Christian Nayar, Vinay Kalsi, Rizwan Hamid, Julian Shah and Tina Rashid
Q. A 35-year-old woman is referred to your clinic with problems of urinary frequency, urgency, urgency incontinence and nocturia. How will you approach this patient’s problems?
A. I will review her in my specialist clinic. I would like to elucidate the following points from her history:
When did the symptoms first appear?
Are there any exacerbating factors?
Are there any associated obstructive symptoms or proven urinary tract infections (UTIs)? How many (if any) pads does she have to wear throughout the day, are they damp or soaked through?
How is this problem impacting on her quality of life?
Is there any history of neurological disease?
Is there any history of previous pelvic surgery/pelvic cancer/pelvic radiotherapy?
Is there any relevant smoking history?
Ask for information about fluid intake including caffeinated beverages.
What medications is she taking?
What has she tried in the past to improve the problem, i.e. conservative methods/lifestyle changes/medications?
Q. What initial tests would you perform?
A. I would request the following:
Urine dipstick analysis and urinary culture if appropriate.
Uroflowmetry and post-void bladder scan.
A bladder diary of at least 3 days’ duration.
If suprapubic pain or non-visible haematuria is present then I will organise urine cytology and a flexible cystoscopy.
Note: If an elderly woman presents with these symptoms then I would perform urine cytology and
a flexible cystoscopy initially, in order to exclude bladder pathology, e.g. bladder stone, carcinoma in situ or overt bladder cancer.
Q. What is the difference between a bladder diary and a frequency-volume chart?
A. A bladder diary records the type and volume of fluid intake, incontinence episodes and number of pads used along with a recorded chart of urinary frequency and voided urine volume (i.e. functional bladder capacity). A frequency volume chart records only the volume of fluid intake, urinary frequency and incontinence episodes.
Q. How would you diagnose nocturnal polyuria from a bladder diary?
A. Nocturnal polyuria is present when an increased proportion of the 24-hour output occurs at night (normally during the 8 hours when the patient is in bed). The nighttime urine output excludes the last void before sleep but includes the first void of the morning. The International Continence Society (ICS) standardisation committee defines nocturnal polyuria as nocturnal urine production exceeding 20% of 24-hour urine output in younger adults and 33% in older adults [1].
Q. What do you understand by the term overactive bladder (OAB)?
A. The ICS/International Urogynecological Association (IUGA) defines OAB as a symptom syndrome of urgency with or without incontinence usually accompanied by urinary frequency and nocturia, in the absence of pathological (e.g. UTI, stones, bladder tumour) and metabolic factors (e.g. diabetes).
ICS definitions as related to urinary incontinence are given in Table 11.1.
Table 11.1 Definitions of terminology in overactive bladder and urinary incontinence
|
Overactive bladder syndrome |
A symptom syndrome of urgency with or without incontinence usually accompanied by urinary frequency and nocturia, in the absence of pathological (e.g. UTI, stones, bladder tumour) and metabolic factors (e.g. diabetes). |
|
Urgency |
A sudden and compelling desire to pass urine that cannot be deferred. |
|
Urge urinary incontinence |
Involuntary leakage of urine accompanied by or immediately preceded by urgency. Usually represents a severe form of overactive bladder syndrome. |
|
Stress urinary incontinence |
Involuntary leakage of urine on effort or exertion, or on coughing or sneezing. |
|
Mixed urinary incontinence |
Involuntary leakage of urine associated with urgency and also with exertion, effort, sneezing and coughing. |
|
Increased daytime frequency |
This is the complaint by the patient who considers that he/she voids too often by the day. |
Q. What is the difference between OAB and idiopathic detrusor overactivity (IDO)?
A. OAB is a symptomatic diagnosis while IDO is a urodynamic diagnosis, i.e. urodynamic evidence of detrusor contraction which may be spontaneous or provoked (in the absence of any other pathology OAB is presumed to be the result of IDO).
