Juliana Chan
LEARNING OBJECTIVES
Upon completion of the chapter, the reader will be able to:
1. Differentiate the five types of viral hepatitides by their epidemiology, etiology, pathophysiology, clinical presentation, and natural history.
2. Identify modes of transmission and risk factors among the major types of viral hepatitis.
3. Evaluate hepatic serologies to understand how the type of hepatitis is diagnosed.
4. Create treatment goals for a patient with viral hepatitis.
5. Recommend an appropriate pharmacotherapy for prevention of viral hepatitis.
6. Develop a pharmaceutical care plan for treatment of viral hepatitis.
7. Formulate a monitoring plan to assess adverse effects of pharmacotherapy for viral hepatitis.
KEY CONCEPTS
![]() Prevention and treatment of viral hepatitis may prevent progression to chronic hepatitis, cirrhosis, end-stage liver disease, and hepatocellular carcinoma.
Prevention and treatment of viral hepatitis may prevent progression to chronic hepatitis, cirrhosis, end-stage liver disease, and hepatocellular carcinoma.
![]() Acute viral hepatitis A, B, C, D, and E are primarily managed with supportive care.
Acute viral hepatitis A, B, C, D, and E are primarily managed with supportive care.
![]() Good personal hygiene and proper disposal of sanitary waste are required to prevent fecal–oral transmission of the hepatitis A and E virus.
Good personal hygiene and proper disposal of sanitary waste are required to prevent fecal–oral transmission of the hepatitis A and E virus.
![]() Individuals may minimize their risk of acquiring both hepatitis B and C infection by avoiding contaminated blood products and not indulging in high-risk behavior such as IV drug use.
Individuals may minimize their risk of acquiring both hepatitis B and C infection by avoiding contaminated blood products and not indulging in high-risk behavior such as IV drug use.
![]() Persons at high risk of acquiring the hepatitis B virus (HBV) should be vaccinated with the hepatitis B vaccine at months 0, 1, and 6.
Persons at high risk of acquiring the hepatitis B virus (HBV) should be vaccinated with the hepatitis B vaccine at months 0, 1, and 6.
![]() A vaccine that combines both inactivated hepatitis A and recombinant hepatitis B (Twinrix) is approved for immunizing individuals more than 18 years of age with indications for both hepatitis A and B vaccines.
A vaccine that combines both inactivated hepatitis A and recombinant hepatitis B (Twinrix) is approved for immunizing individuals more than 18 years of age with indications for both hepatitis A and B vaccines.
![]() The drug of choice for chronic hepatitis B depends on the patient’s past medical history, alanine aminotransferase (ALT) level, HBV DNA level, HBeAg status, severity of liver disease, and history of previous HBV therapy.
The drug of choice for chronic hepatitis B depends on the patient’s past medical history, alanine aminotransferase (ALT) level, HBV DNA level, HBeAg status, severity of liver disease, and history of previous HBV therapy.
![]() Hepatitis D infection is possible only if the patient also has the hepatitis B virus; therefore, hepatitis B vaccination can indirectly prevent hepatitis D infection.
Hepatitis D infection is possible only if the patient also has the hepatitis B virus; therefore, hepatitis B vaccination can indirectly prevent hepatitis D infection.
INTRODUCTION
There are five types of viral hepatitis: hepatitis A (HAV), B (HBV), C (HCV), D (HDV), and E (HEV). Acute hepatitis may be associated with all five types of hepatitis and rarely exceeds 6 months in duration. Chronic hepatitis (disease lasting longer than 6 months) is usually associated with hepatitis B, C, and D.
![]() Chronic viral hepatitis may lead to the development of cirrhosis, which may lead to end-stage liver disease (ESLD) and hepatocellular carcinoma (HCC). Complications of ESLD include ascites, edema, hepatic encephalopathy, infections (e.g., spontaneous bacterial peritonitis), hepatorenal syndrome, and bleeding esophageal varices. Therefore, prevention and treatment of viral hepatitis may prevent ESLD and HCC.
Chronic viral hepatitis may lead to the development of cirrhosis, which may lead to end-stage liver disease (ESLD) and hepatocellular carcinoma (HCC). Complications of ESLD include ascites, edema, hepatic encephalopathy, infections (e.g., spontaneous bacterial peritonitis), hepatorenal syndrome, and bleeding esophageal varices. Therefore, prevention and treatment of viral hepatitis may prevent ESLD and HCC.
Viral hepatitis can occur at any age and is the most common cause of liver disease in the world. The true prevalence and incidence may be under-reported because most patients are asymptomatic. The epidemiology, etiology, and pathogenesis vary depending on the type of hepatitis and are considered separately below.
EPIDEMIOLOGY AND ETIOLOGY
Hepatitis A
Hepatitis A affects 1.4 million people yearly worldwide.1 The prevalence is highest in underdeveloped countries including Africa, parts of South America, the Middle East, and Southeast Asia. Australia, parts of western and northern Europe, Japan, and the United States have a lower prevalence. This is primarily due to vaccination programs, but outbreaks still can happen as evidenced by an outbreak in Pennsylvania in 2003.2,3 The number of infections and hospitalizations due to HAV infection annually have decreased markedly since the introduction of the hepatitis A vaccine in 1996.4,5
Table 24–1 Risk Factors for Acquiring Viral Hepatitis
|
Hepatitis A |
|
International travelers to endemic areas (e.g., Africa, Asia, and parts of South America) |
|
Sexual contact with infected persons (e.g., men having sex with other men) |
|
Shellfish infected with HAV (e.g., raw oysters) |
|
Day-care centers or household contacts with people infected with HAV |
|
Health care workers |
|
IV drug users using unsterilized needles |
|
Workers involved with nonhuman primates |
|
Food service handlers Patients with clotting factor disorders |
|
Individuals residing in health care institutions |
|
Hepatitis B and D |
|
Men having sex with other men |
|
Individuals with multiple heterosexual partners |
|
IV drug users using unsterilized needles |
|
Recipients of blood products |
|
Household contacts with acute hepatitis B with open cuts |
|
Health care providers in contact with contaminated needles |
|
Patients undergoing dialysis |
|
Hepatitis C |
|
Recipients of blood products |
|
Health care providers in contact with infected needles |
|
Individuals having multiple sexual partners |
|
Perinatal transmission (less than 5%) |
|
Unprofessional body piercing and tattooing |
|
Hepatitis E |
|
International travelers to endemic areas (e.g., parts of Asia, Africa, and Mexico) |
|
Ingesting foods and drinks contaminated with bodily waste |
HAV is primarily detected in contaminated feces and infects people via the fecal-oral route.4,6 Outbreaks occur primarily in areas of poor sanitation.1,4,5 Individuals at greatest risk of acquiring HAV are listed in Table 24–1.4,7Approximately 50% of the reported cases have no identifiable risk factors.4
To date, there are no documented cases of chronic hepatitis A.1,4 Death associated with HAV is rare and is mostly associated with fulminant hepatitis, with which approximately 100 people die annually.4
Hepatitis B
Hepatitis B is a bloodborne infection affecting more than 2 billion people worldwide.8 Approximately 400 million people have chronic infection, which may lead to cirrhosis and complications of ESLD.8There are 500,000 to 700,000 deaths annually due to hepatitis B.9 Despite having an effective vaccine against HBV, more than 300,000 newly diagnosed infections emerge each year. Fewer than 1% of individuals in North America and western Europe are chronically infected compared with 8% to 10% in developing areas such as Southeast Asia.8
The highest concentration of the HBV is found in blood and serous fluids. Therefore, the primary mode of hepatitis B transmission is either by blood or body fluids through perinatal, sexual, or percutaneous exposure.10 Infants born of mothers who are infected with HBV that is actively replicating have a 90% risk of developing chronic hepatitis B. If an infant residing in an endemic area is not infected at birth, the risk of acquiring chronic hepatitis B is still 30% to 60% within the first 5 years of life from horizontal transmission.11,12 Individuals at greatest risk of acquiring HBV are listed in Table 24–1. Approximately 33% of the reported hepatitis B cases have no identifiable risk factors.10
Hepatitis C
More than 170 million people are infected with hepatitis C worldwide, and more than 4 million have the disease in the United States.13 The prevalence is higher among non-Hispanic blacks than non-Hispanic whites, and men are more likely to be infected than women.14,15 Additionally, genotypes are geographically specific. For example, genotype 1 is commonly found in patients in the United States whereas genotype 4 is common in the Middle East.14,16Approximately 75% of those infected with HCV in the United States have genotype 1, and about 14% and 5% have genotypes 2 and 3, respectively.14,16Genotype does not dictate disease severity or clinical outcomes but is used to determine the duration of therapy and the likelihood of therapeutic response.15
IV drug users utilizing contaminated paraphernalia are responsible for about 60% of HCV transmissions.13 Because of the routine screening of blood products, the risk of HCV transmission via blood transfusion is very low (0.004–0.0004% per unit transfused).13,17 Other populations at risk for acquiring HCV are listed in Table 24–1. Approximately 10% of the individuals infected with HCV have no identifiable risk factors.17
Hepatitis D
Hepatitis D affects approximately 10 million people worldwide. Eastern Asia has the lowest prevalence of HDV despite having the highest prevalence of HBV infections. Areas with the highest prevalence of HDV include the Middle East, West Africa, Western and Central Asia, parts of South America, and the South Pacific islands.18,19
There are three major HDV genotypes that are geographically specific. Genotype 1 primarily affects individuals residing in North America, Europe, Middle East, East Asia, and North Africa.18 Individuals residing in Japan and Taiwan are mostly diagnosed with genotype 2. Patients in northern parts of South America are mostly infected with genotype 3.18,20
The most likely modes of transmitting the HDV are similar to those of HBV, including IV drug users using unsterilized needles and recipients of contaminated blood products. Sexual and perinatal transmission are rare for HDV.18,19 Individuals at greatest risk of acquiring HDV are listed in Table 24–1.
