Karel Everaert1 , An-Sofie Goessaert1 and Marie-Astrid Denys1
(1)
Nopia Research Group, Department of Urology, Ghent University Hospital, Ghent, Belgium
Karel Everaert
Email: karel.everaert@ugent.be
What Do the Guidelines Say?
Current guidelines and recommendations for the diagnosis and treatment of nocturia are included in the guidelines for male lower urinary tract symptoms and benign prostate obstruction, urinary incontinence, overactive bladder, and neurogenic bladder dysfunction. Despite the recognition of the multifactorial etiology, bothersome nocturia is often considered as a symptom associated with other diseases, and not as a distinct condition that requires an individualized treatment. The development of specific guidelines on the management of nocturia is scheduled by the European Association of Urology (EAU).
Clinical Practice
The general perception among caregivers and patients is that nocturia is not harmful, little bothersome, and part of the normal aging process. Guidelines for general practitioners confirm this assumption. Consequently, patients do not complain of nocturia, and caregivers do not see the need to evaluate the symptoms or to find the underlying cause. Furthermore, desmopressin is the only evidence-based pharmacological treatment that is indicated for nocturia. The potentially fatal side effects, if the required precautions are not taken into account, make caregivers reluctant to prescribe this and, consequently, any medication to treat nocturia.
Background
Definition
The ICS (International Continence Society) defines nocturia as the complaint that an individual has to wake at night one or more times to void, with each void preceded and followed by sleep. Getting up once at night is considered as little bothersome, while two nocturia episodes are reported as moderately bothersome, with increasing bother as the number of nocturnal voids increases.
Epidemiology
The prevalence of nocturia increases with age and is similar in both genders. Over one-third of young people (<40 years) report at least one void per night, and even 15 % have to wake up twice or more to void at night. In older persons (>65 years) the prevalence increases to 70–90 % for one nocturia episode, and 30–60 % report at least 2 voids per night.
Intraindividual fluctuations in prevalence, spontaneous resolution, and correlations with body mass index (BMI >25 in women, BMI >30 in men) and drinking habits have been described.
Causes
Nocturia is the result of disturbances in the circadian rhythms of the kidney, bladder, and sleep pattern, which can lead to nocturnal polyuria, 24 h polyuria, reduced functional bladder capacity, and/or sleep disorders.
Nocturnal Polyuria (NP)
Nocturnal polyuria, or the production of an abnormally large volume of urine during sleep, is present in 60–80 % of patients. It is the most important cause of nocturia and commonly defined as a nocturnal diuresis greater than 33 % of 24 h diuresis (NP33 definition), as long as the 24 h urine production is within normal ranges. However, many other definitions are used to define NP:
· Ratio of nocturnal diuresis to 24 h diuresis:
· Nocturnal diuresis/24 h diuresis >20 % in younger adults (ICS definition)
· Nocturnal diuresis/24 h diuresis >33 % in older adults (ICS definition)
· Nocturnal diuresis/24 h diuresis >35 %
· Cutoff values for nocturnal diuresis:
· Nocturnal urine production >0.9 ml/min
· Nocturnal urine production >1.3 ml/min
· Nocturnal urine production >1.5 ml/min (= 90 ml/h)
· Ratio of nocturnal diuresis to body weight:
· Nocturnal urine volume >6.4 ml/kg
· Nocturnal urine volume >10 ml/kg
There are many causes of NP that should be considered when carrying out further investigations (see section “Pathophysiology”).
24 h Polyuria
Patients with a 24 h diuresis exceeding 40 ml/kg body weight suffer from 24 h polyuria. The main causes of 24 h polyuria are diabetes mellitus, diabetes insipidus, or polydipsia. The latter can be primary when the excessive fluid intake is because of cultural, social, or psychological reasons or secondary when the body has to compensate for circulatory collapse.
