Linda L. Wong
Kimi R. Ueda
V. Ram Peddi
Because of advances in critical care and medical treatment, many more patients are living with end-stage renal disease (ESRD). In 2003, more than 324,000 patients in the United States received some form of renal replacement therapy for ESRD. The economic burden of ESRD is staggering, with $27.3 billion spent in the United States in public and private funds in 2003 (1). Renal transplantation is clearly the most cost-effective treatment option for ESRD when compared to all other forms of renal replacement therapy (2,3). The improvement in outcome after renal transplantation has resulted in a more liberal selection of patients. Unfortunately, the demand for kidney transplants far exceeds the supply of available organs. While nearly 70,000 patients currently await renal transplantation in the United States, only 16,477 renal transplant procedures were performed in 2005 (4). As a result, patients on the deceased donor organ transplant waiting list wait prolonged periods and suffer the consequences of chronic disease and associated comorbidities before finally undergoing transplantation. This serious shortage of donor kidneys has prompted many institutions to expand their donor criteria. In an attempt to increase the utilization of suboptimal kidneys, transplantation of both marginal kidneys, a “dual transplant,” into a single recipient has been performed at some centers with good short-term results (5). Furthermore, there has been a renewed interest in the use of “non–heart-beating donors,” also with good short-term results (6,7). Because of these reasons, which may lead to an increase in the incidence of delayed graft function or slow graft function, the critical care management of these patients has become increasingly important. Furthermore, advances in transplant management now allow for long-term survival after transplant. There are now over 100,000 patients living on chronic immunosuppression after renal transplant in the United States, some of whom may present to the critical care unit for unique problems and complications long after they have undergone transplant surgery (8).
Evaluation of Potential Transplant Candidate
Before undergoing renal transplantation, each patient must undergo thorough evaluation, as not all ESRD patients are appropriate candidates for transplantation. Each center has a specific protocol for candidate evaluation, but the main purpose of any evaluation is to identify major contraindications to transplantation including active malignancy, advanced cardiopulmonary disease, active infection, substance abuse, and noncompliance with medical therapy. With most malignancies, a waiting period before transplantation is recommended (time period varies with the type of malignancy) and patients should be thoroughly evaluated for any recurrence or metastasis, which would contraindicate transplantation. There is no completely reliable algorithm for evaluating patients for cardiac disease for renal transplant surgery. General recommendations include noninvasive cardiac stress testing for the following population: diabetics, males older than 45 years, females older than 55 years, family history of premature cardiac disease (myocardial infarction [MI] or sudden death in first-degree male relative younger than 55 or first-degree female relative younger than 65), current cigarette smoking, hypertension, total cholesterol >200 mg/dL, and high-density-lipoprotein cholesterol <35 mg/dL. For those with positive stress testing, coronary angiography would be indicated. Some centers routinely advocate coronary angiography for all diabetics as the incidence of ischemic heart disease is high in this population (9).
Patients undergoing evaluation should be screened for viral hepatitis B and C and HIV, and any active infection should be treated. While viral hepatitis B and C and HIV positivity are not absolute contraindications, patients with advanced forms of these infections are generally not candidates for transplantation.
Other potential relative contraindications to transplantation include obesity, severe peripheral vascular/cerebrovascular disease, and advanced age. Although obesity is not an absolute contraindication, U.S. data on over 27,000 patients have indicated that those with morbid obesity (body mass index [BMI] >35) have a higher rate of delayed graft function, acute rejection, and overall survival, as well as longer hospitalizations (10). Thrombophilia, prostatic disease, high immunologic sensitization, psychosocial problems, and renal diseases with a high recurrence rate such as focal and segmental glomerulosclerosis should be identified during this transplant evaluation. Potential anatomic abnormalities such as severe iliac arterial disease and genitourinary anomalies should also be delineated before transplantation.
Candidates on the deceased donor waiting list should be reassessed periodically for any changes in the status of their medical and psychosocial problems. Potential recipients with diabetes mellitus should be evaluated annually as they often have associated ischemic heart disease. As patients wait longer for deceased organ donors, they will need to be monitored carefully as significant changes in their medical status may occur during the waiting period.
Types of Donors
Kidneys are transplanted from deceased donors after brain death or cardiac death, and from living donors. Brain death is defined by the Uniform Determination of Death Act of 1981 as follows: “an individual is dead if there is irreversible cessation of circulatory and respiratory functions or if there is irreversible cessation of all brain functions of the entire brain, including the brainstem.” A brain-dead donor has suffered head trauma, cerebrovascular accident, cerebral anoxia, or a nonmetastasizing brain tumor. Physicians caring for the patient can diagnose brain death with the assistance of physical exam findings, an apnea test, a nuclear brain flow scan, and an electroencephalogram, though none of these tests is specifically required. It is the responsibility of all health professionals and especially critical care medicine physicians to report all patients with brain death and impending brain death to the local organ procurement organization (OPO). Once family members have accepted that their relative is brain dead, the trained donation coordinator may approach the family to discuss organ donation.
Because of the disparity between organ demand and supply, kidneys that traditionally would not have been used are now being considered. These deceased donors have been defined by the United Network for Organ Sharing (UNOS), the national organization that coordinates organ allocation, as “expanded donors.” Expanded criteria donors (ECDs) include all kidneys procured from donors of age older than 60 or age between 50 and 59 years and at least two of the following: hypertension, serum creatinine >1.5 mg/dL, or death due to a cerebrovascular accident. Some studies have shown that recipients of kidneys with expanded donor criteria have slightly diminished graft function, but comparable long-term graft and patient survival (11). Use of ECD kidneys may offer survival advantages to those on dialysis and should be offered principally to recipients older than 60 years or perhaps allocated to OPOs with longer waiting times (12). This is a controversial area and some centers advocate ECD kidneys to all diabetics older than age 40 if waiting time is long.
In donation after cardiac death (DCD), death is determined by the usual cardiopulmonary criteria to prove the absence of circulation and can be used in clinical scenarios in which the donor does not meet brain death criteria. Conditions that may warrant consideration of DCD include irreversible brain injury, end-stage musculoskeletal disease, and high spinal cord injury. Early reports suggest that the time between extubation of the donor and the initiation of cold perfusion of the organs (warm ischemia) should be less than 60 minutes for successful kidney removal and function, though this does vary somewhat between centers (13).
Living donors are people who have been evaluated extensively both medically and psychosocially for possible donor nephrectomy. Medical evaluation should include thorough history and physical examination, laboratory studies (chemistry panel, complete blood count, hepatitis B and C and HIV testing, ABO typing, tissue typing, cross-match testing), 24-hour urine for creatinine clearance and protein, chest radiograph, computed tomography (CT), or magnetic resonance imaging (MRI) to evaluate both kidneys. Psychosocial evaluation is done to determine the emotional relation of the donor to the potential recipient and to ensure that the donor truly desires to donate and for altruistic reasons (not financial or other gain). An individual should be considered as a potential living donor only if the following basic requirements have been fulfilled:
1. Donor and recipient are ABO blood group compatible.
2. The warm T-lymphocyte cross-match is negative.
3. The person is in excellent physical condition, emotionally stable, and well motivated.
4. The individual is willing to undergo donor nephrectomy, is fully informed about the procedure, and is not under pressure from family members to donate a kidney.
The cytotoxic T-cell cross-match must be negative immediately before transplantation in order to proceed with surgery. A positive high-titer B-cell cross-match is also a contraindication to transplantation; however, transplantation may proceed in the presence of a low-titer B-cell cross-match, provided that the T-cell cross-match and the flow cytometry cross-match are negative (14).
Immediate Preoperative Management
Appropriate recipients are selected based on a list that is generated by UNOS. This list takes into account the following factors: ABO blood type, human leukocyte antigen (HLA) matching, antibody testing, and waiting time. Although potential recipients are familiar to the transplant center physicians, they are carefully evaluated for recent infection or illness with blood tests, chest radiograph, and electrocardiogram (ECG). Because waiting lists are long and patients may have been waiting for several years, other illnesses may have developed in the interim that may contraindicate transplant surgery. Patients may require a treatment of hemodialysis or peritoneal dialysis prior to transplant surgery if there is evidence of hyperkalemia or fluid overload.
Immediate Posttransplant Management
Renal transplantation is carried out in the standard fashion through an incision that exposes the iliac fossa. The donor renal vessels are sutured in an end-to-side fashion to the external iliac artery and vein and a ureteroneocystostomy is created. Patients are monitored with continuous ECG and central venous pressure in the immediate postoperative period. Blood pressures are carefully monitored, as most patients have underlying hypertension and administration of immunosuppressive medications such as corticosteroids can affect blood pressure control. In addition, pain, catecholamine release, and fluid status may contribute to difficulties with blood pressure control. While adequate blood pressure control is important for the integrity of the renal arterial anastomosis, it is equally important to avoid hypotension and therefore prevent renal hypoperfusion and graft thrombosis.
Urine output is carefully monitored on an hourly basis via an indwelling urinary catheter. This urinary catheter also serves to protect the ureteroneocystostomy during the early postoperative period. Any increase in intravesical pressure due to incomplete emptying of the bladder could compromise the newly created anastomosis between the ureter and bladder. Hematuria occurring early posttransplant may be due to bleeding at the ureteral anastomosis, in the bladder, or along the urethra. This can be managed with gentle flushing of the urinary catheter with 20 to 30 mL of sterile saline. Changing the urinary catheter to one of a larger caliber may also help remove clots. Three-way urinary catheters are also used to facilitate continuous bladder irrigation should other measures fail to treat the hematuria.
|
|
|
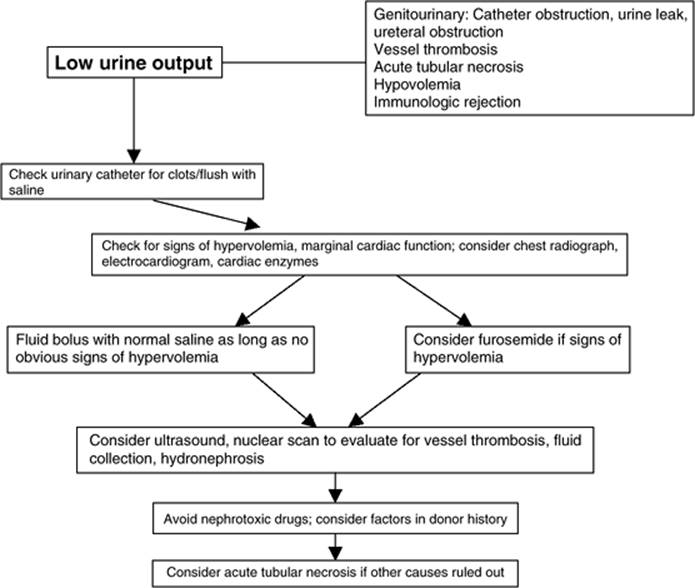
Figure 95.1. Algorithm for management of low urine output following renal transplant. |
Blood glucose monitoring is also done on a regular basis. Many transplant recipients have underlying diabetes mellitus and all patients may have hyperglycemia exacerbation related to administration of steroids and other immunosuppressive agents. Use of continuous insulin infusion and frequent blood glucose monitoring may be necessary to maintain good glycemic control. Optimal control of hyperglycemia in the postoperative period and in critically ill patients has been shown to decrease morbidity and mortality (15,16).