Q. What is the differential diagnosis for this patient’s symptoms?
A. They can be divided into
Urological
UTI
Detrusor overactivity
Urethral syndrome
Urethral diverticulum
Interstitial cystitis
Bladder cancer
Bladder dysfunction
Gynaecological
Cystocele
Pelvic mass
Genital
Vulvo-vaginitis
Urethritis
Urethral caruncle
Atrophy
Medical
Upper motor neuron
lesion
Diabetes mellitus
General
Excessive fluid/caffeine intake
Anxiety
Pregnancy
Q. What are the treatment options for this patient if she has an OAB?
A. The management of OAB should be initiated in a stepwise manner starting with
Lifestyle changes (eliminate caffeinated drinks, stop smoking, lose weight if obese). Bladder re-training and pelvic floor muscle exercises (both shown to be effective in OAB). Pharmacotherapy (efficacy 50%-75%).
Intravesical injection of botulinum toxin A (efficacy 36%-89%, mean 70%, up to a mean time of 6 months).
Neuromodulation (50% cure, 25% significant improvement of symptoms, 25% failure rate). Clam (augmentation) cystoplasty (50% cure, 25% significant improvement of symptoms, 25% failure rate).
Urinary diversion is an option if all else fails in very severe cases.
Note: The first three options in the previous list may be tried in the absence of urodynamic investigation. However, prior to any invasive procedure, urodynamic confirmation of the diagnosis of detrusor overactivity should be sought.
Q. What do you understand by bladder re-training and pelvic floor muscle training (PFMT)?
A. Bladder re-training works on the idea that the central control can be re-learned as it was learnt in infancy. It is done by setting a target time for using the toilet before which the patient should not void. Once this is achieved the time is increased. The patient has to maintain a normal fluid intake.
PFMT was originally described by Kegel. The purpose is to strengthen and rehabilitate the pelvic floor. The aim is to increase the urethral resistance and improve the tone of the pelvic floor. It is performed by long slow contractions and short sharp pull-ups at regular intervals. Generally several sets consisting of 8-10 contractions of each are performed daily.
Q. What is the efficacy of anticholinergics?
A. It varies between 50% and 75%. They help to reduce urgency and incontinence episodes along with reducing frequency of micturition. The voided volume is also increased.
Q. How do anticholinergics work?
A. Anticholinergics are competitive muscarinic receptor antagonists, they have a high binding affinity for the cholinergic muscarinic receptors that mediate contraction of the urinary bladder (and enhance salivation). The majority of muscarinic receptors expressed in the detrusor muscle are M2, however, M3 are the functionally important ones in the detrusor muscle. Anticholinergics in general have a low affinity for other neurotransmitter receptors and other possible targets like calcium channels. Selective anticholinergics result in selective blockade of M2 or M3 muscarinic receptors, with the particular advantage of not affecting brain Ml receptors, and thus having a better side-effect profile than non-selective agents.
Anticholinergics exert a significant effect on the lower urinary tract by reducing spontaneous detrusor muscle activity during the filling phase, decreasing detrusor pressure (and increasing the residual urine).