Reduced Functional Bladder Capacity (RFBC)
A reduced functional bladder capacity can be either global or nocturnal. Although there is no strict definition for reduced bladder capacity up till now, it is believed to be present in 30–50 % of nocturia patients. The nocturnal bladder capacity index can be used to define RFBC (see section “Frequency volume chart (FVC)”). It is associated with pathologies of the filling phase of the bladder such as overactive bladder syndrome and/or the emptying phase of the bladder such as lower urinary tract obstruction and bladder hypocontractility. There are also non-urological causes such as pharmacological agents and learned voiding dysfunctions.
Sleep Disorder
Nocturia is one of the primary causes of sleep disturbance. The proportion of adults with nocturia as primary cause of nocturnal awakenings increases with age: 40 % of younger adults (18–44 years) and 77 % of older adults (>65 years). Questionnaires to assess sleep quality show a correlation between the severity of nocturia and a lower sleep quality. This sleep fragmentation is associated with impaired functioning, quality of life, health, and productivity. Nocturia not only induces sleep disorders, it can also be induced by sleep disorders. The best known sleep disorder that results in nocturia is the obstructive sleep apnea syndrome. Its therapy with continuous positive airway pressure (CPAP) treats the sleep apnea but at the same time also reduces the amount of nocturia episodes.
Pathophysiology
Nocturnal Polyuria (NP)
The rate of urinary output is regulated by complex interactions between urine concentrating and diluting mechanisms. This can only be achieved with an intact cardiovascular, endocrinological, neurological, and renal system. When evaluating disorders in diuresis, it is important to dissociate water diuresis from osmotic diuresis because they are regulated by totally different mechanisms. Water diuresis is the excretion of water without osmoles (free water), while osmotic diuresis is the excretion of osmoles (e.g., sodium, urea, glucose) together with water. An increase in (nocturnal) urine production can originate from abnormalities in glomerular filtration, osmotic diuresis, and water diuresis (Fig. 15.1).
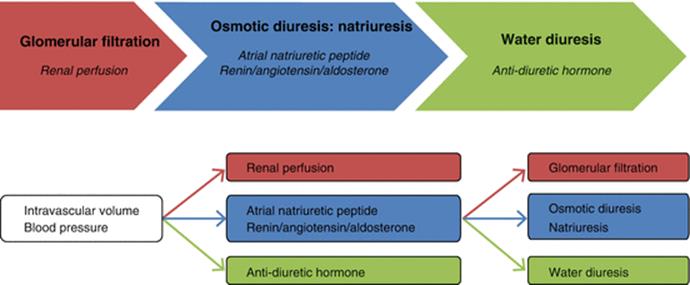
Fig. 15.1
Pathophysiology of nocturnal polyuria
Glomerular Filtration
The glomerulus receives its blood supply from an afferent arteriole of the renal circulation and drains into an efferent arteriole. The resistance of these arterioles is autoregulated and determines the fraction of blood plasma that is filtered through the glomerular capillaries into the Bowman’s capsule, which empties the filtrate into the proximal tubule.
An increase in intravascular volume and blood pressure (e.g., in patients with cardiac failure, hypertension, obesity, reabsorption of peripheral edema, polydipsia) can lead to an increase in glomerular filtration, which also affects osmotic and water diuresis.
In healthy controls, there is a circadian rhythm with a decrease (15–30 %) in glomerular filtration during the night. A subgroup of patients with NP shows an increase in nighttime glomerular filtration. This is called glomerular hyperfiltration.
Osmotic Diuresis
Endocrinological, neurological, renal, and cardiovascular stimuli are responsible for the reabsorption of the majority (95–99 %) of the filtered osmoles together with water. This process mainly takes place in the proximal tubule but also in the loop of Henlé and the distal tubule of the kidney. Natriuresis is the most important type of osmotic diuresis in the pathophysiology of NP. It is regulated by salt dietary intake and several hormones, including the atrial natriuretic peptide (ANP) and the renin-angiotensin-aldosterone system (RAAS). Other types of osmotic diuresis are glucosuria in patients with diabetes mellitus and excretion of urea due to a high-protein diet or hepatic diseases.
