Steven Gabardi and Ali J. Olyaei
LEARNING OBJECTIVES
Upon completion of the chapter, the reader will be able to:
1. Describe the reasons for solid-organ transplantation.
2. Differentiate between the functions of cell-mediated and humoral immunity and how they relate to organ transplant.
3. Describe the roles of the antigen-presenting cells (APCs) in initiating the immune response.
4. Compare and contrast the types of rejection including hyperacute, acute, chronic, and humoral rejection.
5. Define the terms “host-graft adaptation” and “tolerance,” paying close attention to their differences.
6. Discuss the desired therapeutic outcomes and appropriate pharmacotherapy utilized to avoid allograft rejection.
7. Compare and contrast the currently available immunosuppressive agents in terms of mechanisms of action, adverse events, and drug–drug interactions (DDIs).
8. Design an appropriate therapeutic regimen for the management of immunosuppressive drug complications based on patient-specific information.
9. Develop a therapeutic drug-monitoring plan to assess effectiveness and adverse events of the immunosuppressive drugs.
10. Write appropriate patient education instructions and identify methods to improve patient adherence following transplantation.
KEY CONCEPTS 5
![]() T cells are the chief component initiating the immune response against the allograft. The activity of T cells is mediated largely through the synthesis and release of interleukin-2 (IL-2).
T cells are the chief component initiating the immune response against the allograft. The activity of T cells is mediated largely through the synthesis and release of interleukin-2 (IL-2).
![]() Antigen-presenting cells (APCs) are vital in initiation of the immune response and play a role in both direct and indirect allorecognition.
Antigen-presenting cells (APCs) are vital in initiation of the immune response and play a role in both direct and indirect allorecognition.
![]() The goal of pharmacotherapy in transplantation is to induce immunosuppression with a multidrug approach to target various points of the immune system with resultant long-term allograft and patient survival, while minimizing the complications of suppressing the immune system.
The goal of pharmacotherapy in transplantation is to induce immunosuppression with a multidrug approach to target various points of the immune system with resultant long-term allograft and patient survival, while minimizing the complications of suppressing the immune system.
![]() The goals of induction therapy are to improve short-term allograft and patient survival, and to reduce the incidence of acute rejection in the immediate post-transplant period.
The goals of induction therapy are to improve short-term allograft and patient survival, and to reduce the incidence of acute rejection in the immediate post-transplant period.
![]() The calcineurin inhibitors, cyclosporine and tacrolimus, block T-cell activation by inhibiting the production of IL-2. They are associated with significant adverse events, such as nephrotoxicity, cardiovascular disease, post-transplant diabetes, and neurotoxicity.
The calcineurin inhibitors, cyclosporine and tacrolimus, block T-cell activation by inhibiting the production of IL-2. They are associated with significant adverse events, such as nephrotoxicity, cardiovascular disease, post-transplant diabetes, and neurotoxicity.
![]() The antiproliferatives, azathioprine, and the mycophenolic acid derivatives inhibit T-cell proliferation. Myelosuppression is the most significant adverse event associated with these agents.
The antiproliferatives, azathioprine, and the mycophenolic acid derivatives inhibit T-cell proliferation. Myelosuppression is the most significant adverse event associated with these agents.
![]() Sirolimus, a target of rapamycin inhibitor, works by decreasing the ability of T cells to respond to IL-2. The major adverse events associated with this agent are decreased wound healing, hyperlipidemia and myelosuppression. This agent appears to have promising effects in allowing for calcineurin inhibitor withdrawal in some patient populations.
Sirolimus, a target of rapamycin inhibitor, works by decreasing the ability of T cells to respond to IL-2. The major adverse events associated with this agent are decreased wound healing, hyperlipidemia and myelosuppression. This agent appears to have promising effects in allowing for calcineurin inhibitor withdrawal in some patient populations.
![]() Corticosteroids induce a nonspecific immuno-suppression. Due to their overwhelming incidence of adverse events, many practitioners attempt to use low-dose maintenance therapy or, in some cases, complete steroid withdrawal. These agents are also effective in reversing acute rejection.
Corticosteroids induce a nonspecific immuno-suppression. Due to their overwhelming incidence of adverse events, many practitioners attempt to use low-dose maintenance therapy or, in some cases, complete steroid withdrawal. These agents are also effective in reversing acute rejection.
![]() Long-term patient and allograft survival is complicated by several factors, including drug–drug interactions (DDIs) with the immunosuppressive agents, infectious disease, cardiovascular disease, new onset diabetes after transplant, and malignancy. The goals of treating these complications are to prevent allograft damage and improve patient survival.
Long-term patient and allograft survival is complicated by several factors, including drug–drug interactions (DDIs) with the immunosuppressive agents, infectious disease, cardiovascular disease, new onset diabetes after transplant, and malignancy. The goals of treating these complications are to prevent allograft damage and improve patient survival.
INTRODUCTION
The earliest recorded attempts at organ transplant date back thousands of years.1 More than a few apocryphal descriptions exist from ancient Egypt, China, India, and Rome describing experimentation with transplantation. For example, an Indian text from 2nd century BC describes the procedure for nasal reconstruction surgery with the use of autografted skin. Also, Roman Catholic lore has saints Damian and Cosmas replacing the gangrenous leg of a man with the leg of a recently deceased man in the third century AD.1
French surgeon, Alexis Carrel, pioneered the art of surgical techniques for transplantation in the early 1900s.1 Together with Charles Guthrie, Carrel experimented in artery and vein transplantation. Using revolutionary methods in anastomosis operations and suturing techniques, Carrel laid the groundwork for modern transplant surgery. He was one of the first to identify the dilemma of rejection, an issue that remained nearly impossible to circumvent for nearly half a century.1
Prior to the work of Alexis Carrel, malnourishment was the prevailing theory regarding the mechanism of allograft rejection.1 However, in 1910, Carrel noted that tissue damage in the transplanted organ was likely caused by multiple, circulating biological factors. It was not until the late 1940s with the work of Peter Medawar that we began to gain a better understanding of transplant immunology. Medawar was able to define the immunologic nature of rejection using skin allografts. In addition, George Snell observed that grafts shared between inbred animals were accepted but were rejected when transplanted between animals of different strains.1
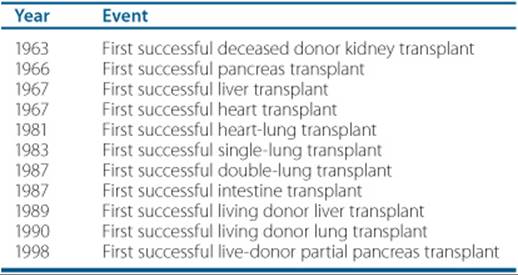
Table 55–1 Solid Organ Transplant History
The seminal work by early transplant researchers event uallyled to the concept of histocompatibility1,2 Histocompati-bility describes the process where polymorphic genes encode cell membrane antigens that serve as targets for immune response, even within a species. Further research in transplant immunobiology has led to an accurate understanding of the immune response after transplantation.1,2
Joseph Murray performed the first successful organ transplant in 1954.1 It was a kidney transplant between identical twins. This was a success in large part because no immunosuppression was necessary due to the fact that the donor and recipient were genetically identical. Murray’s success led to attempts with other organs (Table 55–1).
EPIDEMIOLOGY AND ETIOLOGY
Heart
Nearly five million Americans are afflicted with heart failure.1,3 Cardiac transplantation is one option for patients with severe congestive heart failure. Candidates for cardiac transplantation generally present with New York Heart Association (NYHA) class III or IV symptoms and have an ejection fraction of less than 20%. The general indications for cardiac transplantation include rapidly declining cardiac function and having a projected 1-year mortality rate of greater than 75%. Mechanical support with an implantable left ventricular assist device may be appropriate as bridge therapy while patients await the availability of a viable organ.1,3 Indications for heart transplant include:
• Cardiomyopathy (i.e., dilated myopathy, hypertrophic cardiomyopathy, restrictive myopathy)
• Congenital heart disease
• Coronary artery disease
• Valvular heart disease
Most heart transplants are orthotopic; however, in certain situations, heterotopic cardiac transplants have been performed. There have been a handful of cardiac transplants that involved living donation. Although this seems strange, this occurs when one patient receives a simultaneous heart-lung transplant, but their native heart is well functioning and may be subsequently transplanted into another recipient. This procedure is referred to as a “domino” heart transplant. There were 1,852 heart transplant procedures done in 2009.3
Intestine
An intestine transplant may involve the use of an entire intestine or just a shortened segment. The majority of intestine transplants completed in the United States have involved the transplant of the full organ and are often performed in conjunction with a liver transplant. Although most intestine transplants involve organs harvested from a deceased donor, recent advances in the field have made it possible for living donor intestinal segment transplants. There were 155 intestine transplants (152 deceased donors, 2 living donors) done in 2009.3 Reasons for intestine transplant include:
• Functional bowel problems (i.e., Hirschsprung’s disease, neuronal intestinal dysplasia, pseudoobstruction, protein-losing enteropathy, microvillous inclusion disease)
• Short gut syndrome (i.e., intestinal artresia, necrotizing enterocolitis, intestinal volvulus, massive resection secondary to inflammatory bowel disease, tumors, mesenteric thrombosis)
Kidneys
Over 20 million Americans have chronic kidney disease (CKD), with another 20 million more considered to be at increased risk for the development of kidney disease. End-stage renal disease (ESRD) only constitutes a small portion of those patients with CKD, with over 450,000 patients currently diagnosed with ESRD throughout the United States. However, the ESRD population continues to increase, with projections estimating that more than 660,000 people will carry a diagnosis of ESRD by 2010. All patients with ESRD should be considered for renal transplantation if they are healthy enough to undergo the transplant surgery. A successful kidney transplant offers advantages in terms of both quality and duration of life compared to other renal replacement therapies (i.e., hemodialysis, peritoneal dialysis). It is also more effective than dialysis from a medical and economic perspective. Reasons for kidney transplant include:
• Congenital, familial, and metabolic disorders (i.e., congenital obstructive uropathy, Fabry’s disease, medullary cystic disease, nephrolithiasis)
• Diabetes mellitus (DM)
• Glomerular diseases (i.e., antiglomerular basement membrane disease, focal segmental glomerularsclerosis, IgA nephropathy, hemolytic uremic syndrome, systemic lupus erythematosus, Alport’s syndrome, amyloidosis, membranous nephropathy, Goodpasture’s syndrome)
• Hypertension
• Neoplasm (i.e., renal cell carcinoma, Wilms’ tumor)
• Polycystic kidney disease (PKD)
• Renovascular disease
• Tubular and interstitial diseases (i.e., analgesic nephropathy, drug-induced nephritis, oxalate nephropathy, radiation nephritis, acute tubular necrosis, sarcoidosis)
Most kidney transplant procedures are heterotopic, where the kidney is implanted above the pelvic bone and attached to the patient’s iliac artery and vein. The ureter of the transplant kidney is attached directly to the recipient’s bladder or native ureter. The native kidneys are usually not removed, and data have shown that under most circumstances, removal of the native kidneys does not influence patient and allograft survival. However, special circumstances, such as renal cell carcinoma and PKD, may necessitate native kidney removal.1,3 There were 14,059 (8,812 deceased donors, 5,247 living donors) kidney transplants done in 2009.3
Liver
A liver transplant may involve the use of the entire organ or a segment of the liver. The majority of cases involve utilizing the full organ (deceased donor); however, segmental transplants are gaining popularity. In recent years, segmental transplants have been conducted using living donors. This procedure requires donation of the left hepatic lobe, which accounts for nearly 60% of the overall liver mass. This type of procedure is possible because the liver can regenerate; therefore, both the donor and recipient, in theory, will have normal liver function shortly after the transplant procedure.1,3 There were 5,316 (5,124 deceased donors, 192 partial lobe-living donors) liver transplants done in 2009.3 Reasons for liver transplant include:
• Acute hepatic necrosis (i.e., chronic or acute hepatitis B or C)
• Biliary atresia
• Cholestatic liver disease/cirrhosis (i.e., primary biliary cirrhosis)
• Metabolic disease (i.e., Wilson’s disease, primary oxalosis, hyperlipidemia)
• Neoplasms (i.e., hepatoma, cholangiocarcinoma, hepatoblastoma, bile duct cancer)
• Noncholestatic cirrhosis (i.e., alcoholic cirrhosis, postnecrotic cirrhosis, drug-induced cirrhosis)
Lungs
Lung transplants may involve deceased donation of two lungs or a single lung. More recently, lobar transplants from blood group compatible living donors have been performed for a small segment of the population. Most of the lobar transplants have been performed on cystic fibrosis patients. On rare occasions, a simultaneous heart-lung transplant occurs. This type of procedure is reserved for patients with severe pulmonary and cardiac disease. There were 1,392 (1,391 deceased donors, 1 living donor) lung transplants and 23 simultaneous heart-lung transplant procedures done in 2009.3 Reasons for lung transplant include:
• α-1-Antitrypsin deficiency
• Congenital disease (i.e., Eisenmenger’s syndrome)
• Cystic fibrosis
• Emphysema/chronic obstructive pulmonary disease
• Idiopathic pulmonary fibrosis
• Primary pulmonary hypertension
Pancreas
The exact nationwide prevalence of all diseases of the pancreas has not been fully quantified; however DM, both types 1 and 2, affects nearly 21 million people in the United States alone. Some people suffering from DM may also be afflicted with ESRD. A small percentage of these patients may undergo a simultaneous pancreas-kidney (SPK) transplant, which may be accomplished using organs from deceased or living donors. There were 325 pancreas transplants and 724 SPK procedures done in 2009.3 Reasons for pancreas transplants include:
• DM (i.e., type 1 and 2, DM secondary to chronic pancreatitis, DM secondary to cystic fibrosis)
• Pancreatic cancer
Transplant of a pancreas may involve either the entire organ or a pancreas segment. Currently, whole organ transplant is the most common procedure, with a portion of the duodenum often transplanted along with the pancreas. Living donors are often the source of segmental transplants. In recent years, isolation and transplantation of β islet cells alone have been completed. Islet transplantation is intended to treat organ dysfunction by replacing nonfunctioning islet cells with new ones. In most cases no surgery is needed, and islet cells from a deceased donor’s pancreas are removed and infused into a portal vein of the patient. Islet transplants are still considered experimental, and long-term benefit and/or risk of this procedure needs to be studied extensively.
PATHOPHYSIOLOGY
Major Histocompatibility Complex
The primary target of the immune response against a transplanted organ is the major histocompatibility complex (MHC).1,2 The MHC is a region of highly polymorphic genes located on the short arm of chromosome six. The human MHC is referred to as human leukocyte antigen (HLA). HLA are a set of glycoproteins that are expressed on the surface of most cells. These proteins are involved in immune recognition, which is the discrimination of self from nonself, but are also the principal antigenic determinants of allograft rejection.1,2
The protein products of the HLA have been classified into two major groups, Class I and II:
• Class I: these molecules are expressed on the surfaces of all nucleated cells and are recognized by CD8+ cells, also known as cytotoxic T cells.
• The three subclasses of MHC Class I are HLA-A, HLA-B, and HLA-C.
• Class II: these molecules are expressed solely on the surfaces of antigen-presenting cells (APCs). The APCs serve to stimulate CD4+ cells, also known as helper T cells.
• The three subclasses of MHC Class II are HLA-DP, HLA-DQ, and HLA-DR.
T and B Lymphocytes
Lymphocytes are one of the five kinds of white blood cells. Mature lymphocytes are astonishingly diverse in their functions. The most abundant of the lymphocytes are T lymphocytes (also called T cells) and B lymphocytes (also called B cells).
T Lymphocytes
![]() T cells play a major role in the cell-mediated immuneresponse. These cells are produced in the bone marrow but their final stage of development occurs in the thymus, hence the abbreviation “T.” There are three recognized subclasses of T cells.
