Karen Bordson
Carl P. Weiner
Immediate Concerns
Major Problems
Maternal mortality is defined as deaths occurring during pregnancy or within 6 weeks postpartum, with the cause of death identified as complications related to pregnancy, delivery, or the puerperium (International Classification of Diseases, 9th Revision, codes 630–676). It has decreased significantly over the past century, falling from 850 deaths per 100,000 deliveries in 1900 to 7.5 deaths per 100,000 in 1982 (1). This rate has remained stable at approximately 7.5 per 100,000 deliveries between 1982 and 1996. Hemorrhage and hypertensive disorders are the major contributors to maternal death rates (2). Hemorrhagic disorders can become life threatening and quickly challenge the obstetrician. Appropriate care requires an efficient plan with the understanding of the special complications associated with pregnancy and the gravid uterus. There are two main subtopics in this chapter that the reader needs to consider; these include placental complications (abruption and previa) and the HELLP syndrome (hemolysis, elevated liver enzymes, and low platelets)/disseminated intravascular coagulation (DIC).
As hepatic disorders in pregnancy can be devastating to both fetus and the pregnant patient, this chapter will address liver disorders related to pregnancy, specifically hyperemesis gravidarum, intrahepatic cholestasis of pregnancy, and acute fatty liver of pregnancy.
Stress Points
1. The physician must be aware of the potential hemorrhagic complications to which pregnancy predisposes the patient and fetus, and the physiologic and pathologic risk factors. Rapid diagnosis and treatment are critical to patient safety.
2. Liver disorders can vary from irritating and relatively minor, to life threatening with significant morbidity and mortality.
Hemorrhagic Concerns
Significant bleeding in pregnancy can be quantified by total amount, or by amount and time period over which the bleeding occurred (3,4). Generally, postpartum hemorrhage—defined by the total estimated blood loss—is established when there is greater than 500 mL for vaginal deliveries and more than 1 L for cesarean deliveries; additionally, clinical symptoms and signs with respect to the blood loss are considered in the management.
Coagulation Changes
In pregnancy, if factors are measured, one will note an increase in factors I (fibrinogen), VII, VIII, IX, and X. Functional tests, such as the prothrombin time (PT), partial thromboplastin time (PTT), and bleeding times (BT) should not change in a normal pregnancy.
The reader is asked to refer to Chapter 49 for more detailed description of essential physiologic concerns related to coagulation and Chapter 170 for coagulation disorders.
Placental Complications
Placental Abruption
Placental abruption (abruptio placentae) is a condition in which the placenta separates from the implantation site of the uterus prior to the delivery of the fetus. The area of hemorrhage along the decidua basalis expands as the bleeding progresses. This hematoma may be concealed or present clinically with vaginal bleeding. The underlying mechanism may be related to vascular damage caused by preeclampsia, trauma, cocaine/alcohol use, or chorioamnionitis. Risk factors for abruption include either maternal or paternal (secondhand) smoking, multiparity, prior caesarean delivery, and African American ethnicity (5,6). The incidence ranges between 0.4% and 0.8%, and there is a 15% recurrence rate for a subsequent pregnancy and a 20% recurrence rate for two previous episodes (7). Morbidity and mortality of both the mother and fetus can be significant with this process if the hemorrhage is significant.
Classic clinical manifestations include vaginal bleeding, abdominal pain/uterine irritability, and fetal heart rate abnormalities or fetal distress; of note, however, is that none or all of these symptoms may be present. Ultrasound has limited usefulness as it reveals a retroplacental blood clot in only 15% of cases, thus giving a high false-negative rate (5).
Treatment with fluid resuscitation, adequate oxygenation, and close fetal monitoring is critical. With evidence of significant hemorrhage or fetal distress, delivery must be expedited. It is critical to anticipate additional postpartum complications, such as uterine atony, to limit further hemorrhage.
Placenta Previa
Placental previa occurs with improper implantation of the placenta such that it overlies the internal os of the cervix during the third trimester. Traditionally, placenta previa was referenced with different classifications of previa and low-lying placentas. However, with current ultrasound capabilities, this classification scheme has limited utility.
|
|
|
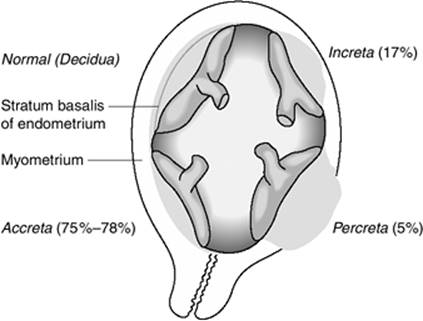
Figure 99.1. Placental implantation abnormalities (public domain image per http://en.wikipedia.org/wiki/Image:Placenta_accreta.png). |
The incidence of placenta previa is noted to be approximately 0.5% (8); however, with the increased rates of cesarean deliveries and advancing maternal age, there is concern regarding an increase in that incidence in the future (9). Risk factors include prior placenta previa, a history of cesarean delivery, a history of suction curettage, maternal age older than 35 years, African American or non-Caucasian ethnicity, and cigarette smoking.