An increase in intravascular volume and blood pressure (e.g., in patients with cardiac failure, hypertension, obesity, reabsorption of peripheral edema, polydipsia) not only stimulates glomerular filtration but also rises the secretion of ANP and inhibits the RAAS, both leading to an increase in natriuresis.
In healthy controls, there is a circadian rhythm with a decrease in nocturnal natriuresis. Some patients with NP, especially older persons, have an absent or even inversed circadian rhythm in natriuresis.
Water Diuresis
In order to decrease water excretion and increase urine osmolality, different endocrinological, neurological, renal, and cardiovascular stimuli are responsible for the reabsorption of free water in the collecting duct of the kidney.
The most important regulator is the antidiuretic hormone (ADH), vasopressin. In response to hyposmolality or an increase in intravascular volume and blood pressure (e.g., in patients with cardiac failure, hypertension, obesity, reabsorption of peripheral edema, polydipsia), the secretion of ADH is inhibited and water diuresis is stimulated.
In healthy controls, there is a circadian rhythm with an increase in ADH during the night, leading to a decrease in water diuresis. A subgroup of patients with NP lacks this circadian rhythm and shows an increased nocturnal water diuresis.
24 h Polyuria
In 24 h polyuria the same mechanisms as in NP play a role. However, in this case, a disturbance in circadian rhythm does not only occur at night but also during daytime.
· Glomerular hyperfiltration as underlying mechanism for 24 h polyuria can occur due to polydipsia or cardiac failure. For a detailed description, see section “Glomerular filtration”.
· Osmotic diuresis in 24 h polyuria is usually caused by glucosuria. Normally all glucose is reabsorbed by the kidneys; however, in untreated or poorly treated diabetes mellitus, the elevated blood glucose levels result in excretion of glucose in urine which leads to excessive water loss.
· Diabetes insipidus is characterized by increased water diuresis over 24 h, regardless of fluid intake. Central diabetes insipidus is caused by a deficiency of ADH, whereas nephrogenic diabetes insipidus is caused by an insensitivity of the kidneys to ADH.
Reduced Functional Bladder Capacity
The pathophysiology of an RFBC depends on the cause. Overactive bladder syndrome is caused by disturbances in the nerves, smooth muscle, and urothelium. Prostate enlargement and bladder, prostate, or urethral cancer resulting in lower urinary tract obstruction can lead to bladder decompensation with increased mass, decreased compliance, and cholinergic denervation. As bladder contractions occur in a response to cholinergic stimuli, any cholinergic medication, for example, beta-blockers and cholinesterase inhibitors, can increase voiding frequency and reduce bladder capacity.
Sleep Disorders
The pathophysiological mechanism of sleep apnea leading to nocturia is based on the hypoxemia due to airway obstruction stimulating ANP release, leading to natriuresis and nocturnal polyuria.
Impact
Nocturia is a major cause of sleep fragmentation and associated with a reduction in quality of life, impairment of daily activities and productivity at work, additional comorbidities (falls, traffic accidents, cardiovascular diseases, metabolic syndrome), and mortality. Although many experts consider nocturia to be clinically significant only when patients void at least twice during the night, the need to get up once to void is often related to disruption of the deep sleep (slow wave sleep) within the first 3 h of sleep, which is considered to have the most impact on quality of life. The first hours of undisturbed sleep are the best parameter to evaluate the impact of Nocturia.
Diagnostic Evaluation
A complete diagnostic evaluation is invaluable to initiate an adapted and individualized treatment. All patients with bothersome nocturia need to complete a frequency volume chart and a questionnaire on sleep quality and lower urinary tract symptoms to diagnose the underlying cause(s) of nocturia: NP, 24 h polyuria, RFBC, and sleep disorders. Patients with NP or 24 h polyuria should have an additional evaluation with a renal function profile to evaluate abnormalities in glomerular filtration, osmotic diuresis, and water diuresis.