Particular attention should be paid to the volume and electrolyte status as the urine output in the immediate posttransplant period can vary from oliguria (frequently due to delayed graft function) to several liters as a result of generous fluid replacement during the surgery and also due to solute-induced osmotic diuresis. Living donor allografts typically have excellent immediate function and may have prompt and marked diuresis. Most transplant centers utilize a center-specific protocol with a fixed-rate maintenance of intravenous fluids usually with 0.9% normal saline at 50 mL/hour or 100 mL/hr together with replacement fluid at two thirds or one half of previous hour urine output. Some recipients may need hourly fluid replacement on a milliliter-for-milliliter basis in order to keep up with fluid losses. Kidneys from expanded donors or donation after cardiac death or with longer cold ischemia times may not have immediate function due to acute tubular necrosis (ATN). These recipients should be kept on a maintenance volume of intravenous fluids and the central venous pressure can be used to guide fluid status (Fig. 95.1). Other factors to consider would include the timing of the last dialysis and the amount of urine produced by the patient before transplant. Hemodialysis treatment shortly before the transplant surgery may render a recipient relatively hypovolemic during the perioperative period. Patients who have not yet been started on renal replacement therapy or who make a normal amount of urine may not have issues with hypovolemia.
Postoperative evaluation of electrolytes should include monitoring of serum sodium, potassium, bicarbonate, calcium, magnesium, and phosphorous. While some patients require bicarbonate supplements, potassium supplements are usually not necessary. However, supplementation may be required in patients with large-volume posttransplant diuresis.
Prophylaxis with subcutaneous heparin to prevent deep venous thrombosis and H2 receptor blockers or proton pump inhibitors to prevent gastric and/or duodenal ulcers are often administered. Patients should be evaluated for the need for dialysis based on their electrolyte, metabolic, and volume status.
Early Complications
The most common complication early posttransplant is an inappropriately low urine output. The differential diagnosis includes (a) obstruction of urine flow anywhere between the renal pelvis and the collection bag; (b) graft hypoperfusion; (c) urinary leak; (d) renal parenchymal disease, usually ATN; and (e) acute rejection in immunologically sensitized patients. If a brisk diuresis was observed in the operating room or has been recorded in previous hours, a sudden reduction in urine flow should immediately raise suspicion of a mechanical problem.
Frequently, blood clots obstruct the urinary catheter. The patient complains of a sense of fullness and need to urinate. “Milking” the urinary catheter tubing poses no risk of contaminating the closed system and usually dislodges the clots. If catheter irrigation is necessary, meticulously sterile technique is used. Sterile saline, 20 to 30 mL, should be instilled retrograde to facilitate mechanically breaking up the clot. Avoid overdistention of the bladder, which risks rupture of the ureteroneocystostomy or bladder closure. If irrigation fails to evacuate the clot, removal of the Foley catheter and replacement with a larger catheter (no. 18 through 20 F) is recommended. If clots still accumulate, a triple-lumen urinary catheter permits continuous bladder irrigation. Rarely, cystoscopy is required to evacuate clots.
Other mechanical problems include obstruction of the ureter or urine leak (17). These should always be suspected when there has been a history of brisk urine flow noted at surgery, but little or none has been noticed since bladder closure. Urine leak can present as severe wound pain, ascites, scrotal or labial edema, and fluid draining from the wound or operative drains with urea nitrogen and creatinine concentrations much higher than serum. Ultrasonography is particularly useful in diagnosing hydroureter or perinephric fluid collections (18). These problems require immediate operative correction.
After exclusion of outflow problems, factors that determine allograft perfusion should be addressed. Norms for “adequate” blood pressure are higher after transplantation, especially in children receiving adult kidneys and patients with limited cardiac contractility. To some degree, all transplanted kidneys have sustained predonation procurement and reperfusion injuries (19). There is an increase in interstitial edema and increased venocapillary resistance, endothelial swelling and denuding, and activation of vasoactive mediators. The resistance of the renal vascular bed is increased. Renal plasma flow requires a higher mean arterial pressure in this setting. The renal transplant recipient usually requires a blood pressure greater than 120/80 mm Hg. The patient's history of average pretransplant pressures is valuable in targeting perfusion pressure.
Unless there is clear evidence of intravascular volume overload, fluid boluses with normal saline are usually required. A transient response may justify further volume expansion. Most dialysis-dependent patients have total-body fluid overload. Their “dry weight,” used to calculate an end point on dialysis, is always in excess of the dry weight they reach with normal renal function. Several centers use low-dose dopamine (2.5 µg/kg/minute) in an attempt to improve renal perfusion. In rare circumstances, the intrarenal vascular resistance may be excessively high, and adequate perfusion pressures do not produce sufficient intrarenal blood flow. This problem dramatically increases the risk of further ischemic injury or even thrombosis. Grafts from pediatric donors, especially those younger than 4 years of age, are prone to thrombosis. As an additional safeguard, in recipients of pediatric en bloc kidneys, low-dose aspirin therapy immediately after surgery to minimize the risk of thrombosis should be considered. Graft thrombosis is rare, but any hope of graft salvage requires immediate return to the operating room.
Delayed Graft Function and Acute Tubular Necrosis
Delayed graft function (DGF) or acute renal dysfunction in the immediate posttransplant period has been a serious and frequent problem in cadaver renal transplantation and occurs in up to 30% of the recipients (20), and up to 35% to 40% in ECD and DCD kidney recipients, respectively. However, this diagnosis should be considered only after all other causes are eliminated. Acute tubular necrosis is the most common histologic feature in patients with DGF. The risk factors associated with an increased incidence of DGF include donor hypovolemia or hypotension, particularly in the presence of nephrotoxic drugs or vasopressors; prolonged cold or warm ischemia times; kidneys procured from older donors and from donors with hypertension or vascular occlusive disease; injury incurred during procurement, preservation, or implantation; and a high (>50%) panel reactive antibody level in the recipient (21,22,23). Living donor kidneys are much less likely to have DGF than deceased donor kidneys. The pathophysiology leading to DGF is complex and incompletely understood and appears to be due to ischemia–reperfusion injury. The short-term and long-term deleterious effects on graft survival that have been demonstrated in patients developing this disorder relate to its association with acute and chronic rejection (23,24). Therefore, protocols were developed to administer antilymphocyte antibodies for the preemptive treatment of acute rejection, during this period of graft dysfunction, when a diagnosis of rejection could be difficult. This led to the development of protocols termed sequential quadruple immunosuppressive therapy, where patients receive antibody induction followed by maintenance immunosuppression, usually with three agents.
Immunologic Causes of Early Graft Dysfunction
Hyperacute rejection is a rare and largely preventable cause of immediate graft failure. It is caused by preformed antibodies present in the recipients' serum at the time of transplantation against donor antigens. These antibodies are the consequence of previous exposure to donor antigens due to blood transfusions, prior transplantation, or pregnancy. It also occurs when transplantation is attempted across ABO-incompatible barriers. The events that lead to hyperacute rejection may occur with such rapidity that the kidney becomes visibly ischemic while the patient is still on the operating table. It always occurs within 24 hours of transplantation. Renal histology shows fibrin thrombi occluding the glomerular capillaries and small vessels with extensive tissue necrosis. Although plasmapheresis and anticoagulation have been advocated, there is no established effective treatment and interventions are seldom successful. A kidney with hyperacute rejection should always be removed promptly. The current cross-match techniques, because of their increased sensitivity, have greatly diminished the incidence of hyperacute rejection. Antibody-mediated (CD4 positive) acute rejection is another form of early rejection that can occur in previously sensitized patients but with an initial negative cross-match. This form of acute rejection is potentially reversible if diagnosed early and treated aggressively with plasmapheresis and intravenous immunoglobulin (25).
Immunosuppression
The different phases of immunosuppressive therapy after transplantation are (a) induction immunosuppression in the immediate posttransplantation period when potent therapy is required to prevent rejection; (b) maintenance immunosuppression for long-term therapy to prevent allograft rejection, but at the same time preserving host defense mechanisms against infections; and (c) intensification of the immunosuppressive therapy for the treatment of an acute rejection episode.
Antilymphocyte antibodies are ideally suited for use as induction immunosuppressive agents and some for the treatment of acute rejection. They have been available for use as immunosuppressive agents since the late 1960s. All early forms of antilymphocyte antibodies were polyclonal, which are made by injecting human lymphocytes into horses, goats, rabbits, or sheep. In contrast to polyclonal antibodies, a monoclonal antibody is highly specific, and recognizes a single antigen epitope. They have a greater potency at lower doses, and have a more predictable and consistent effect. Monoclonal antibodies that are currently approved for use in transplantation are directed either at cell surface receptors such as the CD3/T-cell receptor (TCR) complex (OKT3), or the interleukin-2 (IL-2) receptor (IL-2R; daclizumab and basiliximab). Current maintenance immunosuppression protocols often use the combination of a calcineurin inhibitor, an antimetabolite, and corticosteroids. However, the principles of the different regimens are similar: more intense immunosuppression in the induction phase with gradual reduction in immunosuppression in the maintenance phase. The immunosuppression protocol an institution implements should provide a balance between preventing rejection and avoiding the consequences of overimmunosuppression such as infection and malignancy.
Polyclonal Antibodies
Polyclonal antilymphocyte antibodies are produced by the immunization of rabbits (Thymoglobulin) or horses (Atgam) with human thymocytes. Several mechanisms of action have been proposed to explain the immunosuppressive effect of polyclonal antibodies. These include (a) complement-mediated cell lysis, (b) clearance of lymphocytes by opsonization and subsequent phagocytosis by macrophages, and (c) antibody-dependent cell-mediated cytolysis (26).
Polyclonal antibody treatment induces marked lymphocyte depletion that persists during the entire treatment period. The number of circulating T cells will gradually increase after the cessation of treatment and reach pretreatment levels in several weeks, with significant variability among patients. Each polyclonal antilymphocyte preparation varies in its constituent antibodies. Due to this unpredictable antibody mixture and batch-to-batch variability, treatment responses and side effects are variable between the different preparations (27).