Hepatitis E
Hepatitis E is found worldwide, but acute cases occur primarily in Central and Southeast Asia, the Middle East, and North Africa.21,22 The HEV prevalence rate in the United States is 1% to 3%. The virus is primarily transmitted by the fecal–oral route. Transmission of HEV is more prominent in underdeveloped countries where sanitation is poor.
PATHOPHYSIOLOGY
Hepatitis A
Hepatitis A is a nonenveloped single-stranded RNA virus classified as the Hepatovirus genus under the Picornaviridae family.1,4 The only host for the HAV is humans, with hepatic cells as the primary site for viral replication. As part of the viral degradation process, the HAV is released into the biliary system causing elevated concentrations of the virus in the feces.23
Hepatitis B
Hepatitis B (also known as the Dane particle) belongs to the Hepadnaviridae family24 The HBV is a partially double-stranded DNA virus with a phospholipid layer containing hepatitis B surface antigen (HBsAg) that surrounds the nucleocapsid. The nucleocapsid contains the core protein that produces hepatitis B core antigen (HBcAg), which is undetectable in the serum. Hepatocellular injury from HBV is thought to be due to a cytotoxic immune reaction that occurs when HBcAg is expressed on the surface of the hepatic cells. Fortunately, antibodies against hepatitis B core antigen (anti-HBc) are measurable in the blood, where anti- HBc to immunoglobulin M (IgM) indicates active infection and anti-HBc to IgG relates to either chronic infection or possible immunity against HBV.
Viral replication occurs when hepatitis B envelope antigen (HBeAg) is present and circulating in the blood. The serum HBV DNA concentration is a measure of viral infectivity and quantifies viral replication. Once the hepatitis B infection resolves, antibodies against hepatitis B envelope (anti-HBe) and antibodies against hepatitis B surface antigen (anti-HBs) develop, and HBV DNA levels become undetectable. However, if these antibodies do not develop, then the likelihood of developing chronic hepatitis B increases. This is primarily dependent on the host’s immune system at the time the infection was attained. In immunocompetent individuals, the disease resolves spontaneously in most cases with no further sequelae. In immunocompromised persons, the infection is less likely to be eradicated.24
Natural History of Hepatitis B
The natural history of hepatitis B depends on the age at which infection is acquired. Chronic HBV occurs in less than 5% of those who are older than 5 years of age, whereas the rate is more than 90% in infants born to mothers infected with HBV.10 Approximately 90% of adults infected with HBV develop anti-HBs, which results in lifelong immunity. About 30% of adults with initial symptoms of HBV present with jaundice or fatigue, and about 0.5% exhibit fulminant hepatitis.11,25 Cirrhosis and HCC are the two major complications associated with chronic hepatitis B infections. Patients who develop cirrhosis have a higher mortality rate than those without this complication.11
Hepatitis C
Hepatitis C, first known as non-A, non-B hepatitis, is a bloodborne infection caused by a single-stranded RNA virus belonging to the Flaviviridae family and the Hepacivirus genus.13,16 It is theorized that structural and nonstructural (NS) peptides may be responsible for RNA viral replication, specifically the NS5 peptide. There are 11 genotypes (numbered 1–11) and more than 90 subtypes (genotypes 1a, 1b, 2a, 3b, etc.) that are unique to hepatitis C.13
Antibodies against HCV (anti-HCV) in the blood indicate infection with the HCV. If the infection persists for more than 6 months and viral replication is confirmed by HCV RNA levels, then the person has chronic hepatitis C. Chronic disease may be due to an ineffective host immune system against the HCV. Cytotoxic T lymphocytes are ineffective in eradicating the HCV, thus allowing persistent damage to hepatic cells. Therefore, immunocompromised individuals are less likely to eradicate the HCV.16
Natural History of Hepatitis C
Only 10% to 15% of patients have acute hepatitis C that resolves without any further sequelae. In more than 70% of cases, hepatitis C develops into a chronic disease that is asymptomatic in about 60% to 80% of patients.12,13Approximately 70% of chronic HCV cases progress to mild, moderate, or severe hepatitis. Cirrhosis and its complications occur in 15% to 20% of patients infected with HCV. In 10% to 20% of cases, 20 to 40 years may elapse between the time of exposure and the development of cirrhosis.12 Once cirrhosis is confirmed, the rate of developing HCC increases by 1% to 4% per year.12 Approximately 25% of patients infected with the HCV who develop cirrhosis ultimately die from the disease.13
Hepatitis D
Hepatitis D (originally called delta hepatitis) belongs to the genus Deltavirus of the Deltaviridae family.18,19 The HDV virion is a defective single-stranded circular RNA virus that requires the presence of HBV for HDV viral replication. This is because the hepatitis D virus antigen (HDVAg) is coated by the HBsAg.
The mechanism of hepatic damage induced by HDV is undetermined, but it is known that replication of HDV cannot occur without HBV being present causing either coinfection (both hepatitis B and D infection occurring simultaneously) or superinfection (acquiring HDV after having longstanding disease with HBV).18,19
Hepatitis E
Hepatitis E is a nonenveloped single-stranded messenger RNA virus of unclassified genus.21 The HEV is similar to HAV in that the virus is found in contaminated feces, thus infecting people via the fecal–oral route. High HEV levels in the bile often prompt viral shedding in the feces. The severity of hepatic damage is dependent on the HEV strain: Mex 14, Sar 55, or the US 2 strain.22 No cases of chronic hepatitis E have been documented.
CLINICAL PRESENTATION AND DIAGNOSIS
Diagnosis of Viral Hepatitis
Diagnosing viral hepatitis may be difficult because most infected individuals are asymptomatic.4,10,12,13 Because symptoms cannot identify the specific type of hepatitis, laboratory serologies must be obtained (Table 24–2). In addition, liver function tests may be obtained to assess the extent of cholestatic and hepatocellular injury. However, the definitive test to determine the amount of damage and inflammation of hepatic cells is a liver biopsy.
Hepatitis A
The diagnosis of hepatitis A is made by detecting immuno-globulin antibody to the capsid proteins of the HAV. The presence of IgM anti-HAV in the serum indicates an acute infection. IgM appears approximately 3 weeks after exposure and becomes undetectable within 6 months. In contrast, IgG anti-HAV appears in the serum at approximately the same time IgM anti-HAV develops but indicates protection and lifelong immunity against hepatitis A.1
Hepatitis B
Hepatitis B is diagnosed when HBsAg is detectable in the serum. The nucleocapsid of the HBsAg contains the core protein that produces HBcAg, which is undetectable in the serum. The presence of antibodies against anti-HBc to IgM indicates active infection, and anti-HBc to IgG relates to either chronic infection or possible immunity against HBV.8,10
Viral replication occurs when HBeAg is present. Measurement of HBV DNA is used to determine viral infectivity and assess and quantify viral replication. Once the hepatitis B infection resolves, anti-HBe and anti-HBs develop, and HBV DNA levels becomes undetectable. Chronic hepatitis B is separated into two types, HBeAg-positive or HBeAg-negative.
Hepatitis C
Hepatitis C is diagnosed by testing for anti-HCV in the serum. The disease is confirmed by the presence of HCV RNA. HCV RNA levels quantify viral replication and are used to determine if antiviral treatment for HCV is effective. Once a hepatitis C infection has been confirmed, further blood work should be obtained to determine the individual’s genotype (1–11). HCV genotyping is used to determine the likelihood of response to antiviral therapy.13
Hepatitis D
Hepatitis D infection requires the presence of HBV for HDV viral replication. Measuring HDV RNA levels in the serum by polymerase chain reaction (PCR) confirms the presence of HDV and is the most accurate diagnostic test. The presence of IgM antibodies to HDV Ag (IgM anti-HD) indicates active disease, and IgG anti-HD also becomes detectable if the infection does not resolve spontaneously. Unlike the antibodies developed against HAV, HDV antibodies do not confer immunity.
Hepatitis E
The diagnosis of hepatitis E is based on the presence of anti-HEV antibodies; IgM anti-HEV. A test for hepatitis E RNA levels is available for use in clinical trials.21
Clinical Presentation and Diagnosis of Viral Hepatitis
Symptoms
• Most patients infected with any type of viral hepatitis have no symptoms.
• Patients with symptoms may experience any of the following: flu-like symptoms, fevers, fatigue/malaise, anorexia, nausea, vomiting, diarrhea, dark urine, pale-appearing stools, pruritus, and abdominal pain.
Signs
• Jaundice may be evident in the whites of the eyes (scleral icterus) or skin.
• An enlarged liver (hepatomegaly) and spleen (splenomegaly) may be present.
• In fulminant hepatitis with hepatic encephalopathy, patients may have asterixis and coma.
• In rare instances, extrahepatic symptoms may develop: arthritis, postcervical lymphadenopathy, palmar erythema, cryoglobulinemia, and vasculitis.
Laboratory Tests
• See Table 24–2.
Table 24–2 Interpretation of Viral Hepatitis Serology Panels


PREVENTION AND TREATMENT OF VIRAL HEPATITIS
Desired Outcomes
General desired outcomes for treating hepatitis are to: (a) prevent the spread of the disease; (b) prevent and treat symptoms; (c) suppress viral replication; (d) normalize hepatic aminotransferases; (e) improve histology on liver biopsy; and (f) decrease morbidity and mortality by preventing cirrhosis, HCC, and ESLD.