Clinical symptoms include painless vaginal bleeding beginning in the second or third trimester. Ultrasound is then performed to confirm or rule out the diagnosis. Management is expectant unless maternal bleeding or fetal heart rate abnormalities/fetal distress necessitates imminent delivery via cesarean section. If the patient is stable—meaning no bleeding—and the fetal surveillance is reassuring, the patient is closely monitored on pelvic rest (nothing per vagina, no vaginal exam, no intercourse) until fetal lung maturity or 37 weeks' gestation, at which time a cesarean delivery is performed. Risks of placenta previa include other placental implantation abnormalities, such as placenta accreta, placenta increta, and placenta percreta (Fig. 99.1). The physician must be aware of these risks at the time of delivery and be prepared for a possible cesarean hysterectomy (hysterectomy performed at the time of the cesarean delivery) if necessary.
Hemolysis, Elevated Liver Enzymes, and Low Platelets (HELLP) Syndrome and Disseminated Intravascular Coagulation (DIC)
The topic of preeclampsia/eclampsia is discussed in Chapter 98, Cardiac Disease and Hypertensive Disorders in Pregnancy.
The acronym, HELLP, for the syndrome consisting of hemolysis, elevated liver enzymes, and low platelets, was first used by Weinstein in 1982 (10). The clinical entity was first noted by Pritchard et al. in 1954 (11). It is currently thought to be a distinct variant, rather than a progression, of the preeclampsia/eclampsia continuum. The incidence is rare, with Bhattacharya and Campbell (12) noting 13 cases of HELLP in a population of 4,188 patients with preeclampsia (310 per 100,000 patients). Although much speculated, the true cause is unclear. Older theories dealt with long-chain 3-hydroxyacyl-CoA (LCHAD) and other fatty acid oxidation defects. However, these have not been proven to be major risk factors in HELLP (13,14). Current research has found associations with genetic mutations of the Fas gene and regulation of the immune system (15,16). There are also studies regarding the prognostic values of hyaluronic acid (17) and serotonin (18) to evaluate liver function and platelet activation, respectively. Risk factors have been shown to include African Americans (19) and a history of prior pregnancy with HELLP. The recurrence rate has been reported as 14% (20).
HELLP is a disease with significant morbidity and mortality, both maternal and perinatal. In a prospective study of 442 pregnancies with HELLP, the risk of maternal death was found to be 1.1% (21). Significant maternal morbidity included DIC (21%), placental abruption (16%), acute renal failure (7.7%), pulmonary edema (6%), and rare occurrences of subcapsular liver hematoma and retinal detachment (22). Additionally, case reports of hepatic rupture (23,24,25,26) have been documented. Fetal outcome is typically related to the necessity to proceed with preterm delivery. Neonatal outcomes include risk of intensive care requirements, mechanical ventilation, sepsis, and intraventricular hemorrhage (27).
The clinical features and laboratory evaluation of HELLP have not been firmly defined. Generally, the findings reflect the disease process on the vascular supply of the maternal liver. The hemolysis can be noted by an abnormal peripheral smear, elevated serum bilirubin, low serum haptoglobin levels, elevated lactate dehydrogenase (LDH) of subtypes LDH1/LDH2, or a fall in the hemoglobin (22). Elevated liver enzymes, generally aspartate transaminases (AST), alanine transferase (ALT) and/or bilirubin, are present; however, there is no strict definition of the degree of elevation. There is also great variability in establishing the criteria for low platelets, varying from 150,000 to less than 50,000 cells/µL. Patients with HELLP also have altered vascular reactivity (28), and methods of prediction of HELLP by Doppler ultrasound have been examined, revealing a decrease in dual hepatic blood supply preceding the onset of HELLP (29,30). Objective parameters for DIC include prolonged prothrombin time (PT) and activated partial thromboplastin time (aPTT), elevated fibrinogen degradation products, and elevated D-dimers; as fibrinogen is increased in a normal pregnancy, the value in DIC may decrease to “normal” (nonpregnant) values, so it is not used as an objective parameter.
Treatment of HELLP includes supportive care in a facility suited for such high-level care. Prompt delivery of the fetus is indicated if the patient is beyond 34 gestational weeks, or sooner if the disease has progressed to multiorgan dysfunction, DIC, liver infarction or hemorrhage, renal failure, suspected placental abruption, or a nonreassuring fetal status (22).
There is more controversy regarding the recommendations if the pregnancy is less than 34 weeks' gestation and there are only mild to moderate laboratory abnormalities. Generally, expectant management and corticosteroids for fetal lung maturity are given with delivery after completion of the course of steroids. There is significant debate over use of steroids for treatment of the laboratory abnormalities of HELLP. Some studies have shown clinical benefit (31,32), whereas others, including a Cochrane Database review (33), find insufficient evidence of beneficial effect. This topic, among others, was specifically discussed at the 2004 Annual Meeting of the Society for Maternal-Fetal Medicine (34), with the conclusion that insufficient evidence of beneficial effect exists and there is a need for further studies. Additionally, the benefit of plasma exchange therapy has been shown to improve treatment outcome (35). Heparin therapy, however, is associated with further bleeding complications (36). Management of DIC must address the underlying cause (37); transfusion of both packed red cells and component therapy as indicated, as well as fluid replacement and oxygenation, are critical. There are investigations examining the role of solvent-detergent plasma (38) and aprotinin (39) in HELLP, the results of which appear safe and improve laboratory indices of coagulopathy.