T cells play a major role in the cell-mediated immuneresponse. These cells are produced in the bone marrow but their final stage of development occurs in the thymus, hence the abbreviation “T.” There are three recognized subclasses of T cells.
• Cytotoxic T cells (CD8+) promote target cell destruction by activating cellular apoptosis or aggressively killing the target cell via the release of cytotoxic proteins.
• Helper T cells (CD4+) are the great communicators of the immune response. Once activated, they proliferate and secrete cytokines that regulate effector cell function. Some helper T cells secrete cytokines that recruit cytotoxic T cells, B cells, or APCs, while others secrete cytokines that turn off the immune response once an antigen has been destroyed.
• Regulatory T cells, or suppressor T cells, suppress the activation of an immune response. The activity of these cells in organ transplant is not well elucidated.
B Lymphocytes
B cells play a large role in the humoral immune response. In humans, B cells are produced and mature in the bone marrow. The human body produces several types of B cells. Each B cell is unique, with a distinctive cell surface receptor protein that binds to only one particular antigen. Once B cells encounter their antigen and receive a cytokine signal from helper T cells, they can further differentiate into one of two cells, plasma B cells or memory B cells. Plasma B cells secrete antibodies that induce the destruction of target antigens through a process known as opsonization. Memory B cells play an important role in long-term immunity. Once formed to a specific antigen, memory B cells are capable of rapidly responding to subsequent exposures to their target antigen.
Antigen-Presenting Cells
![]() APCs are vital in initiation of the immune response. An APC is a cell that displays a foreign antigen complexed with MHC on its cell surface. Its major responsibility is to present these foreign antigens to T cells. T cells can identify this complex using their T-cell receptors (TCRs). There are three main types of APCs: dendritic cells (DCs), macrophages, and activated B cells. DC are present in tissues that are in contact with the environment, such as the skin and the lining of the nose, lungs, stomach, and intestines. They are responsible for antigen phagocytosis. After phagocytosis, they express the foreign antigen on their cell surface and then migrate to the lymphoid tissues to interact with T and B cells to initiate the immune response. Macrophages’ main role is in the removal of pathogens and necrotic debris. However, like DCs, macrophages also phagocytize antigens and express them on their cell membranes to present to T cells in order to initiate an immune response. The first time an antigen is encountered, the DCs and macrophages act as the primary APCs. However, if the same antigen is encountered again, memory B cells become the most important APC because they initiate the immune response quickly after antigen presentation. It appears that both the DCs and macrophages have the most activity in terms of allorecognition.
APCs are vital in initiation of the immune response. An APC is a cell that displays a foreign antigen complexed with MHC on its cell surface. Its major responsibility is to present these foreign antigens to T cells. T cells can identify this complex using their T-cell receptors (TCRs). There are three main types of APCs: dendritic cells (DCs), macrophages, and activated B cells. DC are present in tissues that are in contact with the environment, such as the skin and the lining of the nose, lungs, stomach, and intestines. They are responsible for antigen phagocytosis. After phagocytosis, they express the foreign antigen on their cell surface and then migrate to the lymphoid tissues to interact with T and B cells to initiate the immune response. Macrophages’ main role is in the removal of pathogens and necrotic debris. However, like DCs, macrophages also phagocytize antigens and express them on their cell membranes to present to T cells in order to initiate an immune response. The first time an antigen is encountered, the DCs and macrophages act as the primary APCs. However, if the same antigen is encountered again, memory B cells become the most important APC because they initiate the immune response quickly after antigen presentation. It appears that both the DCs and macrophages have the most activity in terms of allorecognition.
Allorecognition
![]()
![]() Recognition of the antigens displayed by the transplanted organ (alloantigens) is the prime event that initiates the immune response against the allograft. There are currently two accepted pathways for T-cell allorecognition, direct and indirect pathways:
Recognition of the antigens displayed by the transplanted organ (alloantigens) is the prime event that initiates the immune response against the allograft. There are currently two accepted pathways for T-cell allorecognition, direct and indirect pathways:
• Direct pathway: donor APCs migrate out of the allograft into the recipient’s lymph nodes and present donor MHC molecules to the TCR of the recipient’s T cells.
• Indirect pathway: recipient APCs migrate into the graft and phagocytize alloantigens. The donor MHC molecules are then expressed on the cell surface of the recipient’s APCs and presented to recipient T cells in the lymph nodes.
T-cell activation
![]() Whether it is by the direct or indirect pathway, in order for a T cell to become activated against the transplanted organ, two interactions, or signals must take place between the APCs and the recipient’s T cells1,2:
Whether it is by the direct or indirect pathway, in order for a T cell to become activated against the transplanted organ, two interactions, or signals must take place between the APCs and the recipient’s T cells1,2:
• Signal 1 is the interaction of the TCR with the foreign antigens presented by the APCs.
• A second, costimulatory signal, known as Signal 2, must also take place for T-cell activation. This signal is an interaction between one of several costimulatory receptors and paired ligands on the cell surfaces of the APCs and T cells, respectively. This interaction is of the utmost importance, as Signal 1 in the absence of Signal 2 induces T-cell anergy.
Once activated, T cells undergo clonal expansion under the influence of cytokines, specifically interleukin-2 (IL-2). These steps elicit an antidonor T-cell response that results in graft destruction.
Mechanisms of Acute Rejection
After activation, cytotoxic T cells emerge from lymphoid organs to infiltrate the graft and trigger the immune response. These cells have been shown to induce graft destruction via two mechanisms: (a) secretion of the cytotoxic proteins perforin and granzyme B and (b) induction of cellular apoptosis through interaction with various cell surface receptors. Besides the cytotoxic T cells, several other cell lines may play a role in allograft destruction including B cells, granulocytes, and natural killer cells.
Types of Rejection
Hyperacute Rejection
Hyperacute rejection is an immediate recipient immune response against the allograft due to the presence of preformed recipient antibodies directed against the donor’s HLA. This type of reaction generally occurs within minutes of the transplant. The organ must be removed immediately to prevent a severe systemic response. Those patients at highest risk for hyperacute rejection include any patients that have preformed HLA or ABO blood group antibodies, including patients with a history of a previous organ transplant, or multiple blood transfusions, as well as mothers receiving transplanted organs from their children. Hyperacute rejection has been largely eliminated due to routine surveillance testing completed prior to the transplant.
Acute Rejection
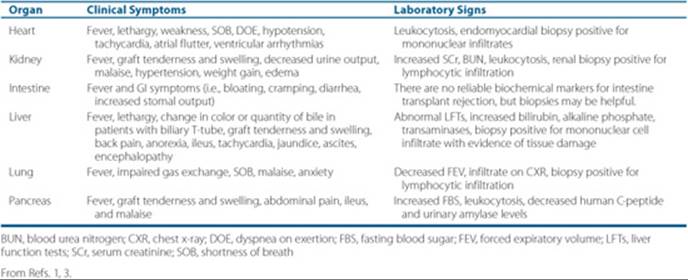
Acute rejection is a cell-mediated process that generally occurs within 5 to 90 days after the transplant procedure; however, it can occur at any time post-transplant. This reaction is mediated through alloreactive T cells as discussed previously in the Mechanisms of Acute Rejection section. Organ specific signs and symptoms of acute rejection can be seen in Table 55–2.1,3
To avoid acute or chronic rejection, assessment of pretransplant immune risk factors of recipients plays an important role in the prevention of immune-mediated allograft injuries. Evaluation of the presence or absence of alloantibodies and T cell activities to HLA antigens plays a significant role in individualization of immunosuppressive therapy. Patients with a high panel of reactive antibodies (PRA) have a greater risk of immune mediated injuries to the transplanted allograft. The PRA test measures the recipient’s mismatches and preformed antibodies against 50 to 60 different individuals (not donor).4 If 25 cells react, it is considered 50% reactive (PRA of 50%). Patients with higher PRAs and preformed antibodies have lower long-term allograft survival. Although PRA is a sensitive test and has predictive value, lymphocytes directly obtained from donor is a superior method of immune monitoring before and early after transplant.4 The assay is aimed to detect the presence of antibodies directed against the HLA antigens of the donor. In this setting, presence of donor-specific antibodies (DSA) are identified. In one study, the allograft survival was significantly lower in patients with DSA. Thus, detecting DSA and presence of high PRA may indicate the need to enhance immunosuppression to improve post-transplant long-term outcomes and allograft survival rate.
Humoral Rejection
Also known as antibody-mediated rejection, humoral rejection is the process of creating graft-specific antibodies.1,5 This type of rejection occurs less frequently than cell-mediated acute rejection. Humoral rejection is characterized by deposition of immunoglobulins and complement in allograft tissues. Treatment for this type of rejection is not well defined; yet several reports have shown that treatments such as plasmapheresis, immunoglobulin therapy, rituximab and/or antithymocyte globulin, or other B cell targeted agents may be effective.
Table 55–2 Organ-Specific Signs and Symptoms of an Acute Rejection Episode
Chronic Rejection
Chronic rejection has traditionally been thought of as a slow, insidious form of acute rejection, resulting in worsening organ function over time. The exact immunologic processes of chronic rejection are poorly understood; however, many believe that both the cell-mediated and humoral immune systems and drug-induced toxicities play a vital role in its development. Currently, retransplantation is the only effective treatment option.1,6
Host-Graft Adaptation
The term host-graft adaptation describes the decreased immune response against the allograft over time.2 This phenomenon is evident by the reduced incidence of acute rejection episodes seen months after the transplant procedure. In theory, host-graft adaptation is thought to be secondary to a weakened T-cell response to the donor antigens when patients are receiving maintenance immunosuppression.2
Tolerance
Tolerance is the process that allows organ-specific antigens to be accepted as self.2,7 This would mean that the immune system would cease to respond to the allograft and immunosuppressive medications would not be required. Immune tolerance has been achieved in the lab, but has yet to be successfully accomplished in humans.2,7 The definition of “achieved tolerance” is highly variable and subjective. Currently, a number of protocols focusing on testing clinically-safe regimens to achieve chimerism or tolerance are being studied.
TREATMENT
Desired Outcome
![]() The major focus of transplant practitioners is to achieve long-term patient and allograft survival.2,8 Short-term outcomes (e.g., acute rejection rates, 1-year graft survival) have improved significantly since the first successful transplant due to an improved understanding of the immune system and enhancements in surgical techniques, organ procurement, immunosuppression, and post-transplant care. Despite the success in improving short-term outcomes, the overall frequency of graft loss remains higher than desired.1,2
The major focus of transplant practitioners is to achieve long-term patient and allograft survival.2,8 Short-term outcomes (e.g., acute rejection rates, 1-year graft survival) have improved significantly since the first successful transplant due to an improved understanding of the immune system and enhancements in surgical techniques, organ procurement, immunosuppression, and post-transplant care. Despite the success in improving short-term outcomes, the overall frequency of graft loss remains higher than desired.1,2
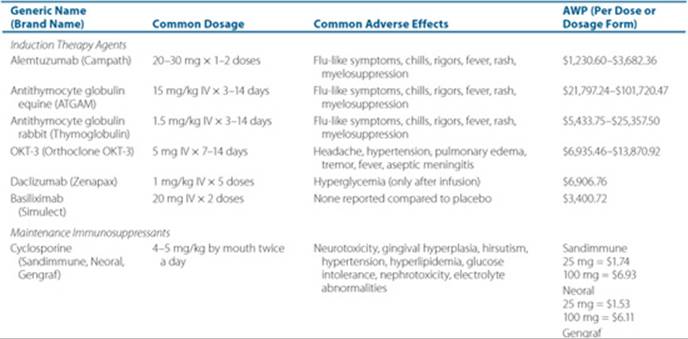
It is imperative that transplant practitioners be aware of the specific advantages and disadvantages of the available immunosuppressants, as well as their adverse drug reaction and drug-drug interaction (DDI) profiles. There are generally considered to be three stages of medical immunosuppression: (a) induction therapy, (b) maintenance therapy, and (c) treatment of acute rejection episodes. ![]() Overall, the immunosuppressive regimens utilize multiple medications that work on different targets of the immune system. Please refer to Table 55–3 for a list of all currently available immunosuppressive agents.2,8,9
Overall, the immunosuppressive regimens utilize multiple medications that work on different targets of the immune system. Please refer to Table 55–3 for a list of all currently available immunosuppressive agents.2,8,9
Immunosuppressive Therapies—Induction Therapy
![]() The goal of induction therapy is to provide a high level of immunosuppression in the critical early post-transplant period, when the risk of acute rejection is highest.2,8,10–12 This stage of immunosuppression is often initiated intraoperatively or immediately postoperatively and is generally concluded within the first 7 to 10 days after transplantation. Induction therapy is not a mandatory stage of recipient immuno-suppression. However, since acute rejection is a major concern in solid organ transplant recipients and its impact on chronic rejection is undeniable, induction therapy is often considered essential to optimize outcomes.2,8,10–12
The goal of induction therapy is to provide a high level of immunosuppression in the critical early post-transplant period, when the risk of acute rejection is highest.2,8,10–12 This stage of immunosuppression is often initiated intraoperatively or immediately postoperatively and is generally concluded within the first 7 to 10 days after transplantation. Induction therapy is not a mandatory stage of recipient immuno-suppression. However, since acute rejection is a major concern in solid organ transplant recipients and its impact on chronic rejection is undeniable, induction therapy is often considered essential to optimize outcomes.2,8,10–12
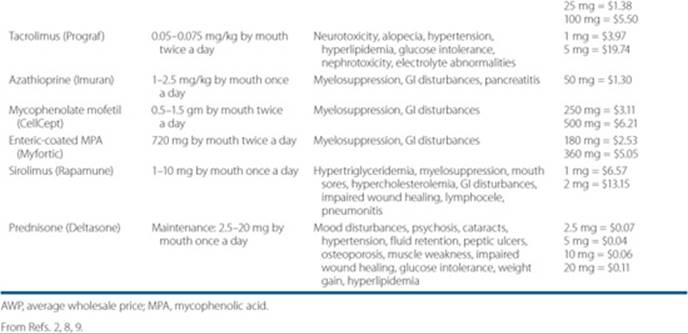
Table 55–3 Currently Available Immunosuppressive Agents
Goals of Induction Therapy
![]() First, the induction agents are highly immunosuppressive, allowing for significant reductions in acute rejection episodes and improved 1-year graft survival. Second, due to their unique pharmacologic effect, these agents are often considered essential for use in patients at high risk for poor short-term outcomes, such as those patients with preformed antibodies, history of previous organ transplants, multiple HLA mismatches, or transplantation of organs with prolonged cold ischemic time, or from expanded criteria donors. Specifically in renal transplant recipients, induction therapy plays an important role in preventing early onset calcineurin inhibitor-induced nephrotoxicity. With the use of induction agents, initiation of calcineurin inhibitors can be delayed until the graft regains a modicum of function.8,11,12
First, the induction agents are highly immunosuppressive, allowing for significant reductions in acute rejection episodes and improved 1-year graft survival. Second, due to their unique pharmacologic effect, these agents are often considered essential for use in patients at high risk for poor short-term outcomes, such as those patients with preformed antibodies, history of previous organ transplants, multiple HLA mismatches, or transplantation of organs with prolonged cold ischemic time, or from expanded criteria donors. Specifically in renal transplant recipients, induction therapy plays an important role in preventing early onset calcineurin inhibitor-induced nephrotoxicity. With the use of induction agents, initiation of calcineurin inhibitors can be delayed until the graft regains a modicum of function.8,11,12
The improved short-term outcomes gained from induction therapy come with a degree of risk. By using these highly immunosuppressive agents, particularly the antilymphocyte antibodies (ALA; Muronomab-CD3 [OKT-3], the antithymocyte antibodies, and alemtuzumab), the body loses much of its innate ability to mount a cell-mediated immune response, which increases the risk of opportunistic infections and malignancy.8,12 Cytokine release syndrome is a common complication of T-cell depleting agents following first two doses and require methylprednisolone, diphenhydramine, and acetaminophen 30 to 60 minutes before infusion.