For hepatitis B, additional treatment goals include: (a) seroconversion or loss of HBsAg; (b) seroconversion or loss of HBeAg; and (c) achieving undetectable HBV DNA levels. Additional goals for chronic hepatitis C include achieving undetectable HCV RNA 6 months post hepatitis C therapy by obtaining a sustained virologic response (SVR).26
General Approach
Managing viral hepatitis involves both prevention and treatment. Prevention of hepatitis A and B (and indirectly for hepatitis D) can be achieved with immune globulin or vaccines. ![]() Acute viral hepatitis A, B, C, D, and E are primarily managed with supportive care. Individuals with mild to moderate symptoms rarely require hospitalization. Occasionally, hospitalization is required in individuals experiencing significant nausea, vomiting, diarrhea, and encephalopathy. Liver transplantation may be required in rare instances if fulminant hepatitis develops.
Acute viral hepatitis A, B, C, D, and E are primarily managed with supportive care. Individuals with mild to moderate symptoms rarely require hospitalization. Occasionally, hospitalization is required in individuals experiencing significant nausea, vomiting, diarrhea, and encephalopathy. Liver transplantation may be required in rare instances if fulminant hepatitis develops.
Patient Encounter, Part 1
A 41-year-old Caucasian man is required by his employer to obtain a physical exam. His only complaint is fatigue for the past year that he attributes to working overtime at the steel mill. He has no significant past medical history. He reports being stressed at times from an impending divorce and from needing to take care of his five young children.
PMH: Patient never had any suicidal ideations in the past or history of depression.
PSH: Appendectomy in 1987 at the age of 27 that required blood transfusions
FH: Mother with osteoporosis and father alive and well
SH: He was in a monogamous relationship. Single now with no significant other. Smoked a pack of cigarettes per day times 15 years but quit 5 years ago; used illicit drugs once in the past; drinks daily for the past 30 years; has one tattoo on the left arm done unprofessionally; employed as a steel mill worker
Meds: None
ROS: Complains only of irritability and mild depression; no nausea, vomiting, diarrhea, abdominal pain, or anorexia; never had an episode of jaundice, pale stools, or tea-colored urine
PE:
VS: BP 128/80 mm Hg, P 80 bpm, RR 20/minute, T 370°C (98.6°F), wt 70 kg (154 lb), ht 5’9“ (175 cm)
Abd: Soft, nontender, normal liver span; no hepato-splenomegaly, no ascites.
Labs:
• Sodium 141 mEq/L (mmol/L), potassium 4.1 mEq/L (mmol/L), chloride 99 mEq/L (mmol/L), CO2 21 mEq/L (mmol/L), BUN 20 mg/dL (7.14 mmol/L), serum creatinine 1.2 mg/dL (106 μmol/L), glucose 98 mg/dL (5.4 mmol/L)
• Hemoglobin 16.1 g/dL (161 g/L or 10.0 mmol/L), hematocrit 48.4% (0.484), WBC 5.1 × 103/mm3 (× 109/L), platelets 135 × 103/mm3 (× 109/L)
• Aspartate aminotransferase (AST) 69 IU/L (1.15 μKat/L), alanine aminotransferase (ALT) 92 IU/L (1.53 μKat/L)
• Total bilirubin 1.0 mg/dL (17.1 μmol/L), albumin 3.7 g/dL (37 g/L), alkaline phosphatase 164 IU/L (2.73 μKat/L), TSH 1.3 micro IU/mL (mIU/L)
• Anti-HAV IgM (-), anti-HAV IgG (-), anti-HBs (+), HBsAg (-), HBeAg (-), anti-HBc IgG (-), anti-HBc IgM (-), anti-HBe (-), HBV DNA less than 2,000 IU/mL, anti-HCV (+), genotype 2; HCV RNA 91,230 IU/mL
• Liver biopsy: Mild inflammation and minimal fibrosis (grade 1, stage 1 disease) consistent with chronic hepatitis C
What information is suggestive of viral hepatitis?
What risk factors does he have for viral hepatitis?
What additional information do you need before creating a treatment plan for this patient?
Patients with viral hepatitis B, C, and D may develop chronic disease leading to ESLD and HCC. Treatment is available for chronic liver disease associated with HBV, HCV, and HDV.26
Hepatitis A Prevention
![]() Good personal hygiene and proper disposal of sanitary waste are required to prevent fecal–oral transmission of the H AV.1,4,6 This includes frequent handwashing with soap and water after using the bathroom and prior to eating meals. Drinking bottled water, avoiding fruits, vegetables, and raw shellfish harvested from sewage-contaminated water in areas where HAV is most endemic will also minimize the risk of becoming infected with hepatitis A.
Good personal hygiene and proper disposal of sanitary waste are required to prevent fecal–oral transmission of the H AV.1,4,6 This includes frequent handwashing with soap and water after using the bathroom and prior to eating meals. Drinking bottled water, avoiding fruits, vegetables, and raw shellfish harvested from sewage-contaminated water in areas where HAV is most endemic will also minimize the risk of becoming infected with hepatitis A.
Individuals at high risk of acquiring hepatitis A (Table 24–1) should receive either serum immune globulin or the hepatitis A vaccine, depending on their personal circumstances, as described below.4,27
Immune Globulin
Immune globulin (IG) is a solution containing antibodies from sterilized pooled human plasma that provides passive immunization against various infectious diseases, including hepatitis A.4 Immune globulin is available for either intravenous (IGIV) or intramuscular (IGIM) administration, but only IGIM is used for prevention of hepatitis A. IGIM does not confer lifelong immunity, but it is effective in providing pre- and postexposure prophylaxis against HAV.4
Adverse effects of IGIM are rare. There have been reports of anaphylaxis in individuals who have immunoglobulin A deficiency after receiving repeated IG administration. Therefore, these patients should not receive IGIM. IGIM is not contraindicated in pregnant or lactating women or infants requiring hepatitis A immunization. The thimerosal-free preparation should be used in infants.4
IGIM should be injected into a deltoid or gluteal muscle. It does not affect the immune response of inactivated vaccines, oral polio virus, or yellow fever vaccine. The administration of live vaccines (e.g., measles, mumps, rubella [MMR] vaccine) concomitantly with IGIM may decrease the immune response significantly; thus, MMR and varicella vaccines should be delayed for at least 3 and 5 months, respectively, after IGIM has been administered. Additionally, IGIM should not be given within 2 weeks of the MMR administration or within 3 weeks of the varicella vaccine to maximize the efficacy of the immunization.4
Pre-exposure Prophylaxis
Pre-exposure prophylaxis with IGIM is indicated for individuals at high risk of acquiring the HAV who: (a) are less than 12 months of age; (b) elect not to receive the hepatitis A vaccine; or (c) cannot receive the hepatitis A vaccine (e.g., because of allergy to the components alum or 2-phenoxyethanol). Because active vaccine immunity takes several weeks to develop, travelers who are older adults, immunocompromised, have chronic liver disease or other chronic medical conditions who plan to depart for endemic areas within 2 weeks and have not received the hepatitis A vaccine should receive IGIM. If the duration of travel is less than 3 months, these individual should receive a dose of IG 0.02 mL/kg and hepatitis A vaccine at the same time, but administered at different injection sites.4,27
If the travel duration is expec ted to be greater t han 2 mont hs, then IG at a dose of 0.06 mL/kg should be administered as the higher dose provides immunity up to 5 months. If protection against HAV is required beyond 5 months, then readministration of IGIM is recommended.4,27
Postexposure Prophylaxis
Individuals in contact with people infected with acute HAV (including household and sexual partners), staff and children from day care facilities, and food handlers of restaurant establishments may be candidates for postexposure prophylaxis. IG is preferred in individuals who are less than 12 months or more than 40 years of age, immunocompromised, diagnosed with chronic liver disease, or have contraindications to the hepatitis A vaccine.4,27
The risk of infection may be decreased by 90% if IGIM 0.02 mL/kg is given within 2 weeks of being exposed to the HAV. IGIM may still be beneficial if it is given more than 2 weeks after exposure to a known case of HAV, as it may decrease the severity of hepatic damage.4,27
Hepatitis A Vaccine
Persons at risk of acquiring the HAV should receive the hepatitis A vaccine when appropriate. The vaccine is effective in providing pre- and postexposure prophylaxis against clinical hepatitis A infections.27,28
Two inactivated hepatitis A vaccines, HAVRIX and VAQTA, are available in the United States and are effective in providing active immunization and preventing clinical hepatitis A. The two vaccines are considered interchangeable, and doses are dependent on age (Table 24–3).4
HAVRIX and VAQTA are effective in providing active pre- or postexposure prophylaxis when given in two injections 6 months apart (referred to as months 0 and 6). Efficacy is defined by measuring antibody response with the modified enzyme immunoassay. For HAVRIX, levels greater than 20 mIU/mL (20 IU/L), and for VAQTA, levels greater than 10 mIU/mL (10 IU/L) are considered protective. After administration of the first dose of vaccine, 94% to 100% of adults and 97% to 100% of children and adolescents develop protective antibody concentrations against the HAV. All recipients over 2 years of age receiving the second dose at month 6 have 100% antibody coverage; therefore, postvaccination measurement of antibody response is not required.4
For pre-exposure prophylaxis, the hepatitis A vaccine is recommended for travelers to endemic hepatitis A countries. It should be administered to healthy international travelers aged 40 years of age and younger regardless of the scheduled dates for departure. This recommendation does not apply to adults more than 40 years old, the immunocompromised, or those with chronic medical conditions with or without chronic liver disease. These individual who plan to depart to an endemic country in less than 2 weeks should receive both the hepatitis A vaccine and IG (0.02 mL/kg).27
For postexposure prophylaxis, the hepatitis A vaccine is effective in preventing clinical infection in healthy individuals between 12 months and 40 years of age when administered within 14 days after exposure.27,28 Individuals outside these age ranges or with significant comorbid conditions should receive IG for postexposure prophylaxis rather than the hepatitis A vaccine because this population has not been studied.27
Table 24–3 Recommended Intramuscular Doses of Hepatitis A Vaccines

The hepatitis A vaccine may provide effective immunity for 8 years in adults and children. Kinetic models have theorized that immunity may last longer than 20 years, but this has not been confirmed in clinical trials.4
The most common adverse effects in adults include injection site reactions (e.g., tenderness, pain, and warmth), headaches within 5 days after vaccination, and fatigue. Children may have feeding disturbances. Local reactions may be minimized by using an appropriate needle length based on the person’s age and size and by administering the injection intramuscularly in the deltoid muscle. Hepatitis A vaccine given during pregnancy has not been evaluated in clinical trials. Since both brands of vaccine are made from inactivated HAV, the risk of developing fetal complications should be minimal.