Q. Which anticholinergics do you know?
A. See Table 11.2.
Table 11.2 Different anticholinergic drugs and their properties
|
Trade name/generic name |
Dose (mg) |
Frequency |
Receptor subtype selectivity |
Active metabolite |
Elimination half-life of drug (hours) |
|
Pro-Banthine/Propantheline |
15 |
tds |
Non-selective |
No |
<2 |
|
Detrusitol/Tolterodine tartrate |
2 |
bd |
Non-selective |
Yes |
2.4 |
|
Detrusitol XL/Tolterodine tartrate |
4 |
od |
Non-selective |
Yes |
8.4 |
|
Regurin/Trospium chloride |
20 |
bd |
Non-selective |
No |
20 |
|
Ditropan/Oxybutynin chloride |
2.5-5 |
bd-qds |
Non-selective |
Yes |
2.3 |
|
Lyrinel XDOxybutynin chloride XL |
5-30 |
od |
Non-selective |
Yes |
13.2 |
|
Detrunorm/Propiverine hydrochloride |
15 |
od-qds |
Non-selective |
Yes |
4.1 |
|
Emselex/Darifenacin |
7.5-15 |
od |
Selective muscarinic M3 receptor antagonist |
Yes |
3.1 |
|
Vesicare/Solifenacin |
5-10 |
od |
Selective muscarinic M2 and M3 receptor antagonist |
Yes |
40-68 |
Q. What are the side effects of anticholinergics?
A. Common side effects of muscarinic receptor blockade include a dry mouth, dyspepsia, constipation, blurred vision and drowsiness. Serious side effects include anaphylaxis, drowsiness/cognitive and memory impairment particularly in the elderly, dementia and cardiac arrhythmias through prolongation of the QT interval. Selective M3 agents are least likely to cause side effects.
Q. What are the contraindications of anticholinergics?
A. The following conditions are contraindications to the use of anticholinergics:
Myasthenia gravis
Narrow-angle glaucoma, uncontrolled
Significant bladder outflow obstruction or urinary retention
Severe/active ulcerative colitis
Toxic megacolon
Gastrointestinal obstruction or intestinal atony
Hypersensitivity to the agent
Q. Are you aware of any studies linking use of anticholinergics and dementia?
A. The association between anticholinergic drugs and dementia/cognitive impairment has been established for some time, but was thought to be reversible on stopping the drugs. However recent studies have suggested that the problem may NOT be reversible. A study from Seattle looked at data from almost 3500 people all over 65 years who had no signs of dementia on entry to the cohort study (recruitment started over 20 years ago). They then compared anticholinergic use over a 10-year period, adjusting for the degree of anticholinergic burden [2].
For those using anticholinergics regularly there was increased risk of dementia and Alzheimer’s compared with no use.
The risk increase was small: A 1.5-fold increased risk of dementia in those using anticholinergics regularly for 3 years.
The relationship was dose dependent - so the more anticholinergics you use the greater the risk of dementia/Alzheimer’s.
During the 10 years of study, when you took the medication was not important - so the effect is not related to recent use. Having ever taken these drugs is related to the same risk as being on them now.
Importantly though, this is an ASSOCIATION not a causation.
Q. Are there any other medications that could be tried?
A. If anticholinergics are not tolerated, ineffective or contraindicated then mirabegron (a 6-3 adrenergic agonist) may be an option.
Q. How does mirabegron work?
A. Mirabegron activates the 6-3 adrenergic receptor in the detrusor muscle in the bladder, which leads to muscle relaxation and an increase in bladder capacity helping the bladder to fill and store urine. The recommended dose is 50 mg once daily and 25 mg in renal or hepatic impairment.
Q. What are the side effects of mirabegron?
A. Tachycardia and UTI have been reported, less commonly reported are dyspepsia, palpitations, atrial fibrillation, hypertension, joint swelling, rash and pruritus.
Q. What are the contraindications to mirabegron?
A. The main contraindications are
Hypersensitivity to the active ingredient
Severe uncontrolled hypertension defined as systolic BP > 180 and or diastolic BP > 110 mm Hg
Q. What is the next step if medical therapy fails?
A. The next step will be to perform a urodynamic study (also known as cystometrogram [CMG]) as further treatment options involve invasive therapies.
