8.1 The Peritoneum and Peritoneal Cavity
The peritoneum, a thin, transparent serous membrane, lines the abdominopelvic cavity. Parietal and visceral layers of the peritoneum enclose the peritoneal cavity, which contains a thin film of serous fluid that facilitates the movement of the viscera during digestion and respiration (see Fig. 7.1).
8.1a Peritoneal Relations
– Structures in the abdomen are defined with respect to their relationship to the peritoneum (Table 8.1; Figs. 8.1 and 8.2).
• Intraperitoneal organs, almost completely enclosed by the visceral layer of the peritoneum, are suspended within the peritoneal cavity by mesenteries, double layers of peritoneum that attach to the body wall.
• Extraperitoneal structures lie posterior or inferior to the peritoneal cavity.
○ Primarily retroperitoneal structures lie posterior to the peritoneal cavity, are not suspended by a mesentery, and are usually covered by peritoneum only on their anterior surface.
○ Secondarily retroperitoneal structures were previously intraperitoneal structures that became fixed to the posterior abdominal wall when their mesentery fused with the parietal peritoneum of the posterior abdominal wall during development.
○ Subperitoneal structures include pelvic organs that lie below the peritoneum.
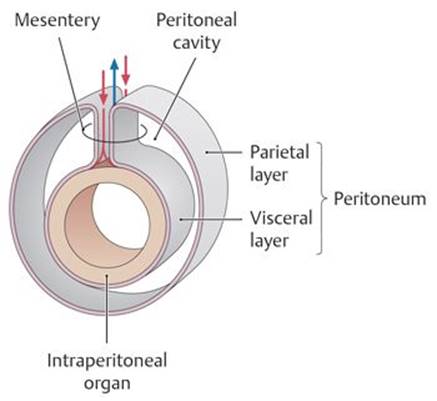
Fig. 8.1 ![]() Peritoneum and mesentery
Peritoneum and mesentery
Red and blue arrows indicate location of blood vessels.
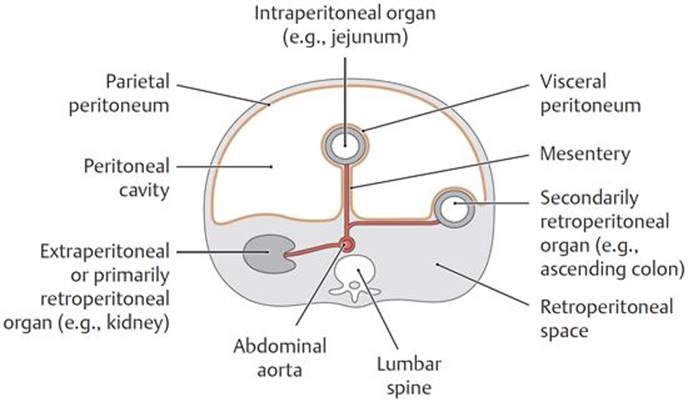
Fig. 8.2 ![]() Peritoneal relations of the organs in the abdomen
Peritoneal relations of the organs in the abdomen
Transverse section through the abdomen showing the peritoneal relationships of abdominal organs. Viewed from above.
TABLE 8.1 ![]() Organs of the Abdomen
Organs of the Abdomen
|
Location |
Organs |
|
|
Intraperitoneal organs: These organs have a mesentery and are completely covered by the peritoneum. |
||
|
Abdominal peritoneal cavity |
• Stomach • Small intestine (jejunum, ileum, some of the superior part of the duodenum) • Spleen • Liver (with the exception of the bare area) • Gallbladder • Cecum with vermiform appendix (portions of variable size may be retroperitoneal) • Large intestine (transverse and sigmoid colons) |
|
|
Extraperitoneal organs: These organs either have no mesentery or lost it during development. |
||
|
Retroperitoneum |
Primarily retroperitoneal |
• Kidneys • Suprarenal glands |
|
Secondarily retroperitoneal |
• Duodenum (descending, horizontal, and ascending) • Pancreas • Ascending and descending colon |
|
– Organs associated with the gastrointestinal tract are intraperitoneal or secondarily retroperitoneal. Organs of the urinary system are retroperitoneal.
8.1b Peritoneal Structures
Most of the abdominal viscera are somewhat mobile during digestion and respiration. Reflections of the peritoneum that connect organs to the body wall or to other organs prevent excessive movement (i.e., twisting), which can compromise normal function. These reflections form mesenteries, omenta, and peritoneal ligaments.
– A mesentery is a double layer of peritoneum that connects intraperitoneal organs to the posterior abdominal wall and transmits vessels and nerves (see Fig. 8.1). There are three major mesenteries in the abdomen (Fig. 8.3):
• The mesentery of the small intestine, or the “mesentery,” is a fan-shaped apron of peritoneum that suspends the second and third parts (jejunum and ileum) of the small intestine.
• The transverse mesocolon suspends the transverse section of the large intestine.
• The sigmoid mesocolon suspends the sigmoid colon of the large intestine in the left lower quadrant.
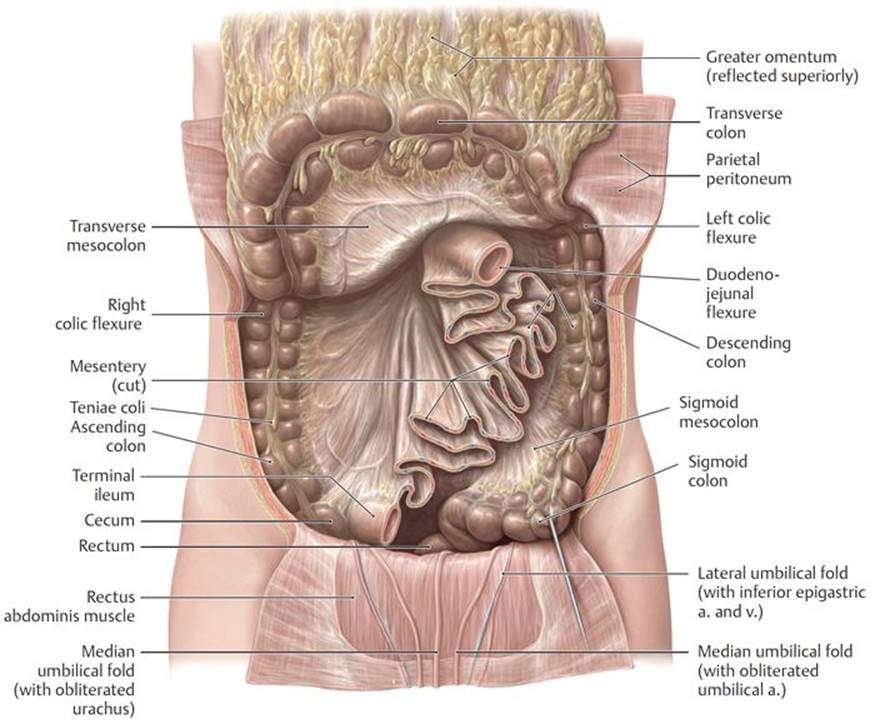
Fig. 8.3 ![]() Mesenteries of the peritoneal cavity
Mesenteries of the peritoneal cavity
Anterior view. Reflected: Greater omentum and transverse colon. Removed: Intraperitoneal small intestine.
– An omentum is a double layer of peritoneum that connects the stomach and duodenum to another organ. There are two omenta (Figs. 8.4 and 8.5; see also Fig. 9.1):
• The greater omentum, a four-layered apron of peritoneum, originates as a double layer of peritoneum from the greater curvature of the stomach and proximal duodenum. It drapes inferiorly, anterior to the coils of small intestine, before looping upward to its distal attachment on the posterior abdominal wall.
○ The gastrocolic ligament is a portion of the greater omentum that adheres to the transverse colon (Fig. 8.6).
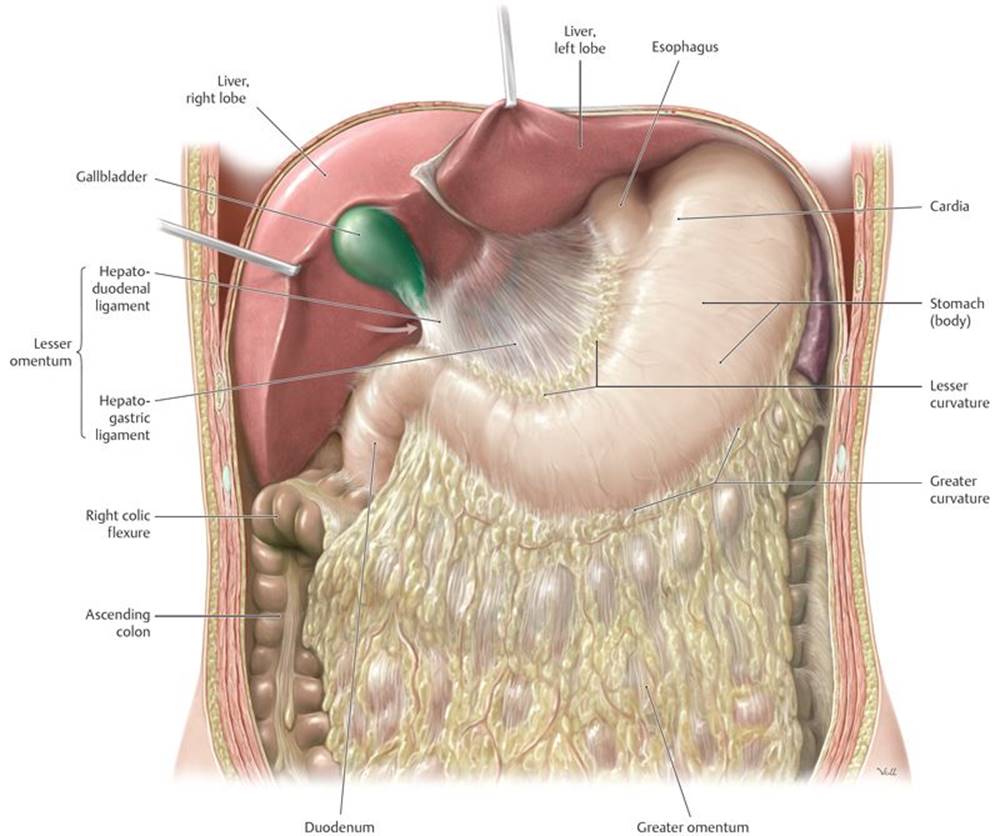
Fig. 8.4 ![]() Greater and lesser omenta
Greater and lesser omenta
Anterior view of the opened upper abdomen. Arrow indicates the omental foramen.