Hepatitis B Prevention
![]() Individuals may minimize their risk of acquiring the hepatitis B infection by avoiding contaminated blood products or indulging in high-risk behavior such as IV drug use. In addition, those who are at high risk of acquiring the HBV (Table 24–1) should be vaccinated with the hepatitis B vaccine.10 Screening pregnant women for hepatitis B and providing universal hepatitis B vaccinations to all newborns is effective in preventing hepatitis B infections.29 In some cases, postexposure prophylaxis with hepatitis B immune globulin (HBIG) may be recommended to prevent the development of acute infection and complications associated with HBV.
Individuals may minimize their risk of acquiring the hepatitis B infection by avoiding contaminated blood products or indulging in high-risk behavior such as IV drug use. In addition, those who are at high risk of acquiring the HBV (Table 24–1) should be vaccinated with the hepatitis B vaccine.10 Screening pregnant women for hepatitis B and providing universal hepatitis B vaccinations to all newborns is effective in preventing hepatitis B infections.29 In some cases, postexposure prophylaxis with hepatitis B immune globulin (HBIG) may be recommended to prevent the development of acute infection and complications associated with HBV.
Hepatitis B Immune Globulin
Hepatitis B immune globulin (HBIG) is a sterile solution containing antibodies prepared from pooled human plasma that has a high concentration of anti-HBs (antibodies to hepatitis B surface antigen). HBIG provides passive immunization for postexposure prophylaxis against the HBV. A single dose of HBIG of 0.06 mL/kg is effective in preventing chronic hepatitis B infections in adults.10 Similar to IGIM, HBIG should only be administered intramuscularly.
The most common side effects of HBIG include erythema at the injection site, headaches, myalgia, fatigue, urticaria, nausea, and vomiting. Serious adverse effects are rare and may include liver function test abnormalities, arthralgias, and anaphylactic reactions. HBIG should be used with caution in individuals who have experienced hypersensitivity reactions to immune globulin or those who have immunoglobulin A deficiency. Similar to IGIM, concomitant administration of HBIG and live vaccines should be avoided because the efficacy of the immunization may decrease significantly.
Hepatitis B Vaccine
The two hepatitis B vaccines available in the United States are Recombivax HB and Engerix-B. These vaccines are produced with recombinant DNA technology by inserting the gene for HBsAg into the plasmid that is synthesized by Saccharomyces cerevisiae cells.![]() Persons at high risk (Table 24–1) of acquiring the hepatitis B virus should be vaccinated with the hepatitis B vaccine at months 0, 1, and 6.The hepatitis B vaccine dose depends on the person’s age (Table 24–4).
Persons at high risk (Table 24–1) of acquiring the hepatitis B virus should be vaccinated with the hepatitis B vaccine at months 0, 1, and 6.The hepatitis B vaccine dose depends on the person’s age (Table 24–4).
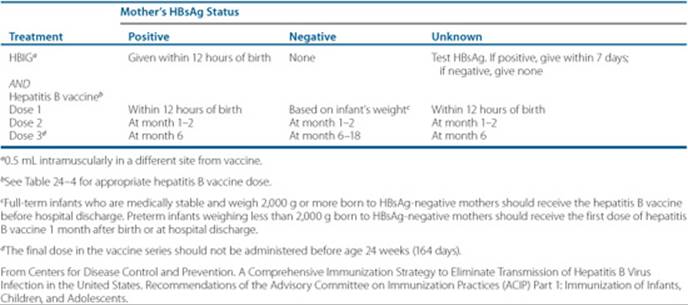
In addition to pre-exposure prophylaxis, the hepatitis B vaccine is indicated after exposure to the HBV to prevent chronic hepatitis B disease. Adults acutely exposed to blood containing HBsAg from an accidental needlestick, sexual contacts, or IV drug use should be offered hepatitis B vaccine with or without HBIG, preferably within 24 hours of exposure based on the source of exposure and the vaccination status of the exposed person (Table 24–5). Postexposure prophylaxis for perinatal exposure is dependent on several factors, including maternal HBsAg status and newborns weight.29 For mothers who are HBsAg-positive, newborns should be immunized within 12 to 24 hours after birth with both the hepatitis B vaccine and HBIG 0.5 mL. If the mother is HBsAg-negative, the newborn should be given only the hepatitis B vaccine (Table 24–6).
Table 24–4 Recommended Intramuscular Dosing Regimens for Hepatitis B Vaccines

Table 24–5 Recommendations for Prophylaxis After Nonoccupational Exposure to the Hepatitis B Virus

Table 24–6 Recommendations for Hepatitis B Prophylaxis to Prevent Perinatal Transmission
For optimal response, the hepatitis B vaccine should only be administered intramuscularly (into the anterolateral thigh region in neonates and infants; the deltoid region in older children and adults) and not intravenously or intradermally. The vaccine should not be given in the gluteal region, as it may result in lower rates of immunity.
The efficacy of the hepatitis B vaccine occurs when antibody concentrations are greater than 10 mIU/mL (10 IU/L). Because most people who complete the vaccination series obtain adequate antibody levels, postvaccination testing is not routinely recommended. The immunogenicity rate is greater than 90% at completion of the three-dose hepatitis B immunization series.10 This regimen is also 85% to 95% effective in preventing perinatal HBV infections.29 The hepatitis B vaccine may provide effective immunity for 10 to 15 years in children and adolescents; however, there may be an anamnestic response requiring booster doses.30,31
Protective antibody levels may be lower in older adults and immunocompromised patients, so postvaccine testing may be warranted 1 to 6 months after completing the vaccination series in these patients.10
The most frequent adverse effects are local reactions at the injection site (pain, tenderness, erythema, swelling, and pruritus), fever, headaches, dizziness, and irritability. Anaphylaxis, a serum sickness–like hypersensitivity syndrome, chronic fatigue syndrome, and neurologic diseases (leukoencephalitis, optic neuritis, and transverse myelitis) have been reported rarely.10 Hepatitis B vaccine is not contraindicated during pregnancy.10
Hepatitis A and B Combination Vaccine
![]() A vaccine that combines both inactivated hepatitis A and recombinant hepatitis B (Twinrix) is approved for immunizing individuals more than 18 years of age with indications for both hepatitis A and B vaccines.10 A 1-mL dose of Twinrix contains the antigenic components of not less than 720 ELISA units of Havrix and 20 mcg of recombinant HBsAg protein of Engerix-B and should be administered at months 0, 1, and 6. Antibody seroconversion for hepatitis A and B was greater than 98% in adult volunteers tested 1 month after a three-dose vaccine series. The side-effect profile of Twinrix is similar to giving each vaccine separately.32
A vaccine that combines both inactivated hepatitis A and recombinant hepatitis B (Twinrix) is approved for immunizing individuals more than 18 years of age with indications for both hepatitis A and B vaccines.10 A 1-mL dose of Twinrix contains the antigenic components of not less than 720 ELISA units of Havrix and 20 mcg of recombinant HBsAg protein of Engerix-B and should be administered at months 0, 1, and 6. Antibody seroconversion for hepatitis A and B was greater than 98% in adult volunteers tested 1 month after a three-dose vaccine series. The side-effect profile of Twinrix is similar to giving each vaccine separately.32
Chronic Hepatitis B Treatment
Patients who are immune tolerant or have inactive hepatitis B (defined as having a positive HBsAg, normal ALT, high or low HBV DNA levels, and mild/minimal inflammation and fibrosis) should not receive treatment because hepatitis B antiviral agents rarely result in HBeAg seroconversion, and long-term treatment leads to drug resistance.33 Patients with elevated ALT (more than two times the upper limit of normal) and positive HBV DNA levels require treatment to delay progression to cirrhosis and prevent the development of ESLD.
Chronic hepatitis B may be separated into two main types: (a) HBeAg-positive (also known as wild type), and (b) HBeAg-negative (known as precore mutant or promoter mutant). The treatment endpoints for HBeAg-positive patients are different from those who are HBeAg-negative because the latter disease does not allow for HBeAg seroconversion.
Patients with HBeAg-positive chronic hepatitis B have elevated HBV DNA concentrations greater than 20,000 IU/mL and detectable HBeAg. In contrast, patients with HBeAg-negative chronic hepatitis B have HBV DNA concentrations greater than 2,000 IU/mL and undetectable serum HBeAg. Thus, an undetectable HBV DNA level, not seroconversion, is considered a treatment endpoint. HBeAg-negative HBV infections are more likely to lead to liver fibrosis and may require lifelong treatment because undetectable HBV DNA levels are difficult to achieve.
![]() The drug of choice for chronic hepatitis B depends upon the patient’s past medical history, ALT, HBV DNA level, HBeAg status, severity of liver disease, and history of previous HBV therapy. The safety and efficacy profile of the medication and the likelihood of developing drug resistance should also be considered.