Liver Concerns
Physiologic Changes Associated with Pregnancy
Pregnancy-related hormones and fetal enzymes significantly affect the maternal liver. Known changes in the liver profile reveal a decrease in serum albumin secondary to the dilutional effect of a 50% increase in maternal plasma volume. There is also an increase in serum alkaline phosphatase due to placental/fetal production. Markers of liver injury, such as aspartate aminotransferase, alanine aminotransferase, and lactate dehydrogenase, will not change in normal pregnancy. Bilirubin and gamma-glutamyl transpeptidase are both significantly lowered (40).
One of the main hormones causing alterations in hepatic physiology is estrogen. Estrogen produces an increase in the hepatic rough endoplasmic reticulum, which increases the production of proteins. The approximate sevenfold increase in estradiol—related to multiple factors, from changes in the binding hormones to changes in metabolism and production—in the first trimester and a further fivefold increase by term stimulates an approximate sixfold increase in the production of the sex hormone–binding globulin (41). Estrogen also has an inverse relationship with bile salt production and bile flow. There is a change in both composition of the bile and in the rate of cholesterol and phospholipid production; these changes produce an increased lithogenicity (42).
Progesterone, another hormone known to cause significant hepatic changes, mainly effects an increase of smooth endoplasmic reticulum and an increase in cytochrome P-450. Additionally, there is notable smooth muscle relaxation of the gallbladder and biliary ductal system. Progesterone can also produce slow wave dysrhythmia in the gastrointestinal tract (43).
It is now thought that there are genetic influences specifically related to MDR3 gene mutations in liver diseases in pregnancy. Refer to Chapter 48 for more detailed description of essential physiologic concerns related to the liver.
Hyperemesis Gravidarum
Hyperemesis gravidarum (HG) is a condition characterized by serious and persistent vomiting that limits fluid intake and adequate nutrition. Clinical manifestations include weight loss greater than 5% of prepregnancy weight, weakness, dehydration, ketosis, and muscle wasting. HG occurs in approximately 0.3% to 2.0% of pregnancies, seems to affect a diverse population with multiple risk factors, and can be associated with a range of outcomes. Studies have associated HG to various hormone levels, including those of human chorionic gonadotropin, estrogen (44), prolactin (45), thyroxine (46), androgens (46), cortisol (47), and maternal prostaglandins (48). Other factors identified included prior history of HG with previous pregnancies (49), female fetal gender (50,51), maternal age, maternal weight (52), and smoking (53). Helicobacter pylori may (54,55,56) or may not (57) have a role. Chronic medical conditions such as history of gastritis, allergies, and gallbladder disease (58) contribute to the risk. Additionally, the interpregnancy interval and paternity (50) have been examined; although the cause cannot be established, the relationship is being studied.
A complete differential diagnosis includes multiple systems; obstetric and gynecologic conditions such as a molar pregnancy, degenerating uterine leiomyoma, or ovarian torsion should be considered. Gastrointestinal causes could include gastroenteritis, gastroparesis, achalasia, biliary tract disease, hepatitis, intestinal obstruction, peptic ulcer disease, pancreatitis, and appendicitis. The patient needs to be evaluated for urinary tract conditions, including pyelonephritis, uremia, and kidney stones. Metabolic diseases, including hyperthyroidism, diabetic ketoacidosis, porphyria, and Addison disease, should be ruled out. Neurologic disorders, drug reactions, and psychiatric conditions are other considerations.
Some studies have found HG to be protective against adverse outcomes (59), whereas more recent studies have failed to prove this relationship (60). Current research shows a relationship between HG and low birth weight that is mostly attributed to poor maternal weight gain (61,62,63). In addition to potentially compromised fetal outcomes, a worsened maternal morbidity and mortality are also noted. Cases of Wernicke encephalopathy (64,65,66,67), central pontine myelinolysis (68,69,70), severe liver injury (71), splenic avulsion (72), pneumomediastinum following esophageal rupture (73), and acute renal failure (74) have been reported.
Treatment for HG is primarily supportive, with antiemetics, fluid therapy, and electrolyte replacement. Natural remedies such as pyridoxine (vitamin B6) and ginger (75) have been shown to be effective. Additionally, behavior modification with avoidance of strong odors/scents and adjustment of diet may be tried. However, if these measures are inadequate, hospitalization and treatment with steroids (76,77,78) and parenteral nutrition may be necessary.