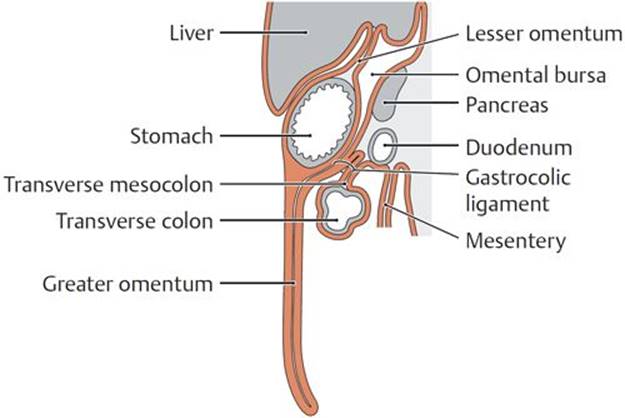
Fig. 8.5 ![]() Peritoneal structures
Peritoneal structures
A Sagittal section.
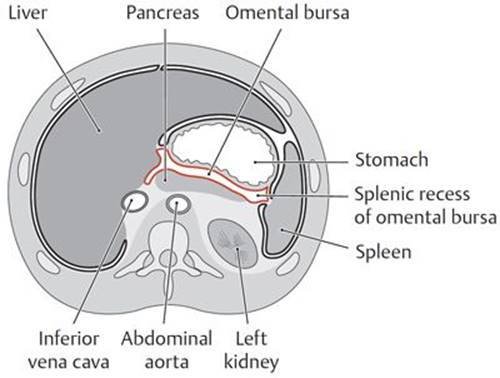
B Transverse section, interior view.
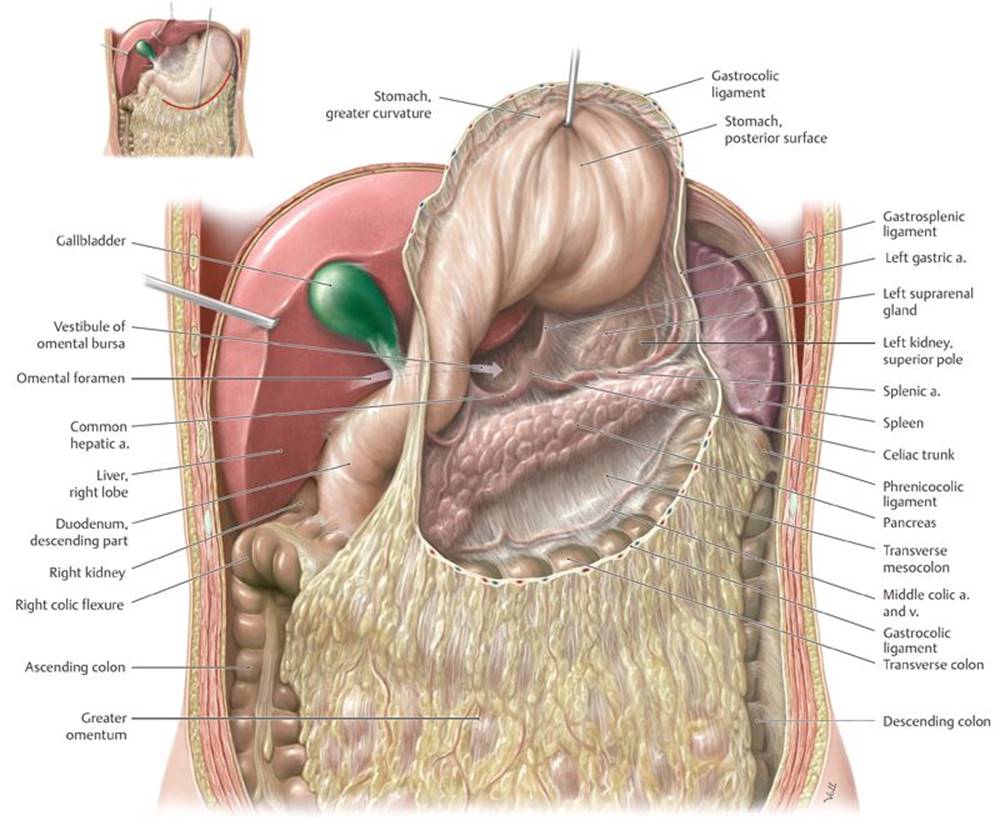
Fig. 8.6 ![]() Omental bursa in situ
Omental bursa in situ
Anterior view. Divided: Gastrocolic ligament. Retracted: Liver. Reflected: Stomach.
○ The gastrosplenic ligament is a lateral extension of the greater omentum that connects the stomach to the spleen and is traversed by branches of the splenic artery (Fig. 8.7).
• The lesser omentum, a double layer of peritoneum, extends from the liver to the stomach and proximal duodenum. It is formed by
○ the hepatogastric ligament, between the liver and stomach, and
○ the hepatoduodenal ligament, between the liver and duodenum, which encloses the structures of the portal triad (the portal vein, hepatic artery, and bile duct) in its free edge.
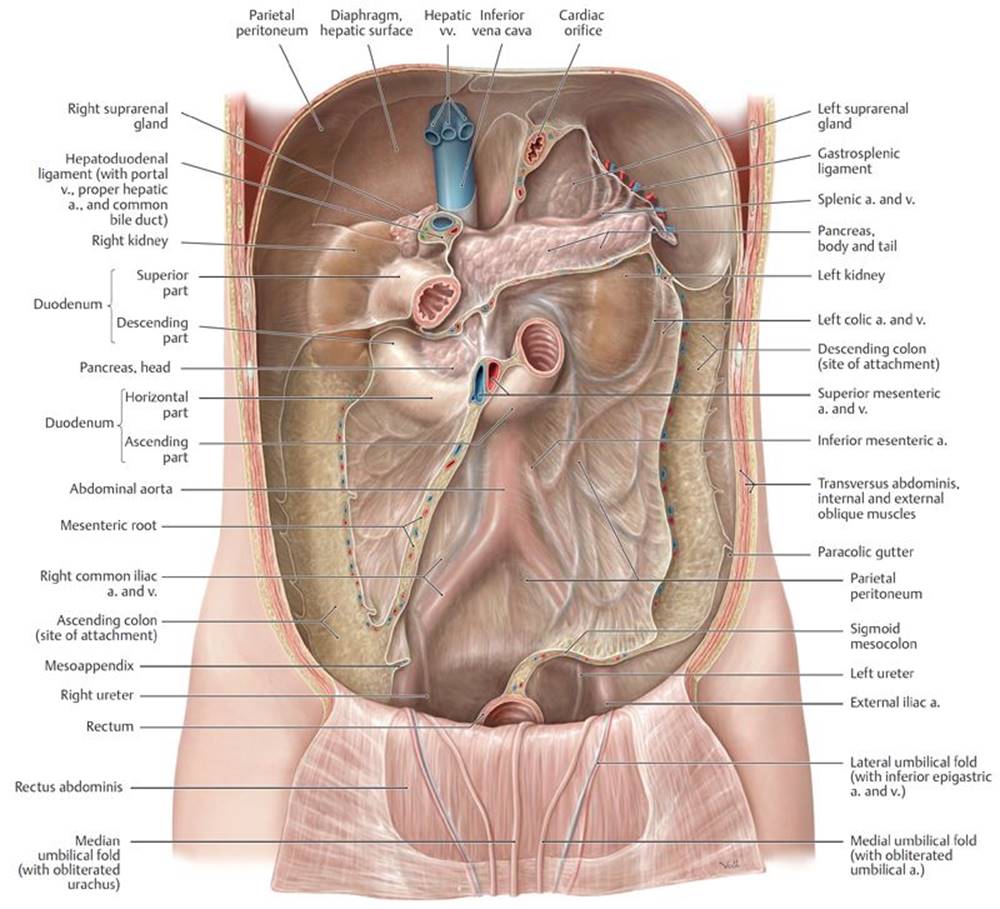
Fig. 8.7 ![]() Posterior wall of the peritoneal cavity
Posterior wall of the peritoneal cavity
Anterior view. Removed: All intraperitoneal organs.
– Peritoneal ligaments are reflections of peritoneum that connect organs to each other or to the body wall. They support the organ in position and may convey their neurovasculature. Individual ligaments are discussed in Sections 9.2 to 9.4 with the specific abdominal organs.
8.1c Neurovasculature of the Peritoneum
The neurovasculature for the parietal and visceral peritoneum is derived from different sources.
– Parietal peritoneum derives its neurovasculature from vessels and nerves of the body wall. Its sensitivity to pain, pressure, and temperature is well localized (felt acutely) through somatic nerves of the overlying muscles and skin.
– Visceral peritoneum derives its neurovasculature from the underlying organs. Autonomic nerves mediate sensitivity to stretching and chemical irritation, but the visceral peritoneum lacks sensitivity to touch and temperature.
– Sensation is poorly localized and is usually referred to regions that reflect the embryological origins of the underlying organ.
• Sensation from foregut structures is referred to the epigastric region.
• Sensation from midgut structures is referred to the umbilical region.
• Sensation from hindgut structures is referred to the pubic region.
8.1d Subdivisions of the Peritoneal Cavity
– The peritoneal cavity is divided into two spaces:
• The greater sac, which includes the entire peritoneal cavity except that space defined as the lesser sac
• The omental bursa (lesser sac), which is a small extension of the peritoneal cavity that lies behind the stomach and lesser omentum (Table 8.2; see also Figs. 8.5 and 8.6). It communicates with the greater sac through a single opening, the omental (epiploic) foramen (Table 8.3).
TABLE 8.2 ![]() Boundaries of the Omental Bursa (Lesser Sac)
Boundaries of the Omental Bursa (Lesser Sac)
|
Direction |
Boundary |
Recess |
|
Anterior |
Lesser omentum, gastrocolic ligament |
– |
|
Inferior |
Transverse mesocolon |
Inferior recess |
|
Superior |
Liver (with caudate lobe) |
Superior recess |
|
Posterior |
Pancreas, aorta (abdominal part), celiac trunk, splenic a. and v., gastrosplenic fold, left suprarenal gland, left kidney (superior pole) |
– |
|
Right |
Liver, duodenal bulb |
– |
|
Left |
Spleen, gastrosplenic ligament |
Splenic recess |
– Attachments of the peritoneum to the body wall that form during development of the gastrointestinal tract further subdivide the greater sac. These attachments can influence the flow of fluid within the cavity (Figs. 8.8 and 8.9).