Currently Available Induction Therapies
Please note that declining worldwide use and the expense associated with manufacturing both muromonab-CD3 and daclizumab have led the makers of these agents to decide to discontinue their production. At the time of this publication, it is expected that the current supply of muromonab-CD3 will last through the end of 2010 and the current supply of daclizumab will last through 2011. Once these supplies have been exhausted, these agents will no longer be available for clinical use.
Basiliximab and Daclizumab
Both of these agents are monoclonal antibodies. Daclizumab is a humanized antibody that is approximately 10% murine and 90% human, while basiliximab is a chimeric antibody that is approximately 30% murine and 70% human.8,10 These agents bind with high affinity to the IL-2 receptor where they act as receptor antagonists. These receptors are present on almost all activated T cells. Their role in induction therapy involves inhibiting IL-2 mediated activation of lymphocytes, which is an important step for the clonal expansion of T cells.
The dose of basiliximab is 20 mg IV given within 2 hours prior to the transplant, followed by a second 20 mg dose on postop day 4.8,9,11 This dosing schedule can be used for both children greater than or equal to 35 kg (77 lb) and adults. Two 10 mg doses with the same dosing schedule should be used for children less than 35 kg (77 lb). There is no specific dosage adjustments needed in renal or hepatic impairment.8,9,11
The FDA-approved dose of daclizumab is 1 mg/kg within 24 hours of transplant surgery and then 1 mg/kg administered every 2 weeks after surgery for a total of five doses.8,9,11 No dose adjustment is necessary in renal impairment but no data are available for dose adjustments in hepatic dysfunction. Several trials have shown that a shorter dosing regimen of daclizumab, two doses given in a similar manner as basiliximab, may be as safe and effective as the full, five-dose course.13,14
Safety is one of the most evident benefits of induction therapy with the IL-2 receptor antibodies. The most common adverse reaction with daclizumab is hyperglycemia, with clinical studies showing that a total of 32% of patients developed hyperglycemia.9,11 The majority of the high glucose levels occurred the day after transplant or in patients with pre-existing DM. All other adverse events in the daclizumab clinical trials showed no statistically significant difference compared to placebo. The incidence of all adverse reactions with basiliximab was similar to placebo in clinical trials.10,12
Antithymocyte Globulin Equine
Antithymocyte globulin equine (eATG) contains antibodies against several T-cell surface markers, including CD2, CD3, CD4, CD8, CD11a, and CD18. After binding to these cell surface markers, eATG promotes T-cell depletion through opsonization and complement-mediated T-cell lysis.8–10 The common dosing strategy for eATG when used for induction therapy is 10 to 30 mg/kg/day IV for 3 to 14 days. The first dose usually begins shortly before or after transplantation.8–10
After T-cell lysis there is a cytokine release. Due to this phenomenon, eATG is associated with several adverse reactions.8–10 The most common of these include fever (63%), chills (43.2%), headache (34.6%), back pain (43.2%), nausea (28.4%), diarrhea (32.1%), dizziness (24.7%), malaise (3.7%), and myelosuppression (leukopenia [29.6%] and thrombocytopenia [44.4%]). The overall incidence of opportunistic infections is 27.2%, with cytomegalovirus (CMV) disease occurring in 11.1% of patients. There are currently no reported pharmacokinetic DDIs with this agent.8–10
Antithymocyte Globulin Rabbit (Thymoglobulin)
Thymoglobulin induces T-cell clearance, but more importantly, it alters T-cell activation, homing, and cytotoxic activities. Compared to eATG, thymoglobulin causes less T-cell lysis due to its multiple mechanisms of immunosuppre-ssion. It is also believed that thymoglobulin plays a role in inducing T-cell apoptosis. Thymoglobulin has been dosed between 1 and 4 mg/kg/day (typically dosed at 1.5 mg/kg/day) and is usually administered for 3 to 10 days after transplantation.8–10 Many renal transplant centers aim to initiate the first dose intraoperatively to help reduce organ reperfusion injury.
Adverse reactions are common and may include fever (63.4%), chills (57.3%), headache (40.2%), nausea (36.6%), diarrhea (36.6%), malaise (13.4%), dizziness (8.5%), leukopenia (57.3%), thrombocytopenia (36.6%), and generalized pain (46.3%).8,10 The incidence of infection is 36.6%, with CMV disease occurring in 13.4% of patients. There are no reported DDIs with the use of thymoglobulin at this time.8–10
Muronomab-CD3
OKT-3 is a murine monoclonal antibody that targets the CD3 receptor. The CD3 receptor is only found on activated T cells and medullary thymocytes.9,12,15 Binding of this agent to the CD3 receptor inactivates the adjacent TCR portion of the T lymphocyte cell membrane, preventing the activation of T lymphocytes. After the first dose of OKT-3, lymphocytes are removed from circulation via opsonization. The lymphocyte count falls precipitously within a few hours of administration of OKT-3.
This agent is dosed at 5 mg/day and is given daily for 10 to 14 days. Lower doses have been used successfully in all organ transplant recipients (2 mg IV/day).15
Due to its ability to cause widespread T-cell lysis after the first dose, OKT-3 has several severe adverse events that manifest within a few hours after administration.9,12,15 These adverse reactions are often referred to as the “first-dose effect” and are usually secondary to cytokine release. The adverse reaction profile of OKT-3 includes fever (77%), chills (43%), dyspnea (16%), nausea (32%), vomiting (25%), diarrhea (37%), and tachycardia (26%). Due to a number of severe and potentially fatal reactions, today the role of OKT-3 is limited to the treatment of severe acute rejection refractory to other T cell depleting agents. One of the major complications of OKT-3 is the development of severe pulmonary edema.9,16,17 In reported cases of this complication, most patients were fluid overloaded at the time of the initial dose. Thus, chest X-ray to rule out any evidence of fluid overload is a must before administration of OKT-3 for the treatment of acute cellular rejection. Another problematic adverse reaction is the development of cytokine nephropathy.9,18 The herbal product echinacea has been theorized to interact with OKT-3, due to echinacea’s proposed ability to stimulate the immune system.9
Alemtuzumab
Alemtuzumab is a recombinant DNA-derived monoclonal antibody that binds to CD52. CD52 is present on the surface of almost all B and T lymphocytes, many macrophages, NK cells, and a subpopulation of granulocytes. This agent’s mechanism of action is believed to be antibody-dependent cell lysis following its binding to CD52 cell surface markers. When used for induction therapy, alemtuzumab produces a rapid and extensive lymphocyte depletion that may take several months to return to pretransplant levels. Although it is not FDA-approved for use in organ transplantation, studies have demonstrated a dose of 20 to 30 mg on day zero and again on either postoperative day 1 or 4 to be effective in preventing acute rejection. However, current studies are evaluating the use of a single 30 mg dose given on postoperative day zero (i.e., the hours immediately following surgery), which has been shown to be as effective but better tolerated than ATG induction.
Alemtuzumab has been associated with serious adverse reactions that include anemia (47%), neutropenia (70%), thrombocytopenia (52%), headache (24%), dysthesias (15%), dizziness (12%), nausea (54%), vomiting (41%), diarrhea (22%), autoimmune hemolytic anemia (rare), infusion-related reactions (15–89%), and infection (37%; CMV viremia occurred in 15% of patients). The FDA recommends that premedication with acetaminophen and oral antihistamines are advisable to reduce the incidence of infusion-related reactions.
Comparative Efficacy—Induction Therapy Agents
The improvements in short-term outcomes gained from the use of induction therapies cannot be denied. However, despite these advances, use of induction therapy has not impacted long-term allograft function or survival. There are a few studies that help to delineate the ideal induction therapy agent. For example, studies comparing thymoglobulin and eATG, show that thymoglobulin is more effective in lowering acute rejection rates and improving 1-year allograft survival.19 Conversely, studies evaluating the use of basiliximab versus antithymocyte globulin demonstrate similar short-term efficacy between both groups.20 However, a more recent analysis of these two agents demonstrated similar results for allograft and patient survival, but a benefit for thymoglobulin in lowering the incidence of acute allograft rejection.21 When choosing an agent for induction therapy, one must weigh the risks versus the benefits. For the most part, the ALAs are considered to be most effective, but are associated with a higher incidence of infectious disease and cancer.
Patient Encounter, Part 1: Medical History, Physical Exam, and Diagnostic Tests
JJ is a 52-year-old woman who presents to your transplant center for a living-related renal transplant.
PMH:
• ESRD—secondary to PKD and failed previous transplant
• One prior renal transplant from husband in 1995, which failed secondary to chronic allograft nephropathy in 2004 (presumably from multiple rejection episodes within the first few years after transplant).
• For the previous transplant the patient was maintained on cyclosporine, mycophenolate, and prednisone.
• Hypertension; hyperlipidemia; insomnia
FH: Father died of a myocardial infarction at age 53, while her mother is alive and living with hypertension, systemic lupus erythematosus, DM, and osteoporosis at the age of 75.
SH: The patient works as a secretary. Was a heavy tobacco user (45 pack years), but quit 3 years ago. She denies alcohol and IV drug use.
Admission Meds: Calcitriol 0.25 mg by mouth once a day; calcium acetate 1,334 mg by mouth three times a day; ferrous sulfate 325 mg by mouth once a day; epo 4,000 units IV every hemodialysis session; zocor 20 mg by mouth once a day at bedtime; metoprolol 100 mg by mouth twice a day; ASA 81 mg by mouth once a day; zolpidem 10 mg by mouth once a day at bedtime
Allergies: Codeine (upset stomach); penicillin (hives); sulfa (rash)
Misc:
• CMV serostatus: Donor is CMV immunoglobulin G (IgG) positive
• CMV serostatus: Recipient is CMV IgG positive
Identify your treatment goals for this patient.
Create a plan for induction therapy (i.e., would you recommend induction therapy, if so, which agent?).
Immunosuppressive Therapies—Maintenance Therapy
The goals of maintenance immunosuppression are to prevent acute and chronic rejection episodes and to optimize patient and graft survival. Antirejection medications require careful selection and dosage titration to balance the risks of rejection with the risks of toxicities.
Common maintenance immunosuppressive agents can be divided into four basic medication classes:
• Calcineurin inhibitors (cyclosporine and tacrolimus);
• Antiproliferatives (azathioprine and the mycophenolic acid [MPA] derivatives);
• Target of Rapamycin (ToR) inhibitors (sirolimus); and
• Corticosteroids (prednisolone derivatives and dexamethasone).
Maintenance immunosuppression is generally achieved by combining two or more medications from the different classes to maximize efficacy by specifically targeting unique components of the immune response. Please refer to Figure 55–1 for a schematic representation of these different drug mechanisms and Figure 55–2 for an example protocol for administration of immunosuppressive medications post-transplant. This method of medication selection also helps to minimize toxicities by choosing agents with different adverse event profiles. Immunosuppressive regimens vary between organ types and transplant centers, but most often they include a calcineurin inhibitor with an adjuvant agent, plus or minus corticosteroids. Selection of appropriate immunosuppressive regimens should be patient-specific. In doing so, the transplant practitioner must take into account patients’ pre-existing disease states, medication regimens, and preferences.
Calcineurin Inhibitors
![]() Cyclosporine and tacrolimus belong to a class of immunosuppressants called the calcineurin inhibitors. These agents are considered by many to be the cornerstone of immunosuppression protocols. The calcineurin inhibitors work by complexing with cytoplasmic proteins (cyclosporine with cyclophylin and tacrolimus with FK binding protein-12).8, 9, 22, 23 These complexes then inhibit calcineurin phosphatase, which results in reduced IL-2 gene transcription. The final outcome is a decrease in IL-2 synthesis and a subsequent reduction in T-cell activation.8,9,22,23
Cyclosporine and tacrolimus belong to a class of immunosuppressants called the calcineurin inhibitors. These agents are considered by many to be the cornerstone of immunosuppression protocols. The calcineurin inhibitors work by complexing with cytoplasmic proteins (cyclosporine with cyclophylin and tacrolimus with FK binding protein-12).8, 9, 22, 23 These complexes then inhibit calcineurin phosphatase, which results in reduced IL-2 gene transcription. The final outcome is a decrease in IL-2 synthesis and a subsequent reduction in T-cell activation.8,9,22,23
Cyclosporine
Cyclosporine USP was first approved by the FDA in 1983, but was associated with a variable oral absorption. The development of a newer formulation, cyclosporine microemulsion USP introduced in 1994, allowed for a more consistent drug exposure due to a more reliable pharmacokinetic profile.24 Cyclosporine microemulsion is the formulation of choice for most transplant centers that use cyclosporine for maintenance immunosuppression due to the above mentioned benefit. The two formulations are not interchangeable.
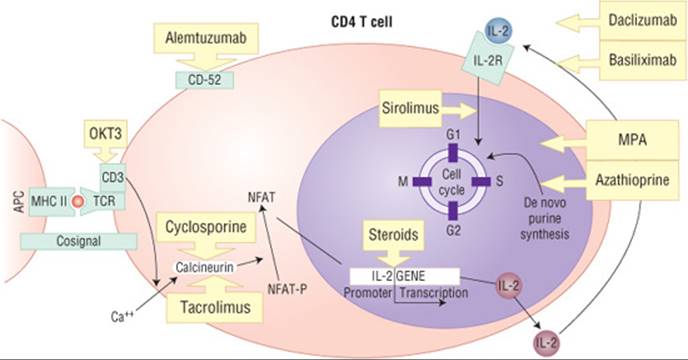
FIGURE 55–1. Identification of the sites of action of the various immunosuppressive medications. Antigen-major histocompatibility complex (MHC) II molecule complexes are responsible for initiating the activation of CD4 T cells. These MHC-peptide complexes are recognized by the T-cell recognition complex (TCR). A costimulatory signal initiates signal transduction with activation of second messengers, one of which is calcineurin. Calcineurin removes phosphates from the nuclear factors (NFAT-P), allowing them to enter the nucleus. These nuclear factors specifically bind to interleukin-2 (IL-2) promoter gene facilitating IL-2 gene transcription. Interaction of IL-2 with the IL-2 receptor (IL-2R) on the cell membrane surface induces cell proliferation and production of cytokines specific to the T cell. (APCs, antigen producing cells; MPA, myophenolic acid; OKT-3, muronomab-CD3.) (From Schonder KS, Johnson HJ. Solid organ transplantation. In: DiPiro JT, Talbert RL, Yee GC, et al., eds. Pharmacotherapy: A Pathophysiologic Approach, 7th ed. New York: McGraw-Hill, 2008:1463.)