Intrahepatic Cholestasis of Pregnancy
Intrahepatic cholestasis of pregnancy (ICP) is the most frequent of the pregnancy-related liver diseases (79), occurring in approximately 1% of pregnancies (80). It is a condition characterized by the progressive pruritus of cholestasis, with elevated fasting bile salts—specifically chenodeoxycholic acid, deoxycholic acid, and cholic acid elevations more than 10 µmol/L—and elevated aminotransferases (81). Clinical manifestations begin in the late second or third trimester and most often will resolve spontaneously within 2 to 3 weeks postpartum. Although the direct cause is unknown, research has shown a strong familial component. Nonetheless, ICP affects specific populations at different rates. For example, ICP occurs in less than 0.2% of pregnancies in women of North American and Central/Western European descent, whereas Scandinavian and Baltic populations show a rate of 1% to 2%, and Chilean and Bolivian populations have shown rates of 5% to 15% (80). The severe form of ICP—bile acid levels more than 40 µmol/L—in the Swedish population is associated with a frame shift mutation in the gene coding for the ATP binding cassette transporter, specifically the ABCB4_5 gene variant (formerly known as multidrug resistance gene 3, MDR3) (82,83,84). Mutations in the bile salt export pump (BSEP) can also predispose a patient to ICP (85). Other possible causes relate to “leaky gut” theories (86). This theory is based on the increased absorption of bacterial endotoxins and the enterohepatic circulation of cholestatic metabolites of sex hormones and bile salts. Research has also shown an association with low maternal serum estrogen (87,88).
Fetal complication rates are directly related to maternal serum bile acids (89). Bile acid levels greater than 40 µmol/L are associated with preterm delivery, fetal asphyxial events, and meconium staining (90). Additionally, case reports of neonatal respiratory distress syndrome (90) and fetal death (91) are noted; on the other hand, maternal morbidity and mortality are low.
Supportive measures for pruritus with antihistamine is inadequate, as it has limited effectiveness and fails to address the bile acid elevation and fetal concerns. Cholestyramine, S-adenosylmethionine, and dexamethasone were the treatments of choice (92). However, newer research is advocating the use of ursodeoxycholic acid (UDCA), which is a tertiary bile acid. Initial use of UDCA was with bear bile in traditional Chinese medicine for the treatment of liver disease (93). Recent research has shown UDCA to be more effective in reducing bile acids and bilirubin (94,95,96,97). Fetal risks are decreased, but not eliminated. Because of this, careful fetal monitoring and delivery at fetal lung maturity should be considered (92). Ondansetron is also being evaluated as a treatment for pruritus; however, no data are noted on fetal benefits of that antiemetic (98).
Acute Fatty Liver Disease of Pregnancy
Acute fatty liver disease of pregnancy (AFLP) is a rare but potentially fatal disease that occurs in the third trimester. Mean gestational ages vary between 34.5 weeks' (99,100) and 37 weeks' gestation (101). Incidence has been documented as 1 in 6,659 births (102) to 1 in 15,900 births (102). It is characterized by significant malaise, nausea/vomiting, anorexia, abdominal pain, and jaundice (103). Clinical signs include hypertension, jaundice, elevated serum transaminases, coagulopathies, thrombocytopenia, and hypoglycemia. A high index of suspicion should be maintained if evidence of these signs and symptoms are noted (104). Imaging studies are often performed but have limited usefulness in making the diagnosis; ultrasound may show nonspecific changes (104). Computerized tomography (CT) has a high false-negative rate (100). Liver biopsy is the gold standard in confirming the diagnosis; however, it is rarely necessary and carries significant maternal risk in the setting of disseminated intravascular coagulation (DIC).
This disease is noted to have significant risks with respect to morbidity and mortality. Older research reported maternal and perinatal mortality rates as high as 75% and 85%, respectively (104). Although the maternal mortality rate has fallen significantly, fetal mortality has remained as high as 66% (101). Maternal morbidity includes coagulopathies (specifically DIC) (105), hepatic encephalopathy (100), respiratory compromise (pulmonary edema or respiratory arrest) (100), and renal insufficiency (102). Current research has found an associated genetic component with mitochondrial trifunctional protein mutations (106,107).
Treatment of this disease is supportive, with management in a higher-level setting, specifically an ICU. Delivery is recommended as efficiently as possible. Debates regarding prolonged inductions and surgical risks of cesarean are common. The decision should be individualized, and should include the patient and her family. Hypoglycemia should be treated with dextrose-containing solutions. Elevated ammonia levels can be decreased with neomycin. Blood transfusions and replacement of clotting factors should be considered as appropriate. AFLP generally resolves within 2 to 3 days postpartum; however, cases of fulminant hepatic failure requiring liver transplantation have been reported (108).
References
1. Chang J, Elam-Evan LD, Berg CJ, et al. Pregnancy-related mortality surveillance—United States, 1991–1999. MMWR Surveill Summ. 2003;52:1–8.
2. Kahn KS, Wojdyla D, Say L, et al. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367:1066–1074.
3. Sobieszczyk K, Breborowicz G. Management recommendations for postpartum hemorrhage. Arch Perinat Med. 2004;10:1–4.
4. Macphail S, Talks K. Massive post-partum haemorrhage and management of disseminated intravascular coagulation. Curr Obst Gynaecol. 2004;14:123–131.
5. Tikkanen M, Nuutila M, Hiilesmaa V, et al. Clinical presentation and risk factors of placental abruption. Acta Obstet Gynecol Scand. 2006;85:700–705.