• The subphrenic recess between the diaphragm and liver is limited by the coronary ligaments and separated into right and left spaces by the falciform ligament.
• The subhepatic space lies between the liver and the transverse colon. A posterior extension of this space, the hepatorenal recess (hepatorenal pouch, Morison’s pouch), lies between the visceral surface of the liver and the right kidney and suprarenal gland. The hepatorenal recess communicates with the right subphrenic recess.
• The supracolic and infracolic compartments are defined by the attachment of the transverse mesocolon on the posterior abdominal wall—with the supracolic compartment above the attachment site and the infracolic compartment below it. The root of the mesentery of the small intestine further divides the infracolic compartment into right and left spaces.
• The paracolic gutters, which lie adjacent to the ascending and descending colons, allow communication between the supracolic and infracolic compartments.
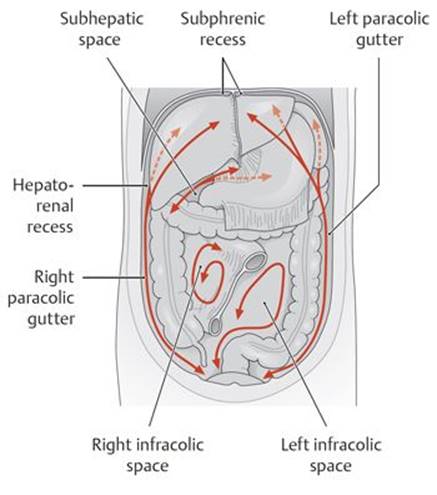
Fig. 8.8 ![]() Drainage spaces within the peritoneal cavity
Drainage spaces within the peritoneal cavity
Anterior view.
TABLE 8.3 ![]() Boundaries of the Omental Foramen
Boundaries of the Omental Foramen
|
The communication between the greater and lesser sacs is the omental (epiploic) foramen (see arrow in Figs. 8.4 and 8.6). |
|
|
Direction |
Boundary |
|
Anterior |
Hepatoduodenal ligament with the portal v., proper hepatic a., and bile duct |
|
Inferior |
Duodenum (superior part) |
|
Posterior |
Inferior vena cava, diaphragm (right crus) |
|
Superior |
Liver (caudate lobe) |
Peritonitis and ascites
Bacterial contamination of the peritoneum following surgery or rupture of an inflamed organ (duodenum, gallbladder, appendix) results in peritonitis, inflammation of the peritoneum. It is accompanied by severe abdominal pain, tenderness, nausea, and fever and can be fatal when generalized throughout the peritoneal cavity. It often results in ascites, the accumulation of excess peritoneal fluid due to a change in concentration gradients that results in loss of capillary fluid. Ascites can also accompany other pathological conditions, such as metastatic liver cancer and portal hypertension. In these cases, many liters of acitic fluid can accumulate in the peritoneal cavity. The fluid is aspirated by paracentesis. The needle is carefully inserted into the abdominal wall so as to avoid the urinary bladder and inferior epigastric vessels.
Peritoneal infections and abscesses
The flow of fluid in the peritoneal cavity can spread intraperitoneal infections and determine the sites of peritoneal abscess formation. Fluid commonly collects in the right and left subphrenic recesses, although abscesses are more likely to form on the right side due to duodenal or appendyceal ruptures. Fluid in the supracolic compartment, such as subphrenic recesses and the omental bursa, can drain to the hepatorenal recess, the lowest part of the abdominal cavity in the supine patient. Therefore, this is a common site of pus accumulation and abscess formation. In the infracolic compartment, the paracolic gutters direct peritoneal fluid and infections toward the pelvis.
8.2 Neurovasculature of the Abdomen
8.2a Arteries of the Abdomen (Fig. 8.9)
– The abdominal aorta supplies abdominal viscera and most of the anterior abdominal wall.
• It enters the abdomen at T12 through the aortic hiatus of the diaphragm and descends along the vertebral column to the left of the midline.
• It terminates at the L4 vertebral level, where it bifurcates into two common iliac arteries.
• A single median sacral artery arises near the bifurcation.
Abdominal aortic aneurysm
Abdominal aortic aneurysms (AAAs) most commonly occur between the renal arteries and the bifurcation of the aorta. When small they can remain asymptomatic, but large aneurysms can be palpated through the abdominal wall to the left of the midline. Ruptured AAAs present with severe abdominal pain that radiates to the abdomen or back. Mortality rates for ruptured aneurysms approach 90% due to overwhelming hemorrhage.
– Table 8.4 lists major branches of the abdominal aorta.
• Paired parietal (segmental) branches supply the structures of the posterior abdominal wall. These include the inferior phrenic and lumbar arteries.
• Paired visceral branches supply organs of the retroperitoneum. These are the middle suprarenal, testicular or ovarian, and renal arteries.
TABLE 8.4 ![]() Branches of the Abdominal Aorta
Branches of the Abdominal Aorta
|
The abdominal aorta gives rise to three major unpaired trunks (bold) and the unpaired median sacral artery, as well as six paired branches. |
||
|
Branch from abdominal aorta Branches |
||
|
Inferior phrenic aa. (paired) |
Superior suprarenal aa. |
|
|
Celiac trunk |
Left gastric a. |
|
|
Splenic a. |
||
|
Common hepatic a. |
Proper hepatic a. |
|
|
Right gastric a. |
||
|
Gastroduodenal a. |
||
|
Middle suprarenal aa. (paired) |
||
|
Superior mesenteric a. |
||
|
Renal aa. (paired) |
Inferior suprarenal aa. |
|
|
Lumbar aa. (1st through 4th, paired) |
||
|
Testicular/ovarian aa. (paired) |
||
|
Inferior mesenteric a. |
||
|
Common iliac aa. (paired) |
External iliac a. |
|
|
Internal iliac a. |
||
|
Median sacral a. |
||
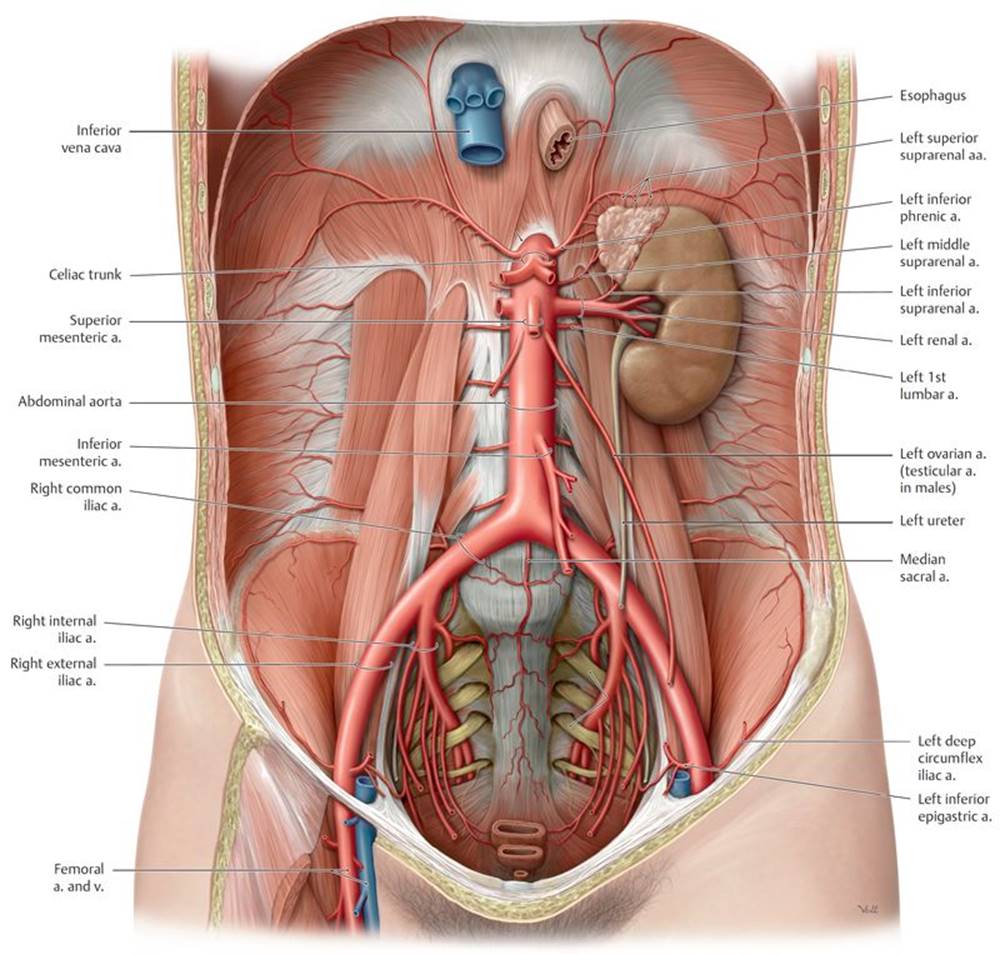
Fig. 8.9 ![]() Abdominal aorta
Abdominal aorta
Female abdomen, anterior view. Removed: Abdominal organs and peritoneum. The abdominal aorta is the distal continuation of the thoracic aorta. It enters the abdomen at the T12 level and bifurcates into the common iliac arteries at L4.
• Three unpaired visceral branches supply the intestines and accessory organs of the gastrointestinal tract:
1. The celiac trunk, a short trunk that arises at T12/L1 and supplies the abdominal foregut. Its branches, the splenic, left gastric, and common hepatic arteries, anastomose extensively with each other (Figs. 8.10 and 8.11).
