David A. Apgar
LEARNING OBJECTIVES
Upon completion of the chapter, the reader will be able to:
1. Describe two different systems for categorizing allergic rhinitis (AR).
2. Describe the basic pathophysiology of AR.
3. List the typical symptoms of AR and identify the most troublesome one.
4. List the reasons for referral to an allergy specialist.
5. Discuss the categories of pharmacotherapy choices for treatment of AR.
6. Rank the pharmacotherapy choices for efficacy in treating nasal congestion.
7. Describe an approach for treatment of mild AR with over-the-counter (OTC) drugs.
8. Create a therapy plan for treatment of moderate–severe AR.
9. Describe how to monitor patients treated for AR.
10. Identify the differences in approach to the treatment of AR for children, pregnant women, and the elderly, compared to the routine approach in adults.
KEY CONCEPTS
![]() Allergic rhinitis (AR) is an allergen-induced and immunoglobulin E (IgE)-mediated inflammatory condition of the lining of the nose and upper respiratory tract.
Allergic rhinitis (AR) is an allergen-induced and immunoglobulin E (IgE)-mediated inflammatory condition of the lining of the nose and upper respiratory tract.
![]() AR can be categorized in different ways.
AR can be categorized in different ways.
![]() AR is a common disorder that can negatively impact quality of life, yet it has been trivialized in the past.
AR is a common disorder that can negatively impact quality of life, yet it has been trivialized in the past.
![]() The goals of treatment of AR are to reduce or minimize the frequency and severity of symptoms; prevent comorbid disorders and complications; improve the patient’s quality of life; improve work attendance and productivity and/or school attendance and performance; and minimize adverse effects of therapy.
The goals of treatment of AR are to reduce or minimize the frequency and severity of symptoms; prevent comorbid disorders and complications; improve the patient’s quality of life; improve work attendance and productivity and/or school attendance and performance; and minimize adverse effects of therapy.
![]() The general approach for treatment of AR is fourfold: avoidance of allergen triggers, pharmacotherapy, immunotherapy, and patient/family education.
The general approach for treatment of AR is fourfold: avoidance of allergen triggers, pharmacotherapy, immunotherapy, and patient/family education.
![]() Routine first-line agents for the treatment of AR are intranasal corticosteroids and antihistamines (oral and/or intranasal, depending on the patient). Adjunctive or secondary choice agents, each of which may have a first-line role in selected patients, include decongestants, cromolyn, montelukast, ipratropium, and intranasal saline irrigation.
Routine first-line agents for the treatment of AR are intranasal corticosteroids and antihistamines (oral and/or intranasal, depending on the patient). Adjunctive or secondary choice agents, each of which may have a first-line role in selected patients, include decongestants, cromolyn, montelukast, ipratropium, and intranasal saline irrigation.
![]() Intranasal corticosteroids are the most effective therapy for AR, especially for nasal congestion. They are first-line agents for severe manifestations and are also used for those with moderate disease not controlled with oral and/or intranasal antihistamines. Their anti-inflammatory mechanism of action probably contributes to this superiority.
Intranasal corticosteroids are the most effective therapy for AR, especially for nasal congestion. They are first-line agents for severe manifestations and are also used for those with moderate disease not controlled with oral and/or intranasal antihistamines. Their anti-inflammatory mechanism of action probably contributes to this superiority.
![]() Second-generation antihistamines are first-line agents, especially for mild or intermittent AR. They are preferred over first-generation antihistamines because of their improved side-effect profile. While effective for most symptoms of AR, they are less effective than intranasal corticosteroids for nasal congestion (intranasal administration is better than oral administration).
Second-generation antihistamines are first-line agents, especially for mild or intermittent AR. They are preferred over first-generation antihistamines because of their improved side-effect profile. While effective for most symptoms of AR, they are less effective than intranasal corticosteroids for nasal congestion (intranasal administration is better than oral administration).
![]() The best application of decongestants in AR is short-term to overcome severe nasal congestion, including facilitating improved efficacy of intranasal agents. The intranasal administration of decongestants should usually not exceed three consecutive days.
The best application of decongestants in AR is short-term to overcome severe nasal congestion, including facilitating improved efficacy of intranasal agents. The intranasal administration of decongestants should usually not exceed three consecutive days.
![]() Generally speaking, the treatment of AR in children is the same as it is for adults, except for limitations in terms of FDA-approved products for some age groups and route of administration issues with some products.
Generally speaking, the treatment of AR in children is the same as it is for adults, except for limitations in terms of FDA-approved products for some age groups and route of administration issues with some products.
INTRODUCTION1-3
Rhinitis is inflammation of the lining of the nose and other parts of the upper respiratory tract. Allergy is only one cause of rhinitis. While there are several other types of rhinitis (see Table 62–1), and some patients can manifest a mixed form (both allergic and nonallergic rhinitis), allergic rhinitis (AR) will be the focus of this chapter. Because ocular symptoms frequently occur in association with AR, another term used is allergic rhinoconjunctivitis. This acknowledges involvement of the bulbar and palpebral conjunctivae in the allergic process. ![]() AR is an allergen-induced and immunoglobulin E (IgE)-mediated inflammatory condition of the lining of the nose and upper respiratory tract.
AR is an allergen-induced and immunoglobulin E (IgE)-mediated inflammatory condition of the lining of the nose and upper respiratory tract.
![]() AR has traditionally been categorized as either seasonal or perennial. Seasonal allergic rhinitis (SAR) is attributed to inhaled allergens (aeroallergens) that have a seasonal variation. These allergens are usually encountered outdoors and are most often plant pollens and substances from molds and fungi. Perennial allergic rhinitis (PAR) is attributed to aeroallergens that are present in the patient’s environment almost continuously throughout the year and are usually encountered indoors. Common perennial allergens are the house dust mite, indoor molds and fungi, insects (especially cockroaches), and companion animals (pets). Some patients are affected year round, but have seasonal exacerbations. These people are probably allergic to both seasonal and perennial aeroallergens. Other patients have only episodic manifestations. These people are probably allergic to aeroallergens that are only occasionally (episodically) encountered. The Joint Task Force on Practice Parameters (representing the American Academy of Allergy, Asthma and Immunology [AAAAI], the American College of Allergy, Asthma and Immunology [ACAAI], and the Joint Council of Allergy, Asthma and Immunology) published practice parameters for the diagnosis and management of AR in August 2008.1 This document also introduces the term “episodic” AR, as a category in addition to SAR and PAR.
AR has traditionally been categorized as either seasonal or perennial. Seasonal allergic rhinitis (SAR) is attributed to inhaled allergens (aeroallergens) that have a seasonal variation. These allergens are usually encountered outdoors and are most often plant pollens and substances from molds and fungi. Perennial allergic rhinitis (PAR) is attributed to aeroallergens that are present in the patient’s environment almost continuously throughout the year and are usually encountered indoors. Common perennial allergens are the house dust mite, indoor molds and fungi, insects (especially cockroaches), and companion animals (pets). Some patients are affected year round, but have seasonal exacerbations. These people are probably allergic to both seasonal and perennial aeroallergens. Other patients have only episodic manifestations. These people are probably allergic to aeroallergens that are only occasionally (episodically) encountered. The Joint Task Force on Practice Parameters (representing the American Academy of Allergy, Asthma and Immunology [AAAAI], the American College of Allergy, Asthma and Immunology [ACAAI], and the Joint Council of Allergy, Asthma and Immunology) published practice parameters for the diagnosis and management of AR in August 2008.1 This document also introduces the term “episodic” AR, as a category in addition to SAR and PAR.
Table 62–1 Types of Rhinitis
Allergic (see Table 62–2 for details)
Nonallergic
Vasomotor (triggered by irritants, cold air, exercise/running, or unidentified factors)
Food/meal related (gustatory)
Infectious
NARES
Occupational
Caused by protein allergens (IgE-mediated) or by irritants/sensitizers (probably non-IgE-mediated)
Other rhinitis syndromes
Hormonally related (pregnancy and menstrual cycle related)
Drug-related
Rhinitis medicamentosa (rebound from overuse of intranasal decongestants)
Drug-induced
Angiotensin-converting enzyme inhibitor (ACEI)
α-Antagonists (used for treatment of BPH and HT)
Phosphodiesterase-5 inhibitors (used for treatment of ED) Aspirin and other NSAIDs (as an isolated side effect of AERD)
Oral contraceptives (controversial)
Atrophic rhinitis
Rhinitis associated with inflammatory or immunologic diseases (e.g., granulomatous infections, RA, SLE, Wegener’s granulomatosis, sarcoidosis, Churg-Strauss syndrome, and others)
ACEI, angiotensin-converting enzyme inhibitor; AERD, aspirin-exacerbated respiratory disease; BPH, benign prostatic hyperplasia; ED, erectile dysfunction; HT, hypertension; NARES, nonallergic rhinitis with esinophilia [on nasal smear] syndrome; NSAIDs, nonsteroidal anti-inflammatory drugs; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus. From Refs. 1-3.