Q. What are the aims of urodynamics studies?
A. Urodynamics has two basic aims:
To reproduce the patient’s symptomatic complaints
To give a pathophysiological explanation by correlating the patients’ symptoms to the urodynamics findings
Q. How will you perform urodynamics also known as cystometrogram (CMG)?
A. This is performed in a dedicated room with specialised urodynamic equipment or in the radiology department where fluoroscopy facilities are available (for videourodynamic studies). The test takes about 40-60 minutes and the aim is to duplicate the patient’s symptoms. An initial urine dipstick is performed in order to exclude possible UTI. A flow test may then be performed and subsequently, following verbal consent a 6-8 F dual lumen catheter is inserted into the bladder having cleaned the external urethral meatus and anaesthetised the urethra - this records the intravesical pressure. Using a dual lumen catheter avoids the need for two separate urethral catheters. The bladder is drained of urine and this initial volume recorded. A 6-8 F single lumen catheter is placed into the rectum - this records the intra-abdominal pressure (true detrusor pressure is calculated by measuring the intravesical pressure and subtracting the abdominal pressure). The lines are then connected to the urodynamic transducers and all lines are flushed through with saline thereby removing all air bubbles from both the tubing and the transducer chambers. All systems are zeroed at atmospheric pressure; the external transducers are placed at the level of the superior edge of the pubis symphysis. An initial cough ensures good subtraction. Contrast medium (or saline in a non-video study) at room temperature is then instilled via a peristaltic pump - medium and fast fill (50-100 mL/min) is often used, however, slower fill rates (10-30 mL/min) approaching the physiological range are mandatory when assessing a neuropathic bladder. During the study notes are made of the initial bladder residual volume, bladder volume at the time of patient’s first sensation of filling, final tolerated bladder volume and final residual volume. During bladder filling the patient is asked to consciously suppress bladder contraction and filling is discontinued at maximum tolerated capacity. Quality control is obtained by asking the patient to cough at regular intervals (usually every minute during the study and at the end of the study). In units where a tipping table is not available the study can be carried out in the sitting or standing position. Patients are asked to stand at the end of the study to assess if there is postural detrusor instability.
Q. What does one look for in the filling phase of a CMG?
A. During the filling phase one notes:
Subtraction of the lines as an indicator of study quality control
Infused volume at which sensations are felt
Evidence of detrusor overactivity (non-provoked or provoked)
Evidence of stress urinary incontinence (e.g. on coughing)
Bladder compliance (see case study on neurourology presented later in this chapter) Maximum bladder capacity
Q. What are the different-coloured traces seen in Figure 11.1?
A. Figure 11.1 demonstrates four traces. These show (from above down) the intra-abdominal (Pabd) and intravesical (Pves) pressures, subtracted pressure, i.e. detrusor pressure (Pdet = Pabd — Pves), flow trace (Qura). A filling trace is also seen (Vin). For quality control purposes a cough is seen approximately every minute. Ideally there should be a cough every minute (ensures consistently good subtraction).
Q. What has happened in Figure 11.2?
A. Figure 11.2 is a CMG trace showing the filling phase only. The white arrow shows the point when the patient stood up.
Q. What has happened in Figure 11.3?
A. In Figure 11.3 there is a sharp decrease in Pdet and Pves (arrowed) due to the Pves (bladder) catheter falling out (the adjacent short peak is the result of the catheter passing out through the external sphincter).
Q. Figure 11.4 is the filling phase of a CMG. What does it demonstrate?
A. Figure 11.4 shows idiopathic detrusor overactivity (white arrow) during the filling phase of a CMG (urgency symptoms in patient present).
Q. What type of botulinum toxin is normally used in urology?
A. Botulinum toxin is a neurotoxin derived from Clostridium botulinum. ttere are seven serotypes of botulinum toxin each with different antigenic profiles and biochemical actions; however, they all have a similar pharmacological effect. Botulinum toxin types A (BoNT/A) and B (BoNT/B) have been developed for clinical use. The available formulations of BoNT/A are BOTOX (Allergan, United States), Dysport (Ipsen, United Kingdom), and Xeomin (Merz, Germany). Each formulation of BoNT/A has its own dosing regimen which is not interchangeable. BOTOX is most commonly used followed by Dysport (former is five times more potent than latter). The 2013 National Institute for Health and Care Excellence (NICE) guidelines for treatment of urinary incontinence in women suggest an initial dose of 200 units when offering botulinum toxin A, but consider 100 units in those women who would prefer a dose with a lower chance of catheterisation and accept a reduced chance of success.