Frequency Volume Chart (FVC)
Patients have to record voided volumes, volume and type of fluid intake, and the time of going to bed and getting up in the morning during 3 days. In case of urinary incontinence, the frequency of urinary leaks has to be reported together with (an indication of) the quantity and the circumstances (e.g., coughing, sneezing, handwashing) (Fig. 15.2).
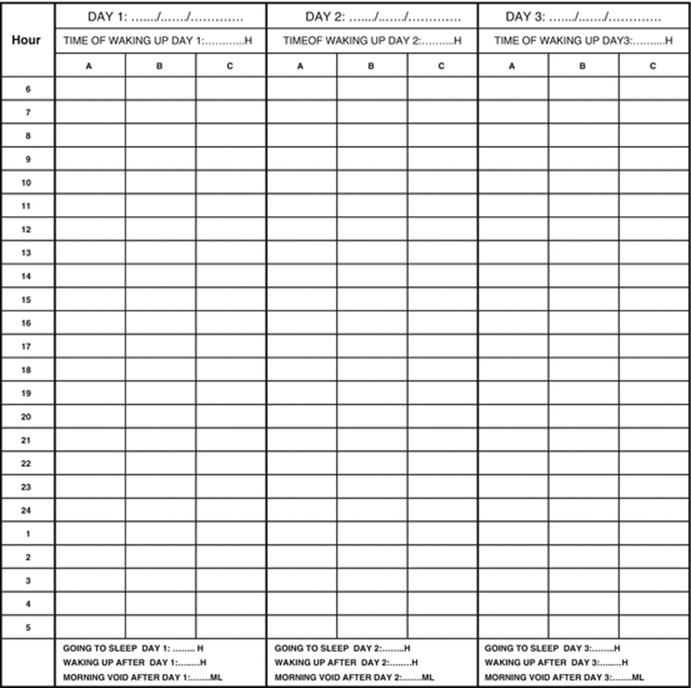
Fig. 15.2
Frequency volume chart. Column A: Write down the voided volumes of each micturition during 3 × 24 h (in ml). Do not forget to note the volume of the first morning void of the next day, the time of going to bed with the intention to sleep and the time of waking up in the morning. Column B: Measure the involuntary urine loss: weight of wet diaper – weight of dry diaper. If that is not possible, give an indication of the estimated urine loss: N1 = some drops of urine; N2 = leakage that requires a new diaper. Describe the situation of the urine leakage (e.g. during coughing, laughing, following urgency, etc.). Column C: Note the amount (in ml) and type of fluid intake (e.g. water, alcohol, coffee, soft drinks, etc.)
A lot of information can be deducted from an FVC (Table 15.1). When considering calculations with volumes, the first morning void of day 1 is excluded but the first morning void of day 2 is included. When considering calculation with frequencies, the first morning void of day 1 is included and the first morning void of day 2 is excluded.
Table 15.1
Information deducted from an FVC
|
Unit |
|
|
Diurnal voiding frequency Daytime voiding frequency Nighttime voiding frequency |
Number |
|
Diurnal urine production Nocturnal urine production (NUP) |
ml |
|
Diurnal diuresis rate Nocturnal diuresis rate |
ml/min |
|
Functional bladder capacity (FBC) = maximal voided volume in 24 h Mean FBC daytime = mean of voided volumes during daytime Mean FBC nighttime = mean of voided volumes during nighttime |
ml |
|
Mean hours of sleep |
h |
|
Diurnal fluid intake |
ml |
|
Frequency of diurnal incontinence episodes Frequency of nocturnal incontinence episodes |
Number |
|
Mean volume of incontinence |
g |
|
Nocturia index (NI) = NUP/FBC → Nocturia if >1 |
/ |
|
NP33 definition: NP index (NPi) = NUP/24 h diuresis → NP if >33 % |
% |
|
NUP90 definition = NUP/h of sleep → NP if >90 ml/h |
ml/h |
|
Nocturnal bladder capacity index (NBCI) = actual – predicted number of voids (= NI-1) → RFBC if >1.3 |
/ |
Nocturnal Polyuria
Various definitions for NP can be used when analyzing an FVC (e.g., NPi33 or NUP90). In order to adapt treatment according to the underlying cause, we suggest to perform a renal function in all patients with NP.