Recognizing that the traditional categories of seasonal and perennial AR are imperfect, another system for categorizing AR has been suggested by the international group Allergic Rhinit is and its Impact on Asthma (ARIA).2 ![]() This alternative system categorizes the manifestations by a combination of frequency and severity. There are two divisions of frequency: intermittent and persistent. Intermittent frequency is defined as AR manifestations occurring less often than 4 days per week or for fewer than four consecutive weeks. Persistent frequency is defined as AR manifestations occurring for four or more days per week and for four or more consecutive weeks. Severity is categorized either as mild or as moderate–severe. Mild manifestations are those that do not cause interference with sleep, daily activities, or work or school performance and which are not “troublesome.” Moderate–severe manifestations were combined because distinction between moderate and severe was not clinically practical. This category includes those patients with manifestations of AR that do cause interference with sleep, impairment of daily activities, problems at work or school, or are “troublesome.” The ARIA document uses IAR (for intermittent) and PER (for persistent) for the two frequency categories. It is important to realize that IAR and PER are not synonymous with the classical categories of SAR and PAR, respectively. The ARIA system results in four categories: mild intermittent, mild persistent, moderate–severe intermittent, or moderate–severe persistent. The ARIA approach was updated in early 2008.2 See Table 62–2 for a summary of these categories of AR.
This alternative system categorizes the manifestations by a combination of frequency and severity. There are two divisions of frequency: intermittent and persistent. Intermittent frequency is defined as AR manifestations occurring less often than 4 days per week or for fewer than four consecutive weeks. Persistent frequency is defined as AR manifestations occurring for four or more days per week and for four or more consecutive weeks. Severity is categorized either as mild or as moderate–severe. Mild manifestations are those that do not cause interference with sleep, daily activities, or work or school performance and which are not “troublesome.” Moderate–severe manifestations were combined because distinction between moderate and severe was not clinically practical. This category includes those patients with manifestations of AR that do cause interference with sleep, impairment of daily activities, problems at work or school, or are “troublesome.” The ARIA document uses IAR (for intermittent) and PER (for persistent) for the two frequency categories. It is important to realize that IAR and PER are not synonymous with the classical categories of SAR and PAR, respectively. The ARIA system results in four categories: mild intermittent, mild persistent, moderate–severe intermittent, or moderate–severe persistent. The ARIA approach was updated in early 2008.2 See Table 62–2 for a summary of these categories of AR.
EPIDEMIOLOGY
![]() AR is one of the most common chronic disorders in the United States.4 One source indicates that it ranks fifth in this category.5 It is estimated that up to 30% of adults and up to 40% of children in the United States are affected.1,4,6–8 The total direct and indirect costs of AR in the United States for 2002 have been estimated to be in excess of 11 billion dollars.1 AR is the most common allergic disease in children.9
AR is one of the most common chronic disorders in the United States.4 One source indicates that it ranks fifth in this category.5 It is estimated that up to 30% of adults and up to 40% of children in the United States are affected.1,4,6–8 The total direct and indirect costs of AR in the United States for 2002 have been estimated to be in excess of 11 billion dollars.1 AR is the most common allergic disease in children.9
![]() Despite this, the disease has historically been trivialized.
Despite this, the disease has historically been trivialized.
The major risk factors for AR are: a family history of allergic disorder; elevated serum IgE levels, especially before the age of 6 years; higher socioeconomic class; positive skin test results; and emigration into a Western industrialized environment.1,2
Table 62–2 Categories of AR
Based on AAAAI/ACAAI Practice Parameter
Seasonal—symptoms present only during specific portions of the year
Perennial—symptoms present throughout the year
Episodic—symptoms present only during intermittent exposure to allergen trigger
Based on ARIA 2008 Update
Mild versus moderate-severe
Mild means no interference with sleep, daily activities, work or school function and attendance, and no troublesome symptoms
Moderate-severe means the presence of any one of the following: abnormal sleep, impairment of daily activities, impairment of work or school function, troublesome symptoms
Intermittent versus persistent
Intermittent means that symptoms are present for less than
4 days/week, or for less than 4 consecutive weeks Persistent means that symptoms are present for more than
4 days/week and for more than 4 consecutive weeks
Any one of the four possibilities of these variables can occur: mild intermittent, mild persistent, moderate-severe intermittent, and moderate-severe persistent
From Refs. 1-3.
Certain disorders occur commonly with AR. The most important example is asthma. Some sources consider AR and asthma as two manifestations on a spectrum within the same disease. As many as 78% of patients with asthma have AR, and up to 38% of patients with AR have asthma.4,8,10 There is evidence that AR can predispose to the development of asthma.1,4,8,10 Other conditions that can occur with AR include sinusitis, obstructive sleep apnea, otitis media with effusion, and nasal polyposis.1
PATHOPHYSIOLOGY1–3,5,10–12
AR is an IgE-mediated disorder of people who are allergy prone. Initial contact is required to sensitize the patient to subsequent exposures. Patients with an inherited tendency to allergic disorders produce T-helper lymphocyte type 2 (Th-2)-directed responses, including production of specific IgE antibodies, to one or more allergens. The details of the process are complex, and still are being defined. Many cell types, intermediate substances (including cytokines) and mediators are involved. In response to subsequent exposures to the trigger antigen(s), there is an early phase and often a late phase allergic response. The distinction has therapeutic implications.
During the early phase, the trigger allergen becomes bound to IgE that is fixed to mast cells in the nasal mucosa. This occurs within minutes of subsequent exposure to the antigen and causes the mast cells to degranulate. This degranulation results in release of preformed mediators, the most important of which is histamine. This step stimulates more mast cells, as well as macrophages, eosinophils, and basophils to produce more substances, including cysteine leukotrienes and prostaglandin D2. These newly produced mediators bind to receptors in the nose and facilitate many of the manifestations of AR. The resultant vasodilation, mucosal edema, and hypertrophy all contribute to nasal congestion. Clear, watery, and often profuse rhinorrhea is also characteristic in this phase, a combined result of mucous secretion and increased vascular permeability. Sneezing and nasal itch are other prominent features of the early phase. Many patients also have ocular symptoms.
The late phase occurs in up to 50% of AR sufferers. It can begin as soon as 2 hours after the early phase and usually peaks within 12 hours. The late phase involves a second release of many of the mediators of the early phase. In addition, the late phase is characterized by an inflammatory component caused by infiltration of several cell types (e.g., mast cells, eosinophils, basophils, neutrophils, and T lymphocytes) into the nasal mucosa. The most significant manifestation during the late phase is nasal congestion that is often severe and long lasting.
A phenomenon known as the priming response is also of importance. This simply means that prolonged and/or repeated allergen exposure makes it easier to stimulate the process resulting in mediator release and symptoms. The inflammatory component that characterizes the late phase probably contributes to this effect. A vicious cycle results in which smaller doses of allergen can create symptoms (i.e., the threshold is lowered). Thus, even when pollen exposure is decreased, symptoms may continue. In some patients, the threshold is lowered to the degree that even irritant substances (e.g., formaldehyde, tobacco smoke, perfumes, automobile exhaust, and other environmental pollutants) may cause symptoms, on a nonallergic basis.
TREATMENT
Desired Outcomes
![]() The goals of treatment of AR are to reduce or minimize the frequency and severity of symptoms; prevent comorbid disorders and complications; improve the patient’s quality of life; improve work attendance and productivity and/or school attendance and performance; and minimize adverse effects of therapy. Until a cure is established, these are the only realistic goals.
The goals of treatment of AR are to reduce or minimize the frequency and severity of symptoms; prevent comorbid disorders and complications; improve the patient’s quality of life; improve work attendance and productivity and/or school attendance and performance; and minimize adverse effects of therapy. Until a cure is established, these are the only realistic goals.
Nonpharmacologic Therapy
![]() The general approach for treatment of AR is fourfold: avoidance of allergen triggers, pharmacotherapy, immuno-therapy, and patient/family education. Three of these four are nonpharmacologic.
The general approach for treatment of AR is fourfold: avoidance of allergen triggers, pharmacotherapy, immuno-therapy, and patient/family education. Three of these four are nonpharmacologic.
Avoidance of allergen triggers, to the extent they have been identified and to the extent such avoidance is possible, underlies the treatment for all patients with AR (see Table 62–3).1,2 Immunotherapy must be administered by a physician. The initial evaluation includes identification of specific allergens to determine individualized therapy. The role of a pharmacist in immunotherapy is appropriate referral of patients to an allergist or immunologist. See Clinical Presentation and Diagnosis for considerations for referral. At the time of this writing, in the United States, subcutaneous injection immunotherapy is the only option.1–3,13,14 In other parts of the world, sublingual immunotherapy is an alternative.9,15–18 Proposed advantages are mostly ease of administration. Questions remain about comparative efficacy, and the details of optimal dosage, frequency of administration, and duration of therapy. Education of the patient as well as the patient’s support system is essential.1 They need to understand the potential seriousness of AR (including complications such as asthma) and the chronic and/or recurrent nature of the disorder. The patient and significant others should be told about the various treatment options, including their relative advantages and disadvantages. Proper understanding and use of current medication in the patient’s regimen should be assured. A better educated patient and support system will result in a better relationship with health care providers and hopefully will optimize patient outcomes.
