Cervical vertebrae
A typical cervical vertebra
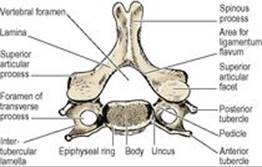
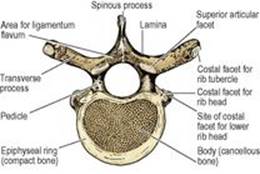
The broad kidney-shaped body is the same size as, or smaller than, the vertebral foramen (Fig. 6.87). On each side the lateral edge is projected up into a posterolateral lip or uncus, and its lower margin laterally is bevelled reciprocal with this. The anterior surface of the body is concave from above down. Basivertebral veins emerge from the posterior surface.
|
|
|
Figure 6.87 C6 vertebra from above. |
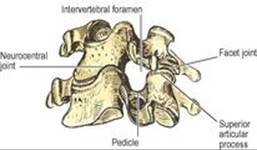
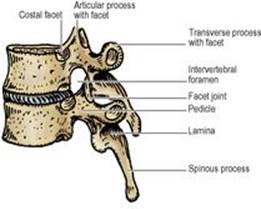
The pedicle is attached below the upturned lip on the body. Thus an intervertebral foramen in the neck is bounded in front by both vertebral bodies and the uncovertebral joint and disc between them (Fig. 6.88). Attached to the pedicle and body is the lateral projection of the transverse process, perforated by its foramen. The proximal part of the posterior bar of bone that projects from the pedicle behind the foramen is the true transverse element; it ends in the posterior tubercle, which is part of the costal element, as is the bar of bone that projects from the body in front of the foramen ends and in the anterior tubercle. The anterior tubercles enlarge progressively from C3 to C6. The large C6 anterior tubercle is the carotid tubercle (of Chassaignac) because the common carotid artery can be compressed against it. The anterior and posterior tubercles are joined by the intertubercular lamella, on the concave upper surface of which lies the anterior ramus of the cervical nerve of the same number (Fig. 6.87). The vertebral artery, with its accompanying sympathetic nerve fibres, and the vertebral venous plexus lie in the foramen of the transverse process, and the posterior root ganglion of the nerve of the same number lies behind it (Fig. 6.109).
|
|
|
Figure 6.88 C3 and C4 vertebrae articulated to show the boundaries of the intervertebral foramen. |
The laminae enclose a relatively large vertebral foramen, somewhat triangular in cross-section. At the junction of pedicle and lamina there are superior and inferior articular processes. The upper facets face obliquely up and back; the lower facets face down and forward.
The spinous process is usually bifid.
Atypical cervical vertebrae
The seventh cervical vertebra is often called the vertebra prominens because of its prominent spine. The vertebra is atypical in that its long spine is not bifid but ends in a rounded tubercle, and the foramen in the transverse process does not transmit the vertebral artery. The foramen is small, and contains the posterior vein when the vertebral vein is doubled. The anterior tubercle is very small; the suprapleural membrane is attached to it.
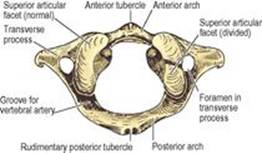
Some of the essential features of the atlas are described on page 425. Its distinctive feature is the lack of a body. The short anterior arch is projected into a tubercle in front (Fig. 6.89), for attachment of the anterior longitudinal ligament and longus colli. The longer posterior arch is grooved by the vertebral artery. The lateral mass carries the weight-bearing articular facets. The lateral mass is projected into the transverse process, which is perforated by the foramen. There are no anterior and posterior tubercles; but the blunt end of the transverse process represents a posterior tubercle and has corresponding muscle attachments: scalenus medius and levator scapulae. The atlas is the widest cervical vertebra, and the tip of its transverse process can be palpated with deep pressure behind the mandibular ramus, 1cm below and in front of the apex of the mastoid process. The internal jugular vein, crossed by the accessory nerve, lies in front of the transverse process.
|
|
|
Figure 6.89 Atlas, from above. The epiphyseal junction between the ossification centre of the anterior arch and that of the right lateral mass has not fused completely. |
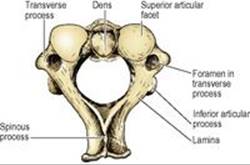
Some of the essential features of the axis are described on page 426. The dens (odontoid process) is characteristic, projecting up from the body between a pair of massive weight-bearing lateral masses (Fig. 6.78). The weight is communicated from these shoulders through the body to the body of C3 vertebra.