There are two formulations of antithymocyte globulin available in the United States: Atgam, an equine polyclonal antithymocyte globulin, and Thymoglobulin, a rabbit polyclonal antithymocyte globulin. Thymoglobulin consists of antibodies specific for T-cell epitopes, including CD2, CD3, CD4, CD8, CD11a, CD18, CD25, HLA-DR, and HLA class I. Comparative studies have demonstrated superior efficacy of Thymoglobulin when compared to Atgam (28,29) and therefore the use of Thymoglobulin has largely superseded that of Atgam.
The most common side effect of polyclonal antibody treatment is the cytokine release syndrome, which usually occurs after the administration of the first few doses. However, these symptoms are not as severe as with OKT3. More severe reactions include the development of skin rashes, hypotension, acute respiratory distress, and anaphylaxis. Polyclonal antibodies often cross-react with antigens on unrelated cells, resulting in such side effects as granulocytopenia, thrombocytopenia, arthralgia, serum sickness, phlebitis, and immune complex glomerulonephritis. Because these agents severely impair the cell-mediated immunity, patients are prone to develop opportunistic infections and posttransplantation malignancies, especially posttransplantation lymphoproliferative disorders (PTLDs).
Thymoglobulin is dosed at 1.5 mg/kg/day, whereas Atgam is dosed at 10 to 15 mg/kg/day. Both antibody preparations are administered as an IV infusion over a period of about 6 hours. Premedication is recommended using high-dose methylprednisolone, an antihistamine, and acetaminophen 1 hour prior to the administration of these antibodies.
Monoclonal Antibodies
OKT3 (Muromonab)
OKT3 is a murine monoclonal antibody directed against CD3, a molecule closely associated with the TCR on the surface of human T cells (30). Antigen recognition by the TCR results in signal transduction via the CD3 molecule and subsequent T-cell proliferation and activation. OKT3 inhibits the CD3/TCR complex, thereby inactivating T lymphocytes. OKT3 is used for induction or for the treatment of acute rejection. The standard dose of OKT3 is 5 mg/day administered intravenously through a central or peripheral line.
The most common side effect of OKT3 is the cytokine release syndrome that typically begins 30 to 60 minutes after the administration of the first few doses and may last for several hours. This syndrome is characterized by fever, chills, tremor, nausea, vomiting, diarrhea, headache, myalgia, chest pain and tightness, and wheezing. This syndrome is believed to be mediated by a massive systemic release of cytokines by activated T cells. The cytokine release syndrome may cause severe pulmonary edema in patients who are fluid overloaded. It is therefore essential to assess the volume status of the patient prior to initiating OKT3 treatment and to induce diureses or dialyze as indicated (31). Cytokine nephropathy, a reversible renal dysfunction, has also been reported. In order to minimize or avoid the cytokine release syndrome, premedication is recommended using high-dose corticosteroids, an antihistamine, and acetaminophen 1 hour prior to the administration of OKT3 (32). Another drawback of OKT3 therapy is the production of human antimouse antibodies by the kidney transplant recipients' immune system. These antibodies may neutralize the efficacy of OKT3 treatment, thus limiting repeated use.
|
Table 95.1 Comparison of basiliximab and daclizumab |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
Immunologic monitoring using flow cytometric determination of the lymphocyte subsets to monitor depletion of CD3+ lymphocytes from the peripheral blood plays an essential role in the treatment of patients receiving OKT3 or antithymocyte globulin preparations. The absolute number of CD3+ cells should remain depressed throughout treatment. The guidelines for the number of CD3+ cells varies from fewer than 10/mm3 to more than 50/mm3 in different studies (33).
Anti-interleukin-2α Receptor Antibodies
IL-2 is a cytokine responsible for the growth and proliferation of activated T cells. During an immune response, IL-2 exerts its effects by binding to the IL-2R on the surface of the antigen-activated T cell. Anti-interleukin-2α receptor antibodies are monoclonal antibodies directed against the IL-2R on activated T cells. These antibodies are used as induction agents for prophylaxis against acute rejection in renal transplant recipients (34,35).
Basiliximab (Simulect) is a chimeric (human and mouse) IgG1κ monoclonal antibody that is administered as an IV infusion of two doses of 20 mg each. The first dose is given within 2 hours prior to transplantation and the second dose is given 4 days after transplantation. Daclizumab (Zenapax) is a humanized IgG1 monoclonal antibody that is administered as an IV infusion of five doses of 1 mg/kg body weight each. The first dose of 1 mg/kg is given prior to transplantation. Subsequent doses are administered every 2 weeks posttransplantation for a total of five doses. Adverse effects of the IL-2R antibodies are minimal and equivalent to placebo in controlled trials. Hypersensitivity reactions have been reported with both antibodies. The two IL-2R antibodies are compared in Table 95.1.
Alemtuzumab (Campath-1H)
Alemtuzumab (Campath-1H) is a humanized monoclonal antibody directed against the CD52 antigen (36,37) found on approximately 5% of the lymphocyte surface, making it the highest-density cell-surface marker on lymphocytes. Targeting of CD52 with antibody has shown to be exceptionally lytic of lymphocytes. The mechanism of action of alemtuzumab includes complement-mediated lysis, cell-mediated killing (antibody dependent cellular cytotoxicity [ADCC]), and induction of apoptosis of targeted cells. Alemtuzumab is a relatively low-affinity antibody, requiring 20 to 50 µg/mL to saturate its receptors (38). Because of the humanization of alemtuzumab, the first-dose effect is relatively mild. There is an associated tumor necrosis factor (TNF)-α and interferon-γ release that can be reduced with steroids. First infusion reactions such as fever, rash, nausea, vomiting, headache, and rigors due to a cytokine release syndrome have been reported with alemtuzumab treatment; however, these effects have been of a low-grade nature and limited with steroid pretreatment (38). Alemtuzumab effectively depletes immune cells, namely T and B lymphocytes; some natural killer (NK) cells; and some monocyte/macrophage lineage. Currently, alemtuzumab is approved for treatment of patients with B-cell chronic lymphocytic leukemia (39) and is not Food and Drug Administration (FDA) approved for use in transplant recipients in the United States. However, since the introduction of this agent for leukemic patients, a number of single-center trials have taken place in renal transplantation with good results (40,41). Results from a recently completed multicenter trial comparing alemtuzumab induction with that of basiliximab in low-immunologic-risk recipients and with Thymoglobulin for high-immunologic-risk recipients are pending.
Rituximab
Rituximab (Rituxan) antibody is a genetically engineered chimeric (human and mouse) monoclonal antibody directed against the CD20 antigen found on the surface of normal and malignant B lymphocytes (42). Rituximab is approved for the treatment of patients with relapsed or refractory, low-grade or follicular, CD20-positive, B-cell, non-Hodgkin lymphoma (43,44). Because of its effects on the B lymphocytes, rituximab is believed to be effective in the treatment of patients with antibody-mediated (humoral) acute rejection and is also thought to have a role in decreasing the panel reactive antibody (PRA) level in sensitized patients. However, it is not FDA approved for the latter indications and has not gained widespread support for use in transplant recipients, except for treatment in patients with PTLD (45).
Calcineurin Inhibitors
Calcineurin inhibitors are currently considered to be the mainstay of immunosuppression regimens following transplantation. They are potent immunosuppressants that inhibit T-cell activation by inhibiting calcineurin phosphatase, a key step in the regulation of cytokine expression. The introduction of calcineurin inhibitors in the mid-1980s has revolutionized the field of transplantation by dramatically reducing acute rejection rates and improving short-term allograft survival (46).
Cyclosporine
Cyclosporine A (CsA), the first calcineurin inhibitor approved for use in transplant recipients for maintenance immunosuppression, binds to cyclophilin in the T cell. The CsA/cyclophilin complex, in turn, inhibits calcineurin phosphatase, which is responsible for the transcription of IL-2. CsA is highly lipophilic and water insoluble. Early formulations (Sandimmune) were administered orally as an oil-based solution. In this form, bioavailability was erratic and highly variable and bile dependant for its absorption. This erratic absorption profile led to the development of a microemulsion formulation (modified cyclosporine, Neoral) that demonstrated a more reliable and predictable absorption. These two formulations are not bioequivalent and are thus not interchangeable. CsA is available in an IV formulation, as an oral solution, and in a capsule form. The IV formulation should be administered as a continuous infusion and should be limited to patients unable to take CsA orally, and the patient should be monitored closely during the infusion process. The dosage should be titrated based on whole blood concentration. The recommended starting dose of oral solution or capsules is 10 to 14 mg/kg/day for the nonmodified CsA and 6 to 12 mg/kg/day of the modified CsA administered 12 hours apart in divided doses. Various generic formulations of CsA are available. In the United States use of CsA has been superseded by that of tacrolimus in the majority of kidney transplant recipients and in almost all pancreas transplant recipients.
Tacrolimus
Tacrolimus (Prograf, FK-506) is a macrolide agent that inhibits IL-2 production in a similar fashion as CsA in the T lymphocyte. However, instead of binding to cyclophilin, tacrolimus binds to the FK binding protein 12 (FKBP-12) and the resulting complex inhibits calcineurin phosphatase. Tacrolimus is available in IV injection and oral capsule dosage forms. The IV form of tacrolimus is also administered as a continuous infusion and because of the risk of neurotoxicity should be limited to select patients unable to take tacrolimus orally. Tacrolimus is readily absorbed in the stomach and should be given orally or through nasogastric tube whenever feasible. The recommended starting dose of oral tacrolimus is 0.2 mg/kg/day administered 12 hours apart in divided doses.