The drug of choice for chronic hepatitis B depends upon the patient’s past medical history, ALT, HBV DNA level, HBeAg status, severity of liver disease, and history of previous HBV therapy. The safety and efficacy profile of the medication and the likelihood of developing drug resistance should also be considered.
Entecavir and tenofovir are recommended as first-line chronic hepatitis B treatments due to profound HBV DNA suppression and minimal resistance.34 Pegylated interferon α-2a is also considered a first-line agent because it lacks drug resistance. Pegylated interferon has replaced unmodified interferon because the pegylated form may be given subcutaneously once weekly rather than three times weekly.
Adefovir is second-line to tenofovir because adefovir is less potent in suppressing hepatitis B viral replication in treatment-naïve patients. Lamivudine is no longer recommended as first-line therapy due to its high rate of resistance.34,35 Patients who are being treated with adefovir or lamivudine and currently responding to treatment should continue with the regimen. However, if there is inadequate virologic response or drug resistance develops, then adding another hepatitis B antiretroviral agent or switching to a more potent drug should be considered. The role of telbivudine in therapy is undetermined due to its intermediate rate of resistance.35 Each therapeutic agent will be described briefly in the sections that follow.
Interferon and Peyglated Interferon
Interferon α-2b and pegylated interferon α-2a are the only interferon therapies approved for treatment of chronic hepatitis B. Unlike other antiretroviral treatments, interferon therapy is effective in suppressing, and in some cases ceasing, viral replication without inducing resistance.
Approximately one-third of HBeAg-positive patients become seronegative after 4 to 6 months of treatment.36,37 Patients with HBeAg-negative hepatitis B may require 12 to 24 months of therapy to achieve an SVR.38,39 The durability of response (likelihood of achieving and sustaining HBeAg seroconversion) is greater than 80% after treatment discontinuation.
Pegylated interferon is interferon that is attached to a polyethylene glycol molecule that increases the half-life of the drug allowing once-weekly dosing versus thrice-weekly administration of unmodified interferon. Pegylated interferon is well-tolerated with similar or better efficacy than unmodified interferon for the treatment of chronic hepatitis B.34,35 However, it should not be used in patients with decompensated liver disease (because it may induce hepatic failure) or in those with significant and unstable medical comorbidities.33
The subcutaneous dose of interferon α-2b (Intron-A) is either 5 million units daily (better tolerated) or 10 million units three times weekly. The recommended treatment duration is 16 to 24 weeks for HBeAg-positive disease and 12 to 24 months for HBeAg-negative disease.35 The approved dose of pegylated interferon α-2a (Pegasys) for chronic hepatitis B is 180 mcg subcutaneously once weekly for 48 weeks.37Interferon doses may need to be adjusted in patients with cytopenias and renal impairment.
Even though the advantages of interferon or pegylated interferon include a finite duration of treatment, lack of resistance, and possible HBsAg loss or seroconversion (development of anti-HBs), there are several significant disadvantages. These include the need for subcutaneous injections and a pronounced adverse-effect profile that may require dosage reductions or treatment discontinuation. The most common adverse effects include injection site reactions and flu-like symptoms (fevers, chills, joint pain, and muscle aches). Systemic adverse effects include fatigue, headache, insomnia, irritability, depression, suicidal ideation, alopecia, and dermatitis. Other rare but significant systemic untoward effects include endocrine abnormalities (thyroid, diabetes), hypertriglyceridemia, GI (diarrhea, anorexia, nausea) and possible ophthalmic changes. Hematologic abnormalities are common including neutropenia, anemia, and thrombocytopenia, which may require either a dose reduction or treatment discontinuation. Refer to the subsequent section on hepatitis C for management of these adverse effects. Approximately 35% of patients develop an ALT flare when treated with interferon. An increase in ALT has been associated with a positive response, but it may lead to hepatic decompensation, which can be fatal. Thus, only patients with compensated liver disease should be considered for treatment with interferon therapy.
Entecavir
Entecavir (Baraclude) is a guanosine nucleoside analogue that is highly potent in inhibiting HBV DNA polymerase. Ente-cavir is effective against HBeAg-positive, HBeAg-negative, and lamivudine-resistant chronic hepatitis B.34,40–43 Resistance rates are low (1–2%) in patients treated with entecavir for up to 5 years in lamivudine-naïve individuals. For patients who were previously treated with lamivudine and switched to entecavir, the resistance rate is approximately 50% at 5 years.34
The dose of entecavir is 0.5 mg once daily for patients naïve to lamivudine and 1 mg once daily for those with lamivudine resistance. Dosage adjustments are required in patients with renal dysfunction. The side effect profile for entecavir is similar to lamivudine and adefovir dipivoxil. Patients treated with entecavir should be monitored for signs and symptoms of lactic acidosis and severe hepatomegaly with steatosis, because some cases have been fatal.
The package labeling for entecavir contains a “black-box” warning indicating that there is a potential for development of resistance to HIV nucleoside reverse transcriptase inhibitors if entecavir is used to treat chronic hepatitis B in patients with untreated HIV infection. Therefore, entecavir monotherapy should not be initiated in patients coinfected with HIV and HBV because resistance to highly active antiretroviral therapy (HAART) may occur.44
Tenofovir Disoproxil Fumarate
Tenofovir disoproxil fumarate (Viread) is an acyclic adenine nucleotide reverse transcriptase inhibitor that is similar in structure to adefovir dipivoxil. Tenofovir inhibits HIV and hepatitis B viral replication and is indicated for HBeAg-positive and HBeAg-negative chronic hepatitis B with compensated liver disease.
Tenofovir is preferred over adefovir for chronic hepatitis B infections because of greater effectiveness in inhibiting viral replication and lack of resistance at week 72.34,45,46 Patients who developed resistance to lamivudine, entecavir or adefovir may benefit from tenofovir.47–49
The dose of tenofovir disoproxil fumarate is 300 mg orally once daily. Dose adjustments are required in patients with renal dysfunction because tenofovir is primarily renally excreted. Tenofovir is well-tolerated with adverse effects similar to adefovir and other hepatitis B oral agents. Several case reports have implicated tenofovir in causing nephrotoxicity and Fanconi’s syndrome in patients coinfected with HIV and HBV.50,51 Patients should be monitored for signs and symptoms of lactic acidosis and severe hepatomegaly with steatosis because some cases have been fatal. Hepatic function should be carefully monitored if treatment is to be discontinued because severe acute exacerbations of hepatitis have been reported with antihepatitis B viral agents.
Adefovir Dipivoxil
Adefovir dipivoxil (Hepsera) is a prodrug of adefovir, an adenosine nucleotide analog that inhibits DNA polymerase. It is effective against HIV and HBV, including HBV resistant to lamivudine, entecavir, tenofovir, and telbivudine. Treatment with adefovir dipivoxil 10 mg daily is comparable to lamivudine in normalizing aminotransferase levels and improving histologic activity.52–54 Resistance to adefovir dipivoxil is minimal for the first few years of treatment but increases to approximately 30% after 5 years of therapy.35,55
The dose of adefovir dipivoxil is 10 mg once daily. The most common side effects include asthenia, abdominal pain, diarrhea, dyspepsia, headaches, nausea, and flatulence. Adefovir dipivoxil is also associated with dose-related nephrotoxicity, which was most commonly seen in HIV patients receiving doses larger than 60 mg. Serum creatinine monitoring is recommended to detect renal tubular injury. The dose must be reduced in patients with renal insufficiency.
Lamivudine
Lamivudine (Epivir-HBV) is an oral synthetic cytosine nucleoside analogue having antiviral effects against HIV and hepatitis B virus. In patients with chronic hepatitis B, lamivudine is effective in suppressing hepatitis B viral replication, normalizing ALT levels, and improving liver histology.33,56,57 Patients with chronic hepatitis B may have a similar or a superior response in achieving these endpoints when compared to interferon or pegylated interferon.34
However, prolonged lamivudine therapy (up to 5 years) may be needed to sustain seroconversion, and lamivudine resistance is as high as 60% to 70% at 5 years.34,35 Due to the high rate of resistance, lamivudine is no longer recommended as first-line therapy for chronic hepatitis B.34
The dose of lamivudine is 100 mg orally once daily for treatment of chronic hepatitis B without HIV coinfections. The dose must be adjusted in patients with renal dysfunction.
Adverse effects are minimal and include fatigue, diarrhea, nausea, vomiting, and headaches. ALT levels should be monitored carefully, as two- to threefold increases may be observed. ALT should also be monitored closely when lamivudine therapy is being discontinued, as increased levels may indicate a flare in disease activity leading to liver failure.
Telbivudine
Telbivudine (Tyzeka) is an L-nucleoside analogue that inhibits HBV replication. It is indicated for HBeAg-positive and HBeAg-negative chronic hepatitis B with compensated liver disease.
Telbivudine offers a slightly more effective reduction in HBV DNA levels and normalization of aminotransferases when compared to lamivudine. However, its benefits in improving histology, HBeAg seroconversion, and HBeAg loss remain to be confirmed.58 Telbivudine resistance is lower than with lamivudine, but rates are significant with continued treatment.
The dose of telbivudine is 600 mg orally once daily. Dosage adjustments are required in patients with renal dysfunction. Adverse effects are similar to other HBV oral agents. Patients should be monitored for signs and symptoms of lactic acidosis and severe hepatomegaly with steatosis, because some cases have been fatal. Myopathy characterized by elevated creatine kinase levels and muscle weakness have been associated with telbivudine.58 ALT and AST levels may become elevated while on treatment at rates similar to lamivudine. Telbivudine lacks HIV activity, and it is not recommended for use in patients coinfected with HIV and HBV because HIV drug resistance may develop with telbivudine monotherapy.