The transverse process has no anterior and posterior tubercles but ends in a rounded tip, which corresponds with the posterior tubercles of lower cervical vertebrae with equivalent muscle attachments. The foramen in the transverse process is not vertical as in the other vertebrae, but is directed upwards and outwards (Fig. 6.90) to communicate a lateral bend to the vertebral artery to enable it to ascend to the transverse process of the wider atlas (Fig. 6.84). An inferior articular process extends down from the junction of pedicle and lamina; its articular facet faces downwards and forwards as in typical cervical vertebrae (Fig. 6.78). The laminae are thick and rounded and project posteriorly into a massive spinous process (Fig. 6.90), the lower surface of which is grooved and ends in a wide bifurcation; the tip of the spinous process thus resembles an inverted U (Fig. 6.84).
|
|
|
Figure 6.90 Axis, from above. |
Thoracic vertebrae
A typical thoracic vertebra
The distinctive feature of a thoracic vertebra is the presence of costal facets (Fig. 6.91). On each side of the body of a typical thoracic vertebra there are a pair of semicircular demifacets (Fig. 6.92). The upper and larger of these is on the body at its junction with the upper border of the pedicle. The smaller lower facet is at the lower border of the body.
|
|
|
Figure 6.91 Typical thoracic vertebra, from above. |
|
|
|
Figure 6.92 Two articulated midthoracic vertebrae from the left. The intervertebral foramen is bounded in front by half of the body of the upper vertebra and the intervertebral disc, at the back by the facet joint, and above and below by pedicles. |
The body is concave from above down around its circumference. The posterior surface of the body is concave from side to side, making the body heart-shaped and the vertebral foramen almost circular in outline (Fig. 6.91). Two large foramina open centrally on the back of the body for the basivertebral veins. The upper and lower surfaces of the body have a heart-shaped ring of compact bone at their margins. This is the fused epiphyseal ring of the body, and it encloses a large central area in which cancellous bone reaches the surface.
The pedicle projects back from the upper half of the body. Its upper border is level with the upper surface of the body. The upper border of the pedicle curves up in a slight concavity to a superior articular process. The lower border curves markedly down to the inferior articular process, so making the upper boundary of the intervertebral foramen. This accommodates the thoracic nerve of the same number as the vertebra. The flat laminae slope downwards and backwards from the pedicles to unite in the midline and complete the neural arch. The superior articular process projects up from the junction of pedicle and lamina. It carries an oval articular facet facing backwards and slightly laterally; so the two articular surfaces lie on the arc of a wide circle, permitting rotation of adjacent bodies. The inferior articular facets are reciprocal, facing forwards and somewhat medially.
The spinous processes of successive thoracic vertebrae slope downwards with gradually increasing declivity as far as T7, below which they progressively level out to become almost horizontal at T12. Thus the tips of the upper four spines lie opposite the bodies of vertebrae one lower in the series, the next four spines (those of T5–8) opposite the upper margin of two vertebral bodies lower, and the lowest spines opposite one lower or their own vertebral bodies.
The transverse process projects backwards as well as laterally from the junction of pedicle and lamina. Its anterior surface expands towards the tip, to carry the characteristic costal facet. The upper six costal facets are concave, the lower ones flat, and the rib tubercles with which they articulate have correspondingly rounded or flat facets. Accordingly, when ribs elevate during inspiration, a rotational movement occurs at the upper costotransverse joints and a gliding movement at the lower joints. The primary curvature of the thoracic vertebral column results in the upper thoracic vertebrae leaning forwards, so their transverse processes are tilted up a little. Thus the neck of the first rib slopes backwards and upwards, a feature that enables the side to which it belongs to be determined (see p. 218).
First thoracic vertebra
The body is broad and not heart-shaped. On the body, at its junction with the pedicle, is a large round facet for the single articular surface of the head of the first rib which does not articulate with the body of C7 vertebrae. There is a demifacet for the second rib at the lower border of the body. The pedicle is attached below the upper margin of the body, as in a cervical vertebra, so the body takes part in the formation of the intervertebral foramen above it as well as below it. These are the foramina for the exit of C8 and T1 spinal nerves.