Clinical Presentation and Diagnosis of AR 1−4,8
Typical Symptoms
Rhinorrhea (usually clear and bilateral; primarily anterior but may have posterior [postnasal drip])
Sneezing
Itching (affecting mostly the nose, but also the palate, throat, eyes, and ears)
Nasal congestion (usually the most troublesome symptom)
Other Symptoms
Sleep disturbances
Headache, mild facial or ear pain or fullness
Cough (especially in those with concurrent asthma)
Fatigue, asthenia, malaise, and irritability
Ocular manifestations (itch, redness, tearing, chemosis, periorbital edema) Presenteeism (impaired performance at work or school)
Absenteeism from work or school
Quality of life impairment (including social function)
Children (especially): rubbing the nose, snorting, sniffling, clearing the throat, learning or attention problems, poor appetite
Signs (Especially Common in Children)
Rubbing the nose (especially with the back of the hand or the palm; so-called allergic salute, which may create a horizontal crease just above the tip of the nose)
Rubbing/scratching at the eyes
Mouth breathing
Dark circles under the eyes
Dennie-Morgan lines or folds
Diagnosis
Typical symptoms, especially in association with exposure to allergen triggers
Other diagnostic testing usually optional, but may be necessary to rule out nonallergic causes of rhinitis or if immunotherapy is a consideration (physical exam, especially of the upper respiratory tract with emphasis on the nose, specific IgE antibody testing by either skin testing or in vitro serum testing, other specialized testing).
Considerations for Referral
Unilateral rhinitis, nasal obstruction without other typical symptoms of AR
Purulent rhinitis, fever, marked facial or ear pain, or recurrent nose bleeds
Ocular symptoms without typical symptoms of AR Unilateral ocular symptoms, photophobia, or vision changes
Severe symptoms
Failure of therapy (nonresponse or adherence limiting side effects or intolerance)
Desire to have specific allergen triggers identified (e.g., by skin testing)
Candidates for immunotherapy
Concurrent asthma, nasal polyposis, sinusitis, or otitis media with effusion
Pharmacologic Therapy
There are three guideline documents, all published in 2008, that are the basis for the summary that follows.1–3 Other sources provide additional information for the treatment of AR.8–10,13,19–27 The recommended approaches begin with allergen avoidance, emphasize patient/family education, and include immunotherapy as an option in selected patients.
The most reasonable plan may include considerations from several of these documents. ![]() Routine first-line agents are intranasal corticosteroids and antihistamines (oral and/or intranasal, depending on the patient). Adjunctive or secondary choice agents, each of which may have a first-line role in selected patients, include decongestants, the mast cell stabilizer/cromone (cromolyn), the leukotriene receptor antagonist (LTRA) (montelukast), the antimuscarinic/anticholinergic (ipratropium) and intranasal saline. In all cases, therapy must be individualized, in cooperation with the patient. Considerations include frequency and severity of specific symptoms, realistic avoidance measures, patient age, patient preferences for route of administration, tolerance of side effects, adherence issues, comorbid disorders, and concurrent therapy. See Table 62–4 of intranasal and oral medications for the treatment of AR.
Routine first-line agents are intranasal corticosteroids and antihistamines (oral and/or intranasal, depending on the patient). Adjunctive or secondary choice agents, each of which may have a first-line role in selected patients, include decongestants, the mast cell stabilizer/cromone (cromolyn), the leukotriene receptor antagonist (LTRA) (montelukast), the antimuscarinic/anticholinergic (ipratropium) and intranasal saline. In all cases, therapy must be individualized, in cooperation with the patient. Considerations include frequency and severity of specific symptoms, realistic avoidance measures, patient age, patient preferences for route of administration, tolerance of side effects, adherence issues, comorbid disorders, and concurrent therapy. See Table 62–4 of intranasal and oral medications for the treatment of AR.
Table 62–3 Allergen Avoidance Measures
Allergen avoidance underlies all other treatments of AR
There are several limitations to implementing allergen avoidance:
• Identification of allergens is necessary to successfully employ avoidance strategies
• Literature support for a clinically significant impact on symptoms from allergen avoidance, especially any single measure, is meager
• Quality of life may be negatively impacted by forced removal of a pet from the household
Outdoor plant pollen and mold/fungi parts:
• Limit outdoor exposure, especially during high pollen conditions (warm sunny days with wind and low humidity) and during mold/fungi spore release (shortly after rains)
• Wear a face mask during activities that disturb the earth and decaying vegetation
• Keep windows and doors closed
• Use air-conditioning when possible, but maintain clean equipment
Indoor allergens (house dust mite, mold/fungi, cockroaches, and pets):
• Use air-conditioning, as above
• Maintain humidity below 50% if possible, and maintain clean equipment
• Clean frequently and thoroughly to prevent mold growth (dilute bleach with detergent)
• Avoid exposed food and garbage to deter insects, especially in the kitchen
• Clean kitchen frequently and thoroughly
• Use roach traps that facilitate removal of allergen-containing bodies
• Vacuum frequently, and consider use of a high-efficiency particulate air (HEPA) filter
• Minimize carpeting, fabric covered furniture, and fabric wall/window coverings
• Cover bedding (pillow, mattresses, box springs) with allergen-proof, zippered cases
• Launder bedding frequently, in hot water (greater than 130°F or 60°C) if possible, to kill mite ova
• Consider acaricide (e.g., benzyl benzoate) treatment of carpets to kill mites and ova
• Put items that cannot be laundered (e.g., soft toys) in a plastic bag and freeze
• Keep pets out of bedroom and bath cats weekly, if possible
Irritants:
• Avoid to the degree possible, all exposure to smoke, chlorine fumes, formaldehyde fumes, and other substances identified as irritant triggers in the patient (e.g., perfumes, newspaper ink)
From Refs. 1, 2.
The guideline document on AR published in August 2008 by the Joint Task Force (for AAAAI and ACAAI) includes an action plan (similar to what is used for asthma). The entire article, with the action plan, is available on the AAAAI website (http://www.aaaai.org/professionals/resources/pdf/rhinitis2008.pdf) in the public domain, for universal access.1 The application of the differently colored zones on the action plan is explained at the bottom of the form, which is on page S25 of the document. Many patients will benefit from having an action plan.
Table 62–4 Intranasal and Oral Medications for AR
Corticosteroids
Intranasal a (budesonide, beclomethasone, ciclesonide, flunisolide, fluticasone [propionate and furoate], mometasone, triamcinolone)
Oral (rarely used)
Parenteral (not recommended)
Antihistamines
Intranasala (azelastine, olopatadine)
Oralb
• First generation/sedating (cautious use in selected patients) (most OTC depending on strength: diphenhydramine, chlorpheniramine, clemastine, and others)
• Second generation/low- or nonsedatinga (desloratadine, fexofenadine, levocetirizine; OTC: loratadine, cetirizine)
Mast cell stabilizer/cromone
Intranasal (OTC: cromolyn)
Decongestant
Intranasal (short-term use) (tetrahydrozoline; OTC: phenylephrine, naphazoline, oxymetazoline)
Oral b (OTC: phenylephrine; BTC c: pseudoephedrine)
LTRA
Oral (montelukast is only one indicated)
Antimuscarinic
Intranasal (ipratropium)
Note: All products are Rx unless indicated OTC.
a First-line choices.
b Some products combine an antihistamine with a decongestant, sometimes with other ingredients.
c Behind the counter (OTC plus other requirements necessary; see the Decongestants section of text).
From Refs. 1–3, 24–28.
First-Line Agents
Corticosteroids
Corticosteroids are usually administered by the intranasal route for the treatment of AR. Occasionally, a short course of oral therapy (burst and taper) is necessary. This oral use of corticosteroids is best applied to overcome severe nasal congestion, particularly that due to rhinitis medicamentosa from intranasal decongestants (see Decongestant section below). Parenteral administration of corticosteroids in the management of AR is discouraged.1
![]() Intranasal corticosteroids are considered the most effective therapy for AR. They are recommended as the drugs of choice for severe manifestations, and for those with moderate disease not controlled with oral and/or intranasal antihistamines. They provide very good relief for sneezing, itching, rhinorrhea, as well as nasal congestion and even ocular symptoms. Nasal congestion is often the most bothersome symptom of AR, and the most difficult to control. This is probably because it results from inflammation that predominates in the late phase of the allergic response in AR.
Intranasal corticosteroids are considered the most effective therapy for AR. They are recommended as the drugs of choice for severe manifestations, and for those with moderate disease not controlled with oral and/or intranasal antihistamines. They provide very good relief for sneezing, itching, rhinorrhea, as well as nasal congestion and even ocular symptoms. Nasal congestion is often the most bothersome symptom of AR, and the most difficult to control. This is probably because it results from inflammation that predominates in the late phase of the allergic response in AR. ![]() Intranasal corticosteroids are the best agents for nasal congestion, probably because of their anti-inflammatory mechanism of action.1,13,21 Systemic corticosteroids (i.e., orally administered) are also effective, but they are used only as a last resort due to systemic side effects.
Intranasal corticosteroids are the best agents for nasal congestion, probably because of their anti-inflammatory mechanism of action.1,13,21 Systemic corticosteroids (i.e., orally administered) are also effective, but they are used only as a last resort due to systemic side effects.