6. Getahun D, Oyelese Y, Salihu HM, et al. Previous cesarean delivery and risks of placenta previa and placental abruption. Obstet Gynecol. 2006;107:771–778.
7. Rasmussen S, Irgens LM, Dalaker K. The effect on the likelihood of further pregnancy of placental abruption and the rate of its recurrence. Br J Obstet Gynaecol. 1997;104:1292–1295.
8. Iyasu S, Saftlas AK, Rowley DL, et al. The epidemiology of placenta previa in the United States, 1979 through 1987. Am J Obstet Gynecol. 1993;168:1424–1429.
9. Oyelese Y, Smulian JC. Placenta previa, placenta accreta, and vasa previa. Obstet Gynecol. 2006;107:927–941.
10. Weinstein L. Syndrome of hemolysis, elevated liver enzymes, and low platelet count: a severe consequence of hypertension in pregnancy. Am. J Obstet. Gynecol. 1982;142(2):159–167.
11. Pritchard JA, Weisman R Jr, Ratnoff OD, et al. Intravascular hemolysis, thrombocytopenia, and other hematologic abnormalities associated with severe toxemia of pregnancy. N Engl J Med. 1954;250:89–98.
12. Bhattacharya S, Campbell DM. The incidence of severe complications of preeclmpsia. Hypertens Pregnancy. 2005;24:181–190.
13. Holub M, Bodamer OA, Item C, et al. Lack of correlation between fatty acid oxidation disorders and haemolysis, elevated liver enzymes, low platelets (HELLP) syndrome? Acta Paediatr. 2005;94:48–52.
14. den Boer ME, Iilist L, Wiiburg FA, et al. Heterozygosity for the common LCHAD mutation (1528g>C) is not a major cause of HELLP syndrome and the prevalence of the mutation in the Dutch population is low. Pediatr Res. 2000;48:151–154.
15. Sziller I, Hupuczi P, Normand N, et al. Fas (TNFRSF6) gene polymorphism in pregnant women with hemolysis, elevated liver enzymes and low platelets and in their neonates. Obstet Gynecol. 2006;107:582–587.
16. Harirah H, Donia S, Hsu CD. Serum soluble Fas in the syndrome of hemolysis, elevated liver enzymes and low platelets. Obstet Gynecol. 2001;98:295–298.
17. Osmers RG, Schutz E, Diedrich F, et al. Increased serum levels of hyaluronic acid in pregnancies complicated by preeclampsia or hemolysis, elevated liver enzymes and low platelets syndrome. Am J Obstet Gynecol. 1998;178:341–3345.
18. Backe J, Bussen S, Steck T. Significant decrease of maternal serum serotonin levels in singleton pregnancies complicated by the HELLP syndrome. Gynecol Endocrinol. 1997;11:405–409.
19. Haddad B, Barton JR, Livingston JC, et al. Risk factors for adverse maternal outcomes among women with HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome. Am J Obstet Gynecol. 2000;183:444–448.
20. Hupuczi P, Rigo B, Sziller I, et al. Follow-up analysis of pregnancies complicated by HELLP syndrome. Fetal Diagn Ther. 2006;21:519–522.
21. Sibai BM. Diagnosis, controversies and management of the syndrome of hemolysis, elevated liver enzymes and low platelet count. Obstet Gynecol. 2004;103:981–991.
22. Sibai BM, Ramadan MK, Usta I, et al. Maternal morbidity and mortality in 442 pregnancies with hemolysis, elevated liver enzymes and low platelets (HELLP syndrome). Am J Obstet Gynecol. 1993;169:1000–1006.
23. Hafeez M, Hameed S. HELLP syndrome and subcapsular liver haematoma. J Coll Physicians Surg Pak. 2005;15:733–735.
24. Herring CS, Heywood SG, Hatjis CG. The multiple challenges in the management of a patient with HELLP syndrome, liver rupture and eclampsia. W V Med J. 2005;101:261–262.
25. Shrivastava VK, Imagawa D, Wing DA. Argon beam coagulator for treatment of hepatic rupture with hemolysis, elevated liver enzymes, low platelets (HELLP) syndrome. Obstet Gynecol. 2006;107:525–526.
26. Araujo AC, Leao MD, Nobrega MH, et al. Characteristics and treatment of hepatic rupture caused by HELLP syndrome. Am J Obstet Gynecol. 2006;195:129–133.
27. Kim HY, Sohn YS, Lim JH, et al. Neonatal outcome after preterm delivery in HELLP syndrome. Yonsei Med J. 2006;47:393–398.
28. Fischer T, Schneider MP, Schobel HP, et al. Vascular reactivity in patients with preeclampsia and HELLP (hemolysis, elevated liver enzymes and low platelet count) syndrome. Am J Obstet Gynecol. 2000;183:1489–1494.
29. Oosterhof H, Voorhoeve PG, Aarnoudse JG. Enhancement of hepatic artery resistance to blood flow in preeclampsia in presence or absence of HELLP syndrome (hemolysis, elevated liver enzymes, and low platelets). Am J Obstet Gynecol. 1994;171:526–530.