Hepatitis C Prevention
The risk factors for hepatitis C and hepatitis B are quite similar; thus, the risk of acquiring the HCV is minimized by avoiding contaminated blood products and high-risk behaviors such as sharing needles among IV drug users. The risk of HCV transmission through a blood transfusion is 1 in 2 million.59 No vaccines are available for preventing hepatitis C, but several are under development.60 High-risk individuals (Table 24–1) should be tested for HCV since most patients will be asymptomatic and unaware they are infected.17
Chronic Hepatitis C Treatment
Individuals with confirmed chronic hepatitis C should be evaluated for treatment with pegylated interferon with or without ribavirin. Interferon α-2a (Roferon A), interferon α-2b (Intron-A), and interferon alfacon-1 (Infergen) are approved for chronic hepatitis C but are no longer recommended because only 12% to 16% of patients achieve an SVR.61,62
Pegylated interferon α-2a (Pegasys) and pegylated interferon α-2b (PEG-Intron) are the preferred treatments for hepatitis C.63,64 Pegylated interferons (interferon attached to polyethylene glycol) have an extended half-life, allowing for once-weekly administration. The SVR to pegylated interferon alone (SVR 25–40%) can be increased by adding ribavirin, a synthetic guanosine analog that inhibits viral polymerase (SVR 45–55%). Consequently, pegylated interferon plus ribavirin is the regimen of choice for chronic hepatitis C.61,62
The most important predictor of response to pegylated interferon is the patient’s genotype. Individuals with genotype 2 or 3 achieve a higher SVR than patients with genotype 1.63,64 Genotype also determines the duration of therapy. The recommended treatment duration for individuals with genotype 2 and 3 is 24 weeks and 48 weeks for genotype 1.61,62
Pegylated interferon is administered subcutaneously and may be given as either a fixed dose or based on body weight. The recommended dose of pegylated interferon α-2a (Pegasys) is 180 mcg once weekly and the adult dose of pegylated interferon α-2b (PEG-Intron) is 1.5 mcg/kg/week.
According to recommended treatment guidelines, the dose of ribavirin is weight based for patients with genotype 1 (less than 75 kg = 1,000 mg daily; 75 kg or more = 1,200 mg daily), whereas genotype 2 and 3 patients receive 800 mg daily regardless of weight.61,62 The ribavirin dose must be reduced in patients with renal impairment and is contraindicated in patients with creatinine clearance less than 50 mL/min.
Adherence to therapy is an important factor in increasing and maintaining SVR. Patients who were adherent with pegylated interferon and ribavirin therapy (taking more than 80% of doses for more than 80% of the treatment duration) had an SVR of 52% whereas those who were not compliant had an SVR of 44%.65
Management of Adverse Effects From Interferon, Pegylated Interferon, and Ribavirin
The type and incidence of adverse effects associated with unmodified interferon and pegylated interferon are similar. Approximately 10% to 30% of patients receiving hepatitis C medications require a dose reduction or treatment discontinuation to minimize side effects.
Most patients treated with pegylated interferon experience flu-like symptoms (fevers, chills, rigors, and myalgias). These symptoms may be mild to moderate in severity and usually occur with the first injection and diminish with continued treatment. The flu-like symptoms may be minimized by premedication with acetaminophen or nonsteroidal anti-inflammatory drugs. Patients may also self-administer pegylated interferon prior to bedtime so they can sleep through it.
Psychiatric adverse effects occur frequently and may include irritability, depression, and rarely, suicidal ideation. Individuals with a history of uncontrolled psychiatric disorders must weigh the risk versus benefit of treatment, as pegylated interferon may exacerbate or worsen the psychiatric condition. Patients who develop mild to moderate psychiatric symptoms may require antidepressants or anxiolytics. Those with severe symptoms including suicidal ideation should discontinue treatment immediately.62
Several hematologic abnormalities are associated with pegylated interferon plus ribavirin therapy. Up to 35% of patients require either a dosage reduction or drug discontinuation due to thrombocytopenia, neutropenia, or anemia.66 A decrease in platelet count of 25% to 30% usually occurs within 6 to 8 weeks after initiation of treatment. Decreasing the dose or discontinuing interferon therapy is rarely required because of significant thrombocytopenia (defined as a platelet count less than 50 × 103/mm3 [less than 50 × 109/L]). However, caution is required in patients with cirrhosis because they may already have low platelet counts prior to starting treatment. Approved therapies for thrombocytopenia are not recommended for interferon-induced thrombocytopenia due to significant adverse effects including pulmonary edema and cardiac arrhythmias. Several pharmacologic agents are under investigation for patients with thrombocytopenia due to chronic liver disease and interferon-induced thrombocytopenia.67 The interferon dose should either be reduced or discontinued if the platelet count declines significantly or symptoms of bruising and bleeding are present.
Neutropenia associated with interferon therapy is defined as an absolute neutrophil count (ANC) of less than 1.0 × 103/mm 3 (1.0 × 1 0 9/L). In rare cases, an ANC less than 0.5 × 103/mm3 (0.5 × 109/L) may be observed. The neutropenia is more common and in some cases more severe with pegylated interferon than with unmodified interferon. Neutropenia usually occurs within the first 2 weeks after initiating either formulation of interferon, with the WBC count stabilizing by week 4 or 6. Neutropenia is reversible upon discontinuing therapy. Granulocyte colony-stimulating factor has been used as an adjunctive therapy for pegylated interferon-induced neutropenia.68,69
Ribavirin causes a dose-related hemolytic anemia, which is more common in patients receiving weight-base dosing than in those taking fixed doses.70 After treatment initiation, the hemoglobin concentration may decrease by 2.5 to 3 g/dL (25–30 g/L or 1.55–1.86 mmol/L) from baseline within 4 weeks. In addition, interferon may slightly suppress bone marrow erythroprogenitor cells. Therefore, a “mixed” anemia (hemolytic anemia and bone marrow suppression occurring simultaneously) develops when both pegylated interferon and ribavirin are used. This is a reversible process with the hemoglobin level returning to baseline within 7 to 8 weeks after either drug has been discontinued. Patients treated taking pegylated interferon and ribavirin may require dosage reductions when hemoglobin levels decrease to less than 10.5 g/dL (105 g/L or 6.51 mmol/L) or they develop intolerable symptoms such as shortness of breath or severe fatigue. Discontinuing ribavirin and blood transfusions may be needed in rare cases when the hemoglobin level falls below 8.5 g/dL (85 g/L or 5.27 mmol/L). If warranted, erythropoietin or darbepoetin-α may be used as adjunctive therapy for ribavirin-induced hemolytic anemia.68,70
All women of childbearing age and men who are able to father a child should use two forms of contraception during ribavirin therapy and 6 months after treatment because ribavirin has been documented to cause teratogenic and embryocidal effects.
Hepatitis D Prevention and Treatment
![]() Hepatitis D infection is possible only if the patient also has the hepatitis B virus present; therefore, hepatitis B vaccination can indirectly prevent hepatitis D infection. Although there are no FDA-approved treatments for hepatitis D, interferon and pegylated interferon have been shown to be effective in normalizing aminotransferase levels and sustaining virologic response.71 Various interferon doses have been evaluated, with the most effective treatment being 9 million units three times weekly.72 Seventy-one percent of patients who were treated with this regimen for 48 weeks had normalized ALT levels.72 Several small trials have evaluated pegylated interferon for HDV with conflicting results.71 Adverse effects and monitoring parameters for interferon and pegylated interferon are similar to treatment for hepatitis C. In some situations, patients infected with hepatitis D who develop hepatic decompensation and ESLD may need to undergo liver transplantation.
Hepatitis D infection is possible only if the patient also has the hepatitis B virus present; therefore, hepatitis B vaccination can indirectly prevent hepatitis D infection. Although there are no FDA-approved treatments for hepatitis D, interferon and pegylated interferon have been shown to be effective in normalizing aminotransferase levels and sustaining virologic response.71 Various interferon doses have been evaluated, with the most effective treatment being 9 million units three times weekly.72 Seventy-one percent of patients who were treated with this regimen for 48 weeks had normalized ALT levels.72 Several small trials have evaluated pegylated interferon for HDV with conflicting results.71 Adverse effects and monitoring parameters for interferon and pegylated interferon are similar to treatment for hepatitis C. In some situations, patients infected with hepatitis D who develop hepatic decompensation and ESLD may need to undergo liver transplantation.
Patient Encounter, Part 2: Creating a Care Plan
Based on the information presented, create a care plan for this patient’s hepatitis. Your plan should include:
(a) a statement of the drug-related needs and/or problems;
(b) the goals of therapy;
(c) a patient-specific detailed therapeutic plan;
(d) a follow-up plan to determine whether the goals have been achieved; and (e) a follow-up plan to identify potential adverse effects of therapy.
Hepatitis E Prevention and Treatment
Hepatitis E is similar to hepatitis A in that the mode of transmission is via the fecal–oral route. Therefore, the most effective ways to prevent acquiring the virus are good personal hygiene and proper disposal of sanitary waste. Frequent handwashing and avoiding contaminated foods and vegetables decrease the risk of infection.
At present, only acute cases of hepatitis E have been documented.21,22 Currently there are no commercially approved vaccines available to prevent hepatitis E; however, a recombinant hepatitis E vaccine undergoing Phase II/III study has produced promising preliminary results.73
OUTCOME EVALUATION
• Monitoring for efficacy in patients treated for chronic hepatitis B or C includes evaluating aminotransferase levels and viral loads.