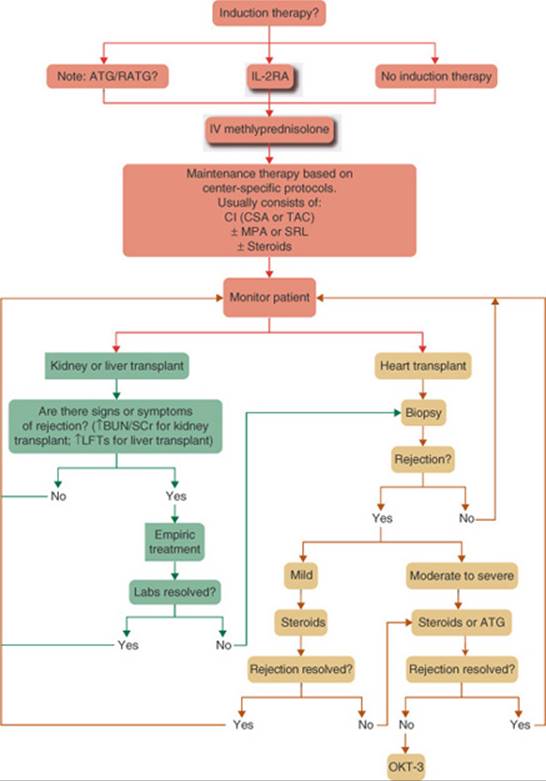
FIGURE 55–2. Example protocol of immunosuppressive medication use in organ transplantation. Center-specific protocols may use rabbit antithymocyte immunoglobulin (RATG), an interleukin 2 receptor antagonist (IL-2RA), or no induction therapy. In any situation, patients receive IV methylprednisone prior to, during, or immediately following the transplant operation. The patient then will begin the maintenance immunosuppressive regimen. The center-specific protocol will specify which calcineurin inhibitor (cyclosporine or tacrolimus) is used in combination with mycophenolate mofetil or sirolimus with or without steroids. Patients then are monitored for signs and symptoms of rejection. If rejection is suspected, a biopsy can be done for definitive diagnosis, or the patient may be treated empirically for rejection. Empirical treatment generally involves administration of corticosteroids. If signs and symptoms of rejection are resolved with empirical therapy, the patient will continue to be monitored according to the center-specific protocol. If rejection is confirmed by biopsy, treatment may be based on the severity of rejection. High-dose corticosteroids are used most frequently for mild to moderate rejection. RATG can be used for moderate to severe rejections or steroid-resistant rejections. Severe rejection episodes that are not resolved with steroids or RATG are treated with OKT-3. (BUN, blood urea nitrogen; CI, calcineurin inhibitor; CSA, cyclosporine; IL2RA, interleukin 2 receptor antagonist; LFT, liver function test; MPA, mycophenolic acid; OKT-3, moronomab-CD3; SCr, serum creatinine; SRL, sirolimus; TAC, tacrolimus.) (From Schonder KS, Johnson HJ. Solid Organ Transplantation. In: DiPiro JT, Talbert RL, Yee GC, et al., eds. Pharmacotherapy: A Pathophysiologic Approach, 7th ed. New York: McGraw-Hill, 2008:1466.)
The usual oral adult dose of cyclosporine ranges from 3 to 7 mg/kg/day in two divided doses.9 The appropriate selection of the starting dose usually depends on the organ type, the patient’s pre-existing disease states, and other concomitant immunosuppressive agents utilized. Cyclosporine microemulsion is available as 25 mg and 100 mg individually blister packed capsules and an oral solution. An IV formulation is also available. When converting a patient from oral to IV, the dosage should be reduced to approximately one-third of the oral dose.9
Cyclosporine whole blood trough concentrations have traditionally been obtained to help monitor for efficacy and safety. Therapeutic trough levels (C0) may range from 50 to 400 ng/mL (50–400 mcg/L or 42–333 nmol/L). Target levels should be individualized for each patient, usually depending on the organ transplanted, patient’s condition, method of assay (high-performance liquid chromatography [HPLC], monoclonal, polyclonal), and time since transplantation. Newer studies suggest that monitoring of concentrations at 2 hours postdose (C2) correlates better with toxicity and efficacy when compared to C0.25
Tacrolimus
Tacrolimus (also known as FK506) is the second calcineurin inhibitor and was approved by the FDA in 1997. Even though cyclosporine and tacrolimus both belong to the same general medication class, there are several differences between the two. First, looking at efficacy, some studies suggest that tacrolimus-based regimens are associated with improved short-term survival when compared with cyclosporine-based regimens.26 However, newer data suggest that there is no significant difference in acute rejection rates between cyclosporine and tacrolimus.27 In recent years, tacrolimus has become the workhorse calcineurin inhibitor in many transplant centers, due in large part to a more favorable adverse reaction profile.23
Oral starting doses of tacrolimus range from 0.1 to 0.2 mg/kg/day in two divided doses. Tacrolimus is available in 0.5-, 1-, and 5-mg capsules and as an injectable.9 The IV formulation is usually avoided due to the risk of anaphylaxis because of its castor oil component and nephrotoxicity. Tacrolimus C0whole blood levels should be monitored (12 hours after the last administered dose) and maintained between 5 and 15 ng/mL (5–15 mcg/L), again depending on the transplanted organ, patient’s condition, and time since transplant.9
Adverse Drug Reactions
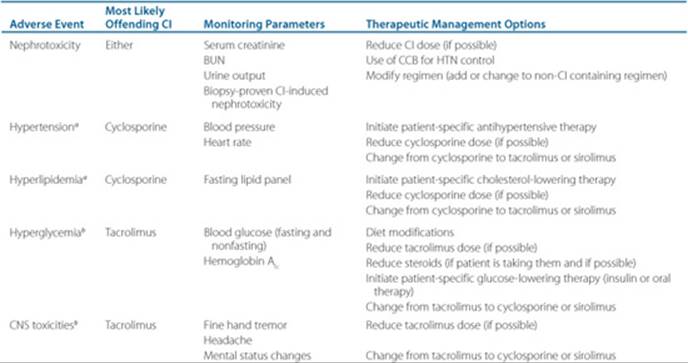
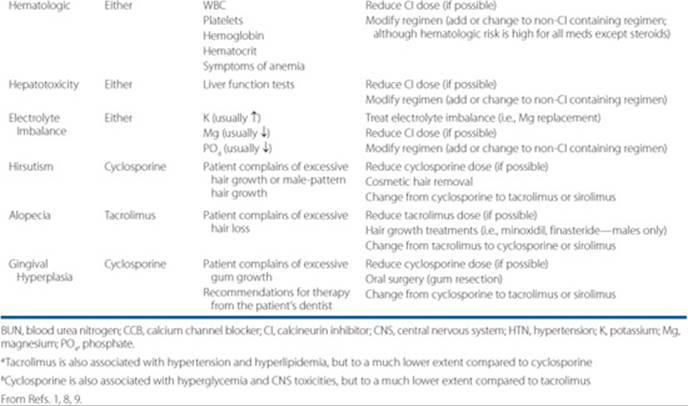
![]() One of the major drawbacks of the calcineurin inhibitors is their ability to cause acute and chronic nephrotoxicity. Acute nephrotoxicity has been correlated with high doses and is usually reversible. Chronic calcineurin inhibitor toxicity, however, is typically irreversible and is linked to chronic drug exposure. Table 55–4 expands upon the more common calcineurin inhibitor-induced adverse events.
One of the major drawbacks of the calcineurin inhibitors is their ability to cause acute and chronic nephrotoxicity. Acute nephrotoxicity has been correlated with high doses and is usually reversible. Chronic calcineurin inhibitor toxicity, however, is typically irreversible and is linked to chronic drug exposure. Table 55–4 expands upon the more common calcineurin inhibitor-induced adverse events.
Comparative Efficacy—Calcineurin Inhibitors
Several studies have assessed the clinical efficacy of cyclosporine versus tacrolimus. Most of the studies have shown similar long-term patient and allograft survival. Some renal transplant studies have demonstrated improved renal function in the tacrolimus treated patients. The most significant difference between the two agents appears to be their adverse drug reaction profiles.1–3
Antiproliferatives
These agents are generally considered to be adjuvant to the calcineurin inhibitors or possibly sirolimus. The medications included in this class are azathioprine and the MPA derivatives.
Azathioprine
Azathioprine was originally approved by the FDA in 1968 as an adjunct immunosuppressant for use in renal transplant recipients. It is available in oral and IV dosage forms.9 Prior to the advent of cyclosporine, the combination of azathioprine and corticosteroids was the mainstay of immunosuppressive therapy. Over the past 10 years, the use of azathioprine has declined markedly, due in large part to the success of the MPA derivatives which are more specific inhibitors of T-cell proliferation. ![]() Azathioprine is a prodrug for 6-mercaptopurine (6-MP), a purine analog. 6-MP acts as an antimetabolite and inhibits DNA replication with a resultant reduction in T-cell proliferation.9 The typical oral dose of azathioprine for organ transplantation is 3 to 5 mg/kg once a day.9 The maintenance dose is usually reduced to 1 to 2 mg/kg/day within a few weeks post-transplant. Dose reductions due to severely impaired renal function may be necessary since 6-MP and its metabolites are renally eliminated.9 Trough concentrations of 6-MP are not monitored; however, most clinicians often monitor for signs of myelosuppression and liver dysfunction.
Azathioprine is a prodrug for 6-mercaptopurine (6-MP), a purine analog. 6-MP acts as an antimetabolite and inhibits DNA replication with a resultant reduction in T-cell proliferation.9 The typical oral dose of azathioprine for organ transplantation is 3 to 5 mg/kg once a day.9 The maintenance dose is usually reduced to 1 to 2 mg/kg/day within a few weeks post-transplant. Dose reductions due to severely impaired renal function may be necessary since 6-MP and its metabolites are renally eliminated.9 Trough concentrations of 6-MP are not monitored; however, most clinicians often monitor for signs of myelosuppression and liver dysfunction. ![]() Myelosuppression (mainly leukopenia and thrombocytopenia) is a frequent, dose-dependent and dose-limiting complication (greater than 50% of patients) that often prompts dose reductions.9 Other common adverse events include hepatotoxicity (2–10%) and GI disease (10–15%; mostly nausea and vomiting). Importantly, pancreatitis and venoocclusive disease of the liver occurs in less than 1% of patients following chronic azathioprine therapy.9
Myelosuppression (mainly leukopenia and thrombocytopenia) is a frequent, dose-dependent and dose-limiting complication (greater than 50% of patients) that often prompts dose reductions.9 Other common adverse events include hepatotoxicity (2–10%) and GI disease (10–15%; mostly nausea and vomiting). Importantly, pancreatitis and venoocclusive disease of the liver occurs in less than 1% of patients following chronic azathioprine therapy.9
Mycophenolic Acid Derivatives
Mycophenolate mofetil was approved by the FDA in 1995 and enteric-coated MPA in 2004. Both agents are considered to be adjunctive immunosuppressants. ![]() Both mycophenolate mofetil and enteric-coated MPA are prodrugs for MPA. MPA acts by inhibiting inosine monophosphate dehydrogenase, a vital enzyme in the de novo pathway of purine synthesis. Inhibition of this enzyme prevents the proliferation of most cells that are dependent upon the de novo pathway for purine synthesis including T cells.8,9,28–30
Both mycophenolate mofetil and enteric-coated MPA are prodrugs for MPA. MPA acts by inhibiting inosine monophosphate dehydrogenase, a vital enzyme in the de novo pathway of purine synthesis. Inhibition of this enzyme prevents the proliferation of most cells that are dependent upon the de novo pathway for purine synthesis including T cells.8,9,28–30
Mycophenolate mofetil is available in 250 mg and 500 mg capsules, an oral suspension (100 mg/mL; in cherry syrup) and as an injectable.9 Usual doses of mycophenolate mofetil range from 1,000 to 3,000 mg/day in two to four divided doses. The conversion between oral and IV mycophenolate mofetil is 1:1. Enteric-coated MPA is available in 180-mg and 360-mg tablets. The appropriate equimolar conversion between mycophenolate mofetil and enteric-coated MPA is 1,000 mg of mycophenolate mofetil to 720 mg of enteric-coated-MPA.28,31 The recommended starting dose of enteric-coated MPA is 720 mg given twice daily.12 It appears that conversion of mycophenolate mofetil to enteric-coated MPA is safe, but more studies are needed to determine the exact role of enteric-coated MPA in the immunosuppressive armamentarium. MPA trough concentrations can be monitored; however, they are not routinely recommended.
Table 55–4 Management of Common Adverse Effects of Calcineurin Inhibitors
![]() The most common adverse events associated with these agents are GI (18-54%; diarrhea, nausea, vomiting, and gastritis) and myelosuppression (20-40%).8,12,28–30 Despite being enteric-coated, enteric-coated MPA has produced the same degree of GI adverse events as mycophenolate mofetil.28 However, recent data suggest that there is a benefit in converting patients with documented mycophenolate-induced GI disease from mycophenolate mofetil to enteric-coated MPA.
The most common adverse events associated with these agents are GI (18-54%; diarrhea, nausea, vomiting, and gastritis) and myelosuppression (20-40%).8,12,28–30 Despite being enteric-coated, enteric-coated MPA has produced the same degree of GI adverse events as mycophenolate mofetil.28 However, recent data suggest that there is a benefit in converting patients with documented mycophenolate-induced GI disease from mycophenolate mofetil to enteric-coated MPA.
Comparative Efficacy—Antiproliferatives
Due to the results of several studies, the MPA derivatives have replaced azathioprine as the antiproliferative agent of choice in most organ transplant centers. The MPA derivatives are generally considered to provide a more specific immunosuppressive effect compared to azathioprine. Mycophenolate mofetil and enteric-coated mycophenolate acid have similar safety and efficacy data in renal transplant recipients. The decision to choose one agent over another is a purely practitioner-dependent preference.
Target of Rapamycin Inhibitors
Sirolimus
Sirolimus is currently the only FDA-approved ToR inhibitor. One of its derivatives, everolimus, is in phase III clinical trials and has been approved for use in some European countries.32 Sirolimus is a macrolide antibiotic that has no affect on calcineurin phosphatase.8,33,34 Studies have shown that sirolimus may be used safely and effectively with either cyclosporine or tacrolimus as a replacement for either azathioprine or mycophenolate mofetil.35 Sirolimus can also be used as an alternative agent for patients who do not tolerate calcineurin inhibitors due to nephrotoxicity or other adverse events.36 ![]() At this time, the most exciting data for sirolimus point to its ability to prevent long-term allograft dysfunction when used as a substitute for the calcineurin inhibitors in renal transplant recipients.33,35,36
At this time, the most exciting data for sirolimus point to its ability to prevent long-term allograft dysfunction when used as a substitute for the calcineurin inhibitors in renal transplant recipients.33,35,36
![]() Sirolimus inhibits T-cell activation and proliferation by binding to and inhibiting the activation of the mammalian ToR, which suppresses cellular response to IL-2 and other cytokines (i.e., IL-4, IL-15).9,33
Sirolimus inhibits T-cell activation and proliferation by binding to and inhibiting the activation of the mammalian ToR, which suppresses cellular response to IL-2 and other cytokines (i.e., IL-4, IL-15).9,33
Sirolimus is available in a 1-mg and 2-mg tablet and a 1 mg/mL oral solution. The current FDA approved dosing regimen for sirolimus is a 6 mg loading dose followed by a 2 mg/day maintenance dose.9 It was recommended that this agent does not require therapeutic drug monitoring. However, most centers do check trough concentrations and adjust doses to reach goal concentrations.37 Most clinicians who use sirolimus utilize a loading dose of 5 to 15 mg/day for 1 to 3 days to more rapidly achieve adequate immunosuppression.33,35,36 Maintenance doses of sirolimus usually range from 1 to 10 mg/day given once daily. Sirolimus blood C0 levels should be obtained and maintained between 5 and 20 ng/mL, depending on the institution-specific protocols.37 Switching between immunoassays may produce different results that may be clinically significant. Of note, sirolimus has a half-life of approximately 62 hours, which means that it will not reach steady state after dosage changes for several days.9
![]() The most common adverse events reported with sirolimus are leukopenia (20%), thrombocytopenia (13-30%), and hyperlipidemia (38-57%).9,3 Other adverse effects include delayed wound healing, anemia, diarrhea, arthralgias, rash, hyperglycemia, pneumonitis, and mouth ulcers. Sirolimus has a FDA black-box warning in newly transplanted liver and lung recipients.9 In liver transplant recipients, use of sirolimus immediately after transplant is associated with an increased risk of hepatic artery thrombosis, graft loss, and death. In lung transplant recipients, bronchial anastomotic dehiscence, including some fatal cases, has been noted in patients treated with sirolimus, tacrolimus, and corticosteroids.
