The flexor muscles in the forearm are arranged in two groups, superficial and deep. The five muscles of the superficial group cross the elbow joint; the three muscles of the deep group do not. The flexor compartment is much more bulky than the extensor compartment, for the necessary power of the grip.
Superficial muscles
These five muscles (Fig. 2.27) are distinguished by the fact that they possess a common origin from the medial epicondyle of the humerus. Three of the group have additional areas of origin. The common origin is attached to a smooth area on the anterior surface of the medial epicondyle (Fig. 2.24).
With the heel of the hand placed over the opposite medial epicondyle, palm lying on the forearm, the digits point down along the five superficial muscles: thumb for pronator teres; index for flexor carpi radialis; middle finger for flexor digitorum superficialis; ring finger for palmaris longus; and little finger for flexor carpi ulnaris.
Pronator teres
Arising from the common origin and from the lower part of the medial supracondylar ridge, the main superficial belly is joined by the small deep head, which arises from the medial border of the coronoid process of the ulna just distal to the tubercle on it. The median nerve lies between the two heads and the ulnar artery passes deep to the deep head (Fig. 2.29). The muscle, forming the medial border of the cubital fossa (Fig. 2.27), runs distally across the front of the forearm to be inserted by a flat tendon into the middle of the lateral surface of the shaft of the radius at the most prominent part of its outward convexity.
Nerve supply. By the first (highest) muscular branch of the median nerve (C6, 7).
Action. The muscle pronates the forearm and is a weak flexor of the elbow.
Test. From the supine position the forearm is pronated against resistance and the muscle palpated at the medial margin of the cubital fossa.
Flexor carpi radialis
Arising from the common origin the fleshy belly gives way in the middle of the forearm to a long tendon (Fig. 2.27) that runs through its own compartment in the carpal tunnel (see p. 81), lying in the groove of the trapezium, and is inserted into the bases of the second and third metacarpals (symmetrically with extensors longus and brevis). The tendon is a prominent landmark towards the radial side of the front of the wrist. The radial artery lies lateral to the tendon, and the median nerve (with the overlying tendon of palmaris longus) medial to it.
Nerve supply. By the median nerve (C6, 7).
Action. It is a flexor and radial abductor of the wrist. It is an important stabilizer of the wrist in finger and thumb movements.
Test. The wrist is flexed and abducted against resistance and the tendon is easily seen and felt.
Flexor digitorum superficialis
The muscle arises from the common origin, the medial ligament of the elbow joint, and the tubercle on the medial border of the coronoid process of the ulna (humeroulnar head). As this muscle was previously called flexor digitorum sublimis, this tubercle was known as the sublime tubercle. A fibrous arch continues the origin across to the radius, where it arises from the whole length of the anterior oblique line (radial head) (Fig. 2.56). The fleshy belly is partly hidden above by the other superficial flexors, and is therefore frequently described as being in an intermediate layer. Its oblique origin, in continuity from the medial epicondyle to the insertion of pronator teres, forms the upper limit of the space of Parona (see p. 69). Above the wrist the tendons of this muscle appear on each side of the palmaris longus tendon. As the tendons pass beneath the flexor retinaculum, the middle and ring finger tendons lie superficial to those to the index and little finger (Fig. 2.39). Their insertion into the middle phalanges of the fingers is considered on page 89. In the forearm the muscle belly has the median nerve plastered to its deep surface by areolar tissue (Fig. 2.28).
|
|
|
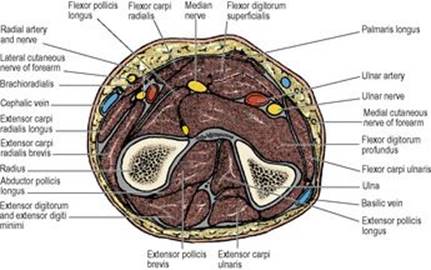
Figure 2.28 Cross-section through the middle of the right forearm, looking towards the elbow. The median nerve adheres to the deep surface of flexor digitorum superficialis, and the ulnar artery is under cover of the muscle more medially. The ulnar nerve is overlapped by flexor carpi ulnaris. The superficial branch of the radial nerve and the radial artery are under cover of brachioradialis. The deep (posterior interosseous) branch of the radial nerve has divided above this level to supply extensor muscles. The anterior interosseous nerve and vessels lie between flexor pollicis longus and flexor digitorum profundus. |
Nerve supply. By the median nerve (C7, 8).