Several meta-analyses have evaluated the relative efficacy of intranasal corticosteroids in comparison with other types of pharmacologic therapy of AR. The majority (but not all) of the literature suggests that intranasal corticosteroids are superior to intranasal antihistamines, to oral antihistamines, even when combined with a leukotriene antagonist, and to a leukotriene antagonist alone.1,13
There are currently eight intranasal corticosteroid products available in the United States, including two different salt forms of fluticasone. Most (e.g., budesonide, ciclesonide, fluticasone furoate, mometasone, and triamcinolone) are usually given in a single daily dose. However, fluticasone propionate may be given either once or twice daily; beclomethasone is usually given twice daily; and flunisolide is given two or three times daily. Despite some differences in formulation, potency, chemistry, and pharmacokinetic and pharmacodynamic properties among the products, there is no good evidence that any single product is superior in efficacy. Intranasal corticosteroids are best given regularly, as the onset of action usually takes up to 12 hours and the maximum effects may be delayed up to 7 to 14 days.1,8,10 However, there is evidence that in some people the onset is within 3 to 4 hours, so these agents may even be used on an as needed basis.1,29 When nasal congestion is severe, intranasal administration may not be effective due to limited exposure to the nasal mucosa. In that situation, short-term intranasal decongestants may facilitate better exposure. See Table 62–5 for intranasal corticosteroid products.
The correct technique for administration of intranasal medication is important for optimum efficacy. Consult the individual product labeling for specific instructions. However, also see Table 62–6 for general instructions for the optimal administration of intranasal medications. The technique described maximizes exposure of the drug to the nasal mucosa to optimize efficacy, and minimizes both exposure to the nasal septum and loss of medication down the esophagus. See later for instructions about preparation and use of intranasal saline irrigations.
Most patients tolerate intranasal corticosteroids very well. Local side effects include nasal burning, irritation, and dryness, which may occur in up to 12% of patients.1,8,10,13,22 Also, up to 10% to 12% of patients may experience mild epistaxis.13,23 This may be partly due to the administration technique. Sore throat and headache may be noted by some patients.24 Perforation of the nasal septum is a very rare side effect. This can be minimized by proper administration technique (see Table 62–6), specifically, directing the spray laterally (away) from the (medial) nasal septum.1,10
The older intranasal corticosteroids (beclomethasone, flunisolide, and budesonide) have significant absorption, while the newer products (fluticasone, mometasone, and ciclesonide) have bioavailability of no more than 1% to 2%.13 The decreased absorption minimizes systemic side effects. However, there is still some concern for growth suppression, other manifestations of hypothalamic–pituitary–adrenal (HPA) axis suppression, bone, and ocular effects.13 Several studies have evaluated the effects of intranasal and inhaled corticosteroids on HPA axis suppression and growth.1,13 Most have shown little or no clinically significant effects. The product most implicated with growth suppression is beclomethasone. One study demonstrated suppression in children using the drug for 1 year, but at twice the usual recommended dose.1 There is no confirmation of a causal effect of intranasal corticosteroids on posterior subcapsular cataracts, increased intraocular pressure, or decreased bone density; however, those with risk factors for any of these conditions should be monitored carefully for their development. Ultimately, patient preference for a specific intranasal corticosteroid may be determined more by cost and by formulation differences that affect odor and aftertaste.
Antihistamines
Antihistamines used for the treatment of AR are administered by either the oral or the intranasal route. These agents interact with the H1 (histamine type 1) receptor. Histamine is involved with both the early and the late phases of AR. Activation of H1 receptors in the nose, upper airway mucosa, and the eye produces the common manifestations of AR (sneezing, itching, rhinorrhea, nasal congestion, and ocular symptoms). ![]() The antihistamines are very effective for the sneezing, itching, and rhinorrhea of AR. There is some effect to improve nasal congestion, but less so than for the other symptoms. There is also benefit for the ocular symptoms (e.g., itch, redness, tearing). Intranasal administration is more effective than oral administration for the nasal congestion, but less effective for the ocular symptoms. The onset of action by oral administration is usually within 1 to 2 hours, and that for intranasal administration within 30 minutes.1,8,13 All antihistamines probably provide better relief if used continuously (during symptomatic periods of seasonal AR, or for perennial or persistent AR), but they are also effective used only when needed.
The antihistamines are very effective for the sneezing, itching, and rhinorrhea of AR. There is some effect to improve nasal congestion, but less so than for the other symptoms. There is also benefit for the ocular symptoms (e.g., itch, redness, tearing). Intranasal administration is more effective than oral administration for the nasal congestion, but less effective for the ocular symptoms. The onset of action by oral administration is usually within 1 to 2 hours, and that for intranasal administration within 30 minutes.1,8,13 All antihistamines probably provide better relief if used continuously (during symptomatic periods of seasonal AR, or for perennial or persistent AR), but they are also effective used only when needed.
Table 62–5 Intranasal Corticosteroids

Table 62–6 Administration Instructions for Intranasal Medications
1. Clear the nose of mucus and debris to the extent possible
2. Consult product labeling for preadministration instructions (e.g., shaking the container, priming the spray pump)
3. If seated or standing, do not just tilt head backward. This increases the amount of the dosage lost down the esophagus. This decreases efficacy and increases the potential for systemic absorption and thus systemic side effects
4. If standing, bend the head forward (flex the chin onto the chest) so that the nose is the lowest portion of the head. This is best for nasal sprays
If possible, lie in the prone position with the stomach (ventral side) on a flat surface or kneel down. Then, flex chin onto neck, so that the open nostrils are pointing as far upward, toward the ceiling as possible. This position may be best for nose drops (more volume than sprays)
An alternate position is to lie supine (on the back) on a flat surface, then bend the head backward (extend the head), again, so that the open nostrils point upward toward the ceiling
5. Use the contralateral hand to insert the spray nozzle or dropper into one nostril (i.e., the left hand for right nostril)
6. Use the other hand to occlude the opposite nostril (the one not being medicated)
7. Aim the spray or drops toward the outer (lateral) internal surface of each nostril, and away from the nasal septum (which is the inner or medial surface)
8. Breath in slowly but deeply through the medicated nostril
9. Repeat this procedure to apply medication to the other nostril
10. Consult the product labeling for cleaning instructions
11. See the text for information about preparation and use of saline irrigation
From Refs. 3, 8.
Antihistamine drugs used for AR are technically inverse agonists, not competitive antagonists; however, there may be little clinical significance to the difference.10,13,21 These drugs bind to the H1 receptor, changing its three-dimensional conformation such that it is kept in t he inactive state. This results in downregulation of H1 receptor activity and a decrease in end organ effects. These agents do not prevent release of histamine.
The oral agents are divided into first- and second-generation drugs. The first-generation agents are distributed among six chemical classes, including the more sedating ethanolamine class (e.g., diphenhydramine) and the least sedating alkylamine class (e.g., chlorpheniramine). ![]() Most sources now discourage the routine use of the first-generation agents for AR. This is due to their CNS and anticholinergic side effects. The CNS effects are primarily sedation, as well as impairment of cognitive function and performance of tasks. Studies have shown that decision making and driving or work performance are impaired even when the patient is unaware of any overt effects.1 There is also evidence of decreased performance at school and impaired learning, among pediatric patients.1 Some controversy remains, however, about how common these problems truly are.23 The major anticholinergic (perhaps more accurately stated as antimuscarinic) effects include blurred vision, dry mouth, urinary retention, and constipation. The only possible advantage of the antimuscarinic properties is an additional effect to decrease rhinorrhea. However, some patients complain about the increased thickness of the secretions.21 Another disadvantage of the first-generation antihistamines is that most must be administered three to four times daily. If first-generation antihistamines are recommended by a health care practitioner, care must be taken to educate the patient about these CNS and anticholinergic side effects. Patients who take other sedative substances are prone to an additive effect from the antihistamine. Those taking any other medications with anticholinergic or antimuscarinic properties may experience additive effects from the antihistamine. The elderly are, in general, more sensitive to both types of adverse effects.
Most sources now discourage the routine use of the first-generation agents for AR. This is due to their CNS and anticholinergic side effects. The CNS effects are primarily sedation, as well as impairment of cognitive function and performance of tasks. Studies have shown that decision making and driving or work performance are impaired even when the patient is unaware of any overt effects.1 There is also evidence of decreased performance at school and impaired learning, among pediatric patients.1 Some controversy remains, however, about how common these problems truly are.23 The major anticholinergic (perhaps more accurately stated as antimuscarinic) effects include blurred vision, dry mouth, urinary retention, and constipation. The only possible advantage of the antimuscarinic properties is an additional effect to decrease rhinorrhea. However, some patients complain about the increased thickness of the secretions.21 Another disadvantage of the first-generation antihistamines is that most must be administered three to four times daily. If first-generation antihistamines are recommended by a health care practitioner, care must be taken to educate the patient about these CNS and anticholinergic side effects. Patients who take other sedative substances are prone to an additive effect from the antihistamine. Those taking any other medications with anticholinergic or antimuscarinic properties may experience additive effects from the antihistamine. The elderly are, in general, more sensitive to both types of adverse effects.
Currently available oral second-generation H1 antihistamines are cetirizine, levocetirizine, loratadine, desloratadine, fexofenadine, and acrivastine. All except acrivastine are available alone, and some are marketed in combination with the decongestant pseudoephedrine. At the time of this writing, only cetirizine and loratadine are available OTC. The second-generation antihistamines do not have the anticholinergic effects of the first-generation agents. Based on current literature, no single H1 antihistamine (first or second generation) is clearly superior in efficacy; however, very few head to head comparative studies have been conducted. The oral second-generation antihistamines are effective for the sneezing, itching, and rhinorrhea of AR, but less effective for the nasal congestion. They also improve ocular symptoms. Intranasal antihistamines are better for nasal congestion.