Patient Encounter, Part 3
The patient has received treatment for hepatitis C for 4 weeks, and the following laboratory results have just been obtained:
• Sodium 138 mEq/L (mmol/L), potassium 4.0 mEq/L (mmol/L), chloride 98 mEq/L (mmol/L), CO2 19 mEq/L (mmol/L), BUN 21 mg/dL (7.50 mmol/L), serum creatinine 1.0 mg/dL (88 μmol/L), glucose 103 mg/dL (5.7 mmol/L)
• Hemoglobin 10.1 g/dL (101 g/L or 6.3 mmol/L), hematocrit 30.3% (0.303), WBC 2.2 × 103/mm3 (× 109/L), platelets 104 × 103/mm3 (× 109/L), ANC 0.92 × 103/mm3 (× 109/L)
• AST 41 IU/L (0.68 μKat/L), ALT 32 IU/L (0.53 μKat/L)
• Total bilirubin 1.0 mg/dL (17.1 μmol/L), albumin 3.6 g/dL (36 g/L), alkaline phosphatase 168 IU/L (2.8 μKat/L),
What questions should you ask the patient?
What action should you take at this time?
Patient Encounter, Part 4
What additional information should you counsel your patient about in addition to the side effects associated with the hepatitis C therapy?
Hepatitis B
• Monitor ALT every 12 weeks and HBV DNA levels every 12 to 24 weeks to determine treatment response in all patients with chronic hepatitis B undergoing HBV therapy.34,35
• Monitor HBeAg and anti-HBe every 24 weeks to determine if seroconversion to anti-HBe occurred or HBeAg was lost in patients with HBeAg-positive chronic hepatitis B.35,74
• Monitor HBsAg every 6 to 12 months to determine if HBsAg was lost or anti-HBs developed in patients with HBeAg-negative chronic hepatitis B with persistently undetectable serum HBV DNA levels.35,74
• Reevaluate the patient at month 6 and add a more potent hepatitis B antiviral agent to the current hepatitis B regimen if the viral count remains 2,000 IU/mL or more.34
• Continue treatment in patients who achieved complete virologic response (HBV DNA level less than 60 IU/mL) by week 24.
• Obtain a CBC with differential every 4 weeks and thyroid stimulating hormone and fasting lipid panel evaluated every 12 weeks in patients undergoing pegylated interferon therapy for hepatitis B.35
• For patients receiving tenofovir or adefovir, monitor serum creatinine for nephrotoxicity at baseline and every 12 weeks.
• For patients taking telbivudine, monitor creatine kinase at baseline and periodically (e.g., every 12 weeks), as muscle weakness and myopathy have been observed with therapy.35,50,51,58
Hepatitis C
• SVR is defined as having an undetectable viral load or HCV RNA level at 6 months post treatment.61,62
• Biochemical response is defined as normalization of ALT; monitor ALT levels every 4 weeks.
• Histologic response is defined as improving inflammation and fibrosis as noted by liver biopsy scores. Repeat liver biopsies are conducted primarily in the setting of clinical trials.
• Check the HCV RNA level at week 12 of therapy to determine the effectiveness of treatment. Discontinue treatment if the HCV RNA has not decreased by at least 2 logs or become undetectable by week 12.
• For patient with genotype 1 HCV: If the HCV RNA level is undetectable at week 12 of therapy, continue treatment for at least another 36 weeks (48 weeks total). Obtain an HCV RNA level to determine end-of-treatment response at the end of the 48-week treatment and repeat at 6 months post-therapy to determine SVR.
• For patients with genotype 2 and 3 HCV: Check the HCV RNA level at week 12. If HCV RNA is undetectable, continue treatment for a total of 24 weeks. Repeat the HCV RNA 24 weeks after completion of therapy to determine SVR.
• In patients receiving treatment with pegylated interferon with or without ribavirin, monitor the WBC, ANC, platelets, and hemoglobin levels either weekly or biweekly during the first month of therapy and monthly thereafter if stable.
Patient Care and Monitoring
1. Evaluate the patient for risk factors for acquiring viral hepatitis (Table 24–1).
2. Educate patients to avoid hepatotoxic agents (e.g., some dietary supplements).
3. Educate patients to avoid consuming any alcohol if viral hepatitis has been diagnosed. Alcohol may further worsen the liver disease and if on treatment, may decrease the effectiveness of therapy.
4. Determine if the patient has been vaccinated against hepatitis A and B. If not, then vaccinate accordingly (Tables 24–3 and 24–4).
5. Obtain a thorough past medical history focusing on psychiatric disorders, cardiac disorders, endocrine disease, and renal insufficiency.
6. Review the liver biopsy report (if available) to determine the severity of liver damage and need for chronic hepatitis B or C treatment.
7. Assess for adverse effects in patients with hepatitis B or C treated with pegylated interferon with or without ribavirin.
8. Encourage medication compliance with viral hepatitis treatments to increase the SVR.
9. Encourage patients to drink at least 8 glasses of water to prevent dehydration while on hepatitis C medications.
10. Educate all women of childbearing age and men who are able to father a child to use two forms of contraception during and 6 months after ribavirin therapy.
11. Provide patient education:
• How to prevent viral hepatitis transmission
• Who should be vaccinated against hepatitis A and B
• Importance of taking all medications at scheduled times
• Adverse effects of interferon, pegylated interferon, and ribavirin therapy
• How to self-administer interferon and pegylated interferon injections
• Importance of appropriate disposal of used needles
• Monitor thyroid stimulating hormone and fasting lipid panel every 12 weeks while on hepatitis C treatment.
• Monitor serum creatinine in patients receiving ribavirin to detect renal insufficiency that may result in ribavirin accumulation and toxicity (e.g., hemolytic anemia).
Abbreviations Introduced in This Chapter


 Self-assessment questions and answers are available at http://www.mhpharmacotherapy.com/pp.html.
Self-assessment questions and answers are available at http://www.mhpharmacotherapy.com/pp.html.
REFERENCES
1. World Health Organization. Department of Communicable Disease Surveillance and Response. WHO/CDS/CSR/EDC/2000.7. http://www.who.int/csr/disease/hepatitis/whocdscsredc2007/en/index.html.
2. Centers for Disease Control and Prevention (CDC). Hepatitis A outbreak associated with green onions at a restaurant—Monaca, Pennsylvania, 2003. MMWR Morb Mortal Wkly Rep 2003;52(47):1155–1157.
3. Wasley A, Samandari T, Bell BP. Incidence of hepatitis A in the U.S. in the era of vaccination. JAMA 2005;294:194–201.
4. Advisory Committee on Immunization Practices (ACIP), Fiore AE, Wasley A, Bell BP. Prevention of hepatitis A through active or passive immunization: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2006;55(RR-7):1–23.
5. Zhou F, Shefer A, Weinbaum C, et al. Impact of hepatitis A vaccination on health care utilization in the U.S., 1996–2004. Vaccine 2007;25:3581–3587.
6. Fiore AE. Hepatitis A transmitted by food. Clin Infect Dis 2004;38:705–715.
7. Keystone JS, Hershey JH. The underestimated risk of hepatitis A and hepatitis B: Benefits of an accelerated vaccination schedule. Int J Infect Dis 2008;12:3–11.
8. World Health Organization. Hepatitis B. http://www.who.int/mediacentre/factsheets/fs204/en/.
9. World Health Organization. Hepatitis B Vaccines. Weekly epidemiological record 2004;79:253–264.
10. Mast EE, Weinbaum CM, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the U.S.: Recommendations of the Advisory Committee on Immunization Practices (ACIP) Part II: Immunization of adults. MMWR Recomm Rep 2006;55(RR-16):1–33.
11. Pan CQ, Zhang JX. Natural history and clinical con-sequences of hepatitis B virus infection. Int J Med Sci 2005;2:36–40.
12. McMahon BJ. The natural history of chronic hepatitis B virus infection. Semin Liver Dis 2004;24(suppl 1):17–21.
13. World Health Organization. Department of Communi-cable Disease Surveillance and Response. WHO/CDS/CSR/LYO/2003. Hepatitis C. http://www.who.int/csr/disease/hepatitis/whocdscsrlyo2003/en/index.html.
14. Rustgi VK. The epidemiology of hepatitis C infection in the U.S. J Gastroenterol 2007;42:513–521.
15. Missiha SB. Ostrowski M. Heathcote EJ. Disease progression in chronic hepatitis C: Modifiable and nonmodifiable factors. Gastroenterology 2008;134:1699–1714.
16. Lauer GM, Walker BD. Hepatitis C virus infection. N Engl J Med 2001;345:41–52.
17. Centers for Disease Control and Prevention. Recommen-dations for prevention and control of hepatitis C virus (HCV) infection and HCV-related chronic disease. MMWR Recomm Rep 1998;47(RR-19):1–39.
18. World Health Organization, Department of Communicable Disease Surveillance and Response. Hepatitis delta. http://www.who.int/csr/disease/hepatitis/HepatitisD_whocdscsrncs2001_1.pdf.
19. Hsieh TH, Liu CJ, Chen DS, Chen PJ. Natural course and treatment of hepatitis D virus infection. J Formos Med Assoc 2006;105:869–881.
20. Shakil AO, Hadziyannis S, Hoofnagle JH, et al. Geographic distribution and genetic variability of hepatitis delta virus genotype I. Virology 1997;160–167.
21. Purcell RH, Emerson SU. Hepatitis E: An emerging awareness of an old disease. J Hepatol 2008;48:494–503.
22. World Health Organization, Department of Communicable Disease Surveillance and Response. Hepatitis E. http://www.who.int/csr/disease/hepatitis/HepatitisE_whocdscsredc2001_12.pdf.
23. Martin A, Lemon SM. Hepatitis A Virus: From Discovery to Vaccines. Hepatology 2006;43(2 Suppl 1):S164–S172.
24. Ganem D, Prince AM. Hepatitis B virus infection-natural history and clinical consequences. N Engl J Med 2004;350:1118–1129.