Action. It is a flexor of the proximal interphalangeal joints, and secondarily of the metacarpophalangeal and wrist joints. It also assists in flexion of the elbow and wrist.
Test. The fingers are flexed at the proximal interphalangeal joints against resistance applied to the middle phalanges, while the distal interphalangeal joints are kept extended.
Palmaris longus
The muscle arises from the common origin. It is absent on one or both sides in about 13% of people. Its long, flat tendon broadens as it passes in front of the flexor retinaculum, to which it is partly adherent (Fig. 2.27). In the palm it splits to form the longitudinally directed fibres of the palmar aponeurosis (see p. 80). The tendon lies in front of the median nerve just above the wrist.
Nerve supply. By the median nerve (C7, 8).
Action. It is a weak flexor of the wrist, and anchors the skin and fascia of the hand against shearing forces in a distal direction. The tendon can be used in tendon transplant procedures.
Test. The wrist is flexed and the tendon palpated when the pads of the thumb and little finger are pinched together.
Flexor carpi ulnaris
The muscle arises from the common origin and by a wide aponeurosis from the medial border of the olecranon and the upper two-thirds of the subcutaneous border of the ulna (Fig. 2.33). The ulnar nerve passes under the tendinous arch between the humeral and ulnar heads of this muscle to enter the flexor compartment of the forearm, where the ulnar nerve and artery are overlapped by the muscle (Fig. 2.28). At the wrist the tendon of the muscle is medial to the nerve and artery. The tendon inserts into the pisiform (a sesamoid bone in the tendon) and, by way of the pisohamate and pisometacarpal ligaments, into the hamate and fifth metacarpal bones.
Nerve supply. By the ulnar nerve (C7, 8).
Action. It is a flexor and an ulnar adductor of the wrist. In radial nerve paralysis the tendon can be transplanted to extend the fingers or thumb.
Test. The wrist is flexed and adducted against resistance and the tendon palpated.
Cubital fossa
The cubital fossa is the triangular area between pronator teres, brachioradialis and a line joining the humeral epicondyles (Fig. 2.29). The roof is formed by the deep fascia of the forearm, reinforced on the medial side by the bicipital aponeurosis. In front of the bicipital aponeurosis lies the median cubital vein with the medial cutaneous nerve of the forearm (Fig. 2.22); the aponeurosis separates these structures from the underlying median nerve and brachial artery. The floor is formed in the main by the brachialis muscle and below by the supinator (Fig. 2.30).
|
|
|
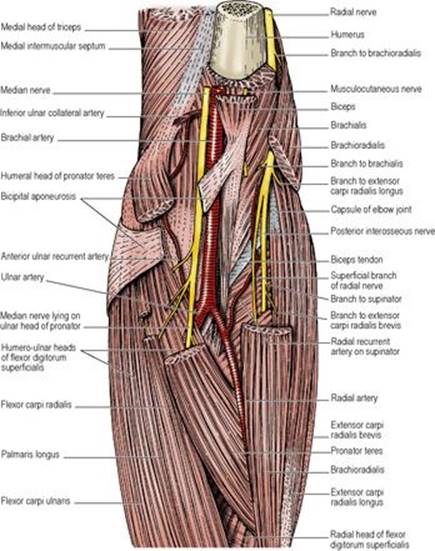
Figure 2.29 Left cubital fossa. The bicipital aponeurosis has been partly removed. The lateral cutaneous nerve of the forearm is seen emerging from deep to the lateral border of biceps. |
The contents of the fossa, from medial to lateral side, are the median nerve, brachial artery, tendon of biceps, and farther laterally the radial nerve and its posterior interosseous branch, which are only seen when brachioradialis is retracted laterally (Fig. 2.29). The artery is palpated here medial to the tendon to define the position for placing the stethoscope when taking the blood pressure. The further courses of the brachial artery and median nerve are discussed below (see pp. 69 and 72). The branches of the radial nerve in the cubital fossa have been described on page 61. The posterior interosseous nerve gives branches to extensor carpi radialis brevis and supinator before disappearing from the fossa by passing between the two layers of the supinator muscle (Figs 2.27 and 2.29) into the extensor compartment (see p. 73). The superficial branch of the radial nerve passes down the forearm under cover of the brachioradialis (see p. 73).