Adverse Effects of the Calcineurin Inhibitors
Both calcineurin inhibitors have a narrow therapeutic window, multiple side effects, and drug interactions. Both drugs are metabolized by the cytochrome P450–3A4 enzyme system; their blood concentrations are affected by drugs that block or induce the cytochrome P450–3A4 enzyme system. Both drugs interact with some of the commonly used antibiotics, antifungal agents, and antihypertensive agents. Their interactions with other commonly used drugs are listed in Table 95.2. Both drugs cause acute and chronic nephrotoxicity. The acute nephrotoxicity is due in part to hemodynamic changes secondary to their vasoconstrictor effects on the afferent arteriole of the glomerulus. This results in a reduction in the glomerular filtration rate, manifested by an increase in the serum creatinine concentration. This acute change is dose related and reversible. However, the lesions associated with calcineurin inhibitor–induced chronic nephropathy may lead to end-stage renal failure. These lesions, which consist of tubulointerstitial striped fibrosis, tubular atrophy, afferent arteriolopathy, and global or focal glomerular sclerosis or collapse, have been well demonstrated in patients with autoimmune diseases treated with cyclosporine, as well as in the various organ transplant recipients: heart, liver, renal, and bone marrow (47,48). The other reported adverse effects of CsA and tacrolimus include hypertension, hyperkalemia, hyperlipidemia, and headache. Adverse effects unique to CsA include hirsutism and gingival hyperplasia, whereas those unique to tacrolimus include alopecia, fine tremor, and hyperglycemia. The adverse-effect profile of both CsA and tacrolimus is compared in Table 95.3.
|
Table 95.2 Common drug interactions with cyclosporine and tacrolimus |
||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
Table 95.3 Adverse-effect profile of cyclosporine A and tacrolimus |
||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||
Dose modifications of both CsA and tacrolimus are based on whole blood trough concentrations. Monitoring of the respective drug concentrations is an essential aid in the management of a transplant recipient for the evaluation of rejection, toxicity, dose adjustments, drug interactions, and compliance. Two methods for monitoring CsA levels in whole blood include high-pressure liquid chromatography (HPLC) and radioimmunoassay, or TDx. For tacrolimus, a microparticle enzyme immunoassay (MEIA) or an enzyme-linked immunosorbent assay (ELISA)-based IMx assay are utilized. Target levels of either drug vary based on the type of assay used, the type of monitoring (trough vs. C2 [drug level 2 hours postdose] vs. AUC [area under the curve]), transplant center standards, time posttransplantation, and the recipients' risk for acute rejection.
Antimetabolites
Mycophenolic Acid
Mycophenolate mofetil (MMF) (CellCept) and enteric-coated mycophenolate sodium (MPS) (Myfortic) contain the active moiety mycophenolic acid (MPA), a reversible inhibitor of inosine monophosphate dehydrogenase (IMPDH), a key, rate-limiting step in the de novo pathway of guanosine nucleotide synthesis. Depletion of the guanosine nucleotides inhibits T- and B-cell proliferation as they are dependent on the de novo pathway of purine synthesis rather than salvage pathways.
The recommended dose of MMF is 1,000 mg orally or IV twice daily divided 12 hours apart. MMF is the prodrug of MPA and allows for increased oral bioavailability. Some centers monitor MPA drug levels for dose adjustments. The MPS equivalent is 720 mg orally twice daily 12 hours apart, although due to differences in absorption, these two formulations are not interchangeable. MPS is not available for IV infusion and the enteric-coated tablets should not be cut, crushed, or chewed.
Adverse effects of MPA include gastrointestinal effects (dyspepsia, nausea, vomiting, diarrhea, and constipation) and bone marrow suppression (leukopenia and thrombocytopenia). Diarrhea, leukopenia, and thrombocytopenia are often dose limiting requiring dose reduction to ameliorate the toxic effects. These patients, however, should be monitored closely, as a relation exists between an increased incidence of acute rejection and decreased MPA doses (49,50).
Azathioprine
Azathioprine (Imuran) is an imidazole derivative of 6-mercaptopurine. It is a purine analog that inhibits DNA and RNA production in the T cell. The initial recommended dose of azathioprine is 3 to 5 mg/kg/day administered orally or IV once daily. Adverse effects of azathioprine include hematologic toxicities (pancytopenia, macrocytic anemia, thrombocytopenia, and leukopenia), alopecia, pancreatitis, and hepatotoxicity. Dose reductions may be required for myelosuppressive toxicities. A potent drug interaction may be seen with the coadministration of azathioprine and allopurinol (a xanthine oxidase inhibitor). Although it is recommended that the dose of azathioprine should be reduced by 75% when coadministered with allopurinol, it is more prudent to avoid the use of these two agents together.
mTOR Inhibitors
Sirolimus (Rapamune) is a macrolide antibiotic produced by Streptomyces hygroscopicus and is structurally similar to tacrolimus. Like tacrolimus, sirolimus also binds to FKBP-12. However, unlike tacrolimus, this complex binds to and inhibits the activation of the mammalian target of rapamycin (mTOR). This interferes with biochemical signal transductions from the cell membrane to the nucleus by inhibiting the stimulation of T cells by IL-2, -4, and -6 and by blocking the CD28 costimulatory signal. Sirolimus is available in oral tablets and oral solution. The recommended initial dose of sirolimus is approximately 6 mg (5–10 mg) loading dose, followed by 2 mg once daily maintenance dose. Dose adjustments are made based on weekly or biweekly trough level monitoring (t1/2 = 62 hours).
Adverse effects of sirolimus include anemia, leukopenia, thrombocytopenia, hyperlipidemia, prolongation of delayed graft function, impaired wound healing, pneumonitis, arthralgia, aphthous mouth ulcers, lymphocele, and diarrhea.
The advantage of sirolimus is due to its lack of nephrotoxicity (51,52). However, when coadministered with CsA, the nephrotoxic effect of CsA can be potentiated (53). Sirolimus is metabolized by the cytochrome P450–3A4 enzyme system and has a similar drug interaction profile as that of the calcineurin inhibitors.
Corticosteroids
Corticosteroids exert their immunosuppressive effects through multiple pathways, the most important of which is through their ability to inhibit cytokine and cytokine receptor transcription. Corticosteroids inhibit the expression of various cytokines responsible for the activation of T cells including IL-1, IL-2, IL-3, IL-6, TNF-α, and interferon-γ (IFN-γ). Corticosteroids function as both induction and maintenance immunosuppressive agents as well as for the treatment of acute rejection episodes. Typical induction protocols call for high-dose methylprednisolone, the first dose administered intraoperatively prior to organ perfusion with tapering doses for the first few days posttransplantation. This is followed by oral prednisone with continued tapering to a baseline maintenance dose. Corticosteroids are typically administered once a day in the morning concurrent with intrinsic cortisol release.
Adverse effects of corticosteroids are numerous and include cosmetic changes, avascular necrosis, cataracts, osteoporosis, impaired wound healing, glucose intolerance, hypertension, hyperlipidemia, increased appetite, hypothalamic–adrenal axis (HPA) suppression, and mood swings.
Corticosteroids were the first used immunosuppressant when renal transplants were done in the 1960s. Because of numerous adverse effects, steroid withdrawal has been attempted, but only with moderate success because of increased acute rejection. However, with the advent of newer and more effective immunosuppressive therapy, there has been a renewed interest in early withdrawal or complete elimination of corticosteroids. Short-term success has been achieved in several small single-center trials and a few larger multicenter trials. Early corticosteroid withdrawal has also been associated with a more favorable cardiovascular risk profile, as evidenced by less hypertension, posttransplant diabetes mellitus (PTDM), and hyperlipidemia (54).
|
Table 95.4 Cytomegalovirus (CMV) risk stratification and treatment options |
||||||||||||||||||||||||||||||
|
Minimizing Opportunistic Infections in the Transplant Recipient
Within the first month following transplantation, surgical wound-related and nosocomial infections are the most common infections observed in renal allograft recipients. As a result, bacterial infections involving the urinary tract, the respiratory tract, the surgical wound, and/or intravenous lines are the ones frequently encountered. In a few instances, infections may be due to reactivation of pre-existing infection in the recipient such as subclinical bacterial infections, especially urinary tract infections and tuberculosis, or transmission of infections from the donor to the recipient.
Infections in the 1-month to 6-month period after transplantation are due to opportunistic organisms, most notably viruses belonging to the herpes group, especially cytomegalovirus (CMV), and due to Candida species and Pneumocystis carinii. Antimicrobial prophylaxis specific to these opportunistic organisms should be given to all renal allograft recipients early posttransplantation. Prophylaxis protocols differ among centers in antimicrobial selection and duration of therapy. Prophylaxis with antifungals such as clotrimazole, nystatin, or fluconazole may be used against Candida infections of the mouth and throat (thrush). Prophylaxis against P. carinii pneumonia (PCP) includes cotrimoxazole; or for those patients with a sulfa allergy, monthly inhaled pentamidine or oral dapsone will provide adequate prophylaxis against PCP. Drug and dose selection of antiviral prophylaxis against CMV infection can be stratified by infection risk based on previous CMV exposure, or the presence of anti-CMV antibodies in the recipient (Table 95.4). Valganciclovir is currently the drug of choice for antiviral prophylaxis against CMV.
Several antimicrobial agents adversely interact with cyclosporine and tacrolimus, and careful consideration should be given to the choice of the antimicrobial agent.
“Stable” Allograft Recipients Readmitted to the Intensive Care Unit
Successful transplantation restores patients to an active and functional life, but it does not prevent subsequent occurrence of atherosclerotic cardiovascular disease, cancer, trauma, infections, and other major problems. Furthermore, the care of transplant patients with other diseases demands an awareness of the long-term problems that are unique to this patient population, and these are also discussed below.
Infections
Viral Infections
Cytomegalovirus is the most important viral infection affecting transplant recipients. CMV infection risk is highest in patients who are CMV IgG seronegative and received an allograft from a CMV-seropositive donor (Table 95.4) or who have received CMV-positive blood transfusion. CMV infection often presents clinically with fever after cessation of anti-CMV prophylaxis and in some instances may present as disseminated or tissue invasive CMV disease affecting the gastrointestinal tract, liver, kidney, or lungs (pneumonitis) and with organ-specific symptoms. CMV is diagnosed by identification and quantification of the viral DNA in the blood by polymerase chain reaction (PCR). Tissue-invasive disease may be diagnosed by the identification of the characteristic owl-eye inclusions on tissue biopsy (55). Treatment of CMV viremia and tissue-invasive CMV disease should be initiated promptly with oral valganciclovir or intravenous ganciclovir. Concomitant treatment with CMV immune globulin may be required in some patients with severe tissue disease. Duration of treatment depends on the extent of the disease and continued positivity of the CMV-DNA by PCR.
Other viral infections that may occur in the immunosuppressed renal allograft recipient include Epstein-Barr virus (EBV), which may lead to the development of EBV-positive lymphomas; herpes simplex virus (types I and II); hepatitis B virus; hepatitis C virus; varicella-zoster virus; and the influenza virus. Treatment of viral infections depends on the type of virus and the extent of the disease. All transplant recipients should receive an annual influenza immunization.