Lower thoracic vertebrae
The tenth, eleventh and twelfth thoracic vertebrae have only single facets on each side of their bodies for articulation with the heads of their same numbered ribs (Fig. 6.93). This facet is at, close to and somewhat below the upper border of the body of the tenth, eleventh and twelfth vertebrae respectively. The last two vertebrae have no costal facets on their small transverse processes. The twelfth vertebra has some lumbar features: the lower articular facet faces laterally and mamillary processes and accessory tubercles are present.
Lumbar vertebrae
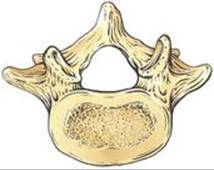
The bodies of lumbar vertebrae increase in breadth from above down, and this is reflected posteriorly by a progressive widening between the articular processes. Thus in L1 and 2 the four processes as seen from behind make a rectangle set vertically; in L3 they may also make a vertical rectangle, or they may be like those of L4 and make a square; in L5 they make a horizontal rectangle. The body shares with the smaller thoracic vertebrae the characteristics of being concave from above down, of having pedicles attached to its upper half, and of being perforated by a pair of basivertebral veins posteriorly. It differs from the heart-shaped thoracic vertebra in being kidney-shaped. The posterior surface is less concave from side to side, so the vertebral canal is somewhat triangular in cross-section (Fig. 6.94).
The transverse processes are variable in length, but the fourth is usually the longest (Fig. 6.74). The transverse process of the fifth, however, is quite characteristic. Short, massive, triangular, its base is attached to both the pedicle and the lateral side of the body itself (Fig. 6.95).
|
|
|
Figure 6.95 L5 vertebra from above. Compare with Figure 6.94 and note that the transverse process extends well forward on to the side of the body, a feature unique to L5. |
The pedicles are stout and form the upper and lower margins of the intervertebral foramina. The laminae do not show such a downward slope as in the thoracic vertebrae. The quadrangular spinous process is roughly horizontal. The upper border is straight but the lower border is concave.
The articular processes are characteristic. The upper pair rise up and carry articular facets that face medially (Fig. 6.94). The articular surfaces are concave from front to back. The lower pair of articular processes project down, face laterally and are convex from front to back.
The transverse processes are fused ribs (costal elements). The true transverse element consists of two small elevations with a groove between them occupied by the medial branch of the posterior ramus of the overlying lumbar nerve. The mamillary process is a convexity projecting back from the margin of the superior articular process; the smaller accessory tubercle lies below this, at the root of the transverse process (Figs 6.94 and 6.96).
The inferior articular processes of the fifth lumbar vertebra face well forwards, and are received into backward-facing facets on the sacrum, and this locking prevents L5 vertebra from sliding forwards down the slope of S1 vertebra. Furthermore, the adjacent bodies are strongly united by the intervertebral disc. Thus, although the sloping lumbosacral joint carries the whole body weight, it is extremely stable. A strongly contracting erector spinae acts as a supporting strap posteriorly. However, if the neural arch is disrupted between the superior and inferior articular processes, i.e. in the so-called pars interarticularis, the body of L5 tends to slip downwards and forwards (spondylolisthesis).
The fifth lumbar vertebra may be fused on one or both sides to the first sacral vertebra, a condition known as ‘sacralization’. More rarely the first sacral vertebra may be partially or completely separate (‘lumbarization’).
Sacrum
Five progressively smaller sacral vertebrae and their costal elements fuse to make this bone, which is triangular in outline and curved with a concavity towards the pelvis. On its lateral aspect it has an auricular surface for articulation with the ilium to make the upper posterior wall of the pelvis. Below the sacroiliac joints the sacrum tapers off down to its apex. The upper surface of the first sacral vertebra forms the base of the sacrum. The body of S1 vertebra is large, and wider transversely; its anterior projecting edge is the sacral promontory. Lateral to the body is the wing-like ala of the sacrum on each side, consisting of fused costal elements and transverse processes. The ala is crossed anteriorly by the sympathetic trunk, lumbosacral trunk and obturator nerve, in that order from medial to lateral. In the anatomical position the upper surface of the base slopes downwards and forwards at 30° or more. From here the sacrum is directed backwards before curving down over the pelvic cavity.