Deep muscles
The group consists of flexor digitorum profundus, flexor pollicis longus and pronator quadratus (Fig. 2.30).
Flexor digitorum profundus
The most powerful and the bulkiest of the forearm muscles, it arises by fleshy fibres from the medial surface of the olecranon (Fig. 2.25), from the upper three-quarters of the anterior and medial surfaces of the ulna, including its subcutaneous border, and from the interosseous membrane. The tendon for the index separates in the forearm; the three other tendons are still partly attached to each other as they pass across the carpal bones in the flexor tunnel and do not become detached from each other until they reach the palm (Fig. 2.30), where they give origin to the four lumbricals. Their insertion into the distal phalanges is described on page 89.
Nerve supply. By the anterior interosseous branch of the median nerve and by the ulnar nerve (C8, T1). Characteristically, these nerves equally share the bellies, those that merge into the tendons for the index and middle fingers being supplied from the median, and for the ring and little fingers from the ulnar nerves. The corresponding lumbricals are similarly supplied.
This distribution of 2:2 between median and ulnar nerves occurs in only 60% of individuals. In the remaining 40% the median and ulnar distribution is 3:1 or 1:3 equally (20% each). Whatever the variation, however, the rule is that each lumbrical is supplied by the same nerve which innervates the belly of its parent tendon.
Action. It flexes the terminal interphalangeal joints and, still acting, rolls the fingers and wrist into flexion. It is the great gripping muscle. Extension of the wrist is indispensable to the full power of contraction of the muscle.
Test. With the fingers extended and the hand lying supine on the table, the distal interphalangeal joints are flexed against resistance with the middle phalanx held in extension.
Flexor pollicis longus
This muscle arises from the anterior surface of the radius below the anterior oblique line and above the insertion of pronator quadratus, and from the interosseous membrane. The tendon forms on the ulnar side of this unipennate muscle and receives fleshy fibres into its radial side down to just above the wrist, a distinctive feature which facilitates identification of the tendon (Fig. 2.30). The tendon passes in the carpal tunnel deep to that of the flexor carpi radialis, then spirals around its ulnar side to become superficial. It extends into the thumb to be inserted into the base of the distal phalanx.
|
|
|
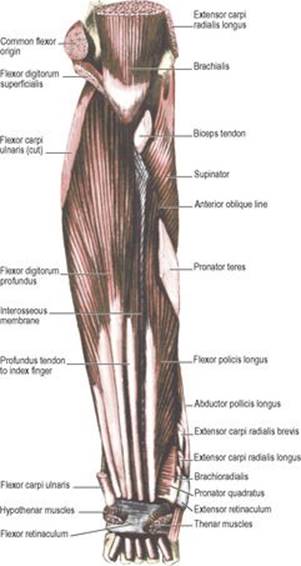
Figure 2.30 Deep muscles of the flexor compartment of the left forearm. The flexor retinaculum remains in place at the wrist. The radial head of flexor digitorum superficialis and the common extensor origin attached to the lateral epicondyle of the humerus have been removed. |
Nerve supply. By the anterior interosseous branch of the median nerve (C7, 8).
Action. It is the only flexor of the interphalangeal joint of the thumb, and also flexes the metacarpophalangeal and carpometacarpal joints of the thumb and the wrist joint.
Test. With the proximal phalanx of the thumb held steady, the distal phalanx is flexed against resistance.