The most common adverse events reported with sirolimus are leukopenia (20%), thrombocytopenia (13-30%), and hyperlipidemia (38-57%).9,3 Other adverse effects include delayed wound healing, anemia, diarrhea, arthralgias, rash, hyperglycemia, pneumonitis, and mouth ulcers. Sirolimus has a FDA black-box warning in newly transplanted liver and lung recipients.9 In liver transplant recipients, use of sirolimus immediately after transplant is associated with an increased risk of hepatic artery thrombosis, graft loss, and death. In lung transplant recipients, bronchial anastomotic dehiscence, including some fatal cases, has been noted in patients treated with sirolimus, tacrolimus, and corticosteroids.
Corticosteroids
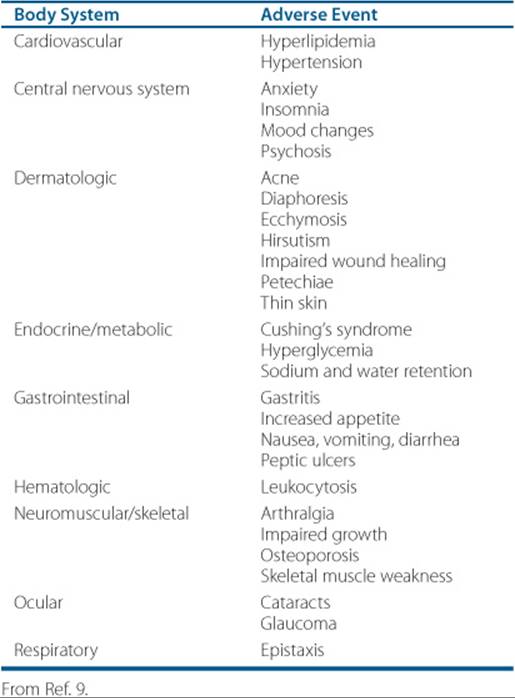
Traditional triple-therapy immunosuppressive regimens have consisted of a calcineurin inhibitor, an antiproliferative or ToR inhibitor, and corticosteroids. In recent years, many protocols have focused on corticosteroid sparing or avoidance. Avoidance or sparing of corticosteroids has been supported in the literature, although more studies are needed to help better characterize which patients should follow these protocols.38–41 A typical taper includes a bolus of IV methylprednisolone 100 to 500 mg at the time of transplant, then tapered over 5 to 7 days to a maintenance low dose of prednisone 5 to 10 mg/day. Although most centers still use low dose steroids for immunologically high risk patients, a number of programs have developed an immunosuppression protocol that completely avoids or withdraws corticosteroids at some point post-transplantation.2,8 At most transplant centers, therapeutic drug monitoring of corticosteroids is not employed. ![]() Corticosteroids are associated with a variety of acute and chronic toxicities. The most common adverse events have been summarized in Table 55–5.9
Corticosteroids are associated with a variety of acute and chronic toxicities. The most common adverse events have been summarized in Table 55–5.9
![]() Corticosteroids have various effects on immune and inflammatory response systems, although their exact mechanism of immunosuppression is not fully understood. It is generally believed that at high doses, the agents are directly lymphotoxic and at lower doses, the corticosteroids act by inhibiting the production of various cytokines that are necessary to amplify the immune response.12
Corticosteroids have various effects on immune and inflammatory response systems, although their exact mechanism of immunosuppression is not fully understood. It is generally believed that at high doses, the agents are directly lymphotoxic and at lower doses, the corticosteroids act by inhibiting the production of various cytokines that are necessary to amplify the immune response.12
The most commonly used corticosteroids are methylprednisolone (IV and oral) and prednisone (oral), although prednisolone and dexamethasone have also been shown to be effective for organ transplantation. Corticosteroid doses vary by center-specific protocols, organ type, and patient characteristics.
Immunosuppressive Therapies—Future Immunosuppressive Agents
The immunosuppressant armamentarium is expanding with novel small molecules (i.e., AEB, bortezimibe, and the Janus-Kinase 3 inhibitors) and biological agents (i.e., costimulatory pathway blockers) currently in clinical development. These newer agents appear promising and may represent the emergence of novel immunosuppressive agents that can deliver immunosuppression without the long-term toxicities. Some currently marketed immunosuppressants may also have beneficial effects in organ transplantation. Several agents, including alefacept, bortezimibe, alemtuzumab (discussed previously), efalizumab, leflunomide, and rituximab, have already been used successfully in renal transplantation.
Table 55–5 Common Adverse Events Associated WithCorticosteroids
Immunosuppressive Therapies—Treatment of Acute Rejection Episodes
Acute rejection is generally treated with a course of high-dose methylprednisolone (250–1,000 mg/day IV for 3 days), which is usually sufficient to ameliorate the rejection episode. If the acute rejection episode is resistant to the initial course of steroids, a second course may be administered or the patient may begin therapy with antithymocyte globulin (1.5 mg/kg/day for 3–14 days). Acute rejection refractory to these treatments may require OKT-3. However, the use of this agent has fallen out of favor due to the severe short- and long-term adverse events associated with its use.
Maintenance Immunosuppressive Therapies—Common Drug–Drug Interactions
![]() As the number of medications that a patient takes increases, so does the potential for DDIs. Disease severity, patient age, and organ dysfunction are all risk factors for increased DDIs. In general, DDIs can be broken down into two categories: (a) pharmacokinetic interactions, and (b) pharmacodynamic interactions.
As the number of medications that a patient takes increases, so does the potential for DDIs. Disease severity, patient age, and organ dysfunction are all risk factors for increased DDIs. In general, DDIs can be broken down into two categories: (a) pharmacokinetic interactions, and (b) pharmacodynamic interactions.
• Pharmacokinetic interactions result when one drug alters the absorption, distribution, metabolism, or elimination of another drug.
• Pharmacodynamic interactions include additive, synergistic, or antagonistic interactions that can affect efficacy or toxicity.
Pharmacokinetic Interactions
Given the large number of medications consumed by transplant recipients, it is no surprise that this patient population is at high risk for DDIs. Pharmacokinetic DDIs pose a major dilemma with the maintenance immunosuppressants. Pharmacokinetic interactions can either result in increased concentrations of one or more agents with an increased risk for drug-induced toxicities, or lowered (i.e., subtherapeutic) drug concentrations, possibly leading to allograft rejection. As mentioned above, pharmacokinetic DDIs can be further categorized into interactions of absorption, distribution, metabolism, and elimination.
Interactions of Absorption
Most DDIs due to altered absorption occur within the intestines. There are a variety of potential mechanisms through which the absorption of the maintenance immunosuppressants is altered, including:
• Drug metabolism within the gut (“Interactions of Metabolism” will be discussed below)
• Alterations in the active transport process
• Changes in intestinal motility
• Chelation interactions
Active transporters (i.e., P-glycoprotein [P-gp]) play an important role in drug-interactions. P-gp, a plasma membrane transport protein, is present in the gut, brain, liver, and kidneys.42,43 This protein provides a biological barrier, eliminating toxic substances and xenobiotics that may accumulate in these organ systems. P-gp plays an important role in the absorption and distribution of many medications. In the GI tract, P-gp is located in the brush borders of mature enterocytes. The colon has the largest percentage of P-gp, while the stomach and jejunum-ileum contain the lowest percentage. P-gp affects the absorption of cyclosporine, tacrolimus, and sirolimus. Some medications can alter the activity of P-gp (inhibit or induce its activity). Medications that are cytochrome P450 (CYP) 3A4 substrates, inhibitors or inducers, also tend to affect P-gp; therefore, the potential exists for several DDIs with the immunosuppressants by this mechanism.42,43 For example, medications that inhibit P-gp activity will increase concentrations of cyclosporine, tacrolimus, and sirolimus due to a reduction in P-gp-dependent drug elimination from the hepatic circulation.
When looking at the ability of drugs that change intestinal motility and their effects on the maintenance immunosuppressants, you can see notable interactions between the prokinetic agents and the calcineurin inhibitors. Metoclopramide has been shown to increase the absorption of cyclosporine and tacrolimus by enhancing gastric mobility and emptying.44
Most of the interactions with mycophenolate mofetil and enteric-coated MPA are due to reductions in intestinal absorption. Aluminum, magnesium, and calcium containing products decrease the peak level of MPA.9 If a patient requires aluminum, magnesium, or calcium, it should be administered at least 4 hours before or after MPA. Of note, iron does not interact with the MPA preparations.45
Interactions of Distribution
Interactions of distribution tend to occur with drugs that are highly protein bound. A drug that is extensively bound to plasma proteins can be displaced from its binding site by another agent that has greater affinity for the same binding site, thereby raising free concentrations of the displaced drug. MPA is the only highly protein bound (97% bound to albumin) maintenance immunosuppressant with a reported DDI by this mechanism. It has been shown that concomitant administration of MPA with salicylates increases the free concentrations of MPA.9 The adverse sequelae of this drug interaction have not been assessed. DDIs studies have not been completed evaluating the MPA derivatives, or the other highly protein bound maintenance immunosuppressants, when used with other highly protein bound drugs.
Interactions of Metabolism
Oxidative metabolism by CYP isozymes is the primary method of drug metabolism.46 The purpose of drug metabolism is to make drugs more water-soluble so they can be more easily eliminated. Cyclosporine, tacrolimus, and sirolimus are all substrates of the CYP3A isozyme system. The majority of CYP-mediated metabolism takes place in the liver; however, CYP is also expressed in the intestine, lungs, kidneys, and brain. Two types of interactions usually occur with medications metabolized via the CYP enzyme system, inhibitory interactions and inducing interactions. Enzyme inhibition occurs when there is enzyme inactivation or mutual competition of substrates at a catalytic site. This usually results in a reduction of drug metabolism leading to increased concentrations of all medications involved. Enzyme induction interactions are just the opposite and occur when there is increased synthesis or decreased degradation of CYP enzymes. This type of interaction can produce decreased concentrations of medications.46 Being CYP3A substrates, it would be anticipated that cyclosporine, tacrolimus, and sirolimus would all experience similar pharmacokinetic DDIs. Table 55–6 details the clinically relevant DDIs that occur with the calcineurin inhibitors and sirolimus due to inhibition or induction of the CYP isozyme system.
One of the most often overlooked DDIs in transplant recipients is the effect corticosteroids have on drug metabolism. Dexamethasone is a CYP3A isozyme inducer, meaning that it may increase the whole blood trough concentrations of cyclosporine, tacrolimus, and sirolimus.9,47 Conversely, methylprednisolone is a CYP3A isozyme inhibitor, and it may reduce the whole blood trough concentrations of cyclosporine, tacrolimus, and sirolimus.9,47This is usually not a noteworthy interaction, since doses of cyclosporine, tacrolimus, and sirolimus are titrated to achieve target concentrations in patients maintained on stable doses of corticosteroids. However, these DDIs may be problematic after pulse dose steroids for treatment of acute rejection or during steroid withdrawal.
Not all metabolic DDIs occur through the CYP system. Azathioprine has a considerable interaction with allopurinol that is not mediated through CYP.48,49 Allopurinol inhibits xanthine oxidase, which is the enzyme responsible for metabolizing 6-MP to inactive 6-thiouricate. Combining these agents can result in 6-MP accumulation and severe toxicities, particularly myelosuppression. It is recommended that concomitant therapy with azathioprine and allopurinol be avoided, but if necessary, azathioprine doses must be reduced to one-third or one-fourth of the current dose.49
Interactions of Elimination
There are very few interactions of elimination with the maintenance immunosuppressants. However, the major interaction through this process involves MPA. MPA is metabolized to MPA-glucuronide (MPAG) via hepatic glucuronosyltransferase.9,28 MPAG is excreted in the bile for elimination in the gut. Deconjugation of MPAG back to MPA by intestinal flora results in a secondary absorption of MPA several hours after its administration.9,28 Several medications have been shown to interfere with the biliary excretion of MPAG, thereby eliminating its reabsorption in the intestines and lowering the overall exposure to MPA. Cyclosporine has been shown to reduce the overall exposure to the MPA derivatives through competitive inhibition of MPAG enterohepatic recirculation.50 MPA levels are lower when it is administered in cyclosporine-based immunosuppression regimens compared to tacrolimus-based regimens. The bile acid sequestrants (i.e., cholestyramine, colestipol, colesevelam) have also been shown to decrease overall MPA exposure through a similar mechanism.51,52
Pharmacodynamic Interactions
In addition to the numerous pharmacokinetic interactions seen with the maintenance immunosuppressants, there also exists the possibility for pharmacodynamic interactions. An in-depth review of pharmacodynamic interactions with maintenance immunosuppressive agents goes beyond the scope of this chapter. However, some common pharmacodynamic DDIs will be discussed. Pharmacodynamic interactions are the backbone of modern immunosuppressive therapies that employ multiple medications with different mechanisms of action resulting in additive immunosuppression. Unfortunately, pharmacodynamic interactions can also be problematic, such as when medications with similar adverse events are used concomitantly. For example, nephrotoxic agents, such as amphotericin B, amino-glysides (i.e., gentamicin, tobramicin, amikacin) and non-steroidal anti-inflammatory drugs (NSAIDs; i.e., napro xen, ibuprofen, ketorolac) may potentiate the nephrotoxic effects of the calcineurin inhibitors.9The use of myelosuppressive agents, such as cotrimoxazole and valganciclovir, could enhance the myelosuppressive effects of induction therapy and the maintenance immunosuppressants.9
Table 55–6 Potential DDIs With the Calcineurin Inhibitors and Sirolimus Mediated Through the Cytochrome P-450 System 3A (CYP3A4) Isozyme
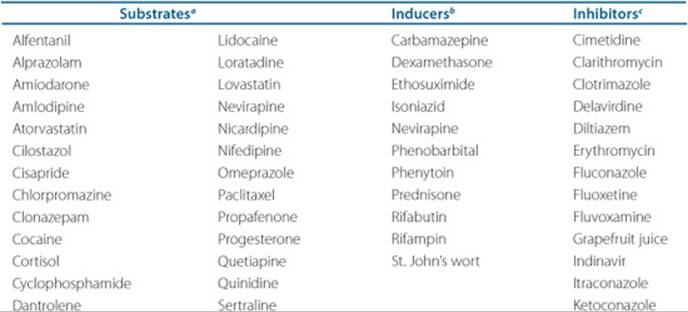
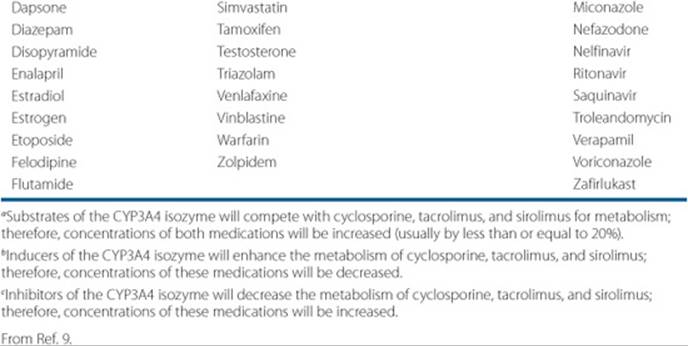
The potential exists for multiple DDIs in transplant recipients due to the complexity of their medication regimens. Practitioners must be diligent in reviewing all medications for potential DDIs. In addition to reviewing prescription medications, it is essential to question patients about the use of both nonprescription and complementary and alternative medicines, as these products also have the potential for significant interactions.