Fungal Infections
Fungal infections are a major concern in the immunosuppressed renal allograft recipient. As with the general population, Candida albicans infections resulting from endogenous flora are common. However, with immunosuppression, these infections can rapidly develop into more serious infections. Other fungal pathogens seen in transplant recipients include nocardiosis, aspergillosis, Cryptococcus, histoplasmosis, coccidiomycosis, blastomycosis, and mucormycosis. Treatment of fungal infections include the use of antifungals specific to the organism, surgical excision (especially in the case of mucormycosis), and reduction in the overall immunosuppression. Careful consideration should be given to the choice of the antimicrobial agent because of drug interactions (azole antifungals) or additive nephrotoxicity (amphotericin B). Invasive fungal infections in transplant recipients are associated with a high risk of graft loss and mortality. Early diagnosis and aggressive treatment can preserve organ function and can be life saving.
Other Opportunistic Infections
Urinary tract infections (UTIs) are a frequent complication of renal transplantation. Although UTIs are frequently asymptomatic, they constitute the major source of bacteremia in this patient population. Therefore, all urinary tract infections, even asymptomatic ones, should be treated appropriately. Fortunately, renal dysfunction is an uncommon complication of urinary tract infections in the transplant recipient. It usually occurs with severe pyelonephritis involving the allograft, usually in the setting of ureteric obstruction or vesicoureteral reflux. Chronic urinary tract infections may require daily prophylactic antibiotic administration.
Renal allograft recipients, especially patients with poor allograft function with a background of intensive acute and chronic immunosuppressive therapy for recurrent rejection episodes, are susceptible to a large range of infections. Empiric treatment should be initiated at the first sign of infection as infections can be aggressive and worsen rapidly.
Gastrointestinal Complications
A wide variety of gastrointestinal complications may occur after transplantation due to infections with organisms such as CMV, Candida sp., and Clostridium difficile; adverse effects associated with immunosuppressive agents; posttransplantation complications of pre-existing conditions such as diverticulitis; and other complications such as acute appendicitis, gastrointestinal bleeding, colonic or small bowel perforations, pancreatitis, and ischemic colitis. Diarrhea is a common problem in transplant recipients and may be related to the immunosuppressive drugs, due to opportunistic infections, or due to pre-existing autonomic dysfunction often related to diabetes mellitus.
Peptic Ulcer Disease
Gastroduodenal ulcers account for most of the gastrointestinal complications posttransplantation and often occur soon after renal transplantation or acute rejection therapy. Gastroduodenal ulcers presenting posttransplantation can be attributed to a variety of causes including pre-existing ulcer history, viral pathogens (CMV in 15%, herpes simplex in 2%), and immunosuppressive agents, mainly corticosteroids (56,57,58,59). The treatment of posttransplantation gastroduodenal ulcers is the same as with the general population. Proton pump inhibitors and H2-receptor blocking agents may be used for both therapy and prophylaxis. Intermittent therapy with calcium, aluminum, or magnesium salts can provide immediate relief; however, coadministration of these agents with MMF (CellCept) may inhibit absorption of the active moiety of this drug in the intestinal tract. All kidney transplant recipients diagnosed with gastroduodenal ulcers should be evaluated for Helicobacter pylori and CMV infection. Clarithromycin (Biaxin), commonly used for the treatment of H. pylori, interacts with CsA and tacrolimus (Table 95.2), and therefore ideally, an alternate antibiotic regimen should be used. For CMV-related gastrointestinal lesions, ganciclovir or valganciclovir treatment should be initiated promptly.
Bowel Perforations
Colonic perforation should be suspected in the presence of one or more of the following: abdominal pain, fever, increased white blood cell count, tenderness, and pneumoperitoneum. These clinical criteria may be blunted in the presence of poor renal function, use of high-dose corticosteroids, or the overall state of immunosuppression. A plain abdominal radiograph, CT scan, or colonoscopy may help in the diagnosis. Mortality rates after colonic perforation can be reduced with minimal delay to perform surgery, broad-spectrum antibiotic therapy, and reduction of immunosuppression. Operative intervention has been shown to improve patient survival significantly (60). Screening for colonic diverticula before transplantation should be applied to all patients older than age 50 years, and a segmental colectomy may be required in patients who have experienced clinical symptoms of diverticulitis (56,60).
Acute Pancreatitis
Acute pancreatitis is an infrequent but severe complication following renal transplantation. A review of the literature has documented an incidence of 2.3% with a mortality rate of 61.3% in 3,253 renal transplant recipients (61). Several etiologic factors have been considered. Azathioprine has been reported to cause pancreatitis with rapid improvement after cessation and with recurrence of symptoms with reinstitution (62). Corticosteroids and cyclosporine have also been reported to cause pancreatitis; however, this association is not as convincing. Other causes of pancreatitis include hyperparathyroidism, CMV infection, biliary tract disease, alcoholism, and hyperlipidemia (63). Although the diagnosis of pancreatitis depends largely on an increase in the serum amylase and/or serum lipase levels, ultrasonography and CT scan may be useful. Intensive medical management with particular attention to volume replacement, electrolyte balance, and nutrition is essential.
Severe diarrhea with ensuing dehydration and acidosis, gastrointestinal bleeding, cholecystitis, and diverticulitis are other commonly encountered gastrointestinal problems in the transplant recipient. Advances in the management of peptic ulcer disease, prophylaxis against CMV disease, and better preparation of recipients prior to transplantation have reduced the overall morbidity and mortality. Several of the gastrointestinal problems may be related to the side effects of the immunosuppressive drugs or due to the net state of overimmunosuppression. Careful consideration should be given to the change in the immunosuppressive agent and to decrease in the dosages of these medications.
Hematologic Complications
Neutropenia is a frequent complication posttransplantation, often as a result of the adverse effects of immunosuppressive medications. Antithymocyte globulin can cause transient decreases in neutrophils that often rebound after cessation of therapy. Maintenance immunosuppression with mycophenolic acid, sirolimus, and prophylaxis with ganciclovir and cotrimoxazole contribute to the development of neutropenia due to their myelosuppressive effects. Careful dose reduction of these agents and/or use of granulocyte-stimulating factors are often required for persistent neutropenia. Of particular importance is that neutropenia can be a sign of CMV infection, and therefore this should always be excluded in transplant recipients with persistent neutropenia.
Anemia is a frequent occurrence in the early posttransplantation period as a result of pre-existing anemia of end-stage renal disease, surgical blood loss, and immunosuppressive medications. Patients with slow or delayed graft function may have a more pronounced and prolonged anemia. Anemia in the late posttransplantation phase can be attributed to a combination of immunosuppressive medications, renal allograft dysfunction, use of angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers, and/or iron deficiency (64). As cardiovascular disease is the leading cause of morbidity and mortality in kidney transplant recipients, it is important to manage anemia aggressively in this patient population with the use of erythropoietin. Furthermore, given the high incidence of coexisting cardiovascular disease in this patient population, blood transfusions should not be withheld for acute indications.
Thrombocytopenia is also a frequent occurrence in renal allograft recipients and often is caused by the immunosuppressive medications. Antithymocyte globulin, valganciclovir, and dapsone can cause transient decreases in platelets. Withholding doses or dose adjustments of the responsible agent may be required for thrombocytopenia. Platelet recovery is rapid, often returning to baseline within days. In rare circumstances, thrombocytopenia may be due to hemolytic uremic syndrome (HUS) that is caused by immunosuppressive drugs (calcineurin inhibitors, sirolimus, OKT3), severe acute vascular rejection, transmission from donor, recurrence of previous HUS, or causes similar to those in nontransplant recipients.
Cardiac and Vascular Diseases
Coronary Artery Disease
Atherosclerotic vascular disease is the major cause of late morbidity and mortality in transplant recipients, and coronary artery disease is the principal cause of death (65,66,67,68,69). In transplant recipients, risk factors for posttransplantation coronary artery disease include increased age, male gender, history of diabetes mellitus, hypercholesterolemia, smoking history, acute renal allograft rejection episodes, and greater cumulative dose of steroids (70). The key to the early detection of significant coronary artery disease in renal transplant recipients without coronary symptoms is repeated evaluation for the known risk factors. The management of transplant patients with coronary artery disease is similar to that of other patients and should include noninvasive exercise or resting diagnostic testing, coronary arteriography, or both. However, some noninvasive screening tests have been shown to be less useful, especially in the presence of diabetes, uremia, and left ventricular hypertrophy (71). With the increasing number of transplantations performed in the elderly and in patients with diabetes mellitus, cardiovascular disease will continue to be a major cause of posttransplantation morbidity. Of particular note, during cardiac catheterization, femoral arterial puncture on the ipsilateral side to the renal transplant should be avoided whenever feasible to reduce the risks of mechanical injury and atheroembolization to the renal allograft.
Cerebrovascular and Peripheral Vascular Disease
Cerebrovascular disease occurs in 1% to 3% of all renal allograft recipients (65,72). There is also an increased risk of peripheral vascular disease (65,68,73,74). A thorough history to elicit symptoms associated with cerebrovascular and peripheral vascular disease and examination of the carotid arteries and peripheral circulation should be performed annually and the presence of a carotid bruit should be further investigated with duplex ultrasonography and magnetic resonance angiography (MRA). In the presence of more than 60% stenosis of the carotid artery, the patient should be referred to the neurovascular surgeon for further evaluation (75).
Successful transplantation does not reduce the rate of atherosclerosis initiated in renal failure. Factors contributing to the high incidence of vascular disease include hypertension, hyperlipidemia, obesity, cigarette smoking, and the presence of pre-existing diabetes mellitus or the development of posttransplantation diabetes mellitus (65). The mortality rate from coronary artery disease was increased 25-fold to that of age-matched and gender-matched controls in an Australian study (76), was increased 10-fold in a study from Stockholm (77), and was increased three- to fourfold in a Minneapolis study (70). By actuarial analysis, 15% of patients who survived with a functioning allograft for 15 years developed peripheral vascular disease (73).
Hypertension
Hypertension is a common complication of renal transplantation and remains an important risk factor for mortality from cardiovascular disease. Posttransplantation hypertension is a major risk factor for graft survival. It is unclear, however, whether this is because of the deleterious effects of hypertension on the structure and function of the renal allograft or whether hypertension is a marker of underlying renal disease (78,79). The causes of hypertension in renal transplant recipients include acute and/or chronic allograft rejection; recurrent or de novo transplant glomerulonephritis; transplant renal artery stenosis; high renin output state from diseased native kidneys; immunosuppressive agents such as steroids, cyclosporine, and tacrolimus; obesity; hypercalcemia; and new-onset essential hypertension (80).