Pronator quadratus
Arising from the ridge on the anteromedial aspect of the distal ulna, the muscle is inserted into the anterior surface of the lower fourth of the radius (Fig. 2.56), and into the triangular area above the ulnar notch.
Nerve supply. By the anterior interosseous branch of the median nerve (C7, 8).
Action. The muscle pronates the forearm and helps to hold the lower ends of the radius and ulna together, especially when the hand is weight-bearing. As a pronator it is more powerful than pronator teres.
Space of Parona
In front of pronator quadratus there is a space (of Parona) deep to the long flexor tendons of the fingers and their synovial sheaths. The space is limited proximally by the oblique origin of flexor digitorum superficialis. The space becomes involved in proximal extensions of synovial sheath infections; it can be drained through radial and ulnar incisions to the side of the flexor tendons.
Neurovascular pattern in the forearm
The general arrangement of the deep arteries and nerves of the forearm is that a nerve runs down each border of the forearm (radial and ulnar nerves), and the brachial artery divides into branches (radial and ulnar arteries) that run down to approach these nerves but do not cross them. The radial artery lies medially beside the radial nerve in the middle third, and the ulnar artery lies laterally beside the ulnar nerve in the distal two-thirds of the forearm. The median nerve, on the deep surface of flexor superficialis, crosses the ulnar artery to lie between the two arteries. Radial and ulnar arteries supply the hand; they run down into deep and superficial palmar arches. The arterial supply for the forearm comes from the common interosseous branch of the ulnar, which divides into posterior and anterior interosseous arteries. The posterior interosseous artery is rather a failure. Assisted at first by branches of the anterior interosseous that pierce the interosseous membrane, it later fails and is replaced by the anterior interosseous artery, which pierces the membrane to enter the extensor compartment. Anterior (from median) and posterior (from radial) interosseous nerves, on the other hand, remain in their own compartments right down to the wrist, supplying muscles; neither nerve reaches the skin.
Three nerves share in the supply of the muscles of the forearm and each nerve passes between the two heads of a muscle. The median nerve passes between the two heads of pronator teres and the ulnar nerve between the two heads of flexor carpi ulnaris. These two nerves share in the supply of the muscles of the flexor compartment. The muscles of the extensor compartment are supplied by the posterior interosseous nerve, which enters the compartment by passing between the two layers of the supinator muscle.
Vessels of the flexor compartment
The brachial artery enters the forearm by passing into the cubital fossa in the midline; halfway down the fossa (at the level of the neck of the radius) it divides into radial and ulnar arteries (Fig. 2.29). The radial usually appears to be the direct continuation of the brachial artery, whereas the bigger ulnar branches off at an angle (Fig. 2.31). Sometimes the brachial artery divides into its radial and ulnar branches more proximally.
|
|
|
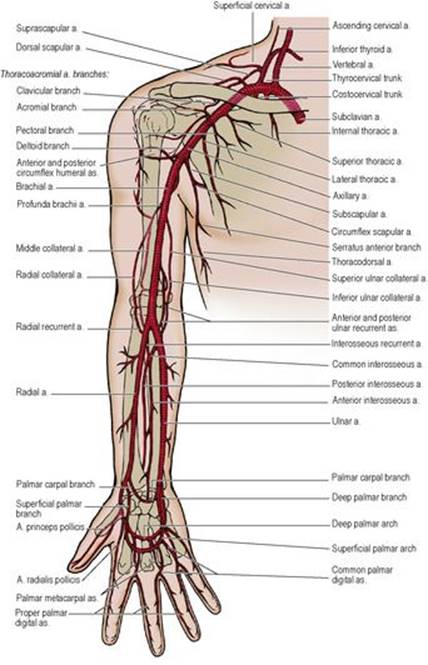
Figure 2.31 Arteries of the upper limb. |
Radial artery
The radial artery passes distally medial to the biceps tendon, across the supinator, over the tendon of insertion of the pronator teres, the radial head of flexor digitorum superficialis, the origin of the flexor pollicis longus, the insertion of pronator quadratus and the lower end of the radius (against which its pulsation can be readily felt). It disappears deep to the tendons of abductor pollicis longus and extensor pollicis brevis to cross the anatomical snuff box (Fig. 2.35). In the upper part of the forearm it is overlapped anteriorly by brachioradialis (Fig. 2.27). Distally it is covered only by skin and by superficial and deep fascia.