Immunosuppressive Therapies—Management of Immunosuppressive Drug Complications
Opportunistic Infections
![]() Solid organ transplant recipients are at increased risk of infectious diseases, which are a chief cause of early morbidity and mortality. The prevalence of post-transplant infection depends on several factors, including clinical risk factors, environmental exposures and the degree of immunosuppression. Anti-infectives are universally prescribed in this population and their use can be split into three different categories:
Solid organ transplant recipients are at increased risk of infectious diseases, which are a chief cause of early morbidity and mortality. The prevalence of post-transplant infection depends on several factors, including clinical risk factors, environmental exposures and the degree of immunosuppression. Anti-infectives are universally prescribed in this population and their use can be split into three different categories:
Patient Encounter, Part 2
Identify your treatment goals for JJ in terms of maintenance immunosuppressants.
Create a plan for maintenance therapy for JJ, making sure to compare and contrast the pros and cons of the different maintenance immunosuppressants.
Identify the potential DDIs that may exist with the addition of the maintenance immunosuppressants and the medications that JJ is currently taking.
• Prophylaxis: antimicrobials given to prevent an infection;
• Empiric: preemptive therapy given based on clinical suspicion of an active infection; and
• Treatment: antimicrobials given to manage a documented infection.
Post-transplant infections generally occur in a standard pattern; therefore, prevention is a key management strategy. The information in this section is designed to only highlight prophylaxis options routinely used in organ transplant recipients. Please refer to Table 55–7 for a list of agents used for the prevention of Pneumocystis jiroveci pneumonia and CMV disease.
Pneumocystis jiroveci Pneumonia
![]() Without prophylaxis, P. jiroveci (formerly Pneumocystis carinii) pneumonia occurs in 5% to 15% of transplant recipients.53 Antipneumocystis prophylaxis is enormously helpful and is generally used in all organ transplant recipients. The duration of prophylaxis is usually 6 to 12 months after transplant, but may be prolonged in highly immunosuppressed patients (i.e., active CMV disease, treatment for rejection) or liver or lung recipients.54Sulfamethoxazole-trimethoprim is the preferred agent for prophylaxis. One of its major advantages is its relatively broad spectrum of activity. Not only is it effective against Pneumocystis pneumonia, but it also has activity against toxoplasmosis and other common bacterial infections. Patients who have sulfa allergies, glucose-6 phosphate dehydrogenase (G6PD) deficiency, or are unable to tolerate sulfamethoxazole-trimethoprim should be given one of the second-line treatments.9 Unfortunately, the second-line agents are antiparasitics and have no meaningful activity against common bacteria. These agents include dapsone, atovaquone, and pentamidine.
Without prophylaxis, P. jiroveci (formerly Pneumocystis carinii) pneumonia occurs in 5% to 15% of transplant recipients.53 Antipneumocystis prophylaxis is enormously helpful and is generally used in all organ transplant recipients. The duration of prophylaxis is usually 6 to 12 months after transplant, but may be prolonged in highly immunosuppressed patients (i.e., active CMV disease, treatment for rejection) or liver or lung recipients.54Sulfamethoxazole-trimethoprim is the preferred agent for prophylaxis. One of its major advantages is its relatively broad spectrum of activity. Not only is it effective against Pneumocystis pneumonia, but it also has activity against toxoplasmosis and other common bacterial infections. Patients who have sulfa allergies, glucose-6 phosphate dehydrogenase (G6PD) deficiency, or are unable to tolerate sulfamethoxazole-trimethoprim should be given one of the second-line treatments.9 Unfortunately, the second-line agents are antiparasitics and have no meaningful activity against common bacteria. These agents include dapsone, atovaquone, and pentamidine.
Table 55–7 Prophylactic Options for Pneumocystis jiroveci Pneumonia and CMV
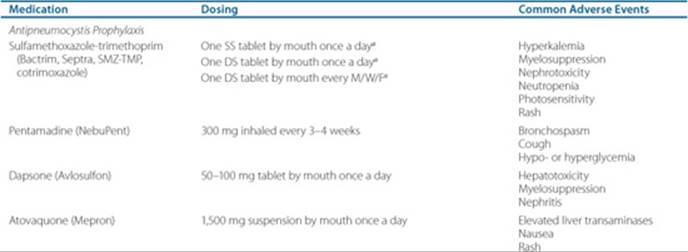
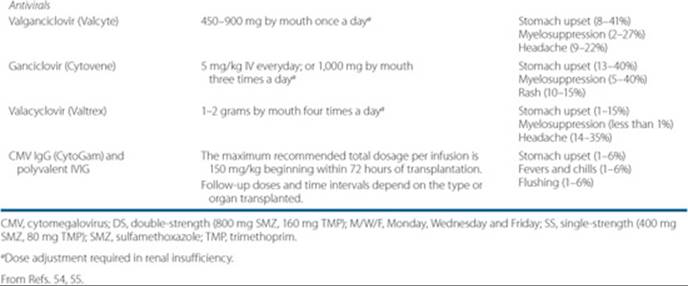
Cytomegalovirus
CMV is the most concerning opportunistic pathogen in transplantation due to its association with poor outcomes.55 CMV infection is present in 30% to 97% of the general population, but CMV disease is typically restricted to immunocompromised hosts.56 The risk of CMV disease is highest among CMV-naive recipients who receive a CMV-positive organ (Donor +/Recipient -).55 Other factors that augment the risk of CMV disease include organ type (lung and pancreas recipients are highest risk) and immunosuppressive agents (ALA use increases risk). CMV disease characteristically occurs within the first 3 to 6 months post-transplantation, but delayed onset disease has been seen in patients receiving antiviral prophylaxis.55
![]() Several antivirals have proven efficacy in preventing and treating CMV.55 Valacyclovir and valganciclovir, prodrugs of acyclovir and ganciclovir, respectively, have improved bioavailability compared to their parent compounds and offer the advantage of less frequent dosing. CMV prophylaxis is classically continued for the first 100 days, or longer, after transplantation.56,57 Both IV ganciclovir and oral valganciclovir may be used for preemptive therapy or for treatment of established CMV disease. The adverse events are similar among these agents and include myelosuppression and GI effects.9
Several antivirals have proven efficacy in preventing and treating CMV.55 Valacyclovir and valganciclovir, prodrugs of acyclovir and ganciclovir, respectively, have improved bioavailability compared to their parent compounds and offer the advantage of less frequent dosing. CMV prophylaxis is classically continued for the first 100 days, or longer, after transplantation.56,57 Both IV ganciclovir and oral valganciclovir may be used for preemptive therapy or for treatment of established CMV disease. The adverse events are similar among these agents and include myelosuppression and GI effects.9
Clinical Presentation and Diagnosis of Pneumocystis jiroveci Pneumonia
General
• Patients may not be in acute distress or they may feel tired (malaise)—symptoms vary from patient to patient.
Symptoms
• Patients may complain of fever, cough, and progressive dyspnea.
Signs
• The most common findings are fever and tachypnea.
• Chest examination may reveal crackles and rhonchi.
Radiographic Tests
• Chest radiographs may be normal in up to 25% of patients.
• The most common radiographic abnormalities are diffuse, bilateral, interstitial, or alveolar infiltrates.
Fungal Infections
Fungal infections are an important cause of morbidity and mortality in solid organ transplant recipients. Immunologic (i.e., immunosuppressants, CMV infection), anatomic (i.e., tissue ischemia and damage), and surgical (i.e., duration of surgery, transfusion requirements) factors contribute to the risk for invasive fungal infections. Mucocutaneous candidiasis (i.e., oral thrush, esophagitis) is associated with corticosteroid and ALA use. ![]() Oral nystatin or clotrimazole troches are effective prophylactic options for the prevention of thrush. However, clotrimazole inhibits the CYP3A system in the gut and can alter immunosuppressive levels.9 The use of systemic fungal prophylaxis, such as oral fluconazole, is controversial due to the potential for DDIs and the risk of developing resistance. The American Society of Transplantation and the American Society of Transplant Surgeons have recommended antifungal prophylaxis in liver, lung, and intestine transplantation.58 The choice of agents depends on the fungal risk in that particular population. For example, liver and intestine transplant recipients are at high risk for candidiasis; therefore, the use of medications that cover Candida spp. is crucial, such as the triazole antifungals (i.e., fluconazole, itraconazole) or the echinocandins (i.e., caspofungin, micafungin). Lung transplant recipients are at high risk for aspergillosis; therefore, it is imperative to use antifungal prophylaxis that covers Aspergillus spp., such as the echinocandins or polyenes (i.e., amphotericin B, lipid-based amphotericin B products).58
Oral nystatin or clotrimazole troches are effective prophylactic options for the prevention of thrush. However, clotrimazole inhibits the CYP3A system in the gut and can alter immunosuppressive levels.9 The use of systemic fungal prophylaxis, such as oral fluconazole, is controversial due to the potential for DDIs and the risk of developing resistance. The American Society of Transplantation and the American Society of Transplant Surgeons have recommended antifungal prophylaxis in liver, lung, and intestine transplantation.58 The choice of agents depends on the fungal risk in that particular population. For example, liver and intestine transplant recipients are at high risk for candidiasis; therefore, the use of medications that cover Candida spp. is crucial, such as the triazole antifungals (i.e., fluconazole, itraconazole) or the echinocandins (i.e., caspofungin, micafungin). Lung transplant recipients are at high risk for aspergillosis; therefore, it is imperative to use antifungal prophylaxis that covers Aspergillus spp., such as the echinocandins or polyenes (i.e., amphotericin B, lipid-based amphotericin B products).58
Hypertension
![]() Cardiovascular disease has been identified as one of the leading causes of death in organ transplant recipients.59 Post-transplant hypertension is associated with an increase in cardiac morbidity and patient mortality in all transplant patients and is also an independent risk factor for chronic allograft dysfunction and loss.60 Based on all of the available post-transplant morbidity and mortality data, it is imperative that post-transplant hypertension be identified and managed appropriately.
Cardiovascular disease has been identified as one of the leading causes of death in organ transplant recipients.59 Post-transplant hypertension is associated with an increase in cardiac morbidity and patient mortality in all transplant patients and is also an independent risk factor for chronic allograft dysfunction and loss.60 Based on all of the available post-transplant morbidity and mortality data, it is imperative that post-transplant hypertension be identified and managed appropriately.
There are several underlying mechanisms responsible for post-transplant hypertension. Some causes of hypertension in transplant recipients may include renal dysfunction, increased sensitivity to endothelin-1 and angiotensin, increased density of glucocorticoid receptors in the vascular smooth muscle, and decreased production of vasodilatory prostaglandins.61 However, one of the most easily recognized causes of post-transplant hypertension is the use of corticosteroids and the calcineurin inhibitors.62,63 Corticosteroids usually cause sodium and water retention,61 thus increasing blood pressure, whereas calcineurin inhibitors are associated with a number of effects that may result in hypertension, including reduced glomerular filtration rate (GFR) and renal blood flow (RBF), increased systemic and intrarenal vascular resistance, sodium retention, reduced concentrations of systemic vasodilators (i.e., prostacyclin, nitric oxide), and increased concentrations of vasoconstrictive thromboxanes.64 When compared with cyclosporine in clinical trials, tacrolimus displayed significantly less severe hypertension, and patients taking tacrolimus required significantly fewer antihypertensive medications at both 24 and 60 months post-transplant.65–67
Patient Encounter, Part 3
Identify your treatment goals for JJ in terms of antimicrobial prophylaxis.
Create a plan for JJ’s antimicrobial prophylaxis, making sure to compare and contrast the pros and cons of the different agents.
Treatment
![]() Controlling hypertension post-transplant is essential in preventing cardiac morbidity and mortality and prolonging graft survival. The target blood pressure in kidney transplant recipients should be less than 130/80 mm Hg. This goal blood pressure may not be suitable for all organ transplant recipients. In such cases, the Joint National Committee Seventh Report (JNC7) guidelines should be followed.
Controlling hypertension post-transplant is essential in preventing cardiac morbidity and mortality and prolonging graft survival. The target blood pressure in kidney transplant recipients should be less than 130/80 mm Hg. This goal blood pressure may not be suitable for all organ transplant recipients. In such cases, the Joint National Committee Seventh Report (JNC7) guidelines should be followed.
Lifestyle Modifications
In order to achieve a goal blood pressure, lifestyle modifications including diet, exercise, sodium restriction, and smoking cessation are recommended.67 Unfortunately, lifestyle modifications alone are often inadequate to control hypertension in this high-risk population and antihypertensive medications are usually initiated early after transplant.
Immunosuppressive Regimen Modification
Because tacrolimus has shown the propensity to cause less severe hypertension when compared to cyclosporine, conversion from cyclosporine-based immunosuppression to tacrolimus-based immunosuppression may be one way to help reduce the severity of hypertension in transplant recipients. Conversion to sirolimus, which is not associated with increases in blood pressure, may also be an alternative to the calcineurin inhibitors in patients with difficult-to-treat hypertension. Corticosteroid taper or withdrawal are effective strategies for lowering blood pressure, but are not warranted in all clinical situations.
Antihypertensive Agents
There is no single class of antihypertensive medications recognized as the ideal agent. Numerous factors must be considered when determining appropriate treatment for a given patient, including the safety and efficacy data of the available agents, patient-specific situations, and potential comorbidities, and medication cost. A large majority of patients often require multiple medications to achieve their goal blood pressure. This conclusion is supported by the recommendations of JNC-VII, where combination therapy is regarded as an appropriate first-line therapy.
β-Blockers and thiazide diuretics have proven benefits in reducing cardiovascular disease-associated morbidity and mortality59 Tolerability permitting, these agents are to be considered first-line therapies in most transplant recipients. The angiotensin converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARB) have definite benefits in patients with nephropathy and are believed to have renoprotective effects in most patients. However, due to their ability to cause an initial increase in serum creatinine, these agents should be used cautiously when used in combination with the calcineurin inhibitors. The dihydropyridine calcium channel blockers have demonstrated an ability to reverse the nephrotoxicity associated with cyclosporine and tacrolimus. In general, antihypertensive therapy should focus on agents with proven benefit in reducing the progression of cardiovascular disease and should be chosen on a patient-specific basis.59
Hyperlipidemia
![]() Hyperlipidemia is seen in up to 60% of heart, lung, and renal transplant patients and greater than 30% of liver transplant patients.68–70 As a result of elevated cholesterol levels, transplant recipients are not only at an increased risk of atherosclerotic events, but emerging evidence also shows an association between hyperlipidemia and allograft vasculopathy.70 Hyperlipidemia, along with other types of cardiovascular disease, is now one of the primary causes of morbidity and mortality in long-term transplant survivors.71
Hyperlipidemia is seen in up to 60% of heart, lung, and renal transplant patients and greater than 30% of liver transplant patients.68–70 As a result of elevated cholesterol levels, transplant recipients are not only at an increased risk of atherosclerotic events, but emerging evidence also shows an association between hyperlipidemia and allograft vasculopathy.70 Hyperlipidemia, along with other types of cardiovascular disease, is now one of the primary causes of morbidity and mortality in long-term transplant survivors.71
Elevated cholesterol levels in transplant patients are due to a culmination of factors such as age, genetic disposition, renal dysfunction, DM, proteinuria, body weight, and immunosuppressive therapy. Many of the immunosuppressive agents can produce elevations in serum lipid levels.