Hyperlipidemia
As discussed earlier, cardiovascular disease is the most common cause of posttransplantation morbidity and mortality among long-term renal transplant survivors. As in the general population, posttransplantation lipoprotein abnormalities contribute to the development of cardiovascular and peripheral vascular disease in renal transplant recipients (67,73,81,82). The prevalence of posttransplantation hyperlipidemia ranges from 16% to 78% of recipients (65), depending at which time point posttransplantation serum lipid levels were obtained. Elevations in triglycerides, low-density lipoproteins (LDLs), apolipoprotein B, and total cholesterol levels are common (83,84,85,86,87,88,89,90,91). The pathogenesis of hyperlipidemia in renal transplant recipients is poorly understood and appears to be multifactorial. The numerous factors that have been shown to be associated with hyperlipidemia after renal transplantation are age, body weight, gender, pretransplantation lipid levels, renal dysfunction, proteinuria, concomitant use of diuretics or β-blockers, diabetes, steroid use, and cyclosporine and sirolimus use (81,83,84,85,86,87,88,89,92,93).
New-onset Diabetes after Transplantation
New-onset diabetes after transplantation (NODAT) has been reported in 3% to 40% of transplant recipients with an even higher incidence occurring in African Americans, Hispanics, and patients with a family history of diabetes mellitus, increasing with recipient age and weight (65,66,69,72,94,95,96). NODAT has been attributed to the use of immunosuppressive agents, especially with tacrolimus and corticosteroids; however, cyclosporine has also been implicated (96,97,98,99). Patients with NODAT have a poor outcome in terms of patient and graft survival, with increased mortality resulting from cardiovascular and possibly infectious complications (95,100).
Insulin treatment may be required in patients with NODAT who do not respond to lifestyle modification and oral hypoglycemic agents. About half of patients in whom NODAT develops require insulin. Aggressive treatment with either intravenous or subcutaneous insulin may also be indicated during periods of intercurrent illness and stress.
Graft Dysfunction and Graft Failure
The differential diagnosis of acute allograft dysfunction can be divided into (a) early, occurring <90 days posttransplantation, and (b) late, occurring >90 days after transplantation. It can be further differentiated into medical and surgical problems as outlined in Table 95.5. Some of the more common medical and surgical problems are discussed below.
Acute Rejection
Although acute allograft rejection is the most common cause of graft dysfunction both in the early and late periods, it most commonly occurs during the first 90 days posttransplantation.
Recipients of transplants from living donors have a significantly lower incidence of rejection episodes. Factors significantly associated with the development of acute rejection are HLA mismatch, anti-HLA antibodies reactive to greater than 50% of a lymphocyte panel, retransplantation, African American race, and recipient age under 16 (101,102). The classic clinical features associated with acute rejection are fever, oliguria, weight gain, edema, hypertension, and the presence of an enlarged, tender graft. However, these features are frequently absent, and the most common presentation may be an asymptomatic rise in serum creatinine. An increase in serum creatinine greater than 20% is often the cardinal feature of rejection. Percutaneous needle biopsy of the allograft is the most reliable method of diagnosis of acute rejection. Acute rejection is classified histologically using the Banff 97 classification of renal allograft pathology depending on the severity of lymphocytic infiltration of tubules (tubulitis), arterioles (arteritis), and the renal interstitium (103).
|
Table 95.5 Causes of graft dysfunction and failure |
|||||||||
|
The principles and the management of acute rejection include rapid diagnosis, accurate classification, and prompt administration of antirejection therapy. Currently, corticosteroids and antilymphocyte antibodies represent the main components of antirejection treatment protocols. The decision on treatment of acute rejection is based on histologic severity. One approach is to treat mild acute cellular rejection with a course of 250 to 500 mg of intravenous methylprednisolone administered daily for 3 or 4 days, and moderate and severe acute cellular rejection and acute vascular rejection are treated with a 4- to 7-day course of an antilymphocyte antibody, currently either Thymoglobulin or OKT3.
Chronic Rejection
Chronic rejection is characterized clinically by a progressive decline in renal function, persistent proteinuria, and hypertension. The course of chronic rejection is slow and insidious. Chronic rejection often occurs in conjunction with other histologic causes of allograft dysfunction, namely, acute rejection, calcineurin inhibitor nephrotoxicity, and recurrent or de novo glomerular diseases. The diagnosis of chronic rejection should therefore be based on morphologic characteristics of allograft histology and the clinical observation of a gradual decline in renal allograft function. The pathophysiology of chronic rejection is not completely understood, but most likely involves both immune and nonimmune factors. Risk factors for the development of chronic rejection include delayed graft function, ischemia–reperfusion injury, degree of HLA mismatching, histoincompatibility, acute rejection episodes, inadequate renal mass, hypertension, hyperlipidemia, and cytomegalovirus infection (104). There is no treatment for chronic rejection at the present time.
Urologic Complications
Urologic problems have been reported in between 2% and 20% of all renal transplants (105,106,107,108,109). These complications can include urinary retention, urine leak, and ureteral stenosis. Urinary retention can occur because of a neurogenic bladder (related to diabetes or a congenital neurologic disorder) or perhaps an undetected prostatic hypertrophy. These can be managed with an initially longer period of urinary catheterization and use of α-antagonists (tamsulosin, terazosin, prazosin) to improve bladder emptying. More extreme cases may require long-term intermittent self-catheterization or surgical urinary diversion. Urine leak or stenosis can occur both early and later after renal transplant and will be manifested by a rising serum creatinine. Urine leaks may also result in increased fluid through an operative drain or fluid leakage through the wound. This fluid can be sent for creatinine level to confirm the presence of a urine leak. Ultrasound studies may demonstrate a fluid collection around the allograft or hydronephrosis in the case of ureteral stenosis. Nuclear medicine scans can also be obtained to confirm the presence of a ureteral stenosis or urine leak. Mild cases of ureteral stenosis/leakage can be managed with percutaneous methods including insertion of ureteral stents and transluminal balloon dilation. Many of these stenoses/leaks will require operative management to reimplant the ureter or a more complex urologic procedure using the recipient's native ureter or bladder (105,106,107,108,109).
Vascular Complications
Vascular complications including vessel thrombosis or stenosis have been reported in 2% to 12% of all renal transplants. Vascular complications in general are significantly associated with ATN and graft loss. Early graft dysfunction should be evaluated for vascular complications with ultrasound with Doppler (110). Patients with underlying thrombophilia are at a higher risk for early allograft loss without appropriate anticoagulation. Screening for thrombophilia in those ESRD patients with a history of a thromboembolic event may be appropriate to prevent this. Those patients with graft loss due to vascular thrombosis in the absence of an obvious technical problem should undergo a thrombophilia evaluation before retransplant (111).
Lymphocele
A lymphocele is a collection of lymphatic fluid around the allografted kidney that can occur due to leakage of small lymphatic channels around the iliac vessels at the time of the transplant. The incidence of lymphoceles has been reported from 0.02% up to 26% following renal transplant (112,113,114). Consequences of lymphoceles can include distention due to the fluid collection as well as venous or ureteral obstruction and graft compromise. Treatment of lymphoceles can include percutaneous techniques with drainage and sclerosis of the cavity or may include operative marsupialization via the laparoscopic or open technique. Laparoscopic techniques are less invasive, have less morbidity, and are generally the first line of therapy (114).
Stones
Urinary calculi are a relatively uncommon complication of renal transplantation. Calculi may have been present in the donor kidney or may develop after transplantation. Predisposing factors include obstruction, recurrent urinary tract infection, hypercalciuria, hyperoxaluria, internal stents, and nonabsorbable suture material (115). Open removal of a calculus from the transplanted kidney is rarely necessary. Complete stone removal is usually possible by standard urologic techniques.
Posttransplant Malignancies
Prolonged and intensive immunosuppression impairs the ability of the body to cope with cancers caused by carcinogens such as sunlight or oncogenic viruses and may lead to the development of an unusual assortment of malignancies (116,117). Infections with potentially oncogenic viruses are common in immunosuppressed patients, including EBV-related B-cell PTLD, human papillomavirus, hepatitis B and hepatitis C virus–related hepatocellular carcinoma, and the human herpes virus-8 (Kaposi sarcoma) (117). Malignancies that occur in transplant recipients have a pattern that is very different from that of the general population. The frequency of the cancers that are common in the general population, such as carcinomas of the lung, prostate, breast, and colon and invasive carcinomas of the uterine cervix, are not increased among transplant recipients (116). Most patients who develop malignancies posttransplant have received multiple immunosuppressive drugs and no single agent can be implicated. The natural history of tumors associated with immunosuppression used for renal transplantation may be more aggressive than would be expected in patients without immunosuppression or transplantation. Cancers of the lip and skin are the most common malignancies. In contrast to the general population, squamous cell carcinoma outnumbers basal cell carcinoma and occurs at a much younger age.
PTLDs are the second most common malignancies found in renal transplant recipients, with the bulk being non-Hodgkin lymphomas. The EBV genome has been isolated from many lymphomas in transplant recipients and causes a variety of lesions that range from benign polyclonal B-cell hyperplasia to frank monoclonal B-cell lymphomas (116,118). Risk factors for PTLD include the overall extent of immunosuppression of the patient. Use of monoclonal/polyclonal antibodies for induction and repeated treatments for acute rejection will significantly increase the risk for PTLD (116,119). The clinical symptoms of PTLD may be extremely variable, and a high index of suspicion is required for accurate diagnosis. PTLD may present in the lymph nodes or extranodally. There are two basic clinical patterns with some overlap. The first, occurring in the early (usually <90 days) posttransplantation period, usually manifests with widespread lesions in an EBV-susceptible patient. The second pattern occurs in patients who received long-term immunosuppression and may present several years after transplantation, with lesions confined to a single organ (120,121).
Treatment of PTLD consists of partial or complete withdrawal of immunosuppression. Such treatment carries the risk of allograft rejection and return of the renal allograft recipient to dialysis. Treatment with prednisone may be continued, however, because it is an important component of many cancer chemotherapy protocols. If EBV infection is suspected, treatment with acyclovir, ganciclovir, or valacyclovir should be initiated pending documentation of EBV infection. Other treatment options include interferon-γ therapy to enhance the immune attack on the lymphoma cells; surgical excision or local radiotherapy to localized tumors; and in advanced cases, chemotherapy. Rituximab (Rituxan; Genentech), a monoclonal antibody directed against the CD20 antigen, has been used successfully to treat CD20-positive tumors (122,123,124).
References
1. Kidney and Urologic Diseases Information Clearinghouse. A service of the National Institute of Diabetes and Digestive Diseases and Kidney Diseases, National Institutes of Health. Available at: http://kidney.niddk.nih.gov/kudiseases/pubs/kustats/index.htm. Accessed October 15, 2006.
2. Winkelmayer WC, Weinstein MC, Mittelman MA, et al. Health economic evaluations: the special case of end-stage renal disease treatment. Med Decis Making. 2002;22:417.