Pelvic surface
This concave surface is smooth (Fig. 6.97). Across the midline five diminishing bodies are fused, with four ridges persisting to mark the lines of ossification; these transverse lines represent the intervertebral discs. On each side are the four anterior sacral foramina. The rounded bars of bone between adjacent foramina (costal elements) represent the heads and necks of ribs. The medial boundaries of the anterior sacral foramina are thus formed by the bodies of the sacral vertebrae, but the other three-quarters of their circumference is costal in origin. The rounded bar of bone above the first sacral foramen continues the arcuate line of the ilium to form the posterior part of the pelvic brim (see p. 288).
The mass of bone lateral to the foramina, the lateral mass, is formed by fusion of the costal elements (shafts of ribs) with each other. It is deeply indented by grooves for the anterior rami of the upper four sacral nerves, which pass laterally from the anterior sacral foramina. Piriformis arises from the three ridges (costal elements) that separate the anterior foramina, and from the lateral mass nearby. The sacral anterior primary rami emerging from these foramina lie on piriformis behind its covering fascia (see Fig. 5.56, p. 292). Peritoneum is draped over the front of the upper two bodies and below that level the retroperitoneal rectum lies surrounded by the mesorectum (see p. 293). From the front of the lower sacrum the rectosacral fascia passes downwards and forwards to fuse with the mesorectum 3–5cm above the anorectal junction. Behind this fascia the median sacral artery and vein lie in the midline with some lymph nodes. On each side, the sacral sympathetic trunk lies medial to the sacral foramina, and the lateral sacral vessels lie in front of the piriformis fascia.
Dorsal surface
This convex surface is irregular and rough (Fig. 6.98). In the midline it is closed by fusion of adjacent laminae. The gap above the first sacral laminae is closed by the ligamenta flava attached to the laminae of L5 vertebra. The sacral hiatus below, variable in its extent, indicates failure of fusion of the laminae of S5 and often of S4 vertebrae. This hiatus is closed by fibrous tissue forming the superficial sacrococcygeal ligament. Adjacent spinous processes are fused with each other to produce a midline ridge, the median sacral crest, that projects dorsally from the fused laminae. The superior articular process on S1 vertebra carries a backward facing facet for the synovial joint with L5 vertebra. Below this, medial to the posterior foramina is a line of irregular tubercles that represent fusion of adjacent articular processes of the sacral vertebrae. This low ridge forms the intermediate sacral crest and it is projected below, alongside the sacral hiatus, to end in the rounded sacral cornu. Lateral to the superior articular process is a prominent boss of bone which is the transverse process of S1 vertebra. Below this the transverse processes are fused with each other, making a ridge, the lateral sacral crest, lateral to the posterior foramina. It is marked by bosses of bone that represent the tips of the fused transverse processes. The fused costal elements lie lateral to the lateral sacral crest. The gutter between the median and lateral sacral crests is filled by erector spinae, and the posterior layer of the lumbar fascia that covers it is attached to both crests. Between the lateral sacral crest and the auricular surface are deep fossae for the attachment of the posterior sacroiliac ligament.
Sacral canal
This is triangular in cross-section and curves with the sacrum. The sacral canal contains the meninges which extend down to S2 vertebra. From here the filum terminale (pia mater), piercing the dura, runs down to blend with the periosteum on the back of the coccyx. The space around the dura mater and its prolongations is filled with loose fat and the internal vertebral venous plexus. The posterior root ganglia are contained within the sacral canal and the anterior and posterior rami of sacral nerves emerge separately from the anterior and posterior sacral foraminae.
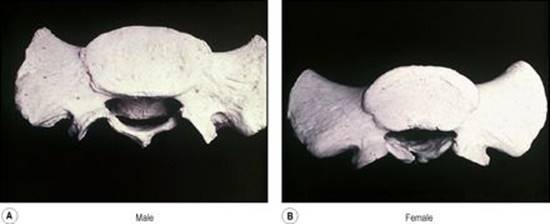
Sex differences are present in the sacrum. The most useful guide is the comparison of the width of the body of S1 vertebra with the width of the lateral mass, or ala. The body is wider than the ala in the male equal to or narrower than the ala in the female (Fig. 6.99). Other differences lie in the curvature of the bone. In the male the anterior surface is gently and uniformly concave; in the female it is flat above and turns forward more prominently below. The auricular surface occupies two and a half vertebrae in the male, but is smaller in the female and may be restricted to two vertebrae.
|
|
|
Figure 6.99 Male and female sacrum from above. In the male the body of the first sacral vertebra is broad and the alae narrow; in the female the body and the alae broad are of approximately equal width. |
Coccyx
This is contracted into four pieces fused together into a small triangular bone joined by its base to the apex of the sacrum at the sacrococcygeal joint (see p. 325). At each side a lateral sacrococcygeal ligament joins the transverse process of the first piece of the coccyx to the inferolateral angle of the sacrum and completes the foramen for S5 nerve anteriorly; posteriorly the foramen is closed by the sacral and coccygeal cornua connected by the intercornual ligament. The upper surface of the coccyx is in the pelvic floor, the lower surface is in the buttock, beneath the skin of the natal cleft.