Treatment
![]() Lowering cholesterol has shown to significantly decrease severe rejection and transplant vasculopathy, and improve 1-year survival in heart transplant recipients.72 Although these results cannot be extrapolated to the other transplant populations, they do demonstrate the potential benefits of aggressive cholesterol lowering in organ transplant recipients. Due to high prevalence of cardiovascular disease among organ transplant recipients, most health care practitioners consider these patients to fall in the highest risk category for lipid lowering as established by the National Cholesterol Education Panel (NCEP) III guidelines. These guidelines call for a calculated LDL (LDL-C) target level of less than 100 mg/dL (2.59 mmol/L).73
Lowering cholesterol has shown to significantly decrease severe rejection and transplant vasculopathy, and improve 1-year survival in heart transplant recipients.72 Although these results cannot be extrapolated to the other transplant populations, they do demonstrate the potential benefits of aggressive cholesterol lowering in organ transplant recipients. Due to high prevalence of cardiovascular disease among organ transplant recipients, most health care practitioners consider these patients to fall in the highest risk category for lipid lowering as established by the National Cholesterol Education Panel (NCEP) III guidelines. These guidelines call for a calculated LDL (LDL-C) target level of less than 100 mg/dL (2.59 mmol/L).73
Lifestyle Modifications
Generally, lowering cholesterol in patients begins with therapeutic lifestyle changes. These changes are initiated either alone or in conjunction with lipid-lowering drug therapy depending on baseline cholesterol levels and other risk factors. Therapeutic lifestyle changes entail a reduction in saturated fat and cholesterol intake and an increase in moderate physical activity.73 As with hypertension, lifestyle modifications alone rarely are effective enough to achieve a goal LDL-C level.70 Modifications of the immunosuppressive regimen and use of cholesterol-lowering medications are often warranted in this patient population.
Immunosuppressive Regimen Modifications
Tacrolimus has shown the propensity to cause less severe hyperlipidemia when compared to cyclosporine. Conversion from cyclosporine-based immunosuppression to tacrolimus-based immunosuppression may be one way to counteract this disease in transplant recipients.70
In past studies, steroid withdrawal in renal transplant patients did lower total cholesterol by 17% and LDL cholesterol by 16%; unfortunately, an 18% decrease in high-density lipoproteins (HDL) levels was also noted in these patients.70
Cholesterol-Lowering Agents
3-Hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors or statins, are considered to be first-line therapy for hyperlipidemia in the general population.70,74–77 However, there is some uncertainty about the pathogenesis of cardiovascular disease in transplant recipients and whether statin therapy will have similar effectiveness in organ transplant recipients. Statins have shown definite advantages when used in heart transplantation, including a reduction in LDL-C and major adverse cardiac outcomes (MACE), as well as an apparent cardioprotective effect. In renal transplant recipients, statins are known to lower LDL-C levels and reduce the incidence of some cardiac events, however, the ability to lower MACE may not be evident in this patient population. Despite these mixed results, statins are still considered the primary therapeutic option for hyperlipidemia in all organ transplant recipients.70
Fibric acid derivatives are an excellent choice for lowering triglycerides, but are not as effective as statins at lowering the LDL-C.70 These agents may play a role in conjunction with statins in patients with both elevated cholesterol and triglycerides. Nicotinic acid is very effective at improving the lipid panel, with excellent results in lowering LDL-C, as well as increasing HDL. However, patient tolerability issues are of concern with this agent. The bile acid sequestrants should be avoided in organ transplant recipients due to their high incidence of GI adverse events, as well as their propensity for pharmacokinetic DDIs with the immunosuppressants. Future studies are needed to establish ideal regimens involving the antihyperlipidemic and immunosuppressive medications in order to decrease morbidity and mortality, and ultimately prevent cardiovascular events.70
New-Onset DM After Transplantation
![]() New-onset DM after transplantation (NODAT) is a serious complication that is often underestimated by transplant practitioners.78 Kasiske and colleagues attempted to quantify the cumulative incidence of NODAT in renal transplant recipients and found that 8.3% of patients developed NODAT at 3 months post-transplant, 12.9% at 12 months, and 22.3% at 36 months.78 Even more alarming is that recent studies have revealed an overwhelming prevalence of impaired glucose tolerance, which is also accepted as a risk factor for long-term morbidity and mortality.78 NODAT is associated with increases in cardiovascular events, with an approximately 22% higher risk of mortality. Patients with NODAT are also more likely to suffer acute rejection episodes and infectious complications than patients without this complication.78
New-onset DM after transplantation (NODAT) is a serious complication that is often underestimated by transplant practitioners.78 Kasiske and colleagues attempted to quantify the cumulative incidence of NODAT in renal transplant recipients and found that 8.3% of patients developed NODAT at 3 months post-transplant, 12.9% at 12 months, and 22.3% at 36 months.78 Even more alarming is that recent studies have revealed an overwhelming prevalence of impaired glucose tolerance, which is also accepted as a risk factor for long-term morbidity and mortality.78 NODAT is associated with increases in cardiovascular events, with an approximately 22% higher risk of mortality. Patients with NODAT are also more likely to suffer acute rejection episodes and infectious complications than patients without this complication.78
Prevention
![]() NODAT prevention mainly consists of identifying patients at risk pretransplant and controlling modifiable risk factors both pre- and post-transplantation.78 The major modifiable risk factors are choice of immunosuppressive therapy and body mass index. For example:
NODAT prevention mainly consists of identifying patients at risk pretransplant and controlling modifiable risk factors both pre- and post-transplantation.78 The major modifiable risk factors are choice of immunosuppressive therapy and body mass index. For example:
• Immunosuppressive medications: steroid minimization and possibly withdrawal are effective strategies for the prevention of NODAT. Also, patients with worsening blood sugars after transplantation who are receiving tacrolimus may benefit from conversion to cyclosporine.78
• Body mass index: a reduction in body weight is always recommended in obese patients prior to the transplant procedure to help lower their NODAT risks.78
Treatment
![]() Lifestyle modifications are always in order in patients who have developed or those who are at increased risk of developing NODAT.78 Insulin therapy and oral hypoglycemic agents are often utilized in those patients where lifestyle modifications alone have not controlled blood glucose. Please refer to the chapter on DM for proper instruction on choosing the appropriate treatment regimens in patients with DM.
Lifestyle modifications are always in order in patients who have developed or those who are at increased risk of developing NODAT.78 Insulin therapy and oral hypoglycemic agents are often utilized in those patients where lifestyle modifications alone have not controlled blood glucose. Please refer to the chapter on DM for proper instruction on choosing the appropriate treatment regimens in patients with DM.
Neoplasia
Skin Cancer
Skin cancer remains the most common malignancy after organ transplantation. The rate of skin cancers occurs from as low as 3.4-fold (melanoma) up to as high as 84-fold (Kaposi’s sarcoma) higher in organ transplant recipients when compared to the general population.79 The incidence of these types of cancers increases with time post-transplant, with one study showing a prevalence rate of 35% among patients within 10 years after transplant.80 More alarming than the high prevalence is the activity of these cancers in the patient on maintenance immunosuppression. Skin cancers in transplant recipients tend to grow more rapidly and are more likely to metastasize.79
The most common risk factors for skin cancer development after transplant include increased age, excessive UV light exposure, high degree of immunosuppression, Fitzpatrick skin types I, II, and III, history of skin cancers, and infection by human papillomavirus.79
It is of the utmost importance that transplant practitioners be vigilant about educating their patients about excessive exposure to the sun.79 Patients should be warned about the risk of skin cancer and be advised on simple methods to limit their risk:
• Use of protective clothing (i.e., long-sleeved shirts and long pants, dark-colored clothing)
• Use of sunscreen daily that is applied to all sun-exposed skin
• Sun protection factor (SPF) 30 or higher is recommended
Patient Encounter, Part 4
JJ has recovered from her transplant procedure and is now doing relatively well. She returns to your clinic one month after the transplant:
Labs:
Na: 141 mEq/L (141 mmol/L)
K: 4.9 mEq/L (4.9 mmol/L)
Cl: 100 mEq/L (100 mmol/L)
CO2: 22 mEq/L (22 mmol/L)
BUN: 22 mg/dL (7.9 mmol/L)
SCr: 1.2 mg/dL (106 μmol/L)
Glucose: 89 mg/dL (4.9 mmol/L)
Lipid panel: Total cholesterol = 271 mg/dL (7.0 mmol/L); LDL-C = 180 mg/dL (4.7 mmol/L); HDL = 30 mg/dL (0.8 mmol/L); triglycerides = 325 mg/dL (3.7 mmol/L)
Tacrolimus: 10.1 mg/dL (10.1 mcg/L)
VS: BP 154/95 mm Hg (152/88 mm Hg repeated); HR 60 bpm
Meds: Tacrolimus 3 mg by mouth twice a day; mycophenolate mofetil 1,000 mg by mouth twice a day; prednisone 10 mg by mouth once a day; atovaquone 1,500 mg by mouth once a day; valganciclovir 450 mg by mouth once a day; vitamin D 800 IU by mouth once a day; calcium carbonate 1,250 mg by mouth twice a day separated from food and mycophenolate; simvastatin 20 mg by mouth once a day at bedtime; metoprolol 100 mg by mouth twice a day; amlodipine 10 mg by mouth once a day; ASA 81 mg by mouth once a day; zolpidem 10 mg by mouth once a day at bedtime
Identify why JJ is taking each agent listed.
What are some treatment options, in addition to Metoprolol 100 mg twice daily and Amlodipine 10 mg daily, for JJ’s elevated blood pressure?
Design a monitoring plan for JJ’s therapy.
Post-transplant Lymphoproliferative Disorders
![]() Post-transplant lymphoproliferative disorders (PTLD) are a major complication in patients following organ transplantation.81 Large series of case reports have demonstrated that the incidence of PTLD is 1% for renal patients, 1.8% for cardiac patients, 2.2% for liver patients, and 9.4% for heart-lung patients. The risk of developing non-Hodgkin’s lymphoma is 28- to 49-fold higher in solid organ transplant recipients compared with the general population. Another independent risk factor is the presence of the Epstein-Barr virus (EBV).81–83 Lymphomas are the most common form of lymphoproliferative disease found in transplant recipients.81
Post-transplant lymphoproliferative disorders (PTLD) are a major complication in patients following organ transplantation.81 Large series of case reports have demonstrated that the incidence of PTLD is 1% for renal patients, 1.8% for cardiac patients, 2.2% for liver patients, and 9.4% for heart-lung patients. The risk of developing non-Hodgkin’s lymphoma is 28- to 49-fold higher in solid organ transplant recipients compared with the general population. Another independent risk factor is the presence of the Epstein-Barr virus (EBV).81–83 Lymphomas are the most common form of lymphoproliferative disease found in transplant recipients.81
The incidence of disease depends on certain factors. These factors include the type of organ transplanted, the age of the transplant recipient, the degree of immunosuppression, the type of immunosuppression, and exposure to EBV.81,83 The mortality rate in these patients is about 50%, with most patients dying shortly after diagnosis. It has also been demonstrated that the risk of developing PTLD is greater in the population of EBV seronegative patients at the time of transplant.83
Another risk factor for the development of PTLD is the type of immunosuppressive regimens used. ALAs have come to be widely used in the prevention and treatment of acute rejection. These agents work by causing widespread T-cell lysis. Immunosuppressive regimens utilizing the ALAs have been proven to increase the risk of PTLD.81
Treatment
![]() Treatment for PTLD is still controversial; however, the most common treatment options include reduction of immunosuppression, chemotherapy,84 and anti-B cell monoclonal antibodies.81 PTLD continues to be a long-term complication of prolonged immunosuppression. Current treatment options are all associated with certain risks. Prevention is the most effective treatment for PTLD. A better understanding in future of the disease process and the risk factors involved with the development of PTLD will aid in the prophylaxis and treatment of this disorder.
Treatment for PTLD is still controversial; however, the most common treatment options include reduction of immunosuppression, chemotherapy,84 and anti-B cell monoclonal antibodies.81 PTLD continues to be a long-term complication of prolonged immunosuppression. Current treatment options are all associated with certain risks. Prevention is the most effective treatment for PTLD. A better understanding in future of the disease process and the risk factors involved with the development of PTLD will aid in the prophylaxis and treatment of this disorder.
OUTCOME EVALUATION
Successful outcomes in solid organ transplantation are generally measured in terms of several separate end points: (a) preventing acute rejection, (b) increasing 1-year graft survival, (c) preventing immunosuppressive drug complications, and (d) improving long-term allograft and patient survival.
The short-term goals after organ transplantation revolve around reducing the incidence of acute rejection episodes and attaining a high graft survival rate. By accomplishing these goals, transplant clinicians hope to attain good allograft function to allow for an improved quality of life. These goals can be achieved through the appropriate use of medical immunosuppression and scrutinizing over the therapeutic and toxic monitoring parameters associated with each medication employed. In addition, transplant recipients should be monitored for adverse drug reactions, DDIs, and adherence with their therapeutic regimen.
The long-term goals after organ transplant are to maximize the functionality of the allograft and prevent the complications of immunosuppression, which lead to improved patient survival. Clinicians must play multiple roles in the long-term care of transplant recipients as, not only must the patient be followed from an immunologic perspective, but practitioners must be focused in identifying and treating the adverse sequelae associated with lifelong immunosuppression including cardiovascular disease, malignancy, infection, and osteoporosis among others. Again, limiting drug misadventures and assuring adherence with the therapeutic regimen is important and should be stressed.
Patient Care and Monitoring
Early Management of Transplant Recipients
• Review any available diagnostic and laboratory data to evaluate the function of the allograft and the health of the recipient.
• Assess the patient’s current medication regimen, including:
• Induction therapy agent:
• Assess for appropriate dose and duration of therapy
• Therapeutic monitoring parameters (organ function)
• Toxic monitoring parameters
• Maintenance immunosuppressive agents:
• Assess for appropriate dose and duration of therapy
• Therapeutic monitoring parameters (organ function)
• Toxic monitoring parameters
• Anti-infective prophylaxis:
• Assess suitability of chosen prophylactic agents (i.e., drug allergies, CMV donor and recipient serostatus)
• Therapeutic monitoring parameters
• Toxic monitoring parameters
• Medications used for comorbidities:
• Assess appropriate selection of these medications for pharmacokinetic and pharmacodynamic DDIs, need (i.e., do renal transplant recipients need to continue to take erythropoietin?), and efficacy.
• Therapeutic monitoring parameters
• Toxic monitoring parameters
• Evaluate the patient for the presence of adverse drug reactions, drug allergies or DDIs.
• Develop patient-specific short-term and long-term therapeutic goals.
• Provide patient education regarding the organ transplant, the complications associated with transplantation,
the need for lifestyle modifications to reduce risk of complications (i.e., wear sunscreen, low-sodium diet) and drug therapy.
• Stress importance of adherence with therapeutic regimen.
Outpatient Management of Transplant Recipients
• Obtain a thorough history of prescription, nonprescription, and complimentary and alternative medication use.
• Maintenance immunosuppressive agents:
• Assess for appropriate dose and duration of therapy
• Therapeutic monitoring parameters (organ function)
• Toxic monitoring parameters
• Anti-infective prophylaxis:
• Assess suitability of chosen prophylactic agents (i.e., drug allergies, CMV donor and recipient serostatus)
• Does the patient need continued prophylaxis therapy?
• When do you stop prophylaxis?
• Therapeutic monitoring parameters
• Toxic monitoring parameters
• Medications used for comorbidities:
• Assess appropriate selection of these medications for pharmacokinetic and pharmacodynamic DDIs, need and efficacy
• Therapeutic monitoring parameters (drug- and disease-specific)
• Toxic monitoring parameters (drug-specific)
• Evaluate the patient for the presence of adverse drug reactions, drug allergies, or DDIs.
• Reassess your patient-specific short-term and long-term therapeutic goals.
• Continue with patient education in regards to the complications associated with transplantation, the need for lifestyle modifications to reduce risk of the complications (i.e., wear sunscreen, low-sodium diet) and drug therapy.
• Re-emphasize the importance of adherence with their therapeutic regimen.
• Assess improvement in quality of life measures such as physical, psychological and social functioning, and well-being.
Abbreviations Introduced in This Chapter
 Self-assessment questions and answers are available at http://www.mhpharmacotherapy.com/pp.html.