24 h Polyuria
In patients with a 24 h diuresis exceeding 40 ml/kg body weight, the most common disorders should be considered by evaluating:
· Fluid intake (polydipsia)
· Glucose or HbA1c and osmotic diuresis on RFP (diabetes mellitus)
· Water diuresis on RFP (diabetes insipidus)
Further diagnosis and treatment have to be organized by an internal medicine practitioner.
Reduced Functional Bladder Capacity
Because there are no cutoff values for a normal bladder capacity, the diagnosis of an RFBC is based on the NBCI (Table 15.1). Further urological investigation with uroflowmetry, ultrasonography, and urodynamics is recommended to explore the cause of the RFBC (e.g., outlet obstruction, hypocontractility of the bladder, overactive bladder syndrome).
Questionnaires on Sleep Quality
The Pittsburgh Sleep Quality Index (PSQI) contains 19 self-rated questions used to measure sleep quality over the past month in the following 7 domains: (1) subjective sleep quality, (2) sleep latency, (3) sleep duration, (4) habitual sleep efficiency, (5) sleep disturbances, (6) use of sleeping medication, and (7) daytime dysfunction (Addendum 1). The 19 items are combined to form 7 component scores, each of which are scaled from 0 (no difficulty) to 3 (severe difficulty). The sum of scores yields a global score which ranges from 0 to 21, with scores above 5 reflecting poor global sleep quality. A polysomnography is recommended when a sleep disorder (e.g., obstructive sleep apnea syndrome) is suspected.
Renal Function Profile (RFP)
A renal function profile is a 24 h test based on the collection of a urine sample every 3 h to analyze diuresis rate, osmolality, and sodium, urea, glucose, and creatinine concentrations (Table 15.2). The voided volume at the time of sample collection has to be registered, as well as volumes of any interim micturition. This test starts in the morning with the first sample 3 h after the first morning micturition. Urinary sample U1 is collected between 9 and 11 am, U2 between 12 and 2 pm, U3 between 3 and 5 pm, U4 between 6 and 8 pm, U5 between 9 and 11 pm, U6 between 12 and 2 am, U7 between 3 and 5 am, and U8 between 6 and 8 am. A blood sample is taken to determine plasma osmolality, sodium, urea, glucose, and creatinine.
Table 15.2
Renal function profile
|
Start |
8 urine collections: 1 collection every 3 h |
|||||||
|
Micturition |
U1 |
U2 |
U3 |
U4 |
U5 |
U6 |
U7 |
U8 |
|
6–8 h |
9–11 h |
12–14 h |
15–17 h |
18–20 h |
21–23 h |
00–2 h |
3–5 h |
6–8 h |
The RFP makes it possible to identify the pathophysiological mechanism(s) of NP. Since there are no cutoff values yet, circadian rhythms are analyzed by comparing the individual values of the 8 urine samples or by comparing the mean daytime and nighttime results.
Glomerular Filtration
The rate at which blood is filtered through all of the glomeruli, and thus a measure of the overall renal function, is the glomerular filtration rate (GFR). This is calculated by using the creatinine clearance, creatinine concentration in the urine sample (UCr), voided volume of the urine sample (V), and plasma concentration of creatinine (P Cr):
![]()
An episode of glomerular hyperfiltration during the night can cause NP.