Development of vertebrae
The vertebrae develop from the sclerotome parts of the mesodermal somites (see p. 23). The sclerotomes surround the notochord and neural tube in a sheath of mesoderm. A series of hyaline cartilaginous rings appears in the mesodermal sheath. Each ring is formed by fusion of adjacent halves (caudal and cranial) of the original somites. Thus the vertebrae lie not in segments of the body wall, but in the intersegmental planes.
Each ring ossifies in three centres to form the centrum and the two halves of the neural arch of a vertebra. The centre for the centrum is initially double, but the two areas rapidly fuse; failure of one half results in a hemivertebra; a series of hemivertebrae is one cause of congenital scoliosis (lateral curvature of the spine). By the eighth week of fetal life ossification has commenced in the centrum and the two halves of the neural arch. At birth a vertebra consists of three ossifying parts, centrum and two half arches, united by cartilage. The half arches unite in the first year after birth, first in the lumbar, then thoracic and finally cervical regions. The centra unite with the arches first in the cervical region, about the third year, but in the lumbar region this union is not complete until the sixth year. Failure of fusion of the vertebral arches in the midline results in the condition known as spina bifida. When the overlying skin is intact this is qualified as being occult. A more severe developmental defect results in a cerebrospinal fluid-filled sac (meningocoele) or a sac containing a part of the spinal cord and nerve roots (myelomeningocoele) being exposed on the surface. These defects are more common in the lumbar or lumbosacral region.
The vertical cylindrical surface of the body is covered with compact bone, but the cancellous bone on the flat upper and lower surfaces remains covered with a layer of hyaline cartilage. The epiphyses for the body appear as bony rings, upper and lower, soon after puberty. They are ridged and grooved reciprocally with the margins of the surfaces of the body (Fig. 6.100). Fusion of the epiphyseal ring and body occurs in the early twenties. Soon after puberty secondary centres appear also at the tip of the spinous process (double in the bifid spines of the cervical vertebrae) and at the tips of the transverse processes of all the vertebrae, and in the mamillary processes of T12 and the lumbar vertebrae. These fuse in the early twenties. The costal elements of cervical and lumbar vertebrae do not have a separate bony centre, but ossify by direct extension from the neural arch. An occasional centre in the costal element of C7 or L1 vertebra may lead to the formation of a cervical or lumbar rib. On the other hand the weight-bearing costal elements of the sacrum have primary ossification centres. In general the development of the five segments of the sacrum resembles that of typical vertebrae. After puberty these segments coalesce from below upwards.
|
|
|
Figure 6.100 L5 vertebra from above. The neurocentral junction has not yet completely ossified. The radial grooves around the anterolateral convexity of the body indicate that the epiphyseal ring had not united. |
The atlas ossifies in the seventh week of fetal life by a centre in each lateral mass. These extend around the posterior arch and unite at the fourth year. In the meantime a centre in the anterior arch has appeared at the first year. Its junction with the bone of the lateral mass cuts across the anterior part of the upper articular surface; these epiphyses fuse at 7 years. This epiphyseal junction may permanently divide the articular surface (as in Fig. 6.89, right side).
Each half of the neural arch of the axis ossifies from a primary centre in the second month; a pair of centres for the centrum, which soon fuse, ossify in the fourth month. The dens is mainly ossified from a pair of centres which appear in the sixth month and join before birth. Thus at birth the axis is in four parts and these fuse with each other in the first few years thereafter; but although the cartilage between the dens and the body ossifies circumferentially, the centre may remain cartilaginous till old age. A secondary centre for the tip of the dens appears at about 6 years and unites with the rest of the dens at about 12 years. As in the case of a typical vertebra, a secondary centre for the lower surface of the body appears at puberty and fuses in the early twenties.