Figure 11.1 Urodynamics trace showing (from top down) intra-abdominal pressure trace, intravesical pressure trace, subtracted detrusor pressure trace and flow trace.
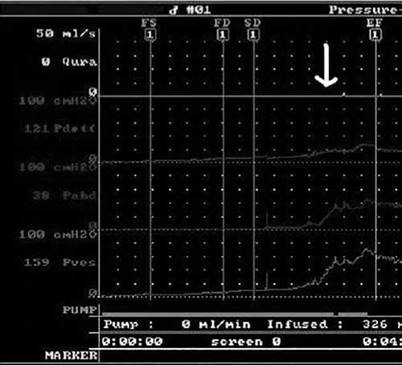
Figure 11.2 Urodynamics trace. The white arrow demonstrates a slight pressure rise (within normal limits) in subtracted detrusor pressure when the patient stands up.
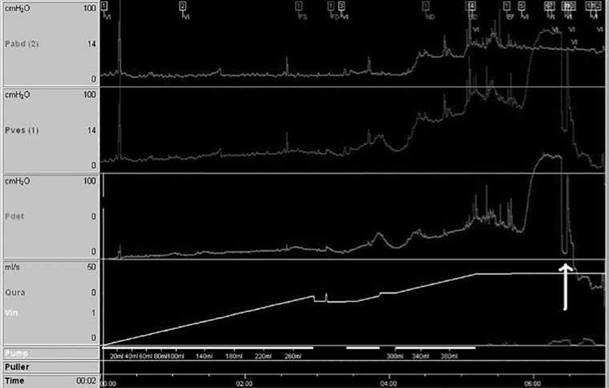
Figure 11.3 Urodynamics trace. The white arrow demonstrates a sudden decrease in detrusor and intravesical pressure as the vesical catheter is expelled from the bladder.
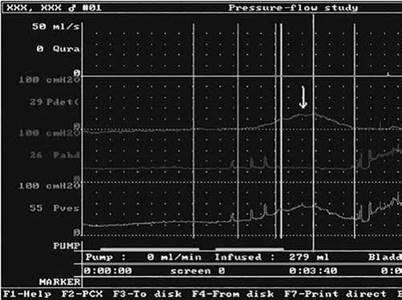
Figure 11.4 Urodynamics trace. The white arrow demonstrates a rise in detrusor and intravesical pressures which would be consistent with a detrusor contraction. Abdominal pressure remains constant at this point.
Q. How does botulinum toxin work and how do you give the injections?
A. Botulinum neurotoxin type A (BoNT/A) temporarily blocks the presynaptic vesicular release of acetylcholine (ACh) at the neuromuscular junction of the parasympathetic nerves supplying the detrusor. This results in a temporary paralysis of the detrusor muscle. BoNT/A prevents the exocytosis of ACh by cleaving SNAP-25 off the SNARE proteins, a complex protein which when intact forms the core of the neuroexocytosis machinery. It is on this premise that intradetrusor injections of BoNT/A were introduced to treat intractable bladder symptoms of detrusor overactivity and is the basis of decrease in detrusor pressures and phasic contractions in both idiopathic and neuropathic bladders. However, patients also report a significant decrease in urgency and hence, it is hypothesised that botulinum toxin also modulates the sensory pathways. This is thought to work by its action on P2X receptors.
Administration of intradetrusor BoNT/A injections has been described under local, regional or general anaesthetic using a flexible or rigid cystoscope. For idiopathic detrusor overactivity typically 200 units of BOTOX (diluted in 20 mL of normal saline) or 750-1000 units of Dysport have been used. There is no standard injection technique. However, intradetrusor injections, as opposed to submucosal injections, with sparing of the trigone are favoured. Again, there is no consensus on the number of injection sites and the dilution of the toxin but generally 20 sites are injected and the volume per injection is usually 0.5-1 mL.