3. Loubeau PR, Loubeau JM, Jantzen R. The economics of kidney transplantation vs hemodialysis. Prog Transplant. 2001;11:291.
4. National transplant statistics, 2005. United Network for Organ Sharing. Available at: www.unos.org. Accessed October 15, 2006.
5. Remuzzi G, Grinyo J, Ruggenenti P, et al. Early experience with dual kidney transplantation in adults using expanded donor criteria. Double Kidney Transplant Group (DKG). J Am Soc Nephrol. 1999;10:2591.
6. Gok MA, Buckley PE, Shenton BK, et al. Long-term renal function in kidneys from non-heart beating donors: a single-center experience. Transplantation. 2002;74:664.
7. Sanchez-Fructuoso A, Sanchez DP, Vidas MM, et al. Non-heart beating donors. Nephrol Dial Transplant. 2004;19(Suppl 3):iii26.
8. U.S. Organ Procurement and Transplantation Network/Scientific Registry of Transplant Recipients, Annual Report 2005.
9. Kasiske BL, Cangro CB, Hariharan S, et al. The evaluation of renal transplant candidates: clinical practice guidelines. Am J Transplantation. 2001;2(Suppl 1):5–95.
10. Gore JL, Pham PT, Danovitch GM, et al. Obesity and outcome following renal transplant. Am J Transplantation. 2006;6:357.
11. Stratta RJ, Rohr MS, Sundberg AK et al. Intermediate-term outcomes with expanded criteria deceased donors in kidney transplantation: a spectrum or specter of quality. Ann Surg. 2006;243:594.
12. Merion RM, Ashby VB, Wolfe RA, et al. Decreased-donor characteristics and the survival benefit of kidney transplantation. JAMA. 2005;294:2726.
13. Bernat JL, D'Alessandro AM, Port FK, et al. Report of a national conference on donation after cardiac death. Am J Transplant. 2006;6:281.
14. Ting A, Welsh K. HLA matching and crossmatching in renal transplantation. In: Morris PJ, ed. Kidney Transplantation: Principles and Practice. 4th ed. Philadelphia: WB Saunders; 1994:109.
15. Furnary AP, Wu Y, Bookin SO. Effect of hyperglycemia and continuous intravenous insulin infusions on outcomes of cardiac surgical procedures: the Portland Diabetic Project. Endocr Pract. 2004;10:21.
16. Finney SJ, Zekveld C, Elia A, et al. Glucose control and mortality in critically ill patients. JAMA. 2003;290:2041.
17. Starzl TE, Broth CG, Putnam CW, et al. Urologic complications in 216 human recipients of renal transplants. Ann Surg. 1973;172:609.
18. Petrek J, Tilney NL, Smith EH, et al. Ultrasound in renal transplantation. Ann Surg. 1977;185:441.
19. Maley HT, Bulkley GB, Williams GM. Ablation of free radical-medicated reperfusion injury for the salvage of kidneys taken from non-heartbeating donors. Transplantation. 1988;45:284.
20. Sola R, Alarcon A, Jimenez C, et al. The influence of delayed graft function. Nephrol Dial Transplant. 2004;19(Suppl 3):iii32.
21. Boom H, Mallat MJ, deFijter JW, et al. Delayed graft function influences renal function, but not survival. Kidney Int. 2000;58:859.
22. Irish WD, McCollum DA, Tesi RJ, et al. Nomogram for predicting the likelihood of delayed graft function in adult cadaveric renal transplant recipients. J Am Soc Nephrol. 2003;14:2967.
23. Shoskes DA, Halloran PF. Delayed graft function in renal transplantation: etiology, management and long-term significance. J Urol. 1996;155:1831.
24. Ojo AO, Wolfe RA, Held PJ, et al. Delayed graft function: risk factors, and implications for renal allograft survival. Transplantation. 1997;63:968.
25. Rocha PN, Butterly DW, Greenberg A, et al. Beneficial effect of plasmapheresis and intravenous immunoglobulin on renal allograft survival of patients with acute humoral rejection. Transplantation. 2003;75:1490.
26. Bonnefoy-Berard N, Revillard JP. Mechanisms of immunosuppression induced by antithymocyte globulins and OKT3. J Heart Lung Transplant. 1996;15:435.
27. Rossi SJ, Schroeder TJ, Hariharan S, et al. Prevention and management of the adverse effects associated with immunosuppressive therapy. Drug Saf. 1993;9:104.
28. Gaber AO, First MR, Tesi RJ, et al. Results of the double-blind, randomized, multicenter, phase-III clinical trial of Thymoglobulin versus Atgam in the treatment of acute graft rejection episodes after renal transplantation. Transplantation. 1998;66:29.
29. Brennan DC, Flavin K, Lowell JA, et al. A randomized, double-blinded comparison of Thymoglobulin versus Atgam for induction immunosuppressive therapy in adult renal transplant recipients. Transplantation. 1999;67:1011.
30. Ortho Multicenter Transplant Study Group. A randomized clinical trial of OKT3 monoclonal antibody for acute rejection of cadaveric renal transplants. N Engl J Med. 1985;313:337.
31. First MR, Schroeder TJ, Hariharan S. OKT3-induced cytokine release syndrome: renal effects (cytokine nephropathy). Transplant Proc. 1993;25:25.
32. Chatenoud L, Legendre C, Ferran C, et al. Corticosteroid inhibition of the OKT3-induced cytokine release syndrome: dosage and kinetics prerequisites. Transplantation. 1991;51:334.
33. Peddi VR, Bryant M, Roy-Chaudhury P, et al. Thymoglobulin induction therapy in cadaveric renal allograft recipients: intermittent dosing with CD3+ lymphocyte count monitoring [Abstract]. Transplantation. 2000;69:S160.
34. Vincenti F, Kirkman R, Light S, et al., for the Daclizumab Triple Therapy Study Group. Interleukin-2- receptor blockade with daclizumab to prevent acute rejection in renal transplantation. N Engl J Med. 1998;338:161.
35. Nashan B, Moore R, Amlot P, et al., for the CH1B 201 International Study Group. Randomized trial of basiliximab versus placebo for control of acute cellular rejection in renal allograft recipients. Lancet. 1997;350:1193.
36. Riechmann L, Clark M, Waldmann H. Reshaping human antibodies for therapy. Nature. 1988;332:323.
37. Hale G, Xia MQ, Tighe MJS, et al. The Campath-1H antigen (CDw52). Tissue Antigens. 1990;35:118.
38. Hale G. CD52 antigen as a target for immunotherapy. Transpl Rev. 2003;17:S8.
39. Waldmann H. Development and clinical use of Campath 1H. Transpl Rev. 2003;17:S5.
40. Kaufman DB, Leventhal JR, Axelrod D, et al. Alemtuzumab induction and prednisolone-free maintenance immunotherapy in kidney transplantation: comparison with basiliximab induction. Long-term results. Am J Transpl. 2005;78:426.
41. Shapiro R, Basu A, Tan H, et al. Kidney transplantation under minimal immunosuppression after pretransplant lymphoid depletion with Thymoglobulin or Campath. J Am Coll Surg. 2005;200:505.
42. Nadler LM, Ritz J, Hardy R, et al. A unique cell surface antigen identifying lymphoid malignancies of B-cell origin. J Clin Invest. 1981;67:134.
43. Maloney D, Liles T, Czerwinski D, et al. Phase I clinical trial using escalating single dose infusion of chimeric anti-CD 20 monoclonal antibody in patients with recurrent B-cell lymphoma. Blood. 1994;84:2457.
44. Coiffier B, Haioun C, Ketterer N, et al. Rituximab for the treatment of patients with relapsing or refractory aggressive lymphoma: a multicenter phase II study. Blood. 1998;92:1927.
45. Blaes AH, Peterson BA, Bartlett N, et al. Rituximab therapy is effective for post transplant lymphoproliferative disorders after solid organ transplantation: results of a phase II trial. Cancer. 2005;104:1661.
46. Rosenthal JT, Hakala TR, Iwatsuki S, et al. Cadaveric renal transplantation under cyclosporine-steroid therapy. Surg Gynecol Obstet. 1983;157:309.
47. Myers BD, Newton L, Oyer P. The case against the indefinite use of cyclosporine. Transplant Proc. 1991;23:41.
48. Bennett WM, DeMattos A, Meyer MM, et al. Chronic cyclosporine nephropathy: the Achilles' heel of immunosuppressive therapy. Kidney Int. 1996;50:1089.
49. Hardinger KL, Brennan DC, Mutinga N, et al. Long-term outcome and cost of gastrointestinal complications in renal transplant patients treated with mycophenolate mofetil (MMF). Presented at American Society of Transplantation, May 30–June 4, 2003; Washington DC. Poster #1595.
50. Knoll GA, MacDonald I, Khan A. Mycophenolate mofetil dose reduction and the risk of acute rejection after renal transplantation. J Am Soc Nephrol. 2003;14:2381.
51. Morales JM, Wramner L, Kreis H, et al. Sirolimus does not exhibit nephrotoxicity compared to cyclosporine in renal transplant recipients. Am J Transplant. 2002;2:436.
52. Reitamo S, Spuls P, Sassolas B, et al. Efficacy of sirolimus (rapamycin) administered concomitantly with a subtherapeutic dose of cyclosporine in the treatment of severe psoriasis: a randomized controlled trial. Br J Dermatol. 2001;145:438.
53. Shihab FS, Bennett WM, Yi H, et al. Sirolimus increases transforming growth factor- beta1 expression and potentiates chronic cyclosporine nephrotoxicity. Kidney Int. 2004;65:1262.
54. Matas AJ, Kandaswamy R, Humar A, et al. Long-term immunosuppression, without maintenance prednisone, after kidney transplantation. Ann Surg. 2004;240:510.
55. Ulrich W, Schlederer MP, Buxbaum P, et al. The histopathologic identification of CMV infected cells in biopsies of human renal allografts. An evaluation of 100 transplant biopsies by in situ hybridization. Pathol Res Pract. 1986;1981:739.
56. Benoit G, Moukarzel M, Verdelli G, et al. Gastrointestinal complications in renal transplantation. Transplant Int. 1993;6:45.
57. Troppmann C, Papalois BE, Chiou A, et al. Incidence, complications, treatment, and outcome of ulcers of the upper gastrointestinal tract after renal transplantation during the cyclosporine era. J Am Coll Surg. 1995;180:433.
58. Gianello P, Squifflet JP, Pirson Y, et al. Gastroduodenal complications after transplantation. Clin Transplant. 1988;2:221.
59. Hadjiyannakis EJ, Evans DB, Smellie WAB, et al. Gastrointestinal complications after renal transplantation. Lancet. 1971;2:781.