25. EASL Jury. EASL International Consensus Conference on Hepatitis B: September 13–14, 2002: Geneva, Switzerland. Consensus statement (short version). J Hepatol 2003;38:533–540.
26. Lisker-Melman M, Sayuk GS. Defining optimal therapeutic outcomes in chronic hepatitis. Arch Med Res 2007;38:652–660.
27. Centers for Disease Control and Prevention (CDC). Prevention of hepatitis A after exposure to hepatitis A virus and in international travellers. Updated recommendations of the advisory committee on immunization practices (ACIP). MMWR Recomm Rep 2007;56;41:1080–1084.
28. Victor JC, Monto AS, Surdina TY, et al. Hepatitis A vaccine versus immune globulin for postexposure prophylaxis. N Engl J Med 2007;357:1685–1694.
29. Mast EE, Margolis HS, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the U.S: Recommendations of the Advisory Committee on Immunization Practices (ACIP) part 1: Immunization of infants, children, and adolescents. MMWR Recomm Rep 2005;54(RR-16):1–31.
30. Gabbuti A, Romanò L, Blanc P, et al. Long-term immunogenicity of hepatitis B vaccination in a cohort of Italian healthy adolescents. Vaccine 2007;2 5: 3129–3132.
31. Bialek SR, Bower WA, Novak R, et al. Persistence of protection against hepatitis B virus infection among adolescents vaccinated with recombinant hepatitis B vaccine beginning at birth: A 15-year follow-up study. Pediatr Infect Dis J 2008;27:881–885.
32. Murdoch DL, Goa K, Figgitt DP. Combined hepatitis A and B vaccines: A review of their immunogenicity and tolerability. Drugs 2003;63:2625–2649.
33. National Institutes Of Health Consensus Development Conference Statement. Management of Hepatitis B. October 20–22, 2008. http://consensus.nih.gov/2008/hebB%20draft%20statement%20102208_FINAL.pdf.
34. Keeffe EB, Dieterich DT, Han SH, et al. A treatment algorithm for the management of chronic hepatitis B virus infection in the U.S.: 2008 update. Clin Gastroenterol Hepatol 2008 Aug 23. [Epub ahead of print].
35. Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007;45:507–539.
36. Lau D T-Y, Everhart J, Kleiner DE, et al. Long-term follow-up of patients with chronic hepatitis B treated with interferon alfa. Gastroenterology 1997;113:1660–1667.
37. van Zonneveld M, Honkoop P, Hansen BE, et al. Long-term follow-up of alpha-interferon treatment of patients with chronic hepatitis B. Hepatology 2004;39:804–810.
38. Manesis EK, Hadziyannis SJ. Interferon alpha treatment and retreatment of hepatitis B e antigen-negative chronic hepatitis B. Gastroenterology 2001;121:101–109.
39. Lampertico P, Del Ninno E, Vigano M, et al. Long-term suppression of hepatitis B e antigen-negative chronic hepatitis B by 24-month interferon therapy. Hepatology 2003;37:756–763.
40. Chang TT, Gish RG, de Man R, et al. A comparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B. N Engl J Med 2006;354:1001–1010.
41. Gish RG, Lok AS, Chang TT, et al. Entecavir therapy for up to 96 weeks in patients with HBeAg-positive chronic hepatitis B. Gastroenterology 2007;133(5):1437–1444.
42. Lai CL, Shouval D, Lok AS, et al. Entecavir versus lamivudine for patients with HBeAg-negative chronic hepatitis B. N Engl J Med 2006;354:1011–1020.
43. Sherman M, Yurdaydin C, Sollano J, et al. Entecavir is superior to continued lamivudine for the treatment of lamivudine-refractory, HBeAg(+) chronic hepatitis B: Results of phase III study ETV-026. Hepatology 2004; 40:664A.
44. McMahon MA, Jilek BL, Brennan TP, et al. The HBV drug entecavir: Effects on HIV-1 replication and resistance. N Engl J Med 2007;356:2614–2621.
45. Heathcote EJ, Gane E, DeMan R, et al. A randomized, double-blind, comparison of tenofovir (TDF) versus adefovir dipivoxil (ADV) for the treatment of HBeAg-positive chronic hepatitis B (CHB): Study GS-US-174-0103. Hepatology 2007;46 (Suppl 1):861A.
46. Marcellin P, Buti M, Krastev Z, et al. A randomized, double-blind, comparison of tenofovir (TDF) versus adefovir dipivoxil (ADV) for the treatment of HBeAg-negative chronic hepatitis B (CHB): Study GS-US-174-0102. Hepatology 2007;46(Suppl 1):290A–291A.
47. Leemans WF, Niesters HG, van der Eijk AA, et al. Selection of an entecavir-resistant mutant despite prolonged hepatitis B virus DNA suppression, in a chronic hepatitis B patient with preexistent lamivudine resistance: Successful rescue therapy with tenofovir. Eur J Gastroenterol Hepatol 2008;20:773–777.
48. Reijnders JG, Janssen HL. Potency of tenofovir in chronic hepatitis B: Mono or combination therapy? J Hepatol 2008;48:383–386.
49. Tan J, Degertekin B, Wong SN, et al. Tenofovir mono-therapy is effective in hepatitis B patients with antiviral treatment failure to adefovir in the absence of adefovir-resistant mutations. J Hepatol 2008;48:391–398.
50. Rifkin BS, Perazella MA. Tenofovir-associated nephrotoxicity: Fanconi syndrome and renal failure. Am J Med 2004;117:282–284.
51. Verhelst D, Monge M, Meynard JL, et al. Fanconi syndrome and renal failure induced by tenofovir: A first case report. Am J Kidney Dis 2002; 40:1331–1333.
52. Marcellin P, Chang TT, Lim SG, et al. Adefovir dipivoxil for the treatment of hepatitis B e antigen-positive chronic hepatitis B. N Engl J Med 2003;348:808–816.
53. Hadziyannis SJ, Tassopoulos NC, Heathcote EJ. Adefovir dipivoxil for the treatment of HBeAg-negative chronic hepatitis B. N Engl J Med 2003;348:800–807.
54. Marcellin P, Chang TT, Lim SG, et al. Long-term efficacy and safety of adefovir dipivoxil for the treatment of hepatitis B e antigen-positive chronic hepatitis B. Hepatology 2008;48:750–758.
55. Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al. Long-term therapy with adefovir dipivoxil for HBe Ag-negative chronic hepatitis B for up to 5 years. Gastro-enterology 2006;131:1743–1751.
56. Lai CL, Chien RN, Leung NW, et al. A one-year trial of lamivudine for chronic hepatitis B. Asia Hepatitis Lamivudine Study Group. N Engl J Med 1998;339:61–68.
57. Dienstag JL, Goldin RD, Heathcote EJ, et al. Histological outcome during long-term lamivudine therapy. Gastroenterology 2003;124:105–117.
58. Lai CL, Gane E, Liaw YF, Hsu CW, et al. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med 2007;357:2576–2588.
59. Stramer SL. Current risks of transfusion-transmitted agents: A review. Arch Pathol Lab Med 2007;131:702–707.
60. Strickland GT, El-Kamary SS, Klenerman P, Nicosia A. Hepatitis C vaccine: Supply and demand. Lancet Infect Dis 2008;8:379–386.
61. Dienstag JL, McHutchison JG. American Gastro-enterological Association technical review on the management of hepatitis C. Gastroenterology 2006;130:231–264.
62. Strader DB, Wright T, Thomas DL, Seeff LB; American Association for the Study of Liver Diseases. Diagnosis, management, and treatment of hepatitis C. Hepatology 2004;39:1147–1171.
63. Manns MP, McHutchison JG, Gordon SC, et al. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: A randomised trial. Lancet 2001;358:958–965.
64. Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med 2002;347:975–982.
65. McHutchison JG, Manns M, Patel K, et al. Adherence to combination therapy enhances sustained response in genotype-1-infected patients with chronic hepatitis C. Gastroenterology 2002;123:1061–1069.
66. Fried MW. Side effects of therapy of hepatitis C and their management. Hepatology 2002;36:S237–S244.
67. Afdhal NH, McHutchison JG. Review article: Pharmacological approaches for the treatment of thrombocytopenia in patients with chronic liver disease and hepatitis C infection. Aliment Pharmacol Ther 2007;26 (Suppl 1):29–39.
68. Younossi ZM, Nader FH, Bai C, et al. A phase II dose finding study of darbepoetin alpha and filgrastim for the management of anaemia and neutropenia in chronic hepatitis C treatment. J Viral Hepat 2008;15:370–378.
69. Koirala J, Gandotra SD, Rao S, et al. Granulocyte colony-stimulating factor dosing in pegylated interferon alpha-induced neutropenia and its impact on outcome of anti-HCV therapy. J Viral Hepat 2007;14:782–787.
70. McHutchison JG, Manns MP, Brown RS Jr, et al. Strategies for managing anemia in hepatitis C patients undergoing antiviral therapy. Am J Gastroenterol 2007;102:880–889.
71. Farci P, Chessa L, Balestrieri C, et al. Treatment of chronic hepatitis D. J Viral Hepat 2007;14 (Suppl 1):58–63.
72. Farci P, Roskams T, Chessa L, et al. Long-term benefit of interferon alpha therapy of chronic hepatitis D: regression of advanced hepatic fibrosis. Gastroenterology 2004;126:1740–1749.
73. Shrestha MP, Scott RM, Joshi DM, et al. Safety and efficacy of a recombinant hepatitis E vaccine. N Engl J Med 2007;356:895–903.
74. Hoofnagle JH, Doo E, Liang TJ, et al. Management of hepatitis B: Summary of a clinical research workshop. Hepatology 2007;45:1056–1075.