Fexofenadine has virtually no sedative effects, even at doses higher than usually recommended. Loratadine and desloratadine are not sedative at recommended doses, but can be at higher doses. Cetirizine, levocetirizine, and acrivastine have some sedative effects, even at recommended doses.1 All the oral second-generation agents require some dosage reduction with impaired renal function, although the specific recommendations vary with creatinine clearance.30 To date, none of the currently available oral second-generation antihistamines have been reported to cause QT prolongation or torsade de pointes, as were associated with the two agents that have been removed from the U.S. market (terfenadine and astemizole).13 Most of the oral second-generation antihistamines can be administered once daily (except for the lower dosage forms of fexofenadine), which probably improves adherence.
There are only two intranasal antihistamine products available in the U.S. market at the time of this writing. Both azelastine and olopatadine are considered second-generation agents, although they also have some mast cell stabilizing effects.24 Both are available only by prescription. The most common side effect of these products is a bitter taste. This occurs in up to 20% of patients on azelastine, and probably somewhat fewer on olopatadine.1 Also, there is enough systemic absorption to cause sedation in some patients using azelastine (about 10%) and perhaps somewhat fewer on olopatadine.1 However, there are no direct comparisons of the two agents, so definitive statements regarding their relative efficacy and side-effect incidence cannot be made. See Table 62–7 for the single-agent second-generation antihistamine products.
![]() Many patients with mild to moderate AR are adequately treated with an OTC oral first- or (preferably) second-generation antihistamine alone. Others may prefer the intranasal administration of an antihistamine, but these require a prescription. Still others may prefer fexofenadine by prescription due to the absence of sedation. Some patients will need or prefer combination therapy. If nasal congestion is not relieved by the above regimens, addition of a decongestant is reasonable, either alone or as a combination product (see Decongestant section below). Perhaps even the combination of an oral with an intranasal antihistamine is reasonable for some patients, depending on their preferences. Other pharmacologic agents can be combined with oral and/or intranasal antihistamines, as necessary for optimal control of symptoms (see below).
Many patients with mild to moderate AR are adequately treated with an OTC oral first- or (preferably) second-generation antihistamine alone. Others may prefer the intranasal administration of an antihistamine, but these require a prescription. Still others may prefer fexofenadine by prescription due to the absence of sedation. Some patients will need or prefer combination therapy. If nasal congestion is not relieved by the above regimens, addition of a decongestant is reasonable, either alone or as a combination product (see Decongestant section below). Perhaps even the combination of an oral with an intranasal antihistamine is reasonable for some patients, depending on their preferences. Other pharmacologic agents can be combined with oral and/or intranasal antihistamines, as necessary for optimal control of symptoms (see below).
Patient Encounter, Part 1
AW is a 26-year-old woman who presents to your clinic or store. She moved to this part of the country with her husband and 2-year-old son about 3 months ago. She complains of sneezing and runny nose, which began for the first time as an adult about 2 months ago. Her symptoms are worse when she is outdoors, especially if the weather is windy. She has symptoms almost every day, and the symptoms interfere with her sleep. She awakens tired and feels that way most of the day. She indicates that she has no other medical problems and is taking no chronic medications. She asks your recommendation for OTC treatment.
What symptoms are consistent with AR?
How would you categorize this patient’s condition?
What would you suggest for initial management?
Table 62–7 Single-Agent Second-Generation Antihistamine Products (Oral and Intranasal)

Adjunctive or Secondary Choice Agents
Decongestants
Decongestant drugs are useful to relieve the nasal congestion component of AR.1–3,10,13 This is due to their α1 adrenergic agonist activity, which results in constriction of the vasculature in the nasal mucosa. They do not prevent release of any of the mediators involved in AR. Thus, they do not provide any benefit for the sneezing, itching, rhinorrhea, or the ocular manifestations. Decongestants can be given alone, either by the oral or by the intranasal route. Also, numerous combination products, consisting of a decongestant with an antihistamine (and sometimes other ingredients), are available as oral medications. There are some special considerations for use of decongestants in pediatric and pregnant patients (see the Special Populations section later).
Oral decongestant products are currently limited to pseudoephedrine and phenylephrine (phenylpropanolamine was removed from the market in 2000).10 Pseudoephedrine has been changed from truly OTC to a more controlled status because it is an ingredient in the illicit manufacture of methamphetamine. The new, so-called behind-the-counter (BTC) status, established by the federal Combat Methaphetamine Act of 2005, requires special storage; photo identification of purchasers; a log book of sales, which must be signed by purchasers; and specific limitations on daily and monthly quantities.31,32 Subsequent to this change in status of pseudoephedrine, some manufacturers changed the ingredients of their products by replacing psuedoephedrine with phenylephrine. This was probably to maintain shelf presence in the OTC sales area. However, much controversy surrounds the efficacy of oral phenylephrine. At the time of this writing, the clinical literature suggests that the currently recommended adult dose is minimally effective as a nasal decongestant.33–35
The side effects of orally administered decongestants most often affect cardiovascular function or the CNS. The side effects are primarily due to sympathetic stimulation, and are usually dose-related. Some elevation of blood pressure may occur, but in normotensive and well-controlled hypertensive patients, the elevation is usually small. It is not of clinical significance in most situations, especially considering that these drugs are most appropriately used only briefly or intermittently. Insomnia, nervousness, irritability, and anxiety are relatively common CNS side effects. Some patients may have decreased appetite, tremors, headache, and even hallucinations. Men with benign prostatic hyperplasia (BPH) and other patients with disorders causing bladder outlet obstruction may have increased urinary retention due to α1stimulation of the urethral sphincter. Theoretically, there may be some differences in the side effects between pseudoephedrine and phenylephrine. This is due to their effects on sympathetic nervous system receptors. Pseudoephedrine stimulates both α and β receptors, whereas the effects of recommended oral doses of phenylephrine are essentially limited to stimulation of α receptors. Comparative studies are not available to confirm these differences in the clinical setting.
The intranasal agents currently available include the OTC products phenylephrine, oxymetazoline, and naphazoline, and the prescription product tetrahydrozoline. Product labeling should be followed for dosage, but it is noteworthy that oxymetazoline is the longest acting of these agents, and is usually given only twice daily. Intranasal application of decongestants provides rapid and effective relief of nasal congestion. This therapy may provide relief for nasal congestion, even for those patients already on intranasal corticosteroids.36 However, the continuous use of intranasal decongestants often causes a paradoxical rebound phenomenon of persistent nasal congestion, called rhinitis medicamentosa.1–3,10,37 ![]() While some patients do not develop rhinitis medicamentosa even after several weeks of continuous use of intranasal decongestants, the usual recommendation is to use them for no more than three consecutive days.1 Intranasal decongestants can cause local side effects, including stinging, burning, dryness, and even sneezing. These are usually mild and well tolerated. Due to very limited absorption, the intranasal route rarely causes systemic side effects.1,8,10 Administration technique should be optimized as described in Table 62–6. Should rhinitis medicamentosa occur, the best management is first to discontinue the decongestant, possibly with a taper to minimize worsening the situation. However, the response to withdrawal is often delayed for days. Therefore, it may be necessary to start intranasal corticosteroids, and/or (especially if intranasal corticosteroids are already part of the patient’s regimen) begin a short course of oral corticosteroid.37
While some patients do not develop rhinitis medicamentosa even after several weeks of continuous use of intranasal decongestants, the usual recommendation is to use them for no more than three consecutive days.1 Intranasal decongestants can cause local side effects, including stinging, burning, dryness, and even sneezing. These are usually mild and well tolerated. Due to very limited absorption, the intranasal route rarely causes systemic side effects.1,8,10 Administration technique should be optimized as described in Table 62–6. Should rhinitis medicamentosa occur, the best management is first to discontinue the decongestant, possibly with a taper to minimize worsening the situation. However, the response to withdrawal is often delayed for days. Therefore, it may be necessary to start intranasal corticosteroids, and/or (especially if intranasal corticosteroids are already part of the patient’s regimen) begin a short course of oral corticosteroid.37
Despite the usual good tolerance of recommended doses of oral decongestants, caution is warranted when they are used in patients with cardiac disease (dysrhythmias, angina pectoris, heart failure), hypertension, cerebrovascular disease, bladder outlet obstruction (including BPH), glaucoma (especially closed angle), hyperthyroidism, and possibly diabetes.1,10,13 ![]() The best application of decongestants in AR is short-term to overcome severe nasal congestion, especially to facilitate improved efficacy of (other) intranasal agents (e.g., corticosteroids and antihistamines). The choice between the two routes of administration is based on several considerations, including cost, convenience, patient preference, speed of onset (within 30 minutes orally, within 5–10 minutes for intranasal), and side effects.1,8,38
The best application of decongestants in AR is short-term to overcome severe nasal congestion, especially to facilitate improved efficacy of (other) intranasal agents (e.g., corticosteroids and antihistamines). The choice between the two routes of administration is based on several considerations, including cost, convenience, patient preference, speed of onset (within 30 minutes orally, within 5–10 minutes for intranasal), and side effects.1,8,38
Mast Cell Stabilizer/Cromone1,10,21,22,38
Cromolyn is the only agent in the cromone class that is approved in the United States for treatment of AR. It is available as an OTC intranasal product. The mechanism of action in AR is mast cell stabilization. The drug binds to mast cells, and prevents release of the mediators of AR that would otherwise result from allergen exposure. The drug is moderately effective, but less so than both intranasal corticosteroids and oral or intranasal antihistamines. It does have effects on both early and late phases of AR. Its effects begin within 4 to 7 days of use, but may not be maximal for up to 2 weeks.1 However, it can be used effectively on an as needed basis for episodic exposures to allergen.1 As with all intranasal products, if there is severe nasal congestion, exposure will be limited. Short-term use of a decongestant or an intranasal antihistamine may solve this problem. Cromolyn is very well-tolerated. The most common side effects are mild local stinging and/or burning, sneezing, unpleasant taste, and possibly nose bleed. A disadvantage is the frequency of administration. At least initially, it should be used four times daily. Some patients may need only two or three daily doses when used continuously after the first few weeks at four times daily. It is most useful for patients with mild or intermittent symptoms, in the pediatric population and in pregnant women.