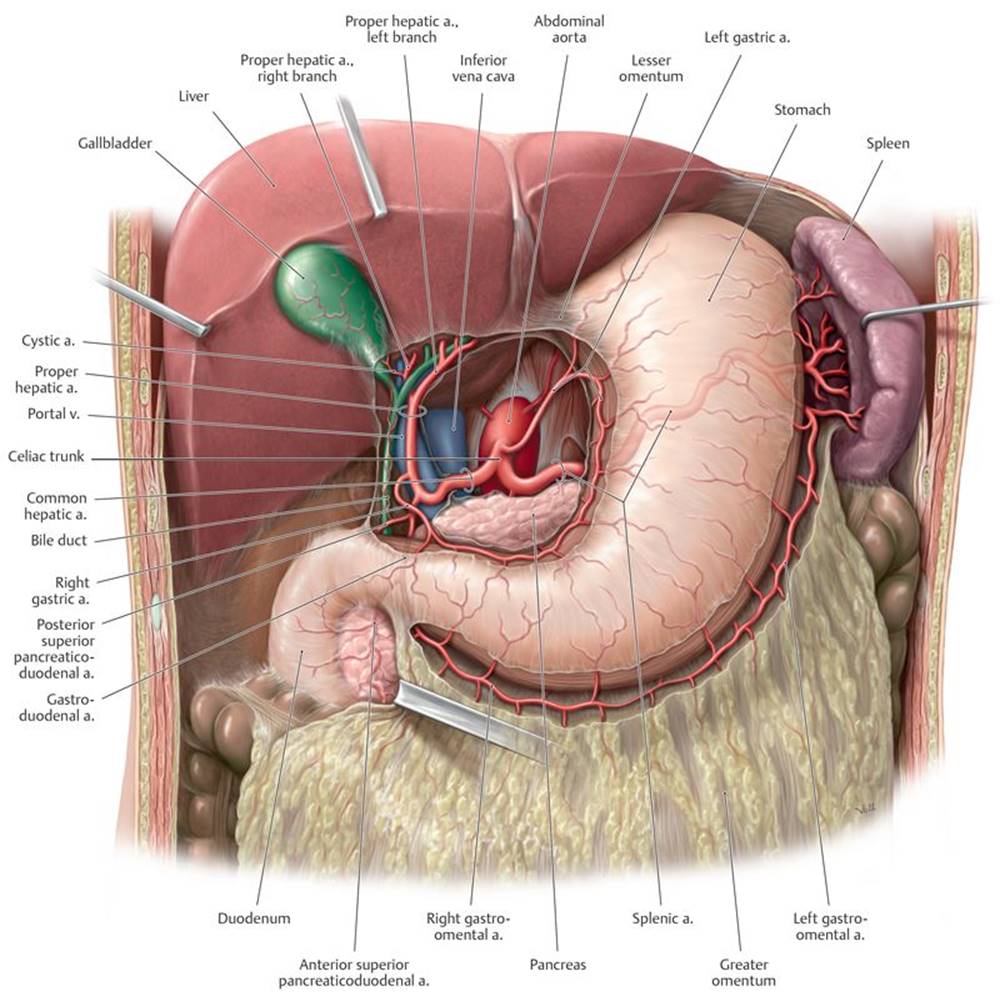
Fig. 8.10 ![]() Celiac trunk: Stomach, liver, and gallbladder
Celiac trunk: Stomach, liver, and gallbladder
Anterior view. Opened: Lesser omentum. Incised: Greater omentum. The celiac trunk arises from the abdominal aorta at about the level of L1.

Fig. 8.11 ![]() Celiac trunk: Pancreas, duodenum, and spleen
Celiac trunk: Pancreas, duodenum, and spleen
Anterior view. Removed: Stomach (body) and lesser omentum.
2. The superior mesenteric artery (SMA), which arises at L1, posterior to the neck of the pancreas. It supplies midgut structures, and its major branches include the inferior pancreaticoduodenal, middle colic, right colic, and ileocolic arteries, as well as a series of jejunal and ileal branches (Fig. 8.12).
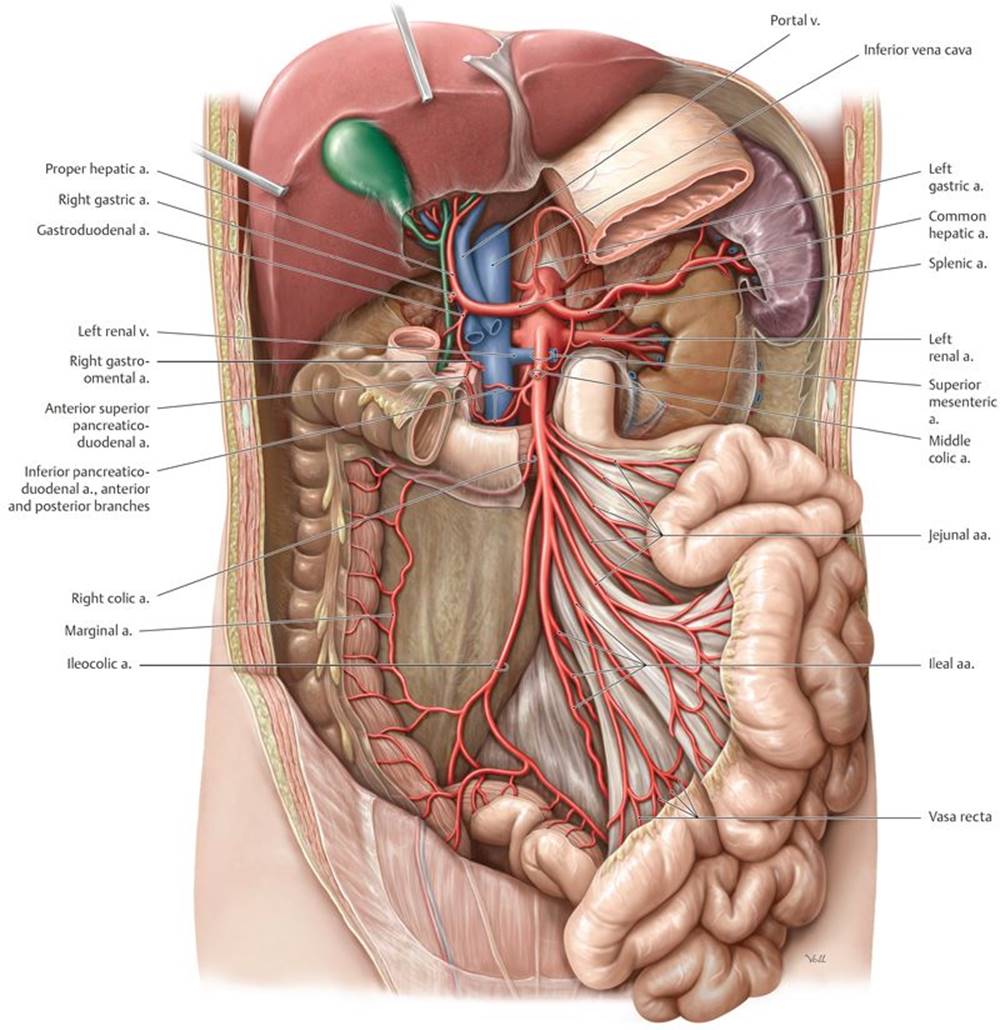
Fig. 8.12 ![]() Superior mesenteric artery
Superior mesenteric artery
Anterior view. Partially removed: Stomach and peritoneum. Note: The middle colic artery has been truncated. The superior mesenteric artery arises from the aorta opposite L2.
3. The inferior mesenteric artery (IMA), which arises at L3 and has the smallest caliber of the three visceral trunks. It supplies the hindgut through its left colic, sigmoidal, and superior rectal branches (Fig. 8.13).
• Common iliac arteries pass along the brim of the pelvis and terminate by bifurcating into two major branches (see Fig. 8.9):
○ The internal iliac artery, which descends into the pelvis
○ The external iliac artery, which gives off the inferior epigastric and deep circumflex iliac arteries before passing into the lower limb as the femoral artery.
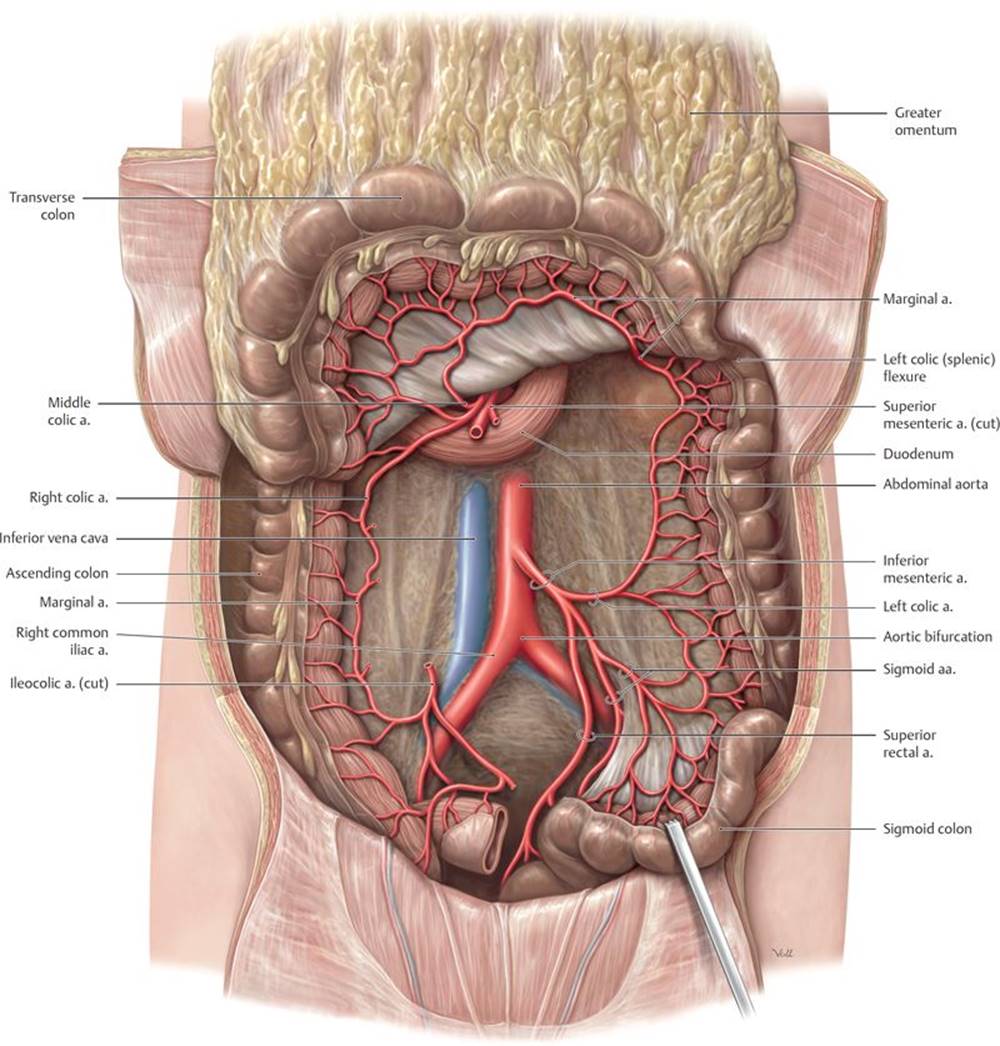
Fig. 8.13 ![]() Inferior mesenteric artery
Inferior mesenteric artery
Anterior view. Removed: Jejunum and ileum. Reflected: Transverse colon. The inferior mesenteric artery arises from the aorta opposite L3.