Self-assessment questions and answers are available at http://www.mhpharmacotherapy.com/pp.html.
REFERENCES
1. Calne RY. Transplantation: Current developments and future directions. Front Biosci 2007;12:3727–3733.
2. Halloran PF. Immunosuppressive drugs for kidney transplantation. N Engl J Med 2004;351(26):2715–2729.
3. The Organ Procurement and Transplant Network (OPTN). Available at http://www.optn.org/latestData/viewDataReports.asp.
4. Remuzzi G, Chiaramonte S, Perico N, Ronco C (eds): Humoral immunity in kidney transplantation. What clinicians need to know. Contrib Nephrol 2009;162:1–12
5. Michaels PJ, Fishbein MC, Colvin RB. Humoral rejection of human organ transplants. Springer Semin Immunopathol 2003;25(2): 119–140.
6. Joosten SA, Sijpkens YW, van Kooten C, Paul LC. Chronic renal allograft rejection: Pathophysiologic considerations. Kidney Int 2005;68(1):1–13.
7. Monaco AP. The beginning of clinical tolerance in solid organ allografts. Exp Clin Transplant 2004;2(1):153–161.
8. Hardinger KL, Koch MJ, Brennan DC. Current and future immunosuppressive strategies in renal transplantation. Pharmacotherapy 2004;24(9):1159–1176.
9. Micromedex Healthcare Series, (electronic version). Greenwood Village, CO: Thomson Healthcare, Inc., 2008.
10. Mohty M, Gaugler B. Mechanisms of action of antithymocyte globulin: Old dogs with new tricks! Leuk Lymphoma 2008;49(9):1664–1667.
11. Mottershead M, Neuberger J. Daclizumab. Expert Opin Biol Ther 2007;7(10):1583–1596.
12. Nashan B. Antibody induction therapy in renal transplant patients receiving calcineurin-inhibitor immunosuppressive regimens: A comparative review. BioDrugs 2005;19(1):39–46.
13. Vincenti F, Pace D, Birnbaum J, Lantz M. Pharmacokinetic and pharmacodynamic studies of one or two doses of daclizumab in renal transplantation. Am J Transplant 2003;3(1):50–52.
14. Soltero L, Carbajal H, Sarkissian N, et al. A truncated-dose regimen of daclizumab for prevention of acute rejection in kidney transplant recipients: A single-center experience. Transplantation 2004;78(10):1560–1563.
15. Whiting JF, Fecteau A, Martin J, Bejarano PA, Hanto DW. Use of low-dose OKT3 as induction therapy in liver transplantation. Transplantation 1998;65(4):577–580.
16. Hooks MA, Wade CS, Millikan WJ, Jr. Muromonab CD-3: A review of its pharmacology, pharmacokinetics, and clinical use in transplantation. Pharmacotherapy 1991;11(1):26–37.
17. Wilde MI, Goa KL. Muromonab CD3: A reappraisal of its pharmacology and use as prophylaxis of solid organ transplant rejection. Drugs 1996;51(5):865–894.
18. Abramowicz D, De Pauw L, Le Moine A, et al. Prevention of OKT3 nephrotoxicity after kidney transplantation. Kidney Int Suppl 1996;53:S39–S43.
19. Brennan DC, Flavin K, Lowell JA, et al. A randomized, double-blinded comparison of Thymoglobulin versus Atgam for induction immunosuppressive therapy in adult renal transplant recipients. Transplantation 1999;67(7):1011–1018.
20. Lebranchu Y, Bridoux F, Buchler M, et al. Immunoprophylaxis with basiliximab compared with antithymocyte globulin in renal transplant patients receiving MMF-containing triple therapy. Am J Transplant 2002;2(1):48–56.
21. Brennan DC, Daller JA, Lake KD, Cibrik D, Del Castillo D. Rabbit antithymocyte globulin versus basiliximab in renal transplantation. N Engl J Med 2006;355(19):1967–1977.
22. Beaty CA, Cymet T. Organ transplantation for the primary care provider: What you need to know to get your patient a new liver or kidney. Compr Ther 2008;34(2):69–76.
23. Golshayan D, Buhler L, Lechler RI, Pascual M. From current immunosuppressive strategies to clinical tolerance of allografts. Transpl Int 2007;20(1):12–24.
24. Cyclosporine microemulsion (Neoral) absorption profiling and sparse-sample predictors during the first 3 months after renal transplantation. Am J Transplant 2002;2(2):148–156.
25. Citterio F, Scata MC, Romagnoli J, Nanni G, Castagneto M. Results of a three-year prospective study of C2 monitoring in long-term renal transplant recipients receiving cyclosporine microemulsion. Transplantation 2005;79(7):802–806.
26. Mayer AD, Dmitrewski J, Squifflet JP, et al. Multicenter randomized trial comparing tacrolimus (FK506) and cyclosporine in the prevention of renal allograft rejection: A report of the European Tacrolimus Multicenter Renal Study Group. Transplantation 1997;64(3):436–443.
27. Levy G, Villamil F, Samuel D, et al. Results of lis2t, a multicenter, randomized study comparing cyclosporine microemulsion with C2 monitoring and tacrolimus with C0 monitoring in de novo liver transplantation. Transplantation 2004;77(11):1632–1638.
28. Gabardi S, Tran JL, Clarkson MR. Enteric-coated mycophenolate sodium. Ann Pharmacother 2003;37(11):1685–1693.
29. Sollinger HW. Mycophenolates in transplantation. Clin Transplant 2004;18(5):485–492.
30. Buell C, Koo J. Long-term safety of mycophenolate mofetil and cyclosporine: A review. J Drugs Dermatol 2008;7(8):741–748.
31. Sollinger H. Enteric-coated mycophenolate sodium: Therapeutic equivalence to mycophenolate mofetil in de novo renal transplant patients. Transplant Proc 2004;36(2 Suppl):517S–520S.
32. Gabardi S, Cerio J. Future immunosuppressive agents in solid-organ transplantation. Prog Transplant 2004;14(2):148–156.
33. Augustine JJ, Bodziak KA, Hricik DE. Use of sirolimus in solid organ transplantation. Drugs 2007;67(3):369–391.
34. Marder W, McCune WJ. Advances in immunosuppressive therapy. Semin Respir Crit Care Med 2007;28(4):398–417.
35. MacDonald AS. A worldwide, phase III, randomized, controlled, safety and efficacy study of a sirolimus/cyclosporine regimen for prevention of acute rejection in recipients of primary mismatched renal allografts. Transplantation 2001;71(2):271–280.
36. Kreis H, Oberbauer R, Campistol JM, et al. Long-term benefits with sirolimus-based therapy after early cyclosporine withdrawal. J Am Soc Nephrol 2004;15(3):809–817.
37. Holt DW. Therapeutic drug monitoring of immunosuppressive drugs in kidney transplantation. Curr Opin Nephrol Hypertens 2002;11(6):657–663.
38. Ahsan N, Hricik D, Matas A, et al. Prednisone withdrawal in kidney transplant recipients on cyclosporine and mycophenolate mofetil—A prospective randomized study. Steroid Withdrawal Study Group. Transplantation 1999;68(12):1865–1874.
39. Liu CL, Fan ST, Lo CM, et al. Interleukin-2 receptor antibody (basiliximab) for immunosuppressive induction therapy after liver transplantation: A protocol with early elimination of steroids and reduction of tacrolimus dosage. Liver Transpl 2004;10(6):728–733.
40. Laftavi MR, Stephan R, Stefanick B, et al. Randomized prospective trial of early steroid withdrawal compared with low-dose steroids in renal transplant recipients using serial protocol biopsies to assess efficacy and safety. Surgery 2005;137(3):364–371.
41. Kaufman DB, Leventhal JR, Koffron AJ, et al. A prospective study of rapid corticosteroid elimination in simultaneous pancreas-kidney transplantation: Comparison of two maintenance immunosuppression protocols: Tacrolimus/mycophenolate mofetil versus tacrolimus/sirolimus. Transplantation 2002;73(2):169–177.
42. Elbarbry FA, Marfleet T, Shoker AS. Drug-drug interactions with immunosuppressive agents: Review of the in vitro functional assays and role of cytochrome P450 enzymes. Transplantation 2008;85(9):1222–1229.
43. DuBuske LM. The role of P-glycoprotein and organic anion-transporting polypeptides in drug interactions. Drug Saf 2005;28(9):789–801.
44. Prescott WA, Jr, Callahan BL, Park JM. Tacrolimus toxicity associated with concomitant metoclopramide therapy. Pharmacotherapy 2004;24(4):532–537.
45. Gelone DK, Park JM, Lake KD. Lack of an effect of oral iron administration on mycophenolic acid pharmacokinetics in stable renal transplant recipients. Pharmacotherapy 2007;27(9):1272–1278.
46. Lynch T, Price A. The effect of cytochrome P450 metabolism on drug response, interactions, and adverse effects. Am Fam Physician 2007;76(3):391–396.
47. van Duijnhoven EM, Boots JM, Christiaans MH, Stolk LM, Undre NA, van Hooff JP. Increase in tacrolimus trough levels after steroid withdrawal. Transpl Int 2003;16(10):721–725.
48. Aronson J. Serious drug interactions. Practitioner 1993;237(1531):789–791.
49. Baroletti S, Bencivenga GA, Gabardi S. Treating gout in kidney transplant recipients. Prog Transplant 2004;14(2):143–147.
50. Gregoor PJ, de Sevaux RG, Hene RJ, et al. Effect of cyclosporine on mycophenolic acid trough levels in kidney transplant recipients. Transplantation 1999;68(10):1603–1606.
51. Ekbal NJ, Holt DW, Macphee IA. Pharmacogenetics of immunosuppressive drugs: Prospect of individual therapy for transplant patients. Pharmacogenomics 2008;9(5):585–596.
52. Anglicheau D, Legendre C, Beaune P, Thervet E. Cytochrome P450 3A polymorphisms and immunosuppressive drugs: An update. Pharmacogenomics 2007;8(7):835–849.
53. Fishman JA. Infection in solid-organ transplant recipients. N Engl J Med 2007;357(25):2601–2614.
54. Pneumocystis jiroveci (formerly Pneumocystis carinii). Am J Transplant 2004;(4 Suppl)10:135–141.
55. Egli A, Binggeli S, Bodaghi S, et al. Cytomegalovirus and polyomavirus BK posttransplant. Nephrol Dial Transplant 2007;(22 Suppl)8:viii72–viii82.
56. Gabardi S, Magee CC, Baroletti SA, Powelson JA, Cina JL, Chandraker AK. Efficacy and safety of low-dose valganciclovir for prevention of cytomegalovirus disease in renal transplant recipients: A singlecenter, retrospective analysis. Pharmacotherapy 2004;24(10):1323–1330.
57. Paya C, Humar A, Dominguez E, et al. Efficacy and safety of valganciclovir vs. oral ganciclovir for prevention of cytomegalovirus disease in solid organ transplant recipients. Am J Transplant 2004;4(4):611–620.
58. Kethireddy S, Andes D. CNS pharmacokinetics of antifungal agents. Expert Opin Drug Metab Toxicol 2007;3(4):573–581.
59. Beaty CA, Cymet T. Organ transplantation for the primary care provider: What you need to know to get your patient a new liver or kidney. Compr Ther 2008;34(2):69–76.
60. Taylor DO, Edwards LB, Mohacsi PJ, et al. The registry of the International Society for Heart and Lung Transplantation: Twentieth official adult heart transplant report—2003. J Heart Lung Transplant 2003;22(6):616–624.
61. Knoll G. Trends in kidney transplantation over the past decade. Drugs 2008;(68 Suppl)1:3–10.
62. Taler SJ, Textor SC, Canzanello VJ, et al. Role of steroid dose in hypertension early after liver transplantation with tacrolimus (FK506) and cyclosporine. Transplantation 1996;62(11):1588–1592.
63. Salifu MO, Tedla F, Aytug S, Hayat A, McFarlane SI. Posttransplant diabetes and hypertension: Pathophysiologic insights and therapeutic rationale. Curr Diab Rep 2008;8(3):221–227.
64. Perico N, Benigni A, Zoja C, Delaini F, Remuzzi G. Functional significance of exaggerated renal thromboxane A2 synthesis induced by cyclosporin A. Am J Physiol 1986;251(4 Pt 2):F581–F587.
65. Tang IY, Meier-Kriesche HU, Kaplan B. Immunosuppressive strategies to improve outcomes of kidney transplantation. Semin Nephrol 2007;27(4):377–392.
66. Jensik SC. Tacrolimus (FK 506) in kidney transplantation: Three-year survival results of the US multicenter, randomized, comparative trial. FK 506 Kidney Transplant Study Group. Transplant Proc 1998;30(4):1216–1218.
67. Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med 2001;344(1):3–10.
68. Kasiske BL. Hyperlipidemia in patients with chronic renal disease. Am J Kidney Dis 1998;32(5 Suppl 3):S142–S156.
69. Tannock LR, Reynolds LR. Management of dyslipidemia in patients after solid organ transplantation. Postgrad Med 2008;120(1):43–49.
70. Mathis AS, Dave N, Knipp GT, Friedman GS. Drug-related dyslipidemia after renal transplantation. Am J Health Syst Pharm 2004;61(6):565–585; quiz 86–87.
71. Kobashigawa JA, Kasiske BL. Hyperlipidemia in solid organ transplantation. Transplantation 1997;63(3):331–338.
72. Kobashigawa JA, Katznelson S, Laks H, et al. Effect of pravastatin on outcomes after cardiac transplantation. N Engl J Med 1995;333(10):621–627.
73. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285(19):2486–2497.
74. Kasiske BL, Heim-Duthoy KL, Singer GG, Watschinger B, Germain MJ, Bastani B. The effects of lipid-lowering agents on acute renal allograft rejection. Transplantation 2001;72(2):223–227.
75. Downs JR, Clearfield M, Weis S, et al. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: Results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA 1998;279(20):1615–1622.
76. Wenke K, Meiser B, Thiery J, et al. Simvastatin reduces graft vessel disease and mortality after heart transplantation: A four-year randomized trial. Circulation 1997;96(5):1398–1402.
77. Katznelson S, Wilkinson AH, Kobashigawa JA, et al. The effect of pravastatin on acute rejection after kidney transplantation—A pilot study. Transplantation 1996;61(10):1469–1474.
78. Davidson J, Wilkinson A, Dantal J, et al. New-onset diabetes after transplantation: 2003 International consensus guidelines. Proceedings of an international expert panel meeting. Barcelona, Spain, February 19, 2003. Transplantation 2003;75(10 Suppl):SS3–SS24.
79. Traywick C, O’Reilly FM. Management of skin cancer in solid organ transplant recipients. Dermatol Ther 2005;18(1):12–18.
80. Navarro MD, Lopez-Andreu M, Rodriguez-Benot A, Aguera ML, Del Castillo D, Aljama P. Cancer incidence and survival in kidney transplant patients. Transplant Proc 2008;40(9):2936–2940.
81. Gottschalk S, Rooney CM, Heslop HE. Post-transplant lymphoproliferative disorders. Annu Rev Med 2005;56:29–44.
82. Markert E, Siebolts U, Habbig S, et al. Evolution of PTLD following renal transplantation in a child. Pediatr Transplant 2009;13(3):379–383.
83. Marques E, Jimenez C, Manrique A, Vallejo GH, Clemares M, Ortega P, et al. Development of lymphoproliferative disease after liver transplantation. Transplant Proc 2008;40(9):2988–2989.
84. Garrett TJ, Chadburn A, Barr ML, et al. Posttransplantation lymphoproliferative disorders treated with cyclophosphamide-doxorubicin-vincristine-prednisone chemotherapy. Cancer 1993;72(9):2782–2785.