Patient Encounter, Part 2
AW returns after 3 weeks of the OTC therapy that you suggested. There is some improvement in her symptoms, but nasal congestion still interferes with her sleep.
What additional information do you want?
What can you offer her in the way of additional OTC therapy?
Patient Encounter, Part 3
AW returns to talk with you 6 months after your first encounter with her. Since talking with you last, her symptoms almost went away completely, until about 1 month ago. Now she notices sneezing, runny nose, itchy nose, and watery itchy eyes even if she is indoors. The symptoms are present every day. She again has trouble sleeping due to nasal congestion. She still has some of the OTC medications you recommended, but they are not working as well now as previously.
How would you characterize her problem now?
What could you suggest now to help her?
Leukotriene Receptor Antagonist
Leukotrienes are involved in the pathophysiology of AR, and in particular contribute to the nasal congestion in the late phase.1 They contribute little if anything to nasal itch and sneezing.38 Leukotriene antagonists have been shown to be effective for some of the manifestations of AR. Montelukast is the only agent in this class with FDA approval for treatment of AR. It is marketed as oral granules, and as both chewable and swallow tablets. The majority of clinical studies published to date indicate that montelukast is inferior to intranasal corticosteroids.1,10,13,38 Montelukast is either equivalent or slightly inferior to oral H1 antihistamines.1,10,24,38 The combination of montelukast with an oral antihistamine shows improved efficacy over either agent alone.13 However, even the combination is probably not better than intranasal cor-ticosteroids.1 The onset of action of montelukast is delayed for a day or more.1 The drug is usually considered to be very well-tolerated with minimal side effects. However, in March 2008, based on reports to the manufacturer, the FDA issued a preliminary report concerning an investigation into cases of behavior change and suicidal ideation in association with the drug.39 It is administered once daily, considered safe (FDA Pregnancy category B and indicated for children as young as 6 months of age), and particularly well-suited to those patients who have concurrent asthma and AR.
Antimuscarinic (Anticholinergic) Agent1
Ipratropium is currently the only antimuscarinic (or anticholinergic) agent indicated for treatment of AR. It is a quaternary ammonium structure, so systemic absorption is minimal. The product is available by prescription as an intranasal spray. Its use is limited to those patients whose rhinorrhea has not been controlled by other therapy (antihistamines and/or intranasal corticosteroids). There are two strengths available. The 0.03% product is approved for AR in children as young as 6 years of age. The 0.06% product is indicated for rhinorrhea associated with the common cold, in children as young as 5 years old. Local side effects are essentially limited to mild epistaxis and nasal dryness.
Saline 1,40,41
Nasal administration of saline is an alternative for treatment of AR. This therapy may benefit any patient with AR. Saline may be administered as drops or a spray, but the irrigation mode of administration is popularly known by several terms, including neti pot, nasal wash, nasal douche, nose bidet, as well as nasal irrigation.40 While less effective than intranasal corticosteroids, it has been shown to improve sneezing and nasal congestion. It can be used either alone or as add-on therapy. It is best to use canning or pickling salt, which has no iodine, preservatives, or other additives, all of which can be irritating. It appears that isotonic saline is as effective as hypertonic solutions.
An approximate isotonic concentration can be made by dissolution of one teaspoonful of noniodized salt (sodium chloride) in one pint of water. The AAAAI has another recipe.41 Their instructions start with preparation of the dry powder component. This is done by combining three heaping teaspoon-fuls of pickling salt with one rounded teaspoonful of baking soda, and mixing thoroughly. Then, one teaspoonful of the dry powder mixture is dissolved in one cup (8 oz) of lukewarm water. It is best if the water is distilled or has been boiled. About 4 oz of this solution will be used to irrigate each side of the nose. Application can be accomplished while the patient is in the shower or leaning over a sink. The head is bent forward and downward, then tilted to the side opposite the treated nostril. That is, the head is tilted to the left if the right nostril will be irrigated. Then, with a bulb syringe or similar device, slowly introduce about 4 oz of the warm saline solution into one side. Soon, the solution will run out of the opposite nostril. The position of the head should be adjusted as necessary to avoid the solution running into the ears or down the throat. Another source has slightly different instructions for preparation and use.40
Nasal irrigation is one delivery method, although the optimal method (spray, drops, nebulizer, or irrigation) is not known. Optimal frequency of administration is also not known. Nasal irrigation is usually given twice daily, but use of smaller volumes as spray products may be given up to four times daily. Local side effects are usually limited to minor nasal irritation. Nausea has been reported.
Patient Encounter, Part 4
AW returns about 1 year later (she is now 27 years old), and asks what you can recommend for her (now 3-year-old) son, who seems to have developed the same AR that she has. Junior is fussy during the day, constantly rubs his nose, sniffles, and sneezes. He does not sleep through the night because of runny nose and congestion. He even snores because his nose is so stuffed up that he has to breathe through his mouth. She notices dark circles and some lines under his eyes. A neighbor gave her some Benadryl-D Children’s Allergy and Sinus and her mother-in-law gave her some Allerfrim. Junior is otherwise healthy, up to date on immunizations and weighs about 16 kg (35 lb). According to the medication labels, the dosage for Junior would be ½ teaspoonful up to four times a day. So, mom has been giving that dose of both medications for the last 2 days. It helps some, but Junior is even more fussy.
What information suggests that Junior also has AR?
What more information do you need?
What would you recommend at this time?
Omalizumab1,22,38
Omalizumab is a monoclonal antibody that binds to IgE. The product is approved for asthma, but not for AR. It is administered by subcutaneous injection. Dosage is determined by the patient’s circulating IgE levels. The cost is high compared to other commonly used modes of therapy for both asthma and AR. Investigational use has demonstrated efficacy in AR, although relative efficacy compared to other modes of therapy for AR is unknown. Its use is best limited to those with concurrent asthma and AR, pending specific approval for AR.
Complementary and Alternative Medicine Therapy
While some would consider saline in the category of complementary and alternative agents, this monograph considers it as an adjunctive mode. Complementary and alternative therapy for AR has been reviewed.42 Consistent evidence for efficacy has not been established and there are some safety concerns.
Special Populations
Children ![]() Generally speaking, the treatment of AR in children is the same as it is for adults. There are, however, limitations in terms of FDA-approved products for different age groups. Also, depending on the age of the patient, there may be administration issues with some products. Most children affected by AR are more than 2 years old, although the disease may begin in children as young as 6 months of age.1
Generally speaking, the treatment of AR in children is the same as it is for adults. There are, however, limitations in terms of FDA-approved products for different age groups. Also, depending on the age of the patient, there may be administration issues with some products. Most children affected by AR are more than 2 years old, although the disease may begin in children as young as 6 months of age.1
There has been concern about use of combination cough and cold products (many contain an antihistamine and a decongestant) in children. In October 2007, the Nonprescription Drug Advisory Committee of the FDA recommended that OTC combination cough and cold products be limited to children 6 years of age and older. This was based on reports of over 100 deaths in association with these combination products.1 Most of these bad outcomes seem to have resulted from inadvertent overdosage, often by giving doses of the same medication from different combination products. In October 2008, the FDA notified consumers and health care providers that the Consumer Health Protection Agency (CHPA) decided to voluntarily modify the labeling of combination cough and cold products to indicate that they should not be used in children less than 4 years old.43 The CHPA is an association comprised of most of the manufacturers of these products. The announcement indicated that the FDA supports this decision.
First-generation H1 antihistamines are discouraged for children as they are for adults, due to the possible detrimental effects on school performance and learning. Second-generation (less sedating) H1antihistamines (primarily for mild or intermittent symptoms) or intranasal corticosteroids (for moderate-severe or persistent manifestations) are first-line modes of therapy. Antihistamines may need to be used even for more severe and/or persistent symptoms in those children who have difficulty with use of intranasal products. If necessary, these two classes can be combined.
See Table 62–7 for dosages of second-generation antihistamines by age groups for which they are indicated. If first-generation antihistamines are used, the health care practitioner should guarantee that the family members or caretakers are carefully and thoroughly educated to read and use the dosage recommendations appropriate for age or weight of the patient, as indicated on the product labeling. They should also be warned about the possibility of a paradoxical CNS stimulant side effect. Special care should be given to avoid administration of the same medication from different (especially combination) products. The most common side effects of second-generation antihistamines in children are similar to those for adults.