The surface marking of the artery is along a line, slightly convex laterally, from medial to the biceps tendon in the cubital fossa to medial to the styloid process of the radius. It can be surgically exposed at its lower end which is the most common site for arterial cannulation.
Ulnar artery
The ulnar artery disappears from the cubital fossa by passing deep to the deep head of pronator teres and beneath the fibrous arch of the flexor digitorum superficialis and the median nerve (Fig. 2.29). It then runs medially and distally on flexor digitorum profundus with the ulnar nerve to its ulnar side and passes down over the front of the wrist into the palm, where it lies in front of the flexor retinaculum and continues as the superficial palmar arch (see p. 81). Ulnar artery pulsation can be felt on the radial side of the tendon of flexor carpi ulnaris just above the pisiform bone.
The surface marking is along a line, slightly convex medially, from medial to the biceps tendon in the cubital fossa to the radial side of the pisiform. It can be surgically exposed at the lower end and followed upwards by displacing flexor carpi ulnaris. The ulnar nerve on the ulnar side of the artery must be safeguarded.
Its chief branch is the common interosseous (Fig. 2.31), which divides into anterior and posterior interosseous branches. The anterior interosseous artery lies deeply on the interosseous membrane between flexor digitorum profundus and flexor pollicis longus, supplying each. Perforating branches pierce the interosseous membrane to supply the deep extensor muscles. Nutrient vessels are given to both radius and ulna. The artery passes posteriorly through the interosseous membrane at the level of the upper border of pronator quadratus.
The posterior interosseous artery disappears by passing backwards through the interosseous space between the upper end of the interosseous membrane and the oblique cord (see p. 72).
Anastomosis around the elbow joint
Recurrent branches, in some cases double, arise from radial, ulnar and interosseous arteries and run upwards both anterior and posterior to the elbow joint, to anastomose with the radial and middle collateral branches of the profunda brachii, and the superior and inferior ulnar collateral arteries (see p. 59 and Fig. 2.31).
Anastomosis around the wrist joint
Both radial and ulnar arteries give off palmar and dorsal carpal branches. These anatomose with each other deep to the long tendons, forming the palmar and dorsal carpal arches. The palmar carpal arch lies transversely across the wrist joint (Fig. 2.31); it supplies the carpal bones and sends branches distally into the hand to anastomose with the deep palmar arch. The dorsal carpal arch lies transversely across the distal row of carpal bones. It sends dorsal metacarpal arteries distally into each metacarpal space and these divide to supply the fingers; they anastomose through the interosseous spaces with the deep palmar arch and the digital branches of the superficial palmar arch. Thus a free anastomosis is established between radial and ulnar arteries through the carpal and palmar arches.
Veins of the forearm
The deep veins are plentiful and accompany the arteries, usually by dual venae comitantes which anastomose freely with each other. They drain the forearm but bring relatively little blood from the hand.
Most of the blood from the palm of the hand passes through to a superficial venous network on the dorsum. From the radial side of this arch the cephalic vein begins in the roof of the anatomical snuffbox and runs up along the lateral border of the limb (Fig. 2.22). It runs in the upper arm lateral to biceps, to the deltopectoral groove, and perforates the clavipectoral fascia to drain into the axillary vein. From the ulnar side of the dorsal venous arch the basilic vein runs up the medial border of the limb. It pierces the deep fascia halfway between elbow and axilla (Fig. 2.22) and becomes the axillary vein at the lower border of teres major.
The median forearm vein drains subcutaneous tissue of the front of the wrist and forearm. It ascends to join the median cubital or basilic vein. Commencing distal to the elbow, the median cubital vein runs proximomedially from the cephalic to the basilic veins. It lies superficial to the bicipital aponeurosis, but has a communication with the deep veins. There are frequent variations from the standard venous patterns just described.