30. Kawabata I, Nakai A, Takeshita T. Prediction of HELLP syndrome with assessment of maternal dual hepatic blood supply by using Doppler ultrasound. Arch Gynecol. Obstet. 2006;274:303–309.
31. van Runnard Heimel PJ, Huisjes AJ, Franx A, et al. A randomized placebo-controlled trial of prolonged prednisolone administration to patients with HELLP syndrome remote from term. Eur J Obstet Gynecol Reprod Biol. 2006;128:187–193.
32. Rose CH, Tigpen BD, Bofill JA, et al. Obstetric implications of antepartum corticosteroid therapy for HELLP syndrome. Obstet Gynecol. 2004;104:10011–10014.
33. Matchaba P, Moodley J. Corticosteroids for HELLP syndrome in pregnancy. Cochrane Database Syst Rev. 2004;(1):CD002076.
34. Norwitz ER, Bahtiyar MO, Sibai BM. Defining standards of care in maternal-fetal medicine. Am J Obstet Gynecol. 2004;191:1491–1496.
35. Eser B, Guven M, Unal A, et al. The role of plasma exchange in HELLP syndrome. Clin Appl Thromb Hemost. 2005;11:211–217.
36. Detti L, Mecacci F, Piccioli A, et al. Postpartum heparin therapy for patients with the syndrome of hemolysis, elevated liver enzymes and low platelets (HELLP) is associated with significant hemorrhagic complications. J Perinatol. 2005;25:236–240.
37. Labelle CA, Kitchens CS. Disseminated intravascular coagulation: treat the cause, not the lab values. Cleve Clin J Med. 2005;72:377–378.
38. Chekrizova V, Murphy WG. Solvent-detergent plasma: use in neonatal patients, in adults and paedriatric patients with liver disease and in obstetric and gynaecological emergencies. Transfus Med. 2006;16:85–91.
39. Stroup J, Haraway D, Beal JM. Aprotinin in the management of coagulopathy associated with amniotic fluid embolus. Pharmacotherapy. 2006;26:689–693.
40. Bacq Y, Zarka O, Brechot J, et al. Liver function tests in normal pregnancy: a prospective study of 103 pregnant women and 103 matched controls. Hepatology. 1996;23:1030–1034.
41. O'Leary P, Boyne P, Flett P, et al. Longitudinal assessment of changes in reproductive hormones during Nnormal pregnancy. Clin Chem. 1991;37:667–672.
42. Lynn J, Williams L, O'Brien J, et al. Effects of estrogen upon bile: implications with respect to gallstone formation. Ann Surg. 1973;178:514–522.
43. Walsh JW, Hasler WL, Nugent CE, et al. Progesterone and estrogen are potential mediators of gastric slow-wave dysrhythmias in nausea of pregnancy. Am J Physiol. 1996;270:506–514.
44. Lagiou P, Tamimi R, Mucci L, et al. Nausea and vomiting in pregnancy in relation to prolactin, estrogens and progesterone: a prospective study. Obstet Gynecol. 2003;101:639–644.
45. Panesar NS, Li CY, Rogers MS. Are thyroid hormones or hCG responsible for hyperemesis gravidarum? A matched paired study in pregnant Chinese women. Acta Obstet Gynecol Scand. 2001;80:519–524.
46. Carlsen SM, Vanky E, Jacobsen G. Nausea and vomiting associated with increasing maternal androgen levels in otherwise uncomplicated pregnancies. Acta Obstet Gynecol Scand. 2003;82:225–228.
47. Jarnfelt-Samsio A. Nausea and vomiting in pregnancy: a review. Obstet Gynecol Surv. 1987;42:422–427.
48. Gadsby R, Barnie-Adshead A, Grammatoppoulos D, et al. Nausea and vomiting in pregnancy: an association between symptoms and maternal prostaglandin E2. Gynecol Obstet Invest. 2000;50:149–152.
49. Trogstad LI, Stoltenberg C, Magnus P, et al. Recurrent risk in hyperemesis gravidarum. BJOG. 2005;112:1641–1645.
50. del Mar Melero-Montes M, Jick H. Hyperemesis gravidarum and the sex of offspring. Epidemiology. 2001;12:123–124.
51. Schiff MA, Reed SD, Daling JR. The sex ratio of pregnancies complicated by hospitalization for hyperemesis gravidarum. BJOG. 2004;111:27–30.
52. Depue RH, Bernstein L, Ross RK, et al. Hyperemesis gravidarum in relation to estradiol levels, pregnancy outcomes and other maternal factors: a seroepidemiologic study. Am J Obstet Gynecol. 1987;156:1137–1141.
53. Zhang J, Cai WW. Severe vomiting during pregnancy: antenatal correlated and fetal outcomes. Epidemiology. 1991;2:454–457.
54. Kuscu NK, Koyuncu F. Hyperemesis gravidarum: current concepts and management. Postgrad Med J. 2002;78:76–79.
55. Lee RH, Pan VL, Wing DA. The prevalence of Helicobacter pylori in the Hispanic population affected by hyperemesis gravidarum. Am J Obstet Gynecol. 2005;193:1024–1027.
56. Verberg MF, Gillott D, Al-Fardan N, et al. Hyperemesis gravidarum, a literature review. Hum Reprod Update. 2005;11:527–539.