Osmotic Diuresis
Osmotic diuresis can be evaluated by comparing total osmotic clearance or individual clearance of sodium, urea, etc. When there is no blood sample available, comparing urinary excretion also provides valuable information.
Clearance
The clearance of an osmole is the volume of plasma cleared of osmotically active particles per unit time. The overall osmolar clearance is calculated by using the concentration of osmolality in the urine sample (Uosm), voided volume of the urine sample (V), and plasma osmolality (Posm):
![]()
The clearance of an osmole X is calculated by using the concentration of X in the urine sample (Ux), voided volume of the urine sample (V), and plasma concentration of X (P x):
![]()
Urinary excretion
As there is a higher rate of osmolar excretion with higher voided volume, all calculations are corrected with the creatinine concentration in the urine sample (UCr):
![]()
U osm = concentration of osmolality in the urine sample
![]()
U x = concentration of X in the urine sample
Mainly nocturnal increases in natriuresis cause NP, but also disturbances in urea and glucose excretion can contribute to the development of NP.
Water Diuresis
Water diuresis can be evaluated by comparing free water clearance. When there is no blood sample available, comparing urinary osmolality also provides valuable information.
Clearance
The free water clearance is the difference between the voided volume of the urine sample (V) and the osmolar clearance. It is the volume of free water subtracted from (positive free water clearance) or added to (negative free water clearance) the plasma per unit time:
![]()
Urinary excretion
Urinary osmolality (Uosm) is a parameter to measure urine concentration. It can range from 50 to 1400 mosm/kg, but the mean 24 h osmolality should be 500–800 mosm/kg. A large value indicates concentrated urine; small values indicate diluted urine.
Smaller values due to a reduced effect of ADH and therefore a higher free water excretion or water diuresis can be observed in patients with NP. Patients with 24 h polyuria and a low 24 h osmolality should be referred to an internal medicine practitioner to exclude diabetes insipidus.
Management
Managing nocturia needs to be based on an approach that targets the underlying cause(s) and takes into account the individual bother (Fig. 15.3). Notice that only desmopressin has a level of evidence (LE) of 1 for the treatment of nocturia.
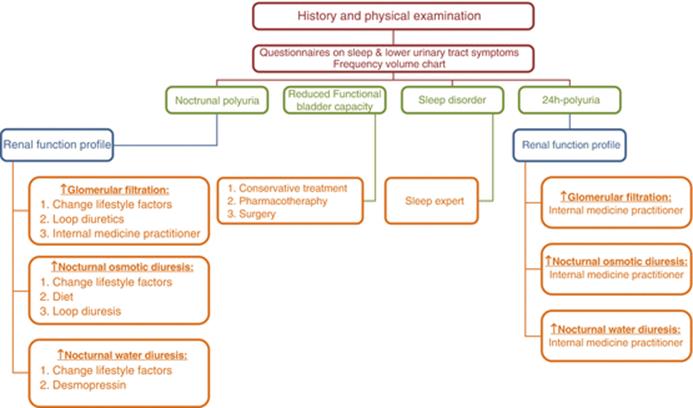
Fig. 15.3
Nocturia assessment. It targets the underlying causes as well as the individual bother
Nocturnal Polyuria
General measures to change lifestyle factors have to be considered in all patients with NP:
· Limit the daily fluid intake to 1.5–2 l.
· Restrict fluid intake in the evening, especially caffeine and alcohol intake.
· Take afternoon naps and elevate the legs to prevent fluid accumulation.
· Wear compression stockings to prevent fluid accumulation.
· Perform positional changes before going to bed.
Glomerular Filtration
Reducing glomerular filtration can be obtained by treating the underlying cause (e.g., hypertension, cardiovascular diseases) by an internal medicine practitioner.
