the nurse to extubate the patient. The nurse drew on her knowledge of similar patients in critical care and believed that the patient needed additional sedative and analgesic treatment rather than removal of the endotracheal tube. She presented the situation to the critical care attending who agreed with her view and requested that the patient receive further analgesic and sedative medications (5).
Critical care attending physicians are ultimately responsible for less experienced medical personnel; however, these more experienced physicians may be present in the unit only during discrete times of the day. Due to their lack of availability, the critical care attending physician may be able to address only a small portion of the educational needs of junior medical team members in explaining the significance of a patient's clinical parameters and observations. Instead, due to their constant presence in the environment, nurses provide a substantive component of the educational needs of critical care fellows and residents in interpreting data obtained from patient monitoring and observation.
Nurses and physicians collectively provide valuable knowledge in making decisions about information obtained from patient data. It is therefore important that any rigid role boundaries between them are broken down. Maintaining rigid role boundaries creates distrust and disrespect between nurses and physicians, thereby hindering future progression of informed decision making. In effect, nurses need to be accepted as the “eyes and ears” of all levels of the critical care medical team to extend their perceptual capabilities.
Communication with Family Members
The admission of a critically ill patient is a stressful time for families, especially in the current health care environment of advanced technology, greater sophistication of interventional treatment, and multiple health professionals providing care. This critical care event can adversely affect the functioning of family members and their ability to communicate and understand complex information (40). If miscommunication is allowed to occur, the likely outcomes are care fragmentation, family alienation, and the development of distrustful relationships between family members and health professionals, and among health professionals themselves. Such disagreements can result in poor-quality patient care. Collaboration among health professionals is required for the comprehensive support and involvement of family members. As nurses are continuously present at the bedside, they need to interact regularly with other health professionals involved in direct patient care to synthesize information in a way that can be easily communicated to family members (41).
In a descriptive study involving interviews with family members, and observations of interactions between family members and intensive care staff, Söderström et al. (40) found that initial impressions had a sustained effect on family members and influenced future interactions. Family members who understood explicit information and implicit messages were open in their interactions with staff, adjusted well to the critical care environment and were more accepting of the situation (40). In other words, a mutual understanding existed between these family members and critical care staff. Explicit information involved details about the rules and policies of the unit, the condition of the patient, and how to behave in front of the patient. There were also implicit messages inherent in the information. For example, the message “you can visit the patient freely” meant “as long as you do not disturb us in our work.” In addition, the message “you can ask questions freely” was conveyed “as long as we find them relevant” (40). Unfortunately, some family members did not fully understand either the explicit information or the implicit messages, and consequently either became withdrawn and quiet or more vocal in their communication by asking many questions. For these individuals, there was a mutual misunderstanding with staff. These family members did not adjust well to the environment and were either ignored or insulted by critical care staff.
It is important that nurses and physicians reflect on how they communicate with family members at initial meetings and in future interactions. Mutual understanding is more likely to occur if information is presented in a clear and unambiguous way. Family members need to have questions answered honestly, and they require regular communication about the patient's progress and prognosis, treatment received, and changes in patient condition (42). They need to be reassured that health professionals care about the patient and support family members in their coping strategies. Family members should be able to speak with the physician and bedside nurse daily, have flexible visiting hours, be able to assist with simple patient care if desired, and have a place where they can be alone.
Summary
Underlying a health care system that is facing pressure to improve efficiency are critical care services, which are predicted to become more important as the population ages, as the boundaries within hospital areas and between health professionals become blurred, and as more specialized technology develops over time. Health professionals need to examine how to adapt their approach to collaborative care in a complex and ever-changing health care climate. By themselves, sophisticated technology and treatment are not sufficient to address the needs of patients and families—positive and conducive relationships are the critical drivers for improved care.
Pearls
· Health professionals need to acknowledge that sometimes power relations between individuals may be unequal, thereby affecting the quality of collaboration that takes place.
· Collaborative care can bring about positive outcomes for patients, their families, health professionals, the health care team, and the health care organization.
· The critical care setting is a complex organizational system comprising various health professionals who need to function as an interdependent team. The challenge is to understand how their roles and functions fit with those of other professions, with the aim of developing solid working relationships.
· The ward round needs to function as a structured process, occurring at a formally designated time every day.
· A daily goals sheet should be used during ward rounds, with input from nurses, physicians, and other health professionals to summarize the plan of prioritized activities for a patient during the course of a day.
· The nursing handover should be considered a time in which nurses can develop strategic plans for patient care and share openly their clinical activities with each other.
· Organizational factors such as the presence of an open or closed unit and time of day can impact on collaborative care. These factors can influence patient outcomes in relation to critical care admission and discharge.
· Comprehensive preparation through orientation programs has been shown to be a vital component for retaining newly employed health professionals in the critical care unit and bringing about collaborative care.
· Due to their constant presence, nurses provide a substantive component of the educational needs of critical care fellows and residents in interpreting data obtained from patient monitoring and observation.
· Collaboration among health professionals is required for the comprehensive support and involvement of family members of patients.
References
1. Leonard M, Graham S, Bonacum D. The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care. 2004;13(Suppl 1):i85.
2. Thomas EJ, Sexton JB, Helmreich RL. Translating teamwork behaviours from aviation to healthcare: development of behavioural markers for neonatal resuscitation. Qual Saf Health Care. 2004;13(Suppl 1):i57.
3. Zwarenstein M, Bryant W. Interventions to promote collaboration between nurses and doctors. Cochrane Database of Syst Rev. 2000;(2):CD000072. Review.
4. Henneman EA, Lee JL, Cohen JI. Collaboration: a concept analysis. J Adv Nurs. 1995;21:103.
5. Manias E, Street A. The interplay of knowledge and decision making between nurses and doctors in critical care. Int J Nurs Stud. 2001;38:129.