See Table 62–5 for dosages of intranasal corticosteroids by age groups for which they are indicated. The consensus of opinion about intranasal corticosteroids and systemic side effects, especially delay in growth, is that most products are safe. The greatest potential for problems may exist with beclomethasone.1 Several products have been studied in children and have not been shown to delay growth. However, not every product has been studied carefully in all age groups. Some of the conclusions about safety are extrapolated from data with inhaled corticosteroids, used for asthma. The local side effects of intranasal corticosteroids are the same in children as for adults.
Other therapy options may be worth consideration for some pediatric patients. Montelukast provides an oral alternative, especially for those who are too young to cooperate with intranasal administration of corticosteroids. It may be used in combination with an oral antihistamine in hopes of providing some additional efficacy. Another advantage of montelukast is that it is indicated for children as young as 6 months. Another option for mild or intermittent symptoms is intranasal cromolyn, primarily due to its excellent safety. This OTC product is labeled for use in children 2 years of age and older. Intranasal ipratropium is indicated for patients 6 years of age or older and may benefit unresponsive rhinorrhea.
Table 62–8 Intraocular Medication
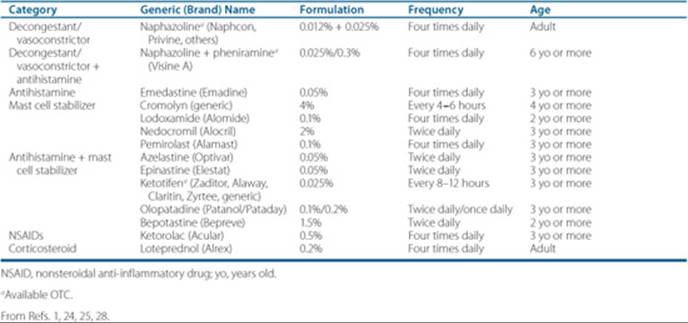
Table 62–9 Routine Approach to Therapy of AR
All patients should practice avoidance of identified allergens to the extent possible
Mild intermittent (including many patients with what some would call seasonal AR)
First line:
Oral antihistamine (OTC, initially; preferably second generation)
Adjunctive/secondary (may use more than one):
Add OTC oral decongestant for nasal congestion
Add short-term OTC intranasal decongestant for refractory nasal congestion
Add nasal irrigation
Consider prescription therapy for inadequate response (see below)
Possibly consider referral for immunotherapy
Persistent or moderate–severe
First line:
Intranasal corticosteroid
Add oral antihistamine for possible additional benefit if necessary
Adjunctive/secondary (may use more than one):
Add short-term intranasal decongestant for refractory nasal congestion
Add nasal irrigation
Add ipratropium for inadequately controlled rhinorrhea
Consider replacement of one first-line agent, if poorly tolerated, with montelukast
Consider referral for immunotherapy
Episodic (no order of preference intended)
Intranasal cromolyn (OTC)
Intranasal antihistamine
Intranasal corticosteroid
Special situations (children, pregnant women, elderly, athletes, ocular symptoms)
See Special Populations section of text
From Refs. 1–3, 8, 10, 19–21, 23, 24, 38.
Pregnant Women1,44
Women who have AR may suffer an exacerbation of symptoms during pregnancy. However, only minor changes in the routine approach to therapy are necessary as a result of the pregnancy. Second-generation antihistamines are generally considered safe, based on an increasing number of studies and experience.1 The same generalization applies to intranasal corticosteroids. However, the products with the best documented safety record are beclomethasone, budesonide, and fluticasone propionate.1 If an intranasal product is started during pregnancy, the wisest choice might be to use budesonide, based on the fact that it is FDA Pregnancy category of B. Cromolyn is also FDA Pregnancy category B, and is considered safe. The disadvantages, however, are frequent administration and lesser efficacy than antihistamines and intranasal corticosteroids. Montelukast is also FDA Pregnancy category B, but some recommend it be used primarily in those with concurrent asthma or in those who have demonstrated a good response prior to pregnancy.1 Ipratropium is FDA Pregnancy category B, despite limited data.44 The decongestants are not considered safe, especially in the first trimester. If nasal congestion is severe enough to warrant consideration for a decongestant, the intranasal route of administration is preferable, due to decreased systemic exposure and the short-term duration of therapy.1
Elderly1,8
Elderly patients can be treated for AR according to the approach for (younger) adults.1,8 However, the elderly may be more sensitive to the sedative and antimuscarinic effects of antihistamines and to the cardiovascular and CNS stimulant effects of decongestants. Also, the aging process can affect the manifestations of AR. Generalized atrophy of nasal tissues can result in more nasal congestion. An increase in cholinergic activity may result in more rhinorrhea.
Patient Encounter, Part 5
After one more year passes, AW returns to your clinic to ask for advice about her father. He has recently moved into town, because he has just retired. He will be living independently. He is 65 years old and has hypertension, and BPH. The daughter (AW) thinks he is taking two medications for his blood pressure, one of which is also partly for his prostate. He has had AR on and off in the past. That is all she knows about his medical history. Since he has moved to town 6 weeks ago, he notices increasing symptoms of AR. His most bothersome symptom right now is a runny nose that is worse than ever before. He bought some OTC diphenhydramine because he ran out of his previous prescription of intranasal triamcinolone. The diphenhydramine has helped some, but incompletely, and it makes him sleepy. She asks for your advice for additional OTC medication until they can get an appointment with a primary care provider for him.
What additional information would you like?
What can you recommend at this time?
Athletes1
The use of certain medications is prohibited during national and international athletic competition. The list of prohibited drugs changes each year, and may not always be consistent among organizations. The most up-to-date information is available from the World Anti-Doping Agency (WADA).45 Additional information may be obtained from the United States Anti-Doping Agency (USADA).46 The USADA website has a “drug reference online” section that is useful.47
Ocular Symptoms 1,24,28
Several products are available for instillation directly into the eyes for those patients with predominant or unresponsive ocular manifestations. They may be appropriate for occasional moderate-severe flares or episodic AR when other modes of therapy are not optimally effective. The combination (antihistamine and mast cell stabilizing) agents may be the most effective, and they have the advantages of rapid onset of action and (usually) only twice daily administration. See Table 62-8 for these products.
Summary of Treatment
Once an agent appropriate for initial therapy is chosen, ongoing management requires repeated checks to ascertain response and freedom from intolerable or adherence limiting side effects. Either “step-up” or “step-down” therapy may be appropriate depending on the individual patient’s response. See Table 62–9 for a summary of the approach to treatment of AR. Table 62–10 attempts to rank the relative effectiveness of the classes of agents for treatment of AR by specific symptoms.
OUTCOME EVALUATION
AR is a common condition that can have a profoundly negative effect on quality of life. It has been trivialized in the past, but is increasingly recognized as a significant health problem. There are several modes of management that can improve patient function.
• Educate patients and their families about the disorder (see Clinical Presentation and Diagnosis).
• Educate patients and their families about allergen avoidance measures (see Table 62–3).
• Assess the patient’s symptom response, tolerance, and adherence at each visit.
• Assess the patient’s administration technique with intranasal products when symptom response or tolerance is not optimal.
Table 62–10 Relative Efficacy (Semiquantitative) by Classes of Agents for Specific Symptoms of AR

Patient Care and Monitoring
1. Determine the patient’s manifestations
What is the most troublesome symptom?
What is the frequency and severity of symptoms?
How do symptoms affect quality of life, work/school performance, and sleep?
What allergen or irritant triggers have been identified?
2. Attempt to rule out complications or comorbid
conditions that preclude self-care (asthma, sinusitis, otitis
media with effusion, and possibly nasal polyposis) and/or
warrant referral to a physician (see Clinical Presentation
and Diagnosis).
3. Determine past attempts at therapy
What has the patient tried previously for these symptoms
(including prescription and all nonprescription [OTC,
herbal, other complementary] forms)?
What was the response to all previous treatments (efficacy and side effects)?
4. Determine other current disorders and treatments
What conditions are medications taken for on a regular basis?
What medications are currently being taken regularly?
5. Assess patient’s understanding of AR and its
management
What does the patient currently do to avoid triggers?
How does/did the patient administer and adhere to current or past treatments?
6. Fill in gaps in patient’s knowledge
Manifestations of AR and its complications
Principles of management (allergen/trigger avoidance, pharmacologic modes, immunotherapy)
Choices for pharmacologic therapy (OTC and
prescription) and determinates (previous experience, ease
of use, tolerability, cost, patient preference, and age)
Discuss realistic goals, which may not be complete elimination of all symptoms
7. Establish a plan appropriate for and with input from the patient
Recommend initial OTC regimen or refer for evaluation for need for prescription therapy
Fill in gaps in patient’s knowledge about allergen avoidance and optimal adherence and administration
technique (where applicable)
8. Reevaluate the patient at appropriate intervals, that
will vary with the individual, but will usually be every
1 to 3 months
Evaluate for efficacy of therapy, including improvement in
symptoms, quality of life, work/school performance
and sleep pattern
Evaluate for tolerance of side effects
Modify the plan as needed (to increase efficacy or modify side effects) including recommendations for a change in medication and/or referral to a physician
• Use or recommend second-generation oral antihistamine therapy for most patients with mild or intermittent (especially seasonal) symptoms (see Clinical Presentation and Diagnosis and Table 62–9).