Lymphatics of the forearm
As elsewhere in the body the superficial lymphatics follow veins, the deep ones follow arteries. From the ulnar side of the hand and forearm the subcutaneous lymphatics run alongside the basilic vein to the supratrochlear nodes. From the radial side the lymphatics run alongside the cephalic vein to the infraclavicular nodes. From the deep parts of the hand and forearm and from the supratrochlear nodes lymphatics pass to the lateral group of axillary nodes (see p. 55).
Nerves of the flexor compartment
The lateral cutaneous nerve of the forearm, the cutaneous continuation of the musculocutaneous nerve, pierces the deep fascia above the elbow lateral to the tendon of biceps and supplies the anterolateral surface of the forearm, by anterior and posterior branches, as far distally as the thenar eminence (Fig. 2.49). The medial cutaneous nerve of the forearm pierces the deep fascia at the middle of the arm and divides into anterior and posterior branches. It supplies the skin of the front of the lower part of the arm and that of the front and back of the medial part of the forearm (Fig. 2.49).
The superficial terminal branch of the radial nerve, the cutaneous continuation of the main nerve, runs from the cubital fossa on the surface of supinator, pronator teres tendon and flexor digitorum superficialis, on the lateral side of the forearm under cover of brachioradialis. In the middle third of the forearm it lies beside and lateral to the radial artery. It then leaves the flexor compartment of the forearm by passing backwards deep to the tendon of brachioradialis and breaks up into two or three branches which can often be rolled on the surface of the tautened tendon of extensor pollicis longus. They are distributed to the radial two-thirds of the dorsum of the hand and the proximal parts of the dorsal surfaces of thumb and lateral two and a half or three and a half fingers (Fig. 2.36), but seepage 96 for the effects of nerve injury.
The median nerve leaves the cubital fossa between the two heads of pronator teres (Fig. 2.29). It passes deep to the fibrous arch of flexor digitorum superficialis and runs distally adherent to the posterior aspect of this muscle. Above the wrist the nerve comes closer to the surface between the tendons of flexor carpi radialis and flexor digitorum superficialis, lying behind and partly lateral to the tendon of palmaris longus (Fig. 2.27). Near the elbow the median nerve gives muscular branches, first to pronator teres and then to flexor carpi radialis, palmaris longus and flexor digitorum superficialis; the branch to the index finger part of this muscle, however, arises in the middle of the forearm. The nerve supplies the elbow and proximal radioulnar joints.
Deep to flexor digitorum superficialis, the median nerve gives off an anterior interosseous branch which runs down with the artery of the same name and supplies flexor digitorum profundus (usually the bellies which move index and middle fingers), flexor pollicis longus, pronator quadratus, and the inferior radioulnar, wrist and carpal joints.
In the distal forearm, above the flexor retinaculum, the median nerve gives off a palmar branch to the skin over the thenar muscles.
The surface marking of the nerve is along a line from a point in the middle of the cubital fossa medial to the brachial artery to a point at the wrist on the ulnar side of the tendon of flexor carpi radialis.
The ulnar nerve enters the forearm from the extensor compartment by passing between the humeral and ulnar heads of origin of flexor carpi ulnaris (Fig. 2.33). It is more easily compressed against the medial surface of the coronoid process than against the humerus, where it lies behind the medial epicondyle (Fig. 2.25). In the forearm the nerve lies under cover of the flattened aponeurosis of flexor carpi ulnaris, with the ulnar artery to its radial side along the distal two-thirds of the forearm. This neurovascular bundle lies on flexor digitorum profundus. Branches of supply are given to flexor carpi ulnaris and the ulnar half (usually) of flexor digitorum profundus. The branch to flexor carpi ulnaris contains C7 fibres brought to the ulnar nerve in the axilla (see p. 54) and C8 fibres; the branch to flexor digitorum profundus contains C8 and T1 fibres.