57. Jacobson GF, Autry AM, Somer-Shely TL, et al. Helicobacter pylori seropositivity and hyperemesis gravidarum. J Reprod Med. 2003;48:578–582.
58. Jarnfelt-Samsioe A, Samsioe G, Velinder GM. Nausea and vomiting in pregnancy—a contribution to epidemiology. Gynecol Obstet Invest. 1983;16:221–229.
59. Weigel RM, Weigel MM. Nausea and vomiting of early pregnancy and pregnancy outcome: a meta-analytical review. Br J Obstet Gynaecol. 1989;96:1312–1318.
60. Weigel MM, Reyes M, Caiza ME, et al. Is the nausea and vomiting of early pregnancy really feto-protective? J Perinat Med. 2006;34:115–122.
61. Bailit JL. Hyperemesis gravidarum: epidemiologic finding from a large cohort. Am J Obstet Gynecol. 2005;193:811–814.
62. Dodds L, Fell D, Joseph KS, et al. Outcomes of pregnancies complicated by hyperemesis gravidarum. Obstet Gynecol. 2006;107:285–292.
63. Fell DB, Dodds L, Joseph KS, et al. Risk factors for hyperemesis gravidarum requiring hospital admission during pregnancy. Obstet Gynecol. 2006;107:2477–1384.
64. Chiossi G, Neri I, Cavazzuti M, et al. Hyperemesis gravidarum complicated by Wernicke encephalopathy: background, case report, and review of the literature. Obstet Gynecol Surv. 2006;61:255–268.
65. Rastenvte D, Obelieniene D, Kondrackiene J, et al. Wernicke's encephalopathy induced by hyperemesis gravidarum (case report). Meicina (Kaunas). 2003;39:56–61.
66. Indraccolo U, Gentile G, Pomili G, et al. Thiamine deficiency and beriberi features in a patient with hyperemesis gravidarum. Nutrition. 2005;21:967–968.
67. Togay-Isikay C, Yigit A, Mutluer N. Wernicke's encephalopathy due to hyperemesis gravidarum—an under-recognized condition. Aust N Z J Obstet Gynaecol. 2001;41:453–456.
68. Tonelli J, Zurru MC, Castillo J, et al. Central pontine myelinolysis induced by hyperemesis gravidarum. Medicina (B Aires). 1999;59:176–178.
69. Burneo J, Vizcarra D, Miranda H. Central pontine myelinolysis and pregnancy: a case report and review of literature. Rev Neurol. 2000;30:1036–1040.
70. Valiulis B, Kelley RE, Hardiasudarma M, et al. Magnetic resonance imaging detection of a lesion compatible with central pontine myelinolysis in a pregnant patient with recurrent vomiting and confusion. J Neuroimaging. 2001;11:441–443.
71. Vitoratos N, Bottsis D, Detsis G, et al. Severe liver injury due to hyperemesis gravidarum. J Obstet Gynaecol. 2006;26:172–173.
72. Nguyen N, Deitel M, Lacy E. Splenic avulsion in a pregnant patient with vomiting. Can J Surg. 1995;38:464–465.
73. Liang SG, Ooka F, Santo A, et al. Pneumomediastinum following esophageal rupture associated with hyperemesis gravidarum. J Obstet Gynaecol Res. 2002;28:172–175.
74. Hill JB, Yost NP, Wendel GD Jr. Acute renal failure in association with severe hyperemesis gravidarum. Obstet Gynecol. 2002;100:1119–1121.
75. Jewell D, Young G. Interventions for nausea and vomiting in early pregnancy. Cochrane Database Syst Rev. 2003;(4):CD 000145.
76. Moran P, Taylor R. Management of hyperemesis gravidarum: the importance of weight loss as a criterion for steroid therapy. Q J Med. 2002;95:153–158.
77. Nelson-Piercy C, Fayers P, de Swiet M. Randomised, double blind, placebo-controlled trial of corticosteroids for the treatment of hyperemesis gravidarum. BJOG. 2001;108:9–15.
78. Bondok RS, El Sharnouby NM, Eid HE, et al. Pulsed steroid therapy is an effective treatment for intractable hyperemesis gravidarum. Crit Care Med. 2006;34:2781–2783.
79. Lammert F, Marschall H, Glantz A, et al. Intrahepatic cholestasis of pregnancy: molecular pathogenesis, diagnosis and management. J Hepatol. 2000;33:1012–1021.
80. Ropponen A, Sund F, Riikonen S, et al. Intrahepatic cholestasis of pregnancy as an indicator of liver and biliary diseases: a population-based study. Hepatology. 2006;43:723–728.
81. Beuers U, Pusl T. Intrahepatic cholestasis of pregnancy—a heterogeneous group of pregnancy-related disorders? Hepatology. 2006;43:647–649.
82. Dixon PH, Weerasekera N, Linton KJ, et al. Heterozygous MDR3 missense mutation associated with intrahepatic cholestasis of pregnancy: evidence for a defect in protein trafficking. Hum Mol Genet. 2000;9:1209–1217.