Intake of short-acting loop diuretics (e.g., furosemide) 5–6 h before going to bed can stimulate diuresis during the day instead of the night. A decrease in nocturnal voiding frequency is demonstrated in older men with lower urinary tract symptoms. It can safely be combined with desmopressin and alpha-blocker. Always be aware of adverse effects such as postural hypotension, fluctuations of glycemia, and electrolyte disturbances. Especially in older persons, the levels of creatinine, sodium, chloride, potassium, magnesium, and calcium should be checked at baseline, after 3 days and after 7 days of treatment, and after every change in dosage.
Osmotic Diuresis
Salt (or protein) restriction might be a treatment option in patients with an increased nocturnal natriuresis (or urea excretion), but it has not yet been evaluated in patients with NP. A study in patients with nephrogenic diabetes insipidus showed a reduction in urine output of 20–50 % after the combination of salt restriction and intake of hydrochlorothiazide/amiloride or hydrochlorothiazide/indomethacin (LE 3).
Administration of short-acting loop diuretics (e.g., furosemide) 5–6 h before going to bed in order to stimulate diuresis during the day instead of the night is also a treatment to consider (see section “Glomerular filtration”).
Water Diuresis
Desmopressin (solid tablet, 0.2–0.4 mg, or orally disintegrating tablet, 60–240 μg) is a synthetic analogue of the endogenous ADH and currently the only proven pharmaceutical treatment for nocturia caused by NP (LE 1). A better efficacy and safety profile is found in women with an even lower dose of 25 mg ODT. It lowers the nocturnal urine production and improves sleep quality by prolonging the initial sleep period of patients. The beneficial effects have been confirmed on short and long term. Patients have to take it 1 h before going to bed and must not drink 1 h before until 8 h after the intake in order to avoid water intoxication. Adverse effects (e.g., headache, abdominal pain, nausea) are limited. However, there is a risk for potentially fatal hyponatremia, especially in women and individuals older than 65 years. Therefore, the levels of sodium and creatinine need to be checked before initiating the treatment:
· Sodium <135 mmol/l: do not start desmopressin.
· Sodium >135 mmol/l: start with the lowest dose of desmopressin.
· Check sodium levels after 3 days, 7 days, 30 days, and 6 months.
· Check sodium levels after changing the dose.
· Check sodium levels after intake of other medications that can affect sodium levels (e.g., diuretics, antidepressants, antipsychotics, anticonvulsants).
Starting this treatment in patients older than 65 years requires a hospitalization to monitor adverse effects and electrolyte disorders. Polypharmacy is a major problem in this population, and concomitant use of medications that lower sodium levels increases the risk for adverse events.
24 h Polyuria
For this cause of nocturia, the patient has to be treated by an internal medicine practitioner.
Reduced Functional Bladder Capacity
Treatment of an RFBC depends on the underlying cause. It may consist of conservative measures such as bladder training or timed voiding. Pharmacological treatment with anticholinergics, beta-agonists, alpha-blockers, 5-alpha-reductase inhibitors, and phosphodiesterase inhibitors (tadalafil) has been tested in selected populations (LE 2). Surgery is required for specific pathologies (e.g., transurethral resection of the prostate, sacral neuromodulation).
Sleep Disorder
For this cause of nocturia, the patient has to be treated by a sleep expert.
Combining Therapy
A combination of treatments is recommended if there are multiple causes for nocturia.
Points of Interest
· The use of an FVC is mandatory to evaluate the cause of nocturia. It provides a direction for further diagnostic investigations and management of nocturia. Nevertheless, only ¼ of GPs and ½ of urologists use an FVC to evaluate patients with nocturia. Increasing the awareness and stimulating education is imperative.
· The use of an RFP is useful to diagnose the underlying cause of NP and 24 h polyuria and can direct us toward the optimal treatment. Future research is required to prove this.
· A better knowledge of desmopressin will decrease the resistance and fear to use this medication. For example, a better knowledge of safety estimation using age, gender, and baseline sodium levels is important. To increase safety, prescribers also have to be aware of other medications that can cause hyponatremia when initiating desmopressin.