Q. What are the efficacy and potential side effects of intravesical injection of botulinum toxin?
A. The efficacy for idiopathic detrusor overactivity ranges from 36% to 89% (mean 70%). The effects last from 4 to 10 months (mean 6 months) (note BoNT/A is much more effective in neurogenic detrusor overactivity).
The local side effects include pain, UTI (<5%), bleeding (<5%), no benefit, need for further injections, need for temporary self-catheterisation (very variable, but approximately may be necessary in 10%-15%). The generalised side effects include flu-like symptoms, dry mouth and malaise.
Q. Are you aware of any long-term effects of repeated injections or that botulinum toxin loses its efficacy after repeated injections?
A. No significant bladder fibrosis has been reported on histological examination after repeated injections. Also seven repeat injections have not demonstrated any decrease in efficacy of BOTOX.
Q. What is the basis of sacral neuromodulation (SNM)?
A. The precise mechanism of action is not fully recognised. SNM can be used in the treatment of intractable detrusor overactivity and also women with urinary retention due to a primary disorder of sphincter relaxation (Fowler’s syndrome). It is thought that the continuous use of mild electrical activity to stimulate the sacral afferents (mainly S3) to the bladder and pelvic floor modulates local neural reflexes and inhibits bladder contraction. There is also evidence to suggest that signals from higher brain centres involved in the control of micturition are also affected thus explaining its use in the mentioned conditions.
Q. How is the SNM delivered?
A. This is a minimally invasive procedure and can be performed under general or local anaesthesia. Generally a two-stage technique is used as it has been shown that the two- stage method improves the efficacy from 50% to 75% for refractory IDO. Initially a test implant (stimulation wire) is inserted into the S3 foramina. This is attached to a temporary pulse generator device that the patient wears externally. The patient goes home and keeps a bladder diary and records her symptoms for 2 weeks. This is compared with a pre-operative evaluation. A greater than 50% benefit in symptoms entitles the patient to have the second stage, i.e. permanent electrode fitted into the S3 foramen with the pulse generator being implanted in a pouch superficial to the posterior superior iliac crest.
Q. What are the efficacy/side effects and complications of SNM?
A. It is thought to be effective in 60%-75% of cases of IDO (efficacy rates are higher in women with Fowler’s syndrome). Should the procedure prove to be efficacious then the beneficial effects should be long term; however, the battery life of the latest implants is about 7 years after which the unit will require revising. Previously the main complication was migration of the lead but this has reduced after introduction of the tined (barbed) lead. Occasionally the patient complains of pain at the site of implantation of the pulse generator or in the lower limb. The explantation rate is 10% and this is mainly due to infection or lack of sustained efficacy.
Q. What is a clam augmentation cystoplasty and how does it work?
A. The principle of an augmentation cystoplasty is to bivalve the bladder coronally (like a clam) and patch the defect with a piece of bowel, generally ileum is used (ileocystoplasty) however other bowel segments have been described (Figure 11.5). This impairs bladder contraction, lowers the detrusor pressures and increases the capacity of the bladder. It decreases the amplitude of contractions by preventing sustained detrusor contractions.

Figure 11.5 Bladder bivalved coronally and ileal augmentation cystoplasty being performed.
Q. What are contraindications for clam augmentation cystoplasty?
A. These include
Severe inflammatory bowel disease, i.e. Crohn’s disease
Previous pelvic radiotherapy
Critically short bowel
A patient’s unwillingness or inability (due to poor hand function) to perform self-catheterisation
Significant renal impairment (results in inability to compensate for hyperchloraemic metabolic acidosis)
Significant hepatic impairment (results in inability to metabolise NH3)
Q. What are the potential complications of clam augmentation cystoplasty (enterocystoplasty)?
A. These include
Major early complications:
1. Mortality: 0%-2.5% (especially in neurogenic patients due to bladder rupture)
2. Myocardial infarction: 0%-2.5%
3. Thromboembolic events: 1%-7%
4. Re-operation for post-operative bleeding: 0%-3%
5. Wound infection ± dehiscence: 5%-6.5%
6. Small bowel obstruction due to adhesions: 3%—5.5%
7. Fistula: 0.4%-30%
Long-term complications:
1. The need for post-operative intermittent catheterisation - The rate is approximately 50%-60% in idiopathic patients. This generally increases over time.