83. Floreani A, Carderi I, Paternoster D, et al. Intrahepatic cholestasis of pregnancy: three novel MDR3 gene mutations. Aliment Pharmacol Ther. 2006;23:1649–1653.
84. Wasmuth H, Glantz A, Keppeler H, et al. Intrahepatic cholestasis of pregnancy: the severe form is associated with common variants of the hepatobiliary phospholipids transporter gene ABCB4. Gut. 2007;56(2):265–279. Epub 2006 Aug 4.
85. Kubitz R, Keitel V, Scheuring S, et al. Benign recurrent intrahepatic cholestasis associated with mutations of the bile salt export pump. J Clin Gastroenterol. 2006;40:81–85.
86. Reyes H, Zapata R, Hernandez I, et al. Is a leaky gut involved in the pathogenesis of intrahepatic cholestasis of pregnancy? Hepatology. 2006;43:715–722.
87. Reyes H, Simon FR. Intrahepatic cholestasis of pregnancy: an estrogen-related disease. Semin Liver Dis. 1993;13:289–301.
88. Leslie K, Reznikov L, Simon F, et al. Estrogens in intrahepatic cholestasis of pregnancy. Obstet Gynecol. 2000;95:372–376.
89. Glantz A, Marschall HU, Mattsson LA. Intrahepatic cholestasis of pregnancy: relationships between bile acid levels and fetal complication rates. Hepatology. 2004;40:467–474.
90. Zeeca E, De Luca D, Marras M, et al. Intrahepatic cholestasis of pregnancy and neonatal respiratory distress syndrome. Pediatrics. 2006;117:1669–1672.
91. Sentilhes L, Verspyck E, Pia P, et al. Fetal death in a patient with intrahepatic cholestasis of pregnancy. Obstet Gynecol. 2006;107:458–460.
92. Lammert F, Marschall HU, Matern S. Intrahepatic cholestasis of pregnancy. Curr Treat Options Gastroenterol. 2003;6:123–132.
93. Hagey L, Crombie D, Espinosa E, et al. Ursodeoxycholic acid in the Ursidae: biliary bile acid of bears, pandas, and related carnivores. J Lipid Res. 1993;34:1911–1917.
94. Brites D. Intrahepatic cholestasis of pregnancy: changes in maternal-fetal bile acid balance and improvement by ursodeoxycholic acid. Ann Hepatol. 2002;1:20–28.
95. Copaci I, Micu L, Iliescu L, et al. New therapeutical indications of ursodeoxycholic acid. Rom J Gastroent. 2005;14:259–266.
96. Glantz A, Marschall H, Lammert F, et al. Intrahepatic cholestasis of pregnancy: a randomized controlled trial comparing dexamethasone and ursodeoxycholic acid. Hepatology. 2005;42:1399–1405.
97. Zapata R, Sandoval L, Palma J, et al. Ursodeoxycholic acid in the treatment of intrahepatic cholestasis of pregnancy. A 12-year experience. Liver Int. 2005;25:548–554.
98. Schumann R, Hudcova J. Cholestasis of pregnancy, pruritus and 5-hydroxytryptamine 3 receptor antagonist. Acta Obstet Gynecol Scand. 2004;83:861–862.
99. Usta IM, Barton JR, Amon EA, et al. Acute fatty liver of pregnancy: an experience in the diagnosis and management of fourteen cases. Am J Obstet Gnecol. 1994;171:1342–1347.
100. Mjahed K, Charra B, Hamoudi D, et al. Acute fatty liver of pregnancy. Arch Gynecol Obstet. 2006;274(6):349–353. Epub 2006 Jul 26.
101. Castro MA, Fassett MJ, Reynolds TB, et al. Reversible peripartum liver failure: a new perspective on the diagnosis, treatment and cause of acute fatty liver of pregnancy, based on 28 consecutive cases. Am J Obstet Gynecol. 1999;181:389–395.
102. Reyes H, Sandoval L, Wainstein A, et al. Acute fatty liver of pregnancy: a clinical study of 12 episodes in 11 patients. Gut. 1994;35:101–106.
103. Bacq Y. Acute fatty liver of pregnancy. Semin Perinatol. 1998;22:134–140.
104. Kaplan MM. Acute fatty liver of pregnancy. N Engl J Med. 1985;313:367–370.
105. Yucesoy G, Ozkan SO, Bodur H, et al. Acute fatty liver of pregnancy complicated with disseminated intravascular coagulation and haemorrhage: a case report. Int J Clin Pract Suppl. 2005;147:82–84.
106. Isaaca J, Sims H, Powell C, et al. Maternal acute fatty liver of pregnancy associated with fetal trifunctional protein deficiency: molecular characterization of a novel maternal mutant allele. Ped Res. 1996;40:393–398.
107. Blish KR, Ibdah JA. Maternal heterozygosity for a mitochondrial trifunctional protein mutation as a cause for liver disease in pregnancy. Med Hypotheseses. 2005;64:96–100.
108. Ockner SA, Brunt EM, Cohn SM, et al. Fulminant hepatic failure caused by acute fatty liver of pregnancy treated by orthotopic liver transplant. Hepatology. 1990;11:59–64.