60. Carson SD, Krom RAF, Uchida K, et al. Colon perforation after kidney transplantation. Ann Surg. 1978;188:109.
61. Fernandez-Cruz L, Targarona EM, Cugat E, et al. Acute pancreatitis after renal transplantation. Br J Surg. 1989;76:1132.
62. Kawanishi H, Rudolph E, Bull FE. Azathioprine-induced acute pancreatitis. N Engl J Med. 1973;289:357.
63. Fernandez-Cruz L, Targarona EM, Cugat E, et al. Acute pancreatitis after renal transplantation. Br J Surg. 1989;76:1132.
64. Vanrenterghem Y, Ponticelli C, Morales JM, et al. Prevalence and management of anemia in renal transplant recipients: a European survey. Am J Transplant. 2003;3:835.
65. First MR. Long-term complications after transplantation. Am J Kidney Dis. 1993;22:477.
66. Kirkman RL, Strom TB, Weir MR, et al. Late mortality and morbidity in recipients of long-term renal allografts. Transplantation. 1982;34:347.
67. Hill MN, Grossman RA, Feldman HI, et al. Changes in causes of death after renal transplantation, 1966 to 1987. Am J Kidney Dis. 1991;5:512.
68. Rao KV, Andersen RC. Long-term results and complications in renal transplant recipients: observations in the second decade. Transplantation. 1988;45:45.
69. Braun WE. Long-term complications of renal transplantation. Kidney Int. 1990;37:1363.
70. Kasiske BL. Risk factors for accelerated atherosclerosis in renal transplant recipients. Am J Med. 1988;84:985.
71. Braun WE, Marwick TH. Coronary artery disease in renal transplant recipients. Cleve Clin J Med. 1994;61:370.
72. Keown PA, Shackleton CR, Ferguson BM. Long-term mortality, morbidity, and rehabilitation in organ transplant recipients. In: Paul LC, Solez K, eds. Organ Transplantation: Long-Term Results. New York: Marcel Dekker; 1992:57.
73. Kasiske BL, Buijjaro C, Massy ZA, et al. Cardiovascular disease after renal transplantation. J Am Soc Nephrol. 1996;7:158.
74. Vanrenterghem Y, Roels L, Lerut T, et al. Long-term prognosis after cadaveric kidney transplantation. Transplant Proc. 1987;19:3762.
75. Brott T, Toole JF. Medical compared with surgical treatment of asymptomatic carotid artery stenosis. Ann Intern Med. 1995;123:720.
76. Ibels LS, Stewart JH, Mahony JF, et al. Deaths from occlusive arterial disease in renal allograft recipients. BMJ. 1974;3:552.
77. Gunnarsson R, Lofmark R, Nondlander R, et al. Acute myocardial infarction in renal transplant recipients: incidence and prognosis. Eur Heart J. 1984;5:218.
78. Held PJ, Port FK, Blagg CR, et al. Survival and mortality. Excerpts from United States Renal Data System 1990 Annual Report. Am J Kidney Dis. 1990;16(Suppl 2):44.
79. Luke RG. Pathophysiology and treatment of posttransplant hypertension. J Am Soc Nephrol. 1991;2(Suppl 1):S37.
80. Luke RG. Hypertension in renal transplant recipients. Kidney Int. 1987;31:1024.
81. Abdulmassih Z, Chevalier A, Bader C, et al. Role of lipid disturbances in the atherosclerosis of renal transplant patients. Clin Transplant. 1992;6:106.
82. Summary of the second report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel II). JAMA. 1993;269:3015.
83. Cattran DC, Steiner G, Wilson DR, et al. Hyperlipidemia after renal transplantation: natural history and pathophysiology. Ann Intern Med. 1979;91:554.
84. Vathsala A, Weinberg RB, Schoenberg L, et al. Lipid abnormalities in cyclosporine-prednisone-treated renal transplant recipients. Transplantation. 1989;48:37.
85. Kasiske BL, Umen AJ. Persistent hyperlipidemia in renal transplant recipients. Medicine. 1987;66:309.
86. Divaker D, Bailey RR, Frampton CM, et al. Hyperlipidemia in stable renal transplant recipients. Nephron. 1991;59:423.
87. Massy ZA, Kasiske BL. Post-transplant hyperlipidemia: mechanisms and management. J Am Soc Nephrol. 1996;7:971.
88. Duerke TB, Abdulmassih Z, Lacour B, et al. Atherosclerosis and lipid disorders after renal transplantation. Kidney Int. 1991;39:S24.
89. Raine AEG, Carter R, Mann JI, et al. Adverse effect of cyclosporin on plasma cholesterol in renal transplant recipients. Nephrol Dial Transplant. 1988;3:458.
90. Jung K, Neumann R, Scholz D, et al. Abnormalities in the composition of serum high density lipoprotein in renal transplant recipients. Clin Nephrol. 1982;17:191.
91. Averna MR, Barbagallo CM, Sparacino V, et al. Follow-up of lipid and apoprotein levels in renal transplant level in renal transplant recipients. Nephron. 1991;58:255.
92. Kasiske BL, Tortorice KL, Heim-Duthoy KL, et al. The adverse impact of cyclosporine on serum lipids in renal transplant recipients. Am J Kidney Dis. 1991;17:700.
93. Bittar AE, Ratcliffe PJ, Richardson AJ, et al. The prevalence of hyperlipidemia in renal transplant recipients associations with immunosuppressive and antihypertensive therapy. Transplantation. 1990;50:987.
94. Roth D, Milgrom M, Esquenazi V, et al. Posttransplant hyperglycemia increased incidence in cyclosporine-treated renal allograft recipients. Transplantation. 1989;47:278.
95. Sumrani NB, Delaney V, Ding Z, et al. Diabetes mellitus after renal transplantation in the cyclosporine era—an analysis of risk factors. Transplantation. 1991;51:343.
96. Jindal RM. Posttransplant diabetes mellitus—a review. Transplantation. 1994;58:1289.
97. Pirsch JD, Miller J, Deierhoi MH, et al., for the FK506 kidney transplant study group. A comparison of tacrolimus (FK506) and cyclosporine for immunosuppression after cadaveric renal transplantation. Transplantation. 1997;63:977.
98. US multicenter FK506 Liver Study Group. A comparison of tacrolimus (FK506) and cyclosporine for immunosuppression in liver transplantation. N Engl J Med. 1994;331:1110.
99. European FK506 Multicentre Liver Study Group. Randomised trial comparing tacrolimus (FK506) and cyclosporin in prevention of liver allograft rejection. Lancet. 1994;344:423.
100. Sumrani N, Delaney V, Ding Z, et al. Posttransplant diabetes mellitus in cyclosporine-treated renal transplant recipients. Transplant Proc. 1991;23:1249.
101. Koyama H, Cecka JM. Rejection episodes. Clin Transpl. 1992;391.
102. Peddi VR, First MR. Early posttransplant care of renal transplant recipients. Semin Dial. 1999;12:320.
103. Racusen LC, Solez K, Colvin RB, et al. The Banff 97 working classification of renal allograft pathology. Kidney Int. 1999;55:713–723.
104. Monaco AP, Burke JF Jr, Ferguson RM. Current thinking on chronic renal allograft rejection: issues, concerns, and recommendations from a 1997 round table discussion. Am J Kidney Dis. 1999;33:150.
105. Hernandez D, Rufino M, Armas S, et al. Retrospective analysis of surgical complications following cadaveric kidney transplantation in the modern transplant era. Nephrol Dial Transplant. 2006;10:2908.
106. Dalgic A, Boyvat F, Karakayali H, et al. Urologic complications in 1523 renal transplantations: the Baskent University experience. Transplant Proc. 2006;38:543.
107. Juaneda B, Alcaraz A, Buhons A, et al. Endourological management is better in early-onset ureteral stenosis in kidney transplant. Transplant Proc. 2005;37:3825.
108. Pisani F, Iaria G, D'Angelo M, et al. Urologic complications in kidney transplantation. Transplant Proc. 2005;37:2521.
109. Praz V, Leeisinger HJ, Pascual M, et al. Urological complications in renal transplantation from cadaveric donor grafts: a retrospective analysis of 20 years. Urol Int. 2005;75:144.
110. Osman Y, Shokeir A, Ali-el Dein B, et al. Vascular complications after live donor renal transplantation: study of risk factors and effects of graft and patient survival. J Urol. 2003;169:859.
111. Morrissey PE, Ramirez PJ, Gohh RY, et al. Management of thrombophilia in renal transplant patients. Am J Transplant. 2002;2:872.
112. Smyth GP, Beitz G, Eng MP, et al. Long-term outcome of cadaveric renal transplant after treatment of symptomatic lymphocele. J Urol. 2006;176:1069.
113. Atray NK, Moore F, Zaman F, et al. Post-transplant lymphocele: a single centre experience. Clin Transplant. 2004;18:46.
114. Bailey SH, Mone MC, Holman JM, et al. Laparoscopic treatment of post renal transplant lymphoceles. Surg Endosc. 2003;17:1896.
115. Yigit B, Aydin C, Titiz I, et al. Stone disease in kidney transplantation. Transplant Proc. 2004;36:187.
116. Penn I. Cancers complicating organ transplantation. N Engl J Med. 1990;323:1767.
117. Penn I. Tumors in the transplant. In: Jacobson HR, Striker GF, Klahr S, eds. The Principles and Practice of Nephrology. Philadelphia: Mosby; 1995:833.
118. Hanto DW. Polyclonal and monoclonal posttransplant lymphoproliferative diseases (PTLD). Clin Transpl. 1992;6:227.
119. Penn I. The changing pattern of posttransplant malignancies. Transplant Proc. 1991;23:1101.
120. Renoult E, Aymard B, Gregoire MJ, et al. Epstein-Barr virus lymphoproliferative disease of donor origin after kidney transplantation: a case report. Am J Kidney Dis. 1995;26:84.
121. Alfrey EJ, Friedman AL, Grossman RA, et al. Two distinct patterns of post-transplantation lymphoproliferative disorder (PTLD): early and late onset. Clin Transpl. 1992;6:246.
122. Penn I. Immunosuppression—a contributory factor in lymphoma formation. Clin Transpl. 1992;6:214.
123. Milpied N, Vasseur B, Parquet N, et al. Humanized anti-CD20 monoclonal antibody (rituximab) in post transplant lymphoproliferative disorder: a retrospective analysis on 32 patients. Ann Oncol. 2000;1(Suppl 1):113.
124. Faye A, Van Den Abeele T, Peuchmaur M, et al. Anti-CD20 monoclonal antibody for post-transplant lymphoproliferative disorders. Lancet. 1998;352:1285.