2. Stones - The reported rates are highly variable between 0% and 53%. It is generally thought to be approximately 15%. They are more common if there has been an associated Mitrofanoff procedure.
3. Troublesome mucus production - The average daily production from the incorporated bowel segment is 35-40 grams. This does not decrease over time and can lead to infections, stone formation and blockages. Bladder washouts might be required with acetylcysteine to dissolve excess mucus.
4. Bacteriuria and UTI - Almost 100% of patients will have asymptomatic bacteriuria. The incidence of clinically significant UTI is around 4%-43%.
5. Biochemical abnormalities - The presence of permeable bowel in the urinary tract leads to reabsorption of ammonium chloride and excretion of bicarbonate resulting in acid-base imbalance. Ammonium chloride (NH4Cl) which is readily reabsorbed dissociates into ammonia (NH3) and hydrochloric acid (HCl); the HCl in solution in turn dissociates into H+ and Cl- thereby resulting in hyperchloraemic acidosis. However, this is clinically important in few cases (15%) and in these the treatment is administration of bicarbonate. The biochemical changes explain the reason that augmentation cystoplasty is contraindicated in liver and significant renal failure - in these patients the NH3 cannot be metabolized by the damaged liver and the acidosis cannot be corrected by the failing kidneys.
Note: The incidence of this biochemical abnormality happening in a patient with an ileal conduit is much less since the conduit is exactly that, a conduit for urine, and not a reservoir unlike the augmented bladder. Thus the urine in a conduit does not stay in it for sufficient time in order for the exchange to take place (i.e. absorption of NH4Cl).
6. Renal function deterioration - This can happen in 0%-15% of cases. It is more marked in patients who have a creatinine clearance of less than 15 mL/min (corrected for surface area) pre-operatively. However, it has been reported that the renal function has actually improved in 4% of cases.
7. Perforation - Spontaneous perforation is a rare complication (<1%) but carries a mortality of 25% mostly due to delay in diagnosis.
8. Malignancy - There is an increased incidence of cancer in augmented bladders. However, there is a long latent period (>10 years). This is associated with chronic inflammation, urinary stasis and recurrent UTIs. The tumours are generally adenocarcinomas and in the region of the anastomosis. The mechanism seems to be related to bacteriuria. This leads to reduction of urinary nitrates to nitrites by colonic bacteria. This reacts with urinary amines to form N-nitrosamines, which are implicated in carcinogenesis.
9. Bowel changes - ttis usually results in diarrhoea. The symptom is troublesome in up to 30% of cases. Also there can be a decrease in absorption of vitamin B12 and folic acid leading to neurological complications (B12 deficiency may also be due to disruption of the absorptive terminal ileum).
10. Reduced growth potential and increased incidence of fractures in growing children - The hydrogen (from the acidosis) is buffered in exchange for calcium causing demineralisation of bone (this calcium is subsequently lost in the urine). The acidosis in growing children, if present, should be treated with sodium bicarbonate [3].
Q. How do you follow up a patient following an augmentation cystoplasty?
A. Once stable the patients are seen on a yearly basis with an ultrasound scan (USS) of kidneys and a kidneys, ureters and bladder (KUB) x-ray. The biochemical analysis includes evaluation of kidney and liver function and estimation of serum chloride, bicarbonate, vitamin B12 and folic acid levels. ttey are advised to contact the department urgently if they develop recurrent UTIs, haematuria, significant weight loss or severe lethargy. ttey will undergo yearly surveillance cystoscopies from 10 years after operation [4].