– Important anastomoses connect the three unpaired visceral branches of the aorta and provide a collateral blood supply to the intestinal organs (Fig. 8.14).
• The celiac trunk and superior mesenteric artery anastomose in the head of the pancreas through the pancreaticoduodenal arteries and in the body and tail of the pancreas through dorsal pancreatic and inferior pancreatic arteries.
• The superior mesenteric and inferior mesenteric arteries anastomose near the junction of the transverse and descending colons through the middle and left colic arteries. The marginal artery runs along the mesenteric border of the large intestine and connects the ileocolic, right colic, middle colic, and left colic arteries (see Fig. 8.13).
• The inferior mesenteric artery anastomoses with arteries of the rectum through its superior rectal artery (see Fig. 10.18).
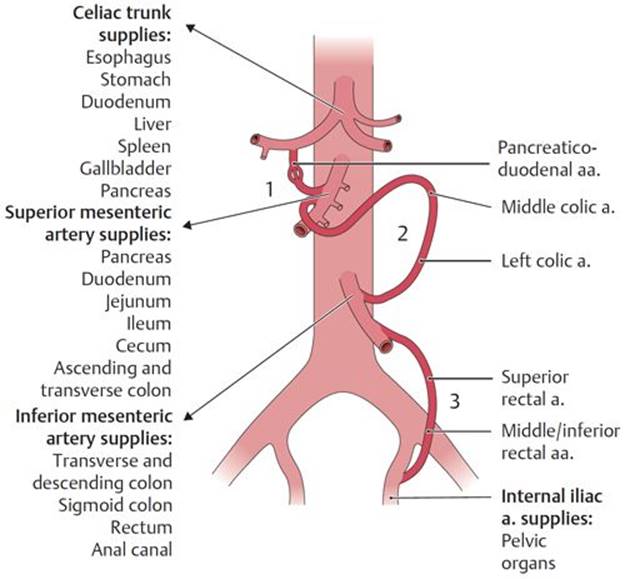
Fig. 8.14 ![]() Abdominal arterial anastomoses
Abdominal arterial anastomoses
Three major anastomoses provide overlap in the arterial supply to ensure adequate blood flow to abdominal areas: (1) between the celiac trunk and the superior mesenteric artery via the pancreaticoduodenal arteries; (2) between the superior and inferior mesenteric arteries via the middle and left colic arteries; and (3) between the inferior mesenteric and internal iliac arteries via the superior and middle or inferior rectal arteries
8.2b Veins of the Abdomen
– The inferior vena cava (IVC) receives blood from retroperitoneal and pelvic organs, walls of the abdomen and pelvis, and the lower limbs (Fig. 8.15).
• It originates at the L5 vertebral level where the common iliac veins merge.
• It ascends along the right side of the vertebral column, passes posterior to the liver, and pierces the central tendon of the diaphragm at the T8 vertebral level, where it enters the right atrium of the heart.
– Table 8.5 lists the tributaries of the inferior vena cava.
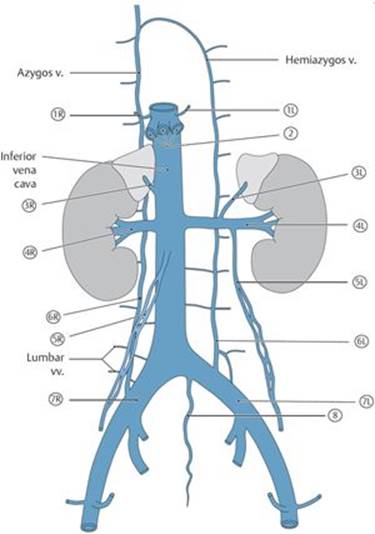
TABLE 8.5 ![]() Tributaries of the Inferior Vena Cava
Tributaries of the Inferior Vena Cava
|
|
Inferior phrenic vv. (paired) |
|
|
Hepatic vv. (3) |
|
|
Suprarenal vv. (the right vein is a direct tributary) |
|
|
Renal vv. (paired) |
|
|
Testicular/ovarian vv. (the right vein is a direct tributary) |
|
|
Ascending lumbar vv. (paired) |
|
|
Common iliac vv. (paired) |
|
|
Median sacral v. |
• Paired common iliac veins drain the external iliac and internal iliac veins.
• Paired inferior phrenic and lumbar veins drain the posterior abdominal wall and diaphragm and accompany the arteries of similar name.
• Veins of the retroperitoneal organs include the right and left renal veins, the right suprarenal vein, and the right testicular or ovarian (gonadal) vein. The suprarenal and gonadal veins on the left side drain to the left renal vein.
• Typically three hepatic veins enter the IVC from the liver immediately below the diaphragm.
– Paired ascending lumbar veins communicate with the lumbar veins and are continuous with the azygos and hemiazygos veins of the thorax. These communications between the lumbar, ascending lumbar, azygos, and hemiazygos veins function as a collateral pathway between the inferior and superior venae cavae (see Fig. 3.6)
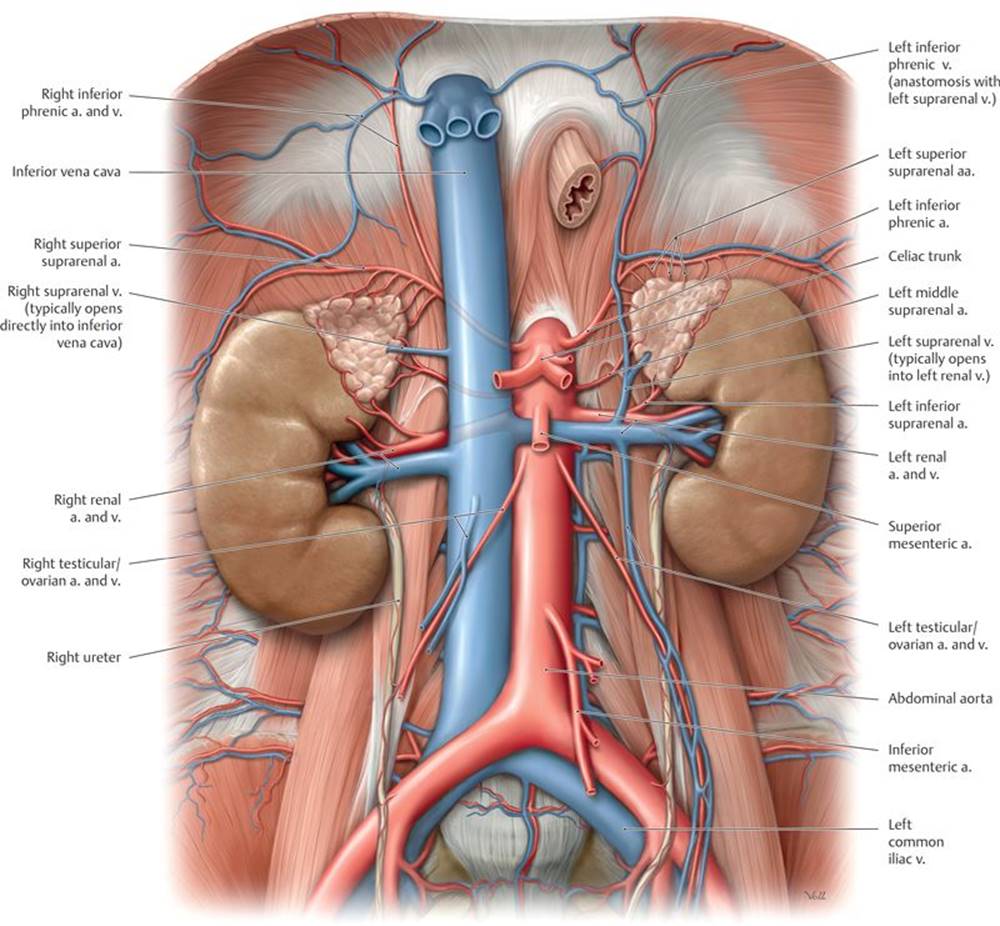
Fig. 8.15 ![]() Inferior vena cava
Inferior vena cava
Anterior view. Removed: All organs except the kidneys and suprarenal glands.
– The hepatic portal vein (usually known as the portal vein), part of the hepatic portal system, shunts nutrient-rich venous blood from the capillary beds of the gastrointestinal tract and its associated organs to sinusoids of the liver (Figs. 8.16 and 8.17). This blood eventually enters the inferior vena cava through the hepatic veins.
– Tributaries of the portal vein include the following:
• The splenic vein, which drains the spleen, and the superior mesenteric vein, which drains the small intestine and most of the large intestine. These two veins unite behind the neck of the pancreas to form the hepatic portal vein.
• The inferior mesenteric vein, which drains the hindgut portion of the gastrointestinal tract. It usually joins the splenic vein but may empty directly into the portal vein.
• Veins from the lower esophagus, stomach, pancreas, duodenum, and gallbladder
– Normal connections between the systemic (caval) venous system and portal venous system, called portosystemic pathways, can become abnormally dilated when there is an obstruction of the portal or systemic circulations (i.e., cirrhosis of the liver or pregnancy). These dilations are most prominent in (Fig. 8.18)
1. esophageal veins,
2. periumbilical veins through the superior and inferior epigastric veins of the abdominal wall,
3. colic veins in the retroperitoneum, and
4. rectal veins of the rectum and anal canal.
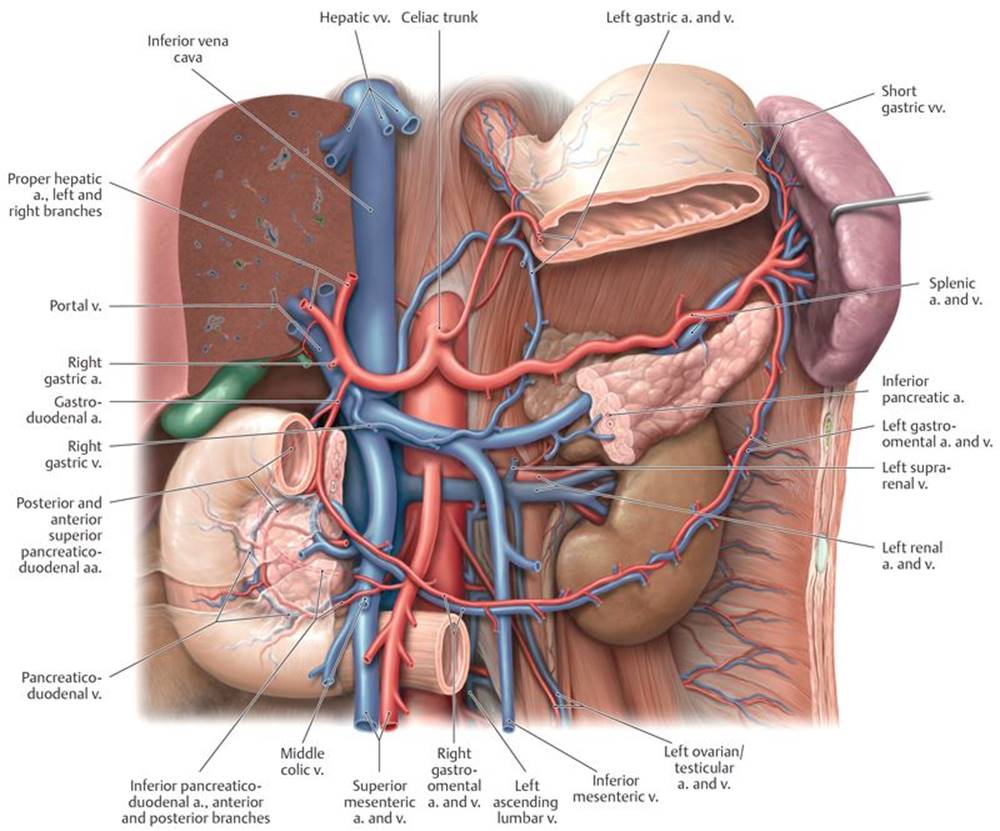
Fig. 8.16 ![]() Portal vein: In situ
Portal vein: In situ
Anterior view. Partially removed: Stomach, pancreas, and peritoneum.
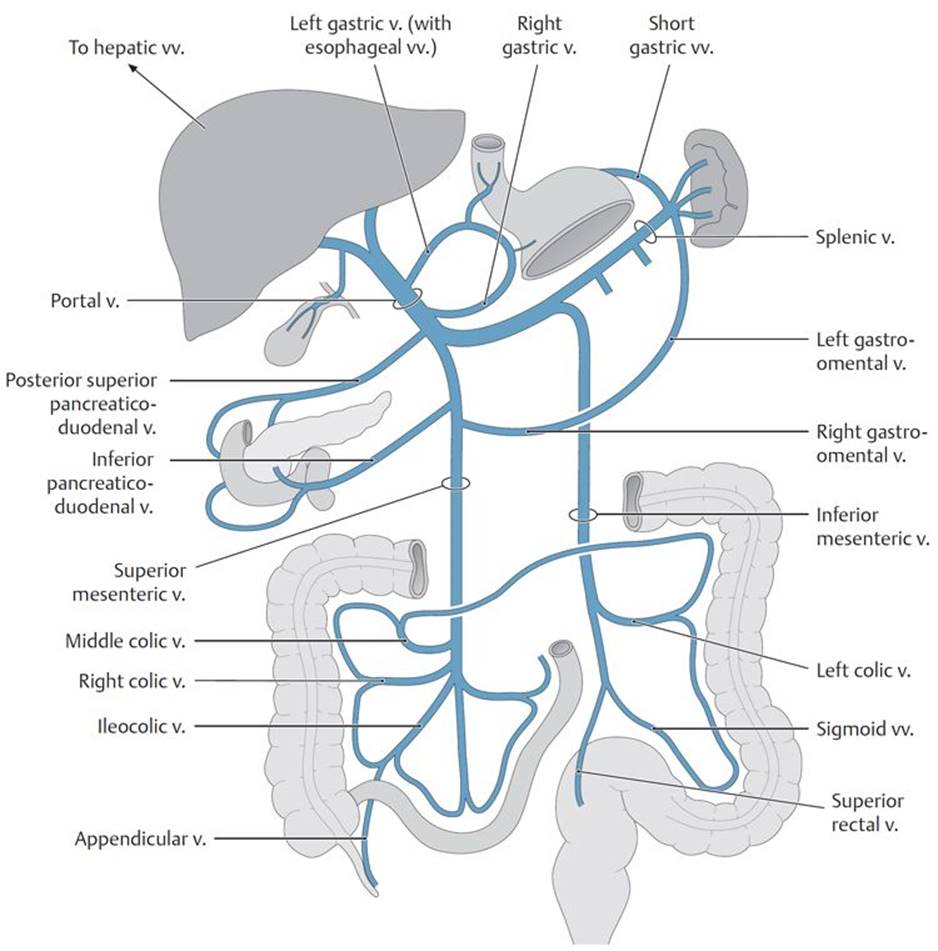
Fig. 8.17 ![]() Portal vein distribution
Portal vein distribution
The portal vein drains venous blood from the abdominopelvic organs supplied by the celiac trunk and superior and inferior mesenteric arteries.
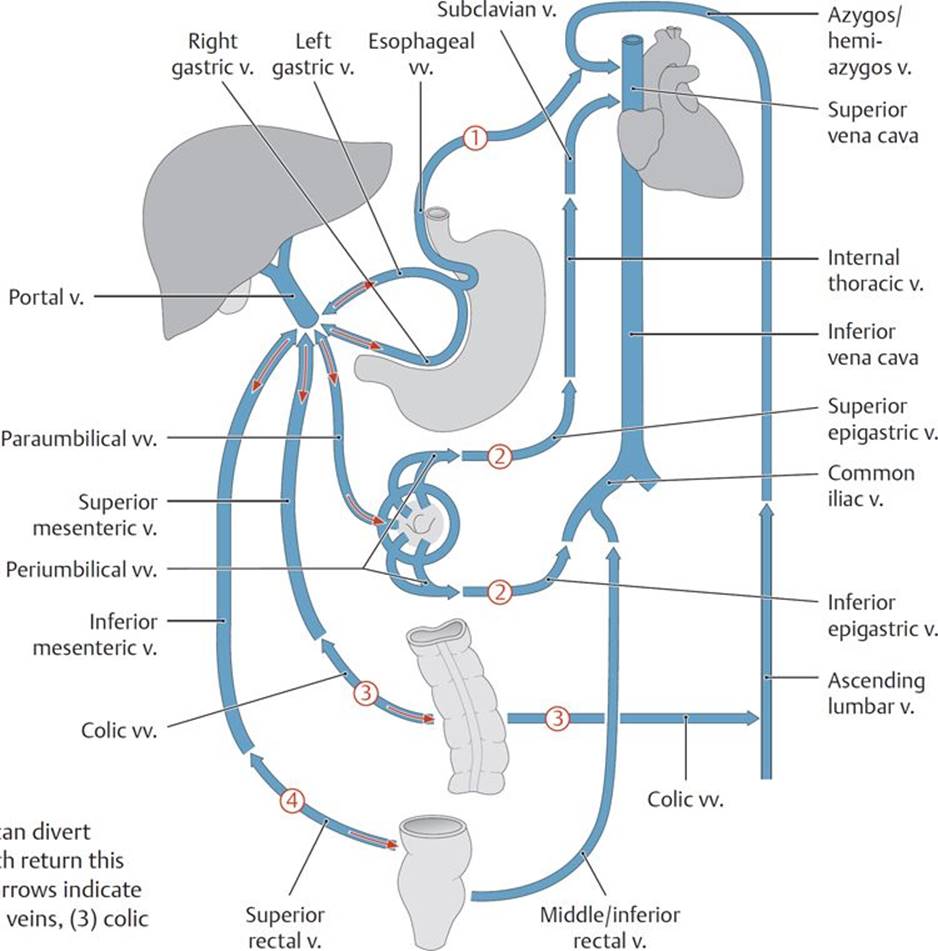
Fig. 8.18 ![]() Portosystemic pathways
Portosystemic pathways
When the portal system is compromised, the portal vein can divert blood away from the liver back to its supplying veins, which return this nutrient-rich blood to the heart via the venae cavae. Red arrows indicate flow reversal in the (1) esophageal veins, (2) paraumbilical veins, (3) colic veins, and (4) middle and inferior rectal veins.
Portal hypertension and surgical portocaval shunts
Portal hypertension occurs secondary to liver disease (e.g., cirrhosis) or thrombosis of the portal vein. Increased resistance to the flow of blood in the portal system forces portal blood through portocaval anastomoses to the systemic circulation. Symptoms of portal hypertension include ascites, caput medusa (enlargement of periumbilical veins on the anterior abdominal wall), varices of the rectal veins (hemorrhoids), and esophageal varices. Symptoms may be relieved by surgically creating a portocaval shunt between the portal and systemic circulations (portal vein to the inferior vena cava or splenic vein to the left renal vein).
Esophageal varices
Submucosal veins of the esophagus drain superiorly to the systemic system (through the azygos veins) and inferiorly to the portal system. When flow through the portal vein is obstructed (as in portal hypertension), these portosystemic anatomoses allow blood in the lower esophagus to drain to the systemic veins. The esophageal varices, enlarged veins that result from this increased flow, can rupture, causing severe hemorrhaging.
8.2c Lymphatic Drainage of the Abdomen
Lymph vessels from the abdominal walls and viscera usually accompany the arteries that supply those regions and ultimately drain to the chyle cistern (if present) or the thoracic duct.
– The cisterna chyli (chyle cistern) is an elongated, lobulated, thin-walled dilation that, when present, gives rise to the thoracic duct. It lies to the right of the T12 vertebral body and receives the lumbar and intestinal trunks (see Fig. 1.20).
– Groups of lumbar lymph nodes drain all of the abdominal viscera (except a small hepatic segment) and most of the abdominal wall (Fig. 8.19; Table 8.6).
• Preaortic nodes, which lie anterior to the abdominal aorta, receive lymph from the gastrointestinal tract (as far as the midrectum) and associated organs. Nodes surrounding the base of the major arteries form preterminal groups, such as the superior and inferior mesenteric nodes. These drain to celiac nodes, which drain to intestinal lymph trunks.
• Lateral aortic nodes (right and left lumbar nodes) lie along the medial border of the psoas muscles, the crura of the diaphragm, and along the inferior vena cava. They drain the abdominal and pelvic walls and the viscera of the retroperitoneum, including the ovaries and testes, and receive lymph from the common iliac nodes, which drain the pelvic viscera and the lower limb. Drainage from these lateral aortic nodes forms a lumbar trunk on each side.
• Retroaortic nodes that lie behind the aorta are considered peripheral nodes of the lateral aortic group and have no specific area of drainage.
• Common iliac nodes drain organs of the pelvis and the lower limbs.
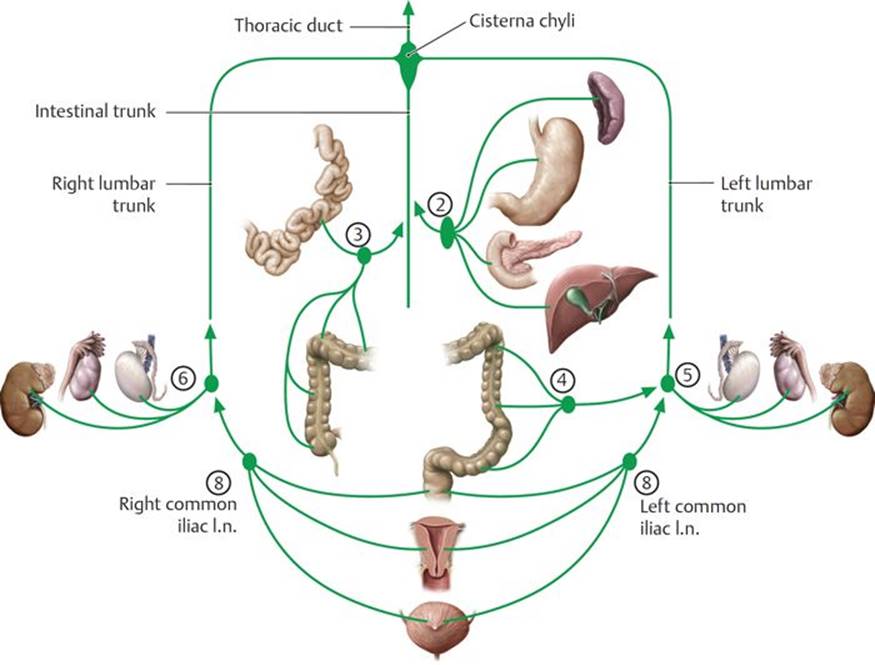
Fig. 8.19 ![]() Lymphatic drainage of the internal organs of the abdomen and pelvis
Lymphatic drainage of the internal organs of the abdomen and pelvis
See Table 8.6 for numbering. Lymph drainage from the abdomen, pelvis, and lower limb ultimately passes through the lumbar lymph nodes (clinically: aortic nodes). The lumbar lymph nodes consist of the right (caval) and left lateral aortic nodes, the preaortic nodes, and the retroaortic nodes. Efferent lymph vessels from the lumbar and preaortic nodes form the lumbar and intestinal trunks, respectively. The lumbar and intestinal trunks terminate in the cisterna chyli.
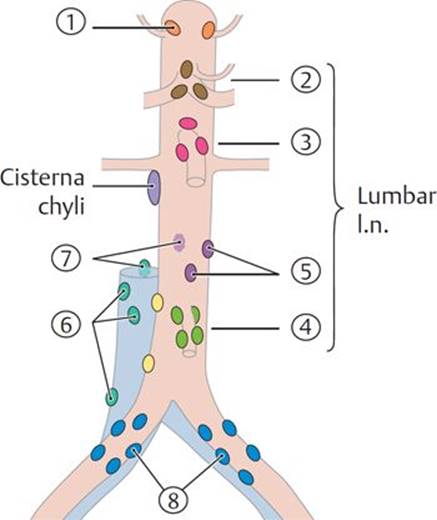
TABLE 8.6 ![]() Lymph Nodes of the Abdomen
Lymph Nodes of the Abdomen
|
|
||
|
Lumbar I.n. |
Preaortic I.n. |
|
|
|
||
|
|
||
|
|
||
|
|
||
|
|
||
|
|
||
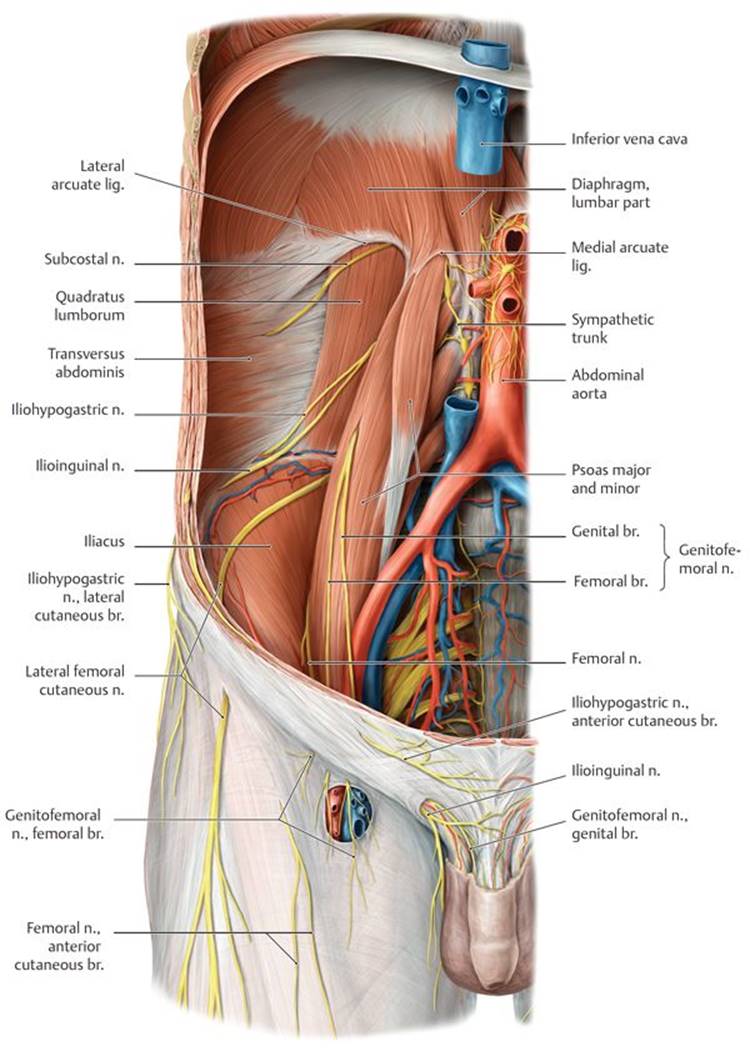
Fig. 8.20 ![]() Nerves of the lumbar plexus
Nerves of the lumbar plexus
Anterior view.
A Lumbar plexus in situ.
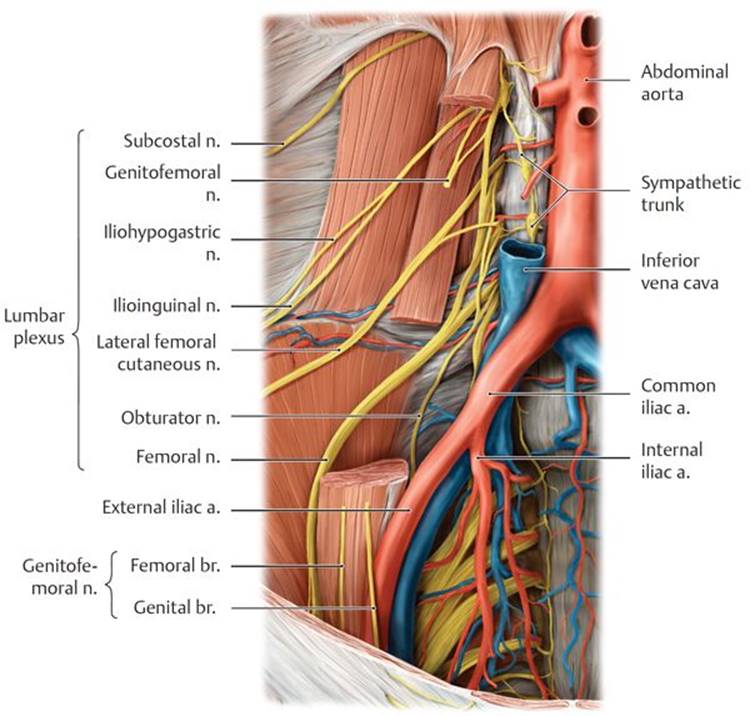
B Lumbar plexus dissection. Windowed: psoas major.
8.2d Nerves of the Abdomen
– Lower intercostal nerves (T7–T11) and the subcostal nerve (T12) continue anteroinferiorly from their position on the thoracic wall to innervate most of the muscles and skin of the anterolateral abdominal wall.
– The nerves of the lumbar plexus, a somatic nerve plexus formed by the anterior rami of spinal nerves T12–L4, emerge from the psoas major muscle on the posterior abdominal wall (Fig. 8.20A and B). Most nerves of this plexus innervate the lower limb (see Section 15.4d and Table 15.1). Branches that innervate the abdominal wall and inguinal region include the
• iliohypogastric and ilioinguinal nerves (L1), which innervate the skin and muscles of the inferior anterior abdominal wall and the skin over the inguinal and pubic regions;
• genitofemoral nerve (L1–L2), whose genital branch innervates the cremaster muscle surrounding the spermatic cord and the skin over the scrotum and labia; and
• short muscular branches (T12–L4) that innervate the muscles of the posterior abdominal wall.
– Lumbar sympathetic trunks, the continuations of the sympathetic trunks in the thorax, descend along the lateral aspect of the lumbar vertebral bodies and give off three to four lumbar splanchnic nerves, which join the autonomic plexuses of the abdomen.
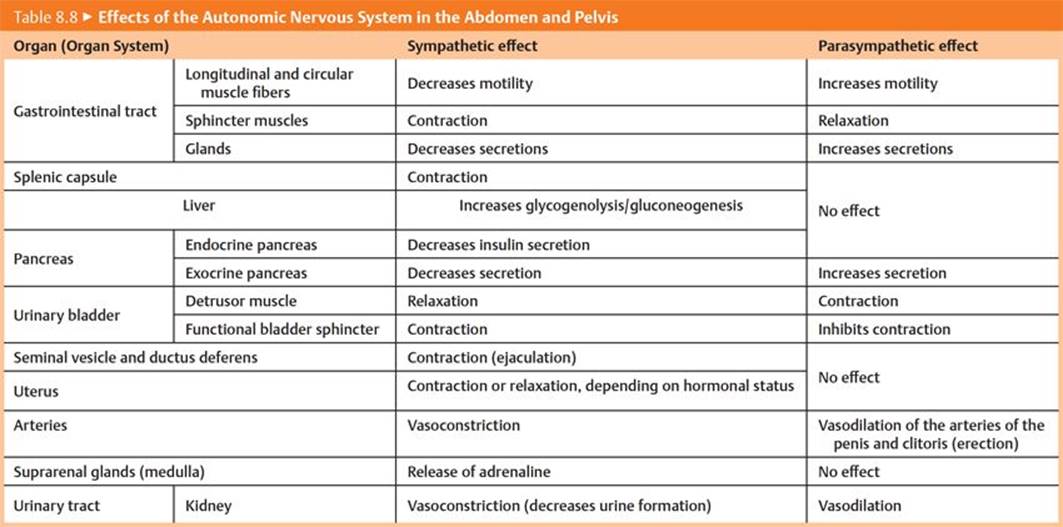
– Autonomic plexuses form along the aorta and travel with the major abdominal arteries to innervate the abdominal viscera (Fig. 8.21 and Table 8.7; Fig. 8.22 and Table 8.8). The plexuses contain
• preganglionic sympathetic nerves that synapse in the ganglia associated with the plexuses. (Note that the sympathetic nerves innervating the adrenal medulla are an exception and do not synapse in these ganglia.) The preganglionic sympathetic nerves arise from
○ thoracic splanchnic nerves (T5–T12) and
○ lumbar splanchnic nerves (T11–L2).
• preganglionic parasympathetic nerves, which pass through the plexuses and synapse in ganglia near their target organ. They arise from
○ the vagus nerves (CN X), which enter the abdomen as anterior and posterior vagal trunks from the esophageal plexus. They supply most of the abdominal viscera, including the digestive tract, except for its most distal segment (the descending colon to the anal canal).
○ pelvic splanchnic nerves (S2–S4), which ascend from the pelvis to innervate the descending and sigmoid colons in the abdomen. They also innervate viscera of the pelvis.
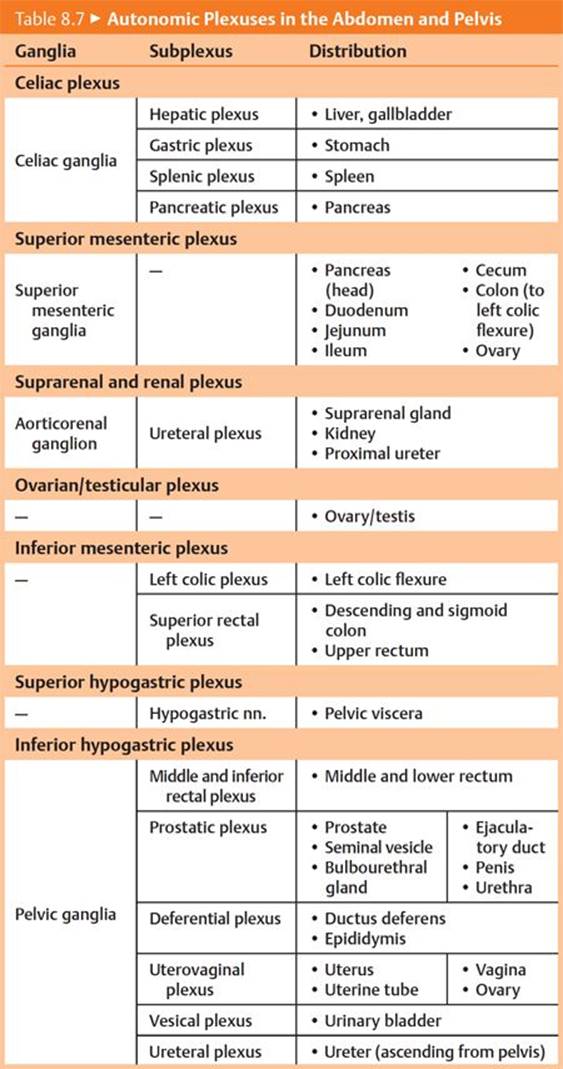
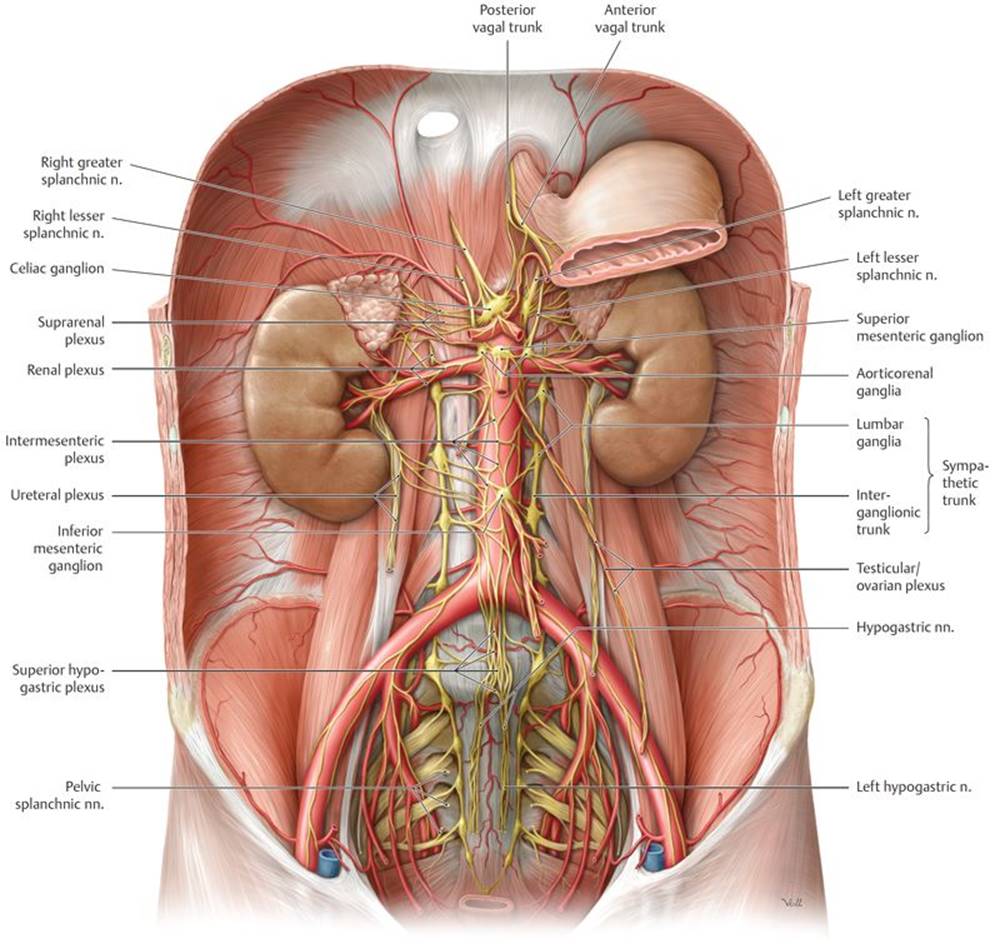
Fig. 8.21 ![]() Autonomic plexuses in the abdomen and pelvis
Autonomic plexuses in the abdomen and pelvis
Anterior view of the male abdomen. Removed: Peritoneum and majority of the stomach.
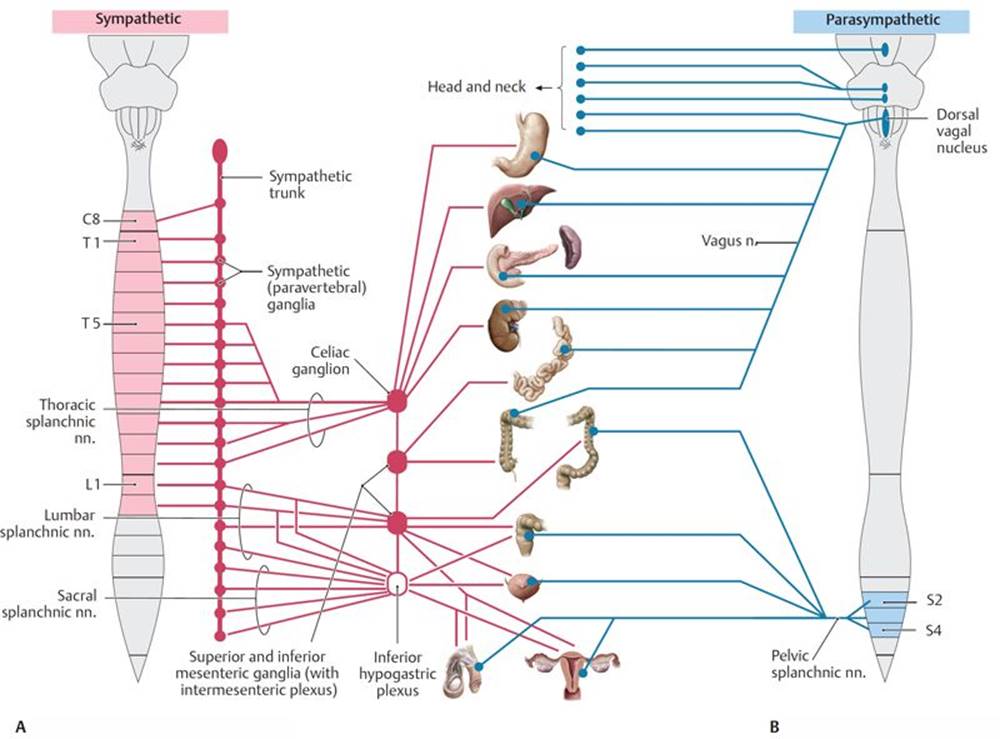
Fig. 8.22 ![]() Sympathetic and parasympathetic nervous systems in the abdomen and pelvis
Sympathetic and parasympathetic nervous systems in the abdomen and pelvis
A Sympathetic nervous system.
B Parasympathetic nervous system.