· Trials to prove the efficacy and safety of combined treatment are needed in the future.
Addendum 1: Pittsburgh Sleep Quality Index (PSQI)
Instructions
The following questions relate to your usual sleep habits during the past month only. Your answers should indicate the most accurate reply for the majority of days and nights in the past month.
During the past month:
1.
2.
3.
4.
|
5. During the past month, how often have you had trouble sleeping because you: |
Not during the past month (0) |
Less than once a week (1) |
Once or twice a week (2) |
Three or more times a week (3) |
|
(a) Cannot get to sleep within 30 min |
||||
|
(b) Wake up in the middle of the night or early morning |
||||
|
(c) Have to get up to use the bathroom |
||||
|
(d) Cannot breathe comfortably |
||||
|
(e) Cough or snore loudly |
||||
|
(f) Feel too cold |
||||
|
(g) Feel too hot |
||||
|
(h) Have bad dreams |
||||
|
(i) Have pain |
||||
|
(j) Other reasons (please describe, including how often you have had trouble sleeping because of this reason(s): ..……………………) |
||||
|
6. During the past month, how often have you taken medicine (prescribed or over the counter) to help you sleep? |
||||
|
7. During the past month, how often have you had trouble staying awake while driving, eating meals, or engaging in social activity? |
||||
|
8. During the past month, how much of a problem has it been for you to keep up enthusiasm to get things done? |
||||
|
Very good (0) |
Fairly good (1) |
Fairly bad (2) |
Very bad (3) |
|
|
9. During the past month, how would you rate your sleep quality overall? |
Scoring
|
Scoring system |
Score |
|
|
1. Subjective sleep quality |
#9 score |
0–3 |
|
2. Sleep latency |
#5a score + #2 score (15 min = 0; 16–30 min = 1; 31–60 min = 2; >60 min = 3) → if sum is equal 0 = 0; 1–2 = 1; 3–4 = 2; 5–6 = 3 |
0–3 |
|
3. Sleep duration |
#4 score → >7 = 0; 6–7 = 1; 5–6 = 2; <5 = 3 |
0–3 |
|
4. Habitual sleep efficiency |
(Total # of hours asleep)/(total # of hours in bed) × 100 → 85 % = 0; 75–84 % = 1; 65–74 % = 2; <65 % = 3 |
0–3 |
|
5. Sleep disturbances |
Sum of scores #5b to #5j → if sum is equal 0 = 0; 1–9 = 1; 10–18 = 2; 19–27 = 3 |
0–3 |
|
6. Use of sleeping medication |
#6 score |
0–3 |
|
7. Daytime dysfunction |
#7 score + #8 score → if sum is equal 0 = 0; 1–2 = 1; 3–4 = 2; 5–6 = 3 |
0–3 |
|
Global score |
Add the 7 component scores together |
0–21 |
Further Reading
Bosch JL, Weiss JP. The prevalence and causes of nocturia. J Urol. 2013;189(1 Suppl):S86–92.
Goessaert AS, Krott L, Hoebeke P, Vande Walle J, Everaert K. Diagnosing the pathophysiologic mechanisms of nocturnal polyuria. Eur Urol. 2015;67(2):283–8.CrossRefPubMed
Hofmeester I, Kollen BJ, Steffens MG, Bosch JL, Drake MJ, Weiss JP, et al. The association between nocturia and nocturnal polyuria in clinical and epidemiological studies: a systematic review and meta-analyses. J Urol. 2014;191(4):1028–33.
Norgaard JP, Hashim H, Malmberg L, Robinson D. Antidiuresis therapy: mechanism of action and clinical implications. Neurourol Urodyn. 2007;26(7):1008–13.
Schmid SM, Hallschmid M, Schultes B. The metabolic burden of sleep loss. Lancet Diabet Endocrinol. 2015;3(1):52–62.