• Recommend intranasal corticosteroid therapy for moderate–severe or persistent (especially perennial) symptoms. Advise additional adjunctive therapy for those with less than optimal control (see Clinical Presentation and Diagnosis and Table 62–9).
• Consider step-up therapy for exacerbations or less than optimal response.
• Consider step-down therapy if symptoms have been minimal or stable for several months (especially if the disorder is primarily seasonal).
• Consider referral to rule out nonallergic causes of rhinitis in nonresponding patients or those with an atypical presentation (see Clinical Presentation and Diagnosis).
• Consider referral for patients who request immunotherapy.
• Consider referral for patients with comorbid conditions, especially asthma.
Abbreviations Introduced in This Chapter


 Self-assessment questions and answers are available at http://www.mhpharmacotherapy.com/pp.html.
Self-assessment questions and answers are available at http://www.mhpharmacotherapy.com/pp.html.
REFERENCES
1. Wallace DV, Dykewicz MS, Bernstein DI, et al. The diagnosis and management of rhinitis: An updated practice parameter. J Allergy Clin Immunol 2008;122(2):S1–S84. [US AAAAI/ACAAAI].
2. Bousquet J, Khaltaev N, Cruzz AA, et al. Allergic rhinitis and its impact on asthma (ARIA) 2008 update. Allergy 2008;63(Suppl 86):S8–S160.
3. Scadding GK, Durham SR, Mirakian R, et al. BSACI guidelines for the management of allergic and nonallergic rhinitis. Clin Exp Allergy 2008;38:19–42.
4. Nathan RA. The burden of allergic rhinitis. Allergy Asthma Proc 2007;28(1):3–9.
5. Broide DH. The pathophysiology of allergic rhinoconjunctivitis. Allergy Asthma Proc 2007;28(4):398–403.
6. Blaiss MS. Allergic rhinoconjunctivitis: Burden of disease. Allergy Asthma Proc 2007;28:393–397.
7. Fletcher RH. An overview of rhinitis. In: Rose BD, ed. UpToDate. Waltham, MA: UpToDate, 2008.
8. Hur SY. Allergic rhinitis. The Rx Consultant 2007;16(3):1–8.
9. Carr W W. Pediatric allergic rhinitis: Current and future state of the art. Allergy Asthma Proc 2008;29(1):14–23.
10. de Bittner MR, Sulli MM, Williams DM. The role of nonprescription antihistamines in the treatment of allergic rhinitis [continuing education monograph on the Internet]. Washington, DC: American Pharmacists Association, 2008.
11. Rosenwasser L. New insights into the pathophysiology of allergic rhinitis. Allergy Asthma Proc 2007;28(1):10–15.
12. deShazo RD, Kemp SF. Pathogenesis of allergic rhinitis (rhinosinusitis). In: Rose BD, ed. UpToDate. Waltham, MA: UpToDate, 2008.
13. deShazo RD, Kemp SF. Management of allergic rhinitis. In: Rose BD, ed. UpToDate. Waltham, MA: UpToDate, 2008.
14. Calderon MA, Alves B, Jacobson M, et al. Allergen injection immunotherapy for seasonal allergic rhinitis [review]. Cochrane Database Syst Rev 2007;Issue 1. Art. No.: CD001936. DOI: 10.1002/14651858.CD001936.pub2.
15. Cox LS, Linnemann DL, Nolte H, et al. Sublingual immunotherapy: A comprehensive review. J Allergy Clin Immunol 2006;117:1021–1035.
16. Pajno GB. Sublingual immunotherapy: The optimism and the issues. J Allergy Clin Immunol 2007;119:796–801.
17. Wilson DR, Torres Lima M, Durham SR. Sublingual immunotherapy for allergic rhinitis [review]. Cochrane Database of Systematic Reviews. 2003, Issue 2. Art. No.: CD002893. DOI: 10.1002/14651858.CD002893.
18. Leatherman BD, Owen S, Parker M, et al. Sublingual immunotherapy: Past, present, paradigm for the future? Otolaryngol Head Neck Surg 2007;136:S1–S20.
19. Carr WW, Nelson MR, Hadley JA. Managing rhinitis: Strategies for improved patient outcomes. Allergy Asthma Proc 2008;29(4):349–357.
20. Lanier B. Allergic rhinitis: Selective comparisons of the pharmaceutical options for management. Allergy Asthma Proc 2007;28(1):16–19.
21. Krouse JH. Allergic rhinitis—Current pharmacotherapy. Otolaryngol Clin North Am 2008;41:347–358.
22. Marple BF, Fornadley JA, Patel AA, et al. Keys to successful management of patients with allergic rhinitis: Focus on patient confidence, compliance, and satisfaction. Otolaryngol Head Neck Surg 2007;136:S107–S124.
23. Plaut M, Valentine MD. Allergic rhinitis. N Engl J Med 2005; 353(18):1934–1944.
24. Drugs for allergic disorders. Treat Guidel Med Lett 2007;5(60):71–80.
25. Drugs@FDA. U.S. Food and Drug Administration. Center for Drug Evaluation and Research. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/.
26. Fluticasone furoate (Veramyst) for allergic rhinitis. Med Lett Drugs Ther 2007;49(1273):90–92.
27. Olopatadine (Patanase) nasal spray for allergic rhinitis. Med Lett Drugs Ther 2007;50(1289):51.
28. Lacy CF, Armstrong L, Goldman MP, et al., eds. Drug Information Handbook 2008–2009. 17th ed. Hudson, OH: LexiComp, 2008.
29. Kirtsreesakul V, Chansaksung P, Ruttanaphol S. Dose-related effect of intranasal corticosteroids on treatment outcome of persistent allergic rhinitis. Otolaryngol Head Neck Surg 2008;139(4):565–569.
30. Aranoff GR, Bennett WM, Berns JS, et al. Drug Prescribing in Renal Failure—Dosing Guidelines for Adults and Children, 5th ed. Philadelphia, PA: American College of Physicians, 2007.
31. American Pharmacists Association (APhA). DEA interim final regulation: Ephedrine, pseudoephedrine, and phenylpropanolamine requirements. September 2006, http://www.pswi.org/government/Pseudoephedrine093006.pdf.
32. U.S. Department of Justice. Drug Enforcement Administration. Office of Diversion Control. Combat Methamphetamine Epidemic Act 2005 (Title VII of Public Law 109–177). http://www.deadiversion.usdoj.gov/meth/index.html.
33. Kollar C, Schneider H, Waksman J, et al. Meta-analysis of the efficacy of a single dose of phenylephrine 10 mg compared with placebo in adults with acute nasal congestion due to the common cold. Clin Therap 2007;29(6):1057–1070.
34. Hendeles L, Hatton RC. Oral phenylephrine: An ineffective replacement for pseudoephedrine? J Allergy Clin Immunol 2006;118(1):279–280.
35. Hatton RC, Winterstein AG, McKelvey RP, et al. Efficacy and safety of oral phenylephrine: Systematic review and meta-analysis. Ann Pharmacother 2007;41:381–390.
36. Barnes ML, Biallosterski BT, Gray RD, et al. Decongestant effects of nasal xylometazoline and mometasone furoate in persistent allergic rhinitis. Rhinology 2005;43(4):291–295.
37. Lockey RF. Rhinitis medicamentosa and the stuffy nose. J Allergy Clin Immunol 2006;118:1017–1018.
38. Greiner AN, Meltzer EO. Pharmacologic rationale for treating allergic and nonallergic rhinitis. J Allergy Clin Immunol 2006;118:985–996.
39. U.S. Food and Drug Administration. Center for Drug Evaluation and Research. Early communication about an ongoing safety review of montelukast (Singulair). http://www.fda.gov/cder/drug/early_comm/montelukast.htm.
40. Rabago D. The use of saline nasal irrigation in common upper respiratory conditions. [continuing education monograph on the Internet]. US Pharmacist. 2008, http://www.uspharmacist.com/oldformat.asp?url=ce/105757/default.htm.
41. AAAAI Rhinosinusitis Committee. Saline sinus rinse recipe. American Association of Allergy Asthma & Immunology. http://www.aaaai.org/patients/publicedmat/sinusitis/rinse_recipe.pdf.
42. Passalacqua G, Bousquet PJ, Kai-Hakon C, et al. ARIA update: I-systematic review of complementary and alternative medicine for rhinitis and asthma. J Allergy Clin Immunol 2006;117:1054–1062.
43. Food and Drug Administration. FDA statement. FDA statement following CHPA’s announcement on nonprescription over-the-counter cough and cold medicines in children. http://www.fda.gov/bbs/topics/NEWS/2008/NEW01899.html.
44. Briggs GG, Freeman RK, Yaffe SJ. Drugs in Pregnancy and Lactation., 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2008.
45. World Anti-Doping Agency (WADA) [homepage on the Internet]. Montreal, Quebec. http://www.wada-ama.org/.
46. U.S. Anti-Doping Agency (USADA) [homepage on the Internet]. Colorado Springs. http://www.usantidoping.org/.
47. U.S. Anti-Doping Agency (USADA) [homepage on the Internet]. Colorado Springs. Drug Reference Online™ (DRO). http://www.usantidoping.org/dro/.