The ulnar nerve emerges from behind the tendon of flexor carpi ulnaris just proximal to the wrist (Fig. 2.27) and passes across the front of the flexor retinaculum in the hand. Before emerging it gives off a dorsal branch which passes medially between the tendon of flexor carpi ulnaris and the lower end of the ulna. The dorsal branch supplies the dorsum of the hand (Fig. 2.36) and of the ulnar one and a half fingers proximal to their nail beds. The small palmar cutaneous branch of the nerve pierces the deep fascia proximal to the flexor retinaculum, and supplies skin of the hypothenar eminence.
The surface marking of the nerve is along a line from the medial epicondyle of the humerus to the radial side of the pisiform bone.
Radioulnar joints
The superior radioulnar joint is a uniaxial synovial pivot joint between the circumference of the head of the radius and the fibro-osseous ring formed by the annular ligament (see p. 63) and the radial notch of the ulnar (Fig. 2.56). The articular inner aspect of the annular ligament is lined by hyaline cartilage. As has already been noted in connection with the elbow joint (see p. 62), the capsule and lateral ligament of the latter joint are attached to the annular ligament and both joints share the same synovial membrane. The membrane lines the intracapsular part of the radial neck and is supported below by the quadrate ligament.
The inferior radioulnar joint is a uniaxial synovial pivot joint between the convex head of the ulnar and the concave ulnar notch of the radius (Fig. 2.57). A triangular, fibrocartilaginous articular disc is attached by its base to the lower margin of the ulnar notch of the radius and by its apex to a fossa at the base of the ulnar styloid. The proximal surface of the disc articulates with the ulnar head. The synovial membrane of the joint projects proximally, as the recessus sacciformis, posterior to the pronator quadratus and anterior to the interosseous membrane.
The interosseous membrane connects the interosseous borders of the radius and ulna. Its fibres run from the radius distally to the ulna at an oblique angle.
The oblique cord is a flat band whose fibres run in opposite obliquity to those of the interosseous membrane; they slope proximally from just below the radial tuberosity to the side of the ulnar tuberosity. The posterior interosseous vessels pass through the gap between the oblique cord and the upper end of the interosseous membrane.
Nerve supplies. The proximal joint shares the nerve supply of the elbow joint (see p. 63), and the distal joint is supplied by the posterior interosseous and anterior interosseous nerves.
Movements
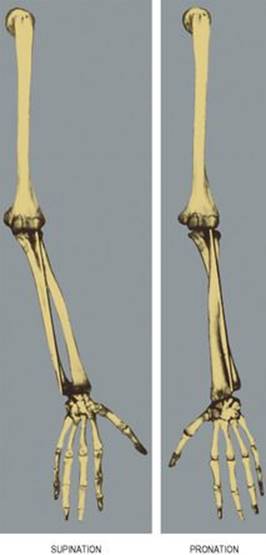
The movements of pronation and supination occur at the superior and inferior radioulnar joints. In full supination, the anatomical position, the radius lies lateral and parallel to the ulna. During pronation, while the head of the radius rotates within the fibro-osseous ring of the proximal joint, the distal radius rotates in front of and around the head of the ulna, carrying the hand with it; and in full pronation the shaft of the radius lies across the front of the ulna with the distal end of the radius medial to the ulnar head (Fig. 2.32). During supination these movements are reversed. The axis of movement of the radius relative to the ulna passes through the radial head and the ulnar styloid. But the ulnar is not usually entirely stationary during pronation and supination. The distal end of the ulna moves slightly posterolaterally in pronation and anteromedially in supination, these movements being effected by anconeus and the bicipital aponeurosis respectively. Supination is the more powerful action and account is taken of this in the design of screws, which are tightened by supination. Supination is carried out by the biceps and supinator, the former being the stronger provided the elbow is in the flexed position. The muscles producing pronation are principally pronator quadratus and pronator teres. About 140° of rotation occurs at the radioulnar joints during pronation–supination. Synchronous humeral rotation and scapular movement increases the range of rotation to nearly 360°.
|
|
|
Figure 2.32 The left limb bones are seen from the front and the axis of pronation–supination is indicated by the black lines. |