6. Jain M, Miller M, Belt D, et al. Decline in ICU adverse events, nosocomial infections and cost through a quality improvement initiative focusing on teamwork and culture change. Qual Saf Health Care. 2006;15:235.
7. Eubanks P. Quality improvement key to changing nurse–MD relations. Hospitals. 1991;65:26.
8. Wheelan SA, Burchill CN, Tilin F. The link between teamwork and patients' outcomes in intensive care units. Am J Crit Care. 2003;12:527.
9. Curley C, McEachern JE, Speroff T. A firm trial of interdisciplinary rounds on the inpatient medical wards. Med Care. 1998;36(8 Suppl):AS4.
10. Schneiderman LJ, Gilmer T, Teetzel HD, et al. Effect of ethics consultations on nonbeneficial life-sustaining treatments in the intensive care setting: a randomized controlled trial. JAMA. 2003;290:1166.
11. Boyle DK, Miller PA, Forbes-Thompson SA. Communication and end-of-life care in the intensive care unit. Crit Care Nurs Q. 2005;28:302.
12. Miller PA. Nurse-physician collaboration in an intensive care unit. Am J Crit Care. 2001;10:341.
13. Shirey MR. Authentic leaders creating healthy work environments for nursing practice. Am J Crit Care. 2006;15:256.
14. Vazirani S, Hays RD, Shapiro MF, et al. Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14:71.
15. Gerardi D. Using mediation techniques to manage conflict and create healthy work environments. AACN Clin Issues. 2004;15:182.
16. Hall P. Interprofessional teamwork: professional cultures as barriers. J Interprofessional Care. 2005;19(Suppl 1):188.
17. Curtis JR, Cook DJ, Wall RJ, et al. Intensive care unit quality improvement: a ‘how to’ guide for the interdisciplinary team. Crit Care Med. 2006;34:211.
18. Day L. Advocacy, agency, and collaboration. Am J Crit Care. 2006;15:428.
19. LeTourneau B. Physicians and nurses: friends or foes? J Healthcare Manage. 2004;49:12.
20. Thomas EJ, Sexton JB, Helmreich RL. Discrepant attitudes about teamwork among critical care nurses and physicians. Crit Care Med. 2003;31:956.
21. Brilli RJ, Spevetz A, Branson RD, et al. Critical care delivery in the intensive care unit: defining clinical roles and the best practice model. Crit Care Med. 2001;29:2007.
22. Haupt MT, Bekes CE, Brilli RJ, et al. Guidelines on critical care services and personnel: recommendations based on a system of categorization of three levels of care. Crit Care Med. 2003;31:2677.
23. Howie JN, Erickson M. Acute care nurse practitioners: creating and implementing a model of care for an inpatient general medical service. Am J Crit Care. 2002;11:448.
24. Rudis M, Brandi K. Position paper on critical care pharmacy services. Crit Care Med. 2000;28:3746.
25. Baggs JG, Schmitt MH, Mushlin AI, et al. Association between nurse-physician collaboration and patient outcomes in three intensive care units. Crit Care Med. 1999;27:1991.
26. Knaus WA, Wagner DP, Zimmerman JE, et al. Variations in mortality and length of stay in intensive care units. Ann Int Med. 1993;118:753.
27. Narasimthan M, Eisen LA, Mahoney CD, et al. Improving nurse-physician communication and satisfaction in the intensive care unit with a daily goals worksheet. Am J Crit Care. 2006;15:217.
28. Manias E, Street A. Nurse-doctor interactions during critical care ward rounds. J Clin Nurs 2001;10:442.
29. Manias E, Aitken R, Dunning T. Graduate nurses' communication with health professionals when managing patients' medications. J Clin Nurs. 2005;14:354.
30. Manias E, Street A. The nursing handover: uncovering the hidden practices of nurses. Int Crit Care Nurs. 2000;16:373.
31. Philpin S. ‘Handing over’: transmission of information between nurses in an intensive therapy unit. Nurs Crit Care. 2006;11:86.
32. Levett-Jones T, Bourgeois S. The Clinical Placement. Marrickville, Australia: Elsevier, 2007.
33. Smith G, Nielsen M. ABC of intensive care: criteria for admission. BMJ. 1999;318:1544.
34. Society of Critical Care Medicine. Guidelines for ICU admission, discharge and triage. Crit Care Med. 1999;27:633.
35. Carson S, Stocking C, Podsadecki T, et al. Effects of organizational change in the medical intensive care unit of a teaching hospital: a comparison of ‘open’ and ‘closed’ formats. JAMA. 1996;276:322.
36. Uusaro A, Kari A, Ruokonen E. The effects of ICU admission and discharge times on mortality in Finland. Int Care Med. 2003;29:2144.
37. Thomason TR. ICU nursing orientation and postorientation practices: a national survey. Crit Care Nurs Q. 2006;29:237.
38. Kirchhoff KT, Dahl N. American Association of Critical-Care Nurses' national survey of facilities and units providing critical care. Am J Crit Care. 2006;15:13.
39. Hardy R, Smith R. Enhancing staff development with a structural preceptor program. J Nurs Care Qual. 2001;15:9.
40. Söderström I-M, Saveman B-I, Benzein E. Interactions between family members and staff in intensive care units—an observation and interview study. Int J Nurs Stud. 2006;43:707.
41. Tracy MF, Ceronsky C. Creating a collaborative environment to care for complex patients and families. AACN Clin Issues. 2001;12:383.
42. Norton SA, Tilden VP, Tolle SW, et al. Life support withdrawal: communication and conflict. Am J Crit Care. 2003;12:548.