The extensor compartment is occupied by the triceps muscle and has the radial nerve and profunda artery running through it. The ulnar nerve passes through the lower part of this compartment.
Triceps
The three heads of this muscle are named long, lateral and medial. The long head arises from the infraglenoid tubercle at the upper end of the axillary border of the scapula. The lateral head has a linear origin (Fig. 2.17) from the back of the humerus, above the groove for the radial nerve, extending up to the surgical neck. The long and lateral heads converge and fuse to form the superficial lamina of the triceps tendon. The medial head arises from the whole of the back of the humerus below the radial groove (Fig. 2.17), and from both intermuscular septa. The medial head is deep to the other two heads and forms the deep lamina of the tendon. Both laminae blend above the elbow and are attached to the upper surface of the olecranon. A few fibres are inserted into the posterior part of the capsule of the elbow joint.
Nerve supply. By the radial nerve (C7, 8). The long and medial heads are supplied by branches given off from the radial nerve in the axilla. In the humeral groove the nerve supplies the lateral head and gives another branch to the medial head, which supplies the anconeus as well. Fractures of the middle of the shaft of the humerus, even though they may damage the radial nerve, are not likely to cause paralysis of triceps because of the high origin of nerve branches.
Action. The muscle is the extensor of the elbow joint. The long head supports the capsule of the shoulder joint when the arm is abducted, and it aids in extending the shoulder joint.
Test. The flexed forearm is extended against resistance and the muscle seen and felt.
Radial nerve
Leaving the axilla as described on page 55, the nerve passes obliquely across the back of the humerus from medial to lateral in a shallow groove between the long and medial heads of triceps, with the profunda brachii artery. The nerve then pierces the lateral intermuscular septum to enter the anterior compartment and runs towards the elbow between brachialis medially and first brachioradialis and then extensor carpi radialis longus laterally (Fig. 2.29). While in the axilla the nerve gives branches to the long and medial heads of triceps and the posterior cutaneous nerve of the arm. At the back of the humerus the radial nerve supplies the lateral head and the medial head again, the branch to the latter supplying anconeus as well. It also gives the lower lateral cutaneous nerve of the arm and the posterior cutaneous nerve of the forearm, which perforate the lateral head. In the anterior compartment of the arm the radial nerve gives branches to brachioradialis, extensor carpi radialis longus and the lateral part of brachialis. The nerve divides into its terminal superficial branch and the posterior interosseous nerve at the level of the lateral epicondyle. It also supplies the elbow joint.
The surface marking of the nerve is from the point where the posterior wall of the axilla and arm meet to a point two-thirds of the way along a line from the acromion to the lateral epicondyle, and thence to the front of the epicondyle.
Ulnar nerve
The nerve courses through the lower part of the extensor compartment and disappears into the forearm by passing between the humeral and ulnar heads of origin of flexor carpi ulnaris (Fig. 2.33). It lies in contact with the bone in the groove behind the base of the medial epicondyle, then lies against the medial ligament of the elbow joint, which it supplies (Fig. 2.25).
Elbow joint
This is a synovial joint of the hinge variety between the lower end of the humerus and the upper ends of radius and ulna (Fig. 2.23). It communicates with the proximal radioulnar joint.
|
|
|
Figure 2.23 Radiographs of the elbow joint: A anteroposterior projection; B lateral projection. (Provided by Dr R. Sinnatamby, Addenbrooke's Hospital, Cambridge.) |
The lower end of the humerus has the prominent conjunction of capitulum and trochlea (Fig. 2.24). The capitulum is a portion of a sphere which articulates with the upper surface of the head of the radius. It projects forwards and downwards, and is not visible on the posterior aspect of the humerus (Fig. 2.55). In contrast the trochlea, which lies medial, is a grooved surface that extends around the lower end of the humerus to the posterior surface of the bone and articulates with the trochlear notch of the ulna. The groove of the trochlea is limited medially by a sharp ridge that extends further distally. Laterally a blunter ridge blends with the articular surface of the capitulum more proximally. Thus a tilt is produced at the lower end of the humerus that accounts in part for the carrying angle of the elbow. Fossae immediately above the capitulum and trochlea receive the head of the radius and coronoid process of the ulna, respectively, in full flexion; posteriorly a deep fossa receives the olecranon in full extension.
|
|
|
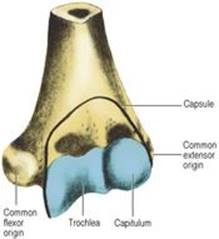
Figure 2.24 Lower end of the left humerus, showing the line of attachment of the capsule of the elbow joint. |
The upper surface of the cylindrical head of the radius is spherically concave to fit the capitulum.
The upper end of the ulna shows the deep trochlear notch. A curved ridge crosses the notch connecting the prominences of coronoid process and olecranon (Fig. 2.57); the ridge fits the groove in the trochlea of the humerus. The obliquity of the shaft of the ulna to this ridge accounts for most of the carrying angle at the elbow.
The capsule is attached to the humerus at the medial and lateral margins of the trochlea and capitulum, respectively, but in front it is attached above the coronoid and radial fossae (Fig. 2.24), and at the back above the olecranon fossa. Distally, the capsule is attached to the margins of the trochlear notch of the ulna, and to the annular ligament of the proximal radioulnar joint (Fig. 2.26). It is not attached to the radius.
The capsule and lower part of the annular ligament are lined with synovial membrane, which is attached to the articular margins of all three bones. The synovial membrane thus lines the fossae on the lower end of the humerus. The quadrate ligament, which is attached to the lower margin of the radial notch of the ulna and the neck of the radius, prevents downward herniation of the synovial membrane between the anterior and posterior free edges of the annular ligament.
The ulnar collateral (medial) ligament of the elbow joint is triangular and consists of three bands. The anterior band is the strongest. It passes from the medial epicondyle of the humerus to a small tubercle (previously called the sublime tubercle) on the medial border of the coronoid process. The posterior band joins the sublime tubercle and the medial border of the olecranon. A thin middle band connects these two and its grooved surface lodges the ulnar nerve on its way from the arm to the forearm (Fig. 2.25). The radial collateral (lateral) ligament (Fig. 2.26) is a triangular band. Its apex is attached to the lateral epicondyle and its base fuses with the annular ligament of the head of the radius. The anterior and posterior ligaments are merely thickened parts of the capsule. The annular ligament is attached to the anterior and posterior margins of the radial notch of the ulna, and clasps the head and neck of the radius in the proximal radioulnar joint. It has no attachment to the radius, which remains free to rotate in the annular ligament.
|
|
|
Figure 2.25 Left elbow joint from the medial side, with the ulnar nerve lying against the ulnar collateral (medial) ligament. |
|
|
|
Figure 2.26 Radial collateral (lateral) ligament of the left elbow joint, passing from the lateral epicondyle to the annular ligament. |
|
|
|
Figure 2.27 Superficial muscles of the flexor compartment of the left forearm. Brachioradialis has been retracted laterally to show the radial nerve and its posterior interosseous branch, and the brachial artery and median nerve have been displaced medially to show the insertion of brachialis behind biceps. |
Nerve supply. By the musculocutaneous, median, ulnar and radial nerves.
Movements
The only appreciable movement possible at the elbow joint is the simple hinge movement of flexion and extension. From the straight (extended) position the range of flexion is about 140°. This movement does not take place in the line of the humerus, for the axis of the hinge lies obliquely. The extended ulna makes an angle of about 170° with the humerus, the forearm diverging laterally. This so-called ‘carrying angle’ fits the elbow into the waist when the arm is at the side, and it is significant that the obliquity of the ulna is more pronounced in women than in men. However, the line of upper arm and forearm becomes straightened out when the forearm is in the usual working position of almost full pronation (Fig. 2.32). A pathological increase in this ‘valgus’ angle (e.g. from a fractured lateral epicondyle or damaged epiphysis) may gradually stretch the ulnar nerve behind the medial epicondyle and cause an ulnar nerve palsy. The ulnar nerve can also be compressed in the cubital tunnel formed by the tendinous arch connecting the humeral and ulnar heads of flexor carpi ulnaris (see p. 66). This condition may require division of the aponeurotic ulnar origin of the muscle and anterior submuscular transposition of the nerve. In extension the tip of the olecranon lies in line with the humeral epicondyles, but in full flexion these three bony points make an equilateral triangle. This relationship is disrupted in dislocation of the elbow joint. Posterior displacement of the forearm bones at the elbow is usually associated with fracture of the coronoid process. The brachial artery, median and ulnar nerves may be damaged by such an injury. In children the brachial artery and median nerve are at risk in supracondylar fracture of the humerus from forward displacement of the proximal fragment.
Surgical approach
There are several approaches to the elbow joint. A posterior approach is made through a vertical incision which skirts the tip of the olecranon. The ulnar nerve is identified behind the medial epicondyle and protected. An osteotomy detaches the olecranon which is displaced proximally with the triceps insertion. At the conclusion of the procedure the olecranon is reattached with a screw. For a medial approach the ulnar nerve is displaced backwards and the common flexor origin detached to expose the capsule, while on the lateral side the common extensor origin can be similarly detached. On this side the capsule incision must not extend lower than the level of the head of the radius to avoid damage to the posterior interosseous nerve as it winds round the shaft within the supinator.
For aspiration or injection the needle is inserted on the posterolateral side above the head of the radius, with the elbow at a right angle. The same route provides the portal used for initial distension of the elbow